
Abstract
Food insecurity continues to be a critical social determinant of health in the United States. Existing research on food insecurity within clinical populations has focused on specific health conditions. However, this approach may limit the applicability of findings to broader patient groups. In the current study, adult patients (N = 104) identified as food insecure by a medical provider completed measures of food insecurity, mental health, and quality of life. Anthropometric measurements and blood pressure were also collected. After adjusting for sociodemographic factors, multiple linear regression analyses determined greater food insecurity was associated with higher levels of anxiety and depression. There was not a significant effect of food insecurity on quality of life, BMI, systolic blood pressure, or diastolic blood pressure. Results show that adults receiving medical care may be especially vulnerable to the effects of food insecurity, where there can be detrimental effects on mental health.
Introduction
Food insecurity, defined as limited ability to access enough safe and nutritious foods for an active and healthy life, remains a significant social determinant of health in the United States (United States Department of Agriculture [USDA], 2015). In 2023, approximately 13.5% of U.S. households, or 18 million households, experienced food insecurity at some point during the year (Rabbitt et al., 2024). This represents a slight increase from the previous year, highlighting the ongoing challenges that many Americans face in accessing adequate, nutritious food (Rabbitt et al., 2023). Risk of food insecurity is greater for individuals experiencing mental health problems and chronic disease (Coleman-Jensen et al., 2013) and is often a result of inadequate financial resources, limited access to transportation (Ver Ploeg et al., 2009), low nutrition literacy (Gregório et al., 2018), and stressors related to poverty (Wolfson et al., 2021).
Importantly, individuals experiencing food insecurity are at increased risk of cardiovascular disease (CVD; Chang et al., 2022), obesity (Pan et al., 2012), and other chronic health problems (Gregory and Coleman-Jensen, 2017). Most studies examining food insecurity in clinical populations have been conducted on specific health conditions, such as human immunodeficiency virus (HIV), surgical trauma, diabetes, or cardiometabolic risk (Jones et al., 2025; Murkey et al., 2024; Olstad et al., 2022; Singer et al., 2015). While this approach helps to clarify the unique association between specific diseases and food insecurity, it can limit the generalizability of findings to broader patient groups and may overlook the diverse ways food insecurity affects individuals across different clinical settings and health statuses. Because CVD is the most prevalent disease among patients with chronic conditions, including those mentioned above, the relationship between food insecurity among patients with CVD may be more generalizable to many patients with chronic conditions than other diseases (Aïdoud et al., 2023). This consideration is especially important among older adults in most clinical settings. In one review, 46% of older adults had at least two or more chronic conditions globally (Zhu et al., 2025). In all, the prevalence of CVD among multimorbid patients and increased occurrence of multimorbidity among older adults suggests that the investigation of food insecurity among patients with CVD may be most relevant in clinical settings due to its greater generalizability. Furthermore, healthcare expenditures (e.g. inpatient, emergency department, outpatient) associated with clinical care visits are higher for individuals with food insecurity (Dean et al., 2020); therefore, the clinical environment serves as a unique access point in understanding and addressing food insecurity as a part of clinical care. However, it is important to investigate food insecurity across a broad range of clinical settings, as food insecurity can occur for anyone regardless of their health status. The current study seeks to address these limits by examining physical and mental health in a cohort of individuals across outpatient clinics that serve individuals experiencing food insecurity.
Theoretical framework
Food insecurity is a complex experience that is a part of a broader socioeconomic stress process. The Social Ecological Model (SEM) serves as a framework for examining factors that contribute to and are a result of challenges to food insecurity that can have an impact on health (Goldberg and Mawn, 2015; McLeroy et al., 1988; Tucher et al., 2021; Figure 1). While many studies about food insecurity are centered primarily on intrapersonal factors such as income or race/ethnicity, SEM highlights that individuals experiencing food insecurity are positioned in the context of overlapping and interacting environments. SEM targets five spheres of influence (intrapersonal, interpersonal, organizational, community, and public policy), where people and their environments are interdependent and require consideration when examining the impact on health. Current measures of food insecurity used in nationally representative studies are robust indicators of the extent to which individuals are worried about running out of food or not being able to buy more food. However, they mostly focus on financial resources rather than contextual factors that contribute to or exacerbate food insecurity. Understanding how individuals become food insecure and what they do when they are experiencing food insecurity can provide rich insight into strategies targeting multiple spheres of influence. Applying the SEM helps situate our findings within the clinical context by conceptualizing food insecurity not only as an economic condition but as a multilevel process shaped by environmental constraints, healthcare interactions, and structural determinants. This framework highlights how individuals navigate food insecurity within clinical settings and identify potential intervention points across levels, such as referral pathways, community food resources, social support, and policy-based assistance. In doing so, it provides a more comprehensive explanation of how food insecurity affects health in real-world clinical environments, extending beyond prior work focused solely on individual or demographic factors.
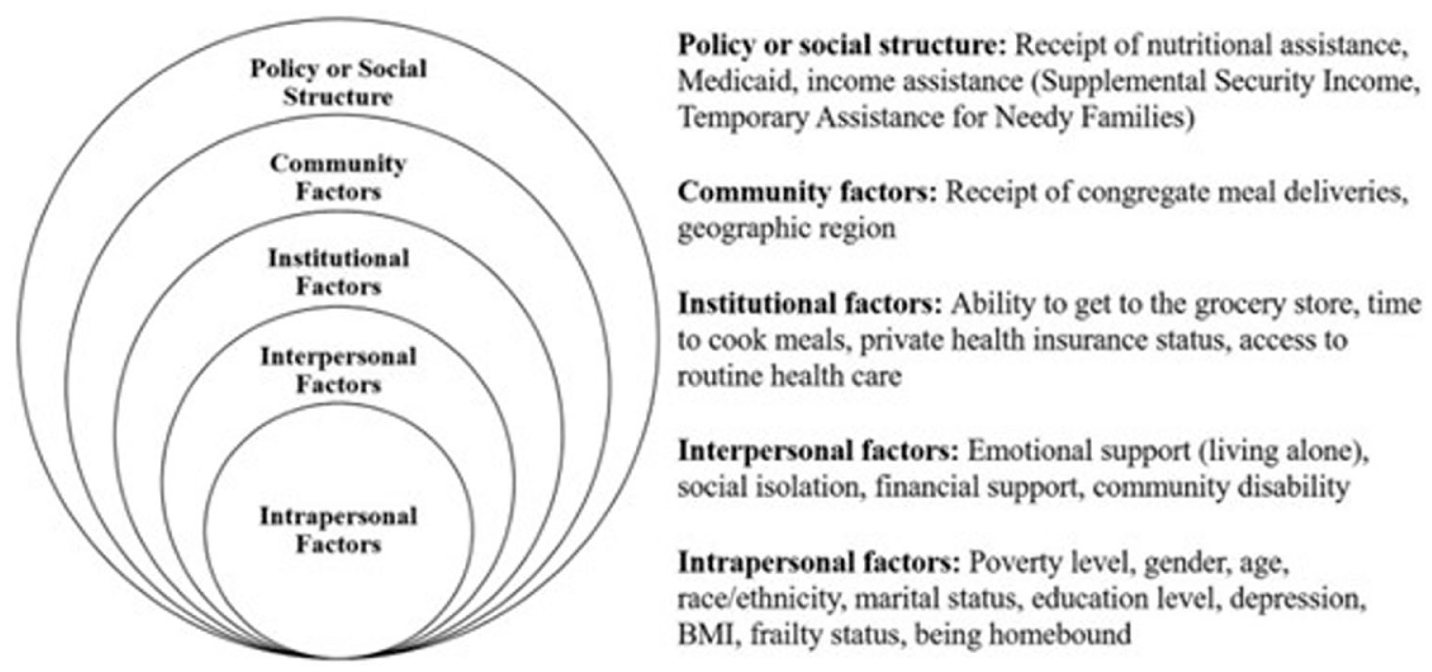
The social ecological model (SEM) of contributing factors to food insecurity (Goldberg and Mawn, 2015; Tucher et al., 2021).
Food insecurity and physical health
Food insecurity directly shapes dietary patterns by limiting access to nutritious foods and increasing reliance on calorie-dense, nutrient-poor options. In turn, this contributes to diet-related illnesses such as CVD and associated risk factors including hypertension or obesity (Brandt et al., 2022; Carvajal-Aldaz et al., 2022). Further, CVD is common across a broad range of health conditions, making it an especially important focus for understanding how food insecurity increases the risk of CVD that can potentially worsen existing health conditions (Redline et al., 2023). Several recent studies have highlighted the severe consequences of food insecurity, including higher rates of fatal and nonfatal coronary heart disease, heart failure, stroke, transient ischemic attack and peripheral arterial disease, and 49% higher odds of mortality (Sun et al., 2020; Walker et al., 2019). Food insecurity has also been shown to be associated with CVD risk factors including hypertension and obesity due to poor dietary intake (Bleich et al., 2023; Larson et al., 2017). Individuals living in households experiencing food insecurity are more likely to consume a diet high in processed foods and low in fruits, vegetables, and whole grains due to limited healthy options in food deserts and food pantries (Leung et al., 2020). Additionally, food insecurity is inherently linked to higher levels of stress, which may elevate the risk for cardiovascular conditions like hypertension (Seligman et al., 2010). Relationships between food insecurity and obesity are multifaceted and are influenced by various socioeconomic factors (Aguiar et al., 2022; Hernandez et al., 2017) as well as mental health (Gardizy et al., 2024), however, many studies focus on adolescent populations or community samples (Huang et al., 2024), underscoring the need to examine adult populations in clinical settings.
Food insecurity and mental health
A robust body of research has demonstrated consistent associations between food insecurity and poor mental health outcomes, including elevated symptoms of anxiety and depression. For example, adults experiencing food insecurity report symptoms of depression at over twice the rate of adults in food-secure households (Reeder et al., 2022). More recently, Juarez et al. (2025) examined food insecurity alongside socioeconomic determinants and found that food insecurity remained a significant predictor of both anxiety and depressive symptoms even after adjusting for financial strain, employment, and demographic covariates. It is not clear if the study included African American/Black or Hispanic/Latinx individuals, limiting generalizability to populations in the southern US. However, this work underscores that the psychological burden of food insecurity extends beyond material hardship and is shaped by complex structural and economic pressures. Worry plays an important role with obtaining adequate and nutritious foods and can be a source of profound stress for individuals experiencing food insecurity that causes increases in anxiety and depression symptoms (Bateson et al., 2025; Leung et al., 2024). Adults with other health problems and food insecurity are particularly vulnerable to depression, and adults with greater economic food insecurity and physical difficulties report higher levels of depression than those in economically secure households (Pak and Kim, 2020; Vaudin et al., 2022). This suggests that among food insecure adults, challenges related to physical health may intensify the relationship between food insecurity and depression. Those with very low food security also report significantly higher rates of depression, anxiety, and perceived stress compared to other low-income adults with high food security, highlighting the impact of food insecurity on mental health beyond economic status (Wolfson et al., 2021). Mental health problems such as anxiety and depression can also create barriers in accessing adequate and nutritious foods by inhibiting the ability for individuals to find and utilize resources, which can contribute to worsening food insecurity for those already experiencing challenges to food access (Gregory and Coleman-Jensen, 2017). However, the current literature on food insecurity and mental health focuses on depressive symptoms in younger populations and mothers (Gallegos et al., 2021; Laurenzi et al., 2020), highlighting the need for more comprehensive research in both male and female participants, as well as a broader cross-section of ages across adulthood.
Quality of life
In addition to physical and mental health outcomes, nationally representative samples have found that food insecurity is linked to poorer quality of life across multiple domains, including decreased cognitive function, reduced social roles, and increased levels of fatigue, pain interference, and sleep disturbance (Hanmer et al., 2021). Other associations have demonstrated that adults living with food insecurity report more days per month with poor physical health compared to food secure adults (Aljahdali et al., 2024). Additionally, food insecurity can foster a sense of social isolation and loneliness, thus compounding the impact on mental wellbeing (Hanmer et al., 2021; Park and Berkowitz, 2024). This pattern also highlights that the impact of food insecurity extends beyond nutrient deficits and financial hardship, suggesting its broader implications on overall health and well-being.
Current study
This study seeks to expand on previous work on food insecurity and health by examining the association of food insecurity and multiple clinical outcomes in a sample of adults in the Deep South, a region with high rates of poverty (Semega et al., 2017), chronic disease (Havranek et al., 2015), and food insecurity (Zekeri et al., 2016), yet that is often underrepresented in research studies. By focusing on Birmingham, this study aims to generate locally relevant insights and inform community-based strategies that address both food insecurity and health. To gain a deeper understanding of the role food insecurity plays across physical and mental health outcomes, the current investigation examined relationships between food insecurity, physical health (blood pressure, body mass index (BMI)), mental wellbeing (anxiety, depression) and quality of life in a clinically diverse sample of adult residents of greater Birmingham experiencing food insecurity. This approach aligns more closely with real-world health care settings, where improving food access can play a vital role in comprehensive patient care. We hypothesized that higher levels of food insecurity would be associated with worse physical health (higher systolic and diastolic blood pressure, and increased BMI), lower mental wellbeing (higher anxiety and depression) and decreased overall quality of life.
Method
Procedure
Adults were recruited beginning June 2024 from a local food pantry that partners with a regional medical center to serve patients identified as food insecure after standard social determinants of health screenings administered during clinic visits. Consistent with Institutional Review Board (IRB) requirements, we are unable to name the specific departments to protect clinic and patient confidentiality. However, referrals included a range of adult ambulatory care settings that serve insured, uninsured, and underinsured patients. We focused specifically on adults receiving care in clinical settings because food insecurity is highly prevalent in patients with chronic health conditions and is associated with higher healthcare utilization and expenditures (Dean et al., 2020). Clinical environments therefore represent a critical access point for identifying and supporting adults experiencing food insecurity, many of whom present with complex physical and mental health needs that may not be recognized in community-based samples. Further, studying food insecurity within clinical settings increases the relevance of findings for real-world patient care. After receiving a referral, patients reached out to the food pantry to schedule a time to pick up a food parcel. When patients arrived at the food pantry, food pantry staff provided study fliers with contact information to call the study site if interested in participating in a study about food access. Eligible adults were also directly recruited from the clinic by trained study staff. Individuals who expressed interest in person or after calling the study site were scheduled for a 1-hour interview. After providing informed consent, participants completed a questionnaire on a study tablet in a private testing room that took approximately 40 minutes to complete. Staff monitored the participants and were available to answer questions or provide clarification. To address physical limitations (e.g. visual impairment) or self-reported difficulty with reading, several participants were offered the opportunity to have the questionnaire read aloud to them. Participants were compensated $30 for their time. The University of Alabama at Birmingham, Institutional Board IRB-300011466-005 (approved 4/26/2024) approved all study procedures and materials.
Measures
Household food insecurity was measured using the six-item USDA Food Security Module (Blumberg et al., 1999). Adults indicated how often in the last 12 months they had experienced each situation related to having or obtaining food (e.g. “In the last 12 months, did you ever cut the size of your meals or skip meals because there wasn’t enough money for food?”). Answers for each item were scored on a three-point scale (0 = Never true, 1 = Sometimes true, 2 = Often true). Items were recoded and dichotomized following the scoring protocol for this module. Specifically, items answered Sometimes or Often true were recoded as 1. Items that were answered Never true were kept as 0. Dichotomized items were summed, with higher scores indicating greater food insecurity.
Anxiety was assessed using the seven-item Generalized Anxiety Disorder scale (Spitzer et al., 2006; e.g. “Over the last two weeks, how often have you been bothered by. . .feeling nervous, anxious, or on edge?”). Answers to each item were rated on a four-point scale: 0 = Not at all to 3 = Nearly every day (Spitzer et al., 2006). Items were averaged, with higher scores indicating greater anxiety.
Depression was measured using the 20-question Center for Epidemiologic Studies Depression Scale (CES-D Scale; Radloff, 1977). Adults indicated how often they felt or behaved in the last week (e.g. “I felt lonely”). Answers were scored on a four-point scale (0 = Rarely or none of the time to 3 = Most or all of the time.) and were then averaged with higher scores indicating more depressive symptoms.
Quality of life was assessed using one question from the PROMIS Global Health Scale (“In general, you would say your quality of life is. . .,”1 = Poor to 5 = Excellent; Cella et al., 2019).
Body mass index (BMI)
Trained research staff performed anthropometric measurements of participants’ height and weight using a stadiometer and scale, respectively. Adults were asked to remove shoes and bulky jackets or sweaters before anthropometric measurements. Two readings were taken for each weight and height to the nearest 0.01 kg or 0.10 cm. If the two readings differed by more than 0.20 kg or 0.50 cm, a third reading was taken. The two closest values were then averaged. If a participant was unable to stand for height and weight measurements, or if the interview was conducted remotely, self-reported values were recorded. A continuous measure of BMI was calculated from these values (BMI = weight (kg)/(height (m))2) and is the value used in the analysis.
Blood pressure
Blood pressure was measured following standardized procedures using a Carescape Dinamap V100 Vital Signs Monitor. Measurements were taken in a seated position with the cuff placed securely on the participant’s upper arm. Two readings were taken and the average of the two readings for both systolic and diastolic pressure was used for analysis. Participants were provided with individualized feedback identifying their classification within standard blood pressure categories (e.g. normal, elevated, stage 1 hypertension, stage 2 hypertension, hypertensive crisis), in accordance with blood pressure categories recommended by the American Heart Association.
Sociodemographics
Participants reported their age, race/ethnicity, sex, and household income. Sex was classified as male or female (0 = male; 1 = female) based on self-reported biological characteristics or medical records. Participant age and monthly household income were measured as continuous values. Due to small subgroup sizes race was recoded so that White adults were coded as 1, whereas other racial/ethnic groups were recoded as 0. Collapsing categories for analytic purposes is consistent with methodological guidance and when acknowledged as a limitation (Ross et al., 2020). Given the limited representation of several racial groups in our sample, dichotomization allowed us to model race consistently with best-practice recommendations.
Data analysis
Descriptive statistics and distributions of all variables were examined. Bivariate relationships between food insecurity, physical health, mental wellbeing, and quality of life were examined with Pearson’s correlations. Separate multiple regressions were performed for each dependent variable (blood pressure, BMI, anxiety, depression, quality of life). Models adjusted for age, sex, race, and household income. All analyses were conducted in SPSS (v. 25).
Power
A priori power analysis was conducted to determine the minimum sample size required for a linear regression model with one primary predictor and four covariates (five predictors total), using an alpha level of 0.05 and a desired power of 0.80. Results indicated that a sample size of approximately 92 participants would be sufficient to detect a medium effect size (f2 = 0.15). The final analytic sample included 104 participants, which exceeds this threshold and is therefore adequately powered to detect medium to large effects.
Results
The sample includes 104 patients from outpatient ambulatory clinics at a large medical center in Birmingham, Alabama (Mage = 52.31 years, SD = 12.36, range = 21.26–89.59; 65% female; 76% Black or African American, 20% White, 1% Native Hawaiian or Pacific Islander, 1% Mixed, 1% Other race,1% not reported; 91% Non-Hispanic/Latino/a). Table 1 provides sociodemographic characteristics for the sample. Missing data (8%) varied across variables and was handled with list wise deletion. Eighty-two percent (82%) of missing values were from participants who completed the research interview remotely and were unable to provide blood pressure, height, or weight measurements. The remaining missing values were from individuals who did not state their monthly income or who skipped the anxiety or depression items. The sample characteristics were similar to the demographic composition of the Birmingham metropolitan area (United States Census Bureau [USCB], 2023). As expected, food insecurity (Cronbach’s alpha = 0.71) was prevalent, with 40% of participants reporting very high food insecurity. The highest number of patients (35%) were referred to the partnering food pantry by a nurse-managed clinic for underserved patients with a diagnosis of heart failure. On average, patients reported low levels of anxiety (M = 1.16, SD = 0.96; Cronbach’s alpha = 0.94) and depression (M = 1.14, SD = 0.61; Cronbach’s alpha = 0.89). On average, patients also rated their quality of life as “poor” to “fair” (M = 2.49, SD = 0.80). Overall, the average BMI of the sample was 34.05 (SD = 10.67), which is classified as obese by the World Health Organization. Further, 59% of the sample met criteria for obesity (results not presented). Additionally, patients’ average blood pressure (systolic blood pressure M = 130.38, SD = 24.58; diastolic blood pressure M = 72.92, SD = 13.25) was just within the range classified as Stage 1 Hypertension by the American Heart Association, which is defined as systolic blood pressure of 130–139 mm Hg (Whelton and Carey, 2018).
Descriptive statistics for key variables among adults with food insecurity (n = 104).
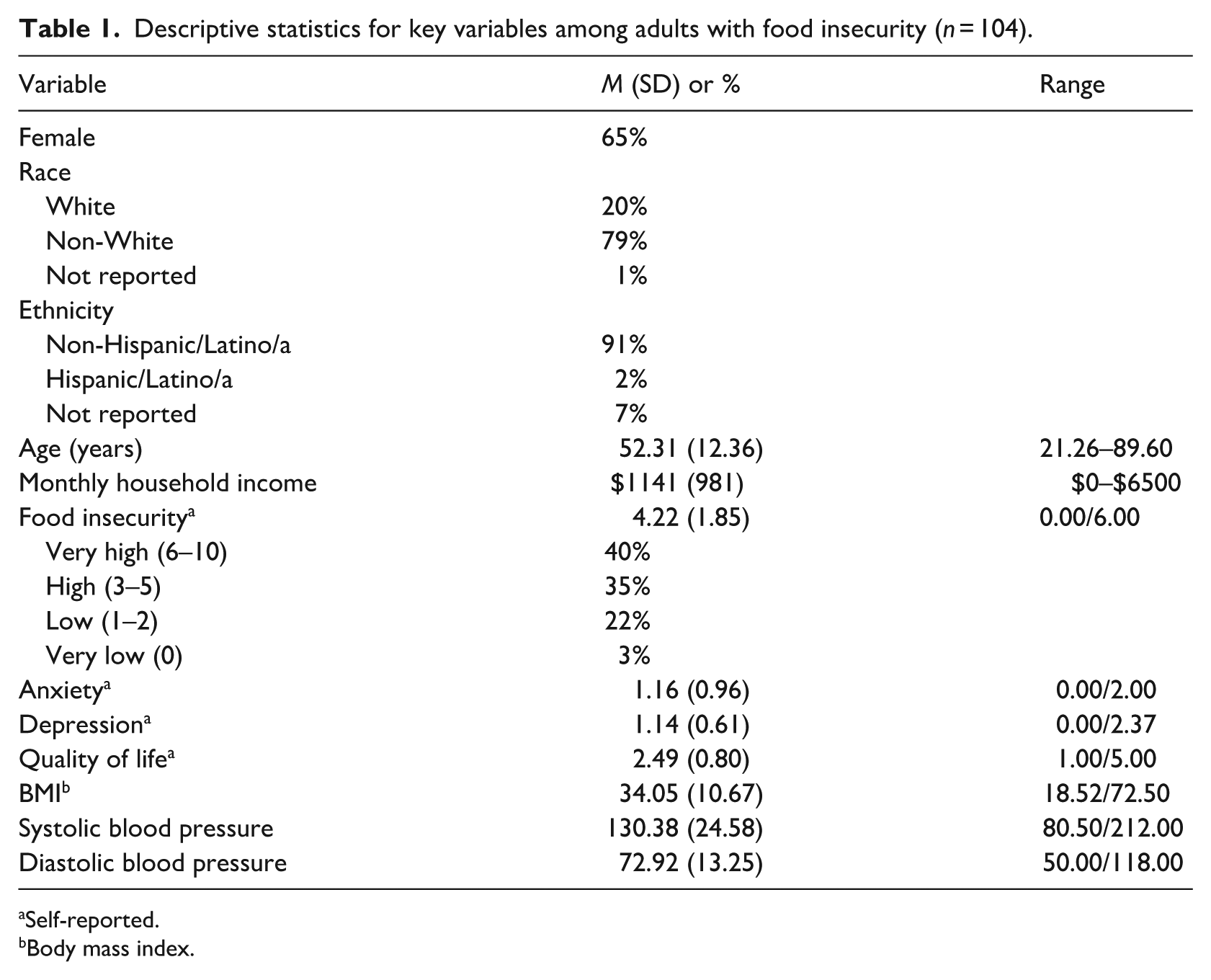
Self-reported.
Body mass index.
Table 2 provides the results from Pearson’s correlations examining bivariate relationships between food insecurity, physical health, mental wellbeing, and quality of life. Pearson product moment correlations demonstrated that greater food insecurity was associated with higher anxiety (r = 0.35, p < 0.01) and depression (r = 0.41, p < 0.01) and inversely related to quality of life (r = −0.27, p < 0.01). Anxiety and depression were positively associated (r = 0.76, p < 0.01) and anxiety was inversely related to quality of life (r = −0.22, p < 0.05). Systolic blood pressure was related to diastolic blood pressure (r = 0.56, p < 0.01), however, BMI was not correlated with any key variables.
Correlations between food insecurity, mental wellbeing, quality of life, and physical health among adults with food insecurity (n = 104).
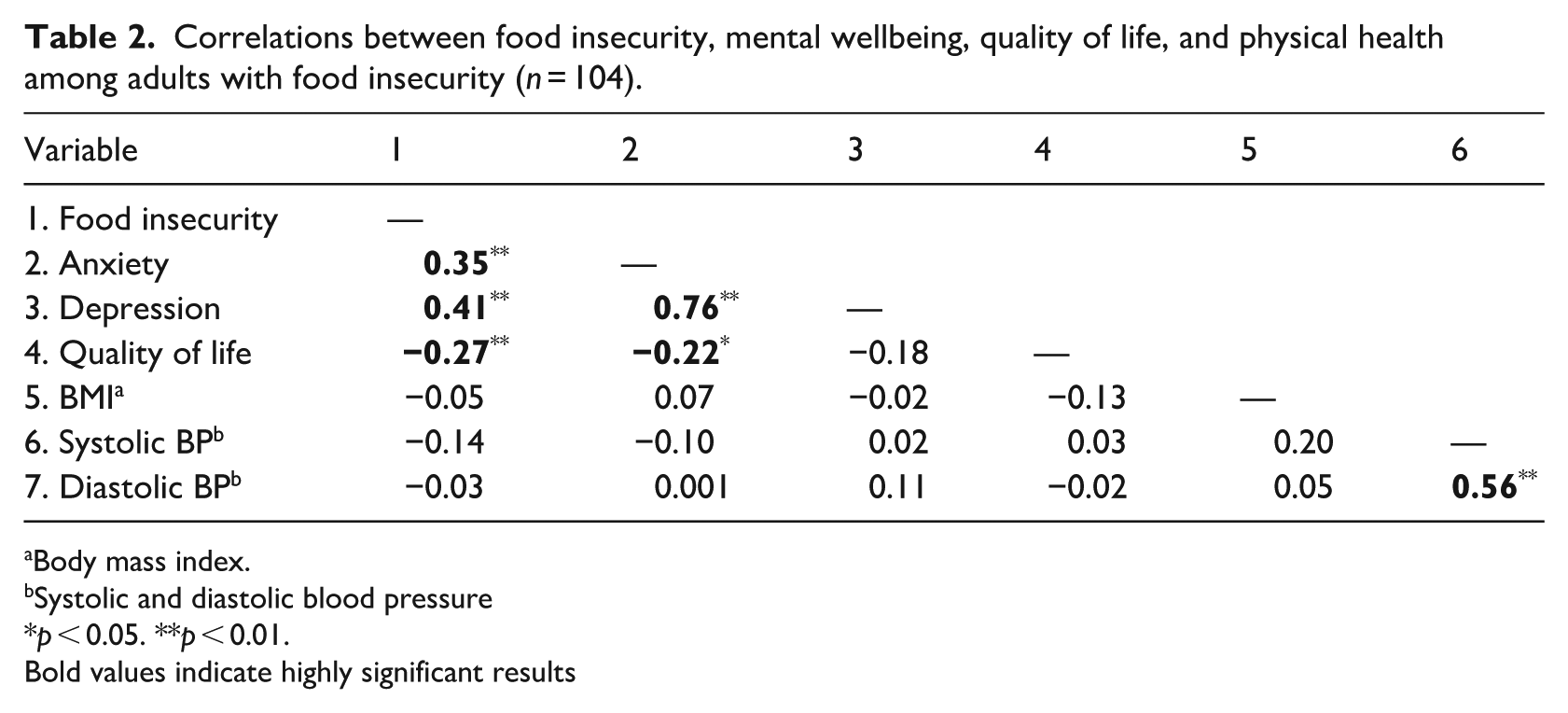
Body mass index.
Systolic and diastolic blood pressure
p < 0.05. **p < 0.01.
Bold values indicate highly significant results
Multiple linear regression analyses revealed that after controlling for sex, race/ethnicity, income, and age, greater food insecurity was associated with higher levels of anxiety (β = 0.32 p < 0.01) and depression (β = 0.40, p < 0.001; Table 3). There was not a significant effect of food insecurity on quality of life (β = −0.22 n.s.), BMI (β = −0.11 n.s.), systolic blood pressure (β = −0.11 n.s.), or diastolic blood pressure (β = −0.04 n.s.).
Standardized beta coefficients for food insecurity, physical health, mental wellbeing and quality of life among adults with food insecurity (n = 104).
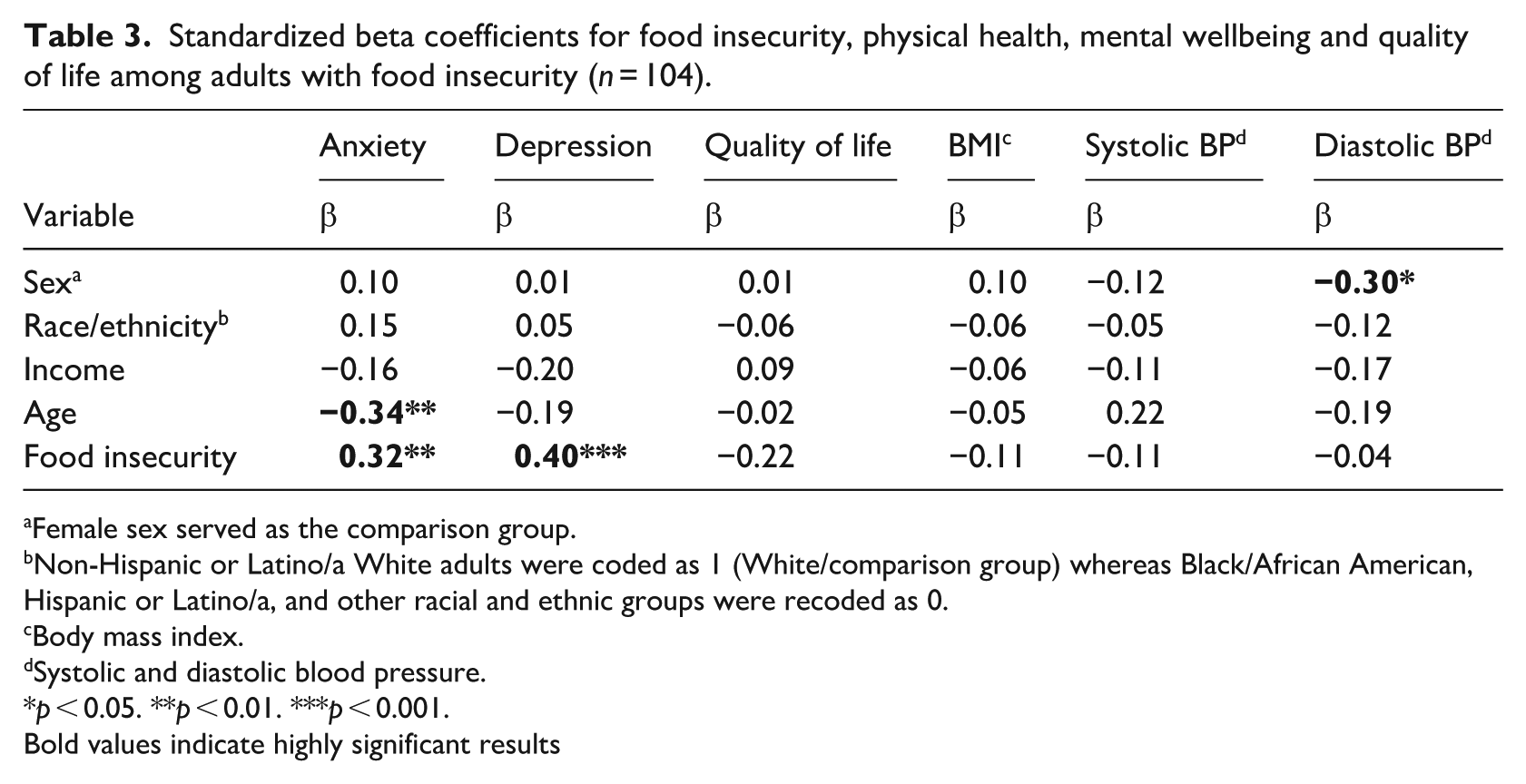
Female sex served as the comparison group.
Non-Hispanic or Latino/a White adults were coded as 1 (White/comparison group) whereas Black/African American, Hispanic or Latino/a, and other racial and ethnic groups were recoded as 0.
Body mass index.
Systolic and diastolic blood pressure.
p < 0.05. **p < 0.01. ***p < 0.001.
Bold values indicate highly significant results
Discussion
The current study examined relationships between food insecurity, physical health (blood pressure, BMI), mental wellbeing (anxiety, depression) and quality of life among patients who utilize a food pantry. We hypothesized that higher levels of food insecurity would be associated with worse physical health (increased BMI, higher systolic and diastolic blood pressure), lower mental wellbeing (higher anxiety and depression) and decreased overall quality of life. Our results showed that increased food insecurity was associated with higher anxiety and depression, which is consistent with previous cross-sectional studies of food insecurity and mental health (Pourmotabbed et al., 2020; USCB, 2023). Food insecurity may contribute to anxiety and depression through several mechanisms. For instance, uncertainty and worry related to food insecurity may result in stress, activating physiological and psychological responses that contribute to anxiety and depression by heightening emotional sensitivity and impairing emotional regulation (Abo Hamza et al., 2024). Similarly, food insecurity is associated with a sense of shame and embarrassment, which may occur when individuals feel compelled to accept food from charitable organizations such as food pantries. For example, waiting in long lines for food packages in public settings can make individuals feel vulnerable to being judged. Mothers who have had to stand in line for food pantry offerings perceived high amounts of stigma and also reported feelings of guilt and isolation that was linked to depression (Liebe et al., 2025).
Contrary to expectations, food insecurity was not significantly related to blood pressure or BMI. One reason for a lack of relationship may have been reliance on a single blood pressure value derived from two readings that were averaged together, which may not reflect an individual’s typical blood pressure, as values can fluctuate due to various factors such as stress, activity level, or time of day (Gordon and Mendes, 2021; Kallioinen et al., 2017). Use of an ambulatory blood pressure monitor (ABPM), which continuously records blood pressure, is useful in recording multiple blood pressure readings throughout the day and may more accurately capture average blood pressure more reliably. Although participants were queried about anti-hypertensive medication, many patients did not know the names of their drugs and/or why they were prescribed, therefore medication use could not be included in the analyses. Similarly, the continuous value for BMI was not related to food insecurity in the current study, which was unusual considering that 59% of the sample met the threshold for obesity as set by the American Heart Association (BMI >30). Higher BMI is common among adults experiencing food insecurity due to reliance on inexpensive, energy-dense foods and limited access to fresh, nutritious options. This pattern is well-documented in regions with high poverty and chronic disease burden, such as the area from which our sample was recruited. Although the average BMI in our sample fell within the obese range, consistent with prior research on food-insecure adults (Brito et al., 2025), BMI was not significantly associated with food insecurity in our analyses. It is possible that some patients with higher food insecurity weighed less than healthier individuals due to poor health (e.g. heart failure), which has been observed in previous studies; however, no patients in the current sample met criteria for being underweight (Milajerdi et al., 2019). Future studies examining food insecurity could use other measures of adiposity (e.g. waist circumference, waist to hip ratio) or utilize whether episodic versus persistent food insecurity predicts weight change. Finally, food insecurity was not uniquely related to quality of life, which is inconsistent with previous work that explored that relationship (Hanmer et al., 2021). One reason for the lack of significance may have been the quality-of-life measure, which was only one item. Although one-item scales for quality of life have been found to be a valid, reliable, and acceptable method of assessing physical, social, and emotional quality of life (Verster et al., 2024), it is plausible in the current sample, that a measure with more items, such as the World Health Organization Quality of Life Instruments (WHOQOL-BREF), which would have provided a more comprehensive evaluation of overall quality of life (Bush et al., 2010).
Implications
Results for the current study have important implications for addressing health outcomes related to food insecurity in the context of clinical care. Adults under the care of a physician or those with undiagnosed health conditions may be particularly vulnerable to the effects of food insecurity and may need additional support to prevent worsening health outcomes related to food insecurity. In the case of mental health problems that are related to food insecurity, clinical care settings can serve as an access point for adults who screen positive for food insecurity. In any context, however, it is critically important that there is a system of follow up and tracking that ensures that these individuals are connected to and can utilize food program resources. Individuals with food insecurity and receiving care for a chronic condition related to diet may greatly benefit from individualized programs that consider the health and barriers to food access that may affect patients experiencing food insecurity. One example of a successful program offered a food pantry collocated within the primary care clinic (Schutz and Brown, 2024). Patients reported that the food pantry was extremely convenient, especially for those who lacked transportation, and aided patients in aligning their diets with physician recommendations. Similarly, initiatives that provide personalized assistance with federal food program (e.g. Supplemental Nutrition Assistance Program (SNAP)) applications can reduce barriers and ensure access to available food resources (Schutz and Brown, 2024). Future studies should examine the impact of establishing a food pantry within the clinic environment while providing greater support in completing applications to determine if these types of programs can reduce food insecurity in adult samples such as the one in the current study. Importantly, food insecurity co-occurs with other socioeconomic factors, such as unemployment, unstable housing, or difficulty paying bills, where wraparound services can provide support and resources. Although food insecurity screening and referral is improving in clinical care settings (Bhatia et al., 2025; Taher et al., 2022), more work can be done to create sustainable, consistent protocols of identifying adults with food insecurity and connecting them with food resources that can improve health outcomes.
Strength and limitations
A strength of the current study was the focus on a clinical sample of adults experiencing food insecurity, which has important implications for patient care in clinical settings. Furthermore, the current study helps to fill a gap in the literature by focusing on a clinical sample of patients who were currently experiencing food insecurity, which is more applicable to real-world health care settings in which addressing food access can be an important component of overall patient care. The findings offer insight that supports the development of targeted inventions that not only improve food access but that also address negative mental health outcomes associated with food insecurity. Nonetheless, this study has a few limitations to consider. Because this study focused on cross-sectional associations rather than intervention effects, we did not assess duration of clinic engagement or long-term changes in food insecurity. Short-term food assistance alone does not resolve chronic food insecurity, and future research should evaluate sustained, multi-level strategies (e.g. clinic-based food access programs, SNAP enrollment support, and ongoing referral pathways) that may have greater impact on long-term food insecurity. Second, the sample size was relatively small (N = 104), which may limit generalizability of the findings and the ability to examine alternative explanations (e.g. clinic selection, ceiling effects, weight loss, etc.) of the reported findings. Survey measures were self-reported (anxiety, depression, quality of life), which introduces the possibility of recall bias and social desirability bias. Third, a single-item quality of life measure, such as the PROMIS global health item, has demonstrated validity and acceptability for broad assessments of well-being, however, it does not fully capture the multidimensional complexity of quality of life. As such, our measure may not have been sensitive enough to detect more nuanced associations between food insecurity and specific quality of life domains (e.g. social functioning, fatigue, sleep, or cognitive health). Future research would benefit from multi-item or domain-specific quality of life instruments to more comprehensively evaluate the ways food insecurity affects overall well-being in clinical populations. Fourth, a single blood pressure reading in-clinic does not provide an accurate measure of blood pressure, as variables like white-coat syndrome could impact blood pressure readings (Townsend and Cohen, 2024). Ambulatory blood pressure monitoring (ABPM) devices would have provided a better understanding of participants’ blood pressure, however, utilizing ABPM was not feasible due to limited resources. Finally, the ability to validate participants’ self-reported health information was limited by lack of access to electronic medical records.
Conclusion
This study adds to the growing body of research linking food insecurity with mental health, showing that individuals currently navigating food insecurity in a clinical setting report significantly higher levels of anxiety and depression. These findings are consistent with prior work and build on this evidence by examining these associations in a clinical population that may face compounding medical and social challenges. This contextualizes our results within an established literature while highlighting the need for clinical screening and integrated support services relevant for clinical care. Overall, these findings underscore the importance of integrating food access into routine clinical services. Screening for food insecurity is critical and finding that a patient has difficulty accessing food may warrant additional mental health screenings. Additionally, mental health screening and support services offered within food pantries or community clinics could help identify individuals at risk earlier and facilitate more timely treatment, potentially mitigating the long-term psychological consequences of food insecurity.
Footnotes
Ethical considerations
The University of Alabama Birmingham, Institutional Board IRB-300002344 (approved 4/26/2024) approved all study procedures and materials.
Consent to participate
Written, informed consent to participate was obtained from all participants prior to the beginning of the study.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is sponsored by the UAB Center for the Study of Community Health, a member of the CDC Prevention Research Centers Program, and is supported by the UAB University-Wide Interdisciplinary Research Centers program.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study contain sensitive health information and cannot be publicly shared due to Institutional Review Board (IRB) restrictions and participant confidentiality. De-identified data may be made available upon reasonable request to the corresponding author and pending IRB approval.
Glossary
CVD: cardiovascular disease
HIV: human immunodeficiency virus
BMI: body mass index
ABPM: ambulatory blood pressure monitor
SNAP: supplemental nutrition assistance program