
Abstract
This qualitative study explores how clinicians with lived experience (LE) of eating disorders (EDs) view their experiences of identity, boundaries, and recovery within NHS England services. Participants (N = 9) were healthcare professionals in NHS England ED services, recruited as part of a wider qualitative study. Semi-structured interviews were conducted and analyzed using reflexive thematic analysis. Four themes were identified: (1) Lived experience as a source of professional motivation versus perfectionistic pressure; (2) Recovery as identity work; (3) Emotional labor, resonance, and self-disclosure; and (4) LE-informed reflections on ED services. LE offered empathy, connection, and optimism, but also required ongoing emotional monitoring, boundary management, and negotiation of professional identity. Findings highlight the value and complexity of LE in ED care and underscore the need for supportive supervision and organizational cultures that recognize both strengths and vulnerabilities associated with integrating LE in practice.
Introduction
An estimated 20%–47% of eating disorder (ED) clinicians have experienced an ED themselves (Bachner-Melman et al., 2021; Warren et al., 2009). Lived experience (LE) may influence career choice, therapeutic stance, and role identity. While existing research highlights both benefits and concerns surrounding LE in ED practice–such as empathy, countertransference, and boundary negotiation–recent workforce pressures and changes in ED service delivery raise questions about how LE clinicians manage their roles.
NHS ED services have faced rising demand, complexity, and resource strain, which shape clinicians’ emotional labor and capacity to manage increasingly difficult presentations (Ayton et al., 2022; Cooksley et al., 2023; Taquet et al., 2021; Wu et al., 2020). Referral rates remain elevated compared to pre-pandemic levels (Gallagher et al., 2025), exacerbating workforce pressure, which may affect clinician wellbeing and service quality, making it essential to explore clinician experiences in this evolving context.
Across mental health professions, LE is increasingly viewed as a strength in clinical work. The Person-of-the-Therapist Training (POTT) model, for example, encourages clinicians to integrate personal insight into their therapeutic role in a reflective and intentional manner (Aponte and Kissil, 2017; King and Russon, 2023). However, empirical evidence on how LE impacts clinical outcomes, self-disclosures, recovery, and readiness to practice remains limited (Bachner-Melman et al., 2021; Pellizzer and Wade, 2024).
Debates around fitness to practice with LE in ED practice exist Bachner-Melman et al. (2021), indicate that ED clinicians were divided in their views on whether LE clinicians should practice without conditions. Most agreed that if LE clinicians do practice, they should meet certain criteria: being in recovery (despite wide variations in how this is defined), having regular supervision and training, possessing high self-awareness, and engaging in past or current therapy. These findings reflect broader tensions around self-disclosure, recovery status, and LE clinicians’ professional readiness to work in ED services.
ED clinicians are at heightened risk of burnout, driven by long working hours, high emotional demands, lack of resources, and patient complexities (Warren et al., 2012). The nature of EDs, including their ego-syntonic features, chronicity, and comorbidities, may further exacerbate stress. Countertransference, or therapists’ emotional reactions to patients shaped by their own vulnerabilities (Gelso and Hayes, 2007), is also common in ED work (Colli et al., 2015). These reactions may involve overinvestment, frustration, hopelessness, or even increased self-criticism about one’s own body (Warren et al., 2009). While some level of countertransference is inevitable, unmanaged emotional responses can contribute to emotional exhaustion and impair therapeutic effectiveness.
Clinicians may also experience moral injury - the psychological distress resulting from actions or inactions that violate one’s moral code (Greenberg et al., 2020; Litz et al., 2009). A recent study found that around one-quarter of healthcare professionals reported symptoms of moral injury, with meaningful impacts on social and occupational functioning (Mantri et al., 2021). Moral injury has been linked to self-blame, guilt, and poor mental health. For LE clinicians, moral injury may be especially salient, as their personal histories may heighten sensitivity to perceived ethical violations or systemic failures. However, empirical data exploring how LE intersects with moral injury is currently lacking.
Despite increasing awareness of the challenges faced by ED clinicians, few studies have focused on the unique experiences of those with LE, particularly in the context of a publicly funded health system such as the NHS. As services have undergone rapid change during and after the pandemic, understanding the experiences and views of LE clinicians is essential for informing workforce policy and service delivery. understand and integrate their personal histories into professional identity, practice, and organizational contexts using a qualitative approach. By centering the voices of LE clinicians, this research aims to identify challenges and strengths within current practice and offer recommendations for supporting clinician wellbeing (defined broadly as mental, emotional, occupational, and physical functioning) and service sustainability.
Research questions: How do clinicians with LE perceive their roles within ED services, and how do their experiences shape their interactions with patients (e.g., navigating boundaries, disclosure, and emotional exhaustion)? What are benefits and tensions arise when drawing on LE in clinical practice? What support systems need to be in place for these clinicians to promote wellbeing?
Methods
Participants and inclusion criteria
Participants (N = 9) were healthcare professionals working in NHS England ED services who were approached as a part of a wider interview study on clinicians’ work-related experiences. Attendees of a training course for adult community NHS ED services in England (Novogrudsky et al., 2025) were invited to complete an interview via email. This invitation email was also forwarded by some clinicians to their colleagues.
LE was defined inclusively as any personally meaningful history of clinically diagnosed ED, subclinical symptoms, or carer experience. This avoided privileging diagnostic categories and reflected how participants themselves described LE.
Participants worked across psychology, nursing, assistant psychology, mental health practice, community support, and peer support roles. Due to small numbers, themes were developed across roles rather than stratifying by discipline. Though recognizing that role-specific experiences may differ (e.g. nurses’ proximity to risk management responsibilities, psychologists’ therapeutic boundary considerations, or peer support workers’ navigation of lived experience), subgroup analysis would have resulted in very small analytic units and limited interpretative coherence. The analytic focus therefore prioritized shared patterns across the multidisciplinary workforce.
Interview schedule
A semi-structured interview schedule was created by the authors. Initial questions focused on clinicians’ careers and professional experiences, followed by questions about professional needs, job satisfaction, and enjoyment, training experiences and needs. Other questions probed clinicians’ personal experience of having or caring for someone with an ED, probing how their personal experiences shaped their professional lives. The research questions were initially formulated to explore clinician wellbeing broadly. During the inductive thematic analysis, it became clear that some participants’ concerns were rooted in their experience of ED, identity, and the tactical use of such. To ensure analytic depth and honor the density of these specific reflections, the present manuscript focuses exclusively on the LE-related portions of the interviews. Consequently, the analytic focus was refined post-data collection to prioritize these themes.
The interview schedule can be found in Appendix 1.
Ethics
This study was granted ethical approval by the KCL Health Faculties (Blue) Research Ethics Subcommittee, HR/DP-22/23–30,046. Considering the potentially distressing content of some of the questions, participants were provided with a range of outside support sources as a precautionary measure, in case further support was needed.
Procedure
Clinicians attending a national ED training program received study invitations. Participation was voluntary and unrelated to training outcomes. Interviews were conducted online, lasted 29–96 minutes (average = 42 minutes; median = 33 minutes), and followed a broad guide covering professional background, LE, identity, boundaries, and role experiences. LE-related material formed the analytic focus due to its centrality across participants’ narratives. To mitigate potential power asymmetries or a perceived ‘obligation’ to participate, the research team emphasized that participation was entirely voluntary and had no bearing on course assessment or progression. No prior supervisory or evaluative relationships existed between the researchers and the participants. After completion, participants were offered a £20 bank transfer for their participation. Consolidated criteria for reporting qualitative studies (COREQ) checklist (Tong et al., 2007) is presented in Appendix 2. This tool provides a framework to ensure explicit and comprehensive reporting of the interview process.
Data analysis
Interviews were anonymized and analyzed in NVivo. A qualitative design using reflexive thematic analysis (RTA) was adopted within a critical realist framework. This position assumes EDs and clinical work have material reality, while participants’ accounts and researchers’ interpretations are shaped by social, contextual, and experiential factors (Willig, 2012). Coding proceeded from semantic descriptions to latent interpretation, focusing on how participants made sense of identity, emotional labor, and boundary negotiation. Themes were developed through iterative, reflexive engagement rather than consensus validation. Themes, subthemes and labels were verified by other authors. Lastly, the methodology and results were sent to participants for review to confirm the validity of the themes.
Reflexivity
Reflexive thematic analysis requires researchers to acknowledge and critically reflect on their own positions, biases, and potential influence on the research process. The primary researcher (KN) is a young White female with lived experience of ED and its treatment within the NHS. Her personal experience and professional aspiration to work as an ED clinician may have shaped her interpretations of the data. To ensure the interviews were driven by participants’ experiences, the researcher withheld disclosure of her own LE history, ensuring participants’ voices remained central in the interviews. CLL, as a carer of two recovered individuals from anorexia nervosa, brought an in-depth understanding of the disorder. While her lived experience helped to engage deeply in data collection, there was a risk of bias interpretating the data. JT and US are clinical academics with many years of experience working as NHS ED clinicians across inpatient (JT) and outpatient (US) service settings. Both are senior clinicians who have provided supervision and contributed to service and treatment development. Both were involved in developing the interview guide, and in sense-checking and meaning making during the analytic process. Reflexivity was actively practiced through regular supervision meetings, and dialog with co-authors, which encouraged critical reflection on interpretative choices and meaning-making. These discussions helped to balance emotional proximity with analytic distance.
Results
Table 1. presents a coding tree with example codes and quotes from the data.
Coding tree.
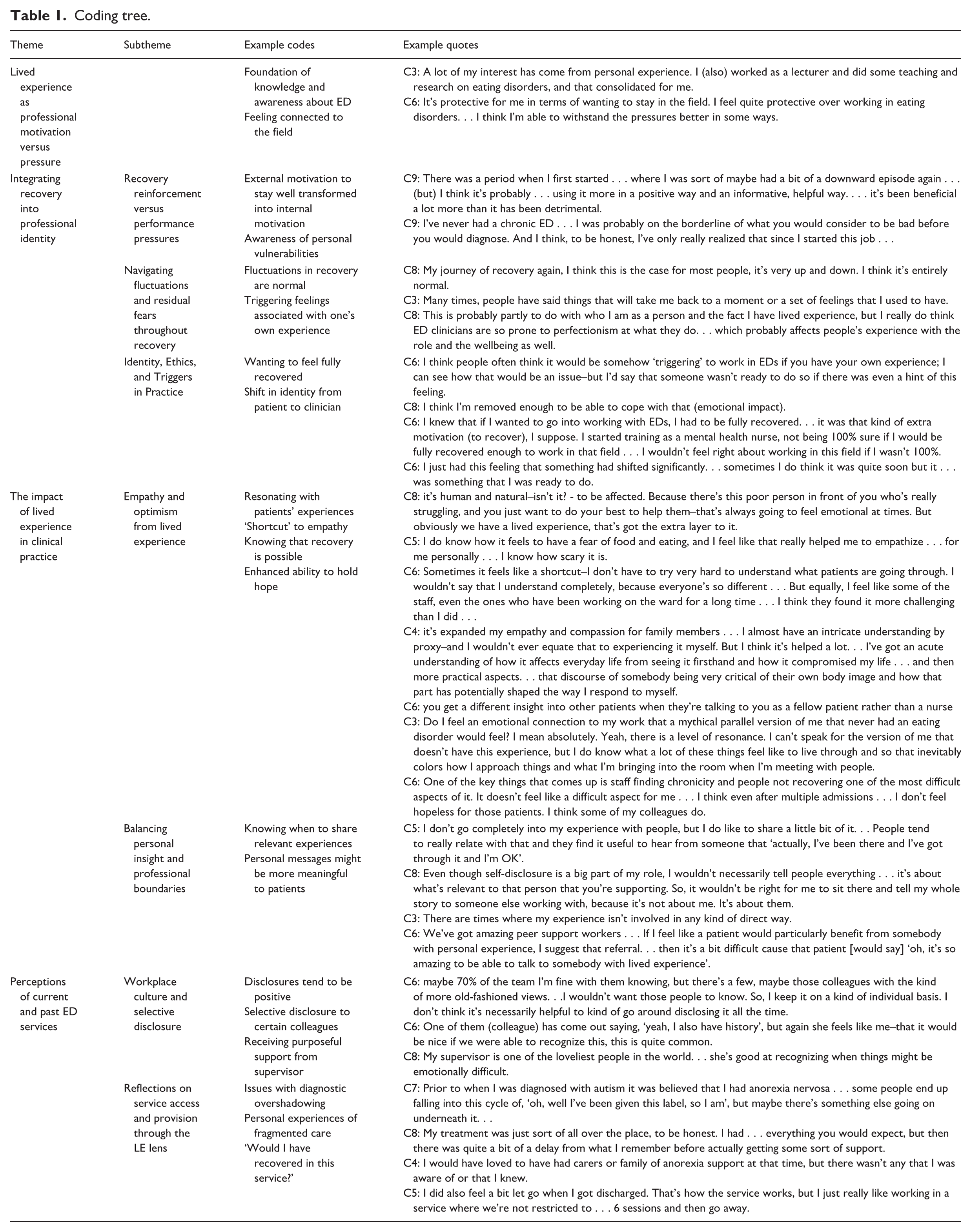
Theme 1: Lived experience as professional motivation versus pressure
Clinicians described LE as central to their decision to work in EDs, often linked to gratitude toward past providers or a desire to ‘give back’. LE also created a sense of responsibility and purpose that sustained engagement in demanding roles. Motivated by the transformative impact of their own therapeutic relationship during their treatment for ED, they aspired to play a similar role in someone else’s recovery. This personal-professional trajectory fostered a strong sense of identity and meaning in their work. This was seen as a factor contributing to role retention, not only leading to heightened dedication but also increased LE clinicians’ tolerance of the challenges associated with ED work.
C5: I have never appreciated anything so much in my life as those people who helped me. I just want to be that, even if it’s just for one person or a small group of people, I want to be that for somebody else.
However, this motivation sometimes intersected with internal pressures. Some clinicians felt compelled to appear ‘fully recovered’, maintain high standards, or manage perfectionistic tendencies rooted in earlier illness experiences. This produced an internal tension between authentic fluctuation and a professional identity of stability. Thus, LE served as both an anchor for meaning and a source of self-surveillance.
Theme 2: Integrating recovery into professional identity
Subtheme: Recovery reinforcement versus performance pressures
LE clinicians expressed the importance of leading by example and its role in reinforcing their recovery. By embodying the guidance they provided to their patients, LE clinicians subsequently felt their own mental strength being bolstered. Similarly, LE clinicians’ work supported their physical recovery as to avoid being questioned about their ED which transpired into reinforcing recovery on all fronts. However, this dynamic was underpinned by ambivalence, where the perceived requirement to ‘embody’ health may have created a parallel pressure to ‘perform’ recovery. While participants reflected on this professional accountability as a catalyst for holistic growth, it nonetheless generated a tension between vulnerability and internalized professional pressures on oneself.
C1: Working at an ED service has probably been quite helpful to me because I think, ‘I can’t be that’ and with integrity, I can’t be at home worrying too much about [ED-related] stuff and then tell people what they need to be doing.
Nevertheless, this gave rise to conversations about being ‘triggered’ and at what point in a LE clinician’s recovery would they be deemed suitable to work in the field.
Subtheme: Navigating fluctuations and residual fears throughout recovery
LE clinicians described recovery as a lifelong process requiring continued self-awareness and coping. Many LE clinicians experienced persistent ED-related thoughts or feelings, suggesting that full recovery did not necessarily mean the complete erasure of past struggles. LE clinicians acknowledged these fluctuations and enduring challenges, sometimes having feelings provoked associated with clinicians’ past EDs by their clinical work, highlighting the longevity of the emotions associated with EDs. Despite some residual fears or food-related distress, LE clinicians felt strong in their recovery - emphasizing persistence over perfection. LE clinicians valued honesty with themselves and others about the reality of residual fears.
C5: Every now and then. . . I get anxiety and I panic . . . It still comes back to me. . .I just kind of say to myself, you’ve done this before, you got through it. It’s OK.
Associated with residual difficulties was the history of perfectionism, which may be seen as both a symptom of the ED and as a predisposing identity factor. LE clinicians recognized how this manifested in LE clinicians’ work, affecting their experience with the role.
Subtheme: Identity, ethics, and triggers in practice
LE clinicians voiced that, whilst it was normal to have past thoughts and feelings arise, they should not feel ‘triggered’ by their work. Ethically, they believed that one would have to be secure in their recovery before engaging in this type of work.
In setting and upholding therapeutic boundaries, LE clinicians felt a degree of emotional detachment from their work, allowing themselves to form effective therapeutic relationships for the betterment of their patients’ care. This additionally protected LE clinicians themselves from becoming overly affected by their work. Having experience of an ED was viewed as a preparation for the challenges associated with ED work, where was almost a sense of inoculation against patients’ reactions to clinicians’ bodies, for instance, after having been in ED treatment.
C6: Long EDU 1 admissions did give me the ability to be in those environments without it affecting me. . . you have to get used to feeling bigger and more well than all the other patients. . . I’ve heard more people without lived experience of ED say that they found working on EDUs difficult because of how patients made them feel about their own eating or bodies.
LE clinicians felt they should be ‘fully recovered’ to practice clinical work. This was both a sort of encouragement for their own recovery and was a commitment to their future patients’ best interests. Despite some reticence and challenges in the early career stages, there was a stark shift in LE clinicians’ identity that related to being recovered. As such, there was a feeling of shifting positions – no longer associating themselves with being a patient but rather holding a clinician’s position. This provided a sense of security and confidence in recovery and work. Despite some initial challenges, many felt their experience enhanced their resilience and ability to maintain boundaries.
C6: I had already transitioned away from being on the ‘patient’ side of things, and formed a ‘new’ identity away from the ED.
Theme 3: The impact of lived experience in clinical practice
Subtheme: Empathy and optimism from lived experience
LE provided intuitive empathy and emotional resonance that often deepened therapeutic relationships, though this ‘shortcut’ to empathy was frequently underpinned by significant emotional labor. Clinicians recognized their own past struggles in patients, experiencing a duality where sadness and heaviness coexisted with healing and connection. While this resonance provided a ‘firsthand’ understanding, it also required clinicians to navigate the risk of overidentification when ‘seeing pieces’ of themselves in their clients.
C8: When I can see pieces of myself in people, it can be quite sad, very sad sometimes. But at the same time, really healing in a weird way, because I’m able to maybe give them that support and empathy that maybe I didn’t receive at certain points in my treatment.
This depth of understanding allowed LE clinicians to connect with patients more intuitively, particularly regarding the fear of food and body changes. However, participants noted that this ‘shortcut’ required active management to ensure personal ‘emotional echoes’ did not cloud clinical boundaries. Beyond rapport, LE enhanced clinicians’ ability to hold hope; having experienced the ‘light at the end of the tunnel’, they could maintain optimism and professional resilience even during clinical stagnation.
C5: It just helps me to persevere because even though it feels difficult to work with this kind of client group, I know how it feels, and I know there’s a light at the end of the tunnel.
In sum, LE facilitated a nuanced empathy and hope, but this was experienced as a complex psychological negotiation where the benefits of shared experience were balanced against the ongoing labor of processing one’s own history within the clinical encounter.
Subtheme: Balancing personal insight and professional boundaries
LE clinicians described self-disclosure as a situationally dependent practice, with many acknowledging how self-disclosure could support patient engagement by fostering hope and strengthening the therapeutic alliance. The ability to share personal insights was more explicit for those in peer support roles, where self-disclosure was structurally embedded. Another benefit included the normalization of patients’ behaviors, showing them that they were not alone in their journey. Some clinicians shared that a brief self-disclosure helped patients feel better understood and less alone.
C8: It can be so powerful; it can just change something. Because you can say to someone all the facts from the textbook and all the things from theory–it won’t hit though, because they’re just like, ‘well, you say that to everyone’. But if you can give that little bit of self-disclosure when relevant, I think it makes a huge difference for people.
However, LE clinicians were mindful of the risks of self-disclosure, including comparison, triggering competitiveness, or loss of privacy. One LE clinician highlighted how self-disclosures could trigger doubt about the validity of the clinician’s recovery.
C6: If someone disclosed, even they were fully recovered, perhaps you would always think, ‘but are they really?’ Or to start thinking, ‘how did my experiences match up to theirs?’
LE clinicians sometimes felt frustrated when personal connections to a patient’s experience could not be shared, but they generally demonstrated awareness of when self-disclosure was appropriate. Used thoughtfully, self-disclosure was seen as a helpful tool, provided that professional boundaries, judgment, and role clarity were maintained.
Theme 4: Perceptions of current and past ED services
Subtheme: Workplace culture and selective disclosure
Given the prevalence of LE clinicians in ED services, some noted an unspoken understanding among colleagues about each other’s motivations for entering the field.
C7: If the team knew a little bit more about me, they would understand my point of view when I come forward with comments . . . But again, there is that understanding that everyone who works in a specified field probably has some link with the background.
However, LE clinicians were more hesitant to directly disclose their experiences everyone, based on concerns about scrutiny from coworkers. Nonetheless, selective disclosure seemed to have positive outcomes, often with others then sharing their experiences as well, creating a deeper working bond. Others reported feeling shame about disclosing their struggles to colleagues despite recognizing the potential benefit of sharing their concerns.
C1: I don’t know how helpful that would be to my colleagues. In one way it could, because it is about being able to be open. . . I’m just not sure if people are looking up to you for guidance and containment and then you tell them ‘I worry about calories’, and things like that. . . I feel like as the consultant psychologist there, I shouldn’t be - it feels like should get over this . . . I suppose I feel a bit ashamed.
Regarding their supervision, LE clinicians valued the opportunity to honestly and openly communicate about their experiences with their supervisors, where supervision provided LE clinicians with a space to process their emotions that arose in their work. Overall, LE clinicians felt able to selectively disclose their experiences to colleagues and supervisors, using their judgment to determine when such disclosures would be appropriate or beneficial.
Subtheme: Reflections on service access and provision through the LE lens
Clinicians’ reflections on their own treatment histories (marked by diagnostic overshadowing and fragmented pathways) evoked a sense of moral injury. The question, ‘Would I have recovered in my own service?’, highlights a profound organizational strain and a sense of institutional betrayal. This experiential knowledge creates a ‘moral discomfort’ when clinicians must work within systems they recognize as inadequate, shifting perspectives toward the ethical burden of navigating systemic limitations while maintaining professional loyalty
C6: I had a really difficult time trying to get help in the first place . . . I tried to mention it to a teacher at school, but they dismissed it. I then went to GP . . . GP just didn’t pick up on it at all. I felt, okay, the problem must be in my own head.’. . . there was something quite blaming about that. . . I must have gone for maybe 15 years with symptoms of ED without having any evidence-based treatments. Which probably was why it was so hard eventually to recover.
Beyond personal care, support for carers and family members was also lacking, highlighting the unmet need for family-based support. Considering their own experiences in ED services, LE clinicians reflected on the state of the services in which they worked. Some questioned whether they themselves would have recovered under current service constraints, expressing discomfort or sadness about system limitations.
C6: It leaves me with a kind of like an uncomfortable feeling - thinking if I had been seen in our service, would I have recovered? I’m sometimes thinking, yeah, they’d probably even discharge me, and I might still be unwell because I wasn’t the ideal patient . . .
These reflections sometimes evoked moral discomfort, particularly when clinicians felt system decisions conflicted with their own values or memories of being unsupported.
C6: It makes it personally more complicated for me in terms of the feelings it might bring up, whether we do or don’t take someone on, or what we offer them.
Discussion
This study examined how clinicians with lived experience of eating disorders (LE) integrate their histories into NHS ED practice. Findings show that LE shapes professional motivation, identity, emotional labor, and clinical judgment in complex and often ambivalent ways. The themes reveal a balance between the benefits of integrating LE (such as enhanced empathy and hope for patients) and the challenges of managing triggers, boundaries, and professional identity. Furthermore, LE clinicians’ reflections on past service experiences highlight systemic gaps that continue to affect patient care and clinician perspectives alike. These findings underscore the importance of supporting LE clinicians through appropriate role preparation, supervision, and organizational culture, whilst also valuing the unique contributions they bring to ED services.
LE offered clinicians a sense of purpose and connection, consistent with wider literature describing LE as a driver of meaning and commitment in mental health work (de Vos et al., 2016; Welch, 2023. Yet participants also reported internalized pressures (such as perfectionism, self-monitoring, and the need to appear consistently recovered) which reflect broader ED norms around control and high standards. These dynamics created tensions between authentic recovery fluctuation and the professional expectation of stability.
The growing recognition of LE in mental health work has also led to an expansion of peer support roles, including for those without formal clinical qualifications (Mutschler et al., 2022). Many peer support workers go on to pursue formal training, illustrating a pathway from LE to learning and clinical practice (Duvall and Hanson, 2024). These roles offer opportunities to build leadership, problem-solving, and self-care skills, while fostering a sense of connection within an LE community (LaMarre et al., 2025). Peer workers often emphasize the need for structured support, including supervision, training, and shadowing (LaMarre et al., 2025). Many also describe a desire to ‘give back’ and frame their role as a form of advocacy, reflecting themes found both in general LE literature (Hartley and Penlington, 2024) and studies on ED peer support (LaMarre et al., 2025). Recognizing these pathways could help services formalize routes from peer support to clinical roles, inform tailored training and supervision structures, and ensure LE-informed career development is supported systemically.
Working in ED services often places LE clinicians in situations that evoke emotionally salient responses. The theme of integrating one’s recovery into professional practice captured both the benefits and internal challenges that LE clinicians may encounter in their roles. Consistent with previous research, the current findings support the view that LE can act as a protective factor against relapses in LE clinicians (Curry and Andriopoulou, 2023; Welch, 2023). This perspective contrasts with concerns sometimes expressed by non-LE clinicians, who may perceive ED work as potentially triggering for those with personal histories of EDs (Bachner-Melman et al., 2021).
LE clinicians derived a strong sense of reward and purpose from their work - two factors that have been associated with a reduced risk of burnout (Duffy, 2022). One key internal reward appears to be the perception that their work is meaningful, a well-established psychological need linked to intrinsic motivation and wellbeing (Deci and Ryan, 1985). Supporting others through challenges they themselves have overcome may foster a deep sense of purpose, which can be psychologically reinforcing for LE clinicians and contribute to sustained engagement in emotionally demanding work.
Additionally, enhanced self-reflection and emotional monitoring–particularly in relation to body image and eating–may help sustain recovery and promote resilience in clinical practice (Curry and Epley, 2022). Another potential mechanism is the implicit motivation to ‘practice what you preach’: LE clinicians may feel a sense of accountability to embody the behaviors and attitudes they advocate in treatment, reinforcing recovery-consistent behaviors. However, this dynamic remains underexplored and warrants further investigation to better understand its potential benefits and risks.
LE clinicians may also be more accustomed to navigating scrutiny or commentary about their bodies or appearance - feedback that can come from both patients and colleagues in ED services ( Jacobs et al., 2010; Yim, 2025). Research suggests that working in ED settings can affect body image satisfaction, depending on clinicians’ baseline body satisfaction and internalization of thin-ideal norms (Levy, 2014). LE clinicians, having already engaged in deep reflection on their relationship with food, body image, and eating, may be more resilient to such influences (Rance et al., 2010). Their prior experiences of receiving judgment or unsolicited comments may enhance their ability to emotionally buffer against this feedback. In contrast, non-LE clinicians who have not been required to interrogate these issues as directly may lack such coping strategies, potentially making them more vulnerable to emotional strain or body image concerns in the clinical context (Rance et al., 2010).
LE clinicians in the current study commonly expressed the view that they should not feel ‘triggered’ by their work, emphasizing the importance of being in a state of ‘full recovery’ before entering clinical roles. However, this raises important questions about how recovery is defined, and at what point in one’s recovery journey an individual might be considered ready or fit to work in ED services. In the current study, recovery itself was not experienced as a fixed endpoint. Instead, participants described a dynamic process influenced by personal history, clinical demands, and professional identity. For some, ED work supported recovery through accountability and reflective practice; for others, it introduced subtle pressures to manage residual symptoms privately. Thus, recovery in ED clinicians appears relational and continually negotiated, aligning with literature describing recovery as fluid and context-dependent.
Notably, research has revealed substantial discrepancies in how recovery is conceptualized by both LE and non-LE clinicians. In one study, some participants defined recovery as ‘only having a few lingering symptoms’, while others required a complete absence of symptoms for over a decade to consider someone recovered (Bachner-Melman et al., 2021). Other studies have sought to apply more standardized recovery criteria–such as those proposed by Bardone-Cone et al. (2010) – which identify body image disturbance as a key factor distinguishing between full and partial recovery. These definitional inconsistencies complicate efforts to establish universal guidelines for fitness to practice among LE clinicians.
A key question regarded how long an individual was to be in recovery before working in ED services. Some guidance suggests a minimum of 2 years of sustained recovery before entering clinical roles with ED patients (Clothier et al., 1994) – though not universally agreed upon. Rather than having a discrete time-period of recovery, some LE clinicians in the current study described a marked shift in identity that solidified their role as a clinician rather than a patient. This transition reinforced their commitment to recovery and to their new professional responsibilities, distancing them from previous disordered behaviors. The adoption of a professional identity served as a powerful motivator to maintain recovery, raising questions about whether rigid temporal thresholds are always the most appropriate criteria for determining readiness to practice.
LE clinicians bring a heightened sense of empathy, hope, and resilience to their work. Having personally navigated recovery, they may hold a stronger belief in the possibility of change, fostering greater optimism and patience in clinical work (de Vos et al., 2016). This perspective can be particularly powerful in moments of clinical stagnation or relapse, where LE clinicians can tolerate uncertainty and remain hopeful. The shared experiential background also appears to facilitate a sense of connection with patients, as LE clinicians can resonate more fully with the emotional and psychological complexities of their patients’ concerns – enhancing rapport and potentially reinforcing their sense of purpose in work (Bachner-Melman et al., 2021; de Vos et al., 2016; Welch, 2023). However, it could equally be likely that LE could trigger overidentification with patients, necessitating that clinicians are able to carefully management their emotional responses, for example, through supervision.
Self-disclosure emerged as one of the most ethically charged aspects of practice. While selective disclosure could strengthen rapport and instill hope (Simonds and Spokes, 2017), LE clinicians also feared triggering comparison, losing control of personal information, or compromising boundaries (de Vos et al., 2016). These dilemmas might be heightened in ED contexts, where the illness often involves competitive tendencies and scrutiny of others’ bodies. LE in ED services therefore differs from LE in other mental health contexts: the physical visibility of recovery, the salience of comparison, and the risk of bodily appraisal create unique constraints on how LE can be used safely in therapy.
LE clinicians also noted the lack of formal guidance surrounding disclosures (Bachner-Melman et al., 2021). Given the emotional and ethical complexities involved, high-quality supervision should be available for LE clinicians’ wellbeing and professional development. Supervisors must be equipped with skills to sensitively navigate self-disclosures and to provide psychologically informed support and safeguarding. This includes creating a safe, non-judgmental environment where LE clinicians feel able to discuss challenges without fear of stigma or professional consequences.
It is well documented that LE provides clinicians with insights into the patient experience (Curry and Andriopoulou, 2023). LE clinicians often have a firsthand understanding of the systemic and emotional barriers associated with accessing treatment, including being dismissed, misdiagnosed, or navigating fragmented care pathways. Many LE clinicians highlighted how such experiences shaped their attitudes toward current service provision. They emphasized a heightened awareness of how invalidating or inaccessible services can be for individuals with EDs, which in turn appeared to enhance their motivation to advocate for more compassionate, patient-centered care. These reflections suggest that LE may not only shape clinical empathy but also fuel a deeper commitment to service improvement.
Overall, the findings show that LE is both a strength and a source of emotional complexity. Clinicians benefit from deeper empathy, meaningful connection, and enhanced insight into patient experiences, but they must also navigate identity pressures, emotional labor, and careful boundary management. Services should recognize these dualities by providing reflective supervision and fostering non-judgmental organizational cultures.
Limitations
Several limitations should be noted. The sample was predominantly Female and White/White British, which limits the generalizability of the findings and restricts the ability to explore how gender or ethnicity may shape work-related experiences. Additionally, LE clinicians experiencing high levels of burnout may have been less likely to participate due to emotional strain or workload pressures. The study also might not have captured LE clinicians with an increase in symptoms or a relapse due to triggers in their work. Conversely, those more affected by their work may have been more motivated to engage, potentially skewing the sample’s experiences. LE was defined inclusively, encompassing diagnosed EDs, subclinical symptoms, and carer experience. This broad definition captures diverse lived realities but may blur distinctions between qualitatively different experiences. Further, participants held varied professional roles with differing expectations around disclosure and boundaries. Our analytic focus on shared patterns may have obscured role-specific dynamics.
Moreover, interviews were relatively short given the breadth of the guide, limiting depth on some constructs. Relatedly, although the interview schedule covered topics such as organizational support and wellbeing, participants centered their narratives on LE, shaping the analytic focus. Fourth, recovery was self-defined and not measured; participants’ accounts reflect subjective experiences that may fluctuate over time. Finally, while team reflexivity was employed, the primary interviewer’s LE may have influenced interpretation. Findings should therefore be understood as situated and interpretive rather than definitive.
Implications and future research
Services should provide supervisors with training on how to support clinicians navigating LE, particularly regarding disclosure, emotional labor, and identity pressures. Organizational cultures that reduce stigma around LE may enable clinicians to discuss challenges openly. Future studies with larger, role-stratified samples could explore differences between clinical and peer roles, and examine how recovery trajectories interact with professional identity over time.
Conclusion
This study explores the unique perspectives of clinicians who also have a personal experience of an ED, revealing how this dual identity shapes their professional role. LE accounts offered nuanced insights into empathy, role boundaries, hope, and frustration with systems. However, their work is shaped by ongoing identity negotiation, emotional labor, and careful boundary management. LE functions as both a resource and a vulnerability. Recognizing and supporting this complexity is essential for sustaining clinicians and enhancing patient care.
Footnotes
Appendix 1
Interview schedule.
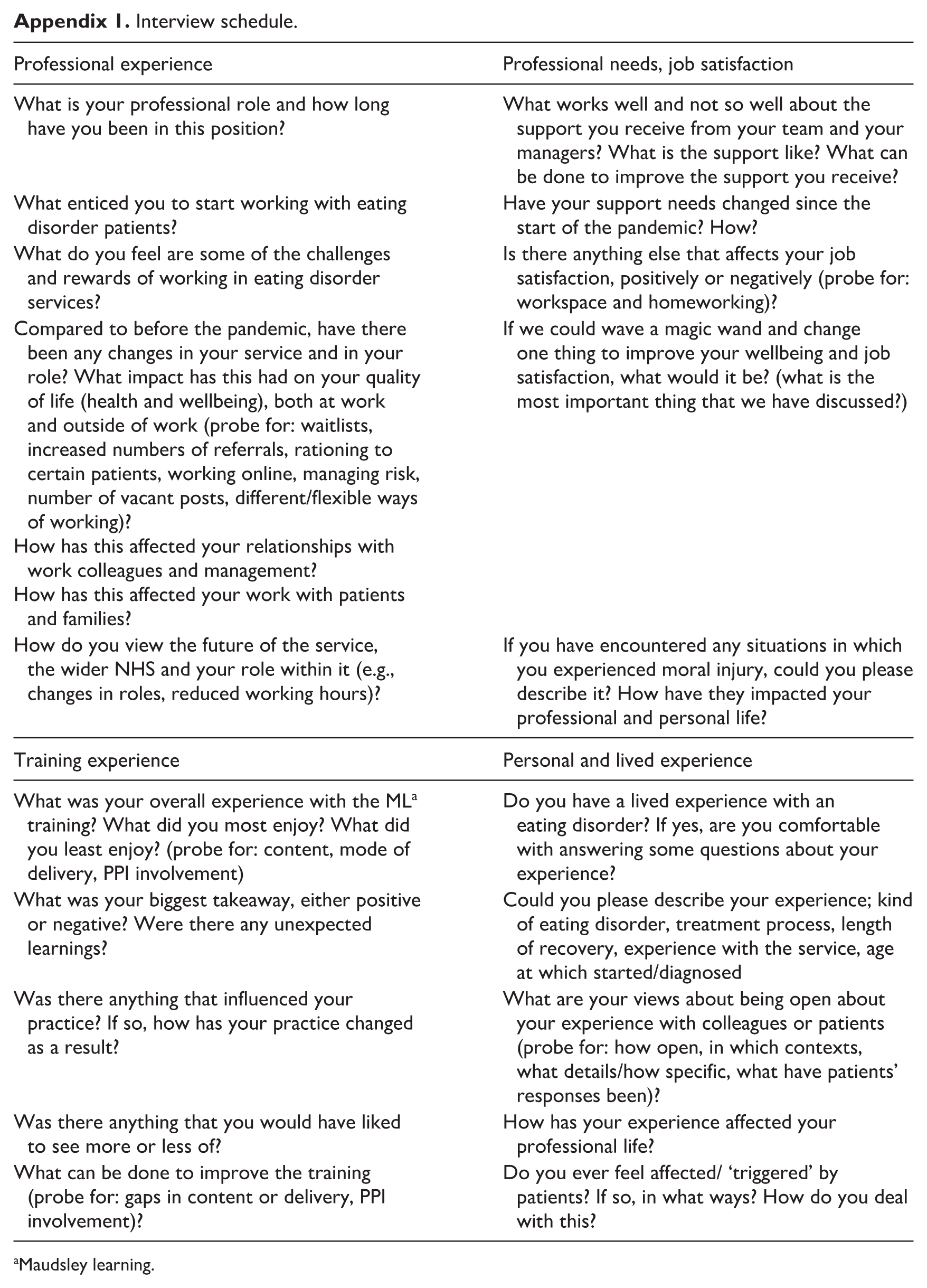
| Professional experience | Professional needs, job satisfaction |
|---|---|
| What is your professional role and how long have you been in this position? | What works well and not so well about the support you receive from your team and your managers? What is the support like? What can be done to improve the support you receive? |
| What enticed you to start working with eating disorder patients? | Have your support needs changed since the start of the pandemic? How? |
| What do you feel are some of the challenges and rewards of working in eating disorder services? | Is there anything else that affects your job satisfaction, positively or negatively (probe for: workspace and homeworking)? |
| Compared to before the pandemic, have there been any changes in your service and in your role? What impact has this had on your quality of life (health and wellbeing), both at work and outside of work (probe for: waitlists, increased numbers of referrals, rationing to certain patients, working online, managing risk, number of vacant posts, different/flexible ways of working)? How has this affected your relationships with work colleagues and management? How has this affected your work with patients and families? |
If we could wave a magic wand and change one thing to improve your wellbeing and job satisfaction, what would it be? (what is the most important thing that we have discussed?) |
| How do you view the future of the service, the wider NHS and your role within it (e.g., changes in roles, reduced working hours)? | If you have encountered any situations in which you experienced moral injury, could you please describe it? How have they impacted your professional and personal life? |
| Training experience | Personal and lived experience |
| What was your overall experience with the ML a training? What did you most enjoy? What did you least enjoy? (probe for: content, mode of delivery, PPI involvement) | Do you have a lived experience with an eating disorder? If yes, are you comfortable with answering some questions about your experience? |
| What was your biggest takeaway, either positive or negative? Were there any unexpected learnings? | Could you please describe your experience; kind of eating disorder, treatment process, length of recovery, experience with the service, age at which started/diagnosed |
| Was there anything that influenced your practice? If so, how has your practice changed as a result? | What are your views about being open about your experience with colleagues or patients (probe for: how open, in which contexts, what details/how specific, what have patients’ responses been)? |
| Was there anything that you would have liked to see more or less of? | How has your experience affected your professional life? |
| What can be done to improve the training (probe for: gaps in content or delivery, PPI involvement)? | Do you ever feel affected/ ‘triggered’ by patients? If so, in what ways? How do you deal with this? |
Maudsley learning.
Appendix 2
COREQ checklist.
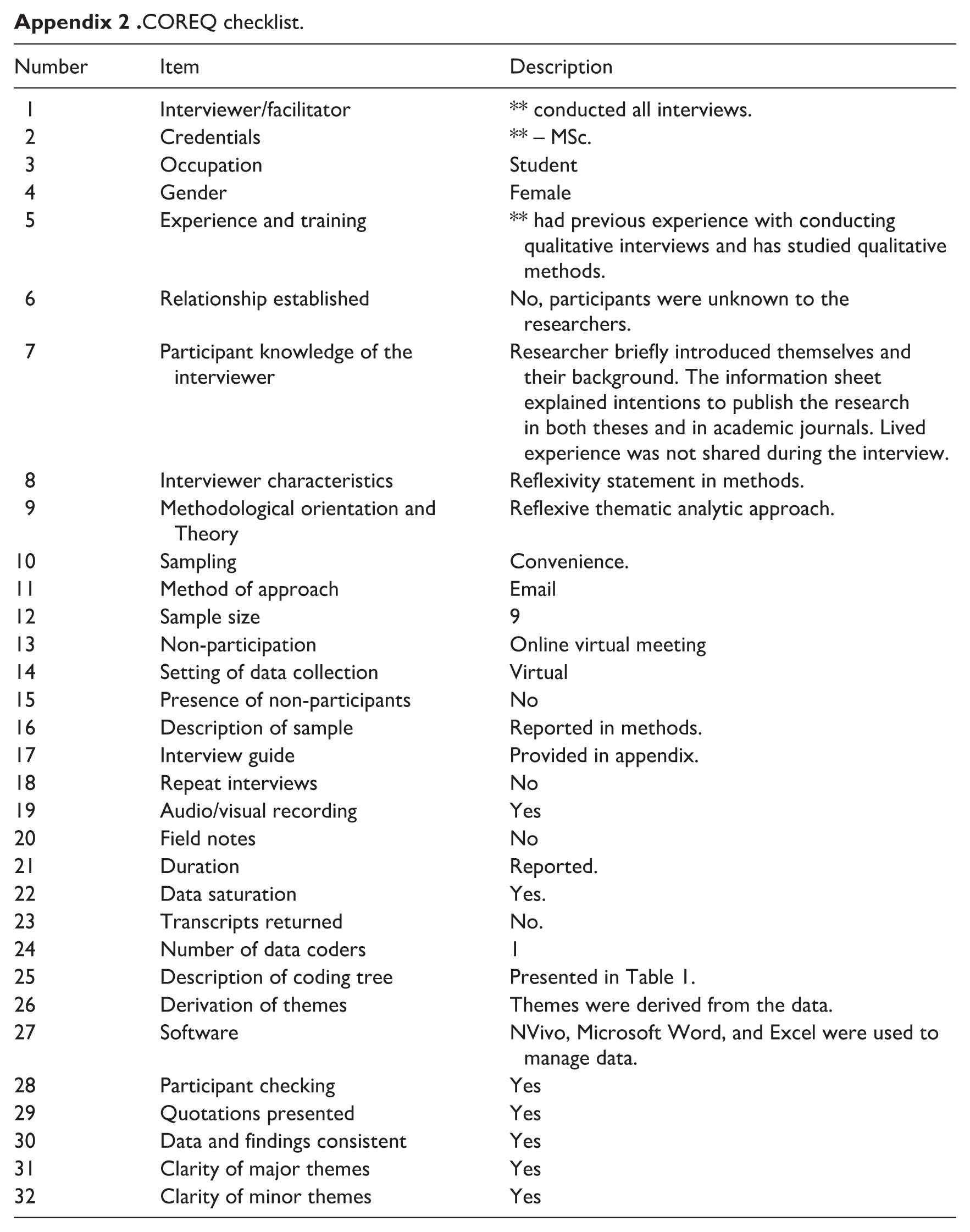
| Number | Item | Description |
|---|---|---|
| 1 | Interviewer/facilitator | ** conducted all interviews. |
| 2 | Credentials | ** – MSc. |
| 3 | Occupation | Student |
| 4 | Gender | Female |
| 5 | Experience and training | ** had previous experience with conducting qualitative interviews and has studied qualitative methods. |
| 6 | Relationship established | No, participants were unknown to the researchers. |
| 7 | Participant knowledge of the interviewer | Researcher briefly introduced themselves and their background. The information sheet explained intentions to publish the research in both theses and in academic journals. Lived experience was not shared during the interview. |
| 8 | Interviewer characteristics | Reflexivity statement in methods. |
| 9 | Methodological orientation and Theory | Reflexive thematic analytic approach. |
| 10 | Sampling | Convenience. |
| 11 | Method of approach | |
| 12 | Sample size | 9 |
| 13 | Non-participation | Online virtual meeting |
| 14 | Setting of data collection | Virtual |
| 15 | Presence of non-participants | No |
| 16 | Description of sample | Reported in methods. |
| 17 | Interview guide | Provided in appendix. |
| 18 | Repeat interviews | No |
| 19 | Audio/visual recording | Yes |
| 20 | Field notes | No |
| 21 | Duration | Reported. |
| 22 | Data saturation | Yes. |
| 23 | Transcripts returned | No. |
| 24 | Number of data coders | 1 |
| 25 | Description of coding tree | Presented in Table 1. |
| 26 | Derivation of themes | Themes were derived from the data. |
| 27 | Software | NVivo, Microsoft Word, and Excel were used to manage data. |
| 28 | Participant checking | Yes |
| 29 | Quotations presented | Yes |
| 30 | Data and findings consistent | Yes |
| 31 | Clarity of major themes | Yes |
| 32 | Clarity of minor themes | Yes |
Ethical considerations
This study was granted ethical approval by the KCL Health Faculties (Blue) Research Ethics Subcommittee, HR/DP-22/23-30046.
Consent to participate
All participants provided written consent prior to their interviews.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: K.N. is supported by a PhD studentship funded by Maudsley Learning. U.S. and J.T. receive salary support from the National Institute of Health Research (NIHR) Biomedical Research Center at the South London and Maudsley NHS Foundation Trust, UK, and King’s College London, UK. The views expressed herein are those of the authors and not necessarily those of the National Health Service (NHS), NIHR or Department of Health and Social Care. U.S. and J.T. are also supported by the Medical Research Council/Arts and Humanities Research Council/Economic and Social Research Council Adolescence, Mental Health and the Developing Mind initiative as part of the EDIFY program (grant number MR/ W002418/1).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author, K.N., upon request.*