
Abstract
Stoic philosophy may be a practical intervention to enhance coping. This randomized clinical trial was conducted between February and May 2025. A total of 52 patients undergoing hemodialysis were randomly assigned to intervention (26) and control (26) groups. The intervention group got 8 weeks of Stoic training. Demographic and spiritual coping strategies questionnaires were completed and were analyzed using SPSS with appropriate statistical tests. The mean change of total spiritual coping strategies and the non-religious dimension (p = 0.001, Cohen’s d = −0.95; and p < 0.001, Cohen’s d = −1.09, respectively) was found to be greater in the intervention group, but was not significantly different (p = 0.08, Cohen’s d = −0.49) in the religious dimension. Teaching Stoicism may enhance the spiritual aspect of coping strategies. Further experimental intervention studies are recommended across diverse settings and different populations, including formal and informal caregivers, patients with chronic illnesses, and students.
Introduction
Millions of new cases of chronic kidney disease (CKD) are diagnosed worldwide each year, often progressing to end-stage renal disease (ESRD; Zhang et al., 2024). While hemodialysis is a vital treatment for kidney failure, it can lead to significant challenges, including depression, poor quality of life, hopelessness, sadness, fear of the future, death anxiety, dissatisfaction with fate, and a sense of meaninglessness (Asadzandi et al., 2022). Furthermore, patients face physical, psychological, social, and financial burdens, increasing the difficulty of coping with this disease (Saffari et al., 2014).
In such circumstances, many individuals rely on emotion-focused coping strategies and emotion regulation (Sadeghifar, 2017). One key strategy is spiritual coping, which plays an important role in helping hemodialysis patients adapt to chronic illness (Işık Ulusoy and Kal, 2020). This approach involves using spirituality, religious beliefs, or religious behaviors to manage stressful life situations (Vitorino et al., 2018). Spiritual coping consists of both positive strategies (such as seeking greater connection with a higher power or finding peace in religious texts) and negative strategies (such as questioning God’s existence, passively delegating problems to God, or viewing stress as divine punishment; Valcanti et al., 2012). Negative spiritual coping can result in a loss of meaning and feelings of disconnection from God and the religious community (Taheri-Kharameh et al., 2016).
Spirituality-related coping can also be categorized as either religious coping (e.g., prayer, supplication) or non-religious (spiritual) coping. Examples of non-religious spiritual coping include meditation, connecting with nature or others, and exploring one’s innermost thoughts within a supportive environment (such as a support group, a spiritual guide, or a close friend; Hawthorne et al., 2011).
Spiritual education and emphasis on the meaning and purpose of life may counteract the spiritual crisis and weakening of spiritual-religious beliefs in people with chronic diseases (Tavassoli et al., 2019) because in the face of these diseases, both believers and non-believers are challenged and seek meaning and purpose in their lives (Baldacchino and Buhagiar, 2003).
Spirituality offers a powerful means of coping with anxiety and fear of death while simultaneously improving the overall health of patients with end-stage renal disease (ESRD). Walton et al. (2002) highlight how spirituality and faith can be a driving force, helping patients accept the realities of dialysis and confront death (Walton, 2002). Effective spiritual coping mechanisms are meaning-making, anxiety reduction, impulse control, evolutionary adaptation, and the reinterpretation of pain and suffering (Burlacu et al., 2019).
Despite the need for spiritual support among patients with ESRD, these needs are often overlooked (Valcanti et al., 2012). Spiritual coping strategies may be modifiable through intervention; therefore, integrating these strategies into the healthcare process for ESRD patients is very important (Santos et al., 2017). By providing practical strategies to enhance spiritual coping, we can effectively support patients undergoing hemodialysis and help them deal with the challenging consequences of their disease (Saffari et al., 2014).
A novel approach to fostering spirituality involves integrating Stoic teachings, which focus on correcting false beliefs and mitigating psychological distress (Irvine, 2008). This philosophical framework emphasizes spiritual exercises designed to accept uncontrollable circumstances (such as chronic illness), and to foster virtue and inner peace (Ding et al., 2023). Stoicism further contributes to spiritual and moral development by strengthening compassion, encouraging the acceptance of a shared human experience, and promoting personal responsibility (Aurelius, 2020). It teaches individuals that suffering and pain can paradoxically imbue life with greater meaning, happiness, and health (Stanbouly et al., 2021).
Stoicism nurtures spirituality not through rituals or complex metaphysics, but through self-cultivation, acceptance of existence, and service to universal reason (Sherman, 2021). This philosophy teaches a dialysis patient how to maintain inner peace amidst life’s storms while remaining kind and benevolent (Brown et al., 2022a). Stoicism begins with turning inward, which enhances spirituality. Through the trichotomy of control, Stoic philosophy teaches the patient that some things are within their control—such as their judgments, thoughts, actions, and desires—while other things are not, such as wealth, reputation, health, and the behavior of others (Long and Spalding, 1904). One must focus their energy on internal matters, which are subject to change, and accept external matters, which are uncontrollable. This is because, firstly, expending energy on them is futile; and secondly, nature, through its inherent rationality—called Logos—moves toward the good, and ultimately, events unfold in such a way that the patient’s good is served. Therefore, the patient should love their fate and accept it—what is philosophically termed Amor Fati (Boostani et al., 2025). This inward attention cultivates a kind of inner peace and sacredness that can enhance spirituality. Stoicism teaches human beings that there is purpose behind hardship. Difficulties and adversities in life can lead to the strengthening of valuable moral qualities in the patient, shaping them into a more resilient, courageous, flexible, and problem-capable individual (Irvine, 2019).
To our knowledge, no evidence-based study on Stoicism has been conducted among dialysis patients worldwide, and the present study is the first evidence-based study on Stoicism in this population. In general, evidence-based studies on Stoicism in various populations are very limited. Therefore, the present study was conducted to evaluate the effect of Stoic teachings on spiritual coping strategies in hemodialysis patients.
Methods
This randomized controlled trial was conducted among hemodialysis patients in Birjand (center of the South Khorasan), between February and May 2025. The sample size was determined using the standard formula for intervention studies, based on statistical parameters reported by Afazel et al. (2013; α = 0.05, β = 0.2, S_1 = 5.06, S_2 = 3.37, M1–M2 = 3.65). This calculation indicated a minimum of 22 participants per group. To account for a potential 15% dropout rate, the final sample size was increased to 26 participants per group.
The study commenced after receiving ethical approval from the National Ethics Committee (Approval ID: IR.BUMS.REC.1404.26). All participants signed written informed consent forms before enrollment.
Participants were selected via convenience sampling and then randomly assigned to the intervention or control group in a 1:1 ratio. Randomization was performed using permuted blocks of size four, ensuring balanced group sizes through six possible sequences. Allocation was concealed using opaque, sealed envelopes, and the process was managed by an independent researcher who was not involved in the study's implementation. Participants were informed of their assigned groups via telephone. Due to the nature of the intervention, blinding was not feasible.
Inclusion criteria
- Aged between 18 and 65 years.
- Provided informed consent.
- Oriented to time and place.
- No history of substance abuse.
- Not currently using antipsychotic medications and no acute psychotic disorders.
- Undergoing hemodialysis for at least 3 months.
- Be Persian-speaking and literate.
Exclusion criteria
- Missing more than two educational sessions.
- Voluntary withdrawal from the study.
- Clinical deterioration preventing continued participation.
- Participant death.
Primary outcomes
The primary outcome of interest was the use of spiritual coping strategies.
Data collection tools
A demographic questionnaire gathered information such as age, gender, marital status, education level, income, duration of dialysis treatment, type of vascular access, number and duration of weekly dialysis sessions, employment status, comorbidities, and current medications. Diabetes, hypertension, hyperlipidemia, and heart disease were considered comorbidities.
The Spiritual Coping Strategies (SCS) scale is a self-administered tool developed by Baldacchino and Buhagiar (2003) to assess spiritual and religious coping. It consists of 20 items divided into two sections:
- Religious coping strategies: This section contains nine items that explore participants’ attitudes toward religion and belief in God.
- Non-religious or spiritual coping: This section consists of 11 items that evaluate humanistic coping strategies related to self, others, and nature.
All items are rated on a four-point Likert scale, ranging from 0 (never used) to 3 (often used). The total score, ranging from 0 to 60, is calculated by summing the responses from all questions; a higher score indicates greater use of spiritual coping strategies. While a specific cut-off point for the SCS has not been established, its validity and reliability have been demonstrated in previous research. For instance, Saffari et al. (2014) conducted a study on Iranian patients undergoing hemodialysis and reported favorable psychometric properties and a Cronbach’s alpha of 0.87 for the scale. The SCS also showed good convergent and divergent validity when assessed against the Duke University Religion Index (DUREL) and the Visual Analogue Scale, respectively. Furthermore, the scale’s test-retest reliability over time has been confirmed (Saffari et al., 2014).
Intervention
The study was implemented in three phases: pre-intervention, intervention, and post-intervention. Initially, participants in both the intervention and control groups were added to separate virtual groups via social media platforms. Baseline questionnaires were completed during this phase.
The intervention content was developed by a qualified researcher under the supervision of academic experts, using authentic Stoic texts such as Love of Destiny, The Stoic Art of Living, The Discourses of Epictetus, and Meditations by Marcus Aurelius, along with insights from Connery et al. (2023). The compiled material was then converted into a podcast series.
The intervention aimed to introduce participants to Stoic philosophy and its practical applications. It began with an initial in-person session to introduce the study objectives and format. For 2 months, participants engaged in 8 weekly educational sessions. Each week, a 20-minute podcast was uploaded to the virtual group, and participants were asked to listen to it before attending a corresponding in-person session. These face-to-face sessions, facilitated by the researcher, were used to discuss podcast content, answer questions, and provide real-life scenarios for practice. The intervention concluded with a final summarizing session in week eight. The findings of some studies indicate that conducting eight training sessions can improve psychological indicators in hemodialysis patients; therefore, eight sessions were also designed in the present study (Adamoli et al., 2025).
One week after completing the intervention, both groups completed the post-test assessments using the research questionnaires. To ensure ethical considerations, participants in the control group were granted access to the podcast content after the study ended. The detailed outline and content of the Stoic teaching intervention are presented in the Supplemental material (Teaching outline).
Data analysis
Data normality was assessed using the Shapiro–Wilk test. Quantitative variables were expressed as means and standard deviations, while categorical variables were reported as frequencies and percentages. Baseline comparisons between the intervention and control groups were performed using independent t-tests for continuous variables and chi-square or Fisher’s exact tests for categorical variables, as appropriate. To assess within-group changes over time, paired sample t-tests were conducted. Additionally, between-group differences at the post-intervention stage were analyzed using multiple linear regression, adjusting for potential confounders. All statistical analyses were performed using SPSS version 27. A p-value of less than 0.05 was considered statistically significant.
Results
Fifty participants (25 in each of the 2 groups) finished the study (Figure 1).
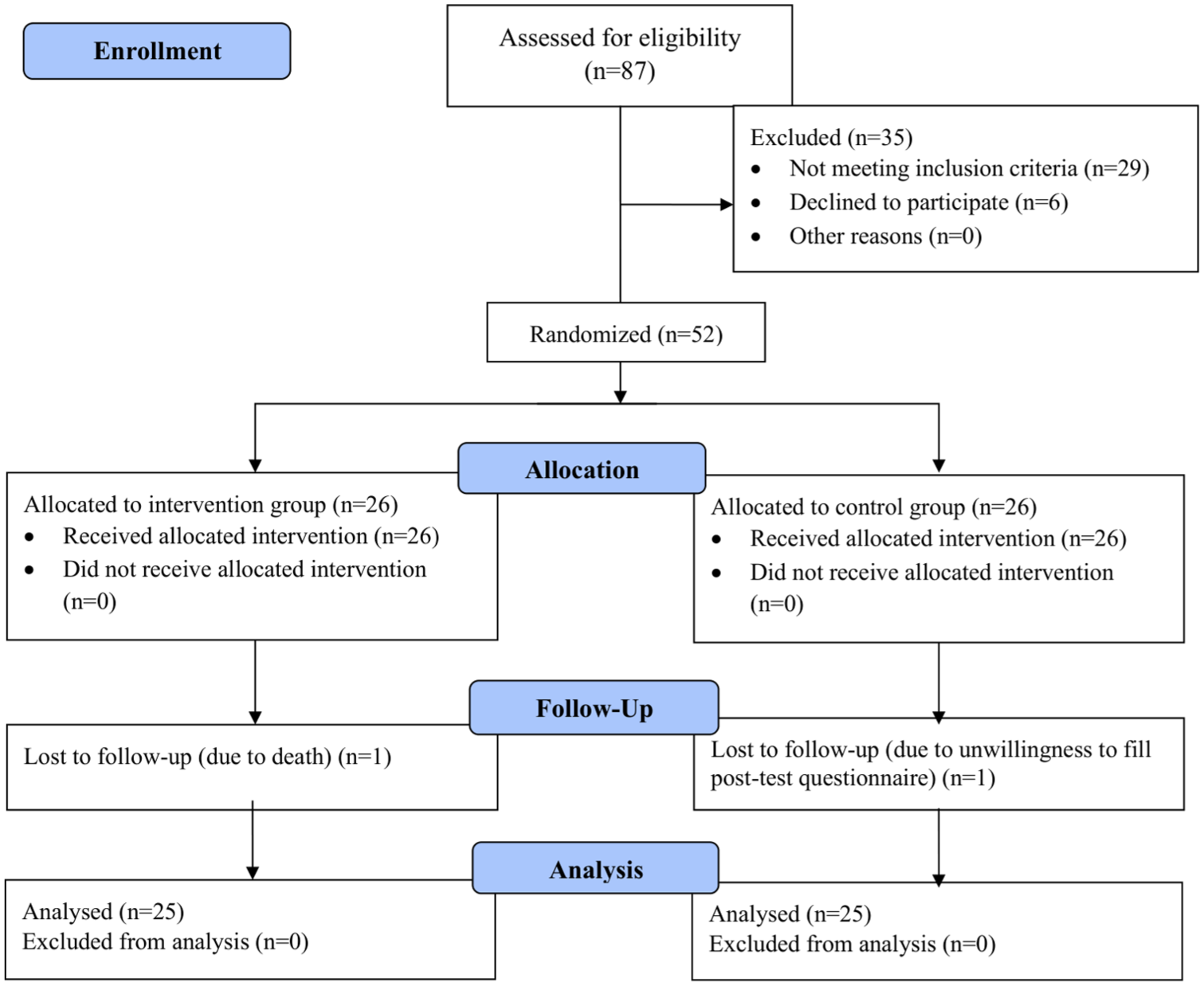
Consort flow diagram of study.
The average age of participants was similar in both the intervention group (Mean: 45.32, SD: 14.45) and the control group (Mean: 54.04, SD: 13.72). In the intervention group, 16 individuals were male, while the control group had 11 males. Additionally, 19 individuals in each group were married. Table 1 compares baseline characteristics between intervention and control groups.
Comparison of demographic characteristics between patients undergoing hemodialysis in the two groups.
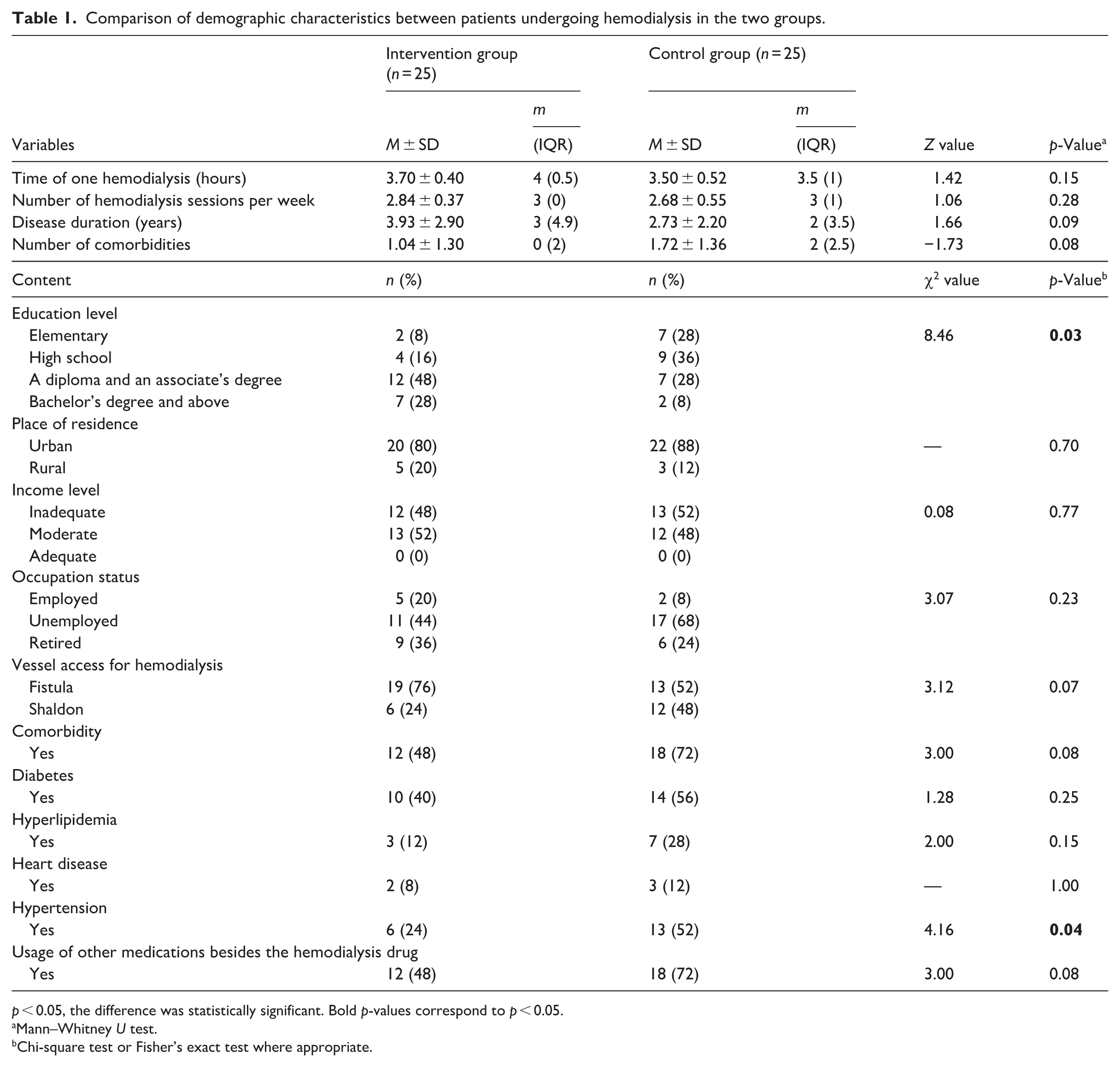
p < 0.05, the difference was statistically significant. Bold p-values correspond to p < 0.05.
Mann–Whitney U test.
Chi-square test or Fisher’s exact test where appropriate.
As shown in Table 2, there was no statistically significant difference between the two groups regarding the mean scores of SCS before intervention (p > 0.05). The mean score of SCS after the intervention was significantly higher in the intervention group compared to the control group (p < 0.05 and Table 2).
Comparison of spiritual coping strategies scores between the two groups before/after the intervention.
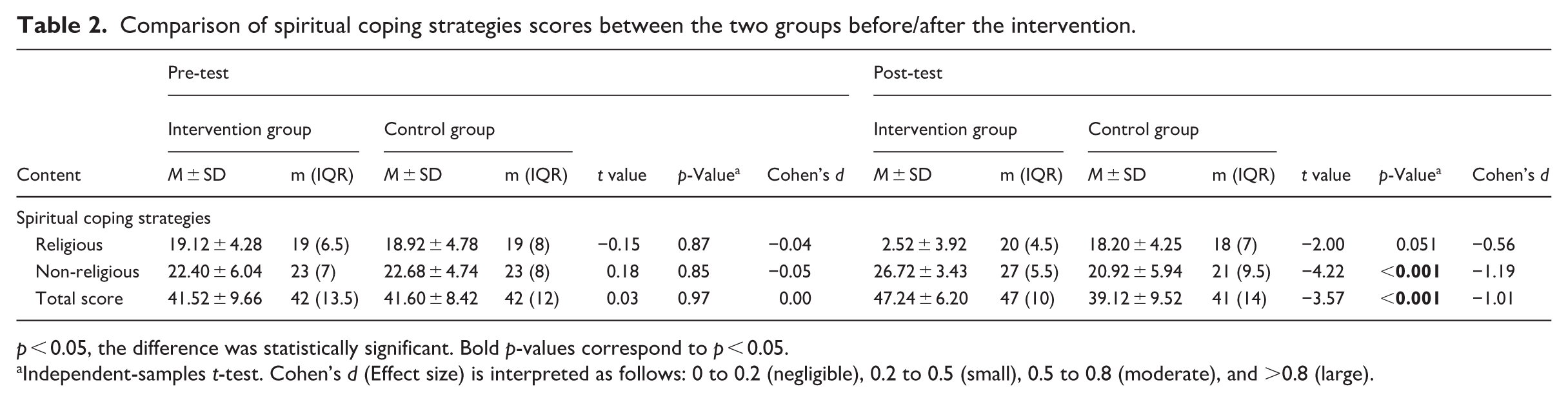
p < 0.05, the difference was statistically significant. Bold p-values correspond to p < 0.05.
Independent-samples t-test. Cohen’s d (Effect size) is interpreted as follows: 0 to 0.2 (negligible), 0.2 to 0.5 (small), 0.5 to 0.8 (moderate), and >0.8 (large).
As shown in Table 3, the mean scores of SCS and their dimensions in the control group did not show a significant difference (p > 0.05). However, mean scores of SCS and non-religious dimension in the intervention group showed a significant difference (p < 0.05); such that the implementation of the intervention improved these scores. More information is provided in Table 3.
Comparison of spiritual coping strategies scores within two groups before/after intervention.
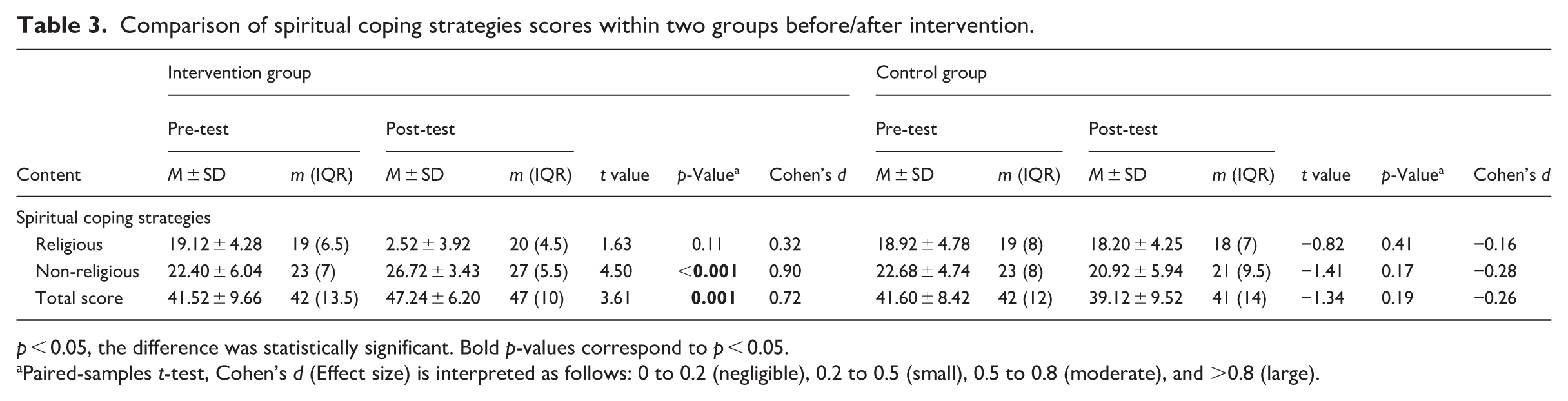
p < 0.05, the difference was statistically significant. Bold p-values correspond to p < 0.05.
Paired-samples t-test, Cohen’s d (Effect size) is interpreted as follows: 0 to 0.2 (negligible), 0.2 to 0.5 (small), 0.5 to 0.8 (moderate), and >0.8 (large).
The comparison of the mean changes in SCS and its dimensions presented in Table 4 shows that the mean change scores of total SCS and the non-religious dimension were greater in the intervention group (p = 0.001, Cohen’s d = -0.95; and p < 0.001, Cohen’s d = −1.09, respectively), suggesting an increase in spiritual coping strategies after the Stoicism educational package training. Furthermore, no statistically significant difference was observed in the mean change score of the religious dimension (p = 0.08, Cohen’s d = −0.49).
Mean change comparison in spiritual coping strategies scores between the two groups.
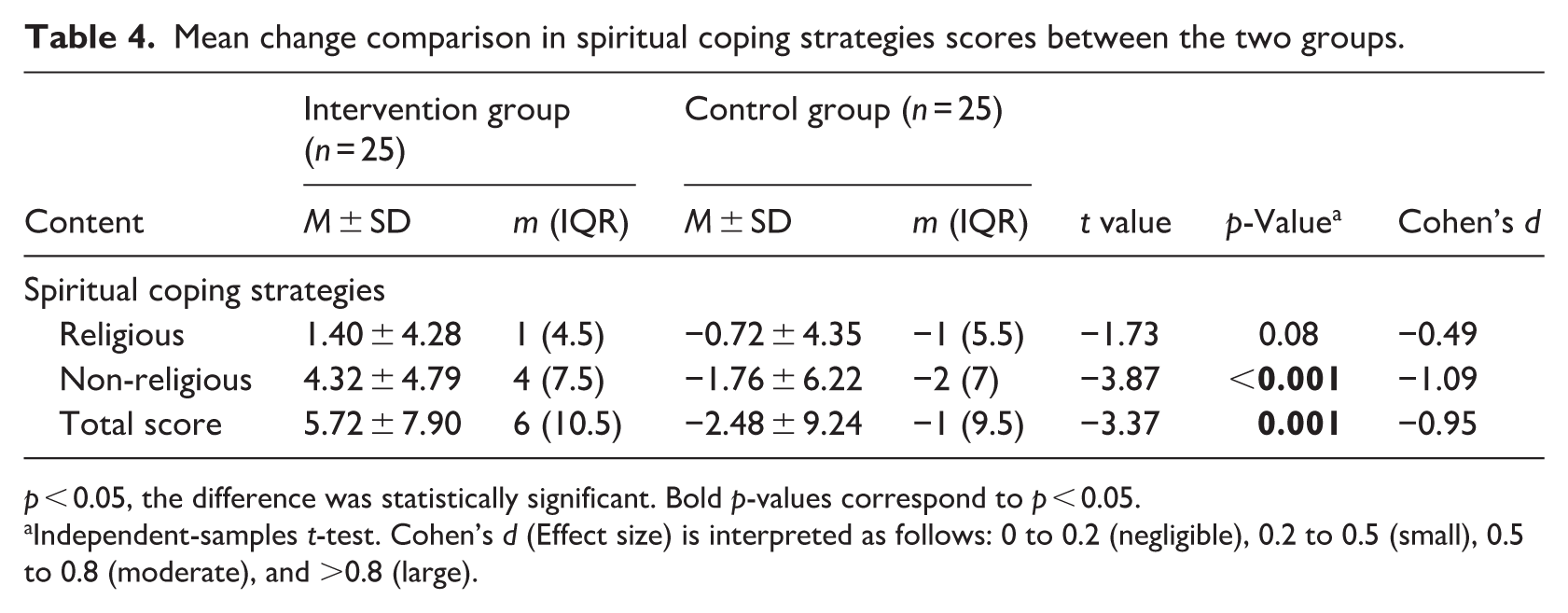
p < 0.05, the difference was statistically significant. Bold p-values correspond to p < 0.05.
Independent-samples t-test. Cohen’s d (Effect size) is interpreted as follows: 0 to 0.2 (negligible), 0.2 to 0.5 (small), 0.5 to 0.8 (moderate), and >0.8 (large).
Multiple regression analysis was used because the two groups differed significantly in terms of hypertension (p = 0.04) and educational level (p = 0.03). Based on analysis results, control of pretest score, hypertension, and education level was significantly associated with an increase in score of spiritual coping strategies in the intervention group (Table 5).
Multiple linear regression models for spiritual coping strategies.
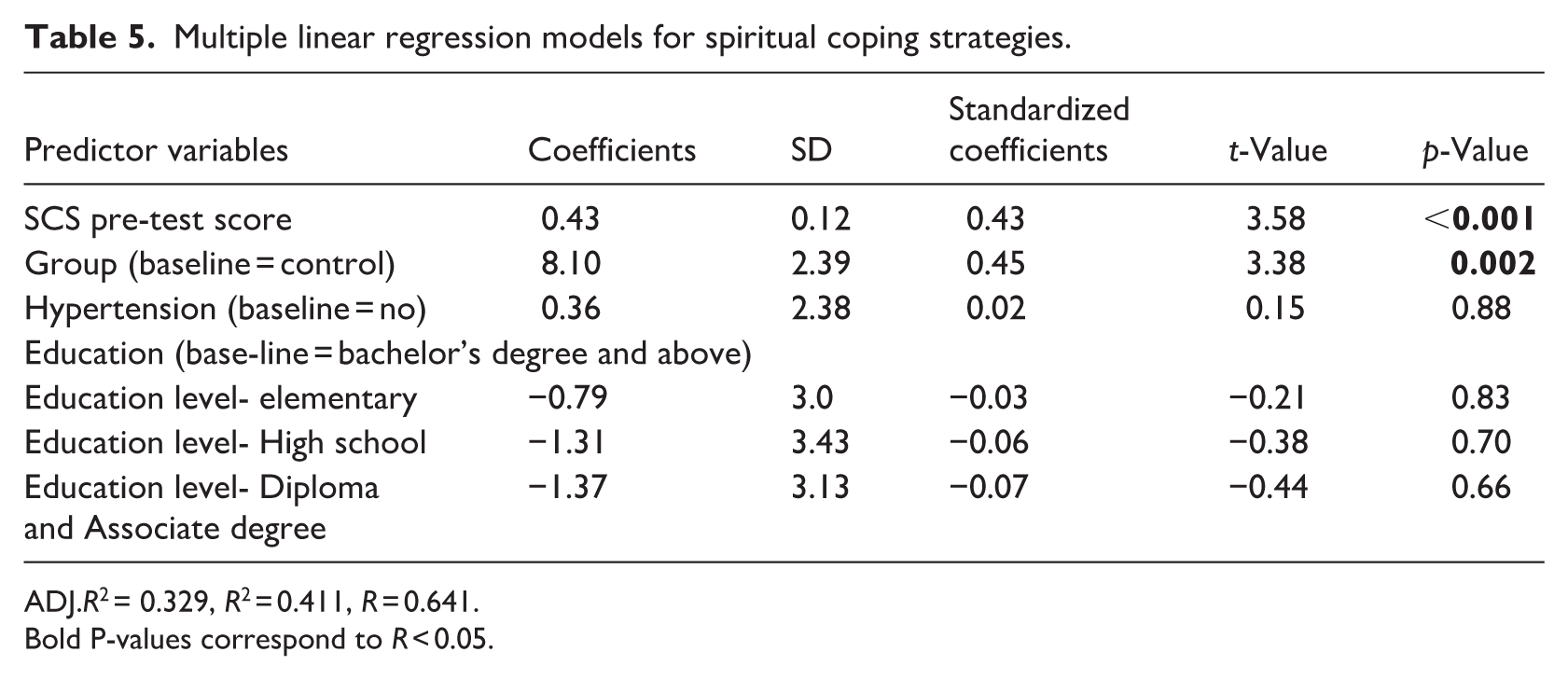
ADJ.R2 = 0.329, R2 = 0.411, R = 0.641.
Bold P-values correspond to R < 0.05.
Discussion
This study examined the influence of Stoic training on spiritual coping strategies in patients under hemodialysis. Although coping strategies demonstrated a significant improvement in the non-religious aspect, no statistically significant improvement was observed in the religious aspect. Given the limited body of research on Stoicism, comparative analyses were drawn from studies most closely aligned with the present investigation. Based on the present study results, Stoicism has improved the spiritual aspect of coping strategies. This finding aligns with the study by Brown et al. (2022a) demonstrated that Stoic training significantly enhanced resilience among medical students (Brown et al., 2022b). As well as Hajizade et al. (2024) found that Stoic training enhanced resilience among operating room staff (Hajizade et al., 2024). Various studies have shown that Stoic teachings improve resilience in different populations, and improved resilience is associated with the strengthening of spiritual strategies. Therefore, it appears that in the present study, Stoic teachings enhanced the non-religious aspect of spiritual strategies through improving resilience as a mediating variable (Cavaliere, 2021; Drumm et al., 2013).
According to Stoic philosophy, existence is an interconnected whole, and the fate of all beings is dependent on each other; therefore, every human should be kind and compassionate to other beings (Aurelius, 2020). From this perspective, a person can love and have compassion for others just when he/she first loves himself/herself despite individual defects and weaknesses (Seneca, 2025). Another spiritual perspective of Stoic philosophy on existence is the meaningfulness of evil in nature. In Stoic thought, good and evil are not separable, and good cannot exist without evil. Just as a person cannot understand the existence of light until he sees darkness, and cannot appreciate the value of health until he gets sick (Cağrı-Mutlu, 2017).
From the Stoic perspective, the world is moving towards goodness, so when an out-of-control problem or calamity arises, the person should accept it as divine providence (The trichotomy of control tenet). It appears that this spiritual thought helps chronic patients, such as patients undergoing hemodialysis, to be more resilient to suffering and maintain peace in their lives (Irvine, 2008).
The Stoic doctrine of negative visualization teaches a person faced with unsolvable adversity, he/they should keep in mind that things could have been worse (Irvine, 2019). For example, a patient who is undergoing hemodialysis can apply this teaching in this way, saying to himself: It is true that I have to undergo hemodialysis three times a week for 4 hours, but I thank God for access to the hemodialysis center and care providers in my city. If my disease were not curable or if these facilities were not there, and I had to go to another city, the situation would definitely be more difficult and worse. It is worth noting that these teachings may deepen patients' view of existence and strengthen the spiritual dimension of coping strategies by changing their attitude towards sufferings and hardships.
The results of the present study showed that Stoicism does not have a statistically significant effect on the religious aspect of coping strategies. In contrast, the study by Akrim et al. (2021) showed that Stoicism and religious coping strategies can be directly related and strengthen some psychological indicators (Akrim et al., 2021). Stoicism is dependent on characteristics such as gender, socioeconomic status, and health conditions (Gomez et al., 2022). The results appear to vary across societies and diverse populations, particularly special groups such as individuals with chronic disease. In other words, the findings of the present study showed that teaching Stoic philosophy significantly improves the non-religious dimension of spiritual strategies in dialysis patients but does not have a significant effect on the religious dimension. This finding indicates that the measurement tool was able to detect the distinction between religious and non-religious dimensions. This distinction can be explained based on the secular and philosophical nature of Stoicism. Stoic philosophy is an ethical system grounded in autonomous rationality, not a religion. Religions are based on belief in supernatural and mythological matters. Stoicism, rather than focusing on rituals or connection with the transcendent, emphasizes individual will, control over judgments, and the redefinition of suffering as an opportunity for practicing virtue and strengthening resilience, courage, problem-solving ability, and fortitude. On the other hand, dialysis patients often possess a pre-existing spirituality rooted in religious teachings that have been formed over many years. These beliefs constitute a stable and extensive semantic network intertwined with culture, tradition, family, and community. Religious beliefs are shaped over a long period, and a short-term intervention cannot bring about change in them. Therefore, it can be said that Stoicism does not replace religious strategies but rather complements them and expands the scope of patients' spiritual strategies. In general, Stoic philosophy can teach people who endure long-term suffering, such as patients under hemodialysis, to pursue an authentic life or independence, self-control, self-compassion, reconciliation with oneself, and gratitude for existence (Seneca, 2025). The teachings that the participants learned during this study are such that they have rational and logical support, thus they primarily enhance the non-religious aspect. These teachings force the participant to think and convince them through reasoning, not through acceptance based on faith. For example, in the “trichotomy of control” technique, the patient is taught that suffering and grieving over kidney failure will not change anything, so they must accept this condition and invest their energy in changeable matters, just as a Paralympic athlete accepts their deficiency in certain physical traits, focuses on the changeable aspects of life, and achieves progress. Longer interventions or the integration of Stoic teachings with religious concepts such as forbearance, patience, contentment, and trust in God may also prove effective on the religious dimension.
Strengths and limitations
Key strengths of the current study include the inclusion of a control group by randomized allocation, and follow-up assessments to monitor adherence to the intervention—features that distinguish it from previous research. This study was conducted at a single center in a single city using non-probability sampling; therefore, the findings may not be generalizable. The participants were not blind; thus, awareness regarding the intervention might have influenced the effects. Other limitations of the present study include the small sample size, which increases the likelihood of type II error. Moreover, since the impact of these teachings is dependent on cultural context and socioeconomic characteristics, caution should be exercised in generalizing the findings. Since the questionnaires were completed through self-report, there is a potential for bias. It appears that because these patients struggle with suffering and hardship on a long-term, chronic basis, an eight-week period is insufficient for improving all dimensions of spiritual strategies, and the duration of training should be extended in future studies.
Conclusion
The current study showed that Stoicism can enhance secular spirituality without compromising the religious identity of patients. Although there are historical narrative reviews and studies that are evidence-based regarding the effects of Stoicism on psychological outcomes, there is a lack of sufficient empirical intervention research. Therefore, further experimental intervention studies are recommended across various settings. These studies should examine different psychological indicators in diverse populations, including formal and informal caregivers, patients with chronic illnesses, and students. Additionally, future research should incorporate longer-term follow-up assessments.
Footnotes
Acknowledgements
We would like to present our special thanks to Mrs. Fatemeh Khaledy, nursing manager at the Special Diseases Center in Birjand, Iran. We are also greatly thankful to the Research Committee of Birjand University of Medical Sciences, Iran, for their support during this study.
Ethical considerations
The present study was approved by the Ethics Committee of Birjand University of Medical Sciences (IR.BUMS.REC.1404.26).
Consent to participate
Participants signed written informed consent forms to participate in the study. They were informed that their participation was voluntary and assured that any information they provided would be kept confidential.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
Study design: AM, AB, and MM; Data collection: AM and AB; Analysis and statistics: AM; Manuscript preparation: AM, AB, and MM. All authors approved the final version for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from AM, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission of AM.