
Abstract
Emerging adults (18–25) experience disproportionate rates of substance use compared to other ages. They also experience a higher level of stress due to an increased need to become self-reliant. This study examines the effects of perceived and COVID-19 related stress on the use of coping strategies and polysubstance use. Participants (N = 117; mean age 19.9 years; 75% female; 32% White) were undergraduates from the MAPme Study. Data was collected during Fall 2020. Multiple regression and path analysis of self-report data from the ASSIST, Brief COPE, PSS, and EPII scales were conducted. Perceived stress was positively (β = 0.38, 95% CI [0.20, 0.57]) and negatively (β = −0.19 [−0.38, 0.001]) associated with avoidant and active coping, respectively. Avoidant coping was positively associated with polysubstance versus mono-substance use (β = 0.46, 95% CI [0.01, 0.91]. Findings indicate that avoidant coping strategies are associated with an escalation of substance and suggest that coping choice may minimize risk for engaging in polysubstance use.
Introduction
Epidemiology of (poly)substance use
In 2020, emerging adults, those 18–25, had the second highest rates of alcohol use compared to other age groups with an estimated 17.3 million people (51.5%) reporting heavy alcohol use, defined as 5+ drinks for females, 6+ drinks for males on five or more days in the past month (NSDUH, 2021). Emerging adults also had the highest rates of cannabis use compared to other age groups, and the second highest rates of tobacco use with 2.9 million (8.6%) reporting cannabis use and 4.7 million (13.9%) reporting cigarette smoking within the past month (NSDUH, 2021). These trends highlight that alcohol, cannabis, and tobacco were disproportionately used by emerging adults compared to other ages.
Since the end of the COVID-19 pandemic, emerging adults have continued to disproportionately use alcohol, cannabis, and tobacco compared to other age groups. The 2022 National Survey of Drug Use and Health (NSDUH) report indicated that 50% of emerging adults consumed alcohol in the past month, compared to 7% for those aged 12–17 (NSDUH, 2022). Further, the proportion of emerging adults consuming alcohol was similar to the proportion of individuals 26 and above, although the latter group has a much larger sample size. Comparable patterns were found for tobacco and cannabis consumption (NSDUH, 2022); indeed, 38.2% of emerging adults consumed cannabis compared to 11.5% for 12–17 and 20.6% for those 26+ years old. In 2023, young adults aged 18–25 had the highest rates of substance use disorder, highest rates of binge drinking in the past month, and highest rates of illicit drug use (NSDUH, 2023). Importantly, findings from NSDUH data post-pandemic (2020 on) noted rising rates of polysubstance use among emerging adults, and specific increases in past month co-use of alcohol with other drugs (NSDUH, 2022).
Polysubstance use, defined as the concurrent use of more than one substance within a given time frame, is associated with poorer health outcomes compared to single substance use, including higher rates of psychopathology as well as decreased memory and decision-making abilities (Connor et al., 2014). In the NSDUH, the rates of alcohol co-use with cannabis and other illicit drugs increased from 19% in 2019 to 21% in 2020 (NSDUH, 2021). Further, there were significant increases of concurrent substance use disorder of alcohol and another drug in emerging adults from 5.9% in 2021 to 7.2% in 2022 (NSDUH, 2022). The increases in both single and polysubstance use in emerging adults highlight the need to further explore this age range and their substance use patterns.
The role of stress on substance use
Stress, defined as emotional or mental strain resulting from adverse or demanding circumstances, is associated with increased substance use in emerging adults (Aseltine and Gore, 2000; Brikmanis and Doran, 2017; King et al., 2018; Windle et al., 2004). Indeed, stress has been associated with a variety of substances and substance use problems, including but not limited to alcohol, nicotine, and cannabis use (Aseltine and Gore, 2000; Brikmanis and Doran, 2017; Clendennen et al., 2021; King et al., 2018; McCreary and Sadava, 2000; Windle et al., 2004). Stressful circumstances have also been associated with increased alcohol use, substance involvement, and substance abuse in emerging adults (Najavits et al., 2017; Roth and Cohen, 1986; Van Den Brink, 2015). A common motive for alcohol use is “using to temporarily reduce negative affect and feelings of stress” (Sinha, 2012). Research supports the diathesis-stress-model of alcohol consumption, which asserts that individual biological predisposition combined with a stressful environment may precipitate increases in consumption (McGrath et al., 2016). Transitioning from high school to college generally comes with an increase in subjective stress (Kerr et al., 2024). This transitional-period stress is associated with increased alcohol use and is often related to social adjustments, rigorous course loads, changes in sleeping and eating habits, and the onset of new responsibilities (Misra and Mckean, 2000; Ross et al., 1999). Public health issues, such as a global pandemic, may also increase stress for individuals.
The COVID-19 pandemic provided a naturalistic experiment of the direct and indirect effects of a stressful situation. Several studies evidenced an increase in an individual’s stress resulting from an inability to control different aspects of their lives; this was particularly true for college students and emerging adults (Johnson et al., 2010; Kroshus et al., 2021; Zhao et al., 2023). Studies have reported that COVID-19 pandemic stress was accompanied by an increase in cannabis, tobacco, and alcohol consumption in emerging adults (Clendennen et al., 2021; Lechner et al., 2021; Papp and Kouros, 2021; Romm et al., 2021). The overall increases in substance use led to greater negative impacts of drug use, including drug overdose deaths (Glober et al., 2020; Imtiaz et al., 2021; Macmadu et al., 2021). COVID-related stress has also been associated with increased depressive symptoms, increased anxiety and a lower ability to cope with stress, resulting in greater presentation of psychopathology (Mushquash and Grassia, 2022; Wang et al., 2020). In a study by Singleton et al. (2023), COVID-related anxiety was positively associated with alcohol and drug use in college students. Overall, these findings suggest a relationship between daily/perceived stress, as well as COVID-specific stress, and substance use, however, much of the literature focuses on individual substance use behaviors, and few studies have examined the negative effect of stress on polysubstance use. Relatedly, assessment of COVID-specific stress effects in the context of daily stressors in an individual’s life has been limited. In other words, failure to evaluate the effect of COVID-specific stressors on human behavior, above typical daily stressors, could lead to biased interpretations.
Substance use & other stress coping skills
While stress is an important risk factor for drug initiation, maintenance, and relapse, the utilization of alternative stress coping skills can be a protective factor (Asberg et al., 2008; Murberg and Bru, 2005; Sinha, 2008). Lazarus and Folkman (1984) proposed an appraisal-based model which defines coping as a response to specific stressful situations, rather than as a stable feature of personality. One’s cognitive appraisal of the situation in terms of challenge, threat and potential benefit, have been found to mediate the relationship between stressors and coping response. A model proposed by Moos and Holahan (2003) emphasizes transitory environmental conditions, such as new life events, which helps to shape coping responses. The literature has identified two groups in which coping strategies tend to fall in: avoidant and active coping.
Avoidant coping strategies direct attention away from a stressor, such as denial of the problem, distraction, and withdrawal from a stressful situation (Taylor and Stanton, 2007). Avoidant coping strategies are associated with poorer mental and physical health outcomes (Chaaya et al., 2025; Taylor and Stanton, 2007). It is important to note that substance use can be considered a form of stress coping (Rice and Van Arsdale, 2010; Taylor and Stanton, 2007). Utilizing other avoidant coping strategies is associated with increased substance use in those with substance use disorder (Naquin and Gilbert, 1996) and negatively associated with abstinence from tobacco in the general population as well as smoking cessation in college students (Hyman and Sinha, 2009). Avoidant coping strategies were also associated with increased cannabis and alcohol use-related problems in adolescents and an increased escalation of cannabis use from adolescence to young adulthood (Eftekhari et al., 2004; Unger et al., 2003). Further, avoidance coping, such as denial and withdrawal, is generally associated with psychological distress and maladaptive behavioral outcomes (Rohde et al., 1990).
In contrast, active coping strategies are aimed at addressing the stressor, such as through problem solving or by seeking emotional support (Taylor and Stanton, 2007). Active coping strategies have been associated with decreased substance use cravings in alcohol use and substance use disorders (Cleveland and Harris, 2010; Moos, 2007; Taylor and Stanton, 2007). Active coping has also been associated with increased abstinence from alcohol and may act as a protective factor against cannabis use during adolescence (González-Yubero et al., 2021; Moser and Annis, 1996; Rothenberg et al., 2020). Further, individuals who rely more on active compared to avoidant coping responses tend to adapt better to life stressors and experience fewer psychological symptoms (Holahan and Moos, 1987).
Another type of coping has also been defined in the literature, religious coping. Religious coping has been described as both active and avoidant, depending on the individual (Pargament et al., 2000). Indeed, there have been mixed results in the literature when using measures of spirituality and prayer (Ano and Vasconcelles, 2005; Taylor and Stanton, 2007). In its active form, a person seeks spiritual connectedness to cope (Pargament et al., 1998). In its avoidant form, individuals struggle to find significance in life to cope with stress (Pargament et al., 1998). In a meta-analysis on the effects of religious coping on mental health, previous studies have found that active religious coping was associated with better psychological adjustment, and avoidant religious coping was associated with poorer psychological adjustment to stress (Ano and Vasconcelles, 2005). Importantly, most people employ multiple coping behaviors when facing stress and may choose both avoidant and active coping skills. Although research suggests that people may have trait-like tendencies toward dispositional coping styles (Ghadimi et al., 2018; Ptacek et al., 2006). Overall, research suggests that avoidant coping is more frequently associated with negative substance use outcomes, whereas active coping has been associated with lower levels of substance use and problems.
To-date, much of the research on coping strategies and substance use focuses on single substance use. There are few studies describing specific profiles of coping strategies in the context of polysubstance use. It is possible that compared to those who choose to engage in single substance use, those who choose to engage in polysubstance use may differ in their number of daily stressors and/or how much they employ specific types of stress coping strategies. Further, substance use itself may cause additional stressors if it interferes with school or relationships. The increased rates of polysubstance use in emerging adults may indicate a failure to employ coping strategies that are protective against substance use compared to those who engage in single substance use. Further, few studies have examined how substance use patterns may be affected by increased challenges to cope with higher stress posed by the COVID-19 pandemic (Son et al., 2020).
Current study goals
We examine the relationships between perceived stress, stress specifically attributable to COVID-19, coping strategies used during the COVID-19 pandemic, and substance use. As coping strategies are used to alleviate stress, we hypothesized that higher levels of either general-perceived or COVID-19-specific stress would be associated with greater frequency of all types of coping strategies. We also hypothesized that participants who use active coping mechanisms would be less likely to endorse polysubstance use compared to participants who use avoidant coping mechanisms more frequently. Due to the mixed literature regarding religious coping strategies, no specific hypothesis regarding the associations between religious coping and polysubstance use endorsement was made. Finally, path models with type of coping strategy as the mediator between both perceived and COVID-19 stress, and polysubstance use were tested.
Materials and method
Sample
The current study used data from the MAPme Study, which was a prospective survey of college students that began in Fall 2018. Participants completed self-report surveys each semester (i.e. “waves”) until graduation. The overall sample at Wave 1 consisted of 303 participants, with 69.6% female (n = 211), 29.7% male (n = 90), and a mean age of 18.58 years (SD = 0.39). Participants were compensated with a $15 gift card for completing the survey.
Analyses for the current study focused on a subset of individuals (N = 117) who participated in the study during Wave 6, which occurred in Fall 2020 during the COVID-19 pandemic and corresponded with the start of the students’ third year in college/university. The sample was predominantly female (N = 86; 74.8%), with a mean age of 19.9 years (SD = 0.41), and racially mixed – with participants who self-identified as White (31%; N = 36), Black (4%; N = 5), Asian (43%; N = 50), Hispanic (2%; N = 2), and Mixed (18%; N = 21). Due to the attrition of our sample from Wave 1 to Wave 6, study variables at Wave 1 were compared across participants who did and did not complete Wave 6 (Table 1). We found no significant differences in stress (t = 1.22, p = 0.22) or the number of substances used (t = 1.79, p = 0.08) at Wave 1 between MAPme participants who completed Wave 6 of the survey and participants who did not.
Comparison of participants at baseline to subset participants at Wave 6.
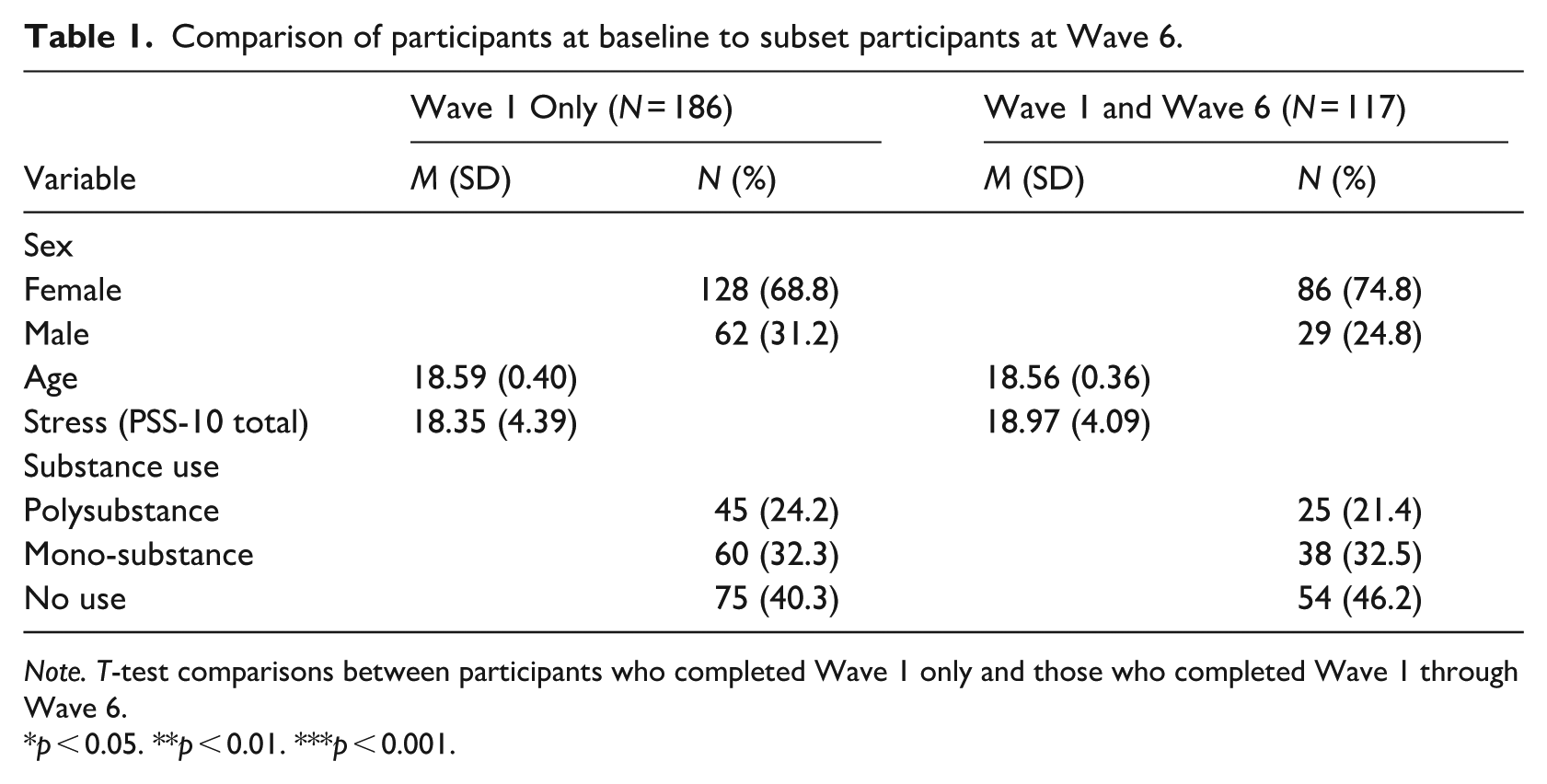
Note. T-test comparisons between participants who completed Wave 1 only and those who completed Wave 1 through Wave 6.
p < 0.05. **p < 0.01. ***p < 0.001.
Ethical statement
The MAPme Project was approved by the Institutional Review Board of Emory University and informed consent for participation and publication of results was obtained prior to data collection (IRB00096137).
Measures
For the current analyses, all measures were administered on REDCap using established behavioral assessments.
Polysubstance use
Substance use was assessed using the Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST), which has been found to be reliable and valid among multiple samples and university students (Group, 2002; McNeely et al., 2014; Onifade et al., 2014). Polysubstance use was defined as the use of at least two of the following substances within the past 3 months: alcohol, tobacco, or cannabis. Analyses compared polysubstance use to no-use (i.e. no substance use) and to monosubstance use (i.e. where participants endorsed using only one type of substance in the past 3 months).
Stress coping strategies
Coping strategies were assessed using the Brief Coping Orientation to Problems Experienced (COPE) survey. The Brief COPE has been shown to be valid and reliable across multiple samples and each item is scored using a Likert scale from 1 to 4 (1 = “I haven’t been doing this at all”, 2 = “I’ve been doing this a little bit”, 3 = “I’ve been doing a medium amount”, 4 = “I’ve been doing this a lot”; Rahman et al., 2021; García et al., 2018; Nunes et al., 2021). Scores were calculated to reflect (a) the frequency of use and (b) the number of avoidant, active, and religious coping strategies. Avoidant coping included four items measuring denial, behavioral disengagement, and withdrawal from a stressful situation, with a minimum score of 4 and a maximum score of 16. While substance use has also been cited as an avoidant coping strategy, it was excluded from the avoidant coping strategies score as to not bias the analyses. Active coping included six items measuring efforts to address the source of the stress, such as, planning, problem-solving, and emotional support, with possible scores ranging from 6 to 24. Religious coping included two items measuring attempts to find comfort in spiritual and religious beliefs, prayer, and meditation, with possible scores ranging from 2 to 8.
Perceived stress
Stress was defined as a continuous sum score measured using the Perceived Stress Scale (PSS) questionnaire (Anwer et al., 2020; Roberti et al., 2006). The current study used the 10-item version of the PSS which has been shown to have better psychometric properties compared to the PSS-14; possible scores range from 0 to 56 (Lee, 2012). In the present sample, the PSS-10 had good internal reliability (α = 0.91).
COVID-19 related stress
To account for COVID-19 specific stressors that may not be captured by the PSS-10 scale, a 20-item version of the Epidemic-Pandemic Impacts Inventory assessed COVID-19 cumulative stress and COVID-19 total stressors (Williams et al., 2023). COVID-19 cumulative stress reflected how the participants perceived that the COVID-19 pandemic had impacted their stress levels. For example, an answer to the question “How has the coronavirus crisis changed your stress levels?” was coded as +2 = “Worsened them significantly,” +1 = “Worsened them moderately,” 0 = “No change”, −1 = “Improved them moderately” and −2 = “Improved them significantly.” COVID-19 total stressors were indicated by the number of stressors due to COVID-19 the participant endorsed experiencing. This included questions such as, “Since the onset of the coronavirus/COVID-19 crisis: have you been suspected of having coronavirus/COVID-19 infection?” and “Has anyone in your family been diagnosed with coronavirus/COVID-19?.” Endorsing yes to experiencing a stressor was coded as 1. The range of possible scores of the COVID-19 total stressors was 0–12.
Statistical analyses
Data cleaning, preparation and generation of descriptive statistics were conducted in R [version 4.1.3] (R Core Team, 2020). Study hypotheses were tested using several path models conducted in Mplus [version 8] (Muthén and Muthén, 2017). Models were fitted using full information maximum likelihood assuming the data are missing completely at random. There are known associations between a person’s level of perceived stress, their substance use, and their coping strategies (Park et al., 2004; Rice and Van Arsdale, 2010; Sebena et al., 2012; Tavolacci et al., 2013). Therefore, we examined the direct and indirect effect (i.e. mediation) of perceived stress and COVID-19-specific stress on polysubstance use versus mono substance use, and on polysubstance use versus no substance use, via various coping strategies (Figure 1). All forms of coping strategies were modeled individually as mediators to account for use of multiple forms of coping. We fitted a model using each exogenous variable (perceived stress and both types of COVID-19 stress) separately and jointly. All analyses controlled for participant age, sex, and race (coded as White vs Non-White).
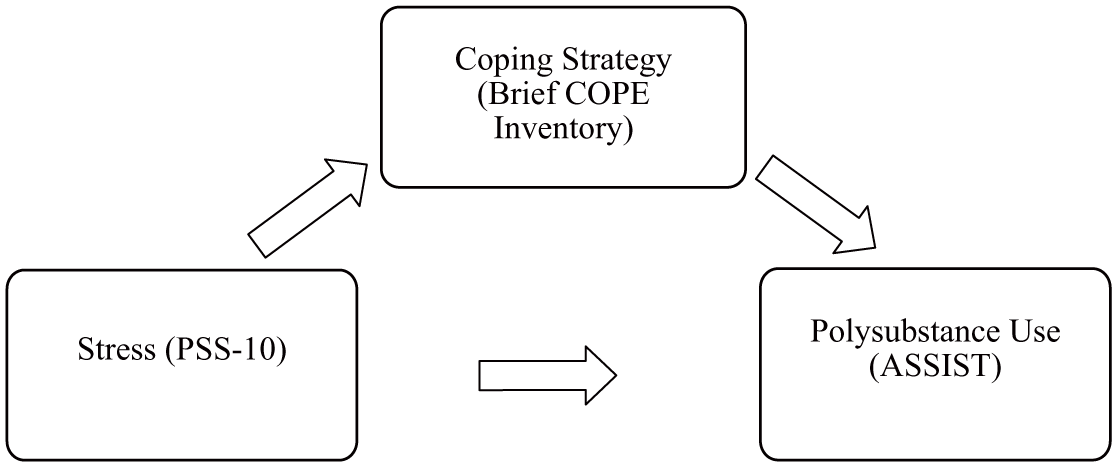
Proposed path model.
We also tested multinomial logistic regressions to examine the effect of perceived stress and frequency of active, avoidant, and religious coping. In the multinomial logistic regression models, the “polysubstance use” category was selected as the reference group. As such, we modeled the odds of a participant endorsing (A) “monosubstance use” versus polysubstance use or (B) “no substance use” versus polysubstance use. Standardized regression coefficients and bootstrapped 95% confidence intervals are reported. Results are interpreted with respect to polysubstance use as the most severe possible outcome. There are some limitations to multinomial logistic regression, such as requiring a large enough sample size to derive reliable parameter estimates. Multinomial logistic regression also relies on assumptions such as the independence of irrelevant alternatives (IIA), which states that the odds of choosing one option over another are independent of the presence or absence of additional alternatives. For the current study, this assumption is met.
Results
Sample descriptives
Generally, substance use was prevalent in the sample, but substance use patterns varied. Approximately 41.9% (N = 49) of participants engaged with no substances (no use), 28.2% (N = 32) primarily used only one substance (mono-use), and 29.9% (N = 28) consumed multiple types of substances in the past 3 months (polysubstance use; Table 2). Focusing on rates of specific substances used across mono- and poly substance use, the majority (57.2%; N = 67) of participants endorsed alcohol use, 16.2% (N = 19) reported tobacco use, and 23.9% (N = 28) used cannabis. The average level of perceived stress observed suggested moderate (M = 20.07, SD = 0.41) stress. Lastly, participants reported that the COVID-19 pandemic moderately worsened their stress levels (M = 1.56, SD = 0.24; Table 2).
Descriptive statistics for participants at Wave 6 (N = 117).
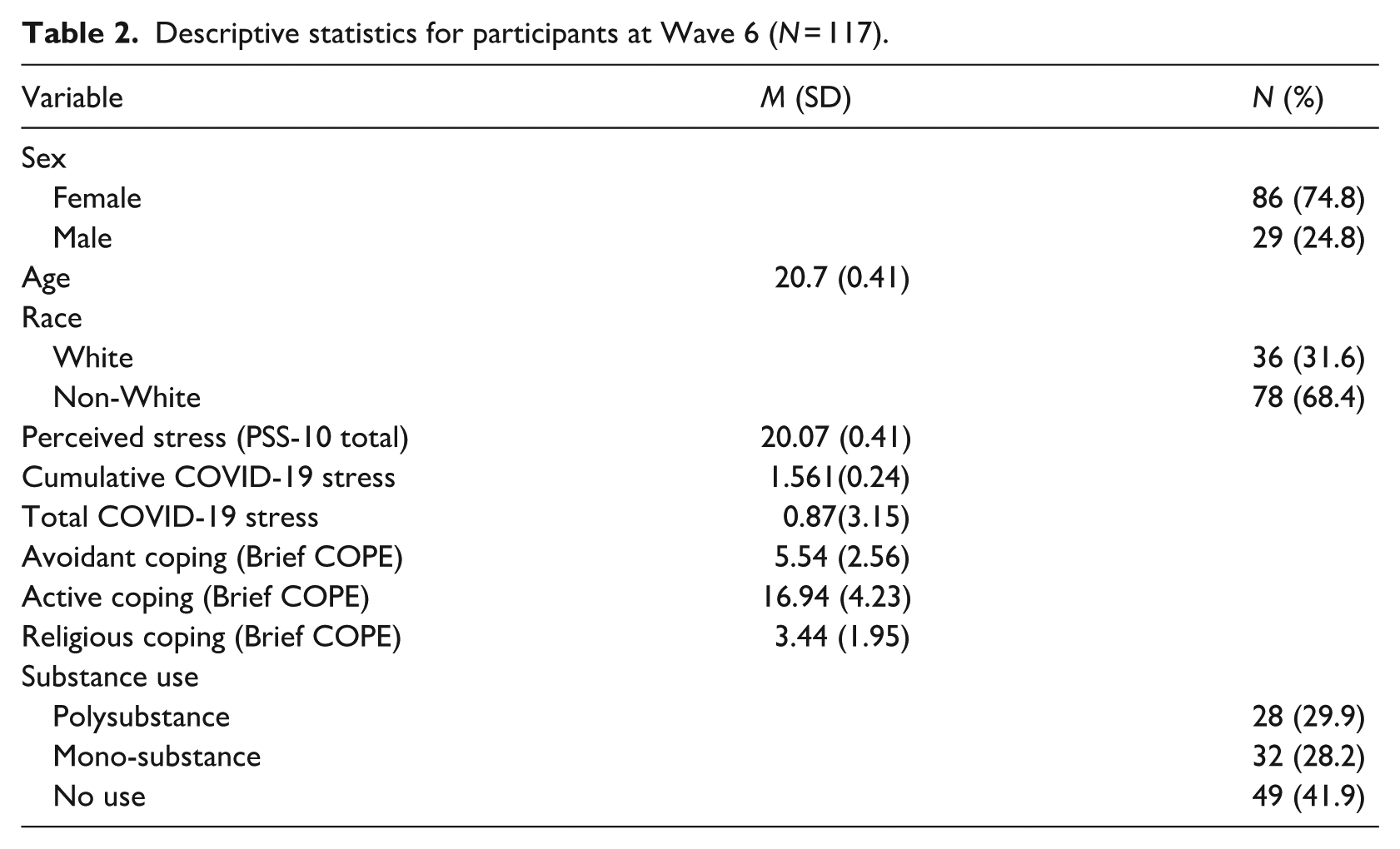
The average frequency of use of avoidant, active, and religious coping strategies varied. With a minimum possible score of 4, the average score for avoidant coping was 5.54 (SD = 2.56) with a maximum score of 16. Comparatively, participants frequently used active coping (minimum = 6, mean = 16.94, SD = 4.23, maximum = 24), reflecting that most of the items of active coping were used “a little bit” or more frequently. When considering religious coping, the average score was a 3.44 (SD = 1.95) with a minimum score of 2 and the highest possible score being an 8, indicating that participants used religious coping moderately frequently. On average, each person rated a score of 2 for each of the two religious coping items, indicating using the strategies “a little bit.”
Table 3 shows zero order correlations between study variables. The correlations between religious, active, and avoidant coping were modest, suggesting that individuals relied primarily on one strategy rather than combinations of them. As expected, general perceived stress was moderately positively correlated with avoidant coping (r = 0.48). Further, both types of COVID-19 related stress were positively correlated with each other (r = 0.25), and perceived stress was solely positively correlated with cumulative COVID-19 stress (r = 0.42).
Zero-order correlations between study variables at Wave 6.
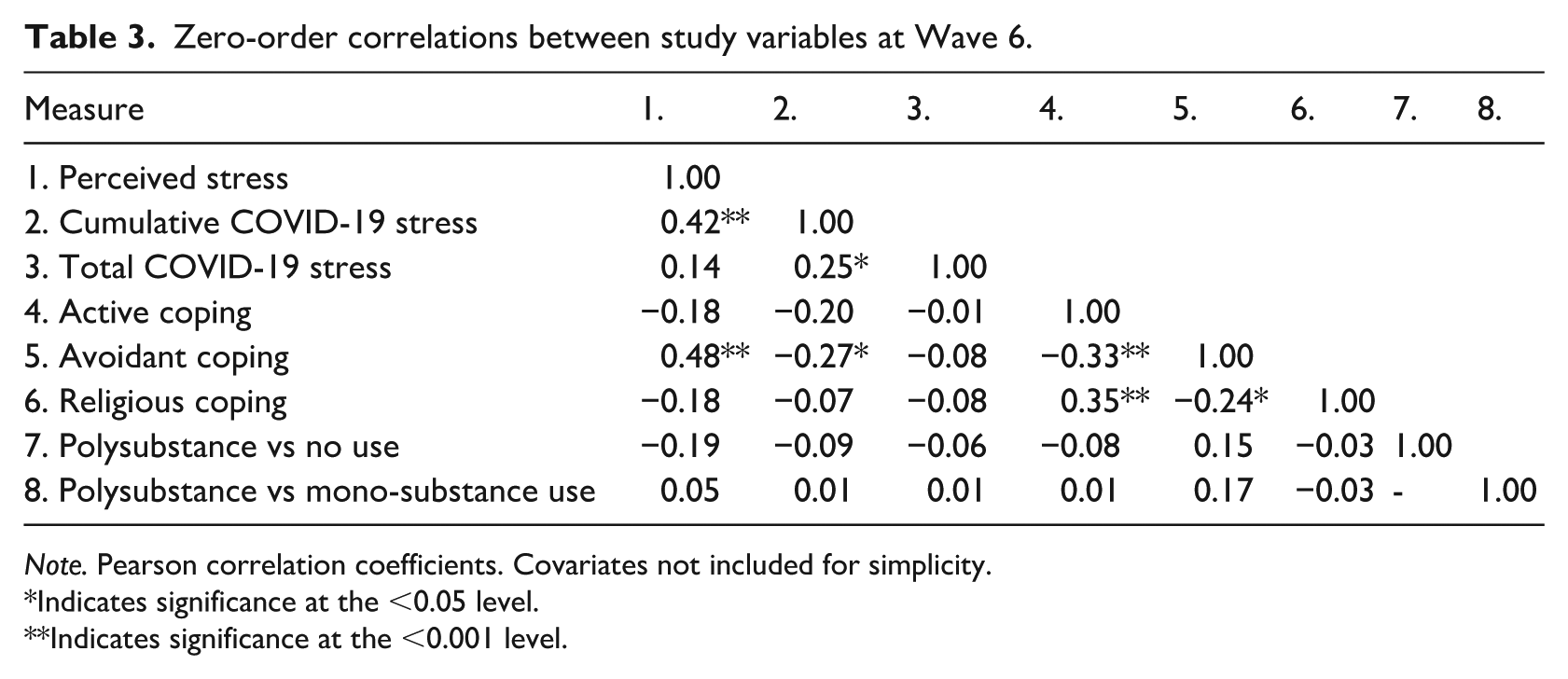
Note. Pearson correlation coefficients. Covariates not included for simplicity.
Indicates significance at the <0.05 level.
Indicates significance at the <0.001 level.
Stress effects on coping strategies and polysubstance use
Table 4 summarizes the direct and indirect effects of perceived stress, cumulative COVID-19 stress, and total COVID-19 stress on drug use; none of our models demonstrated a significant effect of the covariates, as such they are excluded from our tables for simplicity. We found limited evidence for an effect of COVID-19 stress on coping styles over and above perceived stress (see Supplemental Table 1 and Table 4). Perceived stress had a positive direct effect on the likelihood of reporting polysubstance use versus “monosubstance use” across models accounting for active (β = 0.22, 95% CI [0.01, 0.36]) and religious coping (β = 0.26, 95% CI [0.05, 0.47]; Table 4). Perceived stress also had a negative direct effect on polysubstance use versus “no substance use” when avoidant coping was the mediator (β = −0.49, 95% CI [−0.83, −0.16]). Overall, this pattern of results indicates that as stress increases, those who use substances may be more likely to engage in polysubstance use, whereas those who do not typically use, continue not to use. Importantly, perceived stress had a positive indirect effect on polysubstance use when comparing those who used multiple substances to those who used no substances, and avoidant coping was robustly associated with increased likelihood of polysubstance use (β = 0.48, 95% CI [0.21, 0.76]).
Multiple regression showing effects of stress across different levels of substance use, with each coping strategy as a mediator.
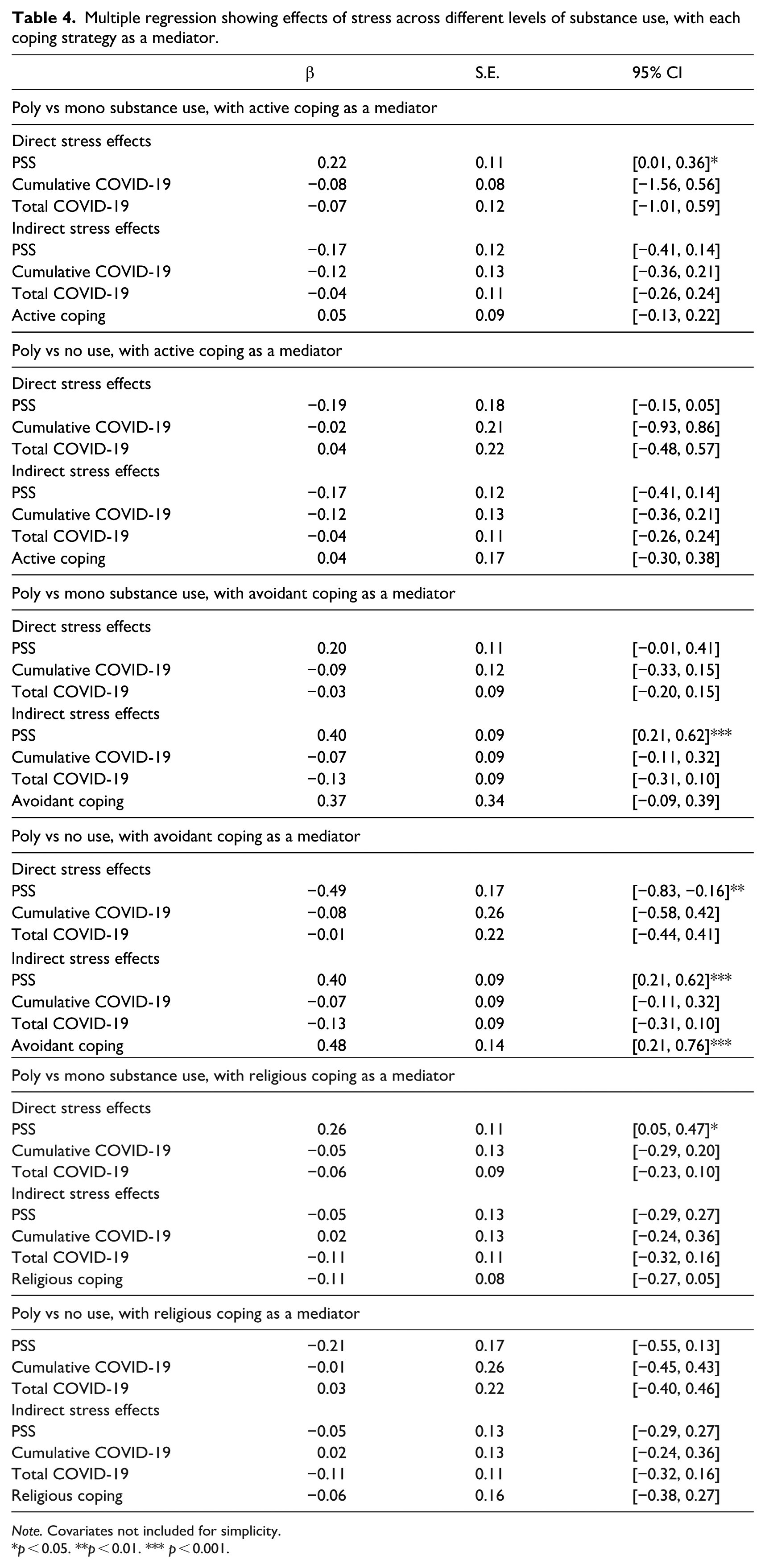
Note. Covariates not included for simplicity.
p < 0.05. **p < 0.01. *** p < 0.001.
When adjusting the model to solely examine perceived stress, we observed that greater perceived stress was positively associated with higher levels of avoidant coping (β = 0.38, SE = 0.09; Figure 2). This aligns with our hypothesis, that higher stress levels would be evident among individuals engaging in greater use of avoidant coping strategies. Furthermore, individuals who used active coping styles tended to have lower levels of stress (β = −0.19, SE = 0.10).
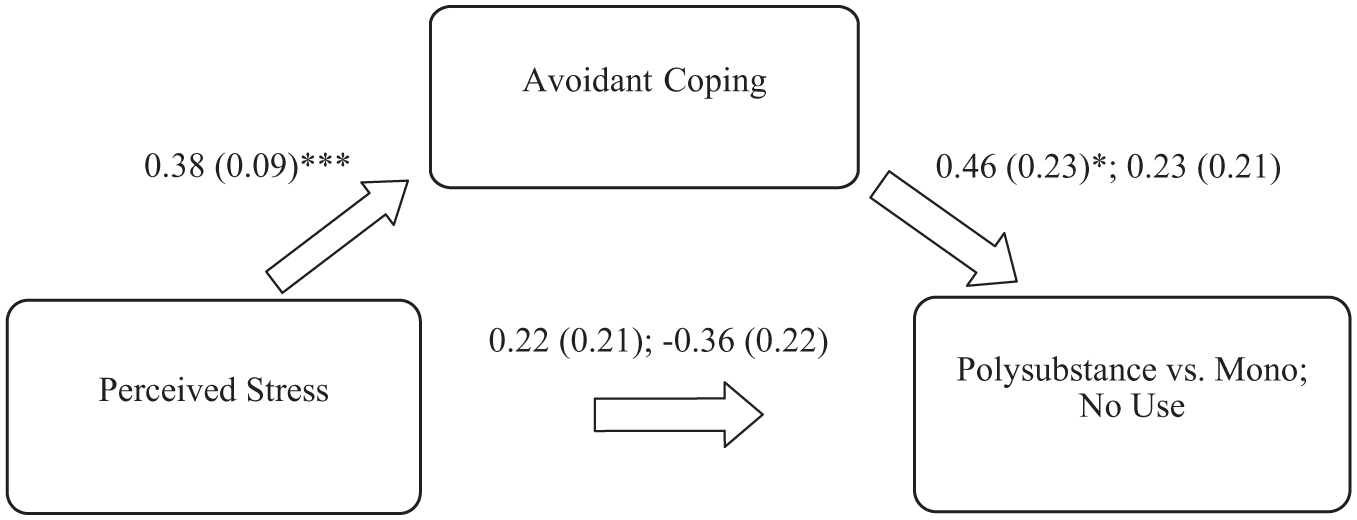
Path model showing association between perceived stress, avoidant coping strategies, Second values for polysubstance versus no use.
Coping strategies effects on polysubstance use
Figures 2–4 summarize the path models examining the association between perceived stress, coping strategies, and substance use level. Avoidant coping was positively associated with polysubstance versus monosubstance use (b = 0.46, 95% CI [0.01, 0.91]; odds-ratio (OR) = 1.48 [1.09, 2.02]) but not polysubstance versus no use (b = 0.23, 95% CI [−0.19, 0.64]; Figure 2). Active coping was not associated with polysubstance versus monosubstance use nor polysubstance versus “no use” (Figure 3). Neither was religious coping for monosubstance versus “no use” (Figure 4). Overall, greater use of avoidant coping strategies increased the likelihood of polysubstance use compared to monosubstance use in this sample, supporting the previous hypothesis; all these models described the data well, with r-squared estimates greater than 0.20 (Table 5).
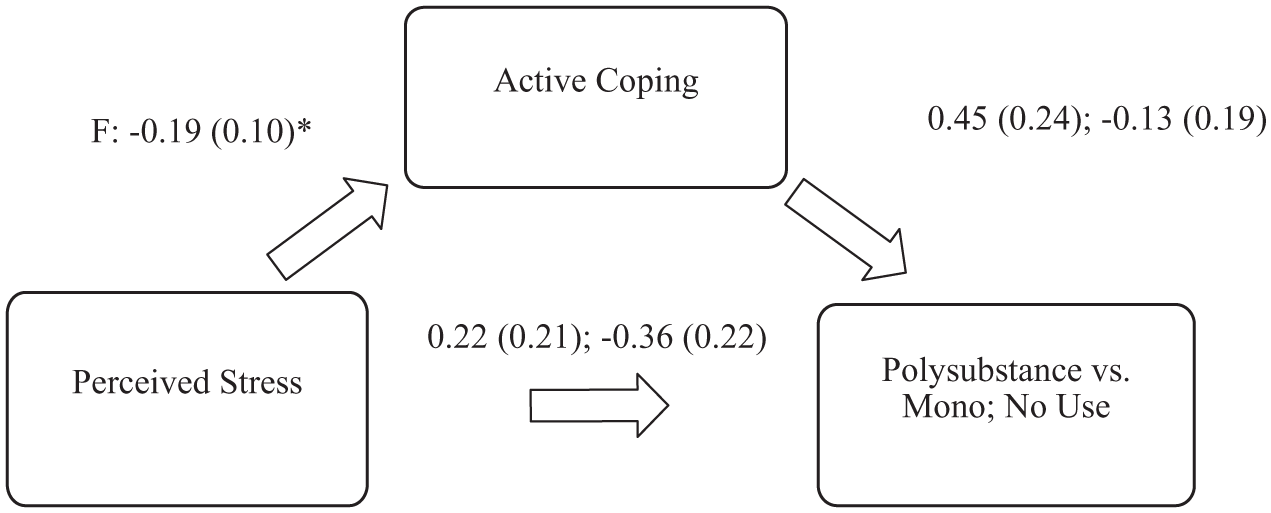
Path model showing association between perceived stress, active coping strategies, and polysubstance use second values for polysubstance versus no use.
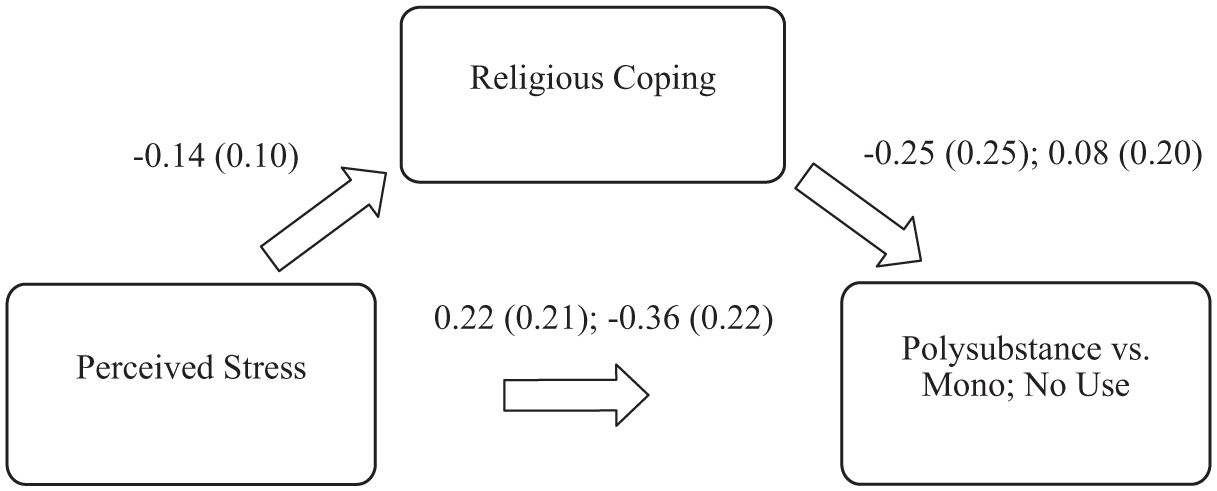
Path model showing association between perceived stress, religious coping strategies, second values for polysubstance versus no use.
R-squared statistics for the models of perceived stress and different coping strategies on substance use.
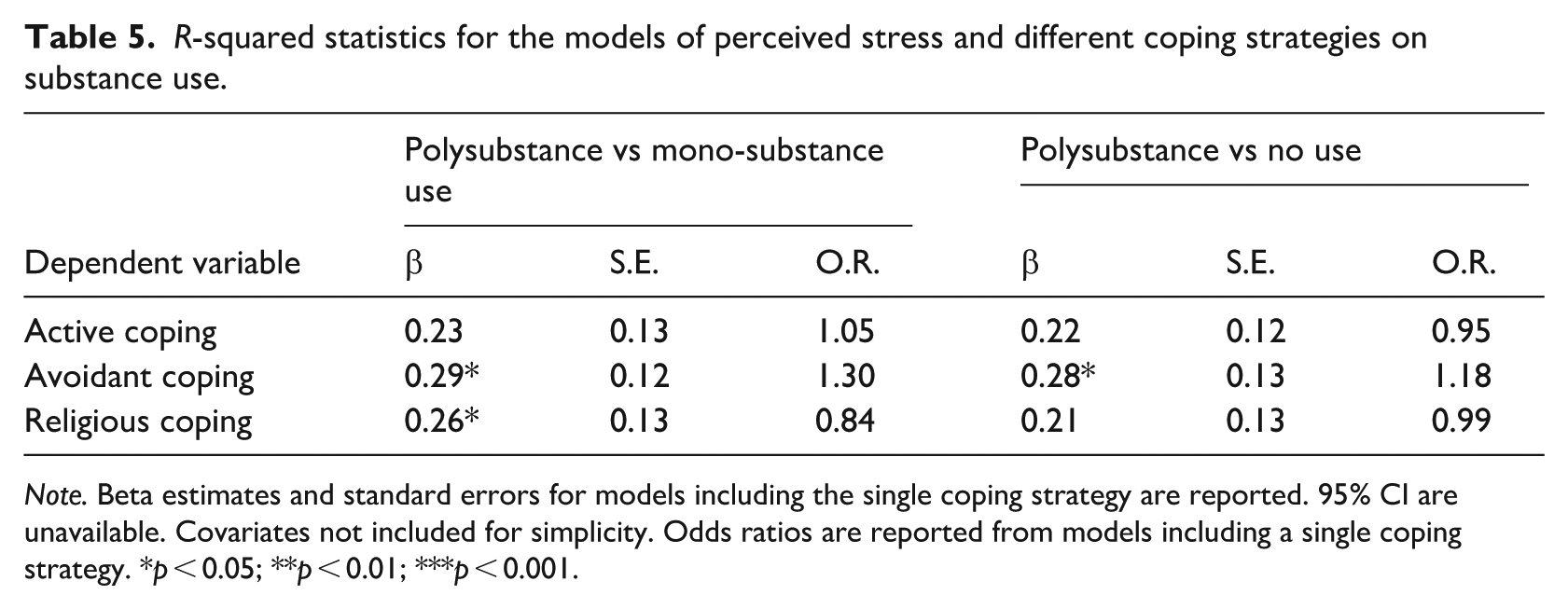
Note. Beta estimates and standard errors for models including the single coping strategy are reported. 95% CI are unavailable. Covariates not included for simplicity. Odds ratios are reported from models including a single coping strategy. *p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
The goal of this study was to examine the relationships between general perceived stress, COVID-19-related stress, coping strategies, and polysubstance use in emerging adults during the COVID-19 pandemic. The current study found that about a third of emerging adults endorsed polysubstance use. There was limited evidence for COVID-19-related stress being related to polysubstance use in comparison to the robust effects observed for perceived daily stress. Overall, this study highlights the importance of stress coping strategies for polysubstance use. Specifically, that increased perceived stress decreases the frequency of using active coping strategies, as well as increases the frequency of using avoidant coping strategies. Altogether, this results in a greater likelihood of polysubstance use.
Stress effects on polysubstance use
Our multiple regression analyses supported our hypothesis that perceived stress would be associated with increased likelihood of polysubstance use. We observed increased risk of substance involvement (i.e. from mono- to polysubstance use) for active coping and religious coping, suggesting that an increase of perceived stress is associated with more severe drinking behavior. Stress was generally associated with greater risk for polysubstance use versus no use. Notably, we observed that stress was also associated with a greater risk for monosubstance use (vs polysubstance use) and that stress’ effect on polysubstance use is partly mediated by avoidant coping strategies. These observations are consistent with other findings in college students (Emery et al., 2021) during the COVID-19 pandemic. Emery et al. (2021), concluded that the COVID-19 pandemic increased perceived stress. This may help to explain why we did not find any evidence of a direct association between risk for polysubstance use with the COVID-19-related stress predictors. Of the two variables, perceived stress appears the more robust stress indicator. The more frequent use of avoidant coping strategies contributed to a greater likelihood of polysubstance use versus monosubstance use. This aligns with prior studies that show that individuals who have difficulty using more constructive stress coping strategies may resort to the use of substances for stress relief (Unger et al., 2003; Wills et al., 1996).
Stress effects on the use of various coping strategies
The findings regarding indirect stress effects on coping strategies suggest that increased stress affects the likelihood of using avoidant coping strategies, as well as an increase in polysubstance use. Similarly, Milas et al. (2021) tested whether coping style mediates the relationship between stress and life satisfaction and found that stress was related to a decrease in life satisfaction. Stress was also found to increase the likelihood of engaging in avoidant coping strategies, such as distracting oneself from the problem (Milas et al., 2021). Taken together these findings suggest that stressful environments play a role in one’s decision to use avoidant coping strategies, and that these coping strategies may be associated with more negative outcomes. This suggests that a person may be able to decrease the likelihood of negative outcomes by engaging in non-avoidant coping strategies. Our path analyses found that increased perceived stress was associated with an increased frequency of using avoidant coping strategies. These findings indicate that the effects of stress on the use of coping strategies may be specific and arise from changes to other processes, such as impeded cognition and decision making (Porcelli and Delgado, 2017). Our observations align with a previous study in which adults with below average stress levels were more likely to use active coping strategies compared to avoidant strategies; similarly undergraduate students with low stress were more likely to employ an active (vs avoidant) coping strategy (Aldwin and Revenson, 1987; Ganesan et al., 2018). We observed a negative association between perceived stress and the use of active coping that could also be due to stress impeding the use of available resources to cope. It is probable that there was no association between stress and religious coping because it can have both a positive and negative effect; we noted opposite effects of religious with active (positive correlation) and avoidant (negative correlation) coping that had differing effects on the risk for poly- and mono-substance use.
Coping strategies’ effects on polysubstance use
The results of the multiple regression also indicated that avoidant coping was positively associated with polysubstance use compared to no use. Individuals who more frequently use avoidant coping techniques may be more likely to engage in polysubstance use. This finding builds on a previous study in which avoidant coping was associated with increased tobacco, cannabis, and alcohol use escalation in adolescents (Wills et al., 2001). Emerging adults who use multiple substances may use avoidant coping strategies more frequently than those who use one or no substances. This is consistent with prior observations that individuals who use substances heavily are less likely to engage in problem-focused coping strategies (Sudraba et al., 2015). This finding aligns with previous work that saw increased substance use over time among adolescents who used more avoidant coping strategies (Kaplan et al., 1986). Although our study provides limited evidence in the way of coping strategies being learned, our observations suggest that these patterns of association, that may be observed as early as adolescence, also exist during emerging adulthood. Lastly, it should be noted that coping strategies were not mutually exclusive – as such, it is not possible to determine if our observations could be due to those who use multiple substances simply having to use more coping strategies in general, regardless of the specific method, because of the negative impacts of using multiple drugs. Despite this challenge, our study provides a potential framework for considering how stress and stress coping strategies together influence substance use behaviors (i.e. polysubstance vs monosubstance or no use) in the emerging adult population. The effect of increased stress on the use of coping strategies has been found in previous studies giving evidence that COVID-19 stress leads to increases in the use of avoidant coping This study is unique in that it combines both the effect of stress on coping and the effect of coping on substance use into a single framework and focuses on polysubstance use in emerging adulthood, a context which requires more information to address the disproportionately higher rates of polysubstance use.
These results have implications for tailoring coping strategies to address stress and reduce substance use. Our findings reinforce the acknowledgment of stress coping strategies in substance treatment programs, such as mindfulness-based interventions (Cavicchioli et al., 2018).
Limitations & future directions
The information presented should be interpreted considering limitations. First, we examined several coping strategies, but we recognize that individuals employ multiple coping strategies at the same time. Our study did not focus on combinations of various styles as we had no a priori evidence as to how these forms of coping may interact; while the correlations between styles were modest (~0.3) larger samples would be needed to examine style interactions. Future studies are necessary to examine how the use of different coping strategies together may interact to affect the relationship between stress and substance use. Second, our sample lacked the necessary power per racial category to examine differences in the observed relationship by these groupings as our sample was majority White followed by Asian American. Additionally, one’s racial identity may coincide with cultural practices, which could affect the types of coping strategies one selects, and we recognize that historical practices and structural biases differentially impact the prevalence rates of substance use and stress by race (Williams, 2018). To account for these group differences, as well as differences in response to stressors (Bulatao, 2004) we controlled for self-reported race, but future studies are needed that focus on recruiting to increase the representation of marginalized groupings to examine how stress and coping strategies effects operate within and between groups. Similarly, both substance use behaviors and coping mechanisms can vary by gender-norms and biological sex (e.g. alcohol metabolism). While the current study controlled for self-reported sex, we were underpowered to examine sex-specific effects on substance use and coping strategies. Future studies should pay particular attention to this. Third, we did not assess participants’ knowledge of various coping strategies to know if their use of behaviors of a particular style is due to preference or lack of knowledge about other strategies. Fourth, we used retrospective measures of substance use and stress, which are subject to recall bias. We limited the effects of memory recall on substance use in the study by using a short interval window of past 90-days for frequency of substance use using the ASSIST survey. Ideally, future studies could utilize ecological momentary assessment to reduce recall bias and better assess the temporal nature of concurrent or sequential substance use or even integrate biomarkers of recent substance use. Fifth, it is important to note that the SAMHSA’s definition of polysubstance use- the use of more than one substance at a time – is different from the current study’s definition– the use as the use of at least two substances: alcohol, tobacco, and cannabis within the past 3 months (NSDUH, 2021). This 90-day timeframe is larger than SAMHSA’s definition for polysubstance use, which implies simultaneous/concurrent consumption. Of particular interest is whether the different definitions of polysubstance use show different patterns of results for the current study compared to prior literature. Using a larger window of opportunity of drug-use allowed us to assess associations between stress and poly-drug involvement, but the current results cannot be generalized to situations involving simultaneous use of these substances. Lastly, the current analysis design and path models suggest mediation but cannot definitively point to causation. Therefore, future longitudinal studies are needed in well-powered samples that have both coping mechanisms and substance use at multiple waves.
Conclusion
Overall, the current findings indicate substantial stress-related increases in polysubstance use among college students during the COVID-19 pandemic. Notably, these effects were (1) not specifically related to COVID-related stressors, and (2) varied as a function of the types of coping strategies employed. Individuals who were more stressed tended to engage in avoidant coping strategies and polysubstance use. Additional research is needed to determine the underlying causes of these associations, which are consistent with pre-pandemic associations between stress and individual drugs of abuse. These findings have implications for tailoring prevention/coping strategies to address stress and potentially reduce polysubstance use among college students.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261434373 – Supplemental material for Associations between stress, coping, and polysubstance use among emerging adults during the COVID-19 pandemic
Supplemental material, sj-docx-1-hpq-10.1177_13591053261434373 for Associations between stress, coping, and polysubstance use among emerging adults during the COVID-19 pandemic by Natalia Jaume-Feliciosi, Jamaiica S. Hurston, Chelsie E. Benca-Bachman and Rohan H. C. Palmer in Journal of Health Psychology
Footnotes
Acknowledgements
We are especially grateful to the undergraduate and graduate student members of the MAPme research team for their efforts in recruitment, administration of the MAPme survey, and cleaning of the data. We are also grateful to all the participants of the MAPme study.
Ethical considerations
This study was approved by the Emory IRB (IRB00096137).
Consent to participate
The MAPme Project was approved by the Institutional Review Board of Emory University and informed consent for participation and publication of results was obtained prior to data collection (IRB00096137).
Consent to publication
As part of the consent form process, participants consented to their data being published.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the National Institute on Drug Abuse (DP1DA042103; awarded to RHCP) and a grant from the Giles Robertson Fund (awarded to the Department of Psychology at Emory University).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors have no conflicts of interest to declare. The authors confirm that the research presented in this article met the ethical guidelines, including adherence to the legal requirements, of the United States of America and received approval from the Institutional Review Board of Emory University.
Data availability statement
Supplemental material
Supplemental material for this article is available online.