
Abstract
Nomophobia is an increasing concern among medical students, yet the psychophysiological mechanisms linking sleep disturbances to this maladaptive health behavior remain insufficiently understood. Guided by the I-PACE model, this study examined whether stress, anxiety, and depression mediate the correlation between insomnia and nomophobia, conceptualizing insomnia as a physiological vulnerability factor. This cross-sectional study included 201 medical students (38.3% preclinical phase and 61.7% clinical phase). Participants completed the Nomophobia Questionnaire, Depression Anxiety Stress Scales, and Insomnia Severity Index. Parallel mediation analysis revealed that although insomnia was correlated with all distress variables, stress emerged as the only significant unique mediator, indicating an indirect-only mediation pattern. Anxiety and depression showed non-significant effects due to statistical suppression, and a reverse model yielded no significant indirect effects. These findings suggest that insomnia contributes to nomophobia primarily through heightened stress, underscoring the importance of sleep hygiene and stress regulation in preventive health interventions for medical students.
Keywords
Introduction
Nomophobia (no mobile phone phobia) is defined as the fear or anxiety of being separated from one’s smartphone and is increasingly conceptualized in the literature as a maladaptive coping-related behavior, particularly among young adults (Zwilling, 2022). Given that smartphone addiction shares neurobiological and behavioral commonalities with established compulsive behaviors (Montag and Reuter, 2015), nomophobia is increasingly viewed as a marker of difficulties in behavioral regulation (Oraison and Wilson, 2024). Individuals with high nomophobia levels typically exhibit low tolerance for uncertainty and impaired attention processes (Ercengiz et al., 2024), characteristics that can impact functioning in cognitively demanding environments such as medical education (Ward et al., 2017).
Medical students represent a distinct high-risk group due to the unique nature of their training, which is characterized by heavy academic loads, clinical shifts, and chronic sleep deprivation (Almojali et al., 2017; Kubrusly et al., 2021). While smartphones are essential tools for accessing clinical information, this functional necessity often blurs the line between utility and dependence (Agostini and Petrucco, 2023). Studies consistently report high rates of problematic phone use among medical students, linking it to poor sleep quality and academic burnout (Akbaş Güneş and Gücük, 2020; Baykan et al., 2021). However, the specific mechanisms linking physiological dysregulation—such as insomnia—to nomophobia remain complex and not fully disentangled.
Within a health psychology perspective, the I-PACE (Interaction of Person–Affect–Cognition–Execution) model provides a useful lens to conceptualize how psychophysiological vulnerability (e.g. insomnia) interacts with affective stress responses to shape maladaptive health-related coping behaviors (Brand et al., 2019). According to this framework, sleep deprivation functions not merely as a consequence but as a fundamental physiological stressor that depletes cognitive resources and impairs emotional regulation (Baglioni et al., 2016). When experiencing emotional distress, individuals may utilize smartphones as a maladaptive coping mechanism; while this provides short-term comfort, it reinforces a self-perpetuating pattern of dysregulated use rather than effective stress management (Caba-Machado et al., 2024; Gnardellis et al., 2023).
While stress has been frequently highlighted as a key correlate in the emergence of nomophobia, evidence suggests that sleep disorders play a specific role in the psychophysiological profile of this phenomenon (Daraj et al., 2023; Jahrami, 2023). In medical students, poor sleep hygiene and late-night phone use can create a bidirectional pattern that exacerbates both stress and phone dependency (Gunasekar et al., 2025; Teker and Yakşi, 2021). Although depression is distinct from anxiety, it often co-occurs in high-stress academic environments and may reflect avoidance-based coping patterns of smartphone overuse (Elhai et al., 2018). Furthermore, previous literature often reports stress, anxiety, and depression as a cluster of symptoms, making it difficult to distinguish which of these emotional states is the primary driver of nomophobia when insomnia is present.
Regarding potential confounding factors, relevant sociodemographic and health-related characteristics were considered, given their potential associations with both technology use behaviors and sleep-related outcomes. Previous studies have shown that these factors may influence levels of nomophobia and related psychological symptoms, although findings remain inconsistent (Bano et al., 2021). In addition, emerging evidence suggests that general health indicators may also be linked to sleep disturbances and sedentary behaviors, including excessive smartphone use (Gunasekar et al., 2025). These considerations highlight the importance of accounting for such variables in order to better isolate the specific contribution of psychological factors (Salk et al., 2017).
Accordingly, the primary aim of this study is to clarify the relative statistical contributions of stress, anxiety, and depression in the relationship between insomnia and nomophobia among medical students.
Hypotheses: Based on the I-PACE framework:
Materials and methods
Research design and sample size
This study employed a cross-sectional, correlational research design and was conducted among students at the Faculty of Medicine, Karadeniz Technical University. The study was approved by the Institutional Ethics Committee Decision No: 24237859-23, Date: 15.01.2025. In addition to ethical approval, written institutional permission was obtained from the dean’s office of the faculty of medicine to conduct the study within academic and clinical training settings. Between March and July 2025, the researcher visited the faculty of medicine, various departments of affiliated hospitals, and training classes at these hospitals to inform students about the study. To control for the potential confounding effects of academic scheduling, data collection was conducted during regular lecture weeks, explicitly avoiding mid-term and final examination periods. Additionally, participants completed the online questionnaires at a time and in an environment of their own choosing. Before the questionnaires were completed, the aims, procedures, potential risks, and benefits of the study were clearly explained to all participants. Participants were informed that participation was voluntary and that they had the right to withdraw from the study at any time without penalty. All data were collected anonymously to ensure participant confidentiality; therefore, individual follow-up for participants reporting elevated levels of distress was not possible. In line with ethical standards, participants were provided with a debriefing statement at the end of the survey, which included information about available psychological counseling services at the university.
The sample size was determined based on a power analysis performed using G*Power 3.1.9.2 software. In line with similar studies in the literature examining the relationship between nomophobia and psychological distress (Kubrusly et al., 2021), a medium effect size (f2 = 0.15), 90% power (1−β = 0.90), and α = 0.05 significance level were accepted. Based on a multiple regression model accounting for insomnia severity, stress, anxiety, depression, gender, and educational phase, the minimum required sample size was calculated as 138. This approach ensured adequate power for detecting indirect effects in mediation analyses. Ultimately, the study was completed with 201 participants, exceeding the required statistical power.
Participant selection criteria
Exclusion criteria were applied a priori to enhance internal validity and reduce confounding factors: (1) not being a registered medical student, (2) submitting incomplete questionnaires (>5% missing data), and (3) reporting a current or past psychiatric diagnosis. Information regarding psychiatric history was obtained via participants’ self-reports on the sociodemographic data form; no medical records were accessed.
Initially, 233 medical students participated in the study. Thirty-two (32) individuals were immediately excluded based on their self-reported psychiatric history. No further statistical outliers were excluded, and there were no missing data in the final dataset. Consequently, the final sample consisted of 201 participants.
Instruments
Research data were collected using the following tools, which were completed online in the form of self-reports by students who voluntarily participated in the study:
Sociodemographic data form
Prepared by researchers to obtain information on age (years), height (cm), weight (kg), psychiatric history, and educational phase (year of study). BMI was calculated based on self-reported height and weight. Based on this form, participants were categorized into two educational phases: Preclinical Phase (Years 1–3) and Clinical Phase (Years 4–6). Gender was assessed using a binary self-report item (female/male) to align with the university’s standardized institutional data registry.
Nomophobia questionnaire (NMP-Q)
The level of nomophobia was determined using the NMP-Q, which was developed by Yildirim and Correia (2015) and adapted into Turkish by Yildirim et al. (2016). It is a measure consisting of 20 items answered on a seven-point Likert scale and four dimensions. Based on the score obtained from the scale, 20 points and below indicates no nomophobia, 21–59 indicate mild nomophobia, 60–99 indicates moderate nomophobia, and 100–140 indicates severe nomophobia. In the original validation study of the research, the internal consistency coefficient was Cronbach α = 0.92. An example item is: “I would feel anxious if I could not check my smartphone for a while.”
Depression anxiety stress scales (DASS-21)
The DASS-21, developed by Lovibond and Lovibond (1995) to measure depression, anxiety, and stress levels, was used. Its Turkish adaptation was performed by Sariçam (2018). The scale is a four-point Likert type scale consisting of seven questions each measuring depression, stress, and anxiety (21 items in total). In the normal sample, the internal consistency coefficients were found to be α = 0.87 for the depression subscale, α = 0.85 for the anxiety subscale, and α = 0.81 for the stress subscale.
Insomnia severity index (ISI)
Developed to assess the severity of insomnia symptoms, the ISI was created by Bastien and colleagues (Bastien et al., 2001). Its validity and reliability in Turkish were established by Boysan and colleagues (Boysan et al., 2010). The scale consists of seven items answered using a five-point Likert-type scale. ISI scoring is evaluated in four categories, starting from clinically insignificant levels (0–7), followed by the insomnia threshold (8–14), moderate severity (15–21), and severe clinical insomnia (22–28). In the original validation study of the research, the internal consistency coefficient was Cronbach α = 0.79.
Statistical analyses
Data were analyzed using IBM SPSS Statistics 26.0. No missing data were observed in the final dataset. The normality of the data distribution was assessed using Skewness and Kurtosis coefficients. For all study variables, Skewness and Kurtosis values were found to be within the acceptable range of ±1.5 (Tabachnick and Fidell, 2013), indicating a normal distribution. Descriptive statistics (mean, standard deviation, frequency) were calculated for demographic variables. Group differences by gender and educational phase were examined using independent t-tests, with effect sizes calculated using Cohen’s d (characterized as small = 0.20–0.49, medium = 0.50–0.79, and large ⩾ 0.80). Relationships between nomophobia, DASS-21 subscales, and ISI were assessed using Pearson correlation analysis (characterized as r < 0.30 = weak, 0.30–0.49 = moderate, and ⩾0.50 = strong correlation).
Prior to mediation analysis, regression assumptions were verified. The normality of residuals and independence of errors were assessed using the Durbin-Watson statistic. Multicollinearity was evaluated using Variance Inflation Factors (VIF) with a critical threshold of 5. Since data were collected via self-report measures, Harman’s single-factor test was conducted to assess common method bias with a threshold of 50%.
To test the study hypotheses, the PROCESS Macro for SPSS (Model 4) developed by Hayes (2022) was utilized. Unlike previous studies that treat emotional distress as a monolith, this study utilizes a parallel mediation model to examine whether insomnia is associated with nomophobia through general stress or specific symptoms like anxiety and depression. Model 4 was specifically selected to statistically disentangle the specific indirect effects of stress, anxiety, and depression simultaneously (parallel mediation). In this model, insomnia severity was entered as the independent variable (X), nomophobia as the dependent variable (Y), and DASS-21 subscales (stress, anxiety, depression) as parallel mediators. Gender and educational phase were included as covariates to control for potential confounding effects. Significance of indirect effects was determined using 5000 bootstrap resamples (95% Confidence Intervals). Finally, given the cross-sectional nature of the study, an alternative reverse mediation model (Nomophobia→Stress/Anxiety/Depression→ Insomnia) was tested to evaluate directional specificity and rule out reverse causality. Statistical significance was set at p < 0.05.
Results
Descriptive Statistics and gender comparison
The study sample (N = 201) consisted of 62.6% female (n = 126) and 37.4% male (n = 75) medical students, with a mean age of 22.08 ± 2.47 years and a mean BMI of 23.46 ± 4.09 kg/m2. Descriptive statistics and gender comparisons are presented in Table 1. Regarding scale reliability in the current sample, all instruments demonstrated robust internal consistency: NMP-Q (α = 0.94), DASS-21 depression (α = 0.84), anxiety (α = 0.82), stress (α = 0.83), and ISI (α = 0.77).
Descriptive statistics of participants and gender comparisons.
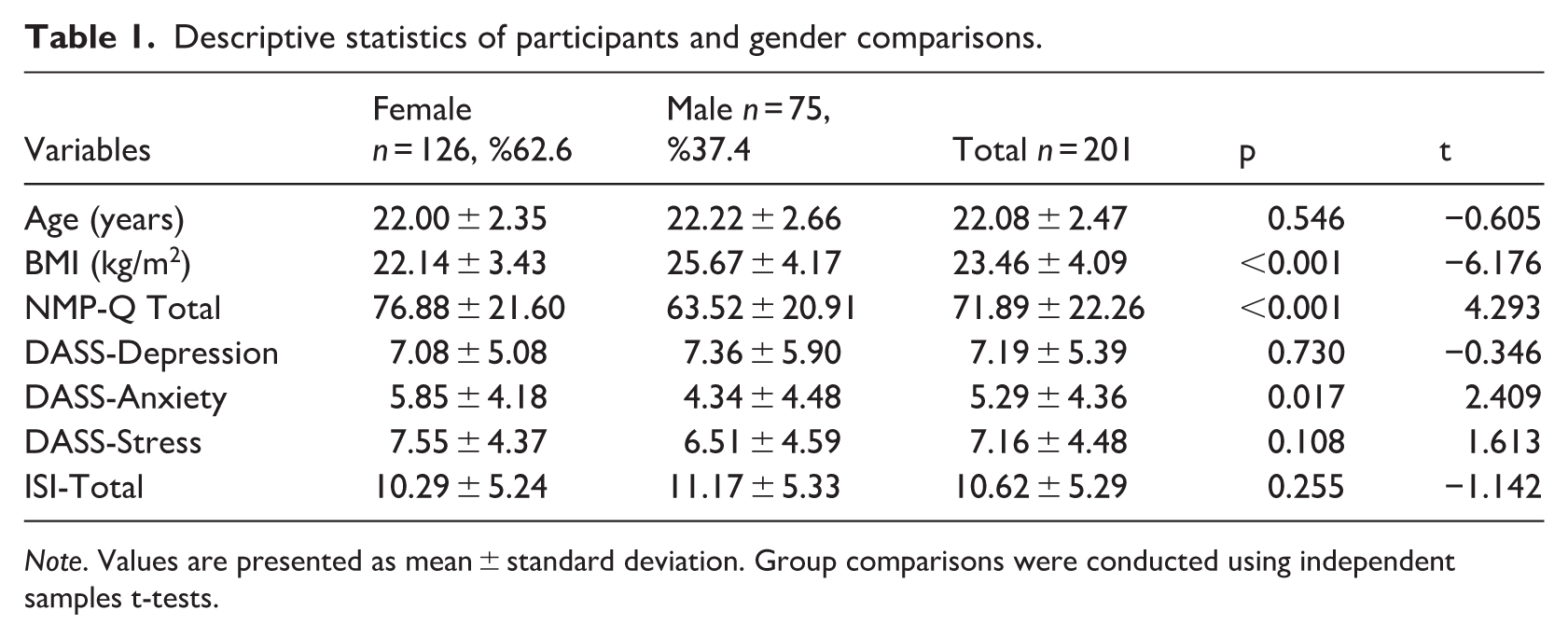
Note. Values are presented as mean ± standard deviation. Group comparisons were conducted using independent samples t-tests.
Female students had higher nomophobia scores (76.88 ± 21.60) compared to males (63.52 ± 20.91, Cohen’s d = 0.63, p < 0.001). Regarding psychological symptoms, female students had significantly higher anxiety scores (Cohen’s d = 0.35, p = 0.017), whereas no significant gender differences were found for depression, stress, or insomnia levels (p > 0.05).
Comparisons based on the educational phase (Table 2) revealed that preclinical students (Years 1–3) experienced significantly higher levels of depression (Cohen’s d = 0.50, p = 0.001), anxiety (Cohen’s d = 0.41, p = 0.005), stress (Cohen’s d = 0.59, p < 0.001), and insomnia severity (Cohen’s d = 0.56, p < 0.001) compared to students in the clinical phase (Years 4–6). However, nomophobia levels did not differ significantly between the two educational phases (p = 0.389).
Comparison of nomophobia, psychological distress, and insomnia severity between preclinical and clinical medical students.
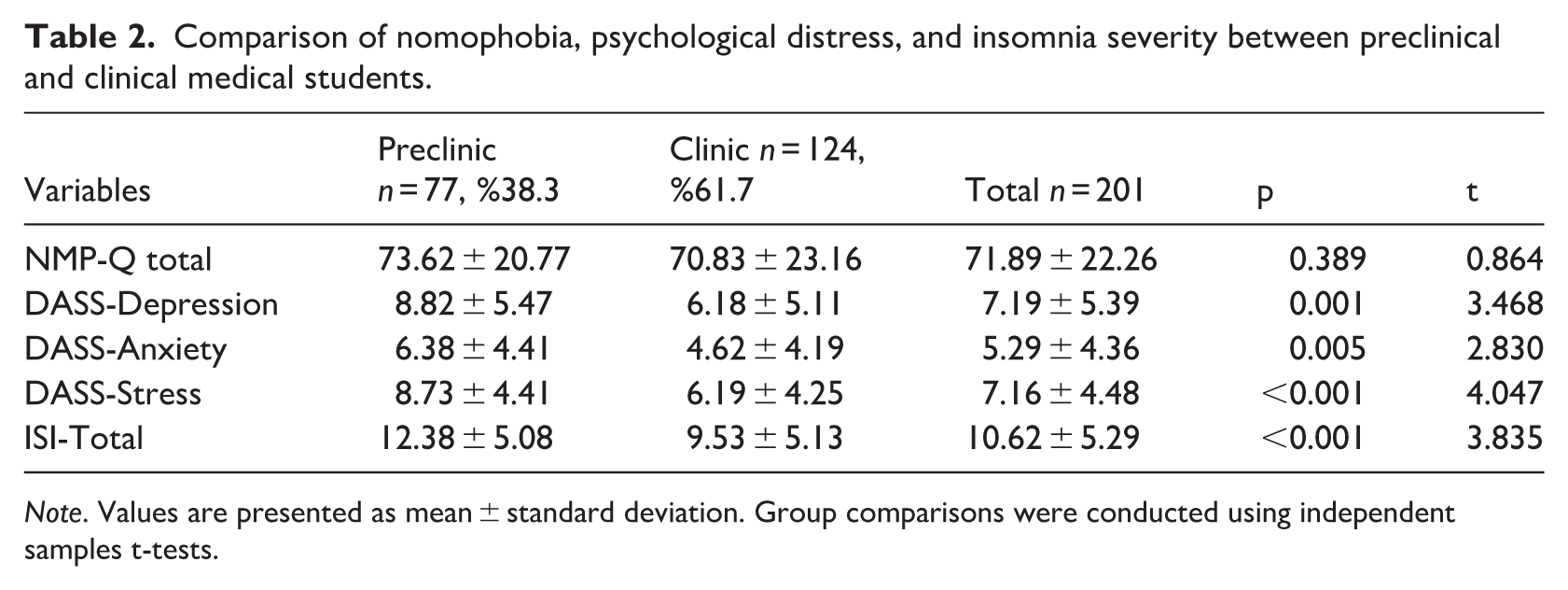
Note. Values are presented as mean ± standard deviation. Group comparisons were conducted using independent samples t-tests.
To contextualize the sample’s baseline characteristics based on established scale cut-offs, participants exhibited, on average, a moderate level of nomophobia (M = 71.89, SD = 22.26) and subthreshold insomnia symptoms (M = 10.62, SD = 5.29). Regarding psychological distress, the overall sample demonstrated relatively normal to mild levels of depression, anxiety, and stress, which is characteristic of a non-clinical student population.
Correlation analysis
Pearson correlation coefficients between study variables are shown in Table 3. Nomophobia scores were significantly and positively, albeit weakly, correlated with stress (r = 0.222, p = 0.002) and anxiety (r = 0.142, p = 0.044). No direct significant correlation was found between nomophobia and depression (p = 0.157) or insomnia severity (p = 0.183).
Correlations between nomophobia and variables.
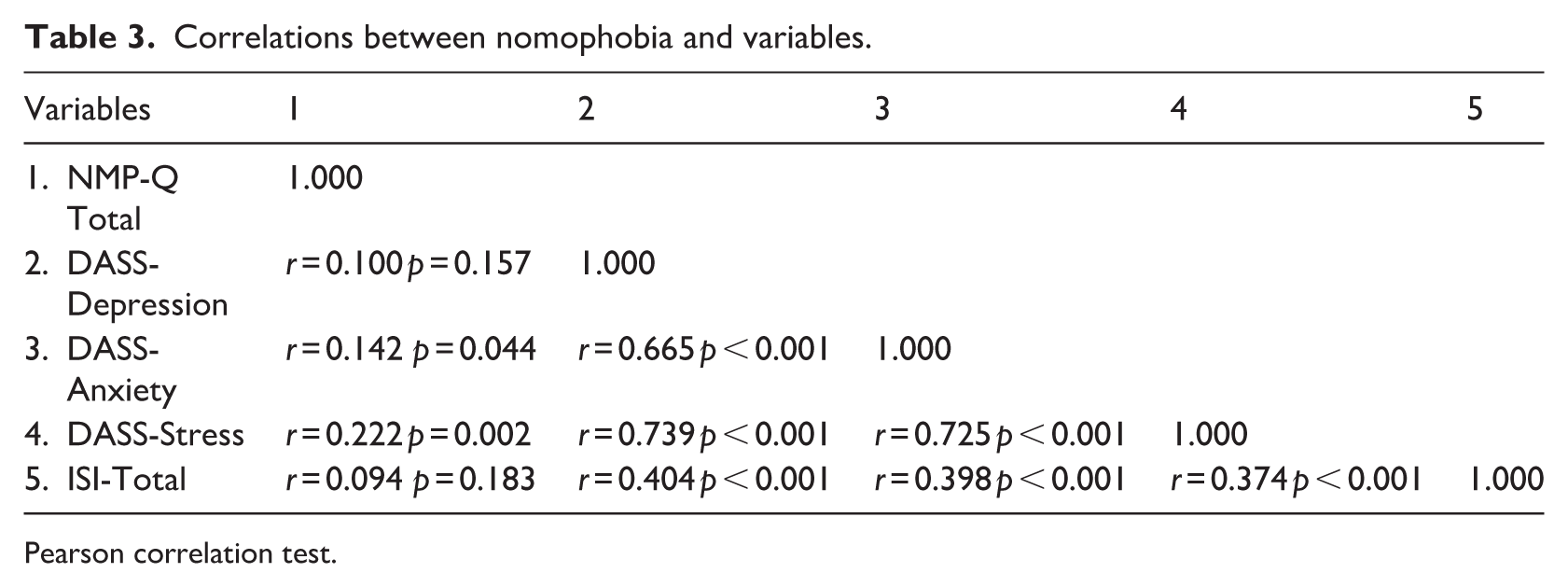
Pearson correlation test.
Notably, insomnia severity showed moderate positive correlations with all three DASS-21 subscales: depression (r = 0.404), anxiety (r = 0.398), and stress (r = 0.374; all p < 0.001). Furthermore, strong inter-correlations were observed among the DASS-21 subscales (r ranging from 0.665 to 0.739, p < 0.001).
Parallel mediation analysis
Preliminary analyses indicated that the assumptions for regression were met. Residuals were approximately normally distributed, and the Durbin–Watson statistic fell within the acceptable range (1.5–2.5), suggesting independence of errors. Multicollinearity was not observed (VIFs < 3, maximum VIF = 2.896). Harman’s single-factor test showed that a single factor accounted for 22.41% of the variance.
The overall model explained 13% of the variance in nomophobia (R2 = 0.13, F(6,194) = 4.85, p < 0.001). The results of the path analysis are illustrated in Figure 1.
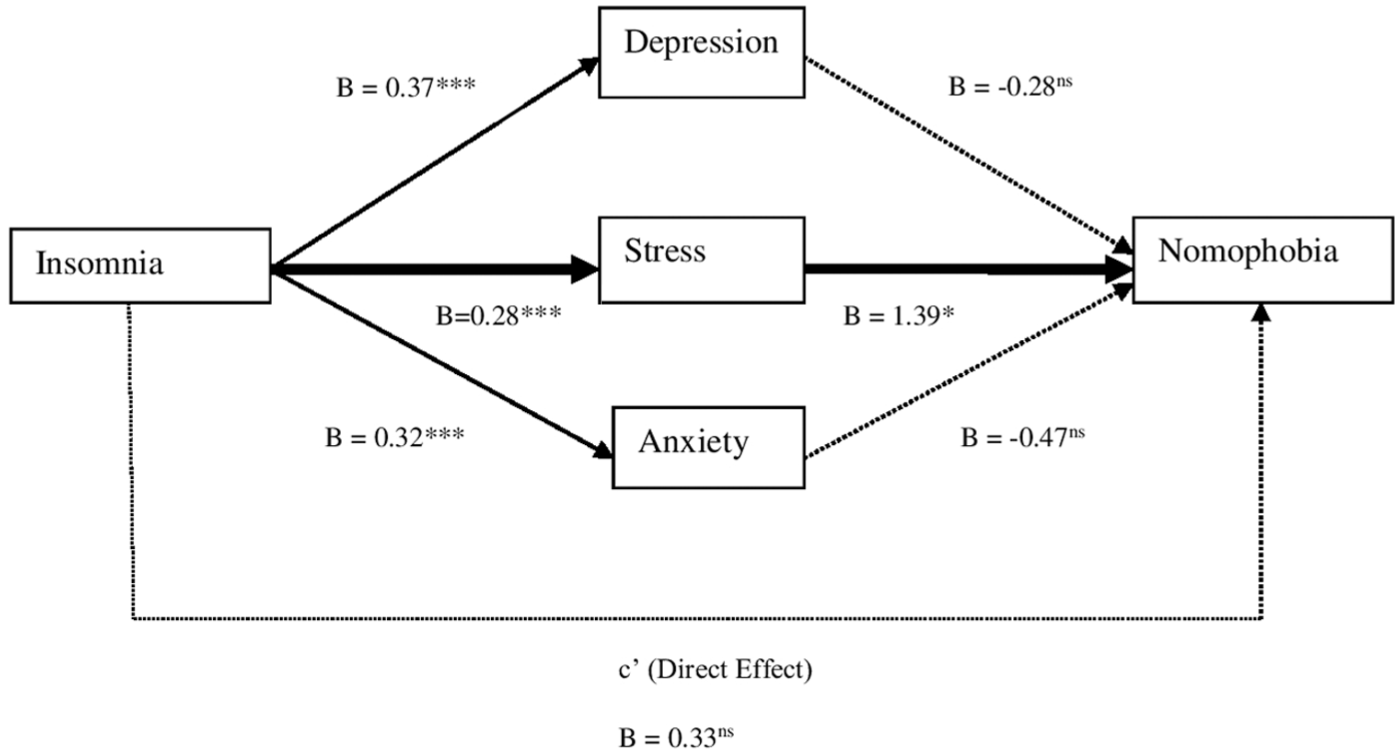
The parallel mediation model illustrating the mediating roles of Stress, Anxiety, and Depression in the relationship between Insomnia and Nomophobia.
The analysis showed that insomnia severity was a significant positive predictor of all three psychological mediators (Path A): stress (B = 0.284, SE = 0.056, p < 0.001, R2 = 0.19), anxiety (B = 0.321, SE = 0.054, p < 0.001, R2 = 0.21), and depression (B = 0.374, SE = 0.068, p < 0.001, R2 = 0.18). When evaluating the pathways from the mediators to nomophobia while controlling for insomnia (Path B), stress was found to be the only significant unique mediator (B = 1.391, SE = 0.566, p = 0.015). In contrast, the unique correlations of anxiety (B = −0.471, p = 0.380) and depression (B = −0.283, p = 0.521) with nomophobia were not statistically significant in the multivariate model.
The assessment of indirect effects using 5000 bootstrap resamples provided critical evidence for the mediation structure. The specific indirect effect of insomnia on nomophobia via stress was statistically significant (B = 0.396, BootSE = 0.188, 95% Bootstrap CI [0.066, 0.815]). However, the specific indirect effects through anxiety (B = −0.151, 95% CI [−0.574, 0.176]) and depression (B = −0.105, 95% CI [−0.453, 0.244]) were non-significant.
Finally, the direct effect of insomnia on nomophobia (c’ path) was not significant (B = 0.330, SE = 0.322, p = 0.306, 95% CI [−0.305, 0.966]). Regarding covariates, gender had a significant independent effect on nomophobia (B = −12.84, p < 0.001), while the educational phase did not (p = 0.927).
Alternative model testing
The results showed that the total indirect effect of nomophobia on insomnia through stress, anxiety, and depression was statistically non-significant (B = 0.0105, 95% Bootstrap CI [−0.0068, 0.0267]). Specifically, the 95% confidence intervals for all individual indirect pathways included zero (Stress: CI [−0.0098, 0.0115]; Anxiety: CI [−0.0044, 0.0158]; Depression: CI [−0.0031, 0.0150]). Additionally, the direct effect of nomophobia on insomnia was also non-significant (B = 0.0163, p = 0.3063).
Discussion
The primary objective of this study was to clarify the pathways between insomnia and nomophobia by disentangling the mediating roles of stress, anxiety, and depression. The most significant finding of this study is that the relationship between insomnia and nomophobia indicates an indirect-only pattern transmitted through psychological distress, specifically stress. This finding aligns with the cognitive control theory (Harvey et al., 2005) and recent resource depletion models (Baglioni et al., 2016; Lin and Huang, 2025). In the context of medical education, poor sleep is known to impair academic performance (Christodoulou et al., 2023); this physiological deficit likely exacerbates the pressure of “academic survival,” thereby depleting the emotional regulation resources required to inhibit maladaptive impulses like smartphone checking. Our findings provide substantial support for the I-PACE (Interaction of Person–Affect–Cognition–Execution) model (Brand et al., 2019), positioning insomnia not merely as a consequence of phone use, but as a psychophysiological vulnerability that is associated with nomophobia through stress–health behavior pathway. It is particularly noteworthy that even subthreshold insomnia and mild levels of psychological distress were sufficient to activate this maladaptive coping pathway, highlighting the sensitivity of medical students to everyday academic pressures.
The moderate levels of nomophobia found in our study are consistent with both international research (Hussein et al., 2024; Kubrusly et al., 2021) and studies conducted in the same national context (Akbaş Güneş and Gücük, 2020; Baykan et al., 2021). As noted by Akbaş Güneş and Gücük (2020), nomophobia in medical students is not merely a technology habit but a well-being risk factor that can impair academic performance and well-being. While previous studies often focus on general correlations (Ayaz-Alkaya et al., 2025; Yigit et al., 2024), our study contributes by disentangling the specific statistical pathways that link sleep disturbances to this maladaptive coping-related behavior.
While correlation analyses showed that anxiety was also related to nomophobia (Bano et al., 2021), its independent effect disappeared in our parallel mediation model. The high degree of overlap indicates that symptoms of stress, anxiety, and depression frequently co-occur and share substantial variance within this sample of medical students, which may obscure their unique contributions in multivariate models. This “suppression effect” suggests that in the presence of high academic demands, general stress serves as a more central affective bridge than specific anxiety or depressive symptoms. Medical students experiencing insomnia-related physiological strain may turn to smartphones not merely out of anxiety, but as a maladaptive “safety signal” or an avoidance-based relief strategy to cope with the resulting general stress (Gnardellis et al., 2023; Shaleha and Roque, 2024).
Interestingly, the observed indirect-only pattern (non-significant direct effect of ISI on NMP) suggests that insomnia does not directly drive the fear of being without a phone; rather, it creates a state of physiological vulnerability that amplifies stress. This interpretation is consistent with Jahrami et al. (2022) and Demirci et al. (2015), who highlighted the “insomnia → emotional arousal → phone use cycle.” Although some literature suggests the reverse direction (Sadeghi et al., 2025), our alternative model testing confirmed the directional specificity of our findings, showing that the reverse pathway (Nomophobia → Insomnia) was not statistically robust in this sample. Thus, improving sleep hygiene may be a prerequisite for effective stress regulation and, consequently, for reducing nomophobia.
Consistent with the literature (Baykan et al., 2021; Kubrusly et al., 2021), female students reported significantly higher levels of nomophobia, anxiety, and stress. It has been suggested that female students’ tendency to use smartphones for emotional regulation and social connection may increase their susceptibility (Zwilling, 2022). However, our mediation analysis showed that the underlying mechanism functions similarly across genders, suggesting that the “stress-bridge” is a universal psychological process in medical education, regardless of gender-specific usage patterns (Bhattacharya et al., 2019; Panova and Carbonell, 2018).
A noteworthy observation in our study concerns the educational phase. While the phase of education was not directly associated with nomophobia levels, it emerged as a significant correlate of stress and depression. Specifically, students in the pre-clinical phase (first 3 years) exhibited significantly higher stress and depression scores compared to those in the clinical phase. This finding aligns with established medical education literature, which consistently reports that the initial years are characterized by intense academic pressure, high theoretical workload, and challenges in adjusting to the medical curriculum (Dyrbye et al., 2006; Rotenstein et al., 2016). Furthermore, in educational systems where medical training commences at the undergraduate level, the transition from high school to a competitive medical school environment often triggers “adjustment disorder-like” symptoms in junior students (Hope and Henderson, 2014). Moreover, there are other unmeasured factors that may be independently associated with the mental health of medical students, such as dysfunctional parenting styles and low self-efficacy beliefs (Siqueira-Campos et al., 2021). Since our mediation model identified “stress” as the key mechanism linking insomnia to nomophobia, pre-clinical students—who already operate at higher baseline stress levels—may be at greater risk of entering this vicious cycle. In this context, insomnia in the early years could more easily trigger the stress threshold required to activate nomophobic behaviors as a coping mechanism.
Clinical significance and future directions
These findings align with the perspective of health psychology, suggesting that nomophobia should be viewed not merely as an isolated clinical condition, but as a maladaptive health behavior emerging from the failure of behavioral regulation under physiological strain. Consequently, university health services should prioritize stress regulation rather than focusing solely on smartphone restrictions. Since the competitive atmosphere of medical education acts as a primary trigger, Mindfulness-Based Stress Reduction (MBSR) programs could be particularly effective in reducing tendencies toward dysregulated smartphone use by enhancing students’ emotional regulation skills (Elhai et al., 2018).
Second, the identification of insomnia as a physiological vulnerability factor emphasizes the critical need for sleep-focused health promotion strategies. Targeting sleep hygiene serves as a fundamental strategy to restore psychophysiological balance, thereby interrupting the stress–health behavior pathway that sustains nomophobia. Preventive programs such as Cognitive Behavioral Therapy for Insomnia (CBT-I) and reducing blue light exposure may have potentially meaningful benefits by lowering the physiological stress load (Alimoradi et al., 2022). Routine screening for sleep disturbances within student health services may be beneficial to facilitate early preventive programs before these symptoms escalate into entrenched behavioral patterns.
Furthermore, our results inform when preventive programs should be implemented. Given that pre-clinical students carry a heavier burden of stress, preventive efforts should be strategically timed during the first 3 years of medical school. Medical faculties should implement regular screenings for sleep quality among Year 1–3 students. Incorporating stress management training early in the curriculum could effectively break the cycle before avoidance-based coping tendencies evolve into chronic patterns.
Finally, considering the multidimensional structure of nomophobia, university health centers should adopt a multi-component approach. Rather than using isolated workshops, comprehensive programs that integrate psychoeducation, stress management, and sleep counseling are recommended. Recent evidence suggests that such holistic preventive programs are significantly more effective in improving behavioral regulation compared to single-modal approaches (Lu et al., 2025).
Limitations
This study has several limitations. First, despite statistical support for directional specificity using Hayes’ PROCESS macro, the cross-sectional design precludes definitive causal inferences. Therefore, the pathways identified in our model (Insomnia → Stress → Nomophobia) should be considered hypothesis-generating rather than confirmatory. Longitudinal studies are needed to substantiate the temporal stability of these mechanisms. Second, the reliance on self-report measures introduces potential bias. Future research should incorporate objective tools, such as actigraphy for sleep and digital tracking logs for smartphone usage, to validate subjective reports. Finally, the sample was drawn from a single medical school, which limits the generalizability of the findings to different cultural contexts or institutional curricula. Furthermore, the binary measurement of gender did not capture the full spectrum of gender identities, presenting a demographic limitation.
Conclusion
This study elucidates the psychophysiological pathways connecting sleep disturbances to nomophobia among medical students. Our results demonstrate that the relationship between insomnia and nomophobia is transmitted through the indirect pathway of stress, identifying stress-related psychophysiological strain as the primary link between physiological sleep deficits and maladaptive smartphone use. Notably, when controlled for stress, the unique effects of anxiety and depression were non-significant, highlighting the central role of academic stress rather than specific emotional symptoms in this population.
Furthermore, while female students exhibited significantly higher levels of nomophobia and anxiety, the structural mechanism (Insomnia → Stress → Nomophobia) remained consistent across genders, suggesting a broadly shared vulnerability pattern driven by the demanding medical curriculum. Consequently, health-focused interventions should move beyond behavioral monitoring approaches targeting smartphone use and focus on improving sleep hygiene and enhancing stress regulation skills. Addressing insomnia as a physiological vulnerability factor represents a potentially critical target for reducing nomophobia among medical students.
Footnotes
Acknowledgements
The authors wish to express their gratitude to all medical students who voluntarily participated in this study.
Ethical considerations
The study was approved by the Ethics Committee of Karadeniz Technical University (Decision Date: 15.01.2025, Decision No: 24237859-23).
Consent to participate
Written informed consent was obtained from all participants involved in the study.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Author contributions
M.K., O.Ö.T. and E.Ö.K. designed the study. M.K. and O.Ö.T. collected the data. M.K. performed the statistical analysis and wrote the first draft of the manuscript. M.K. and E.Ö.K. supervised the study and reviewed the final manuscript. All authors contributed to the interpretation of results and approved the final version for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.*
Declaration of generative AI and AI-assisted technologies
During the preparation of this work, the authors used DeepL Translate to improve language and readability. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.