
Abstract
This study examined the relationship between self-transcendence and hopelessness in hospitalized lung cancer patients. Conducted between February and September 2023 in a hospital in western Türkiye, the cross-sectional study included 400 patients. Data were collected using a Patient Identification Form, the Self-Transcendence Scale (STS), and the Beck Hopelessness Scale (BHS). The mean age was 64.79 ± 9.45 years, with 77.0% of participants being male and 71.7% diagnosed at stage IV. Findings revealed a moderate level of STS (mean = 32.75 ± 6.89) and a high level of BHS (mean = 15.56 ± 5.03). A significant negative correlation was observed between self-transcendence and hopelessness (Model 1: β = −0.371, Model 2: β = −0.260), suggesting that as self-transcendence increases, hopelessness decreases. These findings emphasize, in scientific terms, the necessity of integrating structured psychosocial interventions into lung cancer care to enhance psychological resilience and overall patient outcomes. Supporting self-transcendence may help reduce hopelessness, contributing to improved psychological well-being and quality of life.
Introduction
Cancer is the second leading cause of death worldwide after ischemic diseases (World Health Organization [WHO], 2024). Lung cancer is one of the most diagnosed cancers, with 2.2 million new cases (11.4%) and 1.8 million deaths in 2020 (Sung et al., 2021; WHO, 2023). This type of cancer is a very common and aggressive disease worldwide, with a 5-year relative survival rate of only 8%. In contrast, the 5-year survival rate for patients diagnosed with localized lung cancer is at least 60% (Leiter et al., 2023). The high morbidity and mortality rates may indicate that the disease burden of lung cancer is also quite high. In particular, it has been reported that psychological problems–such as hopelessness, defined as a lack of positive expectations about the future–may be prevalent due to the challenging nature of the disease and its treatment (Martins et al., 2024; Uslu-Sahan et al., 2019).
For lung cancer patients, feelings of hopelessness can affect the severity of diagnosis, uncertainty of prognosis, physical symptoms and quality of life, and are associated with negative emotions, outcomes and expectations (Baczewska et al., 2020; Sullivan et al., 2016). There are studies in literature showing that hopelessness can also be an important indicator of depression and self-harm (Baczewska et al., 2020; Brothers and Andersen, 2009; Liu et al., 2020). Hopelessness as an independent determinant can also increase the risk of death. It can also lead to physiologically abnormal platelet function in older people and cause an increase in heart rate variability, immune function and psychological pain (Zhu et al., 2017). However, it has been found that cancer patients with high levels of hope tend to live longer and have longer symptom-free periods (Nehir et al., 2019). A meta-analysis study (2022) examining levels of hopelessness in a wide range of psychotherapeutic interventions reported that understanding hope in cancer patients has the potential to improve physical functioning, psychological state, and quality of life (Luo et al., 2022). In this context, hopelessness is not only associated with psychological and mental health, but also with physical health (Eskelinen et al., 2015; Luo et al., 2022; Yildirim et al., 2009). In terms of psychological and mental health, hopelessness is known to have a significant negative relationship with perceived social support, spirituality and spiritual well-being (Ata and Kılıç, 2022; Tasan and Citlik Saritas, 2022; Uslu-Sahan et al., 2019).
In his theory of psychosocial development, Erik Erikson mentioned the eight stages of personality and described the eighth stage as hopelessness toward the integrity of the self. He also added that individuals who do not complete the integrity of self-experience hopelessness (Aslan and Hocaoğlu, 2017). So, in the self-transcendence theory, which emerged as a middle-range nursing theory, Reed (2023) reported that hope is one of the indicators of well-being, but well-being is a correlation and result of self-transcendence. This concept can provide a way for individuals to find meaning and purpose beyond their suffering, enabling them to transcend feelings of hopelessness, powerlessness and worthlessness (Martins et al., 2024). By embracing self-transcendence, patients can shift their focus from negative emotions to a deeper sense of connection, spirituality and purpose in life. Self-transcendence therefore refers to the process of moving beyond one’s immediate concerns and focusing on the broader aspects of life and existence (Bovero et al., 2023). In addition, for lung cancer patients facing feelings of hopelessness, self-transcendence may be an important concept for coping with the emotional challenges associated with their illness. In this theory, Reed (1991) proposes that self-transcendence—defined as a sense of connectedness with others, within oneself, or with a purpose beyond the self—may facilitate a sense of well-being, particularly during times of difficulty or adversity. In addition, this concept includes psychological and spiritual behaviors such as sharing wisdom with others, integrating the physical changes of aging, accepting death as part of life, helping others, coping with loss and finding spiritual meaning in life (Kublay and Hallaç, 2022). In this context, self-transcendence can positively influence well-being by transforming stressful events into healing experiences, as long as the self is not harmed (Er et al., 2022; Reed, 2021, 2023). So much so that Er et al. (2022) reported a significant positive relationship between levels of self-transcendence and psychological resilience in their studies of oncology patients. Bovero et al. (2023) in terminal cancer patients and Soriano and Calong (2021) in their studies of women with breast cancer found that there was a positive significant relationship between self-transcendence and spirituality. However, no study was found in the literature that examined the relationship between hopelessness and self-transcendence. From a conceptual perspective, self-transcendence and hopelessness may be understood as closely related yet opposing psychosocial processes in the context of life-threatening illness. Hopelessness reflects a loss of future-oriented meaning, diminished expectations, and a sense of powerlessness, whereas self-transcendence involves an expansion of personal boundaries toward meaning, connectedness, and purpose beyond the self. In patients with lung cancer—who frequently face advanced disease, poor prognosis, and intensive treatment—these two constructs may interact dynamically. While severe illness and symptom burden may intensify hopelessness, self-transcendence may serve as a psychological and spiritual resource that helps individuals reframe their illness experience, sustain meaning, and preserve a sense of inner coherence despite adversity. Thus, examining self-transcendence alongside hopelessness is theoretically relevant, as self-transcendence may represent a potential pathway through which patients cope with existential distress and mitigate feelings of hopelessness in the face of serious illness.
In this context, the primary objective of this study is to examine the relationship between self-transcendence and hopelessness in hospitalized lung cancer patients. The secondary objective is to describe the levels of self-transcendence and hopelessness according to patients’ sociodemographic and clinical characteristics. It is believed that the results obtained can fill the gaps in literature.
Research questions
Is there a significant relationship between self-transcendence and hopelessness among patients with lung cancer?
Does the relationship between self-transcendence and hopelessness remain significant after controlling for clinical and health-related variables?
Methods
Design
A cross-sectional study was conducted between February and June 2023.
Population and sampling
The population of the study consisted of patients diagnosed with lung cancer who served as inpatient treatment in the clinics of a chest diseases and surgery hospital in western Türkiye. The number of patients hospitalized for lung cancer for last year was 2305. Accordingly, the number of samples was calculated on www.openepi.com, and it was determined that at least 330 patients were required to make statistical estimates with a 95% confidence interval and ±5% sampling error. To reduce the generalizability of the study and the margin of error, we reached approximately 480 patients, but approximately 20 patients (4.2%) did not accept the study, and 50 patients (10.4%) were excluded due to exclusion criteria. Ten patients (2.1%) gave incomplete answers to the questionnaires. Therefore, finally 400 patients (83.3%) were included in the study. A convenience sampling method was employed, and all data were collected face-to-face through structured questionnaires by a specialist nurse collaborating in the study.
The inclusion criteria were: being 18 years of age or older, having a confirmed diagnosis of lung cancer, being hospitalized due to lung cancer, being able to speak and understand Turkish, and providing voluntary informed consent. The exclusion criteria were: being hospitalized for reasons other than lung cancer despite having a diagnosis of lung cancer, having a physician-diagnosed Alzheimer’s disease, dementia, delirium, or another psychiatric disorder, not being literate in Turkish, not being informed of the cancer diagnosis by relatives, failing to complete all items in the questionnaires, or withdrawing from the study after enrollment.
According to a post hoc power analysis conducted for Model 2 using G*Power 3.1.9.2, with an R2 value of 0.195 (f2 = 0.242), an alpha level of 0.05, six predictors, and a sample size of N = 400, the achieved statistical power was >99%.
Ethical considerations
Ethics committee approval was obtained from the University of Health Sciences Dr. Suat Seren Chest Diseases and Thoracic Surgery Training and Research Hospital Ethics Committee (2023/16–8) for the study to be carried out; institutional permission was obtained from the Provincial Health Directorate of the hospital where the research was conducted; and permission from the authors was obtained to use the scales. The patients were informed about the study with the informed consent form. Those who agreed to participate and met the inclusion criteria were included in the study. No harmful drugs or interventions were applied to the patients. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Data collection procedures
Following the institutional approvals, the data were collected by face-to-face survey method between February 23 and September 30, 2023, by a specialist nurse researcher who explained the purpose and procedures of the study and asked for written consent to participate in the study to individuals with lung cancer who were admitted to the chest diseases clinics of the hospital where the study was conducted and who met the inclusion criteria. Data of the study; Patient Identification Form, Self-Transcendence Scale—Turkish version (STS; Sariçam, 2015), and Beck Hopelessness Scale—Turkish version (BHS; Durak and Palabıyıkoğlu, 1994).
Data collection tools
Patient Identification Form: It was prepared by the researchers in line with the literature (Dogan and Ozcelik, 2022; Er et al., 2022; Nehir et al., 2019). It consisted of a total of 17 questions consisting of 7 questions including sociodemographic characteristics (age, gender, educational status, marital status, etc.) and 10 questions including characteristics related to health and disease (presence of chronic diseases other than lung cancer, perceived health evaluated as very bad, bad, moderate, good and very good, disease year, cancer stage, duration of treatment, treatments received, number of hospitalizations due to cancer in the last year, presence of metastasis, organs developing metastasis).
Self-transcendence Scale: Developed by Reed (1991) the Self-transcendence Scale consists of 15 items and is a four-point Likert-type scale, with responses ranging from 1 (not at all) to 4 (very much). The original scale includes two sub-dimensions: interpersonal and internal mood. However, better overall scores have been demonstrated by Sariçam’s Turkish adaptation of the scale (2015) the Turkish version of the scale was used in our study. The scale ranges from 15 to 60, with higher scores indicating greater levels of self-transcendence. The internal consistency reliability coefficient for the entire scale was found to be 0.87 (Sariçam, 2015). In our study, the Cronbach Alpha coefficient was calculated to be 0.925.
Beck Hopelessness Scale: Developed by Beck et al. (1974), has a Cronbach’s alpha coefficient of 0.93. The Turkish validity and reliability study of the scale was conducted in 1994 (Durak and Palabıyıkoğlu, 1994). The scale consists of 20 true-false statements, each answer that is true according to the individual receives 1 point, each answer that is false according to the individual receives 0 point and the total score varies between 0 and 20 and the increase in the total score indicates that the level of the individual hopelessness increases. Cronbach’s alpha coefficient was found to be 0.85 and the Turkish version of the scale was used in our study (Durak and Palabıyıkoğlu, 1994). In our study, the Cronbach Alpha coefficient was calculated to be 0.905.
Data analysis procedures
The study data were analyzed on SPSS (Statistical Package for Social Sciences) for Windows 23.0 package. The data were tested for normality using skew/kurtosis values and Kolmogorov-Smirnov. Descriptive characteristics of patients, means and standard deviations (SD) or percentages and frequencies were used.
In the study, independent sample t-test and one-way analysis of variance were used to evaluate the differences between variables for normally distributed data; Kruskal Wallis H test was used for three or more groups that did not comply with normality distribution. Tukey’s b or Dunn’s test was used for post-hoc analyses. Pearson correlation analysis was used to evaluate the relationship between continuous variables. Linear regression analysis was used to assess significant associations. Adjust R2 was used to compare the explanatory power of each linear regression model. All tests were considered significant at a level of p < 0.05, and a 95% confidence interval (95% CI) was used to assess the independent contribution of important factors.
Results
Socio-demographic characteristics
The mean age of the lung cancer patients participating in the study was 64.79 (SD 7) and 57% being 65 years or older. Of the patients, 77% were male, 80.8% had a maximum of 8 years of education, 78% were married, 89% had children, and 78% lived with their spouses and/or children (Table 1).
Socio-demographic characteristics of the patients.
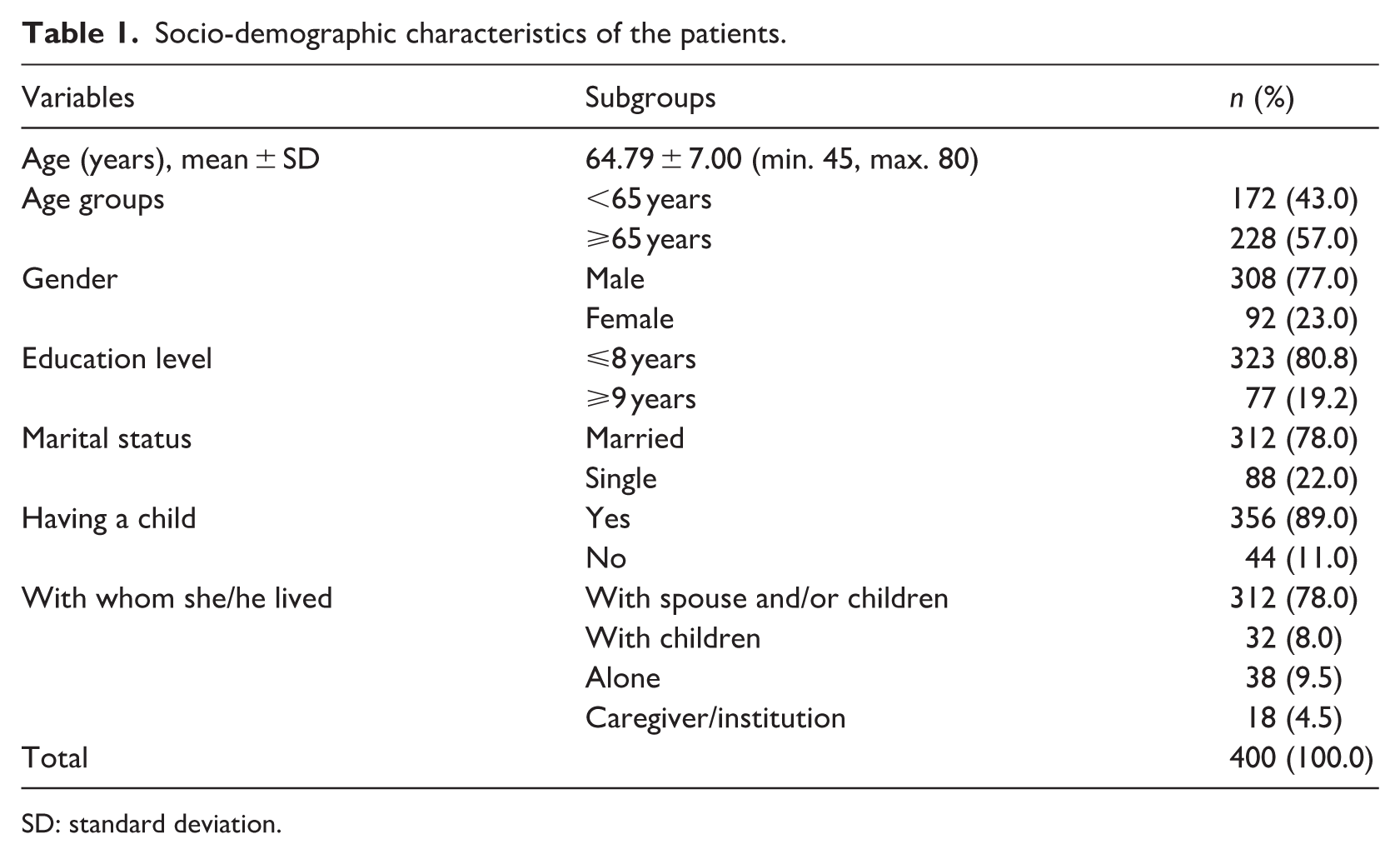
SD: standard deviation.
Descriptive characteristics of patients for the disease
The majority of patients (71.7%) were diagnosed with stage IV lung cancer. The mean duration since diagnosis was 2.32 years (SD 1.19), and 67.6% of the patients had been diagnosed within the past 2 years. The mean duration since treatment initiation was 2.12 years (SD 1.13), with 70.5% of patients having started treatment within the last 2 years. Most patients received chemotherapy (93.9%), followed by radiotherapy (33.8%). Metastasis was present in 72.5% of the patients, with the most common metastatic sites being the brain (46.5%) and bone (46.0%). Among the participants, 89.3% reported having at least one non-cancerous chronic disease. The most frequently reported comorbid conditions were hypertension (45.0%) and diabetes mellitus (44.3%). The number of cancer-related hospitalizations within the past year ranged from one to eight, with a mean of 2.86 (SD 1.37). More than half of the patients (58.5%) experienced three or more hospitalizations during the past year. Patients’ health perceptions ranged from very bad to good, with 50.5% perceiving their health as bad; no patient reported perceiving their health as very good.
The mean Self-Transcendence Scale (STS; Reed, 1991) score was 32.75 (SD 8.84), while the mean Beck Hopelessness Scale (BHS; Beck et al., 1974) score was 15.56 (SD 4.63). According to BHS classification, 77.8% of the patients exhibited severe levels of hopelessness (Table 2).
Disease-related characteristics of patients for the disease.
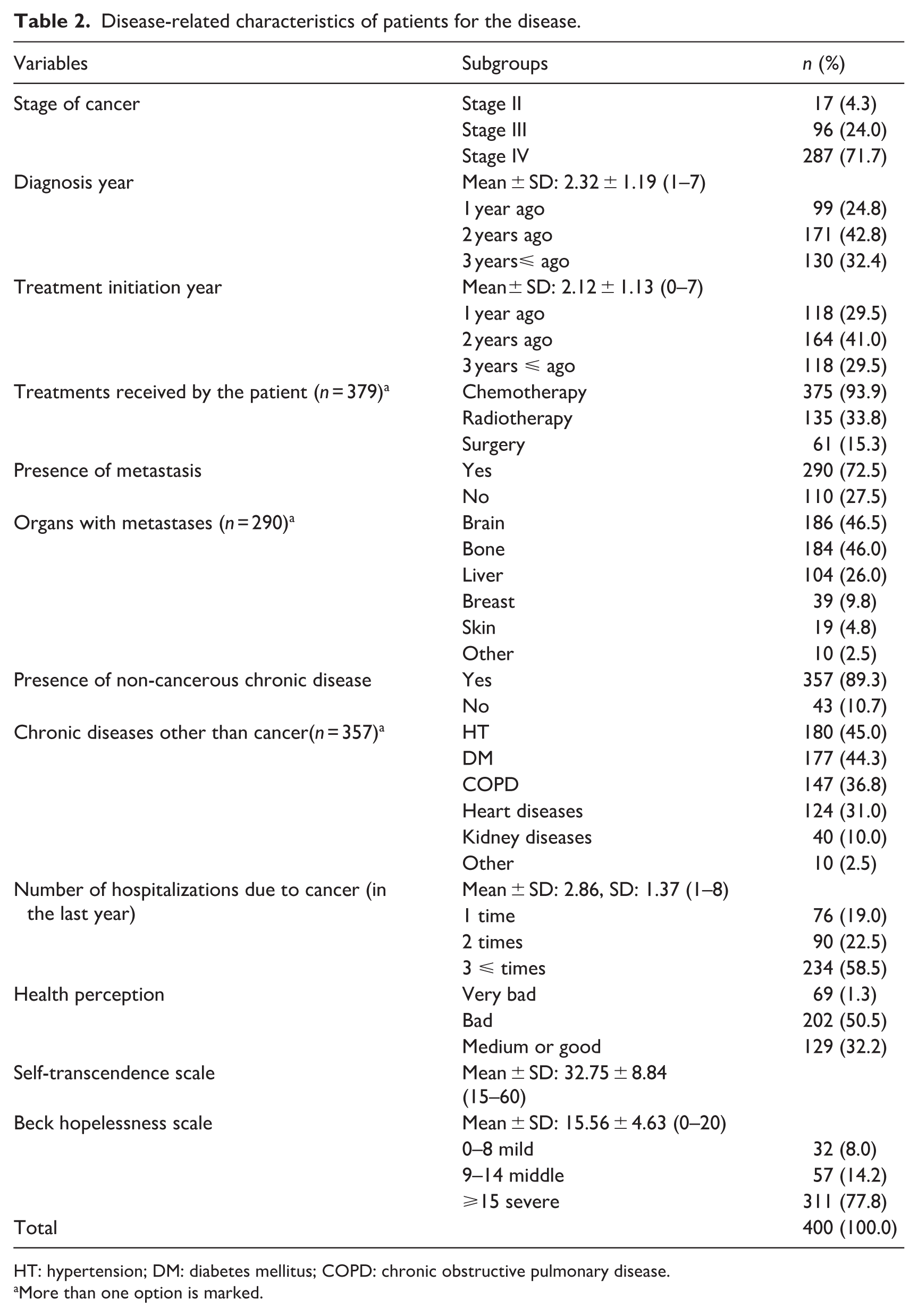
HT: hypertension; DM: diabetes mellitus; COPD: chronic obstructive pulmonary disease.
More than one option is marked.
Patient characteristics according to self-transcendence and hopelessness levels
The mean scores of the STS and BHS were compared according to participants’ sociodemographic and clinical characteristics. The results of the analyses indicated that there were no statistically significant differences in STS and BHS mean scores according to sociodemographic characteristics, including age group, gender, educational status, marital status, having children, and living arrangement (p > 0.05; Table 3).
Patient characteristics according to self-transcendence and hopelessness levels.
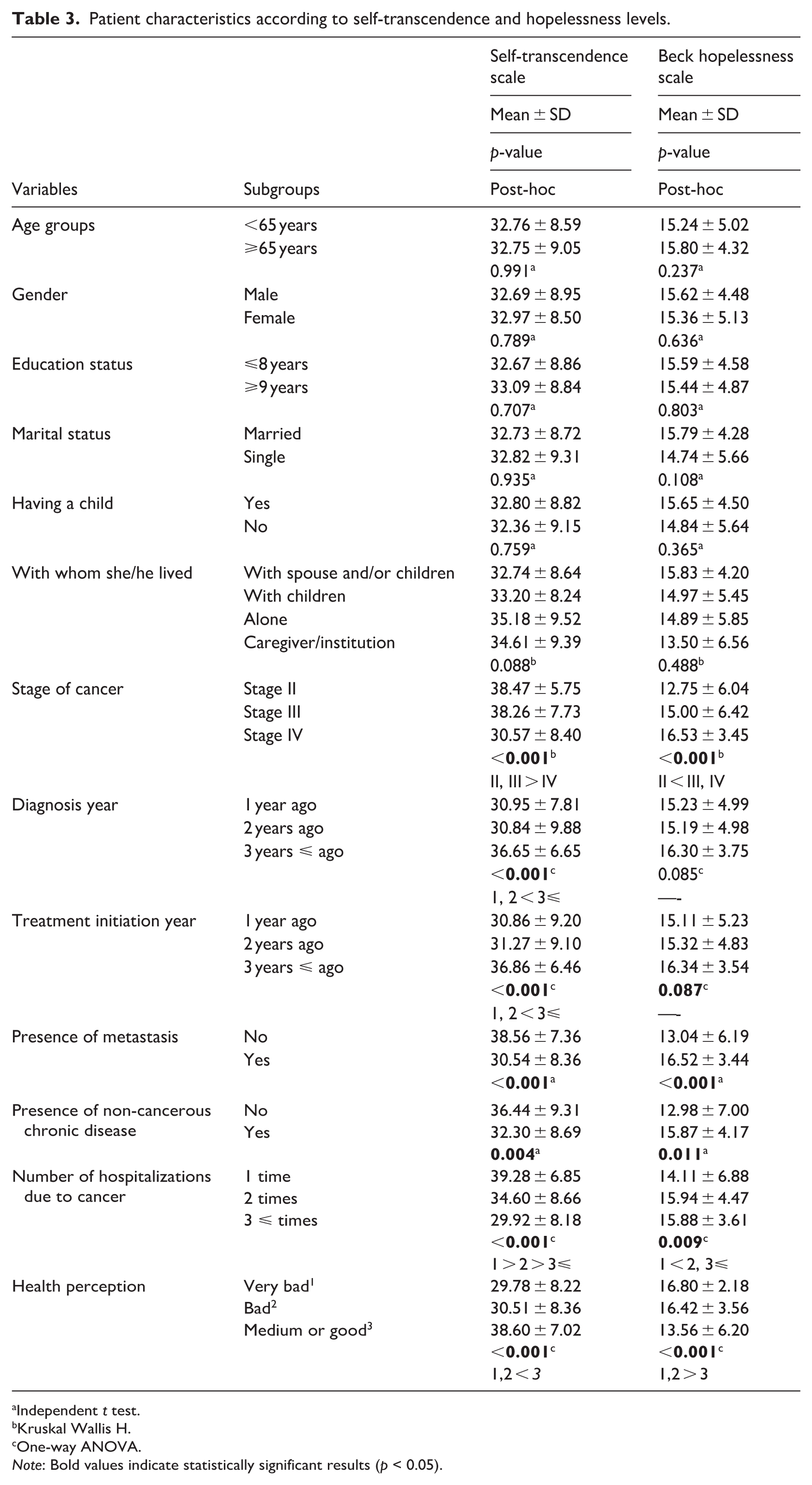
Independent t test.
Kruskal Wallis H.
One-way ANOVA.
Note: Bold values indicate statistically significant results (p < 0.05).
When comparisons were made according to cancer stage, individuals in Stage II and Stage III had significantly higher self-transcendence levels than those in Stage IV (p < 0.001). Regarding hopelessness, the mean BHS score of individuals in Stage II was found to be significantly lower than those in Stage III and Stage IV (p < 0.001). When evaluated according to time since diagnosis, individuals who had been diagnosed for 3 years or longer had significantly higher mean self-transcendence scores compared with those diagnosed for 1 or 2 years (p < 0.001). However, no statistically significant difference was observed in hopelessness levels according to time since diagnosis (p > 0.05). Similarly, analyses based on time since treatment initiation showed that individuals whose treatment duration was 3 years or longer had significantly higher self-transcendence scores than those with a treatment duration of 1 or 2 years (p < 0.001). In contrast, hopelessness levels did not differ significantly according to treatment duration (p > 0.05). In comparisons based on the presence of metastasis, individuals without metastasis had significantly higher self-transcendence scores and significantly lower hopelessness scores compared with those with metastasis (p < 0.001). Furthermore, individuals without non-cancerous chronic diseases demonstrated significantly higher self-transcendence levels than those with chronic diseases (p = 0.004), whereas hopelessness levels were significantly higher among individuals with non-cancerous chronic diseases (p = 0.011). When comparisons were made according to the number of cancer-related hospitalizations, mean self-transcendence scores were found to decrease significantly as the number of hospitalizations increased (p < 0.001). In contrast, hopelessness levels were significantly higher among individuals with two or three or more hospitalizations compared with those who had been hospitalized once (p = 0.009). In analyses based on health perception, individuals who perceived their health as “medium or good” had significantly higher mean self-transcendence scores than those who perceived their health as “bad” or “very bad” (p < 0.001). Conversely, mean hopelessness scores were significantly lower among individuals with a “medium or good” health perception compared with those reporting “bad” or “very bad” health perception (p < 0.001; Table 3).
Linear regression analysis of factors associated with hopelessness
According to linear regression analysis, the relationship between self-transcendence and hopelessness was found to be significant (β = −0.371, p < 0.001). This result shows that lung cancer patients’ hopelessness scores explain approximately 13.6% of the total variance in self-transcendence scores (Adjusted R2 = 0.136, p < 0.001). Each unit increase in self-transcendence was associated with a 0.195 unit decrease in hopelessness (B = −0.195, p < 0.001; Table 4).
Linear regression analysis of factors associated with hopelessness.
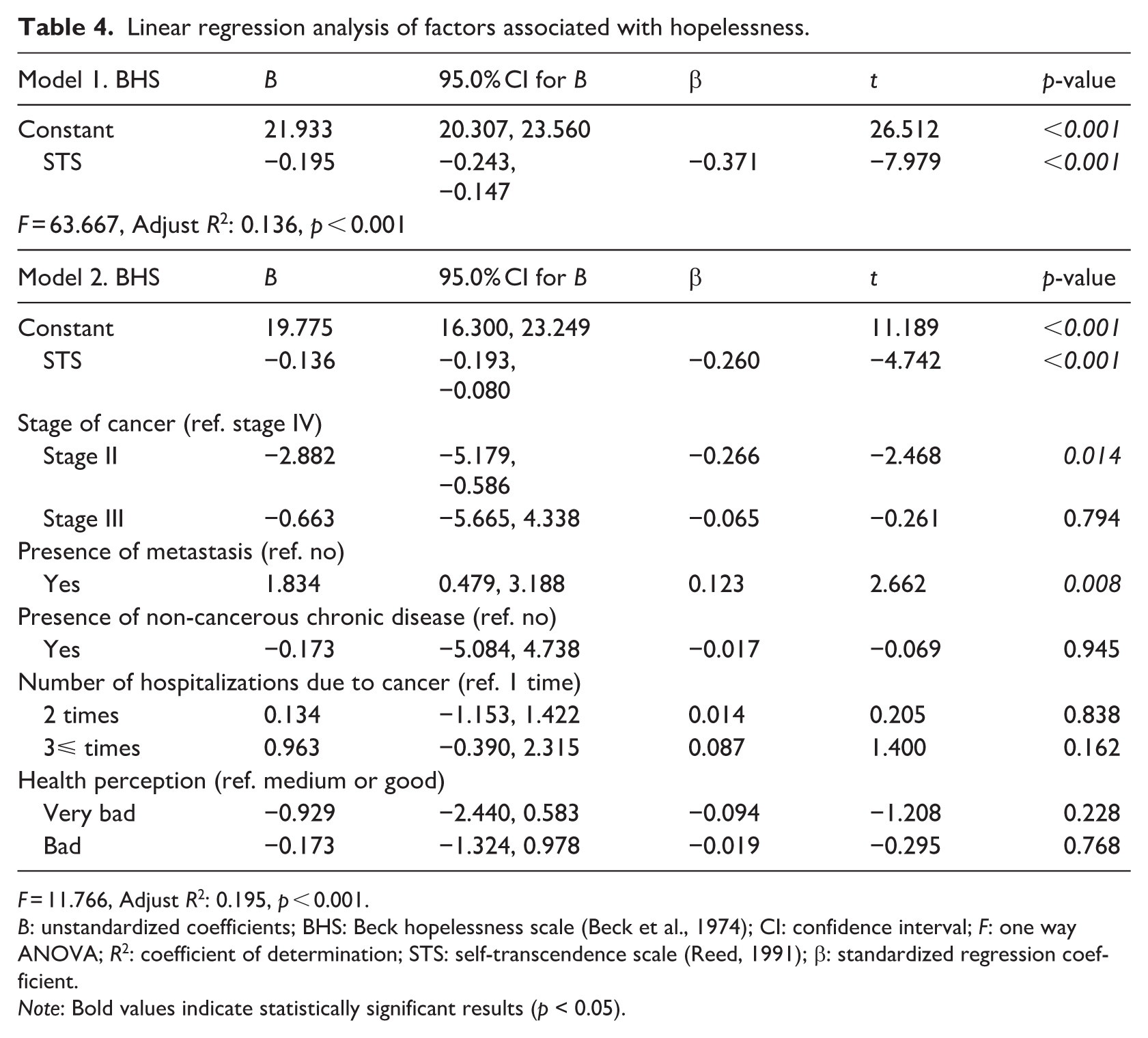
F = 11.766, Adjust R2: 0.195, p < 0.001.
B: unstandardized coefficients; BHS: Beck hopelessness scale (Beck et al., 1974); CI: confidence interval; F: one way ANOVA; R2: coefficient of determination; STS: self-transcendence scale (Reed, 1991); β: standardized regression coefficient.
Note: Bold values indicate statistically significant results (p < 0.05).
According to the multiple linear regression analysis, the relationship between self-transcendence (STS) and hopelessness remained statistically significant after controlling clinical and health-related variables (β = −0.260, p < 0.001). Model 2 was statistically significant (F = 11.766, p < 0.001) and explained 19.5% of the total variance in hopelessness scores (Adjusted R2 = 0.195). In this model, each 1 unit increase in self-transcendence was associated with a 0.136 unit decrease in BHS scores (B = −0.136, p < 0.001). When cancer stage was examined with Stage IV as the reference category, individuals in Stage II had significantly lower levels of hopelessness (B = −2.882, p = 0.014), whereas no significant difference in hopelessness was observed between Stage III and Stage IV (p = 0.794). In addition, the presence of metastasis was found to be significantly associated with higher levels of hopelessness (B = 1.834, p = 0.008). The presence of non-cancerous chronic disease, number of cancer-related hospitalizations, and health perception were not significantly associated with hopelessness (p > 0.05; Table 4).
Discussion
This study may be the first to examine the relationship between self-transcendence and hopelessness in 400 hospitalized lung cancer patients; no similar research has been found in the literature. The average age of the hospitalized lung cancer patients who participated in our study was 64.79 years, and more than half of the participants were 65 years or older. This age group in our study confirms that the risk group for lung cancer is the 55–80 age group (Toumazis et al., 2020). The fact that two-thirds of the patients in the study were male is consistent with the literature showing that lung cancer is more common in men. In fact, the reasons why lung cancer is more common in men include the fact that smoking is more common in men and that men are more exposed to the environment by working in industrial jobs (Olsson and Kromhout, 2021). In addition, the fact that these people have limited access to health services and early diagnosis may also increase risk factors. Indeed, a cohort study (2021) of patients with small cell lung cancer reported that factors associated with better survival were female gender, higher education, higher income and health insurance (Zhou et al., 2021). The fact that the rates of being married and having children were also quite high in our study is to be expected and is in line with the overall population of the country. This is thought to be particularly important in terms of the social support needs of oncology patients. Indeed, it has been reported in the literature that the effect of partner social support may be physiologically mediated through neuroendocrine, neural and immune interactions directly related to cancer. In addition, it has been argued that the hormone oxytocin, which is released during social interactions with family, may indirectly inhibit cancer cell growth by inhibiting the stress response (Krajc et al., 2023). Thus, lack of family support may have a negative impact on the psychological and physical health of patients.
When the characteristics of the patients were examined, the majority of them had stage IV disease and the year of diagnosis was 2 years or less. There was also a higher proportion of patients who started treatment in the last 2 years. These results may show that lung cancer is a cancer that is diagnosed late. The vast majority of patients had metastatic disease. The most common sites of metastases were vital organs such as the brain and bones, while the most common comorbidities were hypertension and diabetes. Complications and treatment of diseases that affect cardiovascular and endocrine health, such as hypertension and diabetes, can worsen cancer prognosis. Conditions such as metastases and comorbidities in lung cancer patients can increase the number of hospitalizations. In fact, in our study, one in three patients was hospitalized four or more times per year. These rates in our study may indicate the disease burden and poor prognosis of lung cancer and explain why lung cancer has high morbidity and mortality rates among cancers. So much so that the difficulty of the disease burden can be demonstrated by the level of patients’ perception of their health, as in our study. While the majority of patients perceive their health as “bad” or “very bad,” very few patients perceive it as “good.” In addition, the absence of patients who perceive their health as “very good” may also indicate the burden of disease and the challenging nature of lung cancer. On the other hand, the average self-transcendence score of lung cancer patients in our study was moderate at 32.75.
Self-transcendence is a psychological concept that indicates an individual’s ability to transcend themselves and can help them find a broader meaning to their current situation and cope with the difficulties they are experiencing (Reed, 2021). In the literature, Yang et al. (2024) reported a mean Self-Transcendence Scale (STS) score of 44.73 in a study including 243 patients with lung cancer, while He et al. (2025) found a mean STS score of approximately 39.14 among 477 lung cancer patients. In a study conducted by Er et al. (2022), the mean self-transcendence score was 45.68 in a mixed cancer patient population, of whom 10.5% had lung cancer, with breast cancer constituting the majority of diagnoses. Similarly, Chen et al. (2020) reported mean STS scores of 42.89 and 44.72 in cancer patients receiving chemotherapy, 21.43% of whom had lung cancer. In addition, He et al. (2022) found a mean self-transcendence score of 45.88 among patients with breast cancer. In contrast, Bozkurt et al. (2025) reported a lower mean STS score (36.95 ± 4.57) among patients with COPD. Given that lung cancer is associated with high mortality and substantial disease burden, patients may experience heightened existential distress. As noted in Reed’s theory (Reed, 2021), although self-transcendence can emerge in the context of vulnerability, its development may be constrained under conditions of overwhelming physical and psychological stress.
Hopelessness, on the other hand, can be defined as an emotional state in which expectations about the future are negative, a sense of hope is lost, and individuals feel helpless in the face of the situations they experience. In this context, the mean hopelessness score of the patients in our study was quite high at 15.56. So high, in fact, that two-thirds of the patients in the study were found to have high levels of hopelessness. When the literature is examined, the mean hopelessness score is; 7.41 for 130 patients with advanced lung cancer who received chemotherapy in thoracic surgery, intensive care and oncology services (Dogan and Ozcelik, 2022); It was reported as 6. Five in a study of 650 oncology patients (Tasan and Citlik Saritas, 2022); 4.15 in a study of 210 patients hospitalized in oncology clinics (Ata and Kılıç, 2022); and 11.63 in 125 oncology patients (Atan et al., 2020). In this context, factors such as the fact that more than half of the lung cancer patients in our study were aged 65 years or older, most of them were diagnosed at an advanced stage, most of them had metastases, about half of them had brain metastases, and almost all of them received chemotherapy, may have caused patients to experience a lot of negative emotions and decreased hope.
When self-transcendence scores were compared according to the sociodemographic characteristics of patients with lung cancer in the present study, no statistically significant differences were observed. This finding suggests that self-transcendence may be relatively independent of basic sociodemographic factors in this population. Consistent with our results, Yang et al. (2024) similarly reported no significant differences in self-transcendence levels according to age, gender, or marital status among patients with lung cancer; however, they noted that individuals with higher educational attainment demonstrated significantly higher self-transcendence levels. The absence of such an association in our study may be related to the overall clinical characteristics of the sample, which largely consisted of patients with advanced-stage disease and a high illness burden, potentially diminishing the influence of sociodemographic factors on self-transcendence. Similarly, when sociodemographic characteristics were examined in relation to hopelessness scores, no significant differences were identified in the present study. In contrast, Dogan and Ozcelik (2022) reported significant differences in hopelessness scores according to age, gender, and educational level, while Tasan and Citlik Saritas (2022) found that age and marital status were significant determinants of hopelessness. The discrepancy between these findings and our results may be explained by the psychological profile of our sample. A substantial proportion of patients in the present study exhibited severe levels of hopelessness, and the sample predominantly comprised individuals with advanced lung cancer and a high disease burden. Under such conditions, the pervasive impact of the illness itself may overshadow the role of sociodemographic characteristics, rendering their influence on hopelessness less pronounced.
When self-transcendence scores were compared according to disease-related characteristics, patients with stage IV lung cancer, those diagnosed and initiated treatment within the first 2 years, individuals with metastasis and non-cancerous chronic diseases, those with a higher number of cancer-related hospitalizations in the past year, and patients who perceived their health as “bad” or “very bad” demonstrated significantly lower levels of self-transcendence. Given that a substantial proportion of the study sample consisted of patients with these characteristics, this distribution may partially account for the relatively low overall mean self-transcendence score observed in the present study. These findings suggest that a high disease burden and poorer perceived health status may constrain individuals’ capacity to engage in self-transcendence.
With respect to hopelessness, significant differences were observed according to cancer stage, presence of metastasis, presence of non-cancerous chronic diseases, number of hospitalizations, and health perception. In line with our findings, patients in Stage III and Stage IV exhibited higher levels of hopelessness compared with those in Stage II; however, the relatively small proportion of Stage II patients in the sample should be taken into consideration when interpreting these results. Contrary to some previous studies, no statistically significant differences in hopelessness were found according to duration since diagnosis or treatment initiation in the present study. This suggests that, rather than the length of time since diagnosis, the current clinical condition and perceived disease burden may play a more decisive role in shaping hopelessness levels among patients with lung cancer. Consistent with this interpretation, patients with metastasis and those with non-cancerous chronic diseases demonstrated significantly higher hopelessness levels. The presence of metastases in vital organs such as the brain and bones, along with common comorbid conditions including hypertension, diabetes, and chronic respiratory diseases, may intensify physical symptoms and functional limitations, thereby exacerbating psychological distress. Previous research has similarly shown that disease stage, metastatic status, and symptom burden are closely associated with hopelessness in patients with lung cancer (Dogan and Ozcelik, 2022). Furthermore, in the present study, hopelessness levels were significantly higher among patients who perceived their health as “bad” or “very bad” compared with those reporting a “moderate” or “good” health perception. This finding aligns with evidence suggesting that poorer health perception reflects diminished quality of life and greater psychological vulnerability. Supporting this view, Aydın Sayılan and Demir Doğan (2020) reported that improvements in quality of life, physical well-being, and social well-being were associated with more positive illness perceptions among patients with cancer.
When the primary aim of the study was considered, a significant negative relationship was identified between self-transcendence and hopelessness. In the initial regression model, self-transcendence alone explained 13.6% of the variance in hopelessness, and each 1 unit increase in self-transcendence was associated with a 0.195 unit decrease in hopelessness. This finding indicates that self-transcendence constitutes a meaningful psychological resource in mitigating hopelessness among patients with lung cancer. Importantly, when clinical and health-related variables were included in the model, the association between self-transcendence and hopelessness remained statistically significant, although its magnitude was attenuated. In the fully adjusted model, self-transcendence continued to independently predict lower hopelessness levels, and the model explained 19.5% of the total variance in hopelessness scores. In this context, each 1 unit increase in self-transcendence was associated with a 0.136 unit reduction in hopelessness. These findings suggest that while self-transcendence exerts a direct protective effect against hopelessness, this relationship is also shaped by the broader clinical context of the disease.
Among the clinical variables included in the model, cancer stage and presence of metastasis emerged as significant predictors of hopelessness. Patients in Stage II exhibited significantly lower levels of hopelessness compared with those in Stage IV, whereas no significant difference was observed between Stage III and Stage IV. In addition, the presence of metastasis was associated with higher hopelessness levels. In contrast, non-cancerous chronic disease, number of hospitalizations, and health perception did not remain significant predictors in the fully adjusted model. Taken together, these results highlight that self-transcendence retains its protective role even after controlling for indicators of disease severity, underscoring its potential relevance as a target for psychosocial and nursing interventions aimed at reducing hopelessness in patients with lung cancer.
The findings of the present study are consistent with previous research emphasizing the role of self-transcendence and related psychosocial resources in psychological adjustment to serious illness (Uğuz et al., 2025). For example, Er et al. (2022) reported that self-transcendence explained 43.59% of the variance in resilience, with each 1 unit increase in self-transcendence leading to a 1.293 unit increase in resilience. Similarly, He et al. (2025) demonstrated that self-transcendence partially mediates the relationship between illness perception and demoralization in patients with lung cancer, suggesting that higher self-transcendence may buffer the negative psychological effects of maladaptive illness perceptions. In addition, studies examining related constructs have reported comparable findings. Tasan and Citlik Saritas (2022) found a significant negative association between spirituality and hopelessness, with spirituality explaining 50.3% of the variance in hopelessness, while Ata and Kılıç (2022) reported that mental well-being explained 32.3% of hopelessness. Moreover, Uslu-Sahan et al. (2019) showed that perceived social support accounted for 35% of the variance in hopelessness among gynecological cancer patients. Although some studies have reported nonsignificant associations between spirituality-related constructs and hopelessness (Atan et al., 2020), differences in sample characteristics, disease stage, and measurement approaches may explain these inconsistencies. Overall, the present findings align with the broader literature indicating that inner psychological resources play a substantial role in mitigating hopelessness in oncology populations.
Consistent with this interpretation, Yang et al. (2024) reported that self-transcendence levels in patients with lung cancer were influenced by both social support and hope, and that each 1 unit increase in hope was associated with an approximately 1.06 unit increase in self-transcendence. Similarly, emerging evidence suggests that self-transcendence is not only directly influenced by psychological factors but also shaped through complex mechanisms involving hope and coping processes. For example, Wang et al. (2025) demonstrated that hope and coping styles exert both independent and chain-mediating effects on self-transcendence among gastric cancer patients undergoing chemotherapy, highlighting the dynamic interplay between cognitive, emotional, and behavioral factors. Taken together, these findings support the clinical importance of assessing self-transcendence alongside hopelessness in patients with lung cancer. From a clinical perspective, healthcare providers—particularly nurses—may consider routinely evaluating these constructs and integrating complementary and supportive interventions aimed at enhancing meaning, connectedness, and inner resources into the care process. For example, Bozkurt and Yildirim (2024) demonstrated that reminiscence therapy applied to palliative care patients reduced psychological symptoms and increased life satisfaction and self-transcendence. Such interventions may contribute to improved treatment adherence, quality of life, and emotional well-being among oncology patients. Nevertheless, further studies conducted in different cancer populations, including non-hospitalized patients with lung cancer, are recommended to confirm and generalize the present findings.
Strengths and limitations
One of the strengths of this study is that it included 400 lung cancer patients, with a >99% sample size, enhancing the generalizability of the results. Additionally, the study may have provided a detailed profile of the lung cancer population in Türkiye. This comprehensive data collection allows for a robust analysis of factors affecting patient well-being. The focus on self-transcendence and hopelessness addresses an important gap in literature. Given the high prevalence and severe impact of lung cancer, understanding these psychological aspects is crucial for improving patient care. Moreover, the study used established and valid scales, such as the Beck Hopelessness Scale (Beck et al., 1974) and the Self-Transcendence Scale (Reed, 1991), ensuring the reliability and validity of the measures. The analysis was compared with existing literature, highlighting similarities and differences with international trends.
However, the study has limitations. The primary limitation is the cross-sectional design, which limits the ability to make causal inferences. Longitudinal studies are necessary to establish causality between hopelessness, self-transcendence, and other variables. Although comprehensive, the study was conducted at a single center, which may limit the generalizability of the findings to other regions or settings within or outside Türkiye. Furthermore, the study primarily focused on quantitative data, which may not capture the full depth and complexity of patients’ experiences with hopelessness and self-transcendence. Including qualitative interviews could provide deeper insights. Lastly, while the study controlled various variables, factors like socioeconomic status and access to healthcare were not fully explored. Future research should consider these aspects to provide a more comprehensive understanding.
Conclusions
Lung cancer patients had moderate levels of self-transcendence and high levels of hopelessness. A significant negative relationship was found between self-transcendence and hopelessness, and self-transcendence alone accounted for a significant proportion of the variance in hopelessness. These findings suggest that healthcare providers, especially nurses, should emphasize complementary and supportive care, including psychosocial support, to increase self-transcendence and reduce hopelessness in lung cancer patients. Given the aggressive nature of lung cancer and its impact on life expectancy, providing supportive care from the time of diagnosis may help to reduce negative emotions, improve adherence to treatment and ultimately improve patients’ quality of life and survival.
Footnotes
Ethical considerations
Ethics committee approval was obtained from the University of Health Sciences Dr. Suat Seren Chest Diseases and Thoracic Surgery Training and Research Hospital Ethics Committee (2023/16–8) for the study to be carried out; institutional permission was obtained from the Provincial Health Directorate of the hospital where the research was conducted; and permission from the authors was obtained to use the scales. The patients were informed about the study with the informed consent form. Those who agreed to participate and met the inclusion criteria were included in the study. No harmful drugs or interventions were applied to the patients. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent to participate
After obtaining verbal consent from the patients participating in the study, a written informed consent form was signed.
Consent for publication
Written informed consent was obtained from all participants or their legally authorized representatives for the publication of anonymized data. No identifying information is included in this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.*