
Abstract
This study examined the predictive effects of social support and sleep quality on postpartum depression among parents. This longitudinal study included 748 participants (374 mothers and 374 fathers) assessed at the first, third, and sixth months postpartum. The study was conducted in Family Health Centers in a central Anatolian city in Türkiye. Data were collected through face-to-face interviews using the Multidimensional Scale of Perceived Social Support, Pittsburgh Sleep Quality Index, and Edinburgh Postnatal Depression Scale. Mothers had higher depression scores, poorer sleep quality, and lower perceived social support than fathers at all time points. In mothers, both social support and sleep quality were negatively associated with depression, whereas in fathers, social support showed a stronger and sleep quality a weaker association. Regression analyses indicated that social support was a stronger predictor of postpartum depression than sleep quality for both parents.
Introduction
Postpartum depression (PPD) is one of the most common mental disorders affecting individuals during the first year after childbirth (Erdoğan and Hocaoğlu, 2020; Uriko et al., 2025). Globally, the prevalence of PPD among women ranges between 6.5% and 20% (Liu et al., 2022; Sharma et al., 2024). In countries where the prevalence exceeds 10%, more than 500,000 women are diagnosed with PPD each year (Tebeka et al., 2021). Although awareness of PPD in mothers has increased in recent years, paternal PPD remains a relatively new and insufficiently recognized condition. This shows that screening and diagnostic practices targeting fathers are still underdeveloped (Demirci and İnan, 2023; Scarff, 2019; Shaheen et al., 2019). However, most existing studies have focused on identifying individual risk factors rather than exploring how paternal depression interacts with maternal mental health or family functioning. A study of men in 27 European countries reported a prevalence of current depressive disorder of 4.9% (Arias de la Torre et al., 2021). Similarly, a meta-analysis by Rao et al. (2020) found a prevalence of 9.8% during pregnancy and 8.8% within 1 year postpartum. A systematic review of studies between 1990 and 2019 showed that paternal PPD ranged from 1.2% to 25.5% (Wang et al., 2021). These findings indicate that paternal PPD is a cross-cultural phenomenon, suggesting that fathers in different sociocultural contexts share similar psychological determinants.
The etiology of PPD is multifactorial, involving biological, psychological, and social determinants. Hormonal changes, shifts in parental identity and roles, fatigue, poor sleep, and low social support are the most frequently reported risk factors (Erdoğan and Hocaoğlu, 2020; Liu et al., 2022; Wedajo et al., 2023). Among these, sleep quality and social support are especially important because they are modifiable and preventable. Poor sleep is often seen as an inevitable part of parenthood but is one of the strongest predictors of PPD (Baattaiah et al., 2023; Parsons et al., 2023; Wedajo et al., 2023). Parsons et al. (2023) reported that parents experience major sleep disruptions when transitioning from pregnancy to the postpartum period, which may impair mental well-being. Kalogeropoulos et al. (2021) found that perceived poor sleep quality was significantly associated with depressive symptoms in fathers, and Kitil et al. (2024) identified infant sleep problems as an important etiological factor in paternal PPD. In mother-focused research, Baattaiah et al. (2023) showed that fatigue and poor sleep quality were linked to depressive symptoms, while McEvoy et al. (2019) demonstrated that poor postpartum sleep predicted later depression.
Along with sleep, perceived social support is another key determinant of parental mental health in the postpartum period. Adequate support helps parents cope with stress and prevents depression, whereas lack of support may intensify depressive symptoms through loneliness and reduced self-efficacy (Zheng et al., 2023). Several studies have shown that social support is negatively correlated with PPD in both mothers and fathers (Garthus-Niegel et al., 2020; Zheng et al., 2023). Motherhood and fatherhood are complementary but interdependent processes. Recent studies show that paternal depression can trigger or worsen maternal depressive symptoms (Uriko et al., 2025), while maternal depression can increase the likelihood of paternal depressive symptoms by two to three times (Balcı Yapalak et al., 2025; Chhabra et al., 2022). This bidirectional relationship affects not only the mental health of parents but also infant development and family dynamics (Gök et al., 2022; Liu et al., 2022; Lutz et al., 2023; Valdes et al., 2023). Therefore, PPD should be viewed not only as an individual disorder but as a family-level mental health concern.
Previous research has generally examined mothers and fathers separately, overlooking interparental influences and the source-specific nature of social support (e.g. from partners, family, or friends). Most studies on PPD and sleep quality have focused only on mothers (Baattaiah et al., 2023; McEvoy et al., 2019; Rudzik et al., 2023) or only on fathers (Kalogeropoulos et al., 2021). Research involving both parents has typically examined PPD in relation to either social support (Zheng et al., 2023) or sleep quality (Parsons et al., 2023). However, no comprehensive study in the literature has simultaneously examined social support and sleep quality among both mothers and fathers. Although existing studies have identified significant associations between these variables, they have not adequately explained how these psychosocial factors interact over time or differ by gender. Moreover, research addressing the source-specific effects of social support (e.g. from partner, family, or friends) or longitudinal changes in sleep quality for both parents remains limited (White et al., 2023). Evaluating mothers and fathers together will contribute to a better understanding of the reciprocal psychosocial dynamics between parents and to the development of family-centered mental health approaches. Therefore, this study aims to holistically assess parental mental health by simultaneously examining social support and sleep quality, the two key psychosocial determinants of postpartum depression. The findings are expected to make a significant contribution to early risk screening, diagnostic practices, and the development of family-based intervention programs that include both parents.
Methods
Design
A longitudinal study design was employed.
Sample size
The study was conducted in Family Health Centers (FHC) in a central Anatolian city. The sample size was calculated using a formula for unknown populations (p = 0.50, q = 0.50, t = 1.96; α = 0.05), with a minimum of 384 individuals required. The study was completed with 748 participants, including 374 mothers and 374 fathers.
Inclusion criteria
Participants were included in the study if they met the following criteria: being first-time parents, having no history of high-risk pregnancy, having a full-term and healthy singleton birth, an infant birth weight between 2500 and 4000 grams, absence of any physiological or psychological problems during the postpartum period, ability to communicate verbally and in writing, and voluntary participation in the study.
Exclusion criteria
Participants were excluded from the study if they had a diagnosis of depression during pregnancy or the postpartum period, if the infant had a health problem requiring prolonged hospitalization after birth, or if the data forms were incomplete or the participant withdrew from the study during the follow-up period.
All 748 participants completed the assessments at all 3 follow-up points; therefore, no attrition occurred during the study.
Data collection tools
Personal information form
This form, prepared by the researchers, includes sociodemographic characteristics of the parents and obstetric information related to the mothers. It consists of a total of 10 questions.
Multidimensional scale of perceived social support (MSPSS)
The Turkish adaptation of this scale was conducted by Eker et al. (2001). The instrument assesses the level of perceived social support and is scored on a seven-point Likert scale. The scale comprises 3 subdimensions and a total of 12 items. Scores range from 12 to 84, with higher scores indicating greater perceived social support. The Cronbach’s alpha coefficient for the scale ranges between 0.80 and 0.95, and in this study, it was found to be 0.89.
Pittsburgh sleep quality index (PSQI)
The Turkish validity and reliability of this scale were established by Ağargün et al. (1996). It evaluates individuals’ sleep quality over the past month. Out of a total of 24 questions, 19 are self-reported, and only these items are included in the scoring. The scale consists of seven components, each scored between 0 and 3. Total scores range from 0 to 21, with higher scores indicating poorer sleep quality. The Cronbach’s alpha reliability coefficient of the scale is 0.800. In this study, the Cronbach’s alpha coefficient for the scale was 0.910.
Edinburgh postnatal depression scale (EPDS)
The Turkish validity and reliability of this scale were established by Engindeniz et al. (1997). The scale is a four-point likert-type instrument consisting of 10 items. Scores range from 0 to 30. Individuals scoring 13 or above are considered at risk for postpartum depression. In this study, the Cronbach’s alpha coefficient for the scale was calculated as 0.88.
Implementation of the study
The initial interviews with parents were conducted during their first postpartum month when they visited the Family Health Center (FHC) for any reason. Eligible parents who met the inclusion criteria were administered the Personal Information Form, MSPSS, PSQI and EPDS in separate settings to minimize bias. During the first interview, contact information was collected from the participants, who were then invited to the Family Health Center for follow-up assessments at the third and sixth months postpartum. All data collection procedures were conducted face-to-face at the FHC, and during each follow-up visit, the MSPSS, PSQI, and EPDS were re-administered to complete the longitudinal data collection process.
Data analysis
The collected data were analyzed using SPSS for Windows 22.0. The normality of the data distribution was assessed using Skewness and Kurtosis values. Descriptive statistics, including frequency, percentage, mean, and standard deviation, were calculated. For inferential analysis, independent samples t-test, Spearman correlation analysis, and regression analysis were performed. A p-value <0.05 was considered statistically significant for all analyses.
Results
Table 1 presents the demographic characteristics of the study participants. The mean age of mothers was 29.41 ± 4.19 years. Of the mothers, 55.3% were high school graduates, 27.2% were employed in stable income-generating jobs, 75.9% reported moderate economic status, 97.3% had planned pregnancies, 64.8% delivered vaginally, and 50.6% had female infants. For fathers, the mean age was 32.28 ± 3.28 years. Half of the fathers (50%) were high school graduates, 82.1% had stable employment, 74.3% reported moderate economic status, and 92.5% had planned for the pregnancy.
Socio-demographic characteristics of parents and obstetric characteristics of mothers.
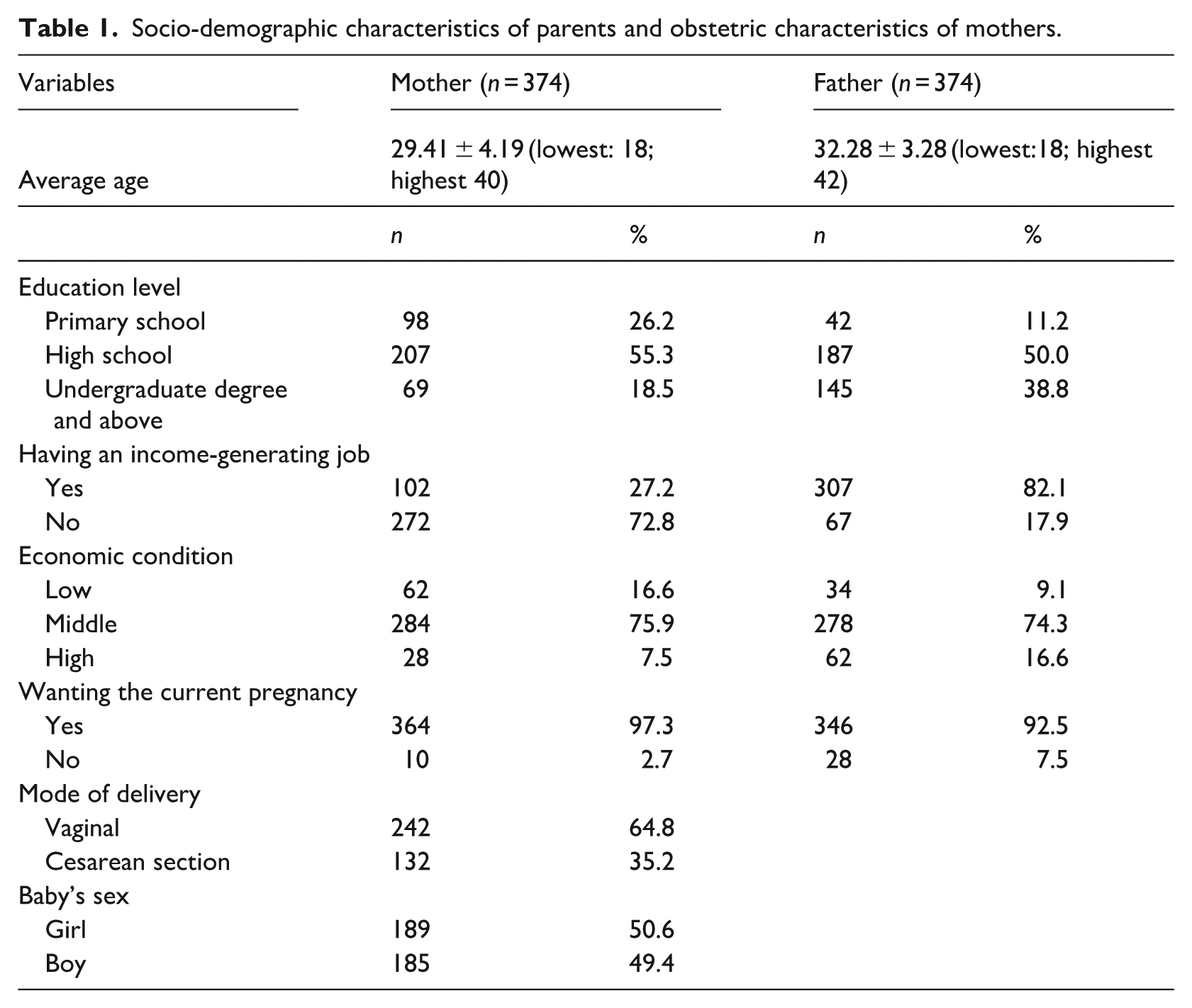
Table 2 presents the average scores of parents on the EPDS and MSPSS scales. The average MSPSS scores of mothers in the first, third, and sixth postpartum months were 60.95 ± 19.46, 59.50 ± 18.17, and 61.65 ± 19.53 respectively, while their average EPDS scores were 6.85 ± 2.14, 15.09 ± 5.30, and 13.95 ± 5.76 respectively. For fathers, the average MSPSS scores in the first, third, and sixth postpartum months were 65.61 ± 17.48, 69.41 ± 12.64, and 68.37 ± 16.88 respectively, and their average EPDS scores were 3.10 ± 1.43, 7.40 ± 2.51, and 5.28 ± 1.30 respectively. In all postpartum periods, mothers had higher EPDS scores and lower MSPSS scores than fathers, and these differences were found to be statistically significant. Cohen’s d values indicated large effect sizes for EPDS scores, whereas for MSPSS scores, the effect sizes ranged from small to moderate levels. When subdimensions were examined, both mothers and fathers showed significant differences in perceived social support from family, friends, and significant others in the first postpartum month (p < 0.05). Mothers had lower scores in all three subdimensions compared with fathers, indicating that fathers perceived higher social support overall.
Parents’ Edinburgh postpartum depression scale and the multidimensional scale of perceived social support mean scores.
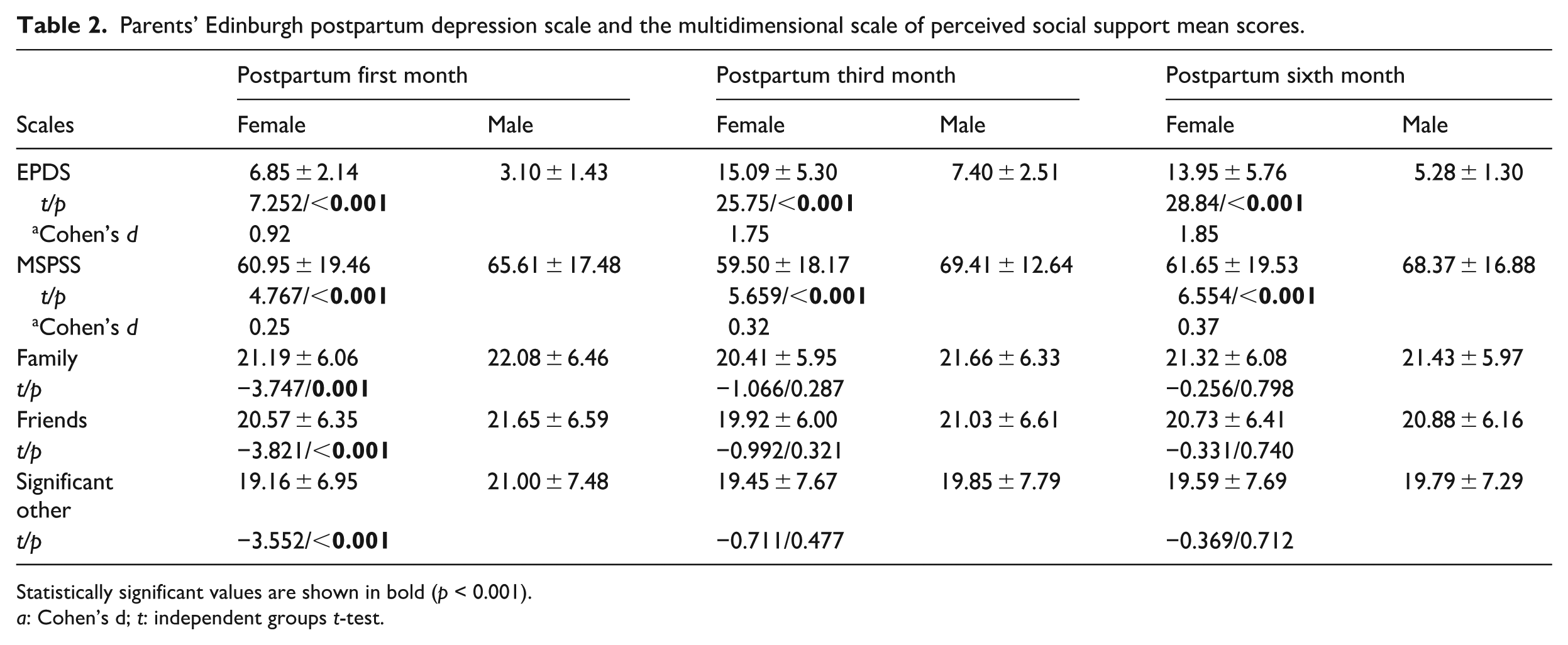
Statistically significant values are shown in bold (p < 0.001).
a: Cohen’s d; t: independent groups t-test.
Table 3 presents the total and subscale scores of the Pittsburgh Sleep Quality Index (PSQI) for mothers and fathers. The mean PSQI scores for mothers in the first, third, and sixth postpartum months were 13.01 ± 2.58, 15.27 ± 2.67, and 10.47 ± 6.75, respectively, while the corresponding scores for fathers were 8.68 ± 5.72, 13.65 ± 4.82, and 7.67 ± 6.96. Across all postpartum periods, mothers demonstrated poorer sleep quality than fathers, as reflected by significantly higher total PSQI scores (p < 0.001). At both the first and sixth months postpartum, mothers had higher scores than fathers in subjective sleep quality, sleep latency, habitual sleep efficiency, and daytime dysfunction, indicating worse performance in these dimensions. In contrast, fathers reported higher use of sleep medication at the third and sixth months postpartum (p < 0.001). Cohen’s d values indicated that the differences between mothers and fathers ranged mostly from medium to large effect sizes, suggesting that postpartum sleep disturbances were more pronounced among mothers throughout the study period.
Parents’ Pittsburgh sleep quality index mean score.
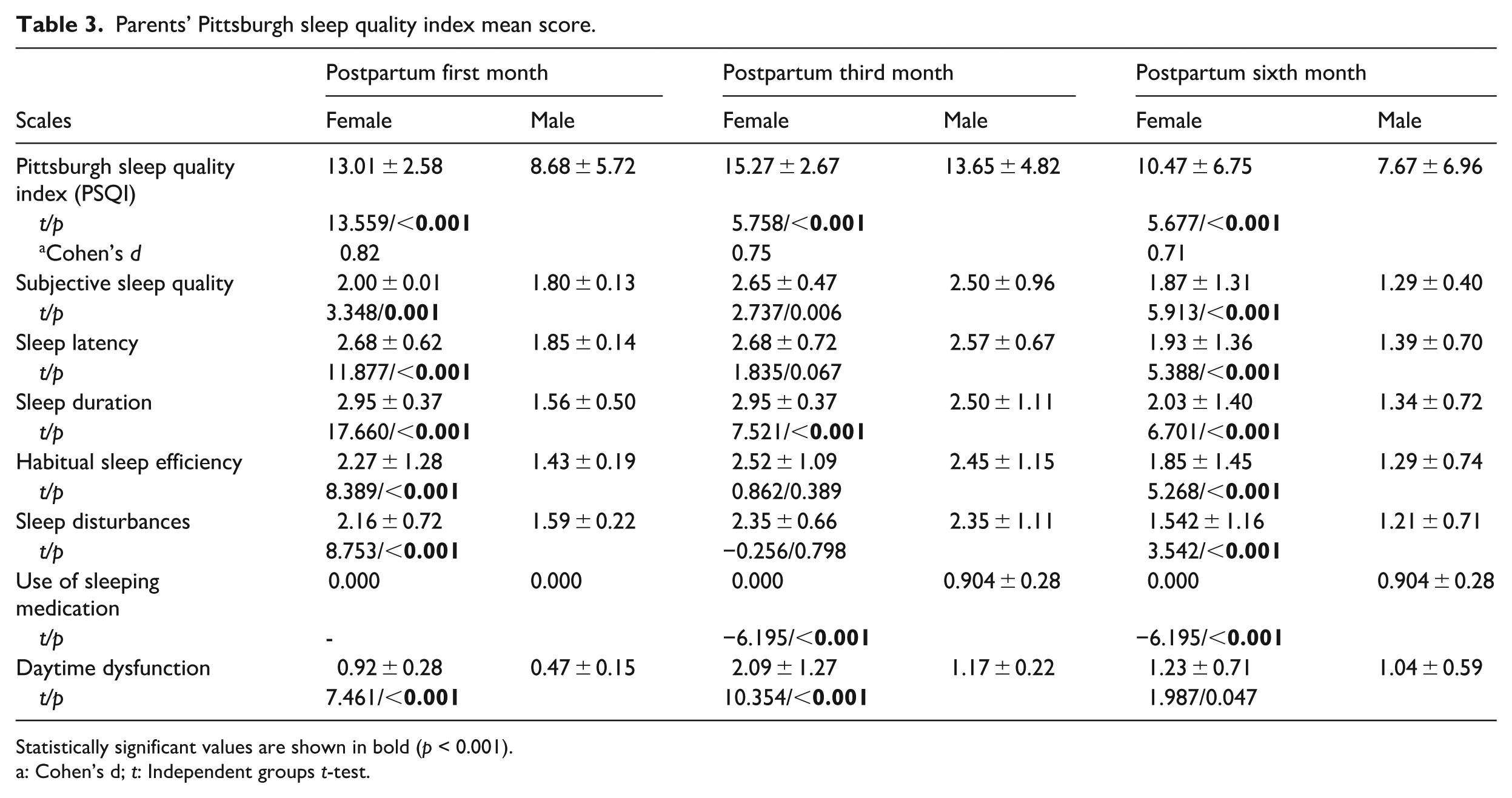
Statistically significant values are shown in bold (p < 0.001).
a: Cohen’s d; t: Independent groups t-test.
Table 4 presents the relationships between parents’ social support (MSPSS), sleep quality (PSQI), and depression (EPDS) scores at the first, third, and sixth months postpartum. Among mothers, a significant and strong negative correlation was found between social support and depression at all time points (r = –0.665, –0.755, –0.778; p < 0.001). A significant negative correlation was also observed between social support and sleep quality (r = –0.662, –0.561, –0.261; p < 0.001), indicating that higher levels of social support were associated with better sleep quality. In addition, a moderate positive correlation was found between sleep quality and depression (r = 0.593, 0.421, 0.329; p < 0.001), indicating that poorer sleep quality was associated with higher levels of depression. Among fathers, significant negative correlations were found between social support and depression at all time points (r = –0.579, –0.458, –0.621; p < 0.001). The correlation between social support and sleep quality was weaker compared with mothers (r = –0.329, –0.307, –0.021). The relationship between sleep quality and depression was also weak and mostly not statistically significant (r = 0.232, 0.062, 0.083). These findings indicate that, for fathers, social support is a more important determinant of postpartum depression than sleep quality.
Relationship between parents’ multidimensional scale of perceived social support, Pittsburgh sleep quality index and Edinburgh postpartum depression scale total mean scores.
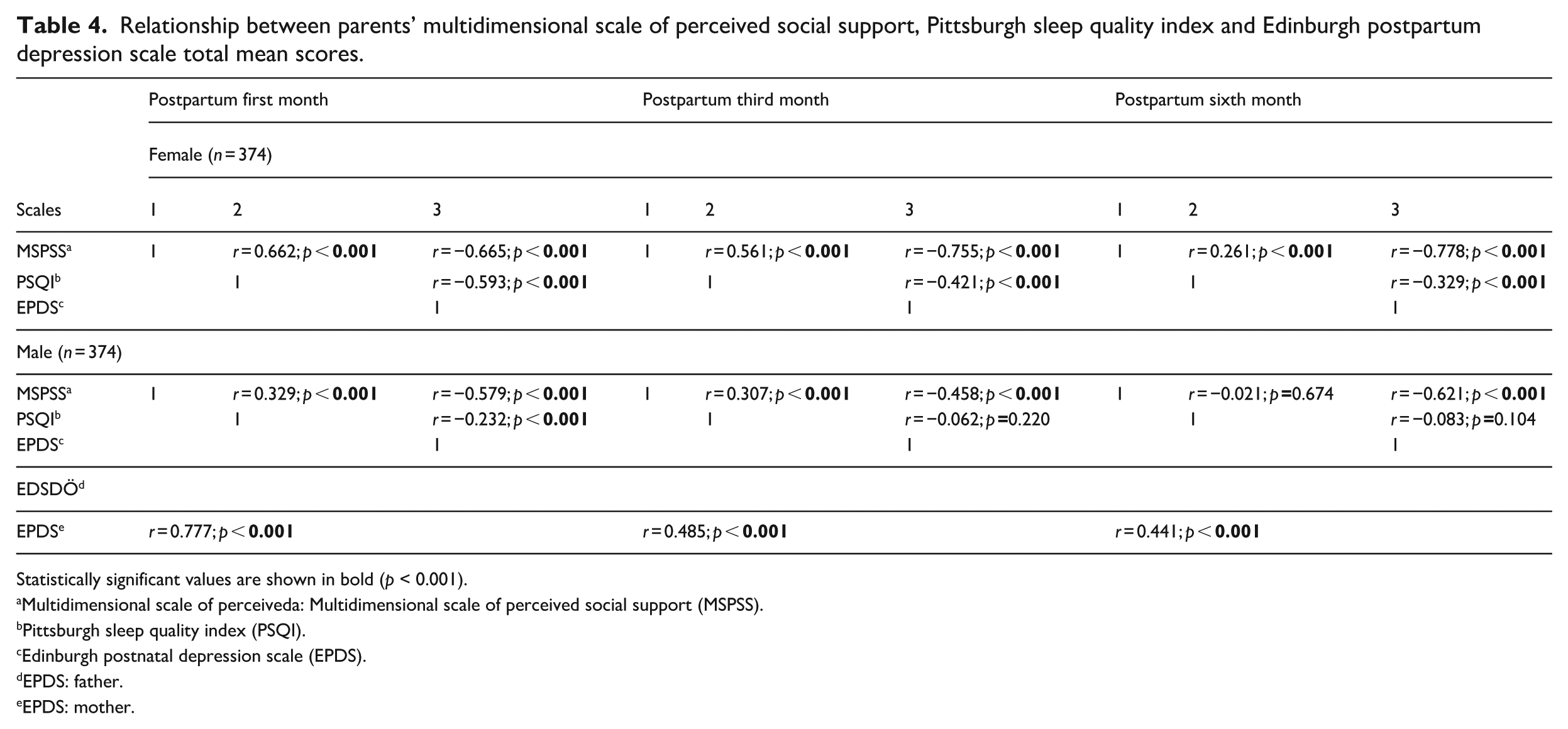
Statistically significant values are shown in bold (p < 0.001).
Multidimensional scale of perceiveda: Multidimensional scale of perceived social support (MSPSS).
Pittsburgh sleep quality index (PSQI).
Edinburgh postnatal depression scale (EPDS).
EPDS: father.
EPDS: mother.
Table 5 presents the predictive effects of social support (MSPSS) and sleep quality (PSQI) on postpartum depression. In mothers, both social support (β = –0.621, R2 = 0.621, p < 0.001) and sleep quality (β = –0.513, R2 = 0.263, p < 0.001) were significant negative predictors of postpartum depression at the first month postpartum. At the third month, social support (β = –0.594, R2 = 0.353, p < 0.001) and sleep quality (β = –0.421, R2 = 0.177, p < 0.001) continued to predict postpartum depression negatively, although the effect sizes slightly decreased. At the sixth month, social support (β = –0.621, R2 = 0.386, p < 0.001) remained a strong predictor, whereas sleep quality (β = –0.329, R2 = 0.108, p < 0.001) was a weaker predictor of depression. In fathers, social support (β = –0.579 to –0.621, p < 0.001) was found to be a significant negative predictor of postpartum depression at the first, third, and sixth months. Sleep quality was a weaker predictor (β = –0.232 to –0.083, p < 0.001), indicating that social support had a stronger influence on paternal depression than sleep quality. Overall, the explanatory power of the model (R2) was higher in mothers than in fathers, suggesting that social support and sleep quality were more effective in explaining postpartum depression among mothers.
Linear regression analysis results of social support and sleep quality predicting postpartum depression.
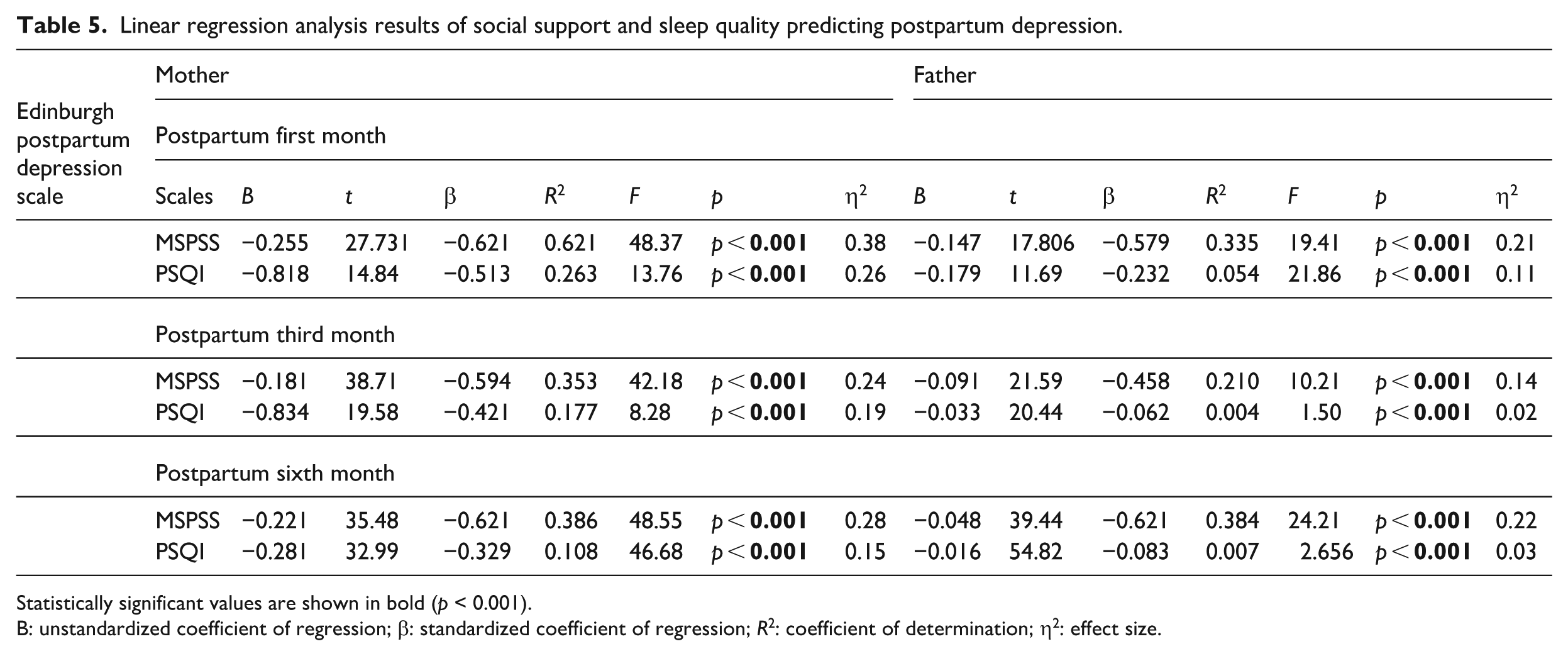
Statistically significant values are shown in bold (p < 0.001).
B: unstandardized coefficient of regression; β: standardized coefficient of regression; R2: coefficient of determination; η2: effect size.
Discussion
This study provides a comparative evaluation of postpartum depression among mothers and fathers during the first 6 months postpartum, with a particular focus on the roles of perceived social support and sleep quality. The findings revealed that although both social support and sleep quality were significantly associated with postpartum depression in both parents, the strength and pattern of these associations differed between mothers and fathers. Social support emerged as a strong protective factor for both parents, whereas the association between sleep quality and depressive symptoms was more pronounced among mothers compared with fathers. These findings suggest that maternal and paternal postpartum depression are shaped by overlapping yet distinct psychosocial mechanisms and highlight the importance of adopting a comparative and family-centered approach in the assessment of postpartum mental health.
The findings demonstrate that higher levels of perceived social support are associated with lower levels of postpartum depression in both mothers and fathers, with a stronger effect observed among mothers. During the postpartum period, social support serves as an important protective factor that facilitates parents’ adjustment to their new roles. This support comprises emotional support (empathy and sharing), instrumental support (help with infant care or household tasks), and informational support (guidance and experience sharing; Lochmannová and Martin, 2025). The findings of this study are consistent with previous research, showing that increased social support among mothers reduces the risk of depression, whereas low social support increases depressive symptoms (Cho et al., 2022; Çınar et al., 2023; Lochmannová and Martin, 2025). This finding can be explained by the fact that mothers, during the postpartum period, face multiple stressors such as adapting to the maternal role, infant care, physical recovery, and social expectations. Social support is a protective factor that facilitates the mother’s adjustment process, helps maintain emotional stability, and alleviates the negative effects of stress (Lochmannová and Martin, 2025; Vaezi et al., 2019). In the cultural context of this study, mothers generally receive support for self-care and infant care from either their own families or their spouses’ families. Although this support contributes to physical and emotional recovery, it may occasionally increase stress due to critical or intrusive attitudes. Moreover, as postpartum care is often provided by the parents’ mothers, fathers tend to remain distant from active caregiving roles. This cultural structure leads fathers to perceive social support mainly through work and peer relationships rather than family interactions. In this study, fathers’ levels of social support were found to be higher than those of mothers, which can largely be explained by the social interactions and friendships provided by full-time employment. In the literature, factors influencing the development of PPD among fathers include increased responsibilities following the birth of a child, financial burdens, role conflicts, and changes in marital relationships (Balcı Yapalak et al., 2025; Wedajo et al., 2023). Insufficient social support exacerbates these factors, heightens stress levels, and predisposes fathers to depressive symptoms. Indeed, several studies have reported that the prevalence of PPD is significantly higher among fathers with low social support (Tarsuslu et al., 2020; Wang et al., 2021; Wedajo et al., 2023). These findings demonstrate that social support plays a direct protective role for both mothers and fathers. The quality and diversity of support sources are critical determinants in assessing the risk of postpartum depression.
In contrast to social support, the relationship between sleep quality and postpartum depression differed in direction and strength depending on the parent. Importantly, as higher PSQI scores indicate poorer sleep quality, the association between sleep quality and depression should be interpreted accordingly. The findings of this study indicate that poorer sleep quality is associated with higher levels of postpartum depression, particularly among mothers. Among mothers, sleep quality was significantly poorer, particularly in the first and third months postpartum, and as sleep quality deteriorated, depression levels increased significantly. In contrast, among fathers, the relationship between sleep quality and depression was weaker and often not statistically significant. The primary cause of sleep disturbances among mothers during the early postpartum period is the assumption of infant care responsibilities, including nighttime feeding and caregiving (Baattaiah et al., 2023; Parsons et al., 2023; Rudzik et al., 2023). This situation often leads to more frequent nighttime awakenings, reduced sleep duration, and increased difficulty falling asleep. Numerous studies have demonstrated that poor sleep quality is strongly associated with the development of PPD among mothers (Baattaiah et al., 2023; Christian et al., 2019; McEvoy et al., 2019; Okun et al., 2018; Rudzik et al., 2023). However, studies addressing the relationship between sleep quality and depression in fathers remain limited. A longitudinal study by Saxbe et al. (2016) found that depressive symptoms observed in the first month postpartum predicted sleep quality at 6 months, and that sleep quality, in turn, predicted depressive symptoms at both 6 and 12 months. Kalogeropoulos et al. (2021), using actigraphy, found no significant relationship between objective sleep parameters (total nighttime sleep duration, nighttime awakenings, sleep efficiency) and depressive symptoms, but reported that fathers’ subjective perception of sleep quality was significantly associated with depression levels. Based on our findings, the stronger association between sleep quality and depression in mothers may be attributed to the fact that infant care during the postpartum period is predominantly the mother’s responsibility, while fathers participate less in nighttime care due to work obligations. Consequently, mothers experience more fragmented sleep and shorter rest periods, which increases depressive symptoms. Therefore, our findings highlight that equitable task-sharing and mutual support between parents during the postpartum period are critical for maintaining psychological well-being.
The findings of this study indicate that postpartum depression should not be addressed solely as an individual mental health problem but rather as a family-centered condition encompassing both mothers and fathers. In Türkiye, postpartum mental health follow-up is conducted in accordance with the Ministry of Health’s Postpartum Care Management Guideline and is directed toward mothers, while no structured screening for paternal postpartum depression is included (Republic of Türkiye Ministry of Health, 2018). This situation may hinder the early identification of depressive symptoms in fathers and lead to the neglect of reciprocal psychosocial interactions between parents. The present findings demonstrate that perceived social support serves as a strong protective factor for both mothers and fathers, whereas poor sleep quality constitutes a particularly salient risk factor for postpartum depression among mothers. These results suggest that current postpartum care practices may be insufficient in addressing parents’ psychosocial needs in a comprehensive manner. Future postpartum care strategies should therefore involve restructuring follow-up programs in primary healthcare settings to include both mothers and fathers, systematically incorporating fathers into mental health screening processes, and developing family-based interventions aimed at strengthening social support networks. In addition, expanding counseling services that promote sleep hygiene and equitable sharing of caregiving responsibilities during the postpartum period may represent effective and sustainable strategies for preventing postpartum depression.
This study provides a comprehensive evaluation of postpartum depression by simultaneously examining both mothers and fathers within a longitudinal framework. By assessing parents at three different postpartum time points, it captures the dynamic nature of psychosocial changes during the early postpartum period. In addition, the concurrent evaluation of social support and sleep quality allows for a more integrated understanding of their roles in postpartum depression. Conducted in a primary care setting in Türkiye, where postpartum services are largely focused on mothers, this study also highlights the importance of incorporating fathers into routine mental health assessment and family-centered care approaches.
Limitations
This study has several limitations. First, the findings cannot be generalized, as the study was conducted in a single center and included only primiparous parents. Second, all data were obtained through self-reported questionnaires, which may have introduced response bias. Third, participants who may have experienced pregnancy- or childbirth-related complications were not specifically excluded, which may have influenced the results. This should be considered when interpreting the findings.
Conclusion
This study examined psychosocial correlates of postpartum depression among mothers and fathers during the first 6 months postpartum using a longitudinal approach, highlighting the importance of a comprehensive evaluation of parental mental health. The findings indicate that perceived social support serves as a strong protective factor for both parents, while sleep quality is more strongly associated with postpartum depression among mothers. The observed differences in the strength of these correlates between mothers and fathers suggest that postpartum depression cannot be adequately understood within a uniform framework. In this respect, the findings underscore the importance of adopting comparative and family-centered perspectives in the assessment of postpartum mental health.
Footnotes
Ethical considerations
Ethical approval for this study was obtained from the Non-Invasive Clinical Research Ethics Committee of Sivas Cumhuriyet University (Approval No: 2023-09/20). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Prior to data collection, all participants were informed about the purpose and procedures of the study, and both verbal and written informed consent were obtained. The authors declare that no external funding was received for this study.
Consent to participate
All participants took part on a voluntary basis and provided written informed consent to participate in the study.
Consent for publication
Consent for publication is not applicable to this review article as no identifiable participant data are included.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used in the current study are available from the corresponding author upon reasonable request*.