
Abstract
As the most important component of human capital, health is a far-reaching and significant dimension in assessing social development. Using data from the 2021 Chinese General Social Survey (CGSS), this study distinguished self-rated, physical, and mental health to examine the association between subjective socioeconomic status (subjective SES) and multidimensional health among Chinese residents, and to test the roles of aging anxiety and education in this relationship. The results indicated that subjective SES was positively associated with self-rated, physical, and mental health. Aging anxiety partially mediated the relationship between subjective SES and each health dimension. Education moderated the associations between aging anxiety and self-rated as well as physical health; however, the moderation for mental health was not statistically significant. These findings highlight several areas warranting policy attention, including community-based psychosocial interventions and lifelong learning initiatives, with potential benefits for health among Chinese residents.
Introduction
Health is not only a fundamental element for the survival and development of individuals but also the cornerstone and destination of high-quality social and economic development (Han and Zhao, 2021). As China is the most populous country in the world, the health status of its population is closely related to the healthy development of the global population. At the beginning of 2020, the outbreak of the COVID-19 pandemic triggered a global public health crisis, and health issues renewed widespread attention from scholars and policymakers. Therefore, it is crucial to explore how to improve the health status of the whole population.
Numerous studies have shown that individuals’ health is associated with many factors, including psychological capital (Turliuc and Candel, 2022), social support (Acoba, 2024), and Internet use (Jin and Kim, 2025). Generally speaking, health status is closely related to socioeconomic status (SES) indicators (Sun et al., 2019). Subjective SES and objective SES are multifaceted constructs that, while significantly correlated, do not fully overlap. This implies that an individual’s subjective SES may differ from their objective SES, and such discrepancies reflect inaccuracies in self-perception (Liu and Liu, 2023). Previous studies have mostly focused on the relationship between objective SES and health. However, compared to objective SES, subjective SES is more valuable in research on individual health and development and can independently predict individual health status (Quon and McGrath, 2014), as it represents the cognitive average of various indicators of objective SES (e.g. income, occupation), yielding a more precise measurement of overall SES (Präg et al., 2016). Moreover, chronological age is associated with SES both objectively and subjectively. Recent research highlights that SES is dynamic across the lifespan, with individuals stepping up or down in perceived standing as they age (Weiss and Kuball, 2025). This dynamic perspective underscores the importance of subjective SES, which captures self-perceptions of one’s place in the social hierarchy and is particularly sensitive to age-related changes in resources and roles. Although previous studies have explored the potential mechanisms of the relationship between subjective SES and health, few scholars have focused on the role of aging anxiety and personal education level.
The Social Determinants of Health (SDH) model posits that an individual’s health status is intricately linked to various social, economic, and environmental factors (Prus, 2011). Subjective SES emerges as a pivotal social determinant, reflecting an individual’s perception of their standing within the societal hierarchy, with lower subjective SES potentially contributing to adverse health outcomes (Ran et al., 2022). Aging anxiety, characterized as a psychological phenomenon, encompasses individuals’ concerns and apprehensions regarding the aging process (Westerhof and Wurm, 2015). Within the SDH framework, aging anxiety is conceptualized as a psychosocial factor linked to an individual’s health perceptions and susceptibility to health risks (Bergman and Segel-Karpas, 2021). Education level is acknowledged as a significant factor within SDH paradigms, with higher educational attainment generally associated with improved health outcomes due to enhancements in health literacy, health-related behaviors, and healthcare access (Raghupathi and Raghupathi, 2020). Therefore, drawing upon the data from the 2021 Chinese General Social Survey (CGSS), this study aims to investigate the relationship between subjective SES and the self-rated, physical, and mental health of Chinese residents by introducing aging anxiety as a mediating variable and education as a moderating variable. The insights derived from this investigation hold the potential to enrich the existing discourse on health in China and offer theoretical implications for academia and policymakers.
Subjective socioeconomic status and health
Subjective SES refers to an individual’s subjective perception of their position in the social hierarchy, and the self-appraisal of one’s location in a socioeconomic system (Jackman and Jackman, 1973). By contrast, subjective social status (SSS) reflects individuals’ perceptions of their relative position within the social hierarchy, often measured by the MacArthur ladder scale (Adler et al., 2000). Although the two are correlated, they are distinct concepts. Subjective SES focuses on the subjective perception of specific resources and status, while SSS emphasizes relative social rank, which are crucial for understanding psychological processes. In this study, we focus on subjective SES, operationalized by individuals’ self-placement on the socioeconomic ladder in the CGSS 2021. This is conceptually aligned with SSS in this dimension. The relationship between subjective SES and health has received widespread scholarly attention since the 1990s. Scholars have mostly adopted the social causation theory to explore the relationship between subjective SES and health. The theory holds that due to unequal positions in the social structure, individuals with higher subjective SES exhibit better health than those with lower subjective SES (Kröger et al., 2015). It is widely believed that individuals’ subjective SES may be related to their health because they are inclined to internalize perceptions of their place in socioeconomic hierarchies through the process of comparison inherent to social interaction. These perceptions, in turn, may be related to individuals’ health (Präg et al., 2016). Some scholars have found that there is a significant relationship between subjective SES and the health of older adults, where higher subjective SES is associated with better health outcomes (Ran et al., 2022). Hoebel and Lampert (2020) further emphasized that while both subjective SES and objective SES indicators are linked to health, they operate through different mechanisms. Moreover, longitudinal evidence also highlighted a reciprocal association between SSS and health-related quality of life, indicating the dynamic nature of this relationship (Euteneuer et al., 2021). Thus, it can be seen that subjective SES serves as a critical indicator within social stratification, which is associated with individuals’ health to some extent. Based on the above research, we proposed the following hypothesis:
The mediating role of aging anxiety
Aging anxiety can be defined as the combined concerns and fears regarding the aging process, including worries about declines in health, financial well-being, changes in appearance, and social losses (Lasher and Faulkender, 1993). Notably, aging anxiety is not exclusive to older adults; it is a lifespan construct relevant to adults of all ages. According to the terror management theory, awareness of aging and mortality is a fundamental human concern that manifests differently across developmental stages (Greenberg et al., 1986). Some scholars argued that the internalization of ageist stereotypes may exacerbate aging anxiety. Especially for young adults, internalizing these negative social views not only strains intergenerational relationships but also triggers serious concerns about their own future aging. Moreover, due to an inaccurate or limited understanding of the aging process, young people often hold stronger negative stereotypes (Barnett and Adams, 2018; Donizzetti, 2019). Consequently, aging anxiety is observable across the lifespan, often emerging in youth and peaking in middle age (Hummert, 1990).
The relationship between aging anxiety and health can be explained by stereotype embodiment theory. This theory holds that individuals assimilate ambient age stereotypes from their sociocultural environment across the lifespan, particularly associating aging with inevitable physical frailty, cognitive decline, and social dependency. Over time, these internalized negative beliefs transition from external societal views to internal self-definitions. Consequently, aging anxiety functions as a psychological response to these internalized threats, triggering physiological stress responses and maladaptive health behaviors that ultimately precipitate declines in health status—a phenomenon described as a self-fulfilling prophecy (Levy, 2009). Consistent with this theoretical framework, empirical research has confirmed that excessive aging anxiety can be linked to increased concern about one’s outward appearance, eating disorders, and fear of maturity, which can result in mental health issues (Mahoney, 2018). The findings by Brunton and Scott (2015) also indicated that higher levels of aging anxiety are associated with poorer health conditions. It has been widely recognized that excessive levels of anxiety can be negatively associated with an individual’s well-being and overall quality of life. Bergman and Segel-Karpas (2021) found that aging anxiety is positively associated with loneliness and depression in middle-aged adults, and high levels of aging anxiety are related to poorer physical health. In summary, much previous research has indicated that aging anxiety is associated with poorer health status. Therefore, we expect that aging anxiety may be negatively correlated with individuals’ health.
Previous studies have explored various predictors of aging anxiety, including social support (Ramírez and Palacios-Espinosa, 2016), frequency of contact with older adults (Yan et al., 2011), and knowledge of aging (Allan and Johnson, 2008). SES has consistently been identified as a critical predictor. Higher levels of objective SES, such as education and income, as well as positive perceptions of subjective SES, are significantly negatively correlated with aging anxiety (Yang and Ge, 2025). However, English et al. (2019) argued that compared with traditional objective indicators, subjective SES can better predict individuals’ subjective perceptions of aging. Their findings show that the higher the participants’ subjective SES, the more likely they were to have a positive attitude toward aging, a younger subjective age, a greater awareness of age-related gains, and a lower awareness of age-related losses. Individuals with lower subjective SES may experience higher levels of aging anxiety because they worry about being unable to support themselves or pay for healthcare after retirement. Conversely, individuals with high subjective SES usually have better educational backgrounds and social capital, which buffers against the fear of future aging through cognitive pathways and social support. Several studies have confirmed that subjective SES is significantly associated with an individual’s attitudes toward aging. For example, scholars have found that individuals with higher subjective SES in childhood exhibit lower levels of anxiety and depression (Morrongiello et al., 2015). Mochcovitch et al. (2016) found that high subjective SES, regular exercise, and the benefits of social security programs can reduce anxiety about aging. Kuball and Jahn (2024) further found that older individuals with initially low subjective SES or perceived downward mobility displayed the highest levels of aging anxiety and negative emotions. Consequently, we expect that subjective SES is negatively associated with aging anxiety.
Additionally, studies suggest that psychological risk factors may play a role in the relationship between subjective SES and health. For instance, Matthews et al. (2010) found that individuals with lower subjective SES experience increased negative emotions, which in turn are negatively related to health. Similarly, Cundiff et al. (2013) confirmed that social psychological vulnerability (e.g. neuroticism, depressive symptoms) mediates the association between subjective SES and self-rated health. Aging anxiety is not only a psychological perception of aging but a distinct emotional response that is linked to health outcomes. While other forms of anxiety may be associated with health, aging anxiety is uniquely positioned as a mediator because it is directly tied to how individuals perceive aging and their coping strategies in later life (Lynch, 2000). In the context of subjective SES, aging anxiety may exacerbate feelings of social exclusion or poor health perception, acting as a bridge between lower subjective SES and poorer multi-dimensional health outcomes. Aging anxiety is directly related to individuals’ self-perception and their engagement with social resources, which can mediate the relationship between subjective SES and health. Furthermore, aging anxiety helps explain why individuals in lower subjective SES groups may experience heightened vulnerability to health declines due to social and psychological factors specific to aging.
Based on the above discussion, we proposed the following hypothesis:
The moderating role of education
Although much empirical research has confirmed the positive association between education and health, the underlying mechanism is still unclear. There are two representative theories for exploring the relationship between education and health, namely, the budget constraint relaxation theory and the strengths reinforcement theory. The budget constraint relaxation theory argues that education relates to health by shaping an individual’s SES (Moen, 1999). From this perspective, education is a pathway to external resources. Chen et al. (2024) stated that education can foster better health outcomes by bolstering individual income. Raghupathi and Raghupathi (2020) found that adults with higher education levels have more employment opportunities, which is linked to better health status and longer life expectancy compared to their less-educated peers. In contrast, the strengths reinforcement theory emphasizes internal capabilities. It posits that the role of education in health creates a “Matthew effect,” namely that individuals with more social resources benefit more from educational achievement. Education can enable people to acquire human capital, which helps improve health (Mirowsky and Ross, 2005). Individuals with higher levels of education possess greater health literacy and stronger cognitive and adaptive abilities, which can enable them to choose healthier lifestyles and behaviors. Belo et al. (2020) observed that older adults with higher education levels are better equipped to regulate their psychological state, have a more positive attitude toward leisure, and can better perceive their physical changes, associated with better mental health.
Previous research indicates that aging anxiety is significantly associated with individuals’ health status; however, this association may depend on human capital. Although Bergman and Segel-Karpas (2021) identified ageism as a positive moderator in the relationship between aging anxiety and health in a sample of middle-aged adults, evidence regarding the moderating role of education remains limited. Studies have shown that individuals with higher education levels are more likely to adopt positive health management practices, such as regular exercise and maintaining healthy dietary habits, and access greater social support. These behaviors help buffer the negative association between aging anxiety and health (Seo and Noh, 2019). Additionally, highly educated individuals tend to view the aging process more positively, thus alleviating their anxiety about aging (Levy et al., 2002). This cognitive change makes education an important factor in buffering the negative associations between aging anxiety and health. Therefore, as an important socioeconomic factor, education may play a significant role in moderating the relationship between aging anxiety and individuals’ health. Accordingly, we formulated the following hypothesis:
Subjective SES, aging anxiety, and health are significantly related, with higher subjective SES linked to lower aging anxiety and better health outcomes. Based on the above research hypotheses, we further propose a moderated mediation model (Figure 1), that is, education may moderate the mediating effect of aging anxiety in the relationship between subjective SES and Chinese residents’ health. More specifically, individuals with a higher education level generally have a higher subjective SES, which can reduce their aging anxiety and promote their health status. Conversely, when they have a lower level of education, they also rate their subjective SES lower, which is associated with increased aging anxiety and poorer health outcomes. Thus, we expect that higher education levels are conducive to improving individuals’ subjective SES and reducing aging anxiety, which in turn is related to their health status. Accordingly, we proposed the following hypothesis:
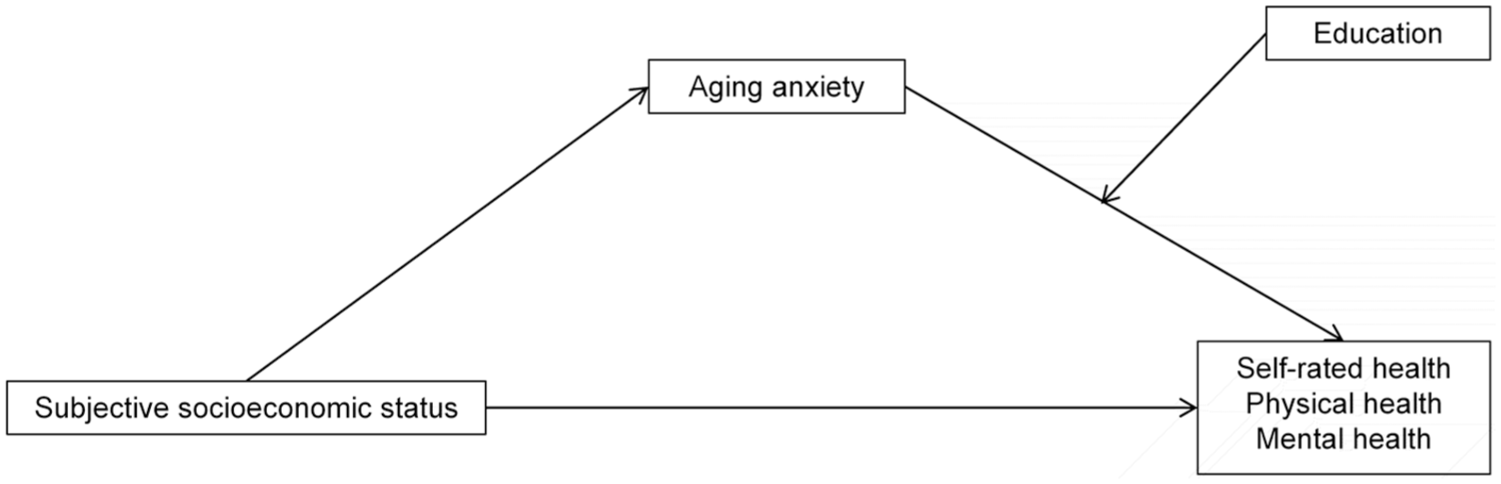
Research framework.
Materials and methods
Participants
This study is an empirical analysis based on data from the CGSS 2021. Launched as the first nationwide, comprehensive, and continuous academic survey in China, the CGSS employs multistage stratified sampling to cover diverse regions, urban and rural areas, and different demographic groups, analyzing the changes and evolution of China’s social structure. Specifically, the sampling process proceeded in four stages: (1) counties/districts were selected from all provinces using probability proportional to size (PPS) sampling; (2) within each selected county/district, townships/streets were sampled using PPS; (3) residential communities or villages were then sampled within each township/street; (4) households were randomly selected within each community/village, from which one adult aged 18 or older was randomly chosen from each household using the Kish grid method. As this study uses publicly available secondary data, Institutional Review Board ethical review and approval were not required. After selecting the target variables, we conducted data cleaning, including screening for missing values and outliers. We sorted the answer scores of the questions corresponding to each variable in descending order and excluded blank questionnaires as well as those with logically inconsistent or invalid responses, ultimately retaining 1913 valid samples.
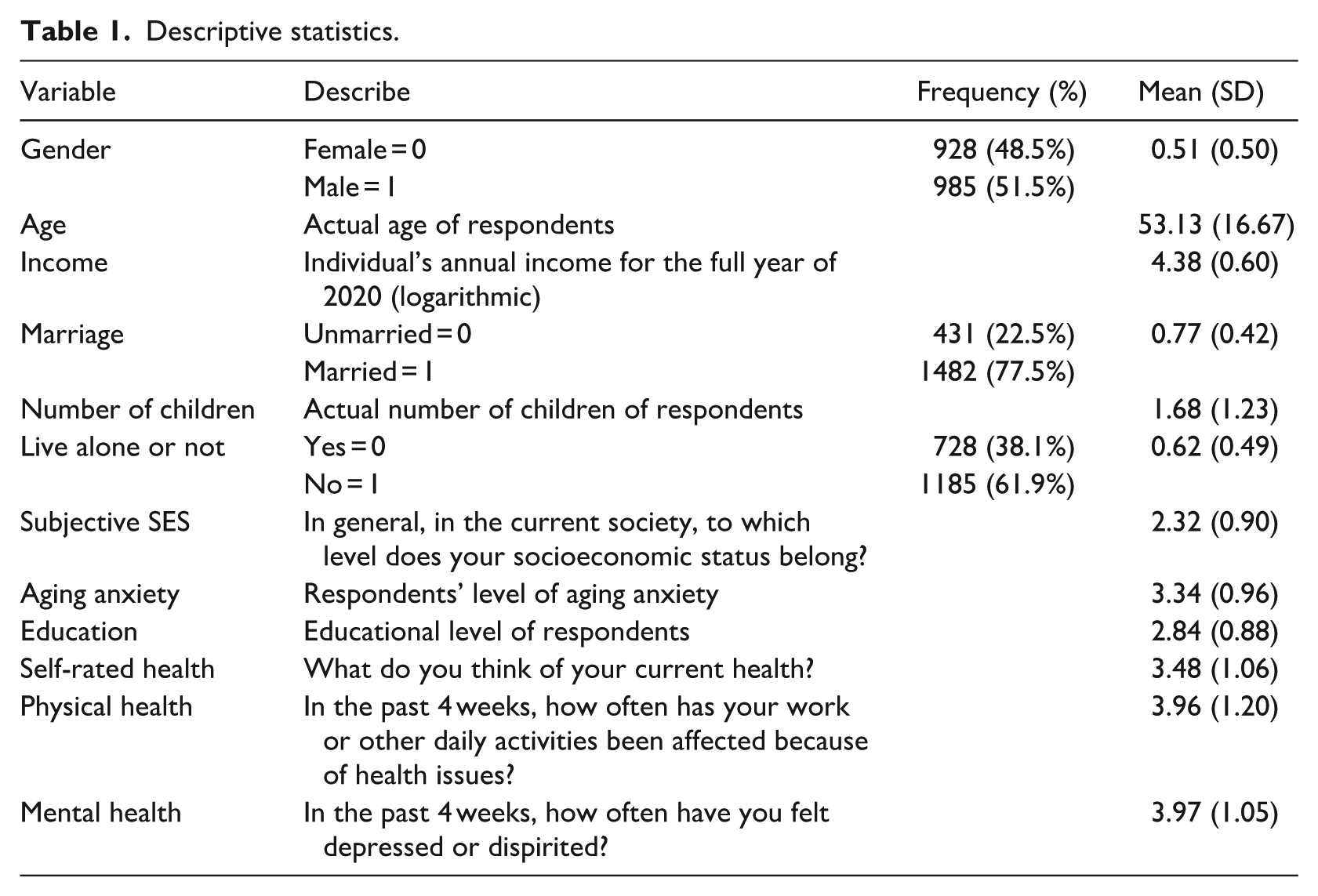
Table 1 presents the descriptive statistics of the sample. Of the total sample, 985 were male (51.5%) and 928 were female (48.5%), with ages ranging from 18 to 95 years (Mean = 53.13). The mean value of the logarithm of the annual personal income in 2020 was 4.38. The majority of respondents (77.5%) were married. Furthermore, the average number of children per respondent was 1.68. Approximately 38.1% of the respondents lived alone.
Descriptive statistics.
Measures
Health status
The dependent variable was health status, comprising three dimensions: self-rated health, physical health, and mental health. It is important to note that these variables represent respondents’ retrospective self-assessments rather than objective clinical indicators. Specifically, self-rated health was measured by the item: “What do you think of your current health?” Physical and mental health were assessed retrospectively based on the respondents’ experiences over the preceding month. Physical health was measured by asking: “In the past four weeks, how often has your work or other daily activities been affected because of health issues?” Similarly, mental health was measured by the item: “In the past four weeks, how often have you felt depressed or dispirited?” Each item was measured on a 5-point Likert scale that ranges from 1 to 5. All items were coded so that higher scores indicate better health status.
Subjective socioeconomic status
Subjective SES was assessed using the question: “In general, at which level does your socioeconomic status stand in the current society?” Participants provided their responses on a 5-point Likert scale, ranging from 1 (lowest) to 5 (highest). Higher scores indicate higher subjective SES.
Aging anxiety
The CGSS 2021 questionnaire includes three items adapted from the Aging Anxiety Scale (AAS), developed by Lasher and Faulkender in 1993, which encompasses dimensions such as fear of self-care, fear of losing the ability to make independent decisions, and fear of financial dependence (Lasher and Faulkender, 1993). The items “I’m worried that I won’t be able to take care of myself when I’m old,” “I’m worried that I’ll have to let others make decisions for me when I’m old,” and “Financial dependence on others is one of my biggest worries about aging” in the questionnaire are used to measure aging anxiety. Each item was rated on a 5-point Likert scale that ranges from 1 (strongly disagree) to 5 (strongly agree). Higher scores indicate higher levels of aging anxiety. The scale demonstrated acceptable internal consistency, with a Cronbach’s alpha coefficient of 0.764. Regarding validity, we conducted Principal Component Analysis (PCA) with Varimax rotation, and all factor loadings exceeded 0.5. Subsequently, a single-factor Confirmatory Factor Analysis (CFA) model was constructed. All fit indices met accepted psychometric criteria (χ2/df = 2.83, CFI = 0.981, TLI = 0.960, and RMSEA = 0.051). Given the brevity of the measure and the simplicity of a three-item one-factor model, these fit indices are reported descriptively and should be interpreted cautiously, serving as a basic check of unidimensional consistency rather than definitive evidence of broad construct validity.
Education
Education served as the moderating variable. We recoded it into a five-level ordinal variable (illiteracy = 1, primary school = 2, junior high school/high school/vocational school = 3, college and undergraduate = 4, graduate and above = 5).
Control variables
Control variables included gender, age, income, marriage, number of children, and live alone or not as control variables. Gender, marriage, and live alone or not were binary variables. Age and number of children were treated as continuous variables. Income represented the respondent’s total annual income from the previous year. To facilitate data processing and address potential skewness, we log-transformed income.
Results
Correlation analysis
Table 2 presents the correlation coefficients of the variables used in this study. The results showed that subjective SES was significantly and positively correlated with self-rated, physical, and mental health (r = 0.207, r = 0.138, r = 0.174, all p < 0.01). There was a significant and negative correlation between subjective SES and aging anxiety (r = −0.173, p < 0.01). Aging anxiety was significantly and negatively associated with self-rated, physical, and mental health (r = −0.151, r = −0.161, r = −0.177, all p < 0.01), respectively. Moreover, education was significantly and positively associated with self-rated, physical and mental health (r = 0.251, r = 0.262, r = 0.150, all p < 0.01). A significant negative correlation was also found between aging anxiety and education (r = −0.086, p < 0.01).
Correlations among the study variables.
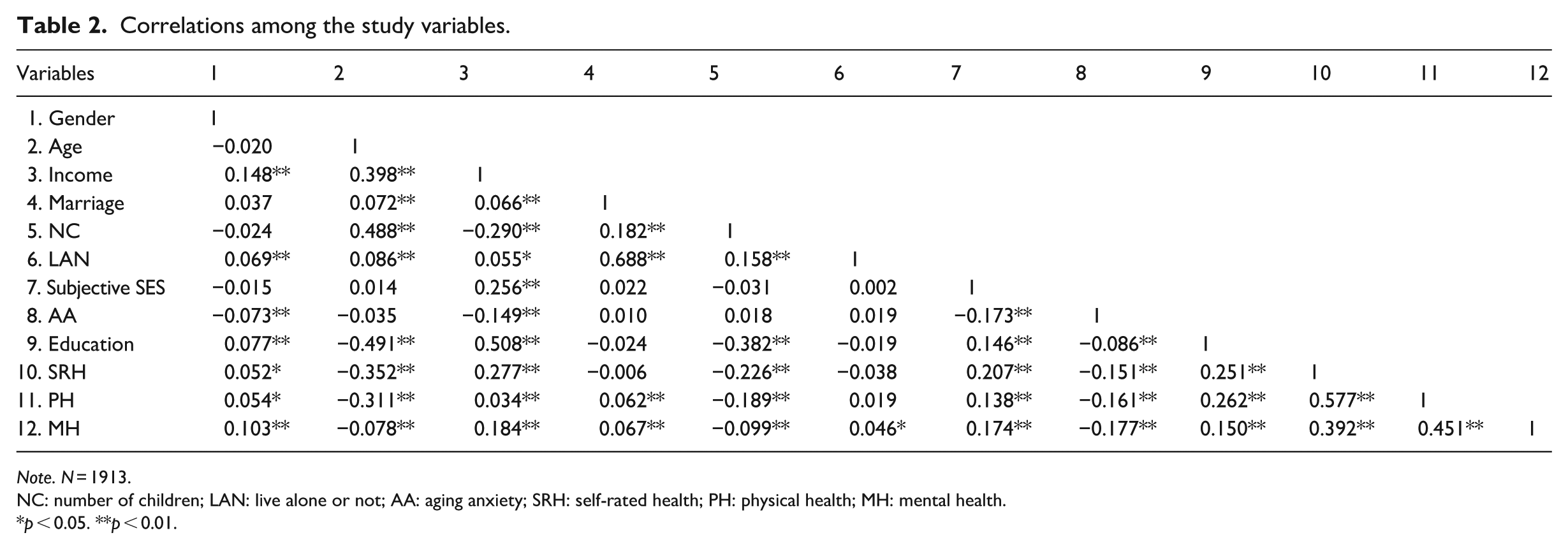
Note. N = 1913.
NC: number of children; LAN: live alone or not; AA: aging anxiety; SRH: self-rated health; PH: physical health; MH: mental health.
p < 0.05. **p < 0.01.
Hypothesis tests
Before conducting the regression analysis, we performed diagnostic tests to ensure that the assumptions of ordinary least squares (OLS) regression were met. Collinearity tests showed that the Variance Inflation Factor (VIF) for all independent variables ranged from 1.06 to 1.94, well below the conservative threshold of 2.5, indicating no multicollinearity among the variables. Furthermore, visual inspections of the residual plots and normal P-P plots confirmed that the assumptions of homoscedasticity and residual normality were not severely violated. To examine the relationship between subjective SES and individuals’ health, we estimated baseline regression models. As shown in Models 1, 3, and 5 in Table 3, subjective SES was significantly and positively associated with self-rated, physical, and mental health (b = 0.217, 0.127, 0.170; β = 0.184, 0.095, 0.146, all p < 0.001). Consequently, hypotheses 1a, 1b, and 1c were supported.
Results of benchmark regression and robustness tests.
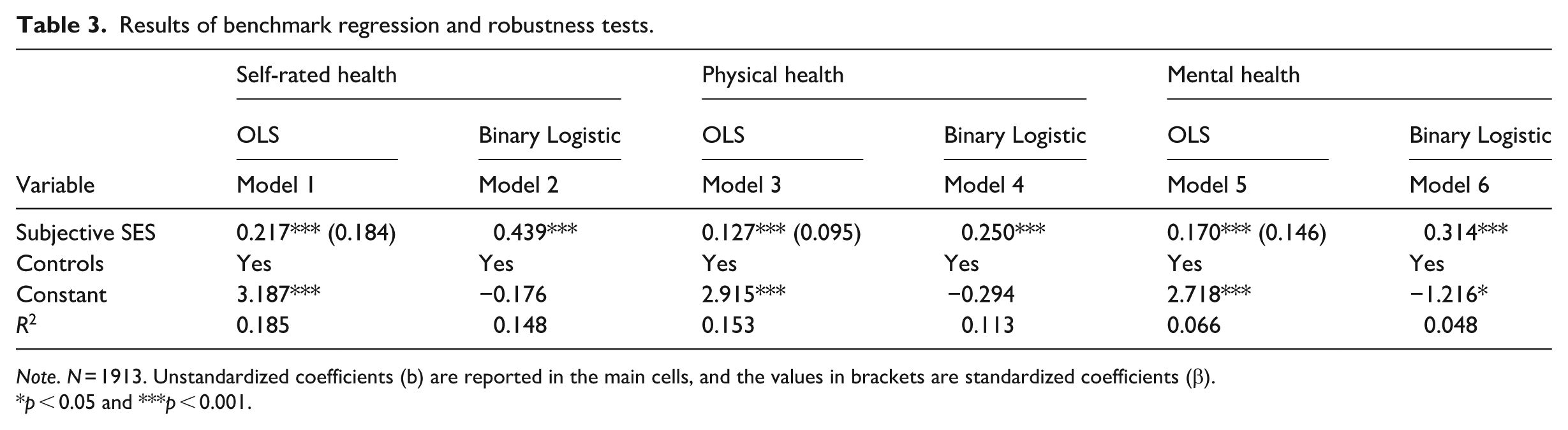
Note. N = 1913. Unstandardized coefficients (b) are reported in the main cells, and the values in brackets are standardized coefficients (β).
p < 0.05 and ***p < 0.001.
For robustness testing, we recoded the dependent variables (self-rated, physical, and mental health) into binary variables and employed binary logistic regression models. Specifically, responses of “very unhealthy,” “unhealthy,” and “average” were coded as 0, while “healthy” and “very healthy” were coded as 1. The findings indicated that subjective SES maintained significant and positive associations with self-rated, physical, and mental health (b = 0.439, b = 0.250, b = 0.314, all p < 0.001). These results were consistent with the baseline findings and further supported hypotheses 1a, 1b, and 1c.
To examine the mediating role of aging anxiety, we employed the PROCESS macro for SPSS to estimate the 95% confidence intervals of the mediating effects. Model 1 in Table 4 reveals that subjective SES was significantly and negatively associated with aging anxiety (b = −0.146, p < 0.001). The results in Models 3, 5, and 7 showed that aging anxiety was negatively associated with self-rated, physical, and mental health (b = −0.128, b = −0.164, b = −0.150, all p < 0.001), respectively. After adding aging anxiety to the regression equation, subjective SES remained significantly related to self-rated, physical, and mental health (b = 0.199, b = 0.103, b = 0.148, all p < 0.001). These findings indicated that aging anxiety partially mediated the association between subjective SES and self-rated (b = 0.019, 95% CI: [0.010, 0.029]), physical (b = 0.024, 95% CI: [0.014, 0.036]), and mental health (b = 0.022, 95% CI: [0.012, 0.034]). Therefore, hypotheses 2a, 2b, and 2c were supported.
Results of the mediating role test for aging anxiety.
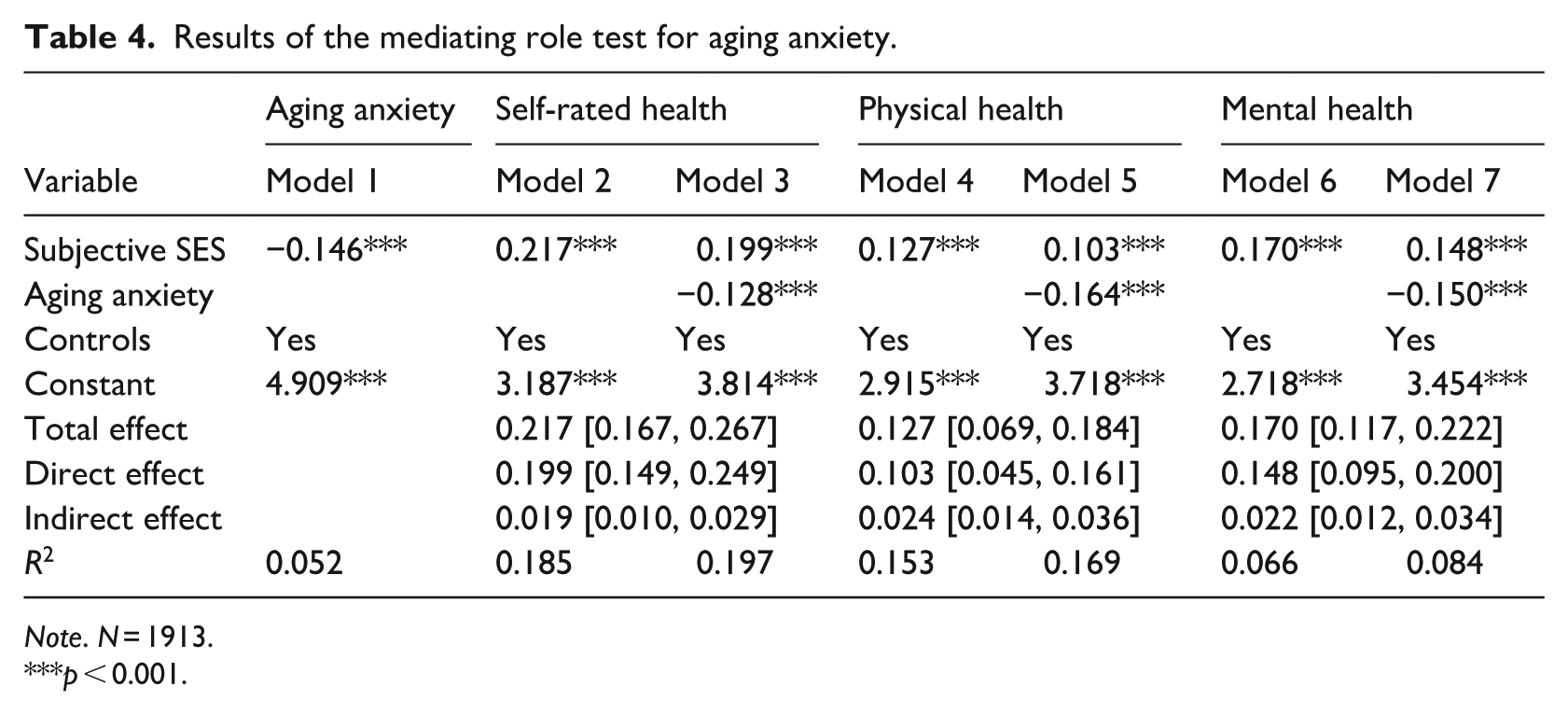
Note. N = 1913.
***p < 0.001.
To test whether the mediating role of aging anxiety varied across different age groups, this study divided the sample into three groups: young adults (18–44 years old), middle-aged adults (45–64 years old), and older adults (aged 65 and above) for separate analysis. As shown in Table 5, in the middle-aged and older adult groups, aging anxiety significantly mediated the relationship between subjective SES and self-rated (b = 0.018, 95% CI: [0.005, 0.036]; b = 0.033, 95% CI: [0.011, 0.059]), physical (b = 0.014, 95% CI: [0.000, 0.033]; b = 0.050, 95% CI: [0.021, 0.086]), and mental health (b = 0.021, 95% CI: [0.007, 0.040]; b = 0.029, 95% CI: [0.010, 0.055]). However, in the young adult group, the mediating effect of aging anxiety was not significant.
Results of the mediating role test for aging anxiety across different age groups.
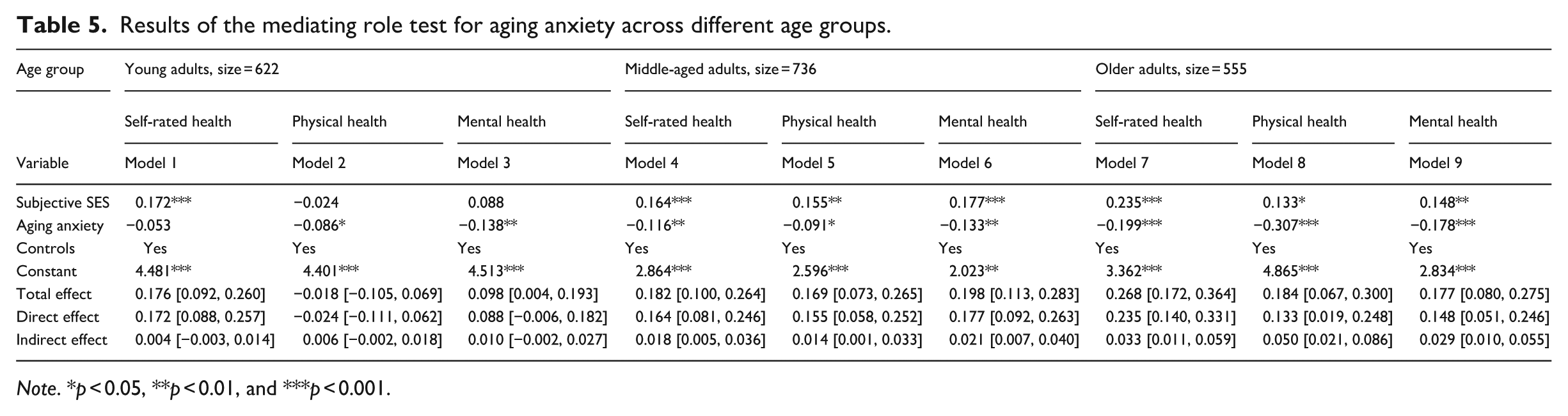
Note. *p < 0.05, **p < 0.01, and ***p < 0.001.
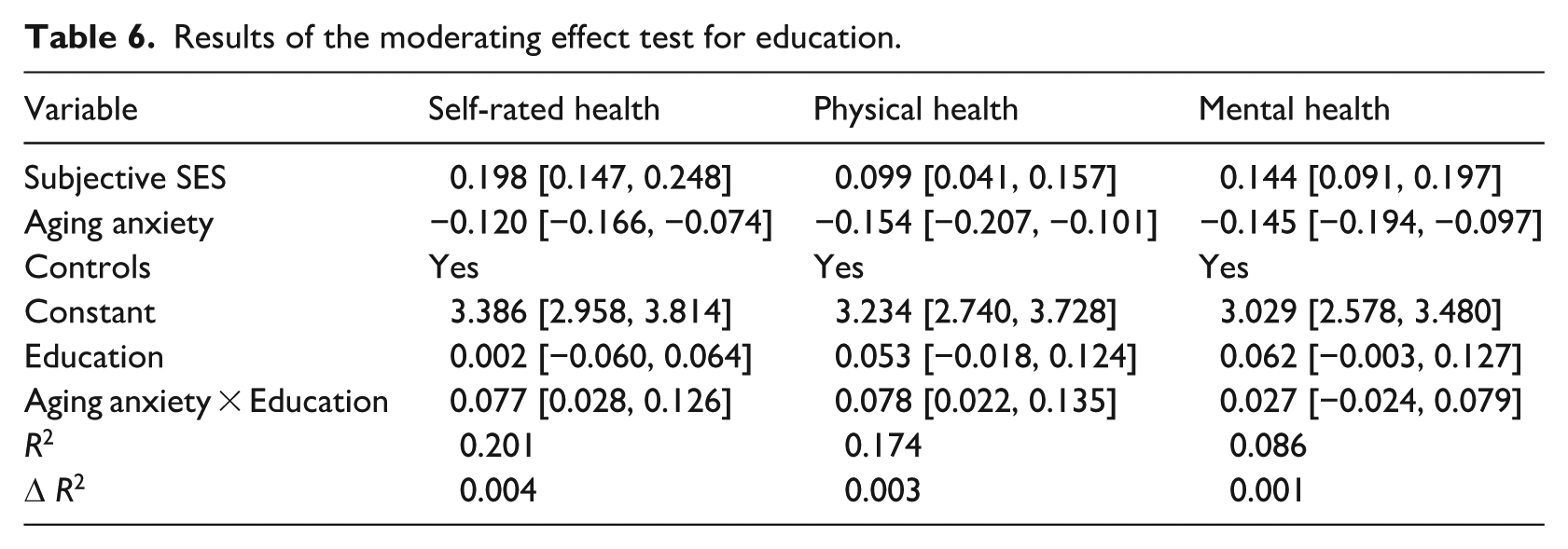
Table 6 shows that aging anxiety was significantly and negatively associated with self-rated (b = −0.120, 95% CI: [−0.166, −0.074]) and physical health (b = −0.154, 95% CI: [−0.207, −0.101]). Moreover, the interaction between aging anxiety and education was significantly and positively associated with self-rated (b = 0.077, 95% CI: [0.028, 0.126]) and physical health (b = 0.078, 95% CI: [0.022, 0.135]). To visualize this pattern, we plotted the simple slopes of aging anxiety on health outcomes at education levels 2, 3, and 4 (primary school; junior/high/vocational; and college/undergraduate). As illustrated in Figures 2 and 3, while aging anxiety negatively predicted health scores across all groups, the negative slopes became noticeably flatter for respondents with higher educational attainment (education = 4) compared to those with lower attainment (education = 2). These findings indicated that education buffered the adverse associations between aging anxiety and both self-rated and physical health. Therefore, hypotheses 3a and 3b were supported. However, the interaction between aging anxiety and education showed no significant association with mental health; thus, hypothesis 3c was not supported.
Results of the moderating effect test for education.
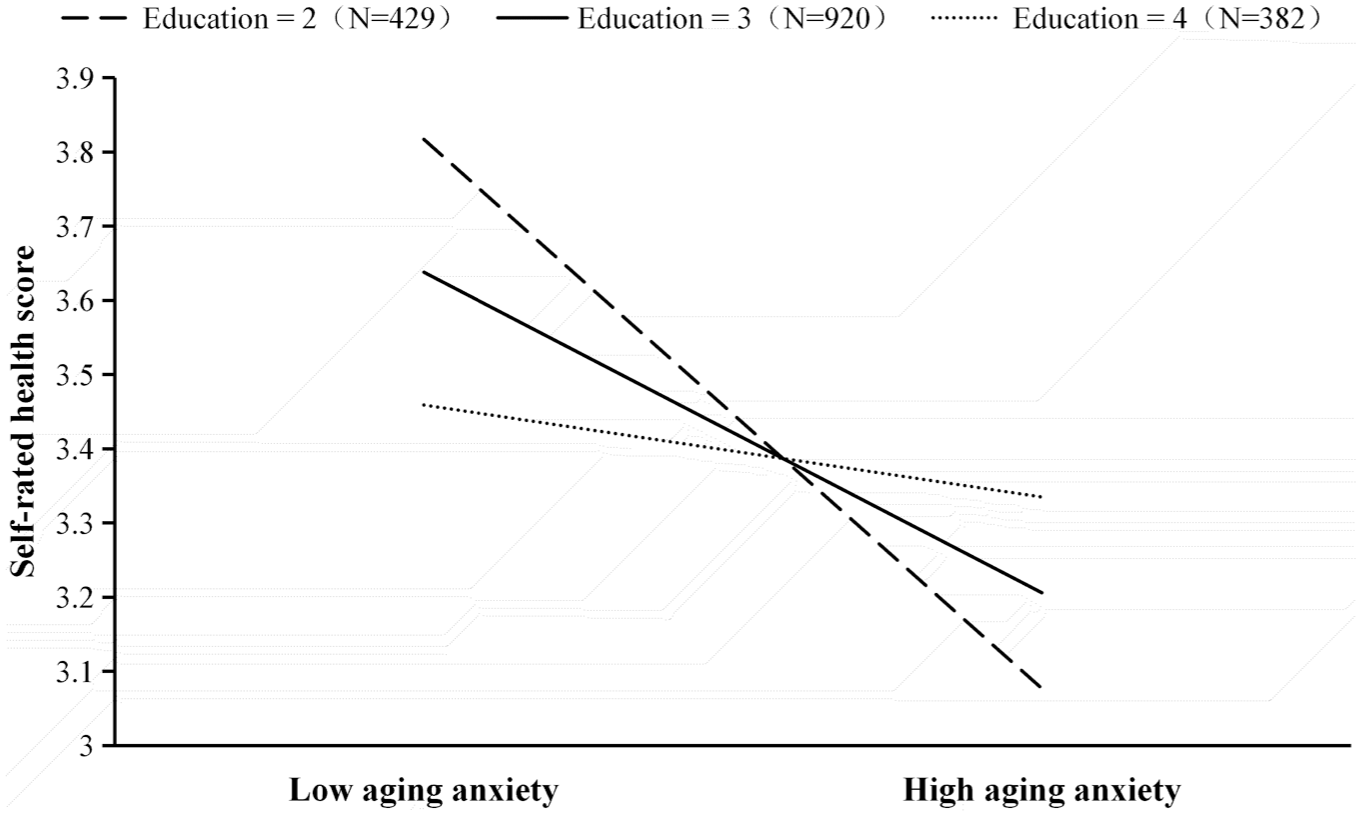
Interaction plot of aging anxiety and education for self-rated health.
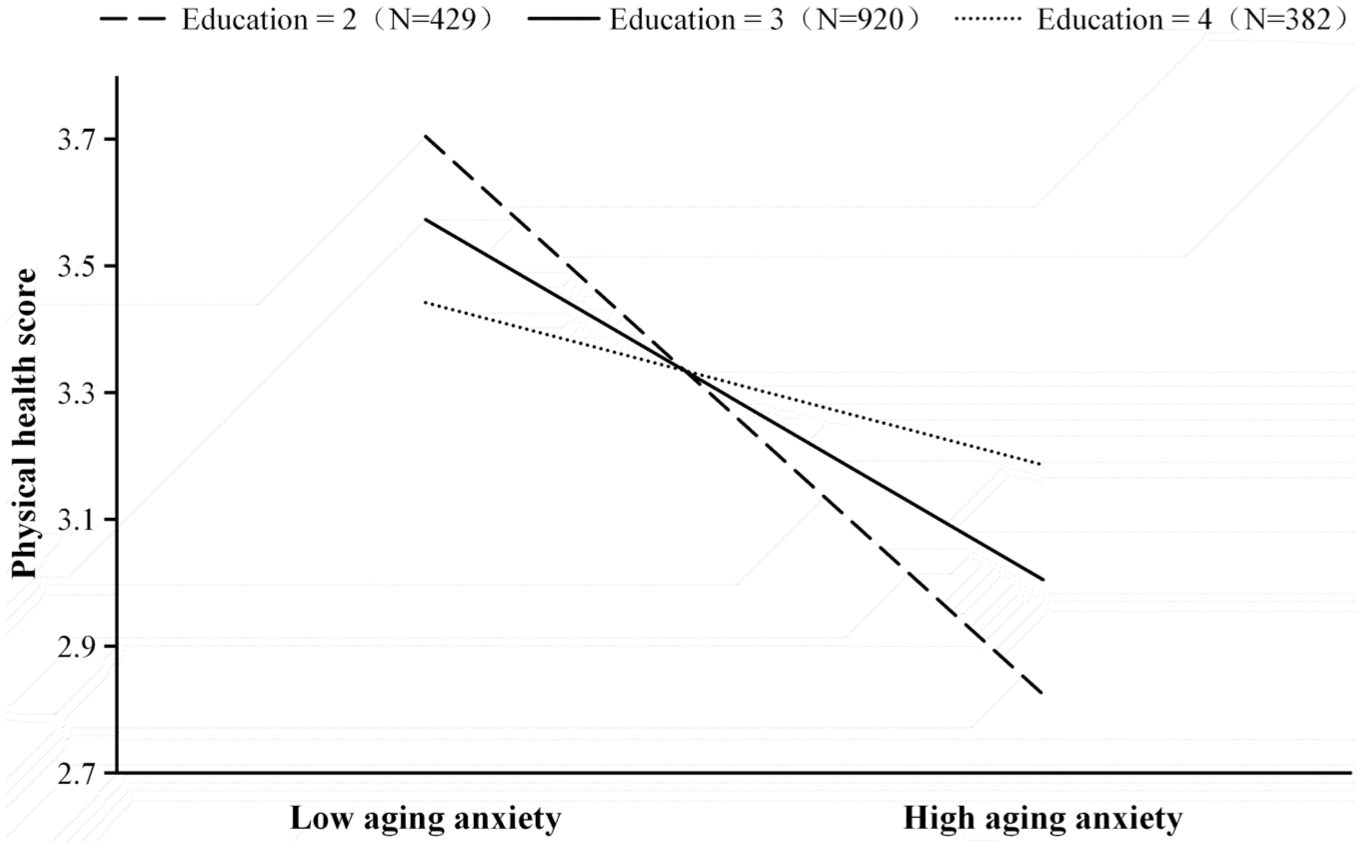
Interaction plot of aging anxiety and education for physical health.
We examined the moderated mediation effect at three observed education levels (education = 2, 3, and 4). As shown in Table 7, for self-rated health, the conditional indirect effects of subjective SES on self-rated health via aging anxiety were significant at education = 2 (b = 0.027, 95% CI [0.014, 0.042]) and education = 3 (b = 0.016, 95% CI [0.008, 0.025]), but not significant at education = 4 (b = 0.004, 95% CI [−0.008, 0.016]). The indirect effect decreased as education increased. Moreover, the index of moderated mediation was also significant (index = −0.011, 95% CI [−0.022, −0.003]), indicating that the indirect effect of subjective SES on self-rated health through aging anxiety was moderated by education. Therefore, hypothesis 4a was supported.
Results for the index of moderated mediation and conditional indirect effects.
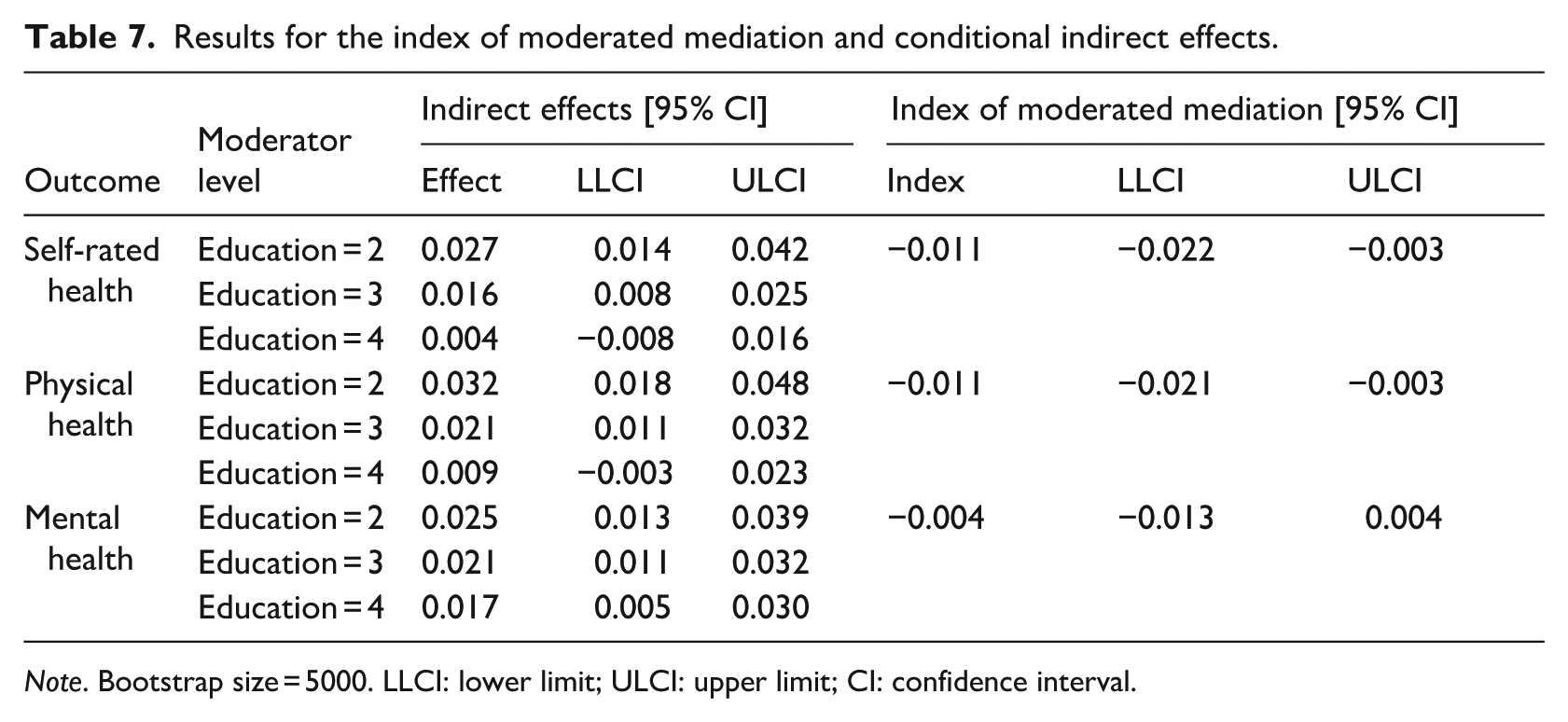
Note. Bootstrap size = 5000. LLCI: lower limit; ULCI: upper limit; CI: confidence interval.
For physical health, the conditional indirect effects were significant at education = 2 (b = 0.032, 95% CI [0.018, 0.048]) and education = 3 (b = 0.021, 95% CI [0.011, 0.032]), but not at education = 4 (b = 0.009, 95% CI [−0.003, 0.023]). The index of moderated mediation was also significant (index = −0.011, 95% CI [−0.021, −0.003]), indicating that education significantly moderated the indirect path from subjective SES to physical health through aging anxiety. Therefore, hypothesis 4b was supported. However, for mental health, the index of moderated mediation was not significant; thus, hypothesis 4c was not supported. Importantly, as detailed in Table 7, the conditional indirect effects for mental health remained statistically significant across all three observed education levels. This indicates that while aging anxiety robustly mediates the relationship between subjective SES and mental health for all respondents, the strength of this specific mediated pathway does not significantly vary with educational attainment.
Robustness check for multiple comparisons
Because the three health indicators were analyzed as parallel dimensions of multidimensional health, to control for the family-wise error rate across our three dependent variables, we additionally applied a Bonferroni correction for multiple comparisons, using an adjusted significance threshold of α = 0.017. Under this more conservative criterion, the core full-sample results remained substantively unchanged. This confirms that our findings are highly robust and not merely artifacts of multiple testing.
Discussion
This study investigated the relationship between subjective SES and the multidimensional health of Chinese residents, as well as the underlying mechanisms of this relationship. First, the results demonstrated that subjective SES was significantly and positively associated with Chinese residents’ self-rated, physical, and mental health, aligning with previous research (Ran et al., 2022).
Second, the findings revealed that aging anxiety partially mediated the relationships between subjective SES and self-rated, physical, and mental health. Additionally, subgroup analyses indicated significant age-related differences in this mechanism. Specifically, the mediating role of aging anxiety was evident primarily among middle-aged and older adults, but not among young adults. This suggests that the significant mediation effects observed in the total sample were primarily driven by the robust signal from middle-aged and older adults. Consequently, including young adults in the main analysis provided a conservative estimate of the mediation effect, as the “non-responsive” younger group likely diluted the overall effect size. Importantly, the correlation between age and aging anxiety was near zero. Therefore, the age-group differences observed here are more plausibly explained by differences in relationship structure rather than differences in levels of aging anxiety across age groups. From a life course perspective, middle-aged and older adults are at stages where aging becomes a more consequential personal and social issue. Physiological decline, role transitions, and increased visibility of age-related stereotypes may strengthen the linkage between aging anxiety and current health status. Consequently, for these groups, individuals with lower subjective SES are more likely to experience heightened aging anxiety, which is associated with poorer health. In contrast, although young adults also experience aging anxiety, their concerns are typically more anticipatory, focusing on future possibilities (e.g. loss of attractiveness or financial independence) rather than immediate physiological decline. Accordingly, these distal concerns may be less strongly associated with their current health status. This finding addresses a critical concern regarding sample composition: while aging anxiety is theoretically measurable in young adults, it does not yet function as a proximal correlate of health for them to the same extent as in middle-aged and older adults.
We acknowledge that although the mediating role of aging anxiety was statistically significant (p < 0.001), the effect sizes were modest. As shown in Table 4, the indirect effects ranged from 0.019 to 0.024 across the three health outcomes. To ensure valid cross-outcome comparisons given the differing response scale variances of our health measures, we computed the proportion of the total effect mediated using fully standardized coefficients. Specifically, based on these standardized effects, the approximate proportion mediated by aging anxiety was 8.7% for self-rated health, 13.0% for mental health, and 18.9% for physical health. Given the large sample size, these results warrant cautious interpretation to distinguish between statistical detectability and practical importance. Nevertheless, we contend that these findings hold meaningful practical significance within the context of social epidemiology. First, health outcomes are multifactorial, determined by a complex interplay of genetics, lifestyle, and medical resources. Subjective SES is a distal determinant that is linked to health through numerous downstream pathways. It is theoretically expected that aging anxiety, as a specific psychological mechanism, would capture only a portion of this broad association, rather than explaining the entirety of the subjective SES-health gradient. Second, from a population health perspective, even small effect sizes can have substantial societal impacts when applied to a massive demographic. In the context of China’s rapidly aging population, identifying aging anxiety as a modifiable psychological pathway is crucial. Unlike structural socioeconomic factors which are difficult to alter, aging anxiety is amenable to psychological intervention. Therefore, even a modest role in the relationship between subjective SES and health via this specific psychological pathway could translate into significant improvements in quality of life for millions of older adults.
Third, the results indicated that education attenuated the negative associations between aging anxiety and self-rated and physical health. However, education did not moderate the association between aging anxiety and mental health. One possible explanation is that individuals with higher education typically possess stronger cognitive abilities, enabling them to rationally interpret the physiological process of aging and thus alleviate aging-related fears and concerns (Allan and Johnson, 2008). However, affective and cognitive responses represent distinct domains. While education can strengthen cognitive appraisal and problem-solving abilities, affective responses, including emotional distress and depressive symptoms, are frequently influenced by factors such as personality traits, life experiences, and cultural background. Aging anxiety encompasses both cognitive and emotional components, and the emotional experience of aging may not be fully mitigated through cognitive resources or educational interventions alone. Therefore, education may have a strong association with individuals’ rational understanding and health management behaviors but a relatively limited moderating effect on the emotional aspects of aging anxiety. Crucially, these findings persisted even after controlling for income and other covariates. Therefore, these results are more consistent with the strengths reinforcement theory, suggesting that education may enhance individuals’ ability to rationally interpret the aging process and engage in healthy behaviors, thereby reducing the negative correlation between aging anxiety and health.
Furthermore, the indirect effects of subjective SES on self-rated and physical health through aging anxiety were also moderated by education. Although education is widely recognized as a significant determinant of health, relatively little attention has been paid to its moderating role in the relationship between subjective SES and health. These findings underscore the importance of considering both cognitive and affective pathways when examining how education is related to health in the context of aging anxiety.
Theoretical implications
This research makes several theoretical contributions. First, prior research has largely emphasized the link between objective SES and health, whereas little attention has been paid to the direct association between subjective SES and health. By examining subjective SES alongside three distinct dimensions of health, our study not only extends the empirical evidence on the subjective SES-health relationship but also moves beyond the single-outcome focus common in earlier work. Consequently, our study enriches the literature on the relationship between subjective SES and individuals’ health within the Chinese context.
Second, our study deepens the understanding of the underlying mechanisms linking subjective SES to the Chinese residents’ health. Although previous research has examined the associations among aging anxiety, subjective SES, and health (Yang and Ge, 2025), few studies have systematically investigated the specific mediating pathways within this framework. By explicitly identifying the mediating role of aging anxiety across self-rated, physical, and mental health, this study extends the literature on aging anxiety within the Chinese context.
Third, our research reveals that education attenuates the negative relationships between aging anxiety and both self-rated and physical health. While previous studies have mostly examined the direct association of aging anxiety on individuals’ health, the boundary conditions of this relationship remain largely unexplored. To date, only one study has examined the moderating role of ageism in this context (Bergman and Segel-Karpas, 2021). Therefore, our study contributes to the literature on aging anxiety by testing the moderating role of education in the above relationships.
Practical implications
Despite the limitations of a cross-sectional design, which precludes strict causal inference, our findings highlight several areas warranting policy attention pending longitudinal or experimental confirmation. First, the positive association between subjective SES and Chinese residents’ health suggests that addressing perceived socioeconomic disparities could be beneficial. While broader macroeconomic interventions, such as labor market restructuring, are beyond the scope of this survey, our results suggest that targeted community support for low-income families may help promote overall health outcomes. Ensuring equitable access to basic medical care, community education, and housing protection also remains essential. Pending stronger causal evidence, such measures may not only alleviate objective deprivation but also improve individuals’ subjective perception of their SES, thereby potentially benefiting their quality of life and health.
Second, because aging anxiety is negatively associated with health outcomes, psychosocial interventions that help individuals manage aging-related worries merit consideration. Expanding access to mental health and counseling services, particularly for older adults, may be one practical direction. Community-based service networks and structured emotional-support activities could help reduce psychological stress and ease aging-related anxiety. In addition, public communication that promotes positive aging and challenges age-related stereotypes may foster a stronger sense of social recognition and belonging.
Finally, given the finding that education buffers the negative relationship between aging anxiety and health, cognitive and informational resources may help mitigate the health implications of aging anxiety. While formal education levels are difficult to alter in later life, policies could aim to mimic this protective effect through lifelong learning initiatives. Continued investment in community educational resources, especially targeting vulnerable groups, is an area for future exploration. Fostering the development of community health education centers and organizing health seminars could empower residents with the knowledge to navigate aging processes more rationally. Ultimately, these efforts may help to elevate overall health literacy, thereby providing the cognitive resources necessary to counteract the adverse effects of aging anxiety.
Limitations and future research
Despite the contributions of this study, several limitations should be acknowledged. First, this study relied on a cross-sectional design, which precludes strict causal inferences. While our model is grounded in theoretical frameworks, we cannot rule out the possibility of reverse causality. Therefore, future studies should utilize longitudinal or panel data to rigorously establish the causal directionality between subjective SES and health. Second, the use of secondary data imposed specific measurement constraints. Some potential confounders could not be included in the research model. More critically, physical and mental health were assessed using single-item retrospective self-assessments rather than multi-item validated clinical scales (e.g. ADL, IADL, or CES-D). While single-item measures are common in large-scale sociological surveys, they generally possess lower reliability than standardized composite instruments. The measurement error inherent in such indicators tends to introduce attenuation bias, suggesting that our study might have underestimated the true strength of the relationships among subjective SES, aging anxiety, and health. Similarly, we acknowledge a potential floor effect in our measurement of subjective SES. The mean subjective SES was 2.32 (SD = 0.90) on a 1–5 scale, which suggests that responses were concentrated toward the lower end. This restricted variance could further attenuate the observed associations between subjective SES and health. Furthermore, the reliance on subjective, retrospective self-assessments lacks objective clinical verification and may introduce systematic biases, such as recall bias or the influence of the respondent’s transient mood. Consequently, the observed effect sizes should be interpreted as conservative estimates. Additionally, aging anxiety was operationalized using the three AAS-derived items available in CGSS, which primarily reflect dependence-related worries. This abbreviated measure does not capture the full multidimensional content of the original AAS; therefore, the findings may not fully generalize to the broader, multidimensional construct of aging anxiety. Future research should prioritize longitudinal designs incorporating clinical-grade psychometric tools to validate these associations with greater precision. Third, while our overall sample size provided excellent statistical power (estimated at 0.990) for the primary significant models, Monte Carlo sensitivity analyses revealed power constraints for specific pathways. Specifically, the power to detect the extremely small index of moderated mediation for mental health was 0.762, and the young adult subgroup was severely underpowered (power ranging from 0.021 to 0.147). Consequently, the non-significant findings in these specific instances cannot be definitively interpreted as a theoretical absence of effects, as they may simply reflect Type II errors. Future research with larger, targeted cohorts is necessary to further investigate these specific mechanisms. Finally, the findings are grounded in the Chinese sociocultural context, which is different from Western individualistic societies. Chinese culture emphasizes filial piety, viewing aging not merely as an individual biological decline but as a transition deeply embedded in family dynamics. Consequently, aging anxiety in China may be uniquely exacerbated by the cultural pressure of becoming a burden to the family or the perceived erosion of traditional family support systems. Furthermore, the cultural emphasis on social hierarchy may amplify the psychological sensitivity to subjective SES, thereby influencing how status is associated with health differently than in egalitarian cultures. Therefore, caution is warranted when extrapolating these results to non-Chinese populations. Cross-cultural comparative research is needed to dissect how differing cultural beliefs and social stratification systems shape the mechanisms linking aging anxiety and health.
Footnotes
Ethical considerations
The data used in this study was a survey conducted by the authoritative institution Renmin University of China. All participants were informed to complete the survey confidentially and anonymously. Based on this background, ethical review and approval was not required for this kind of study in China.
Consent to Participate
Consent to participate was obtained from all participants by the CGSS survey team before data collection. The present study used anonymized, publicly available secondary data and did not involve direct contact with participants.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
ZX-H: Conceptualization, Writing—original draft, Formal analysis. YP-Y & JC-L: Methodology, Formal analysis, Writing—original draft. KP-G: Conceptualization, Writing—original draft, Project administration, Writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Social Science Fund of China [23CSH060].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Preregistration
Because this study involves a secondary analysis of a pre-existing, publicly available dataset (CGSS 2021), the study design and analysis plan were not preregistered.