
Abstract
Depression is the most common mental disorder in older adults, yet it often remains underrecognized and undertreated despite its serious consequences. This study tested the behavioral model of depression in older adults, using a framework synthesized from the original model and recent systematic reviews. It also incorporated developmentally specific constructs, particularly ego integrity, or meaning in life. A total of 215 older adults (M = 73.6; SD = 5.83; 31% male) completed questionnaires measuring model variables. The original model was not supported, as it did not fit the data. Further analysis revealed predictors explaining 61% of depression variance: emotion-oriented coping, lower avoidant coping, lower social support, lower socio-economic status, lower meaning in life, greater acute impairment, and more sleep disturbances. Findings offer clinically relevant insights for improving intervention strategies in late-life depression, emphasizing the value of addressing meaning in life, coping styles, and functional impairment in therapeutic practice.
Introduction
Depression is the most frequent mental health disorder among older adults (World Health Organization, 2023), experienced by 28%–35% of older adults around the world, as noted by recent meta-analyses (Cai et al., 2023; Hu et al., 2022; Zenebe et al., 2021) Depression in older adults is influenced by various biological, social, and psychological factors (e.g. D’Onofrio et al., 2026; Laird et al., 2019; Szymkowicz et al., 2023), and is related to various negative outcomes, such as increased risk of suicide (Cui and Fiske, 2022), reduced quality of life (Voros et al., 2020), reduced independence in instrumental activities of daily living (Coventry et al., 2020) and have the notable burden of disease worldwide (Cheng et al., 2024). On the other hand, it is often undiagnosed and untreated (Faisal-Cury et al., 2022; Voros et al., 2020), prolonging the distress and complicating recovery among older adults. Multiple studies have shown the success of depression treatment in older age, including psychological, physical, and/or medication-facilitated treatments (Liu et al., 2021; Miller et al., 2020). Hence, depression in older adults is a serious public health issue.
To effectively address depression in older adults, it is crucial to develop and empirically test comprehensive models that elucidate its onset and maintenance, integrating developmentally relevant factors such as its relationship with functional impairment. One such model, proposed by Fiske et al. (2009), builds on elements of the behavioral tradition in understanding depression (Figure 1).
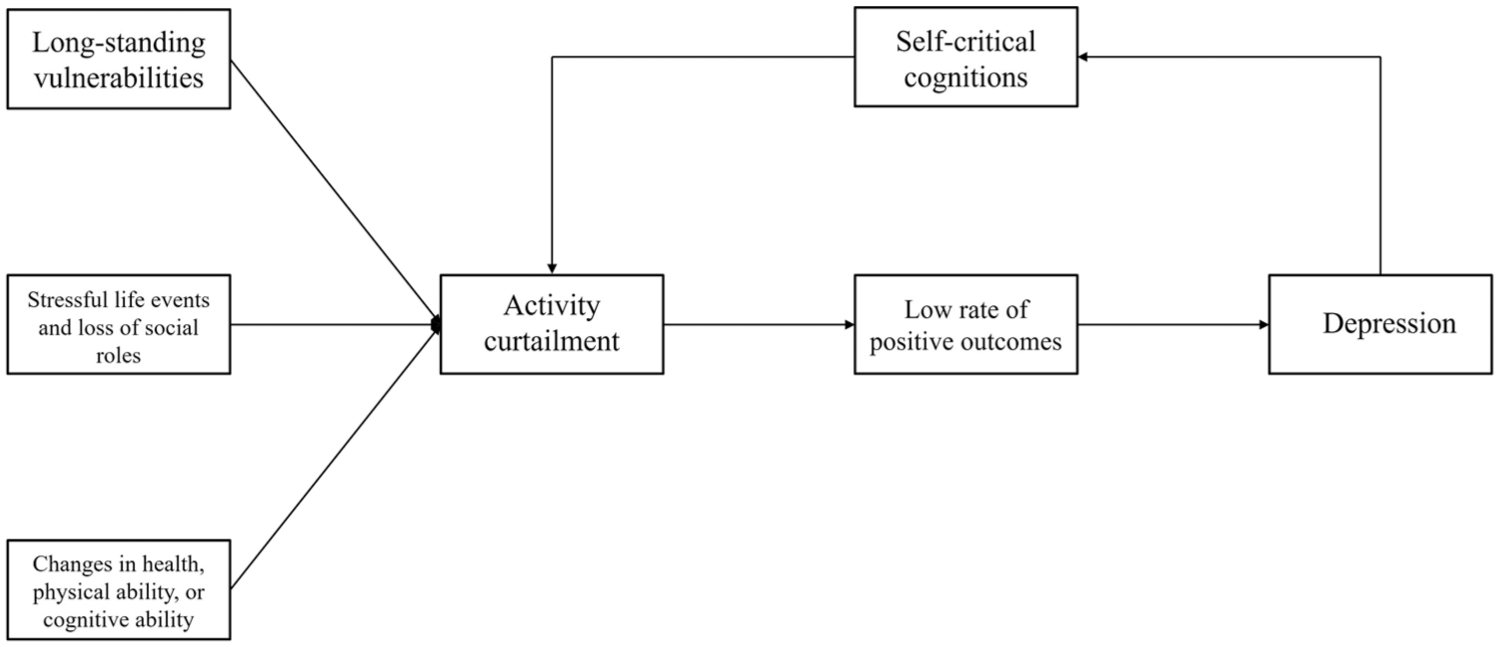
Behavioral model of onset and maintenance of depression.
This model conceptualizes three broad categories of depression predictors: long-standing vulnerabilities; stressful life events and loss of social roles; and changes in health, physical ability, or cognitive ability. Rather than directly causing depression, these factors contribute to the activity curtailment, that is, reduced engagement with the environment, limiting opportunities for positive experiences and outcomes, leading to depression. Additionally, self-critical cognitions that follow depressive affect—such as internal verbalizations about personal failure—serve as both a consequence and further reinforcer of this disengagement, perpetuating a feedback loop that sustains depression (Fiske et al., 2009).
Although this model provides a theoretical and empirically informed framework, to our knowledge, it has never been fully operationalized and tested. Empirical validation is needed to strengthen the understanding of depression in older adults and provide targeted interventions. However, since the model was developed in 2009, it is necessary to reassess its assumptions in light of more recent findings, particularly from recent systematic reviews. It should be noted that the original model primarily focuses on psychological, social, and behavioral determinants of depression in older adults, with less emphasis placed on biological factors. The present study follows this framework.
Present study
In the current study, we used this model as a foundational framework and defined its specific aspects (i.e. variables in each predictor block) based on a synthesis of the original authors’ proposals (Fiske et al., 2009) and the latest research evidence from systematic reviews (Köhler et al., 2018; Maier et al., 2021; Wu et al., 2022; Zenebe et al., 2021).
To preserve the core assumption of the original model regarding long-standing vulnerabilities and their psychological foundations, we retained the concepts of Neuroticism (i.e. Emotionality) and coping with stressful situations, including emotion-oriented and avoidant coping strategies (Fiske et al., 2009), even though they were not assessed in systematic analyses. In addition, we incorporated the concept of lack of social support, as suggested by both the original model (Fiske et al., 2009) and two systematic reviews (Maier et al., 2021; Zenebe et al., 2021). Furthermore, certain socio-demographic variables can be considered long-standing vulnerabilities, such as lower socio-economic status (Fiske et al., 2009; Maier et al., 2021; Zenebe et al., 2021), and a lower educational background (Köhler et al., 2018; Zenebe et al., 2021).
The predictor block of stressful life events and loss of social roles from the original model (Fiske et al., 2009) was further supported by a systematic review indicating the distinct predictive role of acute stress and a history of stressful life events (Zenebe et al., 2021). Therefore, we distinguished between lifetime and acute (past-year) exposure to stressful events to more precisely assess their differential predictive value for depression in older age.
The block addressing changes in health, physical ability, or cognition required refinement. While the original model primarily conceptualized these factors in the context of medical illness (Fiske et al., 2009), a distinction between medical conditions and impairment-related variables appeared more precise, as suggested by previous studies. All systematic reviews identify medical illness as a risk factor (Köhler et al., 2018; Maier et al., 2021; Wu et al., 2022; Zenebe et al., 2021), and at least some forms of impairment (Köhler et al., 2018; Maier et al., 2021; Wu et al., 2022; Zenebe et al., 2021). Following the same analytical approach used for stressful life events, we differentiated between lifetime illness/impairment and acute (past-year) illness/impairment. Lastly, as emphasized in the original model, current sleep disturbances may play an important role in predicting depression in older adults (Fiske et al., 2009), a finding consistently supported by all systematic reviews (Köhler et al., 2018; Maier et al., 2021; Wu et al., 2022; Zenebe et al., 2021).
Furthermore, we argue that the model’s predictive power would be enhanced by incorporating a stronger developmental perspective on aging. A key developmental theory for understanding the psychological dynamics of aging is Erik Erikson’s theory, which describes the eighth and final stage of life—ego integrity—reserved for older adulthood (Erikson, 1987). In his seminal work, Erikson defines ego integrity as a state of mind characterized by “the acceptance of one’s one and only life cycle as something that had to be and that, by necessity, permitted of no substitutions” (Erikson, 1987: 241). Ego integrity, encompassing the process of attributing meaning to one’s life, experiencing a deep sense of certainty in past choices, life satisfaction, gratitude, and an absence of regret, emerges as a complex psychological construct distinctive to older age. Erikson postulates that the failure to reach ego integrity results in ego despair, which has been linked to higher levels of depression (Cetinkol et al., 2020) and lower well-being (van der Kaap-Deeder et al., 2022) in older adults. Therefore, we argue that integrating measures of ego integrity into the model—such as assessments of meaning in life—is essential for a more comprehensive understanding of psychological aging and depression.
Mediator and criterion variables remain consistent with the original model, including activity curtailment, rate of positive outcomes, depression, and self-critical cognitions.
Therefore, the aim of this study was to test the model of the onset and maintenance of depression by Fiske and colleagues (Fiske et al., 2009), incorporating recent findings (Köhler et al., 2018; Maier et al., 2021; Wu et al., 2022; Zenebe et al., 2021) and a developmentally tailored perspective (Erikson, 1987).
Method
Participants
The planned sample size determination followed the suggestion of including at least 10 times more respondents than the number of manifest variables in the model (in this study: 18). Data were collected conveniently from 215 older adults, ranging from 65 to 94 years of age (M = 73.6; SD = 5.83; 31% male). Participants were recruited by a network of trained interviewers within the Red Cross from 14 cities in Serbia, including both urban and rural municipalities. All participants were current or former beneficiaries of various activities organized by the Red Cross, primarily focused on social activities and education.
Measures
The inventories used for the study are the HEXACO Emotionality subscale (Ashton and Lee, 2009), The Coping Inventory for Stressful Situations (Endler and Parker, 1990), The Duke Social Support Index (Koenig et al., 1993), The Meaning in Life Questionnaire (Steger et al., 2006), The Environmental Reward Observation Scale (Armento and Hopko, 2007), The Geriatric Depression Scale (Stolić et al., 2015; Yesavage and Sheikh, 1986), and The Self-critical Cognition Scale (Ishiyama and Munson, 1993). Other inventories are constructed for the purpose of this study, including operationalizations of socio-economic status, educational status, stressful life events, medical illnesses, impairment, sleep disturbance, and activity curtailment. Detailed descriptions of each construct and measure are presented in Supplemental Appendix A.
Procedure
The ethics approval was provided by the Institutional Review Board of the Department of Psychology, Faculty of Philosophy, University of Belgrade (protocol number #2022-017). Instruments that had not been previously translated into Serbian were adapted for this study using a two-way translation process conducted by three psychologists. The translated instruments included the Coping Inventory for Stressful Situations, the Meaning in Life Questionnaire, the Duke Social Support Index, the Environmental Reward Observation Scale, and the Self-Critical Cognition Scale.
Before data collection, trained interviewers from the Red Cross of Serbia participated in a preparatory meeting with the authors to familiarize themselves with the instruments and clarify any concerns regarding the assessment process. Before taking part in the study, participants were informed about their rights. Only those who signed an informed consent form were enrolled in the study.
Data collection took place in 2022, at Red Cross premises, with interviewers administering the survey by reading the instructions, questions, and response options aloud, and then recording participants’ answers. The completion time ranged from 35 to 55 minutes. Upon completing the survey, participants received an explanatory debriefing text designed to mitigate potential distress and provide information on available support resources.
Data analyses
Excluded from the analysis are all respondents who had missing values on the main outcome measure – Geriatric Depression Scale. Descriptive statistics for all scales and correlations between measures were calculated using SPSS 22. The primary analysis employed path analysis to test the model, using AMOS. Model fit was evaluated using the following predefined fit indices: χ2/df, comparative fit index (CFI), normed fit index (NFI), Tucker–Lewis index (TLI), and root mean square error of approximation (RMSEA). Indicators of good fit were: CFI and NFI > 0.90, and RMSEA < 0.08 (Hu and Bentler, 1999), and χ2/df ratio below 2 (Kline, 2005). Previous literature indicates that the predictor variables in the model are not independent; therefore, covariances between these variables are expected and defined in the model based on prior research (e.g. Dunn and O’Brien, 2009; Golovchanova et al., 2021; Greenglass et al., 2006; Halama, 2014; Karimzade and Besharat, 2011; Roohafza et al., 2014).
Data availability
The raw dataset is available on the following OSF link: https://osf.io/wqdv8/overview.
Results
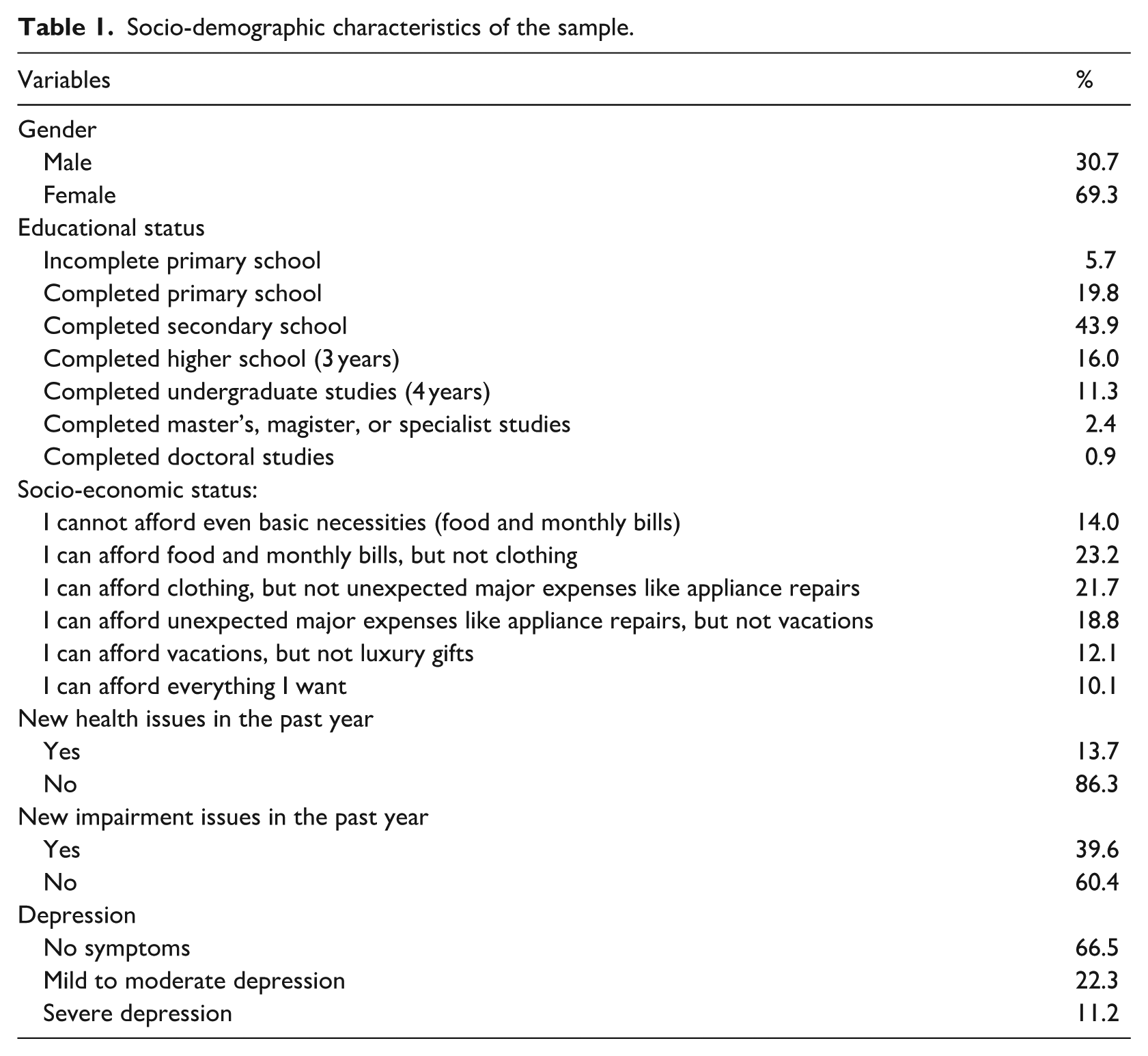
The main socio-demographic characteristics of the sample are shown in Table 1, while a more comprehensive overview is provided in Supplemental Appendix B.
Socio-demographic characteristics of the sample.
The descriptive measures of scales used in the study are presented in Table 2.
Descriptive statistics for scales used in the study.
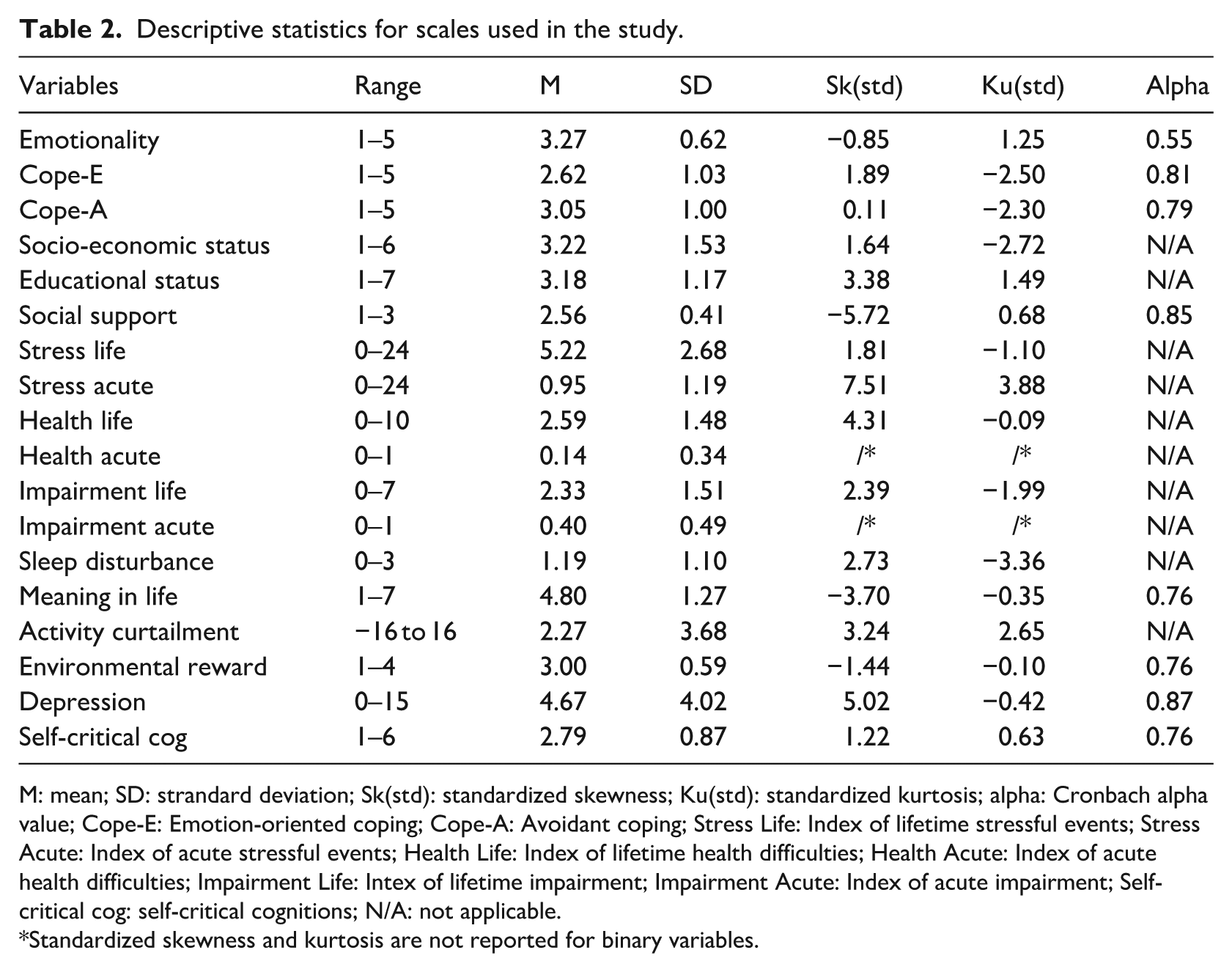
M: mean; SD: strandard deviation; Sk(std): standardized skewness; Ku(std): standardized kurtosis; alpha: Cronbach alpha value; Cope-E: Emotion-oriented coping; Cope-A: Avoidant coping; Stress Life: Index of lifetime stressful events; Stress Acute: Index of acute stressful events; Health Life: Index of lifetime health difficulties; Health Acute: Index of acute health difficulties; Impairment Life: Intex of lifetime impairment; Impairment Acute: Index of acute impairment; Self-critical cog: self-critical cognitions; N/A: not applicable.
Standardized skewness and kurtosis are not reported for binary variables.
Emotionality, Index of lifetime stressful events, Environmental reward, and Self-critical cognitions showed normal distribution, according to standardized skewness and kurtosis. Social support and Meaning in life grouped around higher scores, while the educational status, all health- and impairment-related variables, Activity curtailment, and Depression grouped around lower scores. Acceptable reliability was obtained for all scales used in the study, except for the Emotionality scale. Intercorrelations of all variables are presented in Supplemental Appendix C.
To test the model of onset and maintenance of depression in older adults, a path analysis was employed. The full model structure is presented in Figure 2.
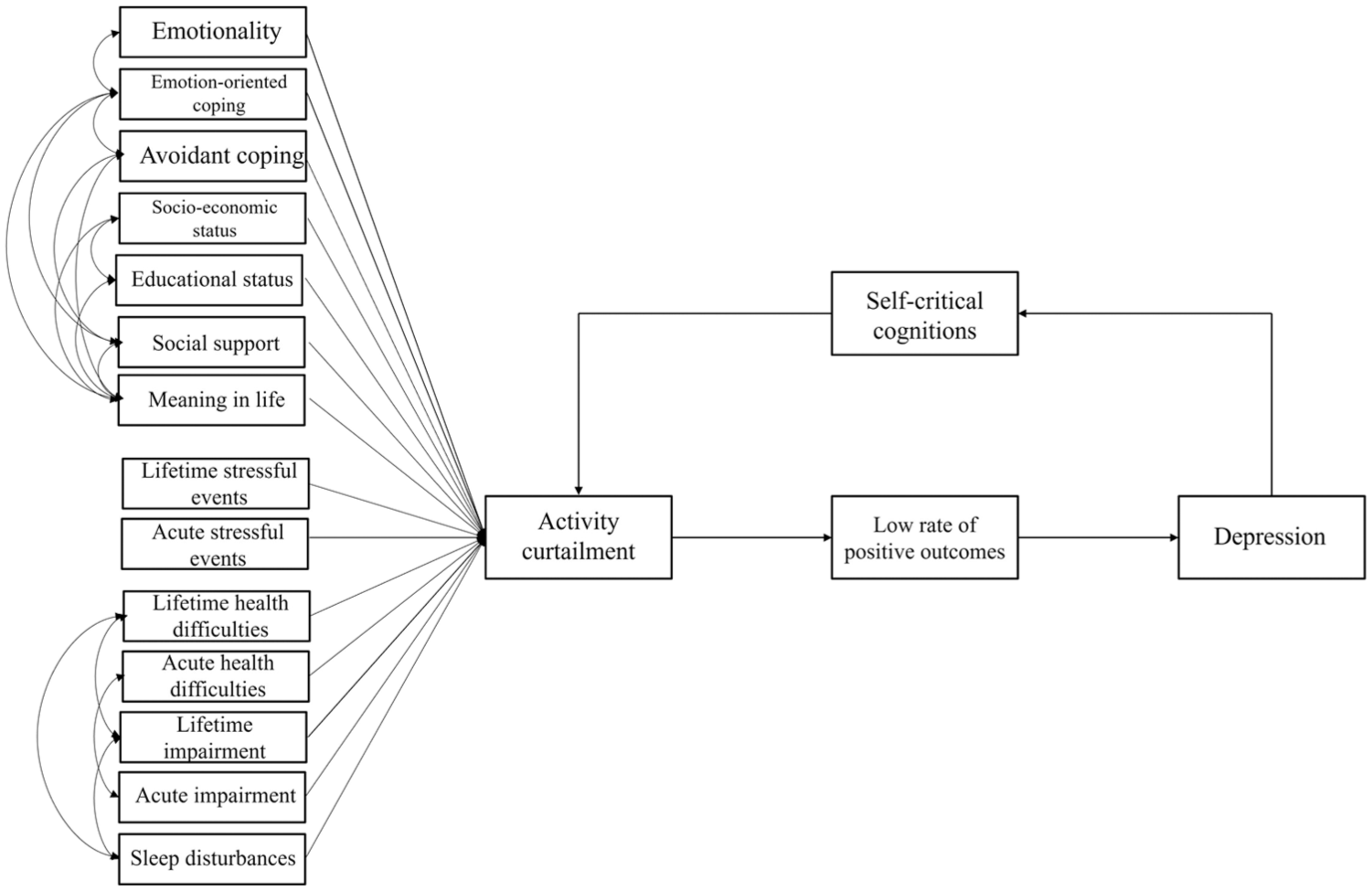
Model structure for path analysis.
The model did not show adequate fit to the data according to any of the indices used [χ2(121) = 482.480, χ2/df = 3.987, p = 0.000, CFI = 0.64, NFI = 0.59, RMSEA = 0.12, TLI = 0.49]. All estimates in the model are listed in Supplemental Appendix D.
According to the authors’ knowledge, the existing literature does not provide recommendations for further adaptations of the original model. Furthermore, the results of this study did not yield unequivocal recommendations that would justify further empirically supported adaptations of the model. Additionally, the key variable in the model, activity curtailment, did not exhibit the expected intensity of relationships with other variables in the model. It showed no significant correlation with most predictor variables, and its correlation with depression itself was also relatively low, around 0.27 (see Supplemental Appendix C).
Considering the lack of adequate theoretical or empirical guidance for further model adaptations from prior literature or this study, and given that one of the central variables, activity curtailment, showed an inadequate and unanticipated relationship with other variables, the research decision was made not to test alternative models. It was concluded that such models would be insufficiently supported both theoretically and empirically. Instead, the focus shifted to comparing the relative contributions of predictors in predicting the severity of depression by applying a multiple linear regression analysis with depression severity as the criterion variable and all predictors in the model as predictor variables. All predictors were entered simultaneously into the multiple linear regression model (enter method). Mediator variables were not analyzed as predictors due to their strong theoretical and empirical connection with depression as the criterion (American Psychiatric Association, 2013; Armento and Hopko, 2007; Fiske et al., 2009). Although some variables showed skewed distributions, assumptions were evaluated at the level of the regression residuals. The distribution of residuals from the regression model did not deviate from normality, based on visual inspection of the histogram and Q–Q plot and a non-significant Kolmogorov–Smirnov test (p > 0.05).
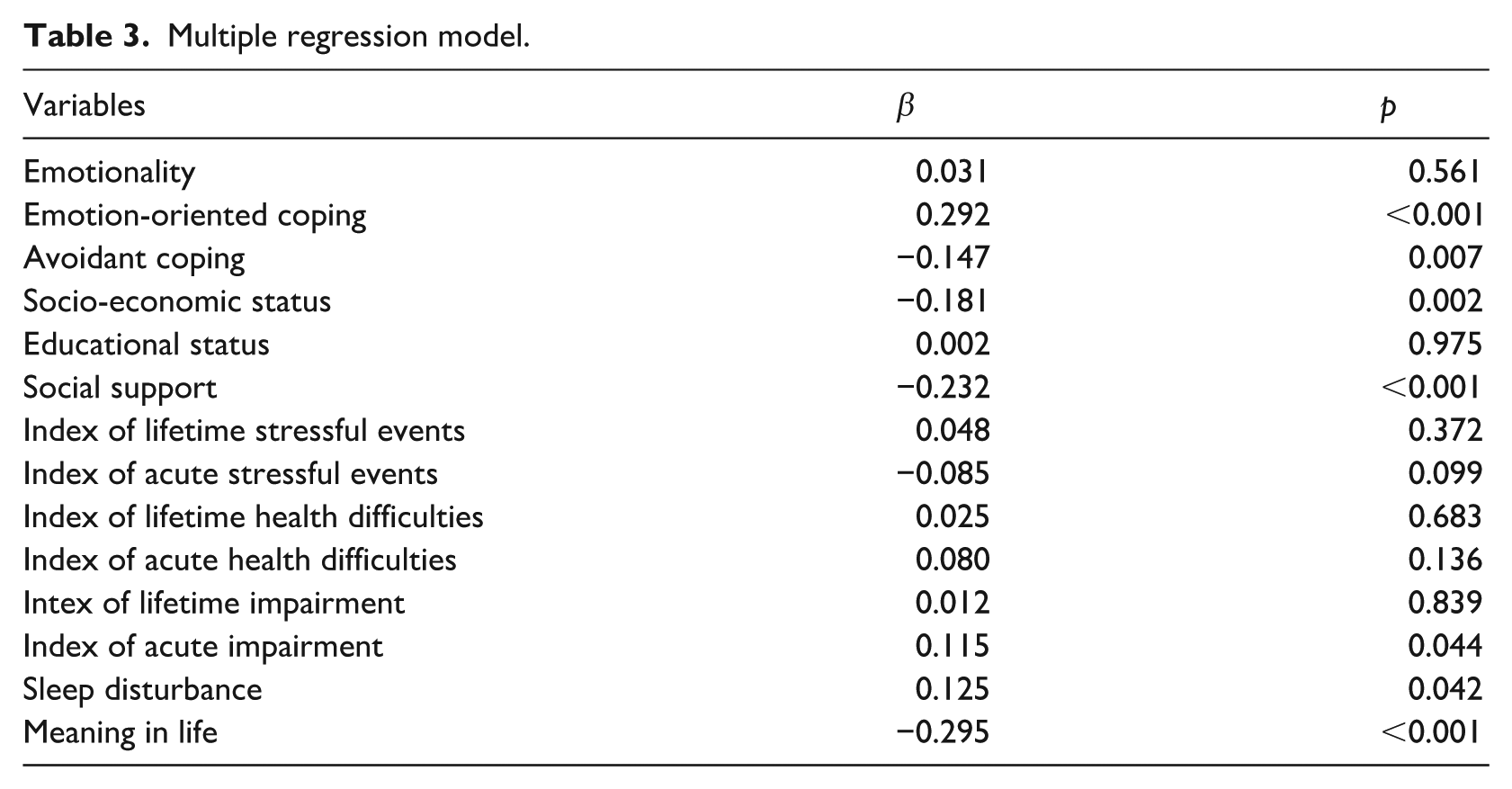
The tested multiple regression model is significant and explains 61% of the variance in depressive symptoms (R2adj = 0.61; F(14) = 20.243, p < 0.001). The results showed that higher levels of emotion-oriented coping, avoidant coping, acute impairment, sleep disturbance, and lower socio-economic status predicted higher depression, while higher social support and meaning in life served as protective factors (Table 3).
Multiple regression model.
Discussion
The aim of this study was to test the model of the onset and maintenance of depression by Fiske and colleagues (Fiske et al., 2009), incorporating recent findings (Köhler et al., 2018; Maier et al., 2021; Wu et al., 2022; Zenebe et al., 2021) and a developmentally tailored perspective (Erik and Erikson, 1987). The study did not support the model of onset and maintenance of depression in older adults. However, additional analysis revealed that emotion-oriented coping, lower avoidant coping, lower social support, lower socio-economic status, higher acute impairment, more pronounced sleep disturbances, and lower meaning in life predict a substantial proportion of variance in depression among older adults.
Behavioral model of onset and maintenance of depression in older adults
This study did not support the model of depression onset and maintenance in older adults (Fiske et al., 2009), as it failed to fit the data according to any predefined fit indices.
Theoretically, this model posits that predictors influence depression indirectly through activity curtailment, which reduces the rate of positive outcomes and triggers depression, which makes activity curtailment central to the model. However, correlation analyses showed weak or nonsignificant links between activity curtailment and most predictor variables (around 0.1–0.2), including only a modest correlation with depression (0.27). If activity curtailment were a key mechanism, stronger associations would be expected. This suggests that reduced activity may not sufficiently explain mediation to depression in older adults, contributing to the model’s poor fit. However, the explanation for the lack of meaningful contribution of activity curtailment may be its inadequate conceptualization in the original model that relies on behavioral tradition. Namely, activity curtailment was assessed across activity types, but the subjective value of these activities was not considered. This behavioral conception contradicts the postulates of Selective Optimization with Compensation (SOC) theory (Carpentieri et al., 2016; Marsiske et al., 1995), which argues that aging individuals adapt to the environment by prioritizing meaningful activities, optimizing their resources, and compensating for losses. Thus, lower activity levels alone may not be sufficient to predict depression without understanding the meaning attributed to these activities, as older adults often adjust their activities in ways that maintain well-being. Some studies indicate this relationship, showing the subjective value of activities to be a strong predictor of depressive symptoms (Agishtein et al., 2013). Hence, future studies should consider the principles of SOC theory when developing alternative versions of the model.
Risk and protective factors for depression
Long-standing vulnerabilities showed relevance in psychological (i.e. coping), social (i.e. social support), and socio-demographic (i.e. SES) domains.
Emotion-focused coping was a significant positive predictor of depression, reinforcing its conceptualization as a maladaptive stress coping strategy consistently associated with depressive symptoms in older adults (Féki et al., 2019; Kraaij et al., 2002a; Kraaij et al., 2002b). Research indicates that this coping strategy directly contributes to depression, independent of stressor type or intensity, while also moderating the impact of stress, particularly severe stressors, amplifying depressive symptoms (Kraaij et al., 2002b). Longitudinal findings also showed that reductions in emotion-focused coping correspond with decreases in depressive symptoms over time (Rodgers et al., 2017).
Avoidant coping, however, demonstrated an unexpected association, with greater use linked to lower depression. While typically considered a maladaptive strategy associated with poor mental health outcomes, including in older adults (Murayama et al., 2020), this result may be influenced by the measurement approach. In this study, some avoidance-related items involved social interactions (e.g. calling a friend in response to stress), potentially confounded with social support. Given the high prevalence of loneliness among older adults (Keck, 2022), social engagement, regardless of its initial function, may serve as a protective factor against depression.
However, it may also be argued that the adaptive value of avoidant coping may shift with age. According to the socioemotional selectivity theory (Carstensen, 2006; Carstensen et al., 1999; Charles and Carstensen, 2010) aging is marked by a motivational shift in which individuals prioritize emotionally meaningful goals. This shift leads older adults to regulate emotions in ways that enhance well-being, including behaviors typically classified as avoidant, such as selective disengagement from distressing situations or avoiding direct confrontation (Birditt et al., 2005; Blanchard-Fields et al., 2007; Charles et al., 2009; Nolen-Hoeksema and Aldao, 2011). Thus, the observed pattern in the data may reflect a strategic reprioritization of goals in later life rather than a maladaptive coping strategy, as it is often considered in younger individuals.
Subjective social support is a key protective factor against depression in older adulthood. Prior research consistently associates subjective social support with lower depression risk, while even social support interventions are shown to be effective in reducing depression symptoms (Lee et al., 2022; Liu et al., 2016; Patra et al., 2017). Moreover, social support serves as a crucial buffer during crises (Alesina and Giuliano, 2010; Bogenschneider et al., 2012). Notably, individuals with greater social support are also more likely to seek help for depressive symptoms (Wang et al., 2023), potentially contributing to better mental health outcomes.
Lower socioeconomic status significantly predicted depression. Prior research consistently links lower SES in older adults to greater depression risk (Kim et al., 2016; Xue et al., 2021), likely due to chronic stressors such as financial insecurity, uncertainty, frequent conflicts, and importantly, an unhealthy lifestyle (Adler and Rehkopf, 2008; Safran et al., 2009; Woolf and Braveman, 2011; Xue et al., 2021). Moreover, limited access to mental health resources may further contribute to this disparity (Bernardini et al., 2021; Ornell et al., 2021). Notably, financial constraints have been identified as a key barrier to seeking professional psychological help in the general population (Živanović et al., 2022).
An unexpected finding in the Lifelong vulnerabilities block was the lack of predictive power of Emotionality for depressive symptoms. While past research links Neuroticism to depression (Hayward et al., 2013; Kendler et al., 2006; Kim et al., 2016), differences in conceptualization between these operationalizations may explain this discrepancy. Unlike Neuroticism in the Big Five (Costa and McCrae, 1992), which includes a Depression facet, Emotionality in HEXACO does not (Ashton and Lee, 2009), potentially weakening its association with depression. Some studies suggest that low Extraversion, particularly Social self-esteem and Liveliness, may be stronger predictors (Međedović et al., 2019). Additionally, the low reliability of the Emotionality scale in this study may have further reduced its predictive validity.
Unexpectedly, neither lifetime nor acute health difficulties, impairments, or stressful events significantly contributed to depression, contrasting with previous findings (Fiske et al., 2009; Köhler et al., 2018; Maier et al., 2021; Wu et al., 2022; Zenebe et al., 2021), and suggesting a lack of predictive power of blocks Stressful life events and loss of social roles, and Changes in health, physical ability, or cognitive ability. Although acute impairment showed a significant effect, this finding should be interpreted with caution due to its marginal significance and suppressor effect, indicated by the absence of a zero-order correlation but a significant effect in regression.
This lack of a direct contribution of these blocks to depression may reflect older adults’ ability to adapt to health challenges and accumulated stressors through effective coping strategies, resource optimization, and compensation (Carpentieri et al., 2016; Marsiske et al., 1995). Over time, individuals develop ways to compensate for physical or functional declines, such as relying on routines or technology that may be a tool for sustaining engagement (Tomaszewski Farias et al., 2018). Similarly, individuals facing stressors may engage in adaptive coping strategies, mitigating their impact on depression, as demonstrated in youth samples (Evans et al., 2015) and suggested by some studies on older adults (Li et al., 2022). Since the regression analysis accounted for empirical correlations between predictors, it is possible that the effects of health difficulties, impairments, and stress were masked by shared variance with psychological functioning variables, such as emotion-focused coping.
However, one health-related variable, sleep disturbance, showed a significant contribution. As the authors of the original model argued, sleep disturbance is an independent risk factor for depression in older adults, often preceding its onset, despite previously being considered a mere manifestation of depression (Fiske et al., 2009). Persistent sleep disturbance has been shown to increase the risk of depression’s development, recurrence, and worsening in this population, with this relationship being bidirectional (Bao et al., 2017; Buysse et al., 2008; Franzen and Buysse, 2008). The significance of sleep disturbance is further supported by several systematic reviews (Köhler et al., 2018; Maier et al., 2021; Wu et al., 2022; Zenebe et al., 2021). In this study, sleep disturbance made a modest contribution. However, given the limited sensitivity of the single-item measure used in this study and in light of robust prior evidence linking sleep disturbance to depression, future studies should consider reevaluating the model using well-established multi-item instruments, such as the Pittsburgh Sleep Quality Index (Buysse et al., 1989) or the Insomnia Severity Index (Morin et al., 2011).
Finally, integrating the developmental perspective of ego integrity into the model proved valuable, as meaning in life emerged as a protective factor against depression in older adults. As central to Erikson’s eighth stage (Erikson, 1987), ego integrity is a defining characteristic of later life, encompassing a sense of meaning, purpose, and acceptance of one’s life as a whole. This finding reinforces the idea that meaning-making is crucial for successful psychological aging, with ego integrity potentially serving as a key protective factor against depression. Beyond theoretical significance, this aligns with previous empirical research demonstrating the link between meaning in life and lower depression in older adulthood (de Maio Nascimento et al., 2024; Lertsuwan et al., 2025; Volkert et al., 2019). Future studies should explore in more depth the core mechanisms and aspects of ego integrity that serve as protection from mental health difficulties.
To conclude the discussion, it is important to note that the frequency of clinically indicative depression in this study (33.5%) aligns with findings from recent meta-analyses, falling within the range of 28%–35% (Cai et al., 2023; Hu et al., 2022; Zenebe et al., 2021). However, since participants verbally reported their answers to interviewers, a methodology that is sometimes assumed to contribute to the under-reporting of depression, it is plausible to suggest that the true incidence of depression may be even higher.
Limitations
Recruitment of Red Cross activities users may bias the sample toward healthier, more socially active individuals, or those with certain traits such as Openness to experience, while immobile, severely ill individuals, or nursing home residents were underrepresented, altogether limiting generalizability. Secondly, due to the small sample size, analyses were conducted on the entire group without age subcategories. However, older age spans decades, with distinct psychological and health characteristics across narrower age groups. The study did not assess the age at which individuals with current depressive symptoms first experienced depression, despite the relevance of distinguishing between early- and late-onset depression. However, the model authors suggest that some older adults with a history of depression (early onset) may still exhibit characteristics of late-onset depression (Fiske et al., 2009). Accordingly, the model was designed to account for both cases (Fiske et al., 2009), a decision we adhered to in this study.
It should be noted that the original model primarily focuses on psychological, social, and behavioral determinants of depression in older adults, with less emphasis placed on biological factors, despite evidence for the biopsychosocial nature of depression in later life (e.g. Laird et al., 2019). Future research should therefore examine how biological determinants could be integrated into the model, as well as how the use of antidepressant medication may influence the observed relationships within the model. Moreover, some variables, such as sleep disturbance, were assessed using single-item measures, a decision made to reduce participant burden and ensure feasibility given the older adult sample, who were required to complete a large battery of instruments. While this approach allowed for practical data collection, it may have limited the statistical power of these variables. Consequently, certain aspects of the model were not explored in sufficient detail and should be reevaluated using more comprehensive assessments in future studies. In addition, the study did not explicitly address the digital aspects of older adults’ lives, which may play an important role in mitigating activity curtailment by enabling engagement through digital technologies. While this is a relevant aspect of older adults’ functioning, it may be more prominent in high-income countries. In Serbia, a middle-income country, digital inclusion among older adults remains limited; for example, 43% of older adults do not use the internet at all (Todorović et al., 2019), and most perceive internet activities negatively (Voza and Fedajev, 2023). Future studies should therefore examine more closely the role of digital technologies in overcoming activity curtailment, as well as potential differences between high-income and low- and middle-income countries.
Finally, a key limitation of this study is its cross-sectional design, which prevents definitive conclusions about the direction of relationships. While grounded in prior theoretical and empirical work, it remains unclear whether some variables—such as meaning in life, emotion-oriented coping, sleep disturbances, social support, and some forms of impairment—are precursors to depression or consequences/manifestations of it. For example, depression may manifest as a sense of meaninglessness, rumination, lower perceived social support, or disrupted sleep. Additionally, the role of coping strategies in mediating the effects of health, impairment, and stress on depression warrants further examination. Given these complexities, longitudinal studies are necessary to clarify the temporal dynamics and potential bidirectional influences among the variables assumed in this model.
Implications
This study highlights the high incidence of depressive symptoms among older adults in Serbia, with one in three individuals affected. Although not epidemiological, the study’s diverse sample offers valuable insights for tailoring mental health interventions in underrepresented contexts. First, given that lower socioeconomic status emerged as a risk factor for depression, mental health services must be cost-free and accessible.
Social support was a key protective factor, pointing to the need for structured community initiatives, such as Centers for Healthy Aging. These should offer preventive programs such as psychoeducation, skill-building, social engagement, and opportunities for meaning-making, such as peer mentoring, creative hobbies, and civic participation. Increasing digital literacy and the use of technology as a means of enhancing social participation should also be explored, as this could contribute to broadening the types of support and engagement provided.
Maladaptive coping strategies were also linked to depressive symptoms, suggesting a role for targeted interventions focusing on stress management, which may include psychoeducation on the nature of stress, effective coping strategies and guidance on how to recognize symptoms of mental health difficulties and when to seek professional support. Moreover, narrative approaches may be effective tools in working with older adults. Psychosocial support programs can be enriched by incorporating personal experiences of participants, allowing individuals to revisit and reinterpret past events. This narrative process fosters new meaning-making and can promote a more hopeful and constructive outlook on the future. While psychosocial interventions are essential, sustainable mental health improvements require systemic measures. Enhancing socioeconomic conditions, expanding lifelong learning opportunities, improving healthcare access, and combating ageism are crucial. These priorities align with the WHO Decade of Healthy Aging framework (World Health Organization, n.d), emphasizing the need for structural reforms in aging policies.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261458206 – Supplemental material for Depression in older adults: Testing the behavioral model of onset and maintenance
Supplemental material, sj-docx-1-hpq-10.1177_13591053261458206 for Depression in older adults: Testing the behavioral model of onset and maintenance by Jana Dimoski, Maša Vukčević Marković, Nataša Todorović, Milutin Vračević and Tamara Džamonja Ignjatović in Journal of Health Psychology
Footnotes
Author note
We declare that this manuscript is entirely original, has not been previously published, and is not presently under consideration for publication elsewhere. The study presents a part of the data from the first author’s master’s thesis (originally written in Serbian language). All named authors have read and approved the manuscript, and no individuals meeting the criteria for authorship are omitted. Additionally, the order of authors presented in the manuscript has received approval from all of the authors.
Ethical considerations
This study was ethically approved by the Institutional Review Board (IRB) of the Department of Psychology, Faculty of Philosophy, University of Belgrade, Serbia (protocol number #2022-017). All participants provided informed consent before being enrolled in the study.
Consent to participate
All participants provided written informed consent before being enrolled in the study.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Author contributions
J.D. Conceptualization; Methodology; Formal analysis; Data Curation; Writing – Original draft; Writing – Review & Editing; M.V.M. Conceptualization; Methodology; Writing – Review & Editing; Supervision; N.T. Investigation; Resources; Writing – Review & Editing; M.V. Investigation; Resources; Writing – Review & Editing; T.Dž.I. Writing – Review & Editing; Supervision
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Partial financial support was received by the Ministry of Science, Technological Development, and Innovation of the Republic of Serbia as part of the funding for scientific research at the University of Belgrade – Faculty of Philosophy (Čika Ljubina 18-20, 11000 Belgrade, Serbia; Contract No. 451-03-137/2025-03/200163).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data transparency statement
The data reported in this manuscript were collected as part of a larger data collection effort. However, no other manuscripts using these data have been submitted or are planned for submission in the near future. A brief, descriptive report intended for the lay public has been published in Serbian.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.