
Abstract
This scoping review mapped interventions targeting disease-related loneliness among people living with chronic diseases and synthesized their underlying mechanisms of change. A systematic search was conducted across CINAHL, MEDLINE, Academic Search Premier, PsycInfo, AMED, Rehabilitation & Sports Medicine Source, and Embase to identify original studies reporting findings from interventions addressing loneliness among adults with chronic disease. Data were analyzed using qualitative content analysis to identify shared mechanisms of change. Seven studies representing six unique interventions were included. Three overarching mechanisms of change were identified: learning-oriented support, trusted relationships, and empathic communication. These mechanisms were observed across interventions and appear to influence participant engagement with interventions for disease-related loneliness. Although the evidence base remains limited, these findings highlight key mechanisms that may inform the development and evaluation of supportive interventions for disease-related loneliness.
Introduction
Loneliness is a common condition, particularly among individuals with chronic disease (Petitte et al., 2015), and it increases with age (⩾70 years; Pinquart and Sorensen, 2001). Together, this indicates that chronic disease and older age are associated with loneliness (Petitte et al., 2015). Loneliness is not solely influenced by the number of social contacts, as individuals may feel lonely even when socially active or feel content despite limited interaction (Hawkley and Cacioppo, 2010). Loneliness is defined as a distressing feeling arising from the perception that one’s social needs are unmet, particularly in terms of the quality of relationships (Gray, 2019; Hawkley et al., 2008; Holt-Lunstad and Smith, 2016; Mansfield et al., 2021). Loneliness is a significant health concern, particularly among people living with chronic diseases (Alqahtani et al., 2024; Holt-Lunstad and Smith, 2016; Petitte et al., 2015) such as chronic obstructive pulmonary disease (COPD), diabetes mellitus, or heart disease. Physical limitations can restrict engagement in everyday life and social activities, which may contribute to declining physical and mental health. Further, reduced social participation, which is also associated with chronic disease, may lead to a mismatch between desired and actual social relationships, intensifying feelings of loneliness and increasing the overall disease burden (Olano-Lizarraga et al., 2023). Besides, loneliness is linked to adverse outcomes such as cardiovascular disease, immune dysfunction, and mental health problems (Hawkley, 2022; Local Government Association, 2016; Perlman and Peplau, 1981).
Several types of interventions have been evaluated for their potential to reduce disease-related loneliness, including counselling, peer support, cognitive restructuring, and physical activity, delivered in group or community settings (Shvedko et al., 2020; Theeke et al., 2016; Zhang et al., 2024). These interventions may help reduce loneliness by fostering emotional expression, social learning, cognitive reframing, and sustained support (Shvedko et al., 2020; Theeke et al., 2016; Zhang et al., 2024). Although these interventions are based on various theoretical frameworks, they typically focus on outcomes rather than on the mechanisms that explain how change occurs (Shvedko et al., 2020; Theeke et al., 2016; Zhang et al., 2024). ‘Mechanisms of change’ is a key concept for understanding the processes through which interventions produce outcomes via participants’ interactions with an intervention (Moore et al., 2015; Skivington et al., 2021). These interactions can include direct engagement, social exchanges, and reflective practices, all of which are essential for participants to internalize knowledge, adjust their behaviour, and achieve the intended outcomes (Illari and Williamson, 2012; Moore et al., 2015; Skivington et al., 2021). As noted by Moore et al., such mechanisms may vary depending on contextual factors and be detected through both quantitative and qualitative data (Moore et al., 2015).
Exploring mechanisms of change can clarify how specific intervention components interact with participants. Identifying these mechanisms can help understand how and why certain interventions are effective in reducing disease-related matters such as loneliness (Moore et al., 2015). It remains unclear whether sufficient knowledge exists to determine which mechanisms are essential to include in intervention studies targeting disease-related loneliness. This scoping review aimed to map interventions targeting disease-related loneliness and to synthesize the mechanisms through which they are intended to work.
Methods
Design
This scoping review followed the Joanna Briggs Institute’s Reviewers manual and PRISMA extension for scoping reviews (PRISMA-ScR; Supplemental File A_PRISMA ScR; Peters et al., 2020; The Joanna Briggs Institute, 2015; Tricco et al., 2018). A scoping review was selected to systematically map the breadth and depth of existing evidence across various research methodologies, irrespective of study quality (Peters et al., 2020; The Joanna Briggs Institute, 2015). The review protocol was pre-registered (DOI 10.17605/OSF.IO/RZEK9).
Search strategy
A systematic literature search was conducted on September 30, 2024, and updated on July 1, 2025. The databases used for the search were CINAHL, MEDLINE, Academic Search Premier, PsycInfo, AMED, Rehabilitation & Sports Medicine Source, and Embase. The search strategy followed the PCC (Population, Concept, and Context) three blocks (Peters et al., 2020; The Joanna Briggs Institute, 2015): (P) patients with a chronic disease, (C) loneliness and social isolation, and (C) interventions aimed at alleviating loneliness (Supplemental File B_Search strategy from Embase). The search strategy was developed in close collaboration between the research authors, including an experienced librarian.
Eligibility criteria
We applied the following in- and exclusion criteria:
Inclusion:
Adults (⩾18 years) with a primary diagnosis of a chronic disease (diabetes, cardiac disease, or COPD)
All peer-reviewed original research records reporting qualitative and/or quantitative findings from interventions aimed at alleviating loneliness
Interventions including both research-based and implemented interventions
Exclusion:
Studies focusing on individuals living in institutional care settings or receiving regular home care for daily activities, as these populations may have substantial functional limitations
Interventions targeting transient (short-term) loneliness, understood as temporary or situational experiences of loneliness not associated with chronic disease or long-term social disconnection
There were no restrictions regarding the publication year, language, or geographic origin.
Selection of records
All records were imported into Covidence (Veritas Health Innovation Ltd.), and duplicates were removed. A pilot screening of 50 randomly selected records was conducted to refine the inclusion and exclusion criteria.
Hereafter, two authors (MBR and MLN) independently screened the records following three steps: (1) screening of title and abstract, (2) screening by reading the full-text, and (3) reference lists of included studies were sought for relevant studies (Peters et al., 2020; The Joanna Briggs Institute, 2015). MBR and MLN conducted the screening of the title and abstract, and in case of disagreements, the author DS was consulted to reach consensus. The full-text screening was conducted in pairs across the authors (DM & MBR and JSJ & MLN), and in case of disagreements, all authors discussed to reach consensus. Following the Joanna Briggs guidelines for scoping reviews, the reference lists of all included records were searched for additional relevant records and were screened using the same process (Peters et al., 2020; The Joanna Briggs Institute, 2015).
Data extraction
Data were extracted in pairs (DS & MBR and MLN & JSJ) to reduce selection bias. A structured data extraction form was designed to capture key information for each study, including author, title, design, aim, population, intervention, mechanisms of change, and conclusion.
Data analysis
Data were analysed using principles from qualitative content analysis (Graneheim and Lundman, 2004). Three authors (DS, MBR, MLN) independently coded the extracted material to identify meaning units and preliminary codes. These were then discussed and refined through collaborative meetings. The analysis moved through an iterative interpretation, identifying patterns in different interventions to generate a synthesized understanding of mechanisms of change. The entire author team contributed to interpreting the data, exploring relationships, and shaping the presentation of findings. The final themes represent an abstraction of recurring patterns identified in the included studies, integrating diverse findings into a coherent synthesis of mechanisms rather than reporting individual study results. Final themes were developed iteratively to reflect latent content and ensure analytic coherence.
Results
Study selection
A total of 6115 records were identified from the systematic literature search, and 3584 remained after duplicates were removed. Of these, 3545 were excluded based on title and abstract, leaving 39 reports sought for retrieval. Despite professional assistance from a librarian, 1 report could not be retrieved, resulting in 38 reports assessed for eligibility, of which 31 were subsequently excluded.
The screening of the reference lists of the included records yielded 44 additional records, from which 28 were selected for screening after duplicates were removed. The titles and abstracts of these additional records were screened, resulting in eight records deemed relevant for full-text screening. However, none of these were included in the final analysis. Hence, a total of seven studies were included in the analysis. The primary reason for exclusion was the ineligibility of intervention and/or population (Figure 1).
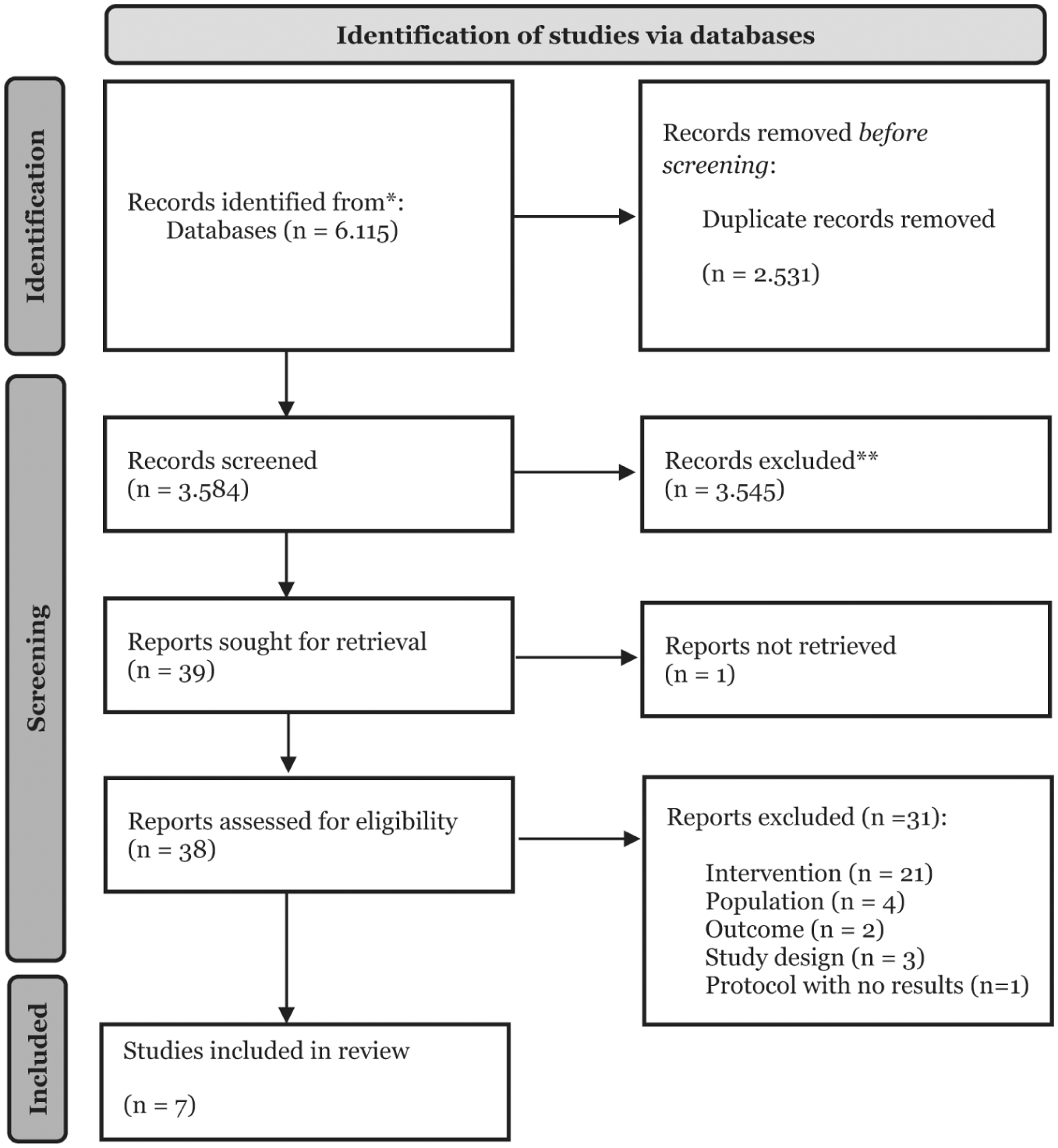
PRISMA-ScR flowchart of study selection process.
Study characteristics
Three studies originated from the USA (Kahlon et al., 2021; Theeke et al., 2015, 2016), while the remaining studies originated from Canada (Alsubheen et al., 2024), England (Shvedko et al., 2020), China (Shvedko et al., 2020), and Denmark (Blakoe et al., 2024). All studies were published between 2015 and 2024, with the majority (n = 5) being published within the last 5 years. Four studies were designed as randomized controlled trials (RCTs; Kahlon et al., 2021; Shvedko et al., 2020; Theeke et al., 2016; Zhang et al., 2024), two as feasibility RCTs (Blakoe et al., 2024; Theeke et al., 2015), and one as a ‘before-and-after’ study (Alsubheen et al., 2024). The sample size varied from 2 to 226 participants (Alsubheen et al., 2024; Blakoe et al., 2024; Kahlon et al., 2021; Theeke et al., 2015, 2016; Zhang et al., 2024). The type of longstanding condition was primarily mixed (n = 5; Kahlon et al., 2021; Shvedko et al., 2020; Theeke et al., 2015, 2016; Zhang et al., 2024), while one study focused on COPD (Alsubheen et al., 2024) and one on cardiac disease (Blakoe et al., 2024). The majority (n = 4) of studies involved interventions delivered through groups (Shvedko et al., 2020; Theeke et al., 2015, 2016; Zhang et al., 2024), while two studies involved interventions delivered individually (Blakoe et al., 2024; Kahlon et al., 2021), and one study did not specify how the intervention was delivered (Alsubheen et al., 2024). Furthermore, two studies reported data on the same intervention (Theeke et al., 2015, 2016); hence, a total of seven studies and six unique interventions were identified.
Although the included studies primarily aimed to explore feasibility and acceptability, several reported preliminary findings on loneliness outcomes. Across the included studies, reported effects on loneliness were generally small and inconsistent (Alsubheen et al., 2024; Kahlon et al., 2021; Theeke et al., 2016; Zhang et al., 2024). Overall, there was substantial heterogeneity in the content, delivery formats, duration, and target populations of the interventions. This variation makes it difficult to identify any consistent pattern or relationship between intervention characteristics and changes in loneliness. No clear link emerged between the proposed mechanisms of change and the reported outcomes on loneliness.
Intervention characteristics
In total, six intervention characteristics were identified across the included studies. These included the following: longstanding condition, intensity, providers, setting, core components, and patient involvement and tailoring. The intervention characteristics are summarized in Table 1.
Study characteristics of included studies.
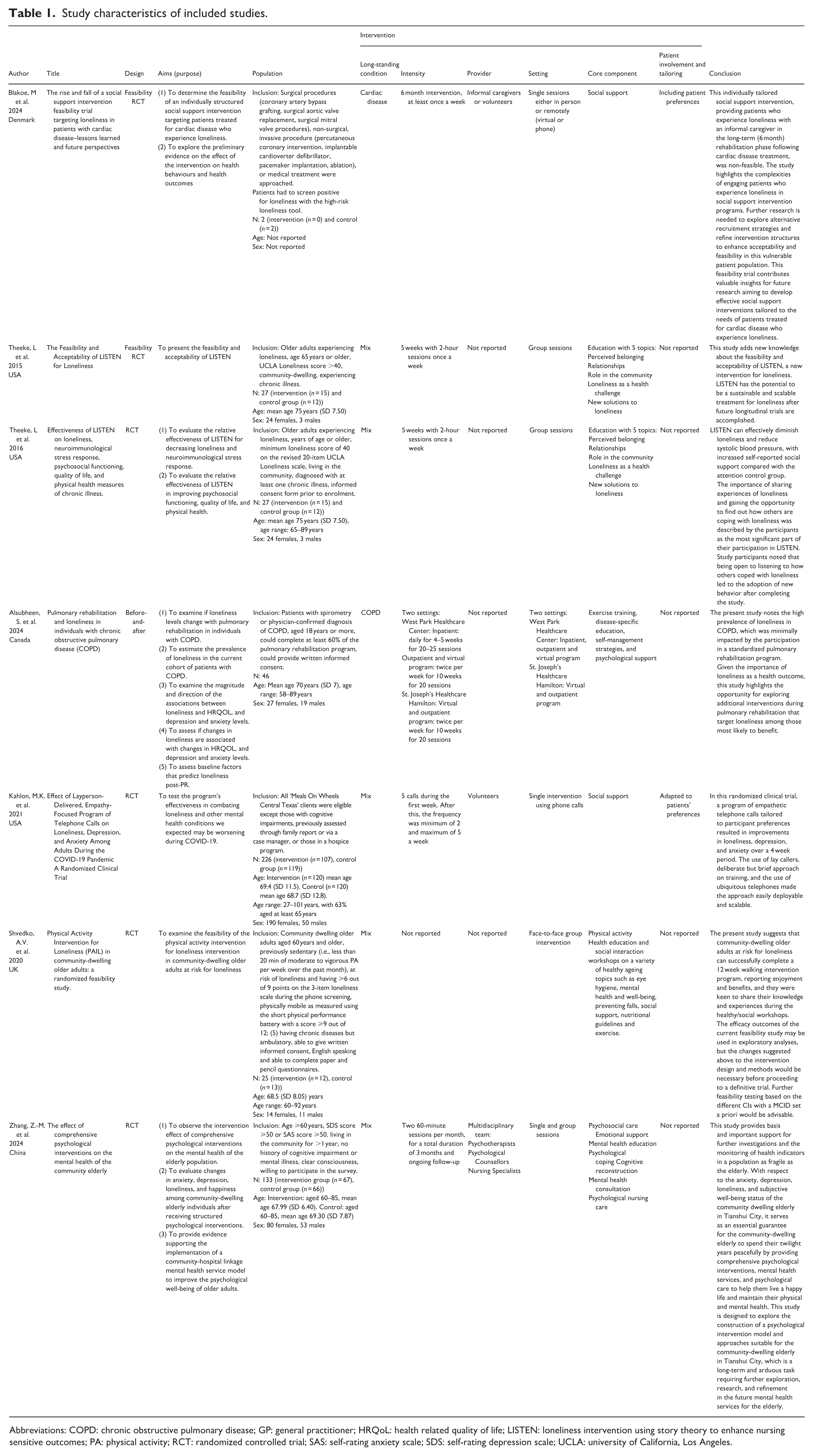
Abbreviations: COPD: chronic obstructive pulmonary disease; GP: general practitioner; HRQoL: health related quality of life; LISTEN: loneliness intervention using story theory to enhance nursing sensitive outcomes; PA: physical activity; RCT: randomized controlled trial; SAS: self-rating anxiety scale; SDS: self-rating depression scale; UCLA: university of California, Los Angeles.
Synthesis of mechanisms of change
Across the six interventions, three overarching mechanisms of change were identified: learning-oriented support, trusted relationships, and empathic communication. These mechanisms are analytically distinguished but inherently interrelated and often co-occurred. The intention was not to present them independently, but to capture both different and connected aspects of how change processes unfold. Overlap between mechanisms, such as the presence of empathy and respect across categories, reflects their interconnected nature rather than conceptual duplication. The synthesis is illustrated in Figure 2.
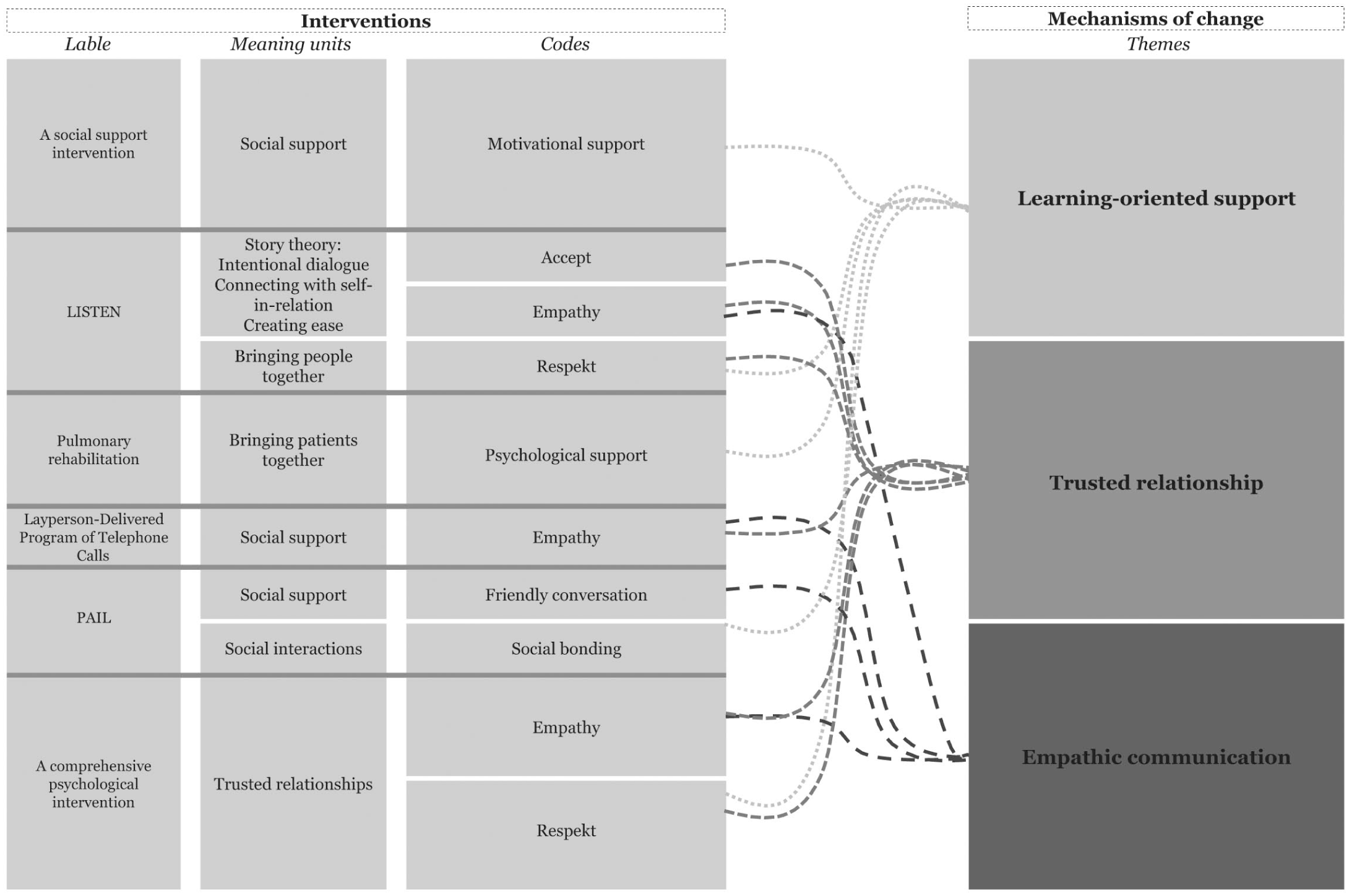
Synthesis of mechanisms of change.
Learning-oriented support
The mechanism of learning-oriented support was explained through how participants received guidance, encouragement, and opportunities for reflection that improved their ability to deal with loneliness. This support was based on emotional safety and respect for the individual’s preferences (Blakø et al., 2023). Guidance was provided through gentle encouragement to take manageable steps toward social engagement or new activities tailored to the participant’s readiness (Zhang et al., 2024). Psychological encouragement facilitated the expression of thoughts and feelings, allowing participants to process their experiences of isolation in a non-judgmental setting (Alsubheen et al., 2024; Theeke et al., 2015, 2016). Respect was shown by acknowledging personal stories, validating emotions, and recognizing boundaries, which strengthened participants’ sense of agency and self-worth (Theeke et al., 2015, 2016; Zhang et al., 2024). Learning-oriented support helped participants explore new coping strategies, gain insight into their own needs and behaviours, and make meaningful changes related to loneliness (Theeke et al., 2015, 2016). Together, these elements refer to a learning process in which participants gain insight and make changes related to loneliness. In both individual and group interventions, learning-oriented support provided the necessary encouragement for participants to turn their insights into action. This mechanism illustrates how reflective and supportive learning processes may contribute to change in interventions aimed at addressing disease-related loneliness.
Trusted relationships
The mechanism of trusted relationship was described through the quality of the interpersonal connection between participants and the provider delivering the intervention. Trusted relationships refer to the ongoing relational bonds that develop over time between participants and intervention providers. The relationship was based on characteristics such as acceptance, empathy, respect, and the providers’ capacity to evoke positive emotions in the patients (Kahlon et al., 2021; Theeke et al., 2015, 2016; Zhang et al., 2024). Participants consistently emphasized the importance of feeling accepted and respected by the providers (Zhang et al., 2024). Respect was evident in how interventionists acknowledged individual differences, showed understanding for diverse life experiences, and approached each person without imposing assumptions. This relational safety enabled participants to share personal stories, process difficult emotions, and feel seen as whole individuals (Theeke et al., 2015, 2016). In both individual and group contexts, the trusted relationship provided the emotional foundation necessary for participants to engage in new reflections and adopt behavioural responses to loneliness. This mechanism highlights the relational processes through which interventions can reduce loneliness among individuals living with chronic diseases.
Empathic communication
The mechanism of empathic communication reflected how participants experienced being genuinely heard, understood, and emotionally met during their interactions with the intervention provider and other participants. Friendly conversations between participants during group walks exemplified empathetic communication, aimed at enhancing peripheral social networking and serving as a form of compensation for lost meaningful social connections (Shvedko et al., 2020). Empathy was conveyed not only through words but through attentive presence, tone of voice, and responsiveness (Theeke et al., 2015). Participants emphasized empathy as a necessary personality characteristic for the interventionists and described how being listened to without judgment and with full attention made them feel safe and valued (Kahlon et al., 2021; Theeke et al., 2015, 2016; Zhang et al., 2024). Interventionists demonstrated sensitivity to individual needs and allowed space for participants to share their experiences in their own way (Theeke et al., 2015). Empathic engagement supported participants in expressing vulnerability, exploring emotions, and developing trust (Theeke et al., 2015, 2016). It laid the foundation for conversations, which in turn enabled participants to reconsider their social and emotional situations. Based on this interpretation this mechanism underscores the communicative pathways that can facilitate change in interventions addressing disease-related loneliness.
Discussion
Understanding mechanisms of change in disease-related loneliness
To our knowledge, this is the first scoping review to examine mechanisms of change across interventions targeting disease-related loneliness among people living with chronic diseases. Mechanisms are understood as entities and activities organized to produce a phenomenon (Illari and Williamson, 2012). In line with our analytical approach, interventions are understood as providing resources and opportunities that participants engage with and act upon, thereby initiating processes that may alleviate loneliness rather than directly causing outcomes. Across studies, we identified three overarching mechanisms: learning-oriented support, trusted relationships, and empathetic communication, which appeared central regardless of the intervention format.
Self-Determination Theory (SDT) provides a useful framework for understanding why these mechanisms may be effective (Ryan and Deci, 2017). According to SDT, well-being and motivation are fostered when three basic psychological needs are met: autonomy, competence, and relatedness (Ryan and Deci, 2017). Learning-oriented support promotes autonomy and competence by enabling participants to explore personal resources and develop strategies for action in everyday life. Trusted relationships and empathic communication both address relatedness, as respect, trust, and non-judgment foster disclosure, validation, and connection. This may be particularly important in chronic disease contexts, where loneliness is often compounded by stigma, shame, or feelings of inadequacy (Brighton et al., 2022; Fan et al., 2023). Viewed together, the three mechanisms can be seen as processes that contribute to the satisfaction of basic psychological needs, thereby helping to explain how interventions may reduce loneliness.
A previously published meta-analysis of SDT-informed interventions in the health domain provides relevant insights for interpreting these findings (Ntoumanis et al., 2021). The meta-analysis showed that autonomy and competence support were consistently promoted, whereas relatedness was less frequently addressed explicitly (Ntoumanis et al., 2021). This is noteworthy in the context of disease-related loneliness, where relational and communicative processes appeared particularly central (Ntoumanis et al., 2021). While the meta-analysis did not examine loneliness as an outcome, it supports the use of SDT as an explanatory framework for understanding the mechanisms identified in this review.
Other reviews provide complementary perspectives. For instance, Kotwal et al. (2021) and Thompson et al. (2022) reported that peer-support interventions for people with chronic diseases may reduce loneliness and improve well-being, highlighting the importance of relatedness (Kotwal et al., 2021; Thompson et al., 2022). In our synthesis, empathic communication, trusted relationships, and learning-oriented support all emerged as mechanisms of change. When interpreted through SDT, these mechanisms correspond to the three basic psychological needs, although relational processes were more frequently articulated in the included studies.
While SDT offers a coherent explanation for the identified mechanisms, the available data do not allow for firm conclusions. Mechanisms were often inferred rather than directly investigated, and the small number of eligible studies limits the generalizability of our findings. These limitations underline the need for future studies to systematically articulate and empirically test mechanisms of change in interventions addressing disease-related loneliness, particularly those rooted in established theoretical frameworks such as SDT.
Methodological considerations
This scoping review followed the methodological guidance of the Joanna Briggs Institute and the PRISMA-ScR framework to ensure transparency, consistency, and reproducibility (Peters et al., 2020; The Joanna Briggs Institute, 2015; Tricco et al., 2016). Adherence to predefined procedures enhances credibility but may limit responsiveness to emerging nuances within the literature. Similarly, preregistration of the protocol in the Open Science Framework strengthened methodological accountability and reduced the risk of bias, yet it also restricted the possibility of refining the research focus as new understandings developed during the review process (Pollock et al., 2024; Tricco et al., 2016). However, defining search terms a priori proved particularly challenging within the preregistered protocol, as methodological concepts lack standardized indexing and terminology varies across disciplines (Martin et al., 2020).
The search strategy was designed to comprehensively cover the breadth of the research field, drawing on multiple databases, and is documented in the registered protocol (The Joanna Briggs Institute, 2015; Tricco et al., 2018). Additionally, the reference lists of included studies were screened for potential inclusion. No limitations were imposed regarding publication year, language, or geographic origin, which represents a methodological strength that supports a more comprehensive synthesis and increases the potential for generalizability across different settings and populations (Peters et al., 2020). Screening and data extraction were performed independently by two authors to minimize bias and increase objectivity. Data extraction followed a predefined table with standardized labels, which facilitated consistency and comparability of the extracted information.
As is standard in scoping reviews, no formal quality assessment of included studies was conducted (The Joanna Briggs Institute, 2015). Therefore, the methodological quality and risk of bias within the included studies remain unknown. Moreover, relevant studies published as grey literature or outside indexed journals may have been missed. Finally, our strict inclusion criteria, particularly the requirement that loneliness be a primary outcome, limited the pool of eligible studies and may affect the generalizability of our findings.
Most records were excluded at the full-text stage because loneliness was not the primary outcome, highlighting the scarcity of interventions explicitly addressing disease-related loneliness. This suggests that loneliness is often treated as a secondary or indirect outcome rather than a primary target. Furthermore, one study could not be accessed in full text despite professional assistance from a librarian, which may have led to the inadvertent exclusion of potentially relevant data. While this limitation is unlikely to have altered the overall conclusions, it reflects broader issues in accessibility and reporting practices within the field. Nevertheless, the search strategy was deliberately broad and inclusive, consistent with the purpose of a scoping review to comprehensively map existing evidence across study designs and conceptual approaches.
Implications for future research
This review highlights the need for more conceptually grounded intervention studies explicitly addressing disease-related loneliness. Across included studies, mechanisms of change were rarely detailed and often had to be inferred from theory, intervention design, and participant experiences (Illari and Williamson, 2012). This lack of explicit reporting limits knowledge accumulation and hinders replication. Although many interventions claimed theoretical grounding, few explained how theoretical concepts were operationalized or linked to outcomes. Mechanisms of change are frequently explored through process or realist evaluations to clarify how contextual factors shape results. Such studies were not identified in this review despite broad inclusion criteria, highlighting their importance for future research to understand how interventions for disease-related loneliness work.
Conclusion
This scoping review mapped and synthesized interventions targeting disease-related loneliness, identifying three central mechanisms of change: learning-oriented support, trusted relationships, and empathic communication. These mechanisms were consistently reported across different intervention formats and appear to shape how participants engage with interventions aimed at reducing loneliness in the context of chronic disease.
The current evidence base remains limited and fragmented, as few interventions explicitly target loneliness as a primary outcome, and the mechanisms of change are rarely described in detail. There is a need for well-designed and theory-informed interventions that clearly articulate how change is expected to occur. Strengthening theoretical and methodological clarity will support future development, evaluation, and implementation of interventions addressing loneliness among people living with chronic disease.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261454659 – Supplemental material for Interventions to alleviate loneliness in chronic disease: A scoping review on mechanisms of change
Supplemental material, sj-docx-1-hpq-10.1177_13591053261454659 for Interventions to alleviate loneliness in chronic disease: A scoping review on mechanisms of change by Maiken Bay Ravn, Dorthe Sørensen, Marianne Lyngmose Nielsen, Camilla Askov Mousing, Tina Helle and Julie Sandell Jacobsen in Journal of Health Psychology
Supplemental Material
sj-pdf-2-hpq-10.1177_13591053261454659 – Supplemental material for Interventions to alleviate loneliness in chronic disease: A scoping review on mechanisms of change
Supplemental material, sj-pdf-2-hpq-10.1177_13591053261454659 for Interventions to alleviate loneliness in chronic disease: A scoping review on mechanisms of change by Maiken Bay Ravn, Dorthe Sørensen, Marianne Lyngmose Nielsen, Camilla Askov Mousing, Tina Helle and Julie Sandell Jacobsen in Journal of Health Psychology
Footnotes
Acknowledgements
The authors gratefully acknowledge the assistance of Maria Viftrup Schneider, information specialist at VIA Library, in conducting the electronic database searches.
ORCID iDs
Ethical considerations
Ethics approval was not required for this review article as no data were collected from participants.
Consent to participate
Consent to participate is not applicable to this review article as no data were collected from participants.
Consent for publication
Consent for publication is not applicable to this review article as no identifiable participant data are included.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request*.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.