
Abstract
This study evaluated the prevalence and intensity of forgiveness in active-duty military orofacial pain (OFP) patients and explored its associations with pain severity, psychological and emotional factors, and sleep disturbance. A retrospective chart review was completed with a cohort of 380 active-duty military personnel diagnosed with OFP. Forgiveness was measured using the Heartland Forgiveness Scale (HFS), while pain severity, psychological factors, and sleep disturbances were evaluated through validated measures. Statistical analyses included multivariable linear regressions to assess predictors of forgiveness and associations with psychological measures. Patients with higher forgiveness demonstrated significantly lower anxiety, depression, sleep disturbances, stress, and anger. However, no significant association was found between forgiveness and pain severity. Results highlighted anger and anxiety as key negative predictors of forgiveness. The findings underscore forgiveness as a relevant psychosocial factor in OFP management, particularly in mitigating emotional distress. Incorporating forgiveness-focused interventions may enhance the biopsychosocial approach to treating chronic OFP.
Introduction
“Forgiveness is setting the prisoner free, only to find out the prisoner was me”,
Forgiveness is a concept often first learned in early childhood from the moment a transgressor pushes one down on the playground. It is emphasized in most major world religions and stands in opposition of vengeance. Forgiveness can be defined as an adaptive trait or behavior where the perception of a transgression is no longer the same; kindness and compassion now replace hatred, avoidance and vindication (Worthington and van Zyl, 2021). A transgression can be defined as an incident of wrongdoing, something that violates one’s expectations of how oneself, others, or the world should be (Thompson et al., 2005). Forgiveness is a prosocial change and asset to humanity as it fosters continued interdependence (Worthington and van Zyl, 2021; Yucel and Vaish, 2021). This change may be directed toward self, others, or a situation (Kim et al., 2021). Forgiveness does not require an interpersonal reconciliation between the two parties and should be thought of as a process within one’s self, an intrapersonal experience (Thompson et al., 2005). This internal process of forgiveness will outwardly display changes in emotions and behavior to view the once negative person or situation as neutral or even more positive (Worthington and van Zyl, 2021).
The benefits of forgiveness have been demonstrated in a variety of diseases including: HIV, coronary artery disease, cancer, and chronic pain (Ford et al., 2013; Friedberg et al., 2009; Kim et al., 2021; Martin et al., 2012; O’Beirne et al., 2020). These studies found that higher levels of forgiveness were associated with higher overall quality of life, lower negative affect, and lower anger. However, the results regarding the association between forgiveness and both physical health and pain severity were mixed in these studies. Forgiveness has also been utilized as part of an adjunct therapy in interventions for veterans with Posttraumatic Stress Disorder (PTSD; Starnino et al., 2019).
Studies in chronic low back and fibromyalgia have found that patients reporting higher forgiveness had fewer physical symptoms, needed less pain medication, had improved sleep quality, and were not as fatigued (Lawler et al., 2005; Lee and Enright, 2014). Carson et al. explored the relationships among forgiveness and pain severity, anger, and psychological distress in a sample of patients with chronic low back pain. Patients with higher forgiveness scores reported lower levels of pain severity, anger, and overall psychological distress (Carson et al., 2005). Conversely, lower levels of forgiveness of self and others have been shown to be associated with higher pain severity, higher catastrophizing, and poor active coping in patients with chronic pain (Offenbaecher et al., 2017; Vallejo et al., 2020).
While forgiveness has been studied in chronic pain conditions like low back pain and fibromyalgia, there is limited research on forgiveness in orofacial pain. Orofacial Pain (OFP) refers to pain disorders of the mouth, face, head, and neck, to include odontogenic and periodontal pains, neurovascular pain and headaches, vascular disorders, neuropathic pains and muscular and joint pains such as that found in temporomandibular disorders (TMDs; AAOP, 2023).
OFP is common, with one survey of 45,711 US households found that 22% of the population reported one or more types of OFP (AAOP, 2023). OFP and TMD have been associated with multiple comorbid conditions to include: chronic fatigue syndrome, fibromyalgia, headache, PTSD, gastroesophageal reflux disease, and psychological distress (AAOP, 2023; de Leeuw and Klasser, 2018). Anxiety and depression are commonly seen OFP, and they have been shown to be a risk factor in the development of TMD (Kindler et al., 2012). Another known risk factor for pain in patients with OFP are sleep disturbance and sleep disorders, which are a common comorbidity (AAOP, 2023; Crandall, 2018). Currently, management and treatment of OFP emphasizes the biopsychosocial approach (Engel, 1977), which may involve an interdisciplinary team (AAOP, 2023; de Leeuw and Klasser, 2018). When approaching patient care within the biopsychosocial model, clinicians may want to consider addressing areas of unforgiveness as an additional strategy for patient care, especially with the growing evidence of the benefits of forgiveness.
Though research supports the benefits of forgiveness in many areas of health, to include pain, its impact in OFP has not been researched. If similar associations between forgiveness and OFP are discovered, it is reasonable to suggest that forgiveness would promote health improvement outcomes for patients with these conditions when managed within a biopsychosocial approach.
The specific aims of this study were to determine (1) the prevalence and intensity of forgiveness in a sample of OFP patients, and (2) the associations among level of forgiveness with pain severity, the type of OFP, anxiety, depression, sleep disturbance, perceived stress, and anger.
Methods
Participants and inclusion/exclusion criteria
A total of 380 active-duty military service members were included in this retrospective cohort study. All patients in this study were evaluated either by an American Board of OFP certified dentist or by a supervised OFP resident. Participants were seen at the OFP Center which is part of the Naval Postgraduate Dental School in Bethesda, MD, a tertiary care referral-based clinic. Each patient completed an intake packet prior to their initial appointment. Data from patient intakes and medical records were collected over a 21-month period with approval from the Walter Reed National Military Medical Center IRB (WRNMMC-0219-0248). Inclusion criteria included an OFP diagnosis fitting one of the following diagnostic categories: myogenous, arthrogenous, neuropathic, neurovascular, intraoral and other. Exclusion criteria excluded patients that were under 18 years of age. All other active-duty patients with complete data were included in this study.
Measures
This study assessed the prevalence and intensity of self-reported forgiveness and other variables through a retrospective chart review. A primary OFP diagnosis was recorded for each patient at completion of their initial examination and was the one determined to be most consistent with the patient’s chief complaint. Diagnosis followed the American Academy of OFP (AAOP) Guidelines for Assessment, Diagnosis, and Management. The AAOP Guidelines are consistent with the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) Axis I diagnoses for TMJ disorders and masticatory muscle disorders and with the International Classification of Headache Disorders, third Edition (ICHD-3) diagnoses for primary headache disorders and most neuropathic pain disorders (Schiffman et al., 2014). Primary OFP diagnoses were placed into one of five diagnostic categories: myogenous (e.g. masticatory myalgia, myofascial pain, temporal tendonitis), arthrogenous (e.g. disc displacement, arthralgia, osteoarthritis), neuropathic (e.g. trigeminal neuralgia, neuropathy), neurovascular (e.g. migraine, other headache type), odontogenic (e.g. cracked tooth), and other (e.g. bruxism, obstructive sleep apnea, cervicalgia). Although it is typical for OFP patients to have more than one diagnosis, this study only considered the first diagnosis for each patient which was determined to be the chief complaint.
Demographics and Health History Questionnaire
All participants completed a brief demographic and health history questionnaire. Recorded information included sex, age, race, ethnicity, military rank, and branch of service.
Pain measures
Patients rated “average pain intensity” and “worst pain intensity” on a numeric rating scale ranging from 0 to 10 (with zero indicating “no pain” and 10 indicating “the worst pain imaginable”). If a patient gave their answer as a range (e.g. worst pain 5–6/10), the greater number (i.e. 6/10) was recorded. Patients were also asked when their pain first began. Pain duration was recorded in months. Again, if the patient gave their answer as a range, the greater duration of pain was recorded.
Anger and stress measures
Patients rated levels of anger and perceived stress on a numeric rating scale ranging from 0 to 10 (with zero indicating “none” and 10 indicating ‘worst possible). If a patient gave a range, the greater number was recorded.
Heartland Forgiveness Scale (HFS)
The Heartland Forgiveness Scale measures an individual’s tendency toward forgiveness (Thompson et al., 2005). It is comprised of 18 questions which are measured as a total score and three subscale sores: forgiveness of self, others, and situations. The Total HFS score can range from 18 to 126 with higher scores suggesting higher level of forgiveness. The HFS has demonstrated good psychometric properties (Thompson et al., 2005).
Generalized Anxiety Disorder-7 (GAD-7)
The GAD-7 is a 7-item measure used to assess presence of symptoms of generalized anxiety over the previous 2 weeks. The GAD-7 is a widely used assessment instrument and has demonstrated good psychometric properties in clinical and research applications (Spitzer et al., 2006). The GAD-7 is a commonly used measure in chronic pain treatment and research with strongly demonstrated reliability and validity (Kroenke et al., 2016).
Patient Health Questionnaire-9 (PHQ-9)
The PHQ-9 is a 9-item measure of the presence and severity of depressive symptoms over the previous 2 weeks. The PHQ-9 is a widely used assessment instrument and has demonstrated good psychometric properties in clinical and research applications (Kroenke et al., 2001). The PHQ-9 is a commonly used measure in chronic pain treatment and research with strongly demonstrated reliability and validity (Orbach and Knibbe, 2016).
Insomnia Severity Index (ISI)
The ISI is a brief instrument that assesses the severity of both nighttime and daytime components of insomnia. It has been validated for use as a screening tool to detect sleep disturbances in research and clinical settings (Bastien et al., 2001), and is effective in assessing insomnia in orofacial pain patients (Dong et al., 2025).
Statistical analysis
Patient demographic, clinical characteristics, and psychological scale scores were reported with descriptive statistics and compared among patients who had a valid HFS total score available (N = 380) by presence of high forgiveness defined by HFS scoring as HFS total (score > 89), self (score > 29), situations (score > 29)) and HFS others (score > 29) scales (Thompson et al., 2005). Bivariate comparisons used two-sample t-tests for continuous characteristics and Chi-square or Fisher’s exact tests for categorical characteristics. To evaluate hypothesized independent associations of pain and psychological scores with forgiveness levels, multivariable linear regression models were fit to HFS total as the outcome with continuous pain, stress, anger, PHQ, GAD, and ISI scores as independent variables and demographic (age (per 10 years), sex, military status) and diagnosis type (arthrogenous, myogenous, or other) as potential confounders. Continuous scale scores were standardized (divided by their standard deviation) to facilitate comparison of effect estimates. Low variance inflation factors (<5) indicated that multicollinearity was not a concern.
Results
Demographic, pain, and psychological characteristics of the patients (N = 380) included in this study are shown in Table 1, by HFS category. The HFS categories, based on cut-scores determined through psychometric validation are Low (<54), Medium (55–89), and High (>89) with higher scores indicative of higher forgiveness. The present study sample only had five patients that scored in the Low category, so they were grouped with patients in the Medium category. Mean age of all patients was 36.1 years old (SD = 8.8) with a range from 20 to 69 years. Most patients were female (53.4%) and white (66.3%). Branch of service was relatively evenly divided among Air Force (26.6%), Army (31.8%), and Navy (22.9%), with the remaining patients serving in the Marines, Coast Guard, and Uniformed Public Health Service (18.7%). Masticatory muscle disorders were the most common primary OFP diagnosis (67.4%), followed by TMJ disorders (17.4%), headache disorders (3.9%), neuropathic pain disorders (3.4%), intraoral disorders (2.9%), and other disorders (5.0%). Mean pain intensity was 4.36 (SD = 1.9) and worst pain intensity was 7.28 (SD = 1.9) on a 0–10 numerical rating scale with 0 meaning no pain and 10 being the worst pain. Duration of pain complaint ranged from 1 month to 312 months with a mean of 52.88 (SD = 58.3) months. Mean perceived stress level was 5.48 (SD = 2.5) and mean anger was 2.48 (SD = 2.4) on a 0–10 numerical rating scale with 0 meaning no stress or anger and 10 being the worst.
Patient characteristics by HFS total score.
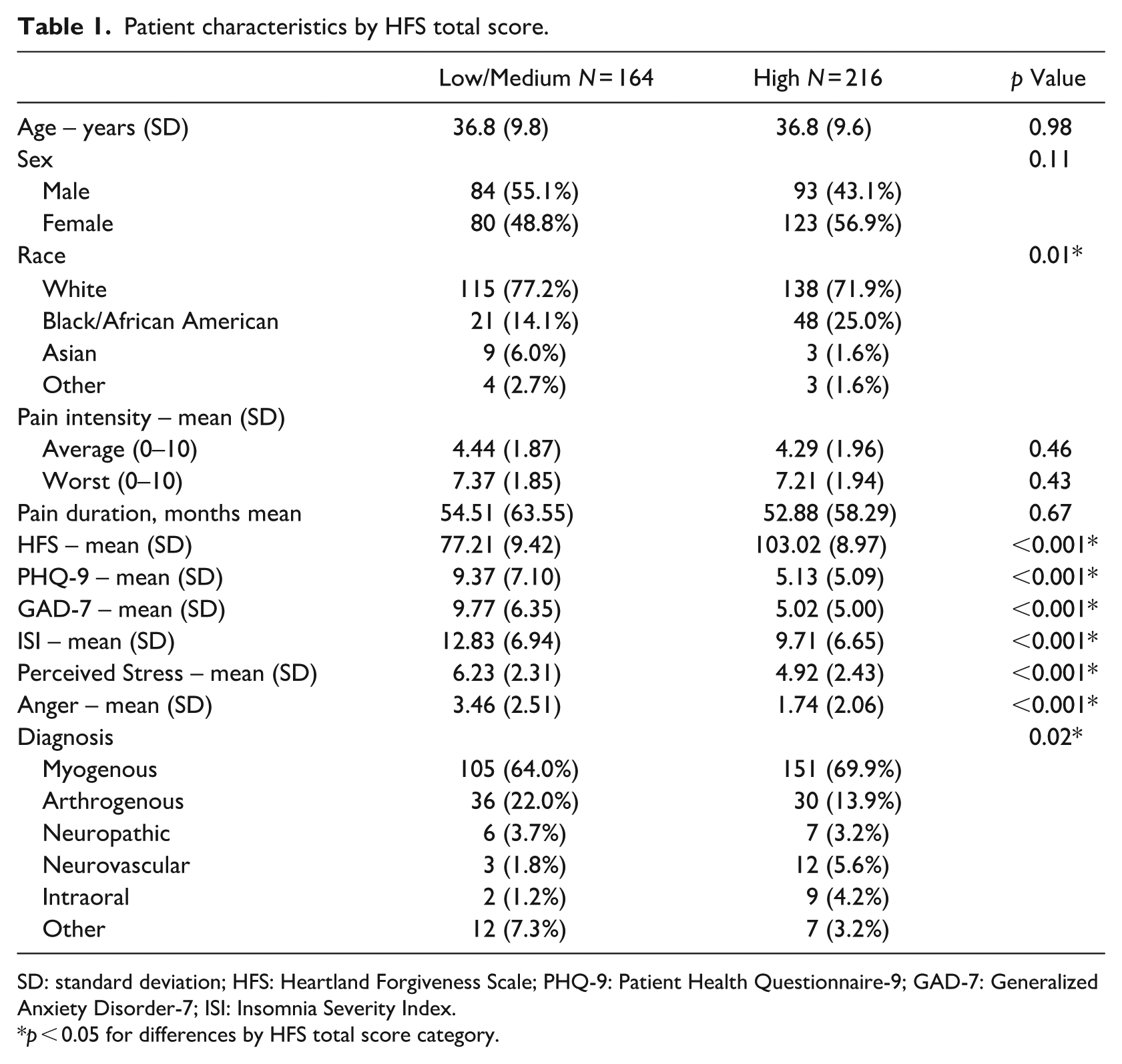
SD: standard deviation; HFS: Heartland Forgiveness Scale; PHQ-9: Patient Health Questionnaire-9; GAD-7: Generalized Anxiety Disorder-7; ISI: Insomnia Severity Index.
p < 0.05 for differences by HFS total score category.
Patients scoring in the Low/Medium forgiveness range (N = 164, 43.2%) were compared to patients scoring in the High forgiveness range (N = 216, 56.8%) on demographic, psychological and functional measures (see Table 1). There was no significant difference in age or sex between the two forgiveness groups. There was a significant difference between the groups on race distribution, most likely due to the higher number of both white and black/African Americans in the High forgiveness group. Diagnostic Category was also significantly different between the two groups, likely due to the higher number of Myogenous cases in the High forgiveness group.
Comparing the two groups on the psychological and functional characteristics, the Low/Medium forgiveness group was significantly higher on anxiety, depression, and sleep disturbance (p < 0.001). The Low/Medium group also reported significantly higher levels of perceived stress and anger (p < 0.001). There was also no significant difference in average or worst pain severity between the two groups. Figure 1 displays differences between the two groups on anxiety, depression, and sleep disturbance.
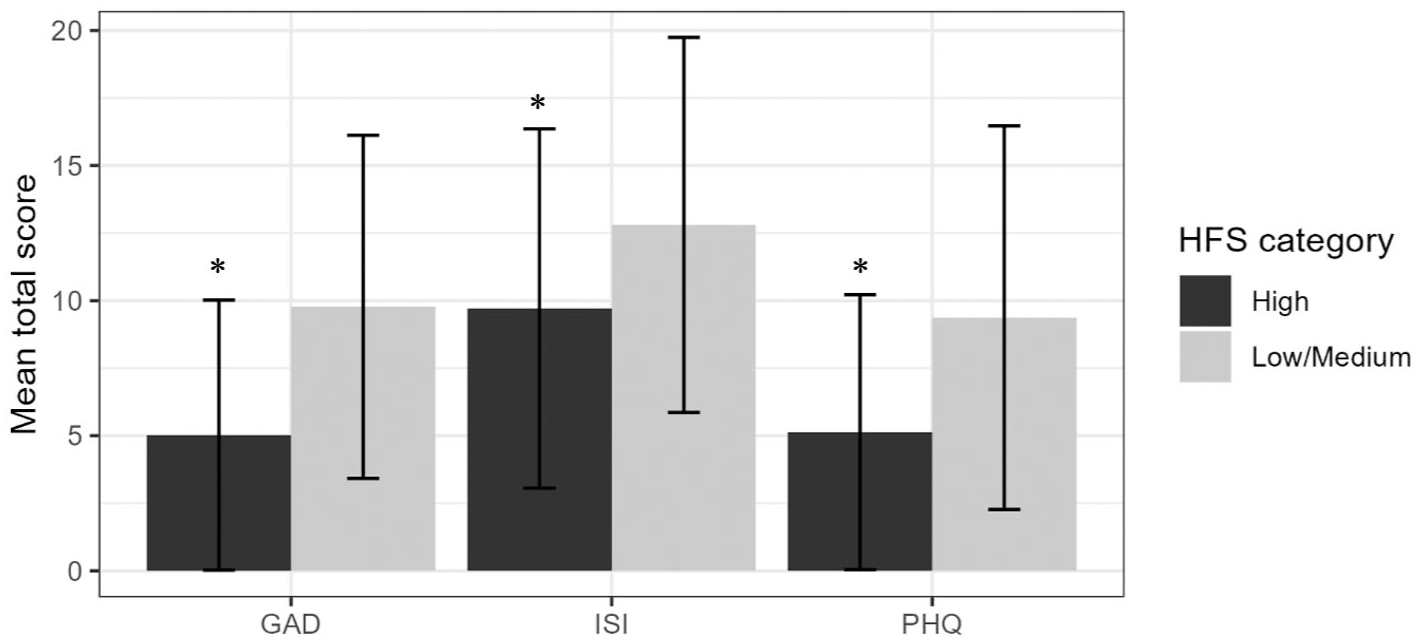
GAD-7 (anxiety), ISI (sleep dysfunction), and PHQ-9 (depression) mean scores stratified by HFS category. Bars represent standard deviation.
Predictors of HFS score
Multiple regression results
In a multivariable model of demographic and clinical characteristics as independent variables and HFS total as the dependent variable, higher GAD score was associated with lower HFS score (Beta = −5.83 per SD GAD increase; p < 0.01). Arthrogenous diagnosis was associated with lower HFS score versus Myogenous (Beta = −6.13; p < 0.01) or other diagnosis (Beta = −5.83; p = 0.02). Higher anger was associated with lower HFS score (Beta = −3.53 per SD anger increase; p < 0.01). See Table 2.
Beta coefficients estimated from multivariable linear regression model of HFS score as dependent variable.
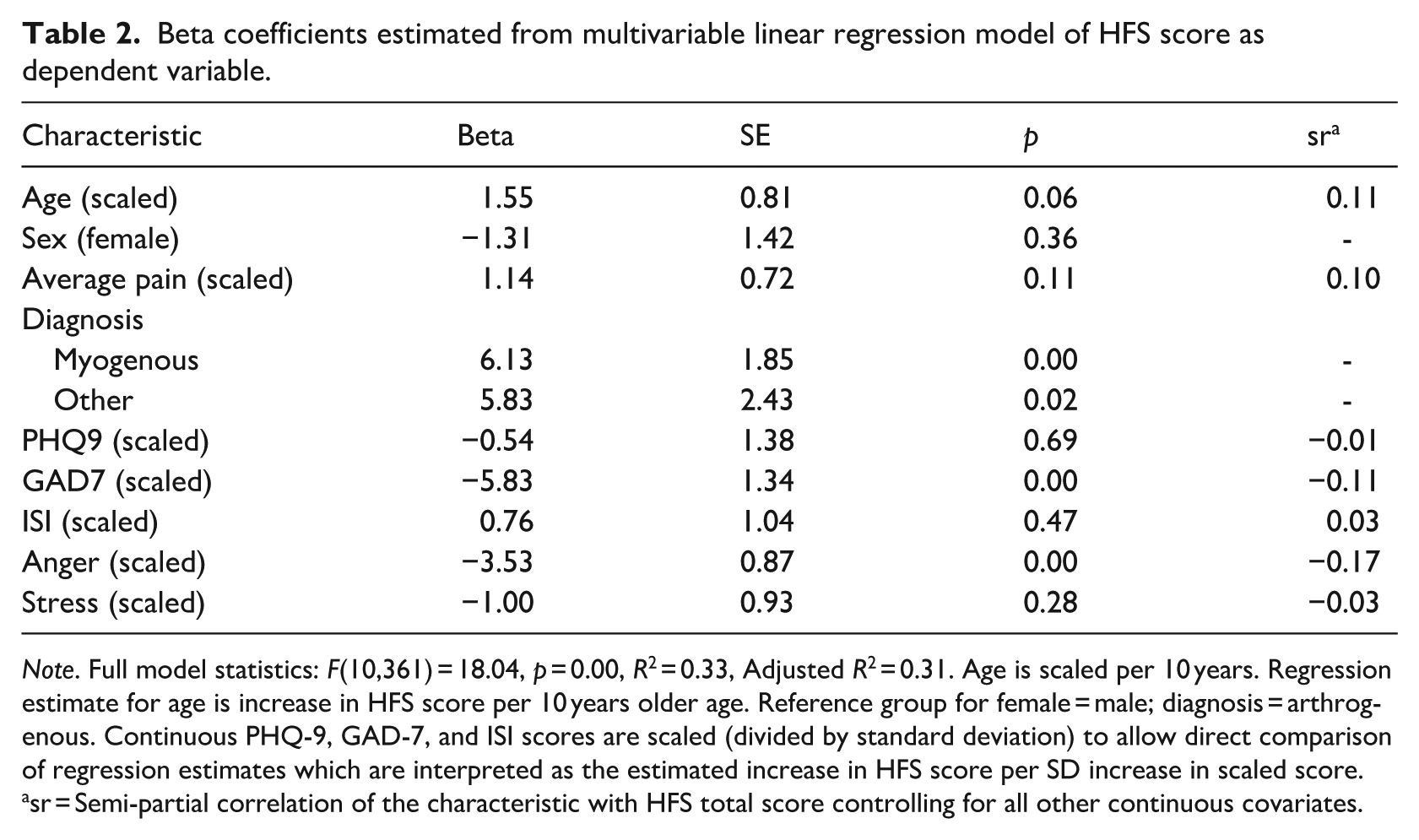
Note. Full model statistics: F(10,361) = 18.04, p = 0.00, R2 = 0.33, Adjusted R2 = 0.31. Age is scaled per 10 years. Regression estimate for age is increase in HFS score per 10 years older age. Reference group for female = male; diagnosis = arthrogenous. Continuous PHQ-9, GAD-7, and ISI scores are scaled (divided by standard deviation) to allow direct comparison of regression estimates which are interpreted as the estimated increase in HFS score per SD increase in scaled score.
sr = Semi-partial correlation of the characteristic with HFS total score controlling for all other continuous covariates.
Discussion
The primary aim of this study was to assess the prevalence and intensity of forgiveness in a active-duty military population with OFP. The present study used the HFS to assess forgiveness. The HFS average forgiveness score in this sample (mean 91.9 and median 92) is comparable to another study on low back pain and forgiveness using the HFS where the median score was 85 (O’Beirne and Harmon, 2024). These results are also similar to the HFS measure normative data that cites 93 as an average forgiveness score, suggesting that the prevalence and intensity of forgiveness in OFP patients is typical to the general population based on normative data for the HFS (Thompson et al., 2005).
This active-duty military sample was divided into two groups based on their HFS scores, which were classified as Low/Medium forgiveness and High forgiveness. There is a substantial proportion of participants in the present study that scored in the high range on the HFS, which is in contrast to a cohort study of low back pain patients where over half the participants were in the low to average forgiveness range (O’Beirne and Harmon, 2024).
The second aim of the study was to evaluate the associations among levels of forgiveness with pain severity, the type of OFP, anxiety, depression, sleep disturbance, perceived stress, and anger. There was not a significant relationship between forgiveness and pain severity, which contrasts with findings from other studies that suggest higher forgiveness is associated with lower pain severity (Carson et al., 2005; O’Beirne and Harmon, 2024). This discrepancy may be due to the complex biopsychosocial nature of chronic OFP, where multiple psychological, social, and physiological factors interplay in ways that are not easily captured by pain severity alone. In this study, pain severity was assessed using a numeric rating scale (NRS), however other validated pain measures exist such as the visual analog scale (VAS), verbal rating scale (VRS), and faces pain scale-revised (FPS-R). In a validity study of pain severity measures, the VAS nor the NRS were associated with additional pain severity factors such as pain unpleasantness and pain interference (Thong et al., 2018). Future studies may consider using the VRS or FPS-R to capture these additional dimensions of the subjective pain experience. (Jensen and Karoly, 2011; Thong et al., 2018). Another option would be using the McGill Pain Questionnaire (MPQ) which assesses the quality and intensity of the subjective experience of pain in multiple dimensions including affective (Melzack, 1975). While the original MPQ is quite lengthy with 78 descriptive words, the short form has 15 words and only takes a few minutes to complete. The MPQ is widely used in pain management and treatment settings and has demonstrated validity in OPF’s (van Wijk and Hoogstraten, 2002).
The five broad diagnostic categories within OFP used in the present study are: myogenous, arthrogenous, neuropathic, neurovascular, intraoral and other. The data suggest that participants with a primary myogenous diagnosis (e.g. masticatory or cervical muscle pain) are more likely to be more forgiving compared to a primary arthrogenous diagnosis (e.g. disc displacement, osteoarthritis). This result is surprising as masticatory muscle pain has been more strongly associated with higher psychological distress in many studies (Bair et al., 2016; Kindler et al., 2012; Lindroth et al., 2002). Other studies support the co-occurrence of psychological distress and dysfunctions of the masticatory muscles, typically in females, however a causal relationship is not clearly established (Wieckiewicz et al., 2017).
Participants in the present study with lower levels of forgiveness demonstrated significantly higher levels of depression, anxiety, sleep disturbance, perceived stress and anger. These results are consistent with other studies that demonstrate lower levels of forgiveness are associated with negative emotions, rumination, and perceived stress (Carson et al., 2005; O’Beirne et al., 2020).
Forgiveness may serve as a buffer for the development of psychological distress and even pain severity. A study of fibromyalgia patients found a positive association between forgiveness and resilience along with a strong relationship between higher resilience and lower pain severity (Saffarinia et al., 2016). It may be that higher forgiveness may strengthen positive coping skills in pain patients which can result in lower affective distress, higher resilience and improvements in daily functioning. Additional support for the potential importance of forgiveness has been demonstrated in veterans diagnosed with posttraumatic stress disorder. In one study, Karaırmak and Güloğlu (2014) found that anger and negative affect mediated the relationship between forgiveness and both PTSD and depression. Indeed a systematic review and meta-analysis evaluating forgiveness therapy for the promotion of mental well-being suggests that forgiveness interventions are effective in reducing depression, anger and hostility and distress (Akhtar and Barlow, 2018).
When evaluating the multivariable linear regression model with HFS as the dependent variable, higher anxiety and anger was strongly associated with lower levels of forgiveness. Anger has been a topic widely studied in pain research. In a recent systematic review of several key anger-related variables that were associated with pain-related outcomes, an association with perceived injustice was significant (Adachi et al., 2022). Forgiveness is a means to heal from the emotional distress caused by the perceived injustice. Anger is a significant factor associated with higher pain severity and chronicity, thus it is reasonable to suggest that forgiveness may act as a buffer or as an effective intervention in pain management (Yarns et al., 2022). This is consistent with a study by Carson, et al. that concluded patients reporting less “forgiveness of others” experience higher chronic back pain intensity and psychological distress mediated by increased state anger (Carson et al., 2005).
While the majority of our sample demonstrated high forgiveness, nearly half (43%, N = 164) of the patients in the present study scored in the low to medium forgiveness range, which was also lower than the general population without chronic pain (Thompson et al., 2005). This finding points to the relationship between the psychological burden in individuals struggling with OFP and highlights forgiveness as a potentially relevant factor in their overall health. Forgiveness interventions may be considered as part of an inter-disciplinary approach in managing the OFP patient. Forgiveness interventions have largely been developed based on the work of Enright and Worthington and can be delivered individually or in group-based settings. These models define forgiveness, emphasizing its potential benefit and encourage developing empathy toward the offender (López et al., 2021). Current literature demonstrates benefits of forgiveness interventions in various chronic pain conditions like fibromyalgia and chronic widespread muscle pain (Bashir et al., 2025; Lee and Enright, 2014).
Current literature supports the benefits of forgiveness interventions within the biopsychosocial model framework. Research done by Witvliet et al. demonstrate that engaging in compassionate reprisal of an offender through active forgiveness will reduce anger, negative affect, and rumination while at the same time increasing empathy and prosocial orientation. Sleep has also been shown to improve with compassionate reprisal, to include faster sleep onset and less sleep disturbances as compared to negatively ruminating about the offense (Witvliet et al., 2022). Their findings show that higher levels of forgiveness are linked to positive psychological, social, and biological outcomes, including reduced anger, restored relationships, and better sleep. Application of a forgiveness intervention in an Orofacial Pain population could also consider integrating such aspects to quantify its effect on pain. A forgiveness intervention may not result in a direct reduction in pain severity, however by modulating affective factors which are known risk factors for the development and chronicity of OFP’s (Fillingim et al., 2013), it aligns with interdisciplinary pain management within a biopsychosocial framework.
This study has several limitations that must be kept in mind when interpreting the data and results. The study sample was restricted to active-duty military personnel. Military members may be less likely to report levels of unforgiveness due to wanting to align oneself within military culture or military clearances. Military culture may encourage patients to present themselves as someone who strongly adheres to military values such as resilience, duty, commitment and service before self. Consequently, service members may have been hesitant to disclose their feelings of unforgiveness at the risk of causing division amongst their units or admitting an emotional vulnerability that may be detrimental to their military career. These social and institutional pressures may have led to underreporting levels of unforgiveness and therefore altered the results. The designs of future studies may benefit from providing anonymous surveys to assess forgiveness, which may aid in reducing pressures of maintaining military bearing and provide a more accurate representation of the emotional experiences of military members with OFP.
Conclusion
In conclusion, this study highlights the complex interplay between forgiveness, psychological well-being, and OFP. While the overall forgiveness levels in this active-duty military sample were relatively high, a substantial portion of participants fell within the low to medium forgiveness range, underscoring the psychological burden associated with OFP. The findings reinforce the association between lower forgiveness and higher levels of anxiety, depression, sleep disturbances, perceived stress, and anger. Although no significant relationship was found between forgiveness and pain severity, the potential role of forgiveness as a psychological buffer in pain management remains evident. Given the growing body of research supporting forgiveness interventions in chronic pain conditions, integrating such approaches into interdisciplinary treatment strategies may enhance overall patient well-being. Future research should further explore the mechanisms underlying forgiveness and pain perception, as well as the efficacy of targeted forgiveness interventions in OFP management.
Footnotes
Ethical considerations
This study was approved by the Walter Reed National Military Medical Center IRB (WRNMMC-0219-0248).
Consent to participate
All participants completed written informed consent and HIPAA documents for this study – Walter Reed National Military Medical Center IRB (WRNMMC-2019-0248).
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data is available on request.*
Disclaimers
The opinions or assertions contained herein are the private ones of the authors and are not to be construed as official or reflecting the view of the Department of the Air Force/Navy/Army, Department of Defense or the Uniformed Services University of the Health Sciences. Research data derived from an approved Walter Reed National Military Medical Center Institutional Review Board protocol number WRNMMC IRB approval (WRNMMC-0219-0248). We are military service members. This work was prepared as part of our official duties. Title 17 U.S.C. 105 provides that copyright protection under this title is not available for any work of the United States Government. Title 17 U.S.C. 101 defines a U.S. Government work as work prepared by a military service member or employee of the U.S. Government as part of that person’s official duties.