
Abstract
To investigate the effects of physical activity on depression and anxiety in heart failure patients. We searched eight major electronic databases covering all records up to December 20th, 2025. The meta-analysis of 46 RCTs (N = 4358) investigated the effects of physical activity on these symptoms. Physical activity was defined as skeletal muscle-induced movement resulting in energy expenditure, encompassing aerobic (walking), resistance (isometric), and mind-body (Tai Chi) forms. The analysis showed physical activity significantly improved depressive and anxiety symptoms. Subgroup analysis revealed combined aerobic-resistance-mind-body training yielded the largest effect for depression, while aerobic-mind-body training was most effective for anxiety. For depression, 4–5 times/week yielded greatest benefits, with ⩽8 weeks as optimal duration. For anxiety, daily physical activity showed largest effect, also with ⩽8 weeks optimal. These findings provide evidence-based references for clinicians to integrate exercise prescriptions into routine psychological care.
Introduction
Heart failure (HF), a clinical syndrome, is the terminal phase of numerous cardiovascular disorders (Bozkurt et al., 2021). With accelerated population aging, recent Lancet reports estimate worldwide HF prevalence at 64.3 million cases, reflecting a 44% increase in incidence across 15 years (GBD 2017 Disease and Injury Incidence and Prevalence Collaborators, 2018; Hao et al., 2019). HF patients typically experience extended illness courses accompanied by significant symptom loads (Lan et al., 2021; Sahlollbey et al., 2020) and impaired psychological health (Rashid et al., 2023).
Symptoms of depression and anxiety were found in more than 50% of patients with HF (Tsabedze et al., 2021). Depression can lead to fatigue, cognitive impairment, and negative self-perception or suicidal thoughts, whereas anxiety may worsen cardiac symptoms, including palpitations and dyspnea. A bidirectional relationship exists between HF and these psychological disorders (Bobo et al., 2020; Rashid et al., 2023). Thus, integrating psychological assessments into routine HF management is essential, and effective interventions should be actively implemented to improve outcomes.
Currently, pharmacological interventions remain the important clinical approach for managing HF patients with comorbid depression (Sbolli et al., 2020). However, these medications frequently induce adverse effects, including somnolence, constipation, and cognitive impairment. Moreover, the use of antidepressants could increase the risk of all-cause death in HF patients (Brouwers et al., 2016; He et al., 2020). Therefore, promoting non-pharmacological therapies is imperative. Cognitive behavioral therapy (CBT) is the most widely used non-drug treatment for depression and is a major psychotherapeutic intervention for anxiety in HF (Balata et al., 2023; Mhanna et al., 2023); however, as its implementation requires significant human resources, developing a more easily disseminable alternative is critical. The American Heart Association (AHA), American College of Cardiology (ACC), and Heart Failure Society of America (HFSA) Guideline recognizes physical activity as an effective non-pharmacological therapy for improving exercise capacity and reducing hospitalization/mortality in HF (Thompson et al., 2024). Furthermore, evidence supports physical activity as an effective, safe, and accessible adjunct intervention for alleviating depression and anxiety across various populations (Li et al., 2023; Wen et al., 2025).
The World Health Organization (WHO) defines physical activity as any bodily movement produced by skeletal muscles that requires energy expenditure (Bull et al., 2020). Numerous studies have investigated the impact of physical activity interventions on depression and anxiety in cardiovascular patients. While some research demonstrates significant improvements in mood symptoms (Chen et al., 2022; Liu et al., 2018; Taylor-Piliae and Finley, 2020), other studies report limited efficacy of physical activity for psychological outcomes in this population (Wrzeciono et al., 2024). A 2014 review demonstrated that physical activity improves depressive symptoms in HF patients (Tu et al., 2014), but subsequent studies have yielded divergent results (Peng et al., 2018; Smolis-Bąk et al., 2015; Teng et al., 2018), necessitating updated evidence synthesis. Evidence for physical activity’s anxiolytic effects in HF is inconsistent, with several trials reporting non-significant results, preventing a definitive consensus (Peng et al., 2018; Teng et al., 2018). Furthermore, studies exhibit significant variability in the type, duration, and frequency of physical activity, which contributes to considerable heterogeneity in findings and leaves the specific effects on depressive and anxiety symptoms in HF patients unclear.
Thus, the objective of this review is to (1) examine the current body of evidence on the influence of physical activity on depression and anxiety in individuals with HF; (2) consider physical activity variables like length, frequency, and type, and explore the effects of training with different characteristics on depression and anxiety in HF patients.
Methods
This systematic review and meta-analysis had been registered in PROSPERO (CRD42024596907). This systematic review follows the PRISMA reporting guidelines (Liberati et al., 2009).
Search strategy
We systematically searched eight electronic databases (PubMed, Web of Science, Embase, Cochrane Central Register of Controlled Trials, CINAHL, CNKI, Wan Fang, and VIP) from database inception through December 20th, 2025, to identify relevant articles. Medical Subject Headings terms, free words, and Boolean operators were used to search for relevant studies. For example, when searching for “heart failure,” we used the subject words “Heart Failure” plus the free words “cardiac failure,” “chronic cardiac failure,” “ventricular dysfunction,” and so on. Furthermore, we examined the reference lists of included studies to locate any other potentially eligible articles. The systematic review considered only studies available in English and Chinese. The detailed search strategy is provided in Supplemental Appendix A.
Inclusion and exclusion criteria
The PICOS framework was applied to screen eligible studies and retrieve full-text articles. The inclusion criteria for this study: (1) patients aged ⩾ 18 years with a diagnosis of HF; (2) the intervention group followed evidence-based physical activity training including aerobic training (e.g. walking, cycling), resistance training (e.g. isometric training), mind-body training (e.g. Tai Chi, Baduanjin), mixed training (aerobic combined with mind-body training, aerobic combined with resistance training, and combined aerobic-resistance-mind-body training), the control group was usual care (e.g. health education); (3) the outcome measures encompassed depression and anxiety, or either one of them; (4) randomized controlled trials. The exclusion criteria: (1) conference papers; (2) studies with insufficient data; (3) republished studies.
Study selection and data extraction
We utilized EndNote 20 to import initially relevant studies and then removed duplicates. Two investigators (AXY and FJL) independently screened titles, abstracts, and full texts for eligibility. A third reviewer (CYR) was consulted to resolve any disputes regarding article inclusion.
Two authors (AXY and CYR) independently extracted study data using a customized extraction template to ensure consistency. The contents mainly included basic information, such as first author, publication date, country, sample size, physical activity parameters (e.g. frequency, type, and duration), and its outcome measure. To ensure data completeness, study authors were contacted when necessary to obtain missing information. Dual independent extraction was followed by systematic cross-checking, and any discordances were adjudicated by an additional reviewer (FJL).
The coding of physical activity interventions was based on established training variables: (1) physical activity type was categorized into aerobic training, resistance training, resistance training, mind-body training, and mixed training (aerobic combined with mind-body training; aerobic combined with resistance training; combined aerobic-resistance-mind-body training); (2) the intervention length was stratified as follows: 8 weeks or less, 9–12 weeks, and more than 12 weeks (Saeed et al., 2019); (3) intervention frequency was categorized into three levels: ⩽3 times, 4–5 times per week, or every day (Exercise at a frequency of 4–5 sessions per week represents “meeting guidelines,” ⩽3 sessions per week is considered “insufficient” and daily exercise constitutes a “high-volume”; Ren and Xiao, 2023; Taylor et al., 2023).
Risk of bias assessment and quality of evidence
Risk of bias assessment was performed in duplicate by two investigators (AXY and CYR) using the Cochrane Risk of Bias 2 (ROB2) tool, assessing six domains: randomization, intervention deviations, missing outcome data, measurement of the outcome, selection of the reported, and overall biases. Using Cochrane standards, bias was rated low, high, or unclear (Sterne et al., 2019). Conflicts were settled by discussion involving a third reviewer (GMJ).
Statistical analysis
We conducted the meta-analysis and subgroup analysis using the package meta in R software version 4.4.1.
Methods of analysis
The outcome measures included in this review were continuous variables. Since different assessment tools were used across the studies to evaluate depression and anxiety, standardized mean differences (SMDs) were utilized to quantify effect sizes, accompanied by 95% confidence interval (CI) calculations.
Heterogeneity was quantified through the I2 statistic, with values <50% considered indicative of acceptable homogeneity. In such cases, fixed-effects models were employed for meta-analysis, while random-effects models were utilized when significant heterogeneity (I2 ⩾ 50%) was detected (Chen et al., 2012).
Assessment of publication bias and sensitivity analysis
Publication bias was assessed using Egger’s regression test when ⩾10 studies were available for meta-analysis (Egger et al., 1997). Studies reporting both anxiety and depression were included in separate meta-analyses. To assess potential unit-of-analysis error, we conducted sensitivity analyses by sequentially excluding one outcome; the pooled effects remained stable, confirming that the overlap did not bias the findings.
Subgroup analysis
Prior to conducting subgroup analysis, we assessed statistical heterogeneity using the I2 statistic. Given the presence of substantial heterogeneity (I2 > 50%, p < 0.1), subgroup analyses were deemed appropriate to explore potential effect modifiers. Additionally, we performed tests for subgroup difference to examine whether the observed effects varied significantly across subgroups. Only variables with a statistically significant test for subgroup differences (p < 0.05) were interpreted as potential moderators. Given the substantial variability across studies in exercise type, frequency, and duration, these factors were prespecified as potential sources of heterogeneity for subgroup analyses. Subgroup analyses examined potential effect modifications by: (a) intervention duration, (b) training frequency, and (c) training type, adopting classification criteria from previous studies.
Results
Study selection
Of the initial 8337 records retrieved 1994 duplicates were eliminated. Subsequent screening yielded 46 studies encompassing 4563 participants for final inclusion, with the selection process visually summarized in Figure 1. Depressive symptoms were reported in 45 studies involving 4325 participants, while anxiety symptoms were reported in 31 studies involving 3295 participants.
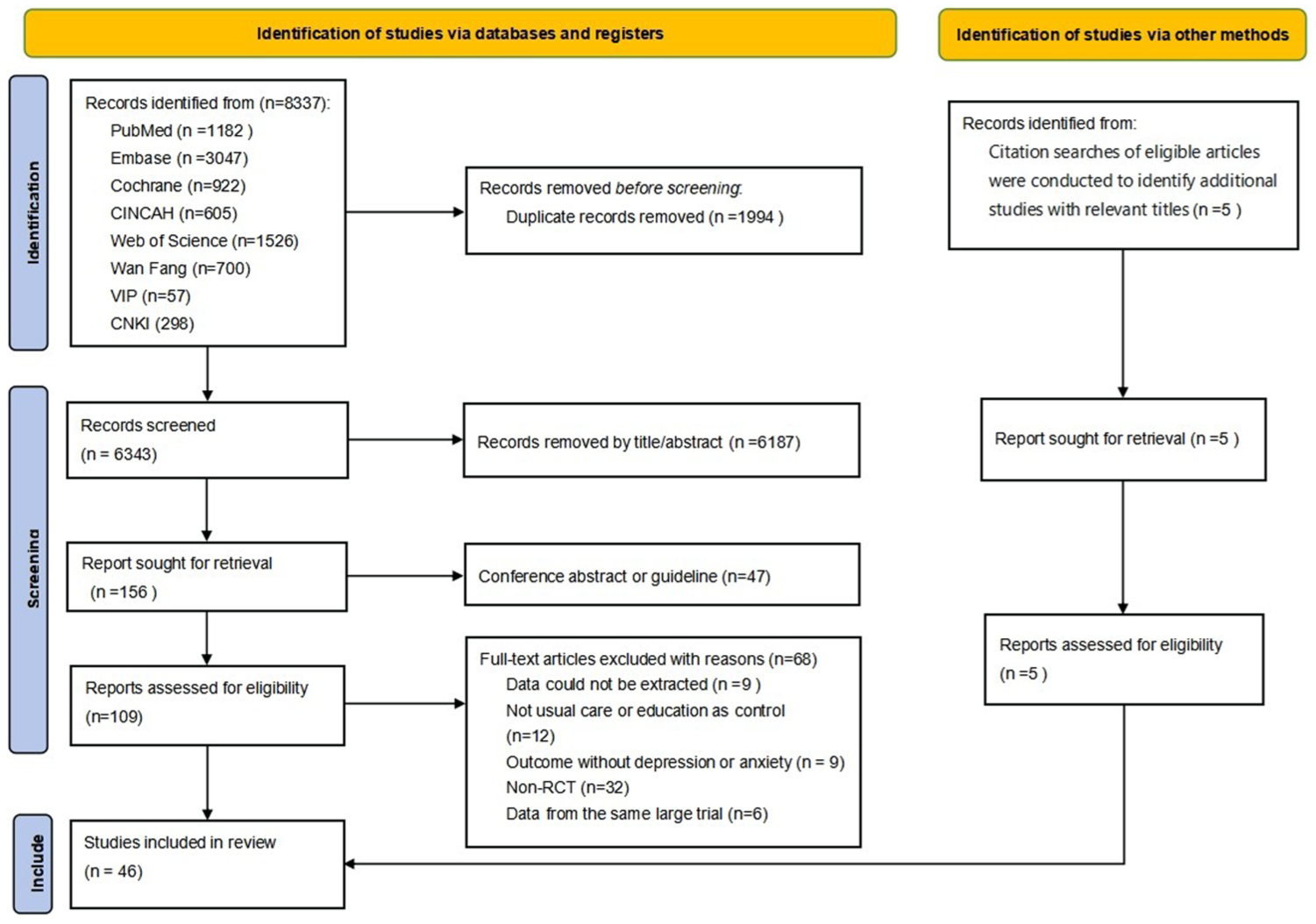
Flow chart of the selection process for this meta-analysis.
Characteristics of the included studies
Study characteristics are presented in Table 1 of Supplemental Appendix A. The publication time frame spanned from 2004 to 2025. Sample sizes varied between 12 and 200 participants. Among the 46 eligible studies, 44 utilized a two-arm design while two employed a three-arm approach.
Intervention and control characteristics
The intervention group’s physical activity modalities were classified as follows: (1) aerobic training (n = 16; Abdelbasset et al., 2019; Gary, 2006; Gary and Lee, 2007; Han, 2022; Hu et al., 2008; Kulcu et al., 2007; Li, 2012; Luo et al., 2019; Mao et al., 2020; Re, 2018; Teng et al., 2018; van Den Berg-Emons et al., 2004; Vetrovsky et al., 2024; Wang et al., 2022; Wu, 2020; Yu, 2023); (2) mind-body training (n = 7) (Barrow et al., 2007; Huang, 2023; Li et al., 2022a; Shan et al., 2023; Yang et al., 2024; Yu et al., 2024; Yuan, 2017); (3) mixed training (n = 20): aerobic combined with resistance training (n = 10; Chien et al., 2011; Duncan et al., 2014; Evangelista et al., 2006; Gary et al., 2012; Ji et al., 2019; Jolly et al., 2009; Koukouvou et al., 2004; Nolte et al., 2015; Norman et al., 2020; Peng et al., 2018) and aerobic combined with mind-body training (n = 6; Chen, 2023; Li et al., 2022b; Pang, 2023; Shen et al., 2018; Tang and Cai, 2010; Zhang, 2024), combined aerobic-resistance-mind-body training (n = 4; Shen, 2022; Song and Zhang, 2022; Zhang et al., 2022; Zhou, 2025), (4) resistance training (n = 1; Smolis-Bąk et al., 2015), and no specific mention of the training (n = 2) (Chen et al., 2020; Zeng, 2020).
The control group received routine care, including medication guidance, health education, and exercise instruction without regular physical activity monitoring, contrasting with the intervention group.
The analyzed interventions exhibited considerable variability in their duration and frequency. The duration of the exercise intervention was defined as the period from the initiation of the intervention to the measurement of the outcome indicators, while training duration spanned 3–48 weeks, with the majority (n = 19) implementing 12-week programs. Session frequency ranged from 1 to 7 days per week, with daily training (n = 15) constituted the most common frequency protocol.
Measured outcomes
The outcome measures included both depression and anxiety. Specifically, 15 studies assessed depression exclusively, one study assessed anxiety exclusively, and 30 studies measured both depression and anxiety. Of the included studies, 5 used the Hamilton Depression Rating Scale (HAMD); 2 used the Hamilton Anxiety Rating Scale (HAMA); 5 used the Beck Depression Inventory (BDI); 1 used the Patient-Reported Outcomes Measurement Information System-29 (PROMIS-29); 5 used the Patient Health Questionnaire-9 (PHQ-9); 4 used the Generalized Anxiety Disorder-7 (GAD-7); 1 used the State-Trait Anxiety Inventory (STAI); 2 used the Geriatric Depression Scale (GDS); 1 used the Multiple Affect Adjective Checklist (MAACL); 1 used the Symptom Checklist-90 (SCL-90); 16 used the Self-Rating Depression Scale (SDS); 11 used the Self-Rating Anxiety Scale (SAS); 8 used the Hospital Anxiety and Depression Scale (HADS); and 1 used the Profile of Mood States (POMS). The included studies administered the respective scales to assess depression and anxiety both before and after the intervention.
Risk of bias of included studies
The risk-of-bias assessment (Figure 2(a)) found that most included studies (89.1%) raised some concerns, while a small number (4.3%) were high risk, primarily due to flaws in randomization and intervention protocols. The detailed risk of bias assessments for individual studies are presented in Figure 2(b).
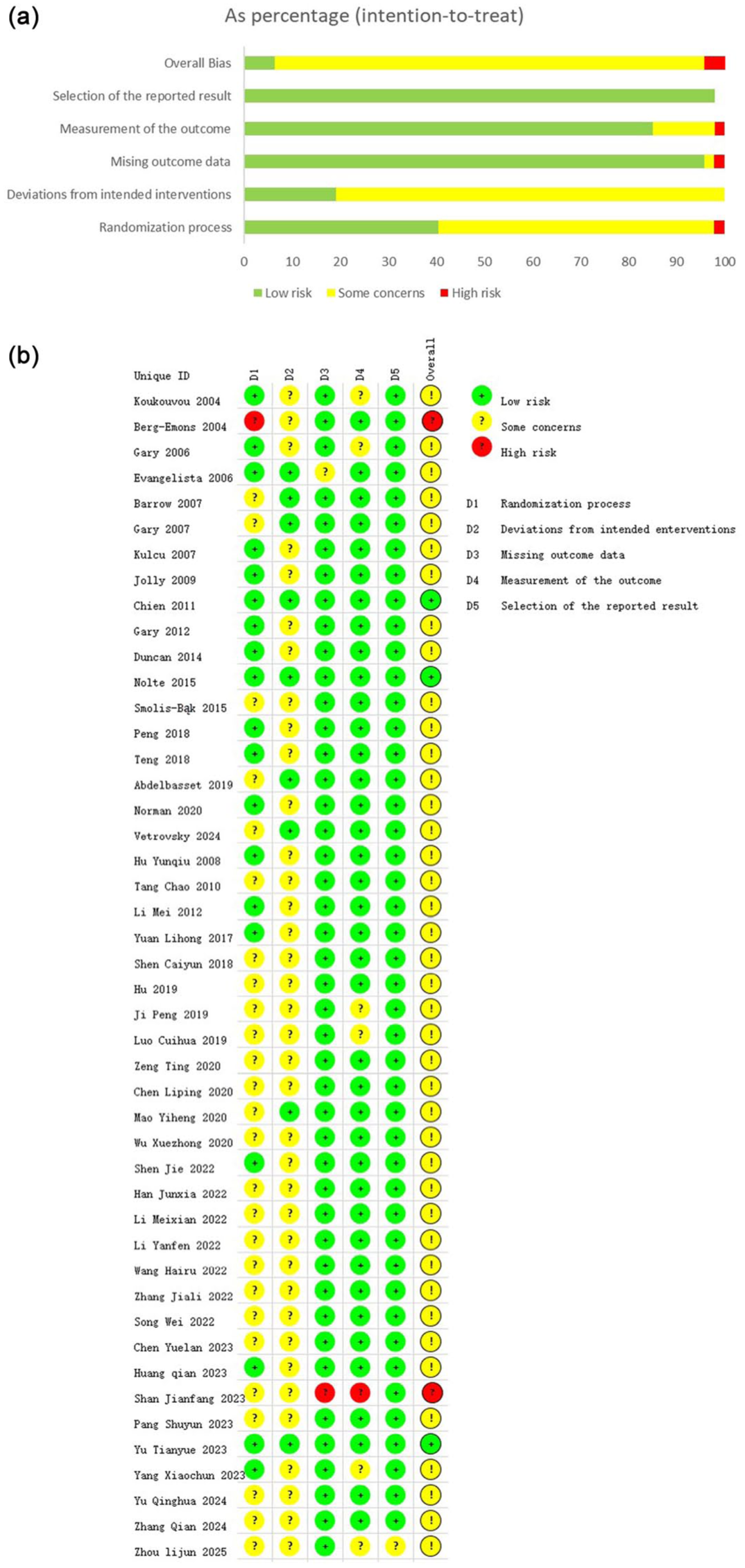
(a) Risk of bias graph of the included study. (b) Risk of bias summary of included study.
The overall effect test of the physical activity intervention
Depression
As shown in Figure 3, the meta-analysis of 45 studies revealed that physical activity interventions significantly improved depressive symptoms (n = 4325, SMD = −0.91, p < 0.001, I2 = 93.2%; Figure 3).
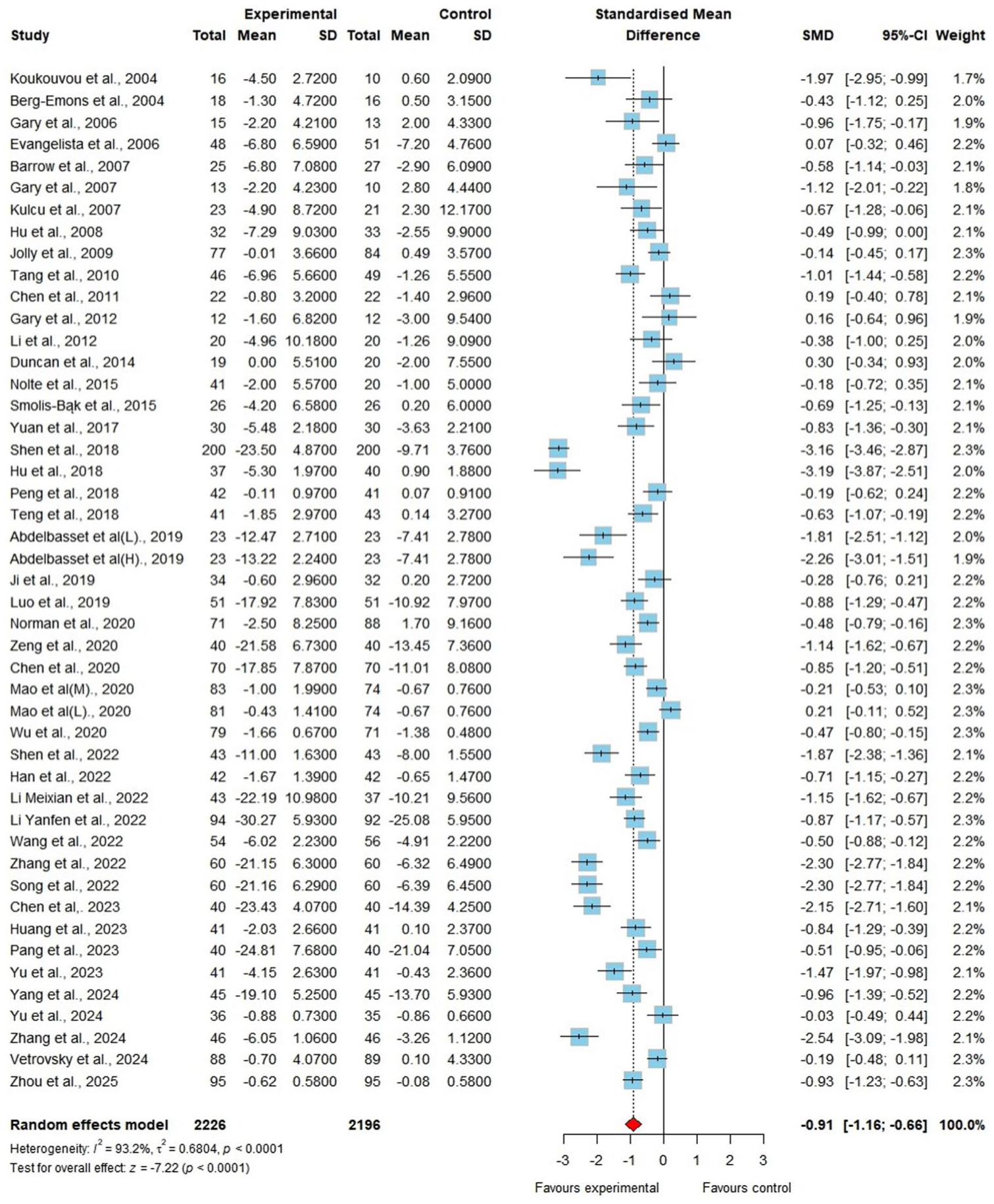
Forest plot of exercise in depression.
Anxiety
A total of 3295 participants across 31 studies evaluated the impact of physical activity on anxiety symptoms. Results indicated statistically meaningful improvements in anxiety symptoms (n = 3295, SMD = −0.87, p < 0.001, I2 = 95.6%; Figure 4).
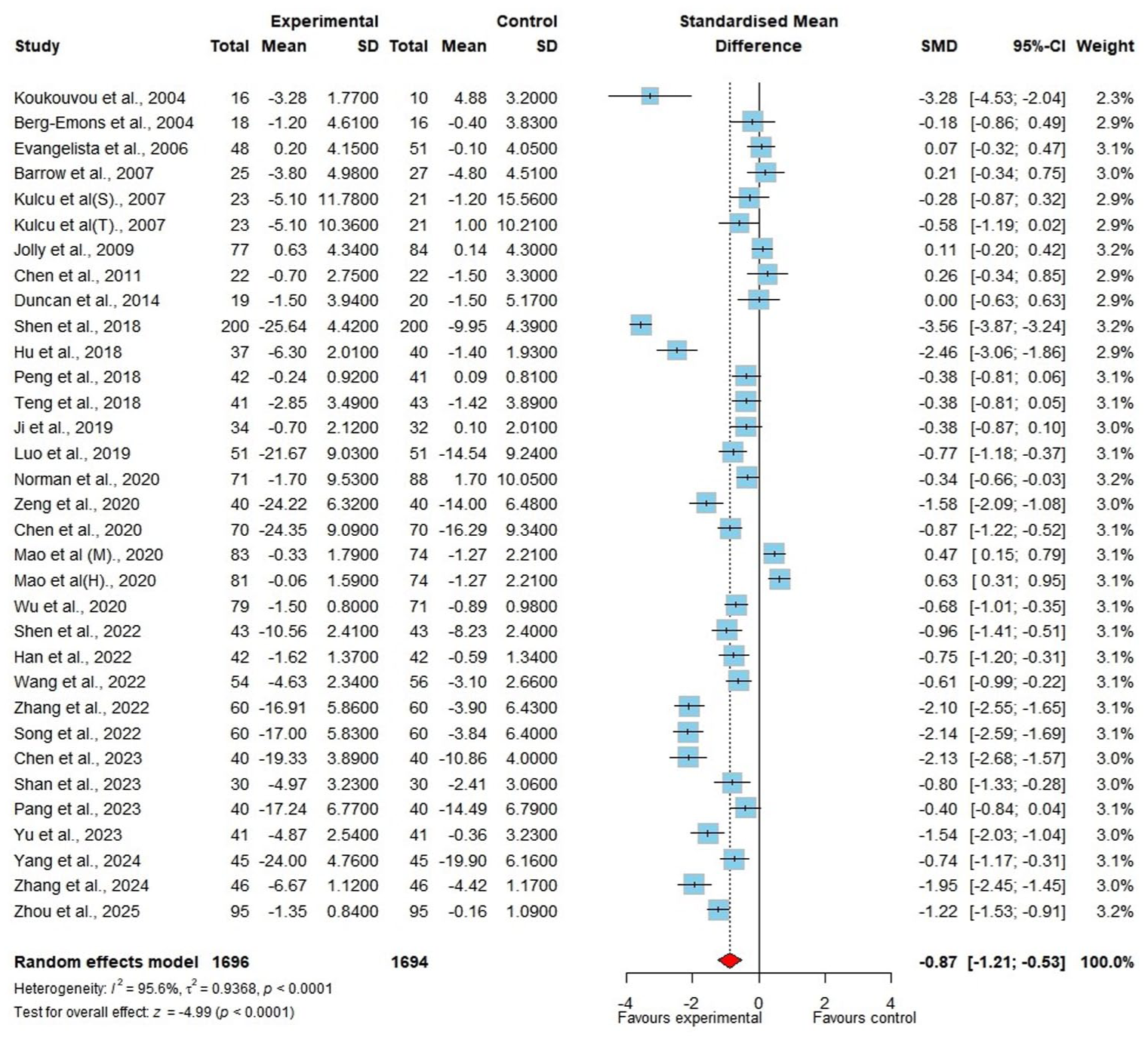
Forest plot of exercise in anxiety.
Results of subgroup comparisons
Subgroup analysis of physical activity interventions for improving depression
Physical activity type
Among the included studies, 16 implemented aerobic training, six employed mind-body training, 10 utilized a combination of aerobic and resistance training, six adopted an approach combining aerobic and mind-body training, an additional four adopted a program combined aerobic-resistance-mind-body training, only one study used resistance training, therefore, meta-analysis was not performed, and two studies did not specific the type of physical activity. The test for subgroup differences indicated a statistically significant interaction (p < 0.001). Notably, combined aerobic-resistance-mind-body training modalities exhibited the most effect on alleviating depression (SMD = −1.83, p < 0.001, I2 = 92.1%), and aerobic training (SMD = −0.86, p < 0.001, I2 = 88%) and mind-body training (SMD = −0.73, p < 0.001, I2 = 62.5%) also improved depressive symptoms in HF patients. No significant improvement in depressive symptoms was observed with hybrid aerobic-resistance training programs.
Physical activity length
The intervention length distribution was as follows: 10 studies implemented programs lasting ⩽8 weeks; 21 studies employed 9–12-week interventions; 12 studies examined programs exceeding 12 weeks; two studies did not report specific length. The most pronounced reductions in depressive symptoms occurred with physical activity interventions lasting under 8 weeks (SMD = −1.23, p < 0.001, I2 = 96.7%). Compared to other lengths, the 9–12 weeks training (SMD = −0.78, p < 0.001, I2 = 85.9%) period yielded the smallest effects. But the test for subgroup differences revealed no statistically significant interaction for length (p = 0.488).
Physical activity frequency
In terms of frequency, 15 interventions involved ⩽ 3 times/week, 15 employed 4–5 times/week, and 15 consisted of daily training. The test for subgroup differences indicated a statistically significant interaction (p = 0.004). Meta-analysis revealed that the smallest effect size occurred with ⩽3 times/week, while the largest antidepressant effect was observed at 4–5 sessions/week (SMD = 1.21, p < 0.001, I2 = 92.1%).
Subgroup analysis of physical activity interventions for improving anxiety
Physical activity type
The training modalities comprised aerobic training (n = 10), aerobic combined with mind-body training (n = 4), aerobic combined with resistance training (n = 8), mind-body training (n = 3), combined aerobic-resistance-mind-body training (n = 4), and two studies did not specify the training type. The test for subgroup differences indicated a statistically significant interaction (p = 0.001). Aerobic combined with mind-body training (SMD = −2.01, p < 0.001, I2 = 91.0%) demonstrated the most largest improvement in anxiety symptoms. In contrast, the meta-analysis revealed that mind-body training and aerobic combined with resistance training did not demonstrate statistically significant improvements in anxiety symptoms.
Physical activity length
Intervention lengths were distributed as follows: ⩽8 weeks (n = 8), 9–12 weeks (n = 10), and >12 weeks (n = 11), with two studies not reporting length data. Training interventions lasting ⩽ 8 weeks demonstrated the largest effect size for anxiety symptom reduction (SMD = −1.14, p < 0.001, I2 = 97.2%), with interventions lasting 9–12 weeks showing the smallest effects. But the test for subgroup differences revealed no statistically significant interaction for length (p = 0.504).
Physical activity frequency
The test for subgroup differences indicated a statistically significant interaction (p < 0.001). For anxiety symptom improvement, daily training demonstrated optimal efficacy (SMD = −1.23, p < 0.001, I2 = 96.9%). However, frequencies below three weekly sessions failed to produce clinically meaningful anxiety reduction.
Detailed forest plots and table of all subgroup analyses are included in Supplemental Appendix B.
Publication bias and sensitivity analysis
Publication bias was assessed via funnel plots and Egger’s test. Funnel plot symmetry and Egger’s regression test both suggested the absence of significant publication bias. Additionally, to evaluate result stability, we conducted sensitivity analyses employing an item-by-item approach. The robustness of meta-analytic results was evidenced by invariant effect sizes across all leave-one-out iterations for both depression and anxiety outcomes (Supplemental Appendix C).
Discussion
We conducted an exhaustive systematic review investigating physical activity programs and their operational parameters for alleviating depression and anxiety in HF patients. The meta-analytic evidence consistently supported physical activity’s significant antidepressant and anxiolytic effects in this population. Subgroup analysis revealed that varying physical activity frequencies and lengths significantly improved depressive symptoms in HF patients. Combined aerobic-resistance-mind-body training demonstrated the most substantial benefit, with optimal outcomes observed at a frequency of 4–5 sessions per week combined with short-term interventions. Regarding anxiety, the largest effect sizes were observed with combined aerobic and mind-body training, particularly when interventions lasted less than 8 weeks.
Effect of physical activity training on depression
This meta-analysis demonstrates that training alleviates depression in HF patients by reducing psychological stress and improving mood, consistent with previous findings (Fan et al., 2024; Schuch et al., 2016). In cardiovascular patients, exercise alleviates depression through dual pathways: by promoting long-term cardiovascular adaptation to enhance functional capacity (Wang et al., 2025), and by modulating the renin-angiotensin-aldosterone system (RAAS) to improve cardiac recovery (Baffour-Awuah et al., 2024).
Subgroup analysis of physical activity’s impact on depressive symptoms
Physical activity training types
Our findings demonstrate that compared to other types of training, combined aerobic-resistance-mind-body interventions were more effective than other types for relieving depression in HF.
Cardiovascular Exercise Guidelines specifically recommend regular aerobic training for patients with chronic HF (Taylor et al., 2023). Of particular significance is the 2004 designation by the National Institutes of Health (NIH) recognizing mind-body training as a distinct category within complementary and alternative medicine (CAM) systems (Barnes et al., 2004). Mind-body training, a low-intensity therapeutic approach, systematically integrates physical activity with mindfulness or meditation. Evidence demonstrates its significant efficacy in alleviating depression among patients with limited mobility or impaired exercise capacity (Chen et al., 2024b).
Comparative effectiveness analysis demonstrated that integrated training programs produced larger effect sizes for depression reduction than singular exercise modalities, consistent with Yu’s earlier reports (Yu et al., 2022). Clinically, personalized, multimodal exercise regimens (aerobic, resistance, and mind-body) optimize depression management by more effectively addressing its multifactorial etiology compared to single-modality interventions.
Frequency and length of physical activity training
The results demonstrate that a training frequency of 4–5 sessions/week yields optimal outcomes. Moderate-intensity exercise with appropriate inter-session intervals appears optimal for antidepressant effects in HF patients. Optimal health benefits appear to follow a dose-response relationship, with moderate training volumes demonstrating significant efficacy, whereas excessive exercise may paradoxically attenuate therapeutic gains (Tian et al., 2024). While there was some numerical variation in effect sizes across length subgroup, the non-significant tests for subgroup differences suggest that these variations are likely attributable to sampling error rather than true differences in efficacy.
Effect of physical activity training on anxiety
Our meta-analysis confirms training reduces anxiety in HF, aligning with Chen et al. (2024a). Most patients with HF perceive their disease progression as uncontrollable, often experiencing anxiety and distress, which negatively impacts treatment adherence and clinical outcomes (Rashid et al., 2023). Empirical evidence has established physical activity as an effective non-pharmacological intervention for anxiety reduction across diverse populations (Schmitt et al., 2019; Wegner et al., 2014).
Potential mechanisms for exercise-induced anxiolysis include: (1) HPA Axis Regulation: Exercise induces plasticity in this key stress-response pathway (Lopresti et al., 2013). (2) BDNF Upregulation: Exercise increases this crucial neurotrophic factor in the hippocampus (Liu and Nusslock, 2018). (3) Enhanced Neurogenesis/Angiogenesis: Exercise promotes the growth of new neurons and blood vessels in the brain (Morgan et al., 2019). (4) Inflammatory Homeostasis: Exercise helps restore balanced inflammatory signaling (Michopoulos et al., 2017). While the proposed mechanisms are likely interdependent and collectively contribute to the anxiolytic effects of exercise in HF patients, it is plausible that inflammatory homeostasis and HPA axis regulation serve as upstream triggers (Slusher and Acevedo, 2023).
Subgroup analysis of physical activity’s impact on anxiety symptoms
Physical activity training types
The present findings demonstrate that the combined aerobic and mind-body training regimen yielded superior therapeutic efficacy in ameliorating anxiety symptoms compared to unimodal interventions. Some scholars (Hautala et al., 2009; Singh et al., 2023) propose that aerobic training can serve as a functional biomarker for assessing whether autonomic nervous system (ANS) activity remains within optimal physiological ranges. Clinical evidence has established mind-body training–characterized by its gentle, deliberate movements–as an effective intervention for anxiety symptom reduction (Li et al., 2019). Combining mind-body with aerobic training not only improves a range of physiological symptoms in patients with HF but also plays a crucial role in mitigating their anxiety symptoms.
Mind-body training showed no significant anxiolytic effects in our study, contrasting with prior evidence (Dong et al., 2024; Wu et al., 2025). This may be attributed to the following factors: (1) This may be attributed to the fact that mind-body training emphasizes internal awareness, requiring participants to maintain a high level of attentional focus to achieve optimal therapeutic effects (Klompstra et al., 2025). (2) Given the inclusion of only three mind-body training studies, the findings require cautious interpretation and warrant validation through future high-quality RCTs.
Frequency and length of training intervention
The results demonstrate that when the training frequency is fewer than three sessions per week, the improvement in anxiety symptoms lacks statistical significance. However, all intervention durations examined demonstrated significant benefits, suggesting that regular, frequent exercise stimulation may be more important than total program length for achieving anxiety relief. The observed limitations may be attributed to prolonged inter-session intervals, which may attenuate habit formation and psychological reward mechanisms (Stubbs et al., 2017). Additionally, although the point estimates varied across duration subgroups, there was an absence of significant subgroup differences. This indicates the robustness of physical activity interventions for anxiety across different durations.
Practical implications
The synthesis demonstrates that physical activity training provides clinically meaningful improvements in depression and anxiety for HF, supporting its integration into management strategies as an evidence-based adjunctive therapy.
Strengths or limitations
This review synthesizes recent evidence for physical activity on depression and is the first to examine its impact on anxiety in HF patients. However, this review has several limitations. First, the characteristics of the interventions included in the study were not fully standardized, with variations in physical activity type, duration, and frequency. Although subgroup analyses were conducted to mitigate this effect, the heterogeneity of interventions across studies still led to substantial heterogeneity, which may affect the results. Future research could further explore additional sources of heterogeneity using meta-regression. Additionally, restricting our search to Chinese and English publications may have introduced a language bias, potentially limiting the comprehensiveness of our findings. Future reviews incorporating multilingual searches are warranted to build upon and enhance this evidence base. Moreover, most included studies were conducted in China, likely because traditional Chinese exercises place emphasis on mind-body cultivation through slow, focused movements, thereby potentially enhancing their positive effects on emotional improvement.
Conclusion
This systematic review demonstrates that physical activity alleviates both depressive and anxiety symptoms in HF patients. The comparative analysis indicates that mixed-mode exercise demonstrates superior efficacy over single-mode exercise in ameliorating symptoms of depression and anxiety. Furthermore, adequate exercise frequency must be maintained to achieve optimal therapeutic outcomes. These results indicate that tailored training programs not only enhance cardiovascular health but also improve mood disturbances in this population. Future network meta-analyses are needed to directly compare training modalities and determine the optimal approach.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261457620 – Supplemental material for Effects of physical activity on anxiety and depression symptoms in patients with heart failure: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-1-hpq-10.1177_13591053261457620 for Effects of physical activity on anxiety and depression symptoms in patients with heart failure: A systematic review and meta-analysis of randomized controlled trials by Xingyue An, Yongrui Cao, Jianglin Fan, Meijia Gao and Shaoying Du in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053261457620 – Supplemental material for Effects of physical activity on anxiety and depression symptoms in patients with heart failure: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-2-hpq-10.1177_13591053261457620 for Effects of physical activity on anxiety and depression symptoms in patients with heart failure: A systematic review and meta-analysis of randomized controlled trials by Xingyue An, Yongrui Cao, Jianglin Fan, Meijia Gao and Shaoying Du in Journal of Health Psychology
Supplemental Material
sj-docx-3-hpq-10.1177_13591053261457620 – Supplemental material for Effects of physical activity on anxiety and depression symptoms in patients with heart failure: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-3-hpq-10.1177_13591053261457620 for Effects of physical activity on anxiety and depression symptoms in patients with heart failure: A systematic review and meta-analysis of randomized controlled trials by Xingyue An, Yongrui Cao, Jianglin Fan, Meijia Gao and Shaoying Du in Journal of Health Psychology
Footnotes
Ethical considerations
This systematic review of previously published literature involved no direct contact with human participants; therefore, ethical approval was not required, and review was conducted and reported in accordance with PRISMA.
Consent to participate
As this study does not involve the collection of primary data from human participants, the concept of obtaining informed consent from individual patients or participants is not applicable.
Consent for publication
Consent for publication is not applicable to this review article as no identifiable participant data are included.
Author contributions
Xingyue An: Writing–review & editing, Writing–original draft, Methodology, Data curation, Conceptualization. Yongrui Cao: Methodology, data curation. Jianglin Fan: Methodology, Data curation. Meijia Gao: Data curation, Supervision. Shaoying Du: Validation, Supervision, Conceptualization, Writing–review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Medical Science Foundation of Hebei University under Grant [number 2021B13]. The funding body had no role in the design of the study, collection, analysis, interpretation of data, or in writing the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Date availability statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study. All data underlying the conclusions drawn in this systematic review are available from the original studies cited in the reference list.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.