
Abstract
This mixed-methods study examines religion’s dual role in postpartum depression (PPD) among 350 Pakistani women. Quantitative findings indicate that positive religious coping strategies, such as Tawakkul and Sabr, were associated with reduced PPD severity, whereas negative religious coping predicted higher symptom severity, mediated by internalized stigma. Qualitative interviews with 45 participants revealed recurring themes of spiritual guilt, the paradox of the “Ideal Muslim Mother,” and tensions between faith-based meanings of suffering and biomedical mental health care. While religious beliefs provided comfort, meaning, and resilience for many women, they also contributed to moral pressure and self-blame that pathologized psychological distress. The study proposes the Sacred Strain Model, highlighting religion as both a protective resource and a potential burden. Findings underscore the need for culturally and religiously congruent maternal mental health interventions that integrate Islamic frameworks alongside clinical care to promote equitable and sustainable postpartum mental health support in Pakistan.
Introduction
Postpartum depression (PPD) affects an estimated 25%–36% of mothers in Pakistan, a prevalence markedly exceeding global averages and representing a critical, under-addressed public health priority (Husain et al., 2017; Zahidie and Jamali, 2021). This disparity underscores the powerful influence of sociocultural context on the etiology, experience, and management of perinatal mental distress. In Pakistan, religion—predominantly Islam—transcends the domain of personal belief to function as a pervasive cultural scaffolding. It structures fundamental aspects of worldview, social organization, gender norms, and the very language of emotion and coping (Aslam and Ali, 2020). For women, this interweaving is particularly profound. Religious prescriptions are inextricably linked to societal constructs of femininity, maternal duty, and family honor (izzat). Motherhood is sacralized, framed not only as a biological and social role but as a spiritual vocation and test (imtihan; Nadir, 2018). The archetype of the “ideal Muslim mother” is one characterized by selfless sacrifice (qurbani), unwavering gratitude (shukr), and resilient patience (sabr). While providing a noble template, this ideal can inadvertently pathologize normative emotional turbulence, framing feelings of exhaustion, despair, or ambivalence as indicators of spiritual deficiency or moral failing.
Health psychology has extensively documented the generally salubrious effects of religious involvement on well-being, identifying primary mechanisms such as meaning-making, provision of social support, promotion of healthy behaviors, and fostering a sense of perceived control or comfort (Koenig, 2012; Pargament, 2011). Pargament’s influential model further refines this understanding through the Brief RCOPE, distinguishing between positive religious coping (PRC: e.g. seeking spiritual connection, benevolent religious reappraisal, collaborative religious coping) and negative religious coping (NRC: e.g. spiritual discontent, punishing God reappraisals, interpersonal religious discontent; Pargament et al., 2011). A robust literature confirms that NRC is consistently associated with poorer mental and physical health outcomes across diverse populations.
However, this binary, primarily individualistic model requires critical contextualization within collectivistic, theocentric societies like Pakistan. Here, religion is less a chosen coping resource and more an inherent, omnipresent facet of reality. Spiritual struggle—defined as tension, fear, or conflict concerning sacred matters—may thus arise not from a lapse of personal faith, but from the profound dissonance experienced when one’s internal reality (e.g. depressive symptoms) clashes with powerful, externally mandated religious and social ideals (Abu-Raiya, 2013; Exline, 2013). The communal nature of religious life means that such struggles are rarely private; they are subject to familial and communal surveillance, where perceived failure carries social repercussions.
This study proposes and tests the “Sacred Strain” model. This model posits that for Pakistani women navigating PPD, religion operates as a dual-axis system. On the resource axis, it provides a culturally resonant, resilient framework for meaning-making (interpreting suffering as a test), emotional regulation (through rituals like prayer (salah), supplication (dua)), and access to tangible social support via religious communities. On the burden axis, it can impose a unique moral-emotional load, where depressive symptoms are cognitively appraised as spiritual failure (naqs-e-iman), divine punishment (saza), or vulnerability to supernatural harm (nazar, jinn). This appraisal fuels internalized stigma and actively deters engagement with biomedical or psychological help-seeking, which is often stigmatized as a secular, Western import antithetical to faith. Thus, this investigation asks: How do positive and negative religious coping strategies interact with entrenched socio-religious norms to predict PPD severity, internalized stigma, and help-seeking pathways among Pakistani women? By employing a mixed-methods design, we seek not only to quantify these relationships but to richly illuminate the lived experience of this sacred strain.
Theoretical framework
This study is grounded in a multi-layered theoretical framework that integrates psychological, cultural, theological, and sociological perspectives. Specifically, it draws upon Pargament’s Theory of Religious Coping (2011) and Syed’s Gender–Cultural Model of Pakistani Mental Health (2018), while being further informed by Critical Feminist Theology in an Islamic context (Wadud, 1999) and Sociocognitive Models of Stigma (Corrigan et al., 2012). Together, these frameworks provide a comprehensive lens for understanding how religious meaning-making, gendered cultural structures, and stigma interact to shape women’s mental health experiences in Pakistan.
First, Pargament’s Theory of Religious Coping conceptualizes religion not as a static or uniformly beneficial force, but as a dynamic system through which individuals seek to conserve existing meanings or transform them in response to stress and adversity. By distinguishing between positive religious coping (PRC) and negative religious coping (NRC), the theory allows for a nuanced examination of how specific religious beliefs and practices function as coping mechanisms with distinct psychological outcomes. This framework is particularly valuable for empirically testing the hypothesized differential pathways through which PRC and NRC influence mental health outcomes in this study.
Second, Syed’s Gender–Cultural Model of Pakistani Mental Health situates these coping processes within the socio-cultural realities of Pakistan. The model highlights how patriarchal gender norms, mehram–ghair mehram boundaries, extended family systems (sasural), and culturally embedded interpretations of Islamic jurisprudence (fiqh) generate unique psychosocial pressures for women. At the same time, these structures prescribe socially acceptable—often religiously framed—modes of coping and emotional expression. This framework underscores the importance of contextual variables such as family structure, educational background, and regional culture as key moderators shaping women’s mental health trajectories.
Third, Critical Feminist Theology within an Islamic framework provides an interpretive lens through which the gendered deployment of religious texts and traditions can be critically examined. Rather than treating religion as inherently oppressive or liberatory, this approach draws attention to how patriarchal readings of religious sources may be mobilized to reinforce normative expectations surrounding women’s social, domestic, and maternal roles. Within this study, it is particularly useful for theorizing the “Ideal Muslim Mother” paradox, wherein religious ideals intended to confer moral value and purpose may simultaneously intensify guilt, self-surveillance, and psychological strain.
Finally, the Sociocognitive Model of Stigma elucidates the mechanisms through which societal attitudes toward mental illness become internalized by individuals. According to this model, public stigma—manifested through moralizing or religiously inflected stereotypes—can evolve into self-stigma, characterized by shame, diminished self-worth, and reduced self-efficacy. This internalization often produces the well-documented “why try?” effect, whereby individuals disengage from help-seeking and treatment. In the present study, this framework is essential for understanding how NRC and prevailing socio-religious norms contribute to treatment avoidance and sustained psychological distress among women. Taken together, this integrated theoretical framework enables a context-sensitive analysis of women’s mental health in Pakistan by linking individual religious coping strategies with broader gendered, cultural, and stigmatizing social processes.
Hypotheses
Method
Research design
This study employed a sequential explanatory mixed-methods design (QUAN → QUAL), consistent with established methodological guidance for theory-building and contextual explanation (Creswell and Plano Clark, 2018). The design comprised two analytically connected phases. Phase 1 (Quantitative) utilized a cross-sectional survey to test hypothesized mediation and moderation pathways between religiosity, religious coping, stigma, and postpartum depression (PPD) severity at the population level. Phase 2 (Qualitative) followed with in-depth phenomenological interviews designed to explain, contextualize, and elaborate upon quantitative patterns by exploring participants’ lived experiences, meaning-making processes, and culturally embedded mechanisms.
Integration occurred at the interpretive stage, where qualitative themes were explicitly mapped onto quantitative pathways to generate a contextualized explanatory framework.
Participants and procedure
Phase 1: Quantitative component
Sample characteristics
The quantitative sample consisted of 350 postpartum women who were between 2 and 12 months postpartum. This timeframe was selected to capture both early-onset and delayed presentations of PPD while ensuring participants had passed the immediate postpartum physiological recovery period (commonly referred to as chilla).
Recruitment strategy
Participants were recruited using purposive sampling from maternity wards and pediatric vaccination clinics in:
Lahore (n = 120)
Karachi (n = 120)
Peshawar (n = 110)
Recruitment sites included three major public-sector hospitals and two well-established private hospitals. The inclusion of Peshawar was methodologically intentional to capture the distinct religio-cultural interface of Pashtunwali within Khyber Pakhtunkhwa.
Inclusion criteria
Participants were eligible if they:
Were 18 years or older
Identified as Muslim
Were residing with their infant
Were proficient in Urdu or Pashto (with translator assistance when required)
Were capable of providing informed consent
Exclusion criteria
Participants were excluded if they exhibited:
Active psychotic symptoms
Acute suicidal ideation requiring immediate clinical intervention
Severe cognitive impairment as identified by attending clinical staff
Data collection procedure
Following approval from the relevant Institutional Review Boards, eligible participants were approached by a trained female research assistant. The study aims and procedures were explained verbally and in writing, and written informed consent was obtained. Questionnaires were administered in a private setting. To accommodate varying literacy levels, instruments were read aloud when necessary. Completion time averaged 40–50 minutes. Participants received a non-coercive compensatory gift pack (infant care items) valued at PKR 500.
Phase 2: Qualitative component
Sub-sample selection
A purposive sub-sample of 45 women was selected from Phase 1 using a maximum variation strategy based on:
i. PPD severity (high vs low EPDS scores)
ii. Negative religious coping (high vs low NRC)
iii. City (Lahore, Karachi, Peshawar)
iv. Family structure (nuclear vs joint)
v. Education level
vi. Sectarian affiliation (Sunni/Shia)
This approach enhanced the analytic depth and transferability of qualitative findings.
Interview procedure
Participants were re-contacted and invited to participate in semi-structured, in-depth interviews lasting 60–120 minutes. Interviews were conducted in Urdu or Pashto, according to participant preference, by a clinically trained female psychologist.
All interviews were audio-recorded with permission, transcribed verbatim, and translated into English by a bilingual expert. Back-translation procedures were employed to ensure semantic and conceptual accuracy (Brislin, 1980).
Quantitative measures
Table 1 provides an overview of all quantitative instruments used in the study.
Overview of all quantitative instruments.
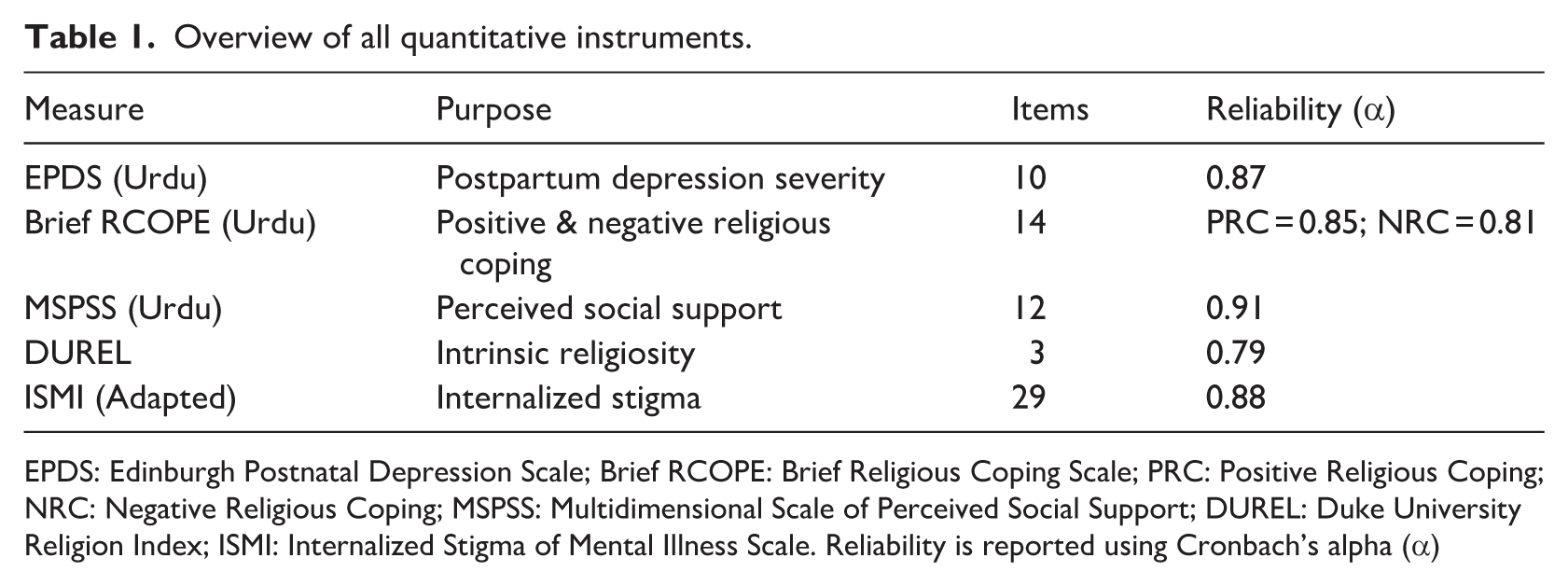
EPDS: Edinburgh Postnatal Depression Scale; Brief RCOPE: Brief Religious Coping Scale; PRC: Positive Religious Coping; NRC: Negative Religious Coping; MSPSS: Multidimensional Scale of Perceived Social Support; DUREL: Duke University Religion Index; ISMI: Internalized Stigma of Mental Illness Scale. Reliability is reported using Cronbach’s alpha (α)
Quantitative measures, purpose, and psychometric properties
Instrument descriptions
Edinburgh Postnatal Depression Scale (EPDS) A 10-item, Urdu-validated screening tool assessing depressive symptoms over the past 7 days. Scores range from 0 to 30, with a cut-off score of ⩾13 indicating probable major depression in South Asian populations (Husain et al., 2017).
Brief RCOPE (Urdu Version) A 14-item measure assessing positive religious coping (PRC) and negative religious coping (NRC). The scale was translated using forward–backward procedures with committee review and cognitive interviewing.
Multidimensional Scale of Perceived Social Support (MSPSS) Assesses perceived support from family, friends, and significant others. The Urdu version demonstrates strong construct validity (Rafiq et al., 2017).
Duke University Religion Index (DUREL) A five-item measure of organizational, non-organizational, and intrinsic religiosity. The intrinsic religiosity subscale served as the primary religiosity predictor.
Internalized Stigma of Mental Illness Scale (ISMI – Adapted) Modified to assess stigma related to “postpartum emotional problems.” Items were reviewed by Pakistani mental health experts for cultural relevance.
Demographic and Religious Proforma Collected data on age, parity, education, income, family structure, ethnicity, sect, prayer frequency, and engagement with spiritual healers (pirs).
Qualitative interview guide
The interview guide was flexible and iterative, allowing emergent themes:
Narrative Opening “Can you tell me about your emotional experience since your baby was born?”
Religious Worldview and Coping “When you face emotional distress, how does your faith help or affect you?”
Meaning-Making of Distress “How do you understand these feelings? Have you discussed them in a religious setting?”
The Ideal versus the Real Mother “What does being a ‘good Muslim mother’ mean to you?”
Help-Seeking Pathways
“What kinds of help have you considered—medical, spiritual, or both?”
Cultural Context (KP only) “How does Pakhtunwali influence how emotional difficulties are handled?”
Analytic strategy
Quantitative data were analyzed using structural path analysis, testing mediation and moderation effects. Qualitative data were analyzed using Interpretative Phenomenological Analysis (IPA), following Smith et al. (2009). Integration was achieved through theoretical triangulation (Figure 1).
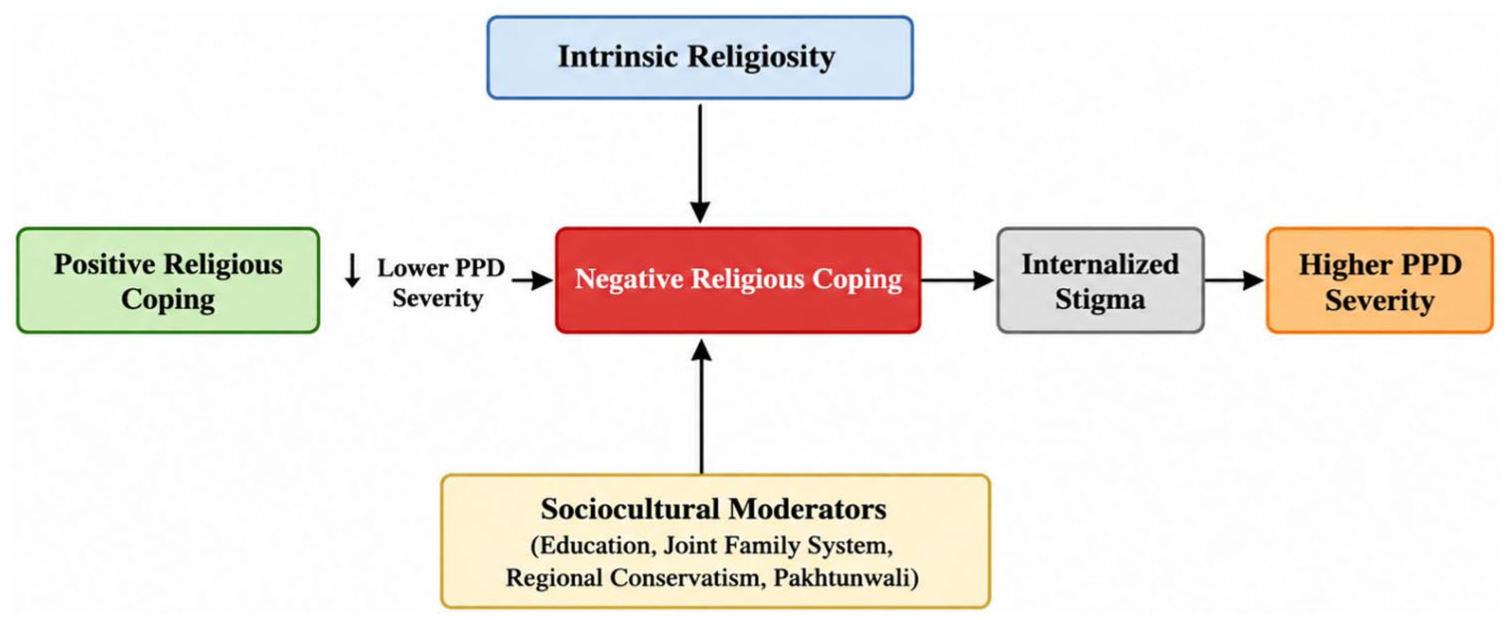
Conceptual integration diagram of the sacred strain model: religion, stigma, and postpartum depression severity.
Data analysis
A convergent, multi-stage analytic strategy was employed to integrate quantitative and qualitative findings in line with best practices for sequential explanatory mixed-methods research.
Quantitative data analysis
Quantitative data were analyzed using IBM SPSS Statistics (Version 28) and AMOS (Version 28), following contemporary guidelines for structural equation modeling (SEM; Kline, 2016).
Analyzes began with data screening and assumption testing. Missing data were minimal (<3% across variables) and handled using expectation–maximization procedures. Univariate normality was confirmed, with skewness and kurtosis values within ±2. Multivariate outliers were assessed using Mahalanobis distance, and internal consistency reliability for all scales was evaluated using Cronbach’s alpha. Zero-order Pearson correlations were then computed to examine baseline associations among intrinsic religiosity, positive and negative religious coping, perceived social support, internalized stigma, and postpartum depression (PPD).
To test Hypotheses 1 and 2, a path-analytic SEM model was specified and estimated using maximum likelihood (ML) procedures. Intrinsic religiosity was modeled as an exogenous variable predicting both positive religious coping (PRC) and negative religious coping (NRC). PRC was specified to predict higher perceived social support and lower PPD severity, whereas NRC was modeled as a predictor of higher internalized stigma, which in turn predicted greater PPD severity. To evaluate partial mediation, direct paths from intrinsic religiosity to PPD and from both coping styles (PRC and NRC) to PPD were retained.
Model adequacy was assessed using multiple fit indices to ensure robust evaluation: the χ2/df ratio (<3.0), Comparative Fit Index (CFI ⩾0.95), Tucker–Lewis Index (TLI ⩾0.95), and Root Mean Square Error of Approximation (RMSEA ⩽0.06) with 90% confidence intervals (Hu and Bentler, 1999).
The significance of indirect (mediated) effects was tested using bias-corrected bootstrapping with 5000 resamples. Mediation was considered statistically significant when the 95% confidence interval did not include zero (Preacher and Hayes, 2008). Key sociodemographic variables—including education level, family structure, and regional location—were examined as moderators through multi-group SEM and interaction testing where theoretically and empirically justified.
Qualitative data analysis
Qualitative interview data were analyzed using Interpretative Phenomenological Analysis (IPA), following the methodological framework articulated by Smith et al. (2009). IPA was selected due to its idiographic orientation and its suitability for examining how individuals interpret and give meaning to emotionally, morally, and spiritually complex experiences such as postpartum psychological distress within religious contexts. Analysis proceeded through a systematic, iterative process. First, each transcript was read multiple times to achieve immersion in the data, accompanied by initial noting that captured descriptive content, linguistic features, and conceptual reflections. These notes were then transformed into emergent themes that articulated participants’ meaning-making processes in concise analytic terms.
Next, emergent themes were clustered within each case to form superordinate themes, preserving idiographic depth and coherence. This was followed by cross-case analysis, during which patterns of convergence and divergence across participants were identified, ultimately leading to the development of higher-order Group Experiential Themes (GETs) that reflected shared experiential structures while respecting individual variation.
To ensure analytic rigor and trustworthiness, several strategies were employed. These included peer debriefing with an independent qualitative coder, yielding approximately 85% concordance in theme identification; member-checking, whereby analytic summaries were shared with a subset of participants for validation; and the maintenance of a comprehensive audit trail documenting analytic decisions, reflexive memos, and theme development.
Ethical considerations
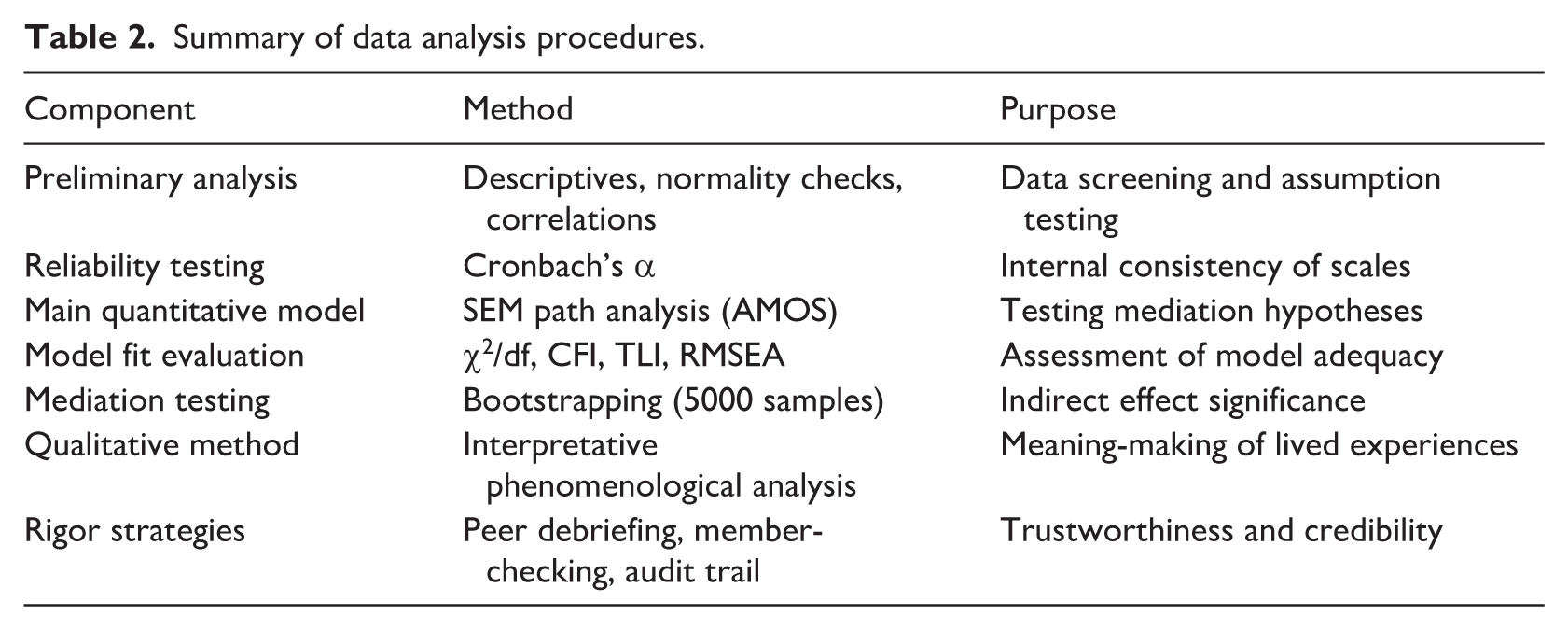
Ethical approval was obtained from the Institutional Review Boards (IRBs) of the lead university in Pakistan and all participating hospitals. Ethical procedures adhered to the principles of the Declaration of Helsinki and APA ethical standards. Given the vulnerability of postpartum women, the principle of non-maleficence was prioritized throughout the study. Participants scoring above the validated EPDS cut-off (⩾13) or expressing acute psychological distress were provided with immediate, confidential on-site counseling by a licensed female clinical psychologist. Where necessary, participants received referrals for free or subsidized ongoing mental health services. Written informed consent was obtained prior to participation. Anonymity was ensured through numerical coding of data, and all identifying information was removed from transcripts. Audio recordings and datasets were stored on encrypted, password-protected devices accessible only to the research team. Participants were informed of their right to withdraw at any point without consequence (Table 2).
Summary of data analysis procedures.
Results
The final sample consisted of 350 postpartum women with a mean age of 27.4 years (SD = 4.8). A majority of participants (62%) resided in joint family systems. Educational attainment was heterogeneous: 28% had fewer than 10 years of formal schooling, 45% had completed matriculation or intermediate education, and 27% held a bachelor’s degree or higher. The mean score on the Edinburgh Postnatal Depression Scale (EPDS) was 14.8 (SD = 5.2), with 52.6% of participants (n = 184) scoring at or above the validated clinical cut-off (⩾13), indicating a high prevalence of probable postpartum depression (PPD) within the sample.
The hypothesized structural equation model demonstrated excellent fit to the observed data, χ2/df = 1.82, Comparative Fit Index (CFI) = 0.97, Tucker–Lewis Index (TLI) = 0.96, and Root Mean Square Error of Approximation (RMSEA) = 0.048, 90% CI (0.032, 0.062). Standardized path coefficients are presented in Figure 2.
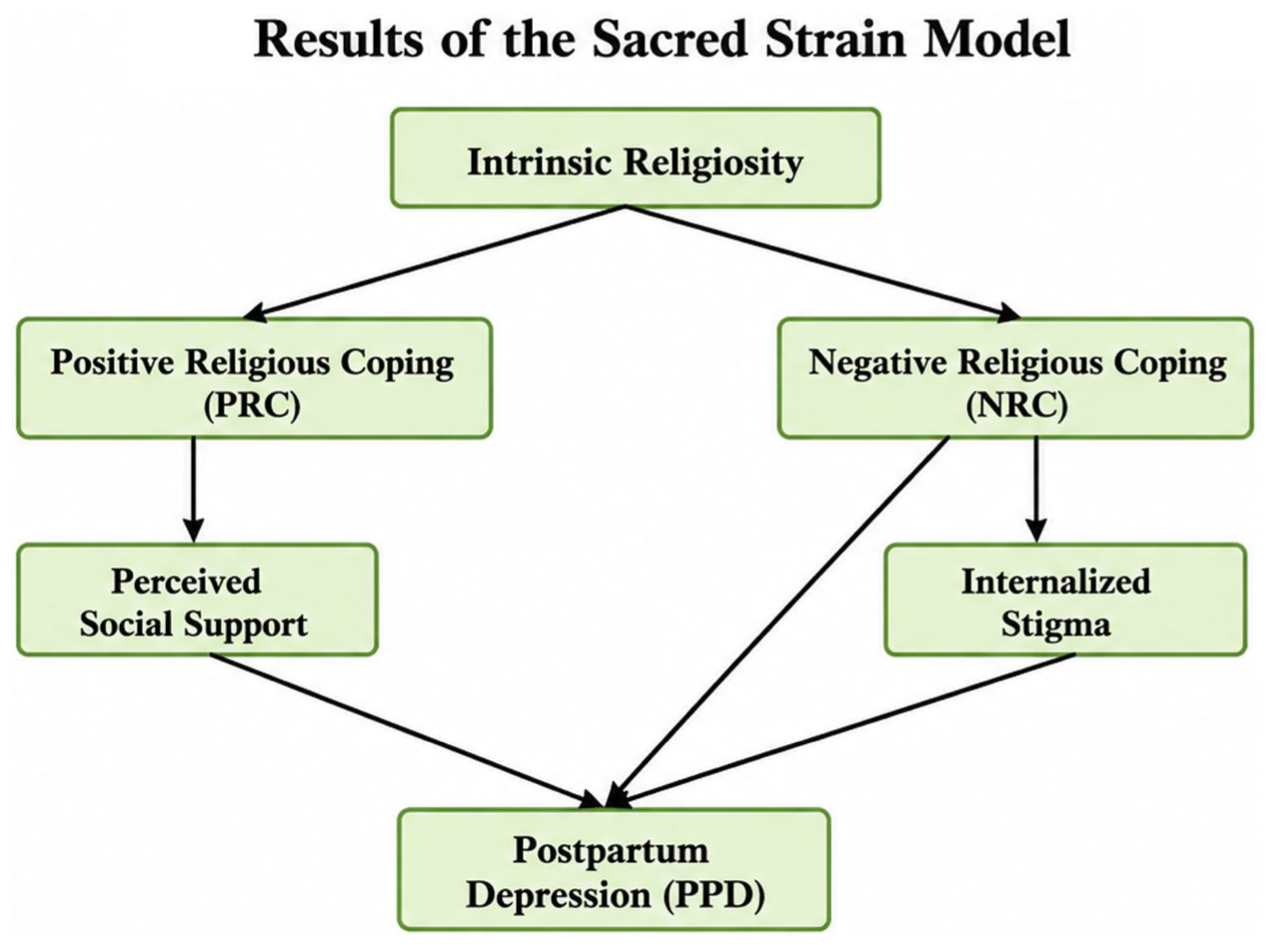
Results of the sacred strain model illustrating the pathways from intrinsic religiosity to postpartum depression (PPD) through positive religious coping (PRC) and negative religious coping (NRC).
Consistent with Hypothesis 1, intrinsic religiosity was a strong positive predictor of positive religious coping (PRC; β = 0.50, p < 0.001). PRC, in turn, significantly predicted higher levels of perceived social support (β = 0.38, p < 0.001) and lower PPD severity (β = −0.22, p = 0.003). The indirect effect of intrinsic religiosity on PPD severity through PRC and perceived social support was statistically significant (β = −0.10, p = 0.002), with bias-corrected bootstrapped confidence intervals excluding zero (95% CI (−.16, −0.05)). These findings indicate that positive religious coping functioned as a protective psychological pathway, translating internalized faith into social and emotional resilience.
In support of Hypothesis 2, intrinsic religiosity was not significantly associated with negative religious coping (NRC; β = 0.08, p = 0.15), suggesting that religious devotion alone did not predispose individuals toward spiritually maladaptive interpretations. However, NRC emerged as a powerful risk factor within the model. NRC strongly predicted higher levels of internalized stigma (β = 0.58, p < 0.001), which in turn significantly predicted greater PPD severity (β = 0.35, p < 0.001). The indirect effect of NRC on PPD via internalized stigma was substantial and statistically significant (β = 0.20, p < 0.001; 95% CI (0.14, 0.27)). In addition, NRC retained a significant direct effect on PPD severity (β = 0.24, p < 0.001), indicating partial mediation and underscoring the cumulative psychological burden of spiritually negative appraisals.
Multi-group analyses further revealed significant sociocultural moderation effects. The NRC → stigma → PPD pathway was significantly stronger among women residing in joint family systems compared to nuclear families (Δχ2 = 8.76, p = 0.01), and among women recruited from Peshawar compared to Lahore and Karachi (Δχ2 = 11.23, p = 0.004). Educational attainment moderated the association between intrinsic religiosity and PRC, with more educated women demonstrating a stronger translation of religiosity into positive coping strategies.
Qualitative analysis of 45 in-depth interviews powerfully illuminated and contextualized these statistical pathways. Across narratives, religious belief systems functioned as both an essential coping resource and a source of psychological strain. Many women described actively mobilizing theological concepts such as tawakkul (trust in God) and sabr (patience) as structured frameworks for enduring emotional pain. Distress was frequently reframed as divine testing (imtihan) or fate (taqdeer), transforming suffering into a morally meaningful struggle rather than passive resignation. For these women, patience was conceptualized as an active spiritual practice—often described as sabr ka amal—imbued with religious merit and existential purpose.
Simultaneously, however, participants articulated a profound moralization of emotional distress. Symptoms of depression—including emotional numbness, irritability, and exhaustion—were frequently interpreted as indicators of spiritual failure or a corrupted heart (qalb). This produced intense spiritual guilt, particularly in relation to culturally idealized notions of the “good Muslim mother,” who is expected to embody gratitude, emotional warmth, and self-sacrifice. The dissonance between this ideal and lived emotional reality emerged as a central amplifier of distress.
Help-seeking narratives revealed a clear hierarchy of culturally sanctioned healing pathways. Religious and spiritual remedies—such as increased prayer, Qur’anic recitation (ruqyah), charity (sadaqah), visits to a pir, or consultation with a maulvi—were almost universally described as the first line of response. Biomedical or psychological care was framed as a last resort, often pursued only after spiritual interventions were perceived to have failed. Seeking psychiatric help carried significant stigma and was frequently equated with weak faith or madness (paagalpan), reinforcing avoidance and delay in treatment.
The communal dimensions of religiosity functioned as a double-edged sword. Collective religious practices sometimes provided profound emotional and social support, reducing isolation and fostering a sense of shared burden. At the same time, these same communal spaces operated as sites of moral surveillance, where women felt compelled to perform happiness and piety to avoid gossip, judgment, or damage to family reputation.
This dynamic was particularly pronounced among Pashtun participants, for whom religious interpretations were inseparably intertwined with Pashtunwali, an honor-based cultural code emphasizing family privacy, control, and reputation. In this context, psychological distress was perceived not only as a spiritual weakness but as a threat to collective honor (izzat), rendering professional help-seeking doubly stigmatized—as both religiously suspect and culturally shameful.
Together, these findings empirically substantiate the Sacred Strain Model, demonstrating how religion operates as a culturally embedded system capable of both buffering against and intensifying postpartum psychological distress, depending on the interpretive and social contexts in which it is enacted.
The results of Figure 2 are presented below, illustrating the structural pathways proposed in the Sacred Strain Model.
Discussion
The present investigation provides robust empirical substantiation for the proposed “Sacred Strain” model, delineating religion not as a monolithic influence but as a profound dialectic within the psychological landscape of Pakistani women experiencing postpartum depression (PPD). This integrated, mixed-methods analysis confirms that religiosity’s impact is contingent, channeled through the specific coping strategies it engenders and the socio-cognitive appraisals it shapes within a collectivistic and patriarchal milieu (Pargament, 2011; Syed, 2018). The quantitative pathway analysis, enriched by the nuanced narratives of the qualitative inquiry, reveals two distinct, concurrent trajectories through which religious belief and practice exert their influence.
On one trajectory, religion functions as a vital psychological and social resource. The finding that positive religious coping (PRC) mediates the relationship between intrinsic religiosity and lower PPD severity aligns with established theories on the salutogenic functions of faith (Park, 2013). In a context where biomedical or psychological models of depression may be unfamiliar or mistrusted, Islamic theodicy offers a culturally legitimate and immediately accessible framework for meaning-making (Ai et al., 2005). As evidenced in the qualitative narratives, concepts such as imtihan (test) and sabr (patience) actively transform experiences of random anguish and suffering into a purposeful spiritual endeavor with teleological significance. This cognitive reframing serves as a critical buffer against hopelessness, a core symptom of depression. Furthermore, religious practice facilitates crucial social integration and perceived support, countering the isolation frequently endemic to the postpartum period, particularly within joint family systems where practical aid may be abundant but empathetic understanding of emotional distress can be lacking (Khan, 2020). Collective rituals, when experienced as supportive (a facet of Group Experiential Theme 4), provide tangible solidarity and reaffirm the woman’s place within a caring community.
Conversely, the second trajectory elucidates a potent burden pathway, wherein religion exacerbates distress through moralization and stigma. The more novel and critical finding is the powerful, stigma-mediated pathway from negative religious coping (NRC) to heightened PPD severity. This pathway, vividly illustrated in the qualitative themes concerning spiritual guilt, help-seeking hierarchies, and cultural honor codes, reveals a toxic synergy. When depressive symptomatology is appraised through a theological lens of divine punishment, abandonment, or personal spiritual failure—core components of NRC—these symptoms cease to be viewed as clinical signs and become moral indictments (Exline, 2013). This moralization of mood acts as a potent fuel for internalized stigma, which Corrigan et al. (2012) identify as a primary driver of the “why try?” effect, eroding self-efficacy and motivation for recovery. This internal, cognitive process is powerfully amplified by external, communal pressures. Within a culture where a mother’s emotional state is often perceived as a reflection of familial piety and social honor (izzat), the admission of psychological vulnerability risks profound social sanction (Nadir, 2018). Consequently, a culturally-encoded hierarchy of healing emerges, as detailed in the qualitative findings, which prioritizes interventions aimed at restoring religious and social standing (e.g. prayer, amulets, visits to pirs) over those addressing the underlying psychological etiology. Biomedical or psychological help-seeking is thus relegated to a last resort, heavily stigmatized as an admission that faith and community remedies have failed, and often only pursued upon the somatization or severe exacerbation of symptoms (Husain et al., 2017). The intensification of this pathway among participants in Khyber Pakhtunkhwa further underscores how embedded cultural codes like Pashtunwali can act as potent amplifiers, layering cultural shame related to honor and privacy upon pre-existing religious guilt (Khan, 2020).
Collectively, these findings mandate a significant evolution in clinical and public health approaches to perinatal mental health in Pakistan, moving beyond mere screening to actively engage with the religious and cultural ecosystem in which distress is embedded. First, therapeutic interventions must adopt a posture of cultural humility and integration. Culturally-Adapted Cognitive Behavioral Therapy (CA-CBT) should train practitioners in “theological restructuring,” working within the client’s religious schema to challenge maladaptive appraisals (Hodge and Nadir, 2008). For instance, the automatic thought “My sadness proves I am a bad Muslim” can be countered with evidence from Islamic tradition, noting that prophets like Yaqub (AS) experienced profound grief (huzn), thereby framing sadness as a human experience within faith, not an indicator of its absence. Behavioral activation can be framed through religiously congruent actions, such as engaging in small acts of charity (sadaqah).
Second, a systematic, respectful collaboration with community religious authorities is essential. Training programs for imams, respected maulvis, and pirs should provide education on recognizing PPD, distinguish it from spiritual lassitude, offer basic supportive counseling frameworks, and establish dignified referral pathways to mental health professionals. This creates a bridged referral system that leverages existing trust to reduce stigma (Abu-Raiya, 2013). Third, intervention models must be family-centric. Psychoeducational initiatives targeting mothers-in-law and husbands can reframe PPD as a condition affecting the nafs (self/psyche) that requires familial support as a religious duty (farz) to safeguard a divine trust (amaanat)—the well-being of both mother and child.
Finally, public health messaging must be co-constructed with religious and cultural authorities. Anti-stigma campaigns featuring endorsements from senior scholars (ulema) and, in relevant regions, tribal elders, can theologically legitimize help-seeking. Messaging can emphasize that caring for one’s mental health is an integral component of preserving the amaanat of one’s body and mind. By honoring the resource pathway while directly mitigating the burden pathway, such an integrated approach fosters a more compassionate and effective landscape for maternal mental well-being, weaving threads of psychological insight into the enduring tapestry of faith.
Limitations and future research directions
While this study offers significant insights, several methodological and conceptual limitations warrant consideration and pave the way for future inquiry. First, the cross-sectional design, while efficient for mapping associations, inherently limits the ability to make definitive causal inferences regarding the directional relationships between religiosity, coping styles, and PPD symptomatology. The observed pathways, particularly the potent link between negative religious coping and depression, may reflect reverse causality or be influenced by unmeasured third variables, such as personality traits or pre-existing anxiety, that predispose individuals to both spiritual struggle and mood disorders (Weber and Pargament, 2014). Second, although efforts were made to include diverse urban and peri-urban settings, the hospital-based recruitment strategy likely engenders a selection bias. The sample may underrepresent women in remote rural communities, those with the most severe stigma-related avoidance of healthcare, and those who deliver at home with traditional birth attendants, thus limiting the generalizability of the findings to Pakistan’s full socioeconomic and geographic spectrum (Atif et al., 2020). Third, despite rigorous translation and validation procedures, the core psychological measures employed—the Brief RCOPE, DUREL, and ISMI—originate from Western, Judeo-Christian contexts. Although they demonstrated good reliability, their structural validity and capacity to fully capture culturally specific manifestations of religious coping, such as the particular phenomenology of waswasa (religious obsessive doubt) or the nuanced social dynamics of consulting a pir, remain open questions (Abu-Raiya and Hill, 2014). The quantitative operationalization of complex, culturally-embedded experiences like “spiritual guilt” may lack ecological validity, a gap the qualitative component helped to illuminate but cannot fully rectify in measurement.
These limitations directly inform a robust agenda for future research. To disentangle causality, prospective longitudinal studies are essential, tracking women from the third trimester of pregnancy through at least the first postpartum year. Such designs would elucidate how religious coping strategies dynamically evolve in response to the stress of childbirth and infant care, and whether early negative religious appraisals predict the subsequent onset or worsening of PPD symptoms, controlling for baseline mood (Rogers et al., 2021). To address the measurement gap, a critical next step is the development and psychometric validation of a culturally-grounded instrument, perhaps titled the Religious and Moral Distress in Motherhood Inventory (RMDMI). This scale would be derived inductively from qualitative data like that gathered here, aiming to quantify the unique constructs of moralized mood, theological conflict, and culturally-shaped help-seeking ambivalence identified in this population, ensuring greater contextual fidelity (Christopher et al., 2014). Furthermore, the clinical implications proposed require empirical testing. The efficacy of Culturally-Adapted CBT (CA-CBT) integrating theological restructuring, and the impact of training programs for religious leaders, must be rigorously evaluated through randomized controlled trials, including cluster-randomized trials at the community or mosque level to assess real-world implementation (Naeem et al., 2021). Finally, an intersectional lens is crucial. Future research must systematically explore how the “sacred strain” manifests differentially across intersecting identities, comparing experiences across Sunni and Shia sectarian lines, analyzing the impact of socioeconomic privilege on access to both religious and psychological resources, and examining the unique challenges faced by religious minorities in Pakistan, such as Christian or Hindu mothers, whose distress may be compounded by religious marginalization (Crenshaw, 1991; Zakar et al., 2021).
Conclusion
For the Pakistani woman navigating the profound transition into motherhood while grappling with postpartum depression, her religious faith defies simplistic categorization as either a straightforward sanctuary or an unambiguous source of conflict. Instead, it constitutes the foundational terrain of her psychological world—a complex soil that can nurture profound resilience through meaning, community, and hope, yet simultaneously cultivate invasive roots of guilt, shame, and existential doubt. The “Sacred Strain” model, empirically substantiated in this study, provides a critical framework for comprehending this inherent ambivalence. It challenges the predominantly etic, often reductive, approach within health psychology that seeks universal correlations between religiosity and well-being, advocating instead for a deeply emic, contextual understanding (Berry, 2013). This perspective recognizes that belief systems are not merely external variables but internalized, lived realities that dynamically shape the cognitive appraisal of distress, the social acceptability of suffering, and the very pathways to healing.
This investigation underscores that the relationship between faith and mental health is mediated not by doctrine itself, but by the functional applications of belief—the specific coping mechanisms it enables and the socio-moral narratives it authorizes within a given cultural matrix (Pargament, 2011). The documented dialectic between positive religious coping, which fosters endurance through sabr and tawakkul, and negative religious coping, which moralizes distress into spiritual failure, illustrates that the same theological wellspring can irrigate both growth and pathology. Therefore, recognizing this constitutive strain is not an academic endpoint but a vital clinical and ethical starting point.
The imperative that follows is translational and transformative. Knowledge of this duality must be cultivated into actionable, compassionate, and culturally courageous praxis. This entails moving beyond a posture of mere cultural competence—awareness of difference—toward what has been termed cultural humility, a lifelong commitment to self-evaluation, redressing power imbalances, and developing mutually beneficial partnerships with communities (Tervalon and Murray-García, 1998). For clinicians, it requires the skill to ethically and effectively engage a client’s religious framework, not as a barrier to overcome but as a primary language in which healing can be co-authored. For public health architects, it demands collaborative alliances with religious scholars and community leaders to co-design interventions and messaging that reframe mental healthcare as congruent with, rather than antagonistic to, spiritual duty.
Ultimately, the goal is an integrative model of care that does not ask women to choose between their faith and their psychological well-being. The task is to weave the threads of evidence-based psychological healing into the enduring, meaningful tapestry of their faith, strengthening the fabric where it supports and gently mending it where it constricts. By honoring the resource while diligently alleviating the burden, health professionals and communities can work together to ensure that the sacred ground of a woman’s psyche becomes a source of sustenance for both her and the new life in her care, fostering holistic resilience rooted in authentic cultural and spiritual integrity.
Footnotes
Ethical considerations
Ethical approval was not applicable for this study. The research did not involve any clinical interventions, experimental manipulation, or collection of personally identifiable or sensitive data. All data were collected through voluntary participation, with informed consent obtained from participants prior to inclusion. The study adhered to the ethical principles of confidentiality, anonymity, and respect for participants’ autonomy, in accordance with international ethical guidelines for social and psychological research. As no institutional review board (IRB) approval was required under these conditions, no IRB number is available.
Consent to participate
Informed verbal consent was obtained from all participants prior to data collection, following a comprehensive explanation of the study objectives, procedures, potential risks, and participants’ rights. Verbal rather than written consent was deemed appropriate and ethically acceptable in this context because the study involved non-invasive procedures, did not include biological sampling or experimental manipulation, and focused exclusively on self-reported information. Ethical clearance was obtained from the relevant institutional review authority approving this consent procedure. Participants were informed that their participation was voluntary and that they could withdraw from the study at any time without any consequences.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.