
Abstract
Interest in finding early markers or risk factors for Alzheimer’s disease (AD) has increased along with intervention options. Subjective memory complaints (SMC), the perception of cognitive decline in individuals with normal cognition, have been one area of focus. SMC are common among older adults and may be more prevalent among Latinos, among whom AD cases will grow rapidly. Fifty-four Latinos (ages 40–64) in a study of the impact of receiving information about one’s AD risk reported current SMC and completed semi-structured qualitative interviews. They discussed the SMC’s causes and consequences, their coping responses, and whether they had sought medical help. Most offered benign or normalizing explanations for their SMC. Many employed compensatory coping strategies that lessened the problem’s practical and emotional consequences. Few discussed the problem with a physician. The findings provide novel insights regarding Latinos’ illness behavior in response to SMC.
Introduction
As the population of adults 65 and older continues to grow worldwide, Alzheimer’s disease (AD) has become a major public health problem. In the United States (US), Latinos will experience the largest increase in cases of AD and related dementias (ADRD) over the next four decades (Quiroz et al., 2022). Among US adults aged ⩾ 65 years, Latinos are about 1.5 times as likely to have ADRD as non-Latino Whites (Alzheimer’s Association, 2025a).
Given the costs of caring for individuals with AD, the US and other countries have initiated national strategies to address the problem. One goal of these efforts has been achieving early diagnosis to allow pharmacological and behavioral interventions that could slow disease progression or delay institutionalization (Kerwin et al., 2022). Yet, there are often long delays between when someone first notices a symptom of AD and diagnosis (Chrisp et al., 2011; Mukadam et al., 2011). Minority older adults, including Latinos, are more likely to experience a missed or delayed diagnosis for dementia than non-Hispanic Whites (Armstrong-Mensah et al., 2024; Quiroz et al., 2022), resulting in diagnosis at a later stage of illness (Mukadam et al., 2011).
Considering the growing emphasis on early detection, identifying prodromal signs or symptoms of AD or risk factors for the disease, such as subjective memory complaints (SMC), is critical. While definitions of SMC differ across studies (Abdulrab and Heun, 2008; Studart and Nitrini, 2016), SMC generally refers to the “subjective perception of cognitive decline compared to previous levels of functioning in individuals with normal cognition” (Warren et al., 2022: 2). While not always a sign or precursor of dementia, SMC are increasingly recognized as an early marker of cognitive decline, including mild cognitive impairment (MCI) or AD (Pike et al., 2022; Wang et al., 2021).
SMC occur in approximately 50% of people aged 50–59 and in 63% of those aged 80–100 (Brigola et al., 2015), and may be more prevalent among Latinos than non-Hispanic Whites (Casillas et al., 2019). For example, in elderly adults recruited from an outpatient memory clinic, Hispanics reported greater memory problems than non-Hispanic Whites, despite being significantly older and having similar levels of objective cognitive impairment (Harwood et al., 1998).
While most SMC literature focuses on the decision to consult a physician, illness behavior (i.e. how people notice, interpret, and respond to symptoms) encompasses the processes that occur before this decision is made (Mechanic, 1986). Research shows that people have expectations about how their bodies should feel and function. When they notice a physical symptom or cognitive problem they regard as abnormal, they typically begin a process of symptom appraisal which involves arriving at a causal attribution for the problem and assessing its significance. Lay notions about a symptom’s cause and significance are often determined by mapping the symptom onto pre-existing illness representations, prototypes, or schema individuals hold of different diseases or conditions (Croyle, 1992; Kirmayer and Bhugra, 2009). These illness representations, which can differ significantly from biomedical models of disease, are constructed based on cultural stereotypes, media portrayals, prior personal/familial illness experiences, and expert information. They typically have five components: (1) identity (i.e. characteristic symptoms), (2) cause, (3) consequences, (4) controllability/curability, and (5) timeline (Lau and Hartman, 1983; Martin et al., 2003). When a symptom is believed to indicate an illness, the individual will usually attribute it to the disease whose illness representation offers the best fit (Cacioppo et al., 1989; Cioffi, 1991). However, if doing so evokes significant fear or threat, as in the case of a life-threatening, highly debilitating, or incurable diseases, they may be motivated to arrive at a benign explanation instead (Smith et al., 2005). The symptom appraisal process will typically lead the individual to pursue one of three courses of action: wait and see if the issue resolves on its own, engage in self-care, or see a physician (Alonzo, 1979; Wyke et al., 2013).
Consistent with the tendency to arrive at a benign or normalizing causal attribution for a symptom, people often try to self-manage their symptoms. Indeed, many symptoms or illness episodes are never brought to the attention of a medical provider, or only after substantial delay (Perry-Young et al., 2018). Alonzo (1979) noted that “containment” may be important in determining if and when a symptom is discussed with a provider. He argued that so long as people can sustain their usual roles and activities and keep the task of managing the symptom as a “side involvement,” they typically will not seek medical care. Rather, they will do so only when they are no longer able to manage the symptom effectively, and it begins to disrupt their normal daily activities.
In this report, we used qualitative interview data to investigate Latinos’ illness behavior in response to perceived memory problems. The findings help fill the current gap in our understanding of how Latinos appraise and respond to such problems. They offer novel contributions that may help explain why Latinos experience delayed diagnosis for AD when emerging medical options and awareness of SMC as a potential early sign of AD have led to an emphasis on early detection.
Methods
Study design
Data come from a community-based longitudinal study on the psychosocial, behavioral, and cognitive impacts of APOE genotype and AD risk information disclosure. To be eligible, individuals had to: (1) self-identify as Latino or Hispanic, (2) be aged 40–64, (3) reside in New York City neighborhoods of Washington Heights, Inwood, Hamilton Heights, Harlem, Morningside Heights, or Manhattanville; (4) speak English or Spanish, (5) have not previously had APOE testing, (6) not been diagnosed with AD, (7) not have a family history of AD suggestive of early onset, autosomal dominant AD, and (8) not have endorsed suicidality on the Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001).
The study had a quantitative (surveys) and a qualitative (interviews) component. Qualitative participants were a purposively selected subsample of the larger survey sample chosen to maximize heterogeneity in AD family history and APOE genotype. Assessments were conducted before risk information disclosure and at 6 weeks, 9 and 15 months after disclosure. The study protocol was approved by the Columbia University Irving Medical Center Institutional Review Board. For a full study description, see Wetmore et al. (2024). This report follows the Standards for Reporting Qualitative Research (SRQR; O’Brien et al., 2014).
Data collection
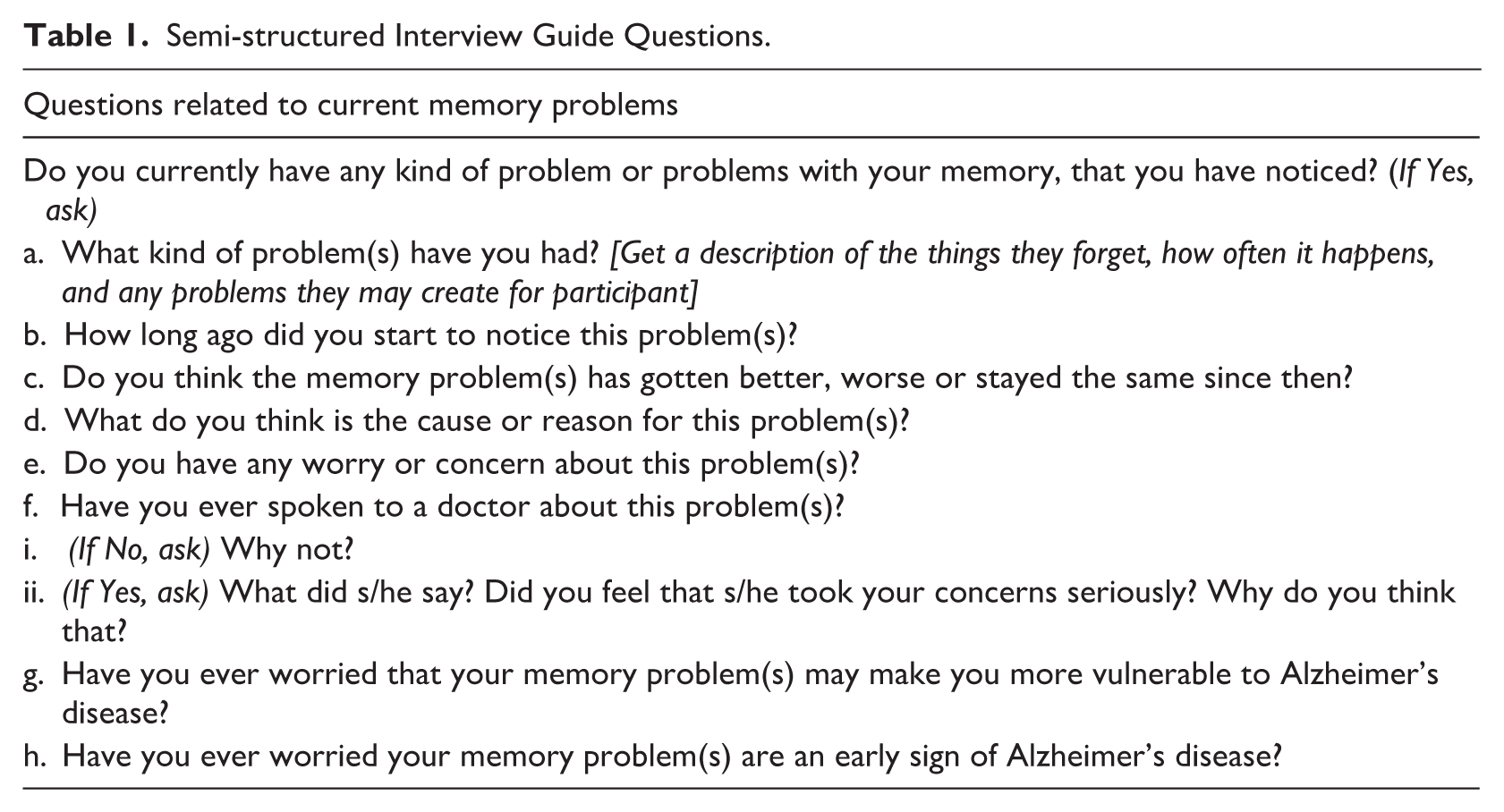
Semi-structured qualitative interviews, conducted over Zoom, were completed in English or Spanish. They averaged 89 minutes, and participants received a $100 gift card for each completed interview. Data for this report comes from baseline interviews conducted between 24 August 2021 and 26 September 2023. Interviews covered a range of topics, including perceived cognitive problems. Participants were asked if they currently experienced any memory or thinking problems. If they were, they were asked a series of follow-up questions (Table 1). Interview data collection, transcription, and translation were completed by two HIPAA compliant commercial firms with experience in health research. Training ensured proper interview guide administration, neutrality in probing and asking follow-up questions, and imparted skills for gaining participants’ trust. Quality checks of transcription and translation occurred throughout data collection.
Semi-structured Interview Guide Questions.
Data analysis
Transcribed interviews were independently coded by two team members in ATLAS.ti Scientific Software Development GmbH (2020). All material related to participants’ responses to interview questions about memory problems were extracted for content analysis (Forman and Damschroder, 2007: 40). This material was read multiple times, including an initial reading aimed at getting a sense of the entirety of the data, followed by readings focused on specific parts of the data relevant to understanding different aspects of participants’ symptom experiences which were tagged using open coding. This, through careful examination of this tagged material, a set of inductive codes were developed. Codes were grouped according to the issues that were the focus of the analysis. Next, through an iterative process the codes were refined, removing code overlap, and adding codes as needed, until a final set of codes was developed. The finalized codes were then applied and refined in an iterative process to a subset of interviews. A detailed audit trail of the code development and coding processes was maintained. It showed that saturation was achieved with 41 cases. We defined saturation as the point in the observation of cases that additional cases did not produce a need for more codes, the refinement of existing codes, or offer new or more nuanced insights regarding the research question.
All qualitative team members were involved in defining the codes and creating the codebook. As a team, we decided that once high inter-coder agreement was achieved, defined as 85% or greater agreement in the application of the codes, the coders would proceed to apply the codes to all remaining transcripts. This criterion was reached early in the preliminary coding process. This was likely in part enabled by the qualitative research team having arrived at the codes/codebook together over numerous team meetings, which allowed a consensus on the meaning and appropriate application of codes to emerge.
The analysis focused on the nature of the memory problems, whether they had worsened, stayed the same or improved over time, participants’ appraisals of their problem’s consequences, what participants did to manage the problems, and how these things influenced their decision to whether to speak with a doctor about their problem. While the first author was responsible for the initial interpretation and write-up of the findings, they were reviewed by other study members who were immersed in the data in different roles and discussed in team meetings. This process ensured that multiple perspectives were considered, and a high level of agreement on the conclusions was reached. Any disagreements were resolved by closely reviewing the data, followed by a team discussion.
Reflexivity was emphasized throughout all stages of the study, from developing interview guides to data analysis and reporting. All members of the qualitative study team were women and held a doctorate or master’s degree. Their training represented a variety of disciplines (sociology, public health, and psychology). Team members had different ethnic and cultural backgrounds. This diversity allowed for a wide range of different perspectives to be considered at each stage of the research. During group discussions, the team members challenged each other’s ideas and possible misconceptions, pointed out potential biases, and collectively modified ideas until a group consensus was reached.
Results
Seventy-eight participants responded to the questions on memory or thinking problems. Of these, 54 reported a memory problem and are the focus of this paper. The 78 participants represented only a portion of the qualitative component sample because these questions were added to the baseline interview guide 14 months after data collection began. They were added because in examining some of the early data we noted that at baseline some participants were spontaneously volunteering that they had memory problems and that this seemed to raise their perceived vulnerability to AD. Therefore, we felt this information might be useful later in understanding participants’ reactions to the risk information they would later receive from us. Adding questions in response to early findings or impressions of data being collected is consistent with the epistemology of qualitative research (i.e. emergent design) in which the research plan remains flexible rather than fixed design, and modifications to one or more design features of the study design may occur as data collection and preliminary analysis precedes. We do not believe our findings were biased by having the perceived memory problem data for only later enrolled participants, as recruitment criteria and methods remained consistent over the course of the study. Comparisons across groups (i.e. those asked the questions, those not asked, and those without memory problems) showed no meaningful differences in gender, age, education, birthplace, caregiving experience, caregiving duration, or primary caregiver status.
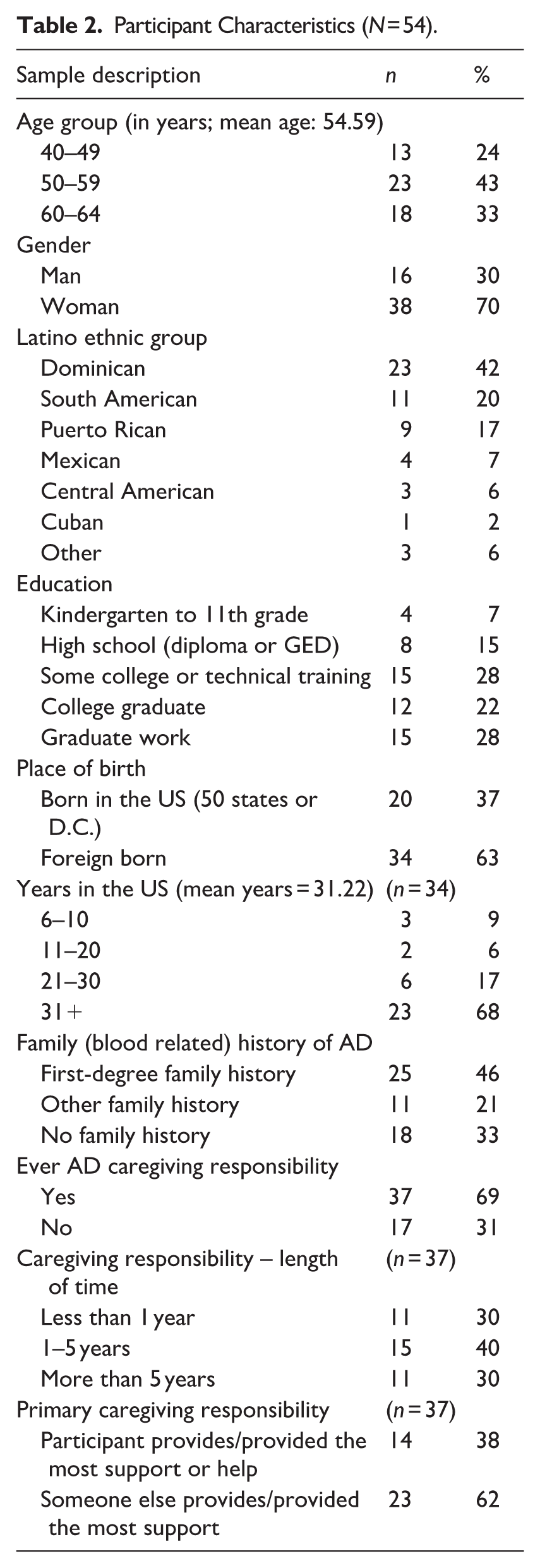
Mean age of the 54 participants who reported SMC was 54.6 years (Table 2). They were primarily women (70%) and well educated, with 50% having a college degree, and Dominican (42%). Dominicans accounted for 42% of the sample.
Participant Characteristics (N = 54).
In the findings presented below (all data analyzed in this report are available in the Supplemental Information File), the following terms are used to convey the approximate proportion given a similar response: Few – No more than a handful of participants; Several – A minority of participants, but more than a few, but fewer than slightly less than a half of participants; About half – Between slightly less and slightly more than half of participants; Majority – Greater than slightly more than half of participants, but less than almost all participants; and Almost all – Almost all participants with only a few exceptions. At the end of each quotation, information is included about participants’ family (blood related) history of AD (first-degree, other, no famhx), and education (high school or less, greater than high school). Broad categories for this information have been used for deidentification purposes. Additionally, when necessary to protect confidentiality, direct and indirect identifiers have been modified.
Nature of the problem
Virtually all perceived problems reported were memory related, including unknowingly repeating themselves, forgetting recent events, word finding difficulties, losing their train of thought, misplacing items, forgetting why they entered a room, forgetting appointments, not remembering how to perform routine job tasks, forgetting things just told to them, forgetting important dates (e.g. birthdays), and forgetting names. Reported durations of SMC ranged from a few weeks to several years.
Changes in the problem
Almost all participants said their memory problems had stayed the same, with only a few reporting problems getting better or worse. One 63-year-old woman attributed the improvement to changes in diet (i.e. eating more fruits/vegetables), supplements (i.e. vitamins, “super foods”) and lifestyle (i.e. exercising and walking). Another 50-year-old woman attributed it to focusing more on things she might forget. Those who said their memory problems had worsened usually meant they were forgetting more things or forgetting the same things more frequently. Participants could not explain why they thought it had worsened, other than when the problem was long-standing assuming it was due to the progressive decline of memory that comes with aging.
Causal attributions for memory problems
Stress
Several said they had no idea about the cause of their SMC. Of those offering an explanation, no one spontaneously attributed it to AD. Rather, they typically proposed a benign or normalizing explanation. Stress was the most frequently mentioned cause, often linked to feeling overextended or trying to do too much at once. For example, when asked what she thought what caused her memory problems, one 54-year-old woman said: I think stress. I do a lot of things together. I have a lot of work around the house; I help with the grandkids. . .. (First-degree famhx/greater than high school)
Aging
Aging was the next most common explanation, especially among participants aged 60–64, who viewed some memory loss as a normal part of getting older. For example, a 64-year-old man said: Well, age, I think. I always say age. I’m not 20 or 25 anymore, which is different. . .I think it’s something that’s normal, that’s due to the aging process. (No famhx/high school or less)
Medical conditions
Current or past medical conditions (e.g. pancreatitis, stroke, ADHD) were offered by several participants as a possible cause of their problem. For example, some attributed their SMC to the after-effects of COVID. In a few instances, their doctors had suggested this as the cause or supported the participants’ belief that the problem was COVID-related. For example, a 49-year-old woman reported: I mentioned it to my doctor, and she told me, "Oh, there are several people who have told me that they had COVID and lost their memory a bit. . .Is that happening to you?” So, she told me that they had mentioned that to her because it’s the only thing that has happened to me in my life. (No famhx/greater than high school)
Sleep problems
A few participants thought sleep problems accounted for their forgetfulness. One 61-year-old woman who was often being told by her daughters she was repeating herself commented: I think a lot of the fact that I forget things lately has been because I have trouble sleeping. I have insomnia. So, [I’m] attributing my memory [loss to the insomnia]. (First-degree famhx/greater than high school)
Strategies to manage memory problems
Using reminders
About half of participants developed strategies to compensate for their memory difficulties, minimizing their consequences. For instance, writing down important dates (e.g. birthdays, appointments) was a common strategy to manage memory problems. A 55-year-old woman reported recording meetings at work to be able to remember what she was asked to do: Yes, at work recently I even have to record meetings because there are times when I forget what they told me I have to do or what they mentioned about what happened, and I forget. Recording, recording meetings and at times I don’t listen to them. (Other famhx/greater than high school)
Others relied on family members to remind them to do things or remember important dates. For example, a 54-year-old woman relied on her daughters for reminders: Because I forget things a lot, I have to always tell the girls to remind me what I have to do on such and such a day. I have to keep telling them to remind me so I don’t forget things. (First-degree famhx/greater than high school)
Some used their smartphone to store important future dates and issue reminder notices to them. A 49-year-old woman used the camera feature to photograph things she wanted to remember since she did not feel she could rely on her memory any longer: It’s very difficult for me to memorize information, [so] I have to take a photo on my cell phone and look at it several times to remember. I wasn’t like that before. (No famhx/greater than high school)
Concealing problem
Few tried to manage their memory problems by concealing them to avoid embarrassment or shame. For example, a 61-year-old school employee shared how she hid her memory problems from students: I’m a [school employee], and then sometimes [students] ask me questions, and they’re like, “But we discussed this,” and I pretend that I remember but I don’t. Sometimes the students [are] walking in the door, and I’m like, “Where were you?” And they’re like, “I went to the bathroom,” and I say, “I gave you permission?” And they say “yeah,” and I know they’re not lying because they’re [still young]. That’s beginning to worry me, that kind of thing. (First-degree famhx/greater than high school).
Memory problem consequences
Minimal disruption but still some distress
Participants SMC rarely caused any meaningful amount of disruption in their daily lives, largely due to the coping strategies they had developed to manage the problem. Nevertheless, a few participants still found their problems frustrating or annoying when they forgot something they knew well. For example, a 44-year-old woman was very distressed when her memory problems left her unable to remember the name of a co-worker with whom she had very frequent contact: Because I think because, yeah, I forget a lot and like friends my age will be like, you know, will say, oh, you know, like I said like do you remember when we did this? And I’m like I don’t know like I don’t remember that, you know? Um, yeah and then there’s like sometimes like my thought will escape me. I’m just like even today, like I was working and I’m like, it’s I was trying to remember, I was about to email someone and it’s someone I work with all the time and I, like for the life of me could not remember the person’s name and I’m like, I’ve emailed this person like every day or like every other day. (Other famhx/greater than high school)
A few also experienced considerable worry when they feared their problem might impede their ability to do their job at work, or felt significant embarrassment when they thought others could see their memory problem and thought less of them as result, for example, a 51-year-old woman described how her memory problems caused her considerable discomfort as she believed her co-workers perceived her to be incompetent: I feel that it makes me look incompetent, and I’m not incompetent. I’m just a little forgetful. I’m very intelligent. I have several degrees. You can’t get [that] if you’re stupid. I’m book smart if that makes any difference. . .However, they won’t use me on other projects because there [are] certain things I forget. I think that’s the reason why they don’t use me. Because they haven’t used me. I’ve been there for a year and a half. They haven’t used me; I feel like that’s because I’m forgetful. (No famhx/greater than high school)
In some cases, participants felt worried when they couldn’t explain their memory problems or noticed some worsening over time. Even those who managed effectively with reminders or notes sometimes feared forgetting to use these strategies and making mistakes.
For others, what they could not remember was not important enough to create any problems. In other instances, forgetting what they wore the day before or which movie they watched the previous night sometimes caused brief concern but had no real impact on daily life or work.
Speaking with a doctor about the problem
Seeking help
Several participants had discussed their memory problems with a doctor, and those who did were reassured there was no cause for concern. As noted above, participants’ physicians often concurred when participants attributed their memory issues to stress, being overextended, or medical conditions like lingering effects of COVID. A few participants reported having brief cognitive assessments, but no problems were found, and there appeared to be no follow-up.
Reasons for not speaking with a doctor
Several indicated they had not discussed their SMC with a doctor because they did not think it was a serious problem. This was the most common explanation for not sharing their problems with a doctor. For example, a 58-year-old woman said: It hasn’t come up. I don’t think about it when I go see the doctor. I don’t think about, you know, if I’m gonna get dementia or Alzheimer’s. I don’t think about that. I don’t tell her that I forget stuff and then I’ll come back to it, I don’t tell my doctor that. I don’t think it’s that serious. (No famhx/high school or less)
A few diminished the significance of their SMC by characterizing them as “small” or “slight” and the things they forgot as “trivial” or “of not much importance.” A 53-year-old woman for example, said her memory problem was not “too serious” because what she forgot was “silly stuff” not “major stuff.” . . . I do have short term [memory problems]. I’ll forget, but I don’t think it’s too serious, to be honest with you. It’ll be kind of silly stuff. Did I do this and stuff like that? Not major stuff, you know, like the stove and stuff. Just small things [like] did I put something away?. . .I notice [it’s] nothing really serious. It could be something simple, but it’s nothing to be alarmed [about]. (First-degree famhx/greater than high school)
Some even suggested they were not forgetful, but rather were choosing, perhaps sometimes unwittingly, to forget information they deemed unnecessary to retain. For instance, a 48-year-old woman explained: Sometimes I get scared because I don’t remember things. . .But I think I’m choosing not to remember cause. . .it’s not meaningful to me. The past is already past. I can’t go back in there again, so I just leave it. You don’t know if it’s because I’m choosing not to remember or if it is because I’m forgetting things and stuff is happening in my brain. I don’t know. (No famhx/greater than high school)
Additionally, some participants attributed their memory problems to aging and viewed them as normal, seeing no need to discuss them with a doctor. A 43-year-old woman said: I talk to friends and family, [and] they say, “Oh, it’s normal. You have two kids. It’s the age; everything’s normal once you have kids and you age.” I think that’s the taboo of everything. They say it’s normal. That’s why people don’t seek help. That’s why I have never actually spoken to my doctor about that. (No famhx/greater than high school)
Finally, some claimed they had more immediate and concerning medical matters to address with their doctors than their SMC. One 64-year-old man who had not spoken to his doctor about his SMC explained: I always talk about other things, like, for example, that I have diabetes. I’m more concerned about that. (No famhx/high school or less)
Problems not attributed to AD
After responding to all of the questions about their memory problems, interviewers asked participants whether their memory problems made them more vulnerable to AD or might be an early sign of it. Almost all gave the same answer to both questions, with slightly more saying “no” than “yes.” Several participants said while they had not had either of these thoughts, they could acknowledge one or both things were at least possible. Thus, while no one spontaneously volunteered AD as a cause of their memory problem when asked if this was something they had thought about, some admitted the thought had crossed their mind but did not believe it explained their problem.
Discussion
Participants’ memory problems ranged from common ones (e.g. misplacing something, forgetting why they entered a room) to potentially more serious ones (e.g. trouble remembering simple words, forgetting what they had done recently, forgetting how to do routine tasks). Participants reported experiencing their problems for varying periods of time, from weeks to years, with almost all saying the problem had stayed the same over time. Almost all offered a benign or normalizing causal attribution for their memory problem, most often mentioning stress, aging, a current or past medical condition, or sleep deprivation. Aging was primarily offered as an explanation by older participants who typically assumed that memory inevitably declined with age.
It is notable that in the context of a study on AD, no one spontaneously offered AD as a probable cause of their problem. It seems unlikely that this was because they did not know memory problems were a symptom of AD. Carrasco et al. (2017) noted that SMC can be “a frequent matter of concern for older adults as they often interpreted them as an early sign of cognitive impairment or even dementia” (Carrasco et al., 2017: 28). Further, 69% of our participants had caregiving experience, in many cases for an extended period of time and may be assumed to be familiar with AD’s symptoms.
Despite not volunteering AD as a cause of their memory problem, when asked whether they worried their memory problem made them vulnerable to AD or was an early sign of AD, nearly half responded “yes.” This suggests that possibly the fear AD evokes, motivated participants to dismiss it as a potential explanation, instead seeking a benign or normalizing attribution. A recent survey (Alzheimer’s Association, 2025b) revealed that more than 83% of US adults reported some level of worry about developing the disease, with 29% of Hispanic Americans expressing a lot of worry. This was more than twice as high as all other groups and more than three times as high as among Whites.
Another possible explanation why no one volunteered AD as a cause of their problem might be that at the time data for this report was gathered, participants had not yet received their genetic test results. Certainly, if some were aware they carried the susceptibility gene for AD, and especially if they also reported a family history of AD, they might have been more inclined to consider mentioning AD as a possible cause of their memory problems. Finally, perhaps because in all but a few cases the problem had not worsened over time, participants were reassured it was not related to AD, which is widely recognized as a progressive disease. Our findings closely parallel those reported in a review of the qualitative literature on subjective cognitive decline (Buckley et al., 2015). They found that healthy older adults with SMC typically did not ascribe their problem to ADRD, despite a strong concern about developing AD. Rather, they predominantly attributed their difficulties to stress, anxiety, other illnesses, medication, and normal aging (Buckley et al., 2015: 6).
Consistent with Alonzo’s (1979) observation that symptoms typically are not brought to a physician’s attention until they become disruptive to people’s daily routines or impede the performance of their social roles, we found very few participants had experienced such difficulties and similarly few had spoken with a doctor about it. In large measure, such “containment” (Alonzo, 1979) of the symptoms was possible because they adopted coping strategies to compensate for their memory difficulties such as relying on others to remind them of appointments or things they had to do, writing things down, and using features of their smart phones to set reminder alerts. Strategies reported by participants in other studies to manage SMC that we did not observe included: establishing and maintaining consistent routines, slowing down the pace and activities in their daily life, reducing complexity by ordering tasks they had to accomplish (Imhof et al., 2006), and having one place to always put something (Buckley et al., 2015; Cromwell, 1994).
While several found their memory problems an occasional source of worry, frustration, or annoyance, few reported experiencing any significant distress except when their memory problems were observed by others, leading to feelings of embarrassment or concerns they were seen as incompetent. Werner (2004) found that while elderly individuals believed their memory decline was a normal consequence of aging, they nevertheless found it embarrassing and stigmatizing when apparent to others. Hill et al. (2021) also found similar emotional reactions in older adults with SMC as we did in some of our middle age sample. A few engaged in what Goffman (1963) called “covering.” This involved hiding their memory problem and pretending to remember things they could not recall, thereby avoiding embarrassment or becoming “discredited.”
Those who had never discussed the problem with a doctor offered a variety of reasons for not doing so. About half normalized their problem and attributed it to stress or expected age-related declines. Others explained they did not think of their memory issue as a “problem” or at least not a particularly troublesome one. For some, this was because of the compensatory strategies they had adopted. Others minimized their problem’s importance by asserting that the things they forgot were unimportant, silly, or trivial, emphasizing that they remembered what truly mattered to them. Only several had spoken to a doctor about their memory problems, and those who did were typically reassured that their issues were normal or likely due to stress or a medical condition. One barrier to our participants seeking a medical opinion about their problem might be the tendency of Latinos not to talk about health problems outside the family and to manage health concerns within it (Martinez and Acosta Gonzalez, 2022).
A variety of variables including personality traits (e.g. neuroticism, trait anxiety) or other kinds of variables (e.g. acculturation, coping strategies, education, etc.) may have influenced participants’ approaches to recognizing, responding to, and reporting memory problems to providers. It was beyond the scope of this paper to try to identify these variables, but this should be investigated in future research.
Our findings are important because there has been a growing emphasis on early AD detection as new treatments are becoming available and SMC has become recognized as a possible early sign of a neurodegenerative disorder. However, since late middle age and older adults are not routinely screened for ADRD, early detection relies heavily on individuals bringing their symptoms to a doctor’s attention. However, this requires recognizing the problem as possibly having a medical cause (de Levante Raphael, 2022). Long delays between symptom recognition and diagnosis, especially among minorities, have been noted (Armstrong-Mensah et al., 2024; Quiroz et al., 2022). Our findings illustrate how the normalization of memory loss as one ages, evidenced by phrases like “having a senior moment,” and the minimization of the problems (e.g. suggesting only unimportant or silly things were forgotten), combined with the use of strategies that reduce the impact of symptoms on daily life, can contribute to delays in speaking with a doctor and diagnosis.
We observed a pattern of illness behavior regarding cognitive symptoms, specifically various memory problems, that closely mirrors the patterns previously described for somatic symptoms, such as a strong tendency to seek non-threatening attributions for their symptoms. In the case of physical symptoms, Robbins and Kirmayer (1991: 1030) have observed, “. . .wherever possible, symptoms will be normalized by attributing them to situational factors such as environmental irritants, temporary fatigue, overexertion, lack of sleep or dietary indiscretion. Only when such a normalizing attribution is clearly not sufficient will symptoms be attributed to a dispositional source such as physical disease, excessive worry, or constitutional weakness.” While Showers and Cantor (1985) have noted that while the social cognition literature tends to emphasize how pre-existing knowledge and illness prototypes or schema influence symptom interpretation and coping responses, individuals can dismiss the most obvious interpretations if they threaten pressing goals, cause distress, or challenge important beliefs.
A noteworthy difference, however, between somatic and cognitive symptoms is the opportunity for self-care. With common physical symptoms, such as pain, abdominal distress, and headaches, many options for self-care (e.g. rest, physical therapy, exercises), and many over-the-counter products (e.g. pain patches, ibuprofen, supplements) are available to ameliorate symptoms without professional assistance. This is less true for memory loss or other cognitive symptoms. Various over-the-counter products claiming to support brain health and enhance memory, concentration, and focus have come to market in recent years, and some well-known supplements (e.g. fish oil, Ginkgo Biloba, ginseng) are used by individuals with cognitive problems to treat them despite unclear evidence of their efficacy (Laditka et al., 2012). Some also believe that certain kinds of mental activities (e.g. crossword puzzles, Sudoku, memory games) can support brain health. In our sample, no one reported using supplements to address their memory problem. While this might suggest more people would seek professional help for cognitive symptoms, we found this was not a common response. Instead, participants were more likely to focus on accommodating their memory problems and minimizing their impact through compensatory strategies, with virtually no mention of efforts to ameliorate or resolve the issue.
Our findings make important and novel contributions to the literature by enhancing our understanding of how Latinos respond to SMC, which can be an early sign of AD or a risk factor for it. Given the growing emphasis on early detection and the greater delays in AD diagnosis that Latinos experience compared to their non-Hispanic White peers, investigating this issue may help reduce health disparities. In addition, most of the existing literature on SMC has focused on adults aged 65+ (Reid and Maclullich, 2006; Roberts et al., 2009), while our sample comprised middle-aged adults ages 40–64 with a mean age of 54.6. Although it may not be generalizable to older Latino populations who may have higher levels of concerns about memory problems, this report provides novel insights into how younger Latinos respond to SMC. Finally, we saw in our participants the common tendency to make benign or normalizing attributions for their memory loss, which can also delay their bringing this problem to a physician’s attention and receiving a timely diagnosis. Physicians, however, do not have to wait for patients to come to them to discuss their cognitive health. Rather, during a routine visit they can inquire about any memory or thinking problem the patient is experiencing or use one of the brief screening tools that have been developed to quickly screen patients (i.e. opportunistic screening) for difficulties that deserve further assessment (Alzheimer’s Association, 2025c). They can also share information available from the Alzheimer’s Association (2024) on how to distinguish between cognitive difficulties that are a normal part of aging from ones that are potentially associated with AD. While community health education can increase Latinos’ awareness of early signs of AD and the benefits of early diagnosis and intervention, earlier entry into care can also result in referrals to community resources including support groups, all which can improve quality of life for patients and caregivers.
There are limitations of the study to acknowledge. First, our participants may have been better informed about AD than many Latinos because they were well educated, with 78% having at least some higher education or technical training after high school. Among the 54 participants, 69% reported ever providing support or help to a family member or close friend with AD, dementia, or serious memory problems. This reflects the Latino cultural value of familism, which emphasizes deep identification with both immediate and extended family members, as well as loyalty, mutual support, and a sense of shared responsibility within the family unit (Sabogal et al., 1987: 398). Familism may also delay AD diagnosis because it promotes care within the family and may discourage seeking outside care until symptoms are severe (Martinez et al., 2022; Martinez and Acosta Gonzalez, 2022).
Further, there were multiple sequential steps and study-related activities that participants had to complete to become part of the final sample and participate in baseline qualitative interviews. Those who went through all those steps may have differed in some significant ways from those who did not, producing selection bias. Additionally, interviews conducted and transcribed in Spanish were translated into English for analysis. While we randomly sampled the Spanish interviews to assess the quality of the transcription and translation and found it to be quite good overall, it is possible that the data from some of the Spanish interviews that were not reviewed may have been compromised by the translation. Finally, while we believe the face-to-face contact of conducting interviews over Zoom facilitated the building of rapport beyond what can be achieved in telephone interviews, we cannot know if it also may have introduced any social bias associated with participants wanting to please the interviewer and present oneself in a way that may be judged positively.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261442545 – Supplemental material for Latinos’ appraisals of and responses to memory problems
Supplemental material, sj-docx-1-hpq-10.1177_13591053261442545 for Latinos’ appraisals of and responses to memory problems by Karolynn Siegel, María Cabán, John B. Wetmore and Ruth Ottman in Journal of Health Psychology
Footnotes
Acknowledgements
We are grateful to the study participants of the “Estudio IDEAL–Información de la Enfermedad de Alzheimer para Latinos” who devoted their time to the research. We thank the Community Engagement Core Resource of Columbia University’s Irving Institute for Clinical and Translational Research. The authors wish to thank Janice Lee, MPH (research assistant) for her assistance in the preparation of this manuscript for submission.
Ethical considerations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Institutional Review Board at Columbia University Irving Medical Center [Protocol IRB-AAAR8269].
Consent to participate
Informed consent was obtained from all study participants.
Consent for publication
Participants signed informed consent for publication of deidentified study findings.
Author contributions
Writing – Original Draft: Karolynn Siegel; Formal analysis: Karolynn Siegel; Visualization: Karolynn Siegel; Funding acquisition: Karolynn Siegel, Ruth Ottman; Conceptualization: Karolynn Siegel, Ruth Ottman; Methodology: Karolynn Siegel, Ruth Ottman; Investigation: Karolynn Siegel, Ruth Ottman, María Cabán, John Wetmore; Project administration: María Cabán, John Wetmore; Supervision: Karolynn Siegel, Ruth Ottman; Writing – Review & Editing: María Cabán, John Wetmore, Ruth Ottman.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (grant numbers R01AG062528 and UL1TR001873).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Clinical trial statement
The study was pre-registered with clinicaltrials.gov before the time of first participant enrollment. ClinicalTrials.gov ID: NCT04471779. Date Registered: July 15, 2020. Registry Name: The IDEAL Study: Information About Alzheimer’s Disease for Latinos in New York City. Study Details | NCT04471779 | Information About Alzheimer’s Disease for Latinos in New York City | ClinicalTrials.gov
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.