
Abstract
This study was conducted to determine the pain beliefs of individuals with chronic illnesses. The mean psychological belief score of the participants was 4.27 ± 1.02, and the mean organic belief score was 3.82 ± 0.68. Women had higher scores on the psychological beliefs subscale (p = 0.002), while married individuals had higher scores on the organic beliefs subscale (p = 0.045). Participants who reported experiencing pain “always” throughout their lives had higher organic (p = 0.016) and psychological (p = 0.001) belief scores. Additionally, those who experienced every day pain in the last 6 months had higher organic belief scores than individuals reporting no pain (p = 0.005). According to the regression analysis, female gender (β = −0.265; p = 0.003) and lifetime pain experience (β = 0.273; p = 0.005) significantly predicted psychological beliefs, while the frequency of pain experienced in the last 6 months significantly predicted organic beliefs (β = 0.242; p = 0.020). Overall, gender, marital status, and pain experience frequency were found to influence pain beliefs.
Introduction
Chronic diseases are health conditions that persist for 1 year or longer, cannot be completely cured, and require lifelong medical treatment and care. In addition to a sedentary lifestyle and unhealthy dietary habits, adverse environmental factors such as air and environmental pollution, poor housing conditions, limited availability of green spaces, and restricted access to healthcare services play a significant role in the increasing prevalence of chronic diseases (Çakmak and Sarı, 2024). Chronic diseases can be classified according to their etiological causes, affected organs or systems, duration, prevalence, functional impairments, and their impact on public health (World Health Organization (WHO), 2005). According to the World Health Organization (WHO, 2025), chronic diseases (noncommunicable diseases) account for approximately 75% of all deaths worldwide. Cardiovascular diseases, cancers, chronic respiratory diseases, and diabetes are the leading causes of these deaths.
The long-term course of chronic diseases, their impact on quality of life, and recurrent symptoms create multidimensional challenges in individuals’ lives. Among these challenges, pain is one of the most common and most debilitating problems. The International Association for the Study of Pain (IASP) defines pain as “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage” (International Association for the Study of Pain (IASP), 2021). This definition demonstrates that pain is not merely a physiological response to a physical stimulus but a complex experience encompassing biological, psychological, and social components. In chronic diseases such as musculoskeletal disorders, diabetes, cancer, COPD, and heart failure, pain occurs as part of the natural course of the disease and negatively affects individuals’ physical, psychological, and social well-being (Bayer and Uzuntarla, 2022; Ceyhan et al., 2022).
The level of pain perceived by an individual is influenced by several factors, including stress, past trauma, psychological state, and social support (Aboushaar and Serrano, 2024). Therefore, in individuals with chronic diseases, pain is not only a symptom but also a determining factor in the course of the disease, treatment adherence, and psychological resilience. Increased neural sensitization, chronic inflammation, and tissue damage contribute to persistent pain, which may lead to sleep disturbances, mood changes, social isolation, and reduced quality of life (Zhang et al., 2025). Decreased ability to perform daily activities, reduced occupational performance, and loss of independence are also frequently observed consequences (Kufacı and Mumcu, 2022).
One of the important factors influencing individuals’ pain experience is their pain-related beliefs. Beliefs are mental structures developed throughout life in interaction with the cultural environment and reflect individuals’ personal assumptions about the world. These beliefs can directly influence treatment adherence, perceived outcomes, and life satisfaction (Shalev et al., 2021). Personal ideas regarding the cause of pain—such as whether pain is of physical or psychological origin—shape individuals’ coping strategies (Birge and Mollaoğlu, 2018). Pain beliefs refer to individuals’ causal interpretations regarding the origin of pain. In other words, they encompass beliefs about whether pain is attributed to physical or psychological factors. This concept differs from broader constructs related to pain that involve cognitive distortions, such as catastrophizing and fear-avoidance beliefs. According to Beck’s cognitive model, individuals’ emotional and behavioral responses are determined not by the events themselves, but by their cognitive interpretations of those events. In this context, cognitive distortions refer to systematic biases in thinking processes (Beck and Haigh, 2014). However, pain beliefs represent individuals’ cognitive attributions regarding their pain. Pain beliefs are commonly examined in two main dimensions: organic and psychological. Because organic pain beliefs conceptualize pain as resulting from physical injury or bodily dysfunction, individuals with such beliefs more frequently adopt problem-focused and biomedical coping strategies in pain management. The most commonly preferred strategies include seeking medical care, adherence to pharmacological treatment, and participation in physical rehabilitation interventions. Organic pain beliefs have generally been reported to be associated with higher levels of treatment engagement and greater adherence to medical recommendations. (Babadağ and Alparslan, 2017; Baird and Haslam, 2013; Özdemir and Afşar, 2023). In psychological pain beliefs, pain is more commonly attributed to emotional states, stress, and cognitive processes. This belief pattern is associated with emotion-focused coping strategies, such as avoidance, catastrophizing, passive coping, and reduced activity levels These coping styles have been associated with reduced treatment engagement and lower adherence to medical interventions (Babadağ and Alparslan, 2017; Kılıç and Alkan, 2021). Recent studies show that pain-related beliefs, as a cognitive construct, play a significant role in pain perception and treatment engagement (Jensen et al., 2021). Pain beliefs are reported to be more prominent in individuals with chronic pain and influence physical mobility, daily functioning, and quality of life (Kılıç and Alkan, 2021). On the other hand, pain beliefs are not independent of one another; rather, they may coexist simultaneously and overlap within individuals.
In addition, sociodemographic factors such as age, gender, marital status, education, socioeconomic status, and geographical and cultural environment, as well as disease-related characteristics, significantly affect individuals’ pain beliefs (Fillingim, 2023; Korkmaz Yaylagül and İmancıoğlu, 2022; van Hecke et al., 2013). In addition, psychological factors are also known to influence pain. For example, depression has been reported to show a stronger association with pain in women, whereas anxiety demonstrates a stronger relationship with pain in men (Keogh, 2025). Age is another important variable influencing pain, and the age-related outcomes of pain perception are complex. Pain is a subjective experience, and multiple cognitive and affective factors contribute to the modulation of pain. Age-related cognitive and emotional changes may affect pain perception. It is well established that the prevalence of chronic pain increases with age, and older adults tend to experience more pain-related problems. Moreover, previous pain experiences may also influence how older individuals respond to painful conditions (Zhi et al., 2024). Similarly, being married has been associated with higher reporting of pain, which may be explained by increased caregiving responsibilities and role-related stress. Individuals with lower economic income tend to report higher psychological pain beliefs, possibly due to increased stress, limited access to healthcare resources, and greater exposure to adverse life conditions. Lower educational levels have been associated with stronger organic pain beliefs, as individuals may be more likely to attribute pain primarily to physical or biomedical causes (Koçoğlu and Özdemir, 2011; Özdemir and Tokaç Akdeniz, 2023). In addition, cultural values, beliefs, and traditions may shape pain beliefs. Differences in pain-related beliefs and coping strategies across countries have been reported, indicating that pain beliefs are influenced by cultural and contextual factors (Ferreira-Valente et al., 2023; Sharma et al., 2020). For example, in some cultures, pain is perceived as something that should be endured, which may lead individuals to limit its expression, whereas in others, openly expressing pain is more acceptable.
Pain is not a symptom present in all chronic illnesses; however, it is one of the most commonly reported experiences among individuals with chronic conditions. In addition, pain may occur intermittently during the course of many diseases. The potential of chronic illnesses to cause physiological changes, functional limitations, and ongoing health-related stressors may influence how individuals interpret pain-related experiences and how they respond to them (Caneiro et al., 2021). For example, beliefs about the identity, causes, duration, and consequences of pain are shaped by previous experiences (Baird and Haslam, 2013; Edwards et al., 2011). In this context, it is not necessary for individuals to experience pain directly; prior experiences and the meaning attributed to pain may influence the development of pain beliefs. Studies examining pain within the framework of the cognitive–behavioral model emphasize the importance of how individuals interpret pain and the meaning they attribute to it (Edwards et al., 2016; Ehde et al., 2014; Turk and Okifuji, 2002; Vlaeyen and Linton, 2000). Within this approach, cognitive processes shaped by individual characteristics are considered to play a significant role in the interpretation of pain and the attributions individuals make regarding their pain (Koçoğlu and Özdemir, 2011). In conclusion, in individuals with chronic diseases, pain is not merely a physiological symptom but is closely intertwined with belief systems, psychological state, and lifestyle. Therefore, understanding and assessing pain-related beliefs is important for identifying individualized coping strategies and highlight the need for a holistic approach within nursing care. Pain beliefs are cognitive beliefs that can be present in all individuals. However, these beliefs may become more prominent in individuals with chronic diseases, for whom pain is one of the most commonly reported symptoms. However, this study does not focus on factors that influence the intensity of pain, but rather on how individuals interpret and attribute meaning to their pain. Although chronic diseases vary in their characteristics, studies examining how individuals with these conditions attribute meaning to their pain appear to be limited. Understanding these attributions is considered important for individualized care and effective pain management. Based on previous literature, it was expected that sociodemographic variables such as age, education level, marital status, and socioeconomic status would influence pain beliefs. Therefore, the present study was conducted to determine the factors affecting pain beliefs in individuals with chronic diseases.
Research Questions:
What are the pain belief levels of individuals with chronic diseases?
Which sociodemographic and clinical variables are significant predictors of organic and psychological pain belief subscale scores?
Methodology
Study setting and participants
The study, designed as a descriptive and cross sectional research, was conducted between November 2024 and June 2025 in the Orthopedics, Cardiology, Internal Medicine, and Neurology clinics of a hospital located in the northwestern region of Türkiye. The sample of the study consisted of individuals with chronic diseases who were hospitalized in these clinics and met the inclusion criteria. The sample size was calculated using G*Power based on Cohen’s classification of effect sizes (Cohen, 1988), taking a medium effect size for multiple linear regression (R2 = 0.13), with 95% power and a 5% margin of error, resulting in a required sample of 122 participants. Data were collected using a convenience sampling method, and the study was completed with 126 patients.
The inclusion criteria for the study were: being hospitalized, having a chronic disease, being willing to participate in the research, and being 18 years of age or older. The exclusion criterion was having insufficient cognitive ability to answer the questionnaire items.
Measures
Patient Information Form
The patient information form was developed by the researchers in line with current literature (Birge and Mollaoğlu, 2018; Koçoğlu and Özdemir, 2011; Özdemir and Afşar, 2023; Özdemir and Tokaç Akdeniz, 2023; Şevgin et al., 2023) to collect demographic and health-related information about the patients. The form includes questions on sociodemographic characteristics such as age, gender, marital status, educational status, and income level, as well as disease-related characteristics such as type of chronic illness and the clinic where treatment is received. In addition, the form contains questions regarding pain characteristics, including the presence of pain and frequency of pain episodes.
Pain Beliefs Scale
The Pain Beliefs Scale was originally developed by Edwards et al. (1992) to evaluate the psychological and organic attributions of individuals with chronic pain regarding the origin of pain and to address a gap in the literature. The Turkish adaptation and reliability study of the scale was conducted by Sertel Berk (2006). The Pain Beliefs Scale consists of 12 items and two subscales, organic pain beliefs and psychological pain beliefs. The organic pain beliefs subscale reflects beliefs that pain primarily results from physical injury or bodily damage (e.g. “Pain results from damage to the tissues of the body.”). The psychological pain beliefs subscale reflects beliefs that pain is influenced by emotional or psychological factors (e.g. “Being anxious makes pain worse.”). It is structured as a likert type scale, with response options scored from 6 (“always”) to 0 (“never”). The score for each subscale is calculated by dividing the total score obtained from the items in that subscale by the number of items. Higher subscale scores indicate stronger pain-related beliefs in the respective dimension, whereas lower scores indicate weaker belief levels. In the Turkish validity and reliability study, the Cronbach’s alpha coefficients were reported as 0.73 for the psychological beliefs subscale and 0.71 for the organic beliefs subscale. In the present study, the Cronbach’s alpha coefficient was calculated as 0.64 for the psychological beliefs subscale and 0.70 for the organic beliefs subscale.
Procedure
The study data were collected by the researchers through face to face interviews conducted in the hospital setting with individuals who were hospitalized, had a history of chronic illness, and met the inclusion and exclusion criteria. Data were collected during time periods that were convenient for the patients. Before the study, the individuals were informed about the purpose of the study and their written and verbal consents were obtained.
Data analysis
Statistical analysis of the study data was performed using IBM SPSS 25.0 (Armonk, NY, USA) software. All analyses were based on 95% confidence interval and p < 0.05 was accepted as significance level. In addition to descriptive statistics (mean, standard deviation, median, frequency, percentage, minimum and maximum values), Shapiro-Wilk and Kolmogorov-Smirnov tests were used to evaluate the distribution properties of the parameters; it was determined that the data showed normal distribution. Accordingly, the relationships between the variables were analyzed by Pearson correlation analysis. In quantitative variables, Independent Groups t test was used for comparisons between two groups (gender, marital status, employment status, pain experience in the past 6 months and year) and One-Way Analysis of Variance (ANOVA) was used for comparisons involving more than two groups (age groups, educational status, income status, chronic disease characteristics, pain frequency in the last 6 months, the last year, and over the lifetime, most frequent type of pain, pain coping methods). In cases where a significant difference was found after ANOVA, Tukey test was applied to determine between which groups the difference was between. It was determined that the data were suitable for multiple linear regression analysis and accordingly, multiple regression analysis was performed to examine the effects of independent variables on the dependent variable. Regression coefficients were calculated using the “Enter” method.
Ethical considerations
Ethics committee and institutional permissions were obtained from the Bezmialem Vakif University Non-Interventional Research Ethics Committee (Date: 27.02.2025/Subject: 64) and the Bezmialem Vakif University Health Practice and Research Center (Date: 09.01.2025/Number: 178346). Permission to use the Pain Beliefs Scale, which was used to collect the research data, was obtained from the author. Written and verbal informed consent forms were obtained from the patients who agreed to participate in the study. The principles of the Declaration of Helsinki were adhered to throughout the study.
Results
Sociodemographic, disease, and pain characteristics
The mean age of the 126 individuals who participated in the study was 60.77 ± 17.54 years, 66.7% of the participants were aged 60 years or older; 55.6% were female, and 81.7% were married. It was found that 40.5% of the patients were primary school graduates, 77.8% were not employed in any job, and 47.6% reported having an income equal to their expenses. Additionally, 35.7% of the participants were hospitalized in Internal Medicine clinics. Regarding chronic disease characteristics, 19% of the individuals had hypertension and 15.9% had diabetes mellitus, followed by heart, lung, and kidney failure diagnoses. A total of 37.3% of the patients stated that they had experienced pain at certain times throughout their lives. Furthermore, 82.5% reported experiencing pain within the past year, and 94.4% reported experiencing pain at a frequency of 1–3 times per week during the past 6 months. Among the reported pain experiences, 52.4% were found to be musculoskeletal in origin. While 74.6% of the patients indicated that they used analgesics to cope with pain, 25% preferred activities such as massage, hot–cold application, prayer, meditation, and walking (Table 1).
Sociodemographic, disease, and pain characteristics (n = 126).
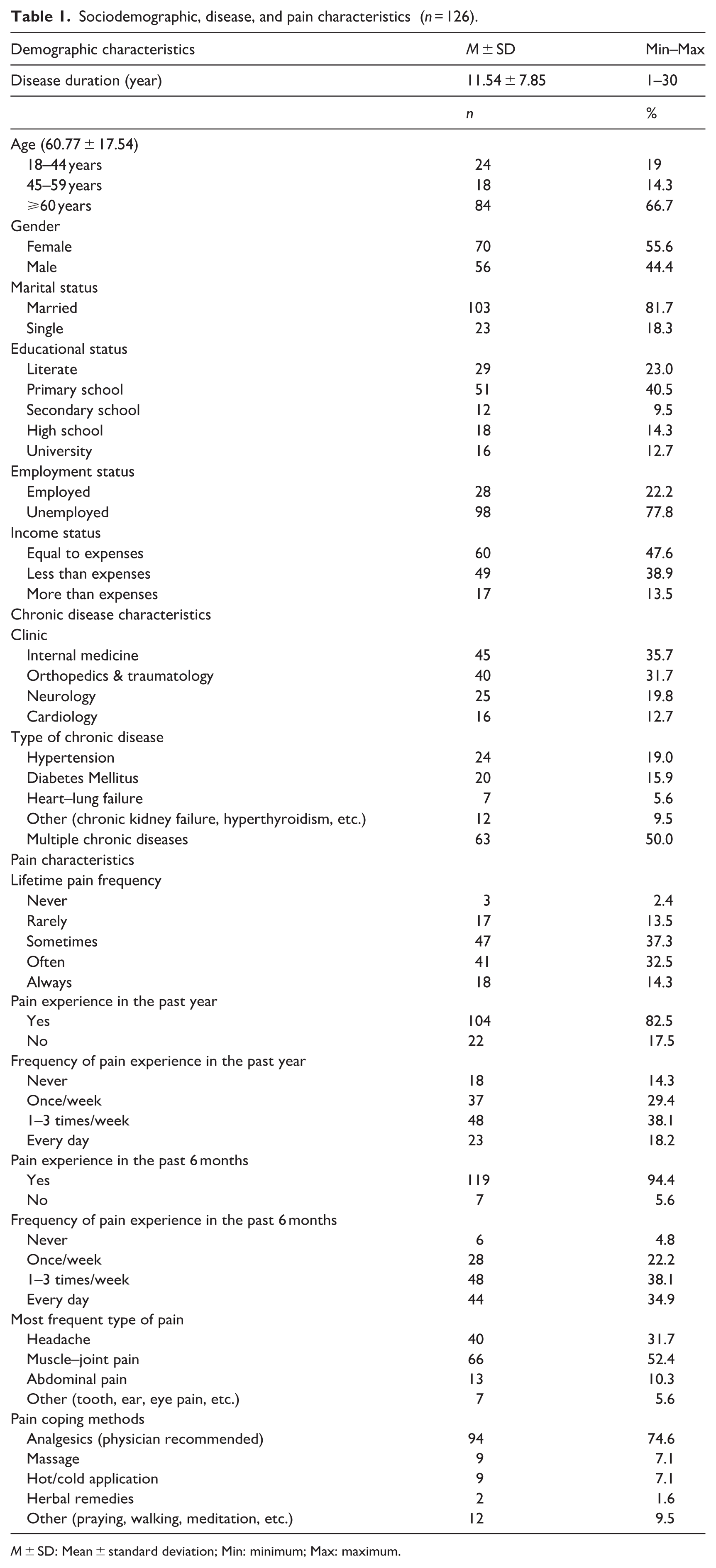
M ± SD: Mean ± standard deviation; Min: minimum; Max: maximum.
Pain beliefs scale results
The mean score of the organic beliefs subscale of the Pain Beliefs Scale was 3.82 ± 0.68, while the mean score of the psychological beliefs subscale was 4.27 ± 1.02. The Cronbach’s alpha coefficients for the scale subscales were 0.70 for organic beliefs and 0.64 for psychological beliefs, respectively (Table 2).
Pain Beliefs Scale results.
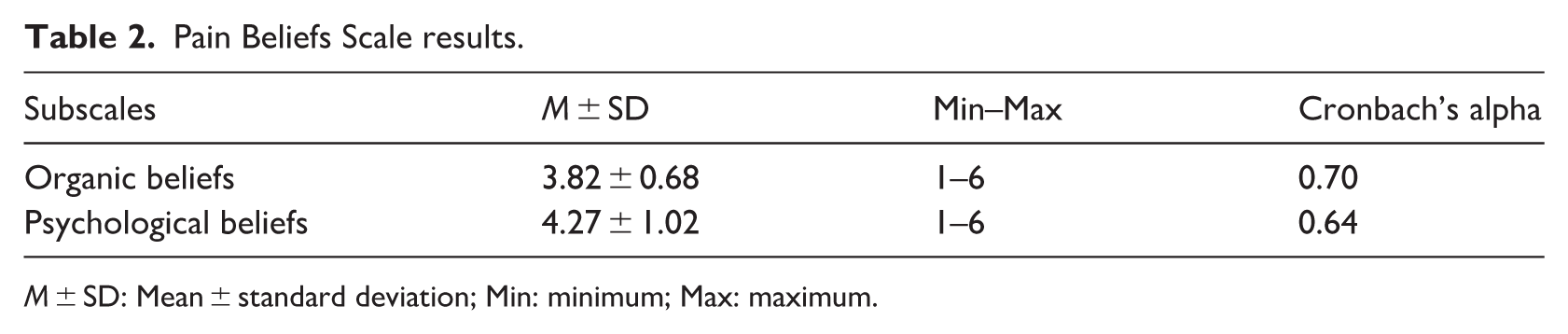
M ± SD: Mean ± standard deviation; Min: minimum; Max: maximum.
Comparison of scale subdimension scores by sociodemographic, disease, and pain characteristics
No significant relationship was found between duration of chronic illness and organic belief (r = 0.128; p = 0.155) or psychological belief scores (r = 0.061; p = 0.500). There were no significant differences in pain beliefs based on age groups, education level, employment status, income status, clinic of treatment, type of chronic illness, or pain-coping methods (p > 0.05). Female participants had higher psychological belief scores than males (p = 0.002), and married individuals had higher organic belief scores than single individuals (p = 0.045). Participants who reported experiencing pain “always” throughout their lifetime had higher psychological (p = 0.001) and organic (p = 0.016) belief scores than those who reported experiencing pain rarely. Although participants who answered “yes” to experiencing pain in the past 6 months had higher organic (p = 0.019) and psychological (p = 0.019) belief scores, when pain frequency was considered, only those experiencing every day pain had higher organic belief scores compared with those reporting no pain (p = 0.005). No significant differences were found between pain beliefs and pain experience or frequency in the past year (p > 0.05; Table 3).
Comparison of scale subscales according to sociodemographic, disease, and pain characteristics.
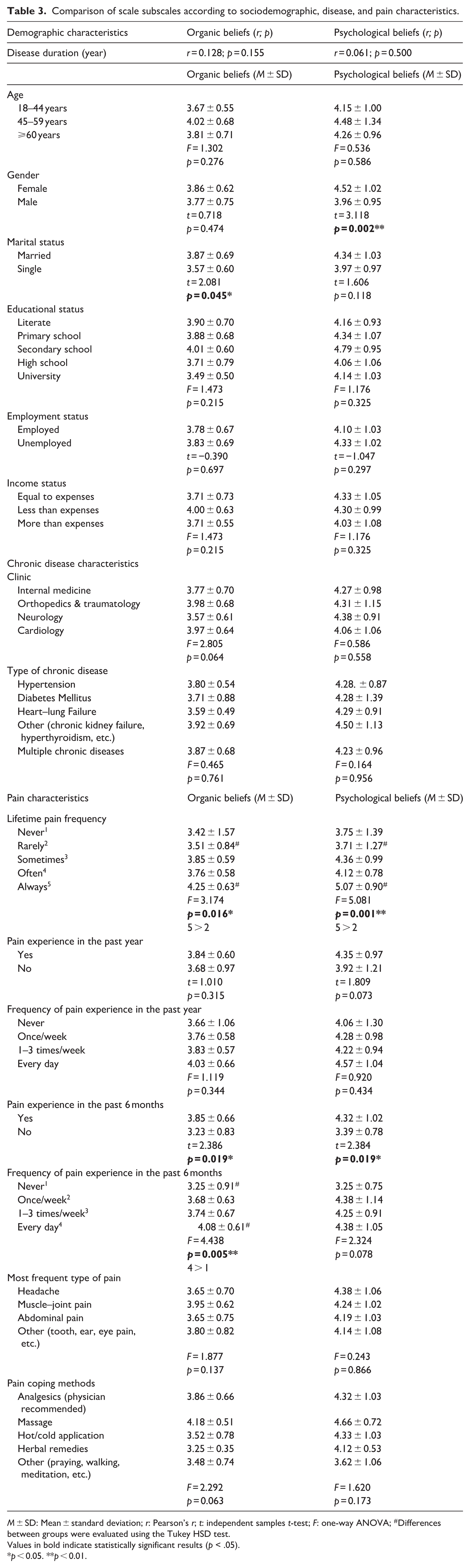
M ± SD: Mean ± standard deviation; r: Pearson’s r; t: independent samples t-test; F: one-way ANOVA; #Differences between groups were evaluated using the Tukey HSD test.
Values in bold indicate statistically significant results (p < .05).
p < 0.05. **p < 0.01.
Predictors of pain belief scale subdimension scores according to regression analysis
The regression analysis results obtained from the study showed that the scores of the organic beliefs subscale were consistent with the independent variables, the overall model was significant, and the independent variables (marital status, lifetime pain frequency, frequency of pain experience in the past 6 months and year) explained 11% of the variance in the dependent variable (R = 0.372, R2 = 0.138, Adjusted R2 = 0.110, F = 4.857, p = 0.001). According to the multiple regression analysis, a one–standard deviation increase in the frequency of pain experienced in the last 6 months resulted in a 0.242 standard deviation increase in organic belief scores (p = 0.020). Marital status did not have a predictive effect on organic beliefs (Table 4).
Multiple linear regression analysis results of the organic belief subscale scores.
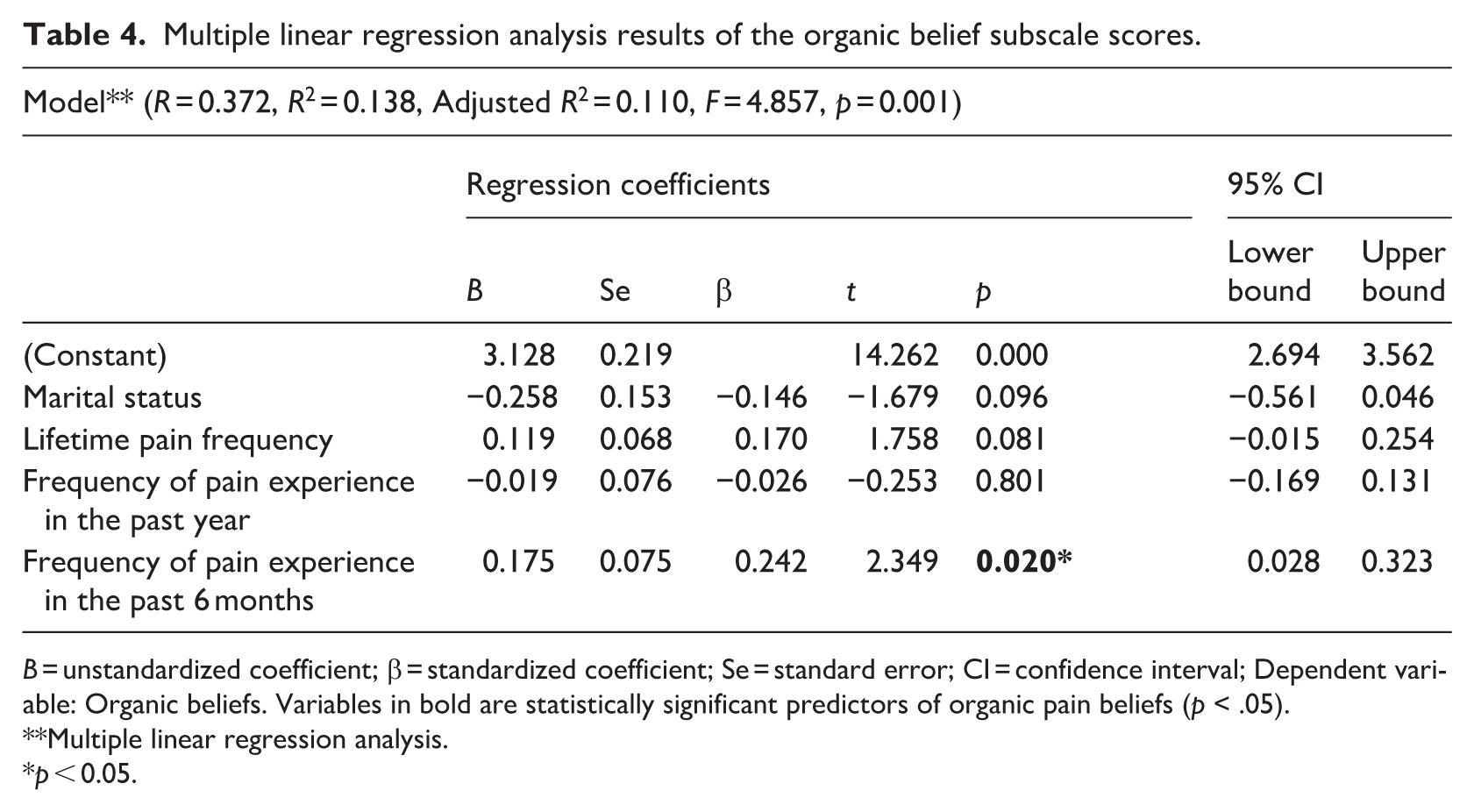
B = unstandardized coefficient; β = standardized coefficient; Se = standard error; CI = confidence interval; Dependent variable: Organic beliefs. Variables in bold are statistically significant predictors of organic pain beliefs (p < .05).
Multiple linear regression analysis.
p < 0.05.
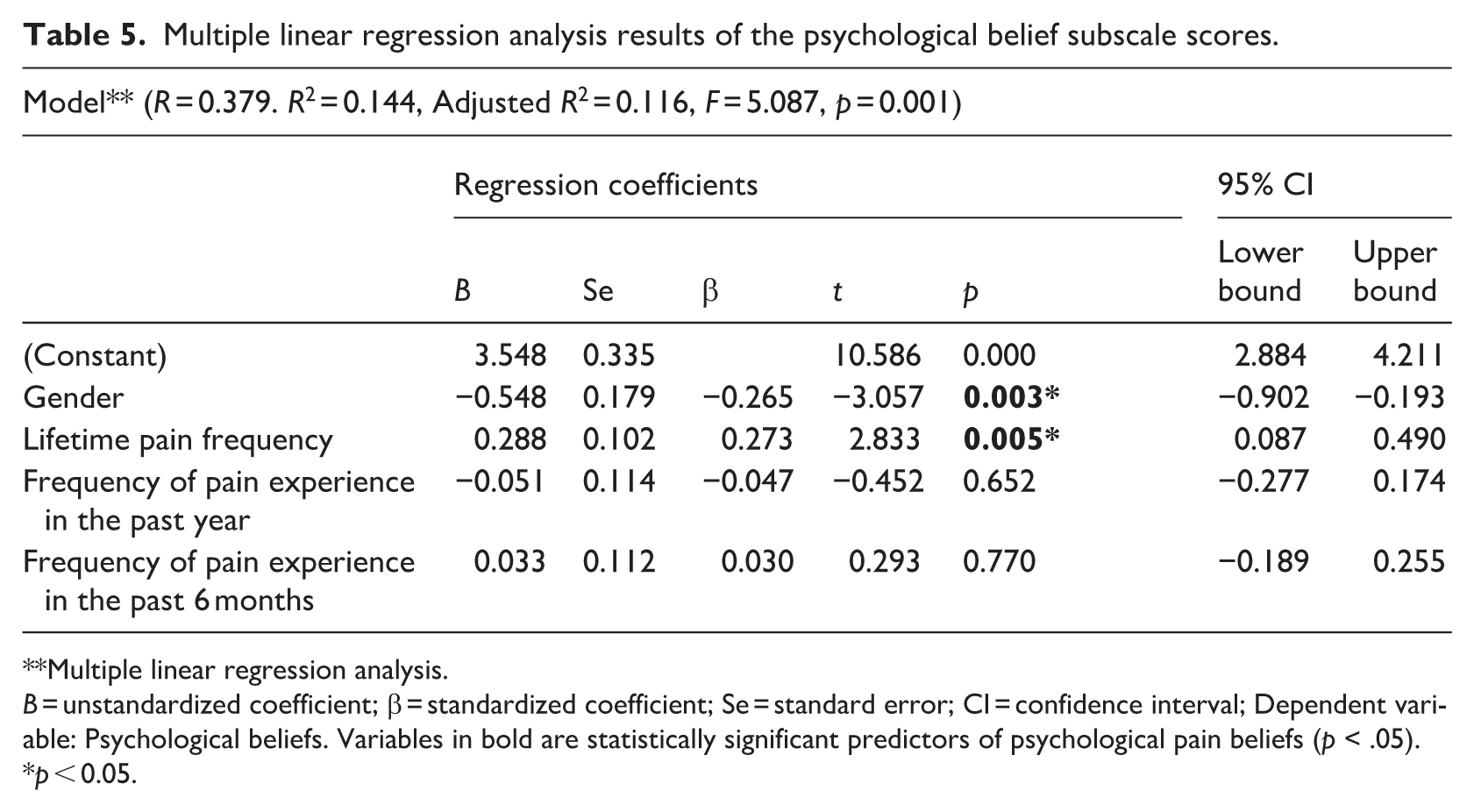
The regression analysis for the psychological beliefs subscale also indicated that the data were consistent with the model, the overall model was significant, and the independent variables (gender, lifetime pain frequency, frequency of pain experience in the past 6 months and year) explained approximately 12% of the variance in the dependent variable (R = 0.379, R2 = 0.144, Adjusted R2 = 0.116, F = 5.087, p = 0.001). A one–standard deviation increase in lifetime pain experience frequency resulted in a 0.273 standard deviation increase in psychological belief scores (p = 0.005). Female gender was also found to significantly predict psychological pain belief scores (p = 0.003; Table 5).
Multiple linear regression analysis results of the psychological belief subscale scores.
Multiple linear regression analysis.
B = unstandardized coefficient; β = standardized coefficient; Se = standard error; CI = confidence interval; Dependent variable: Psychological beliefs. Variables in bold are statistically significant predictors of psychological pain beliefs (p < .05).
p < 0.05.
Discussion
Previous studies have reported that individuals with chronic diseases experience pain more frequently. Chronic diseases that require long-term and complex treatment and care may influence individuals’ attitudes toward pain, their adaptation to pain, and their pain beliefs (Bağci and Doğan, 2022; Ozkan and Cavdar, 2021).
In this study, the sociodemographic, clinical, and pain-specific factors influencing pain-related beliefs in individuals with chronic diseases were comprehensively examined, and important findings were revealed. The results demonstrated that individuals’ perceptions of pain are not solely associated with physiological factors but are also shaped by individual and social variables such as gender, marital status, and pain experience.
In this study, no significant relationship was found between duration of chronic illness and pain beliefs. Additionally, no differences were observed between pain beliefs and either the type of chronic illness or the methods used to cope with pain. The predominance of chronic diseases commonly managed in internal medicine, such as hypertension, diabetes, chronic heart and kidney failure, and chronic pulmonary diseases, within the study sample may have influenced pain belief scores according to diagnosis type. These conditions are among the most prevalent chronic diseases, and individuals with such conditions may experience similar patterns of pain. On the other hand, since the primary diagnoses of patients in surgical clinics were also largely related to these conditions, diagnosis-specific differences in pain beliefs may not have been reflected in the results. Additionally, because the severity of the disease related to the patients’ admission diagnosis was not examined, diagnosis-specific pain beliefs may not have been fully reflected in the results. There were no significant differences in organic and psychological pain belief scores across age groups. Although some studies in the literature report no association between age and pain beliefs (Birge and Mollaoğlu, 2018; Özdemir and Afşar, 2023), other research suggests that increasing age may be associated with higher levels of both organic and psychological pain beliefs (Ulus et al., 2014). Similarly, Kılıç and Alkan (2021) reported that organic pain beliefs increased with age. These findings may be related to the increased frequency and accumulation of pain experiences as individuals grow older. Additionally, because the duration of chronic illness typically increases with age, differences between studies may be attributable to the age distribution and characteristics of the study samples. In the present study, the high proportion of participants aged 60 years and older and the relatively long duration of chronic illness may have contributed to the development of more stable pain beliefs and a greater tendency to accept pain as a result of prolonged pain experiences. When the literature on pain beliefs is examined, several studies report that sociodemographic characteristics such as educational level and income do not influence organic or psychological pain beliefs (Babadağ et al., 2015; Demirci and Özer, 2020; Korkmaz Yaylagül and İmancıoğlu, 2022). However, there are also findings indicating that individuals with basic literacy skills have lower psychological belief scores compared to those with higher levels of education (Birge and Mollaoğlu, 2018). Other studies have reported differences in organic belief scores across educational levels (Özdemir and Afşar, 2023; Özdemir and Tokaç Akdeniz, 2023) and have suggested that individuals with higher educational attainment are more likely to attribute the origin of pain to psychological factors (Sertel Berk, 2006). The variability in findings reported in the literature may be attributed to factors such as sample characteristics, cultural differences, levels of health literacy, and the presence of chronic illnesses. In the present study, the lack of a significant effect of educational level on pain beliefs may be related to the relatively homogeneous distribution of education within the sample, similar health experiences among participants, and the sample size. In the present study, income level was not found to influence pain beliefs, which is consistent with previous research (Birge and Mollaoğlu, 2018; Özdemir and Afşar, 2023). On the other hand, there are also studies indicating that income level may affect psychological (Koçoğlu and Özdemir, 2011) and organic (Özdemir and Tokaç Akdeniz, 2023) belief subscale scores.
The findings of this study showed that women had significantly higher scores than men on the psychological pain beliefs subscale, and that gender was a significant predictor of psychological pain beliefs. Hormonal changes experienced by women can directly influence pain threshold (Nazik and Yılmaz, 2022). These hormonal differences increase women’s biological sensitivity to pain and highlight the psychological dimensions of the pain experience (Bartley and Fillingim, 2013; Nascimento et al., 2020). However, gender differences cannot be explained solely by biological factors. Psychosocial and cultural influences also play an important role in shaping pain beliefs. Women are generally more inclined to express their emotions, more active in seeking social support, and more frequently take on caregiving roles in society (Templeton, 2020). In addition, because women are often closely involved in the pain experiences of family members—such as children, spouses, and parents—their empathetic awareness and pain-related beliefs shaped through observational learning may differ (Şevgin et al., 2023). The findings of the present study are consistent with previous literature indicating that women tend to experience pain more intensely and with greater emotional involvement (Koçoğlu and Özdemir, 2011; Korkmaz Yaylagül and İmancıoğlu, 2022; Şevgin et al., 2023). Similarly, Babadağ et al. (2015) reported higher psychological pain belief scores among female patients. In contrast, some studies have reported higher psychological belief scores among men (Özdemir and Afşar, 2023; Özdemir and Tokaç Akdeniz, 2023), while others have found no significant gender differences (Demirci and Özer, 2020; Sayılan et al., 2025). Such inconsistencies in the literature may be attributable to differences in sample characteristics, living environments, and cultural contexts. Psychological pain beliefs are closely related to emotional states such as anxiety and depression (Babadağ and Alparslan, 2017; Baird and Haslam, 2013). Previous studies have reported that women tend to report higher levels of anxiety and depression than men (Kayrouz et al., 2025; Khan et al., 2025). This may partially explain why women in the present study had higher psychological pain belief scores. In the present study, married individuals were found to have higher scores on the organic pain beliefs subscale compared to single individuals. This finding suggests that pain beliefs are influenced not only by an individual’s own experiences but also by the pain experiences of those around them. Individuals living in nuclear or extended family structures are more frequently exposed to the pain experiences of their spouses, children, or parents. Such exposure may contribute to the development of more organic-oriented pain beliefs (Cano, 2004). The stronger social support systems of married individuals may also enable them to utilize healthcare services more effectively, while simultaneously increasing their attentiveness to pain-related symptoms (Koçoğlu and Özdemir, 2011). Additionally, spouses may influence each other’s health behaviors and exhibit heightened sensitivity to one another’s pain, which can shape pain-related beliefs (Prenevost and Reme, 2017). Although similar findings have been reported in the literature (Ister and Özdemir, 2018), other studies have found that marital status does not significantly affect pain beliefs (Babadağ et al., 2015; Demirci and Özer, 2020; Özdemir and Afşar, 2023). In the present study, no significant difference was found between marital status and psychological pain belief scores; however, psychological belief scores were higher among married participants. This result may be explained by the presence of family-based support systems, including support from spouses and children.
Pain experience and frequency can influence individuals’ pain-related beliefs (Alaca et al., 2020; Kılıçarslan and Erek Kazan, 2021; Rabey et al., 2024). In this study, significant differences were found between pain beliefs and the frequency of pain experienced across the lifespan, within the last year, and within the last 6 months. Individuals who reported experiencing pain “always” throughout their lives had higher organic and psychological pain belief scores compared to those who experienced pain rarely. Similarly, participants who experienced pain in the last 6 months had higher psychological pain belief scores. Regression analysis further revealed that lifetime pain experience significantly predicted organic pain beliefs, whereas continuous pain experienced in the last 6 months significantly predicted psychological pain beliefs. Persistent pain experiences lead not only to physical discomfort but also to emotional and cognitive exhaustion. This may cause individuals to attribute the source of pain primarily to physical factors. Such a belief structure can reduce motivation for treatment and contribute to the perception that pain is uncontrollable or cannot be effectively managed (Bunzli et al., 2015).
Individuals with strong organic pain beliefs tend to assume a direct relationship between the severity of a structural problem in the body and the intensity of the pain experienced (Baird and Haslam, 2013; Kılıçarslan and Erek Kazan, 2021). Pain intensity and the functional impairment associated with it are particularly pronounced in individuals who have a tendency to catastrophize pain. When this tendency is combined with low self-efficacy, psychological distress may become more evident (Jackson et al., 2014; Li et al., 2025). Previous studies have reported that individuals who frequently experience pain—whether in the last 6 months, the last year, or throughout their lifetime—have higher organic and psychological pain belief scores, and that pain experiences influence psychological pain beliefs (Birge and Mollaoğlu, 2018; Demirci and Özer, 2020; Korkmaz Yaylagül and İmancıoğlu, 2022; Özdemir and Afşar, 2023). In a study by Topcu (2018), a negative relationship was found between pain frequency and psychological well-being, and a significant relationship was reported between pain intensity and organic pain beliefs. Furthermore, clinical studies have demonstrated associations between high pain frequency and increased sensitivity, anxiety, depression, and stress levels (Kjøgx et al., 2014). Based on these findings, it may be inferred that lifetime pain frequency mediates the relationship between psychological factors and pain.
The findings of the study showed that individuals’ psychological pain belief scores were higher than their organic pain belief scores. Organic beliefs have been described as increasing individuals’ tendency to attribute pain to external forces such as fate, physicians, or chance, thereby weakening their sense of control. In contrast, psychological beliefs strengthen individuals’ perceived control over their own health and enhance their coping skills (Topcu, 2018). This suggests that chronic pain exerts lasting effects on cognitive processes and leads to the development of stable belief patterns (Babadağ et al., 2015; Demirci and Özer, 2020). Organic beliefs reflect the perception that pain arises primarily from physical damage or bodily dysfunction. Individuals who endorse this perspective are more likely to believe that increased tissue damage results in increased pain intensity. In contrast, psychological beliefs emphasize the role of emotional states—particularly psychological processes such as anxiety and depression—in the onset and persistence of pain (Babadağ and Alparslan, 2017; Baird and Haslam, 2013). All of these findings suggest that persistent perceptions underlying organic beliefs may contribute to the strengthening of psychological beliefs. Consistent with this, previous studies have reported that psychological pain belief scores are higher than organic pain belief scores. (Babadağ et al., 2015; Bağci and Doğan, 2022; Demirci and Özer, 2020; Gülşen et al., 2025; Ister and Özdemir, 2018; Koçoğlu and Özdemir, 2011; Kılıç and Alkan, 2021; Özdemir and Tokaç Akdeniz, 2023; Şevgin et al., 2023; Yildirim et al., 2020), which is consistent with the results of the present study. In a study examining pain beliefs between stroke patients and healthy individuals, it was reported that the stroke group had stronger beliefs related to the psychological dimension (Haslam et al., 2020). In the chronic disease group, pain beliefs appear to be less attributed to organic beliefs, such as tissue injury or other physiology-related conditions. However, there are also studies reporting higher organic belief scores (Birge and Mollaoğlu, 2018; Sayılan et al., 2025).
Although pain is a universally experienced phenomenon, cultural differences may influence pain beliefs, responses to pain, and coping strategies. Culture is shaped by values, beliefs, norms, and practices shared by members of the same cultural group; therefore, individuals who share similar cultural backgrounds may also have similar pain beliefs. However, intercultural differences can affect pain beliefs. For example, while some societies adopt active coping strategies for dealing with pain, others may prefer to endure pain and may even refuse to take medication, attributing different meanings to the pain experience. In addition, individuals may use pain-coping methods that are specific to the traditions of their culture (Cakir, 2019). For instance, a study conducted in Turkish culture reported that women who used traditional methods to cope with pain during menstruation had higher levels of psychological pain beliefs (Işık and Özdemir, 2024). In Turkish society, pain may sometimes be perceived as a condition that should be endured with patience or as a natural part of illness, and individuals may tend to suppress or conceal the expression of pain. However, these tendencies may vary depending on region, socioeconomic status, and educational level. When studies conducted in Türkiye on pain beliefs are examined, it is seen that, in addition to culturally specific traditional coping methods, Western medical approaches are also used (Birge and Mollaoğlu, 2018; Metin and Arslan, 2017; Ordu, 2024; Özdemir and Afşar, 2023). Considering the influence of culture on individuals’ health behaviors and beliefs, these findings appear to be expected in relation to pain beliefs. On the other hand, similar results have also been reported in different cultural contexts (Rajan et al., 2023; Zimmer et al., 2022). Furthermore, it has been reported that determining patients’ pain beliefs and experiences is an important factor in increasing treatment satisfaction and improving pain management (Kose and Sirin, 2023; Wirth et al., 2026). The findings of this study should be interpreted only within the context of individuals with chronic diseases, as all participants had chronic conditions. Accordingly, the study does not aim to demonstrate the effect of chronic illness on pain-related attitudes; rather, it emphasizes how individuals with chronic diseases attribute meaning to their pain and the importance of these attributions. In terms of pain beliefs, these cognitive representations suggest that individuals with chronic diseases may shape their pain perceptions, coping strategies, and psychological adjustment through beliefs related to the nature, identity, and causes of pain developed as a result of their pain experiences. The similarity between the results obtained in the present study and those of other studies conducted in Turkish populations using the same measurement tool suggests that the Turkish adaptation of the scale is valid for the Turkish population.
Limitations
This study was conducted in a single center, which may limit the generalizability of the findings. The use of self-report measures may have led to potential response biases. Additionally, the inclusion of participants with different types of chronic diseases may have introduced clinical heterogeneity; however, this heterogeneity can also be considered a strength, as it allows for a broader understanding of how individuals with diverse chronic conditions interpret and attribute meaning to their pain. Previous studies have shown that pain cognitions are closely associated with psychological factors such as depression and anxiety. However, psychological variables were not assessed in the present study, which may be considered a limitation. Future studies examining pain beliefs in individuals with chronic diseases are recommended to consider the potential role of psychological factors such as depression and to be conducted with larger samples and multicenter designs to validate the findings.
Implications for practitioners and future research
For future research, it is recommended to conduct studies with larger and multi-center samples to enhance the generalizability of the findings. In addition, the cross-sectional design of the present study does not allow for determining the direction or temporal change of the relationship between pain beliefs and pain experience; therefore, longitudinal studies are needed. The finding that women exhibited higher psychological pain beliefs highlights the importance of psychosocial factors, suggesting that future research may incorporate variables such as depression, anxiety, stress, self-efficacy, and social support into analytic models. Moreover, the higher pain belief scores observed among individuals who experience persistent pain underscore the significance of the subjective dimension of the pain experience. Thus, qualitative studies may offer deeper insights into how individuals interpret and make meaning of their pain. While studies on pain beliefs in the literature have mostly focused on specific disease groups, studies that examine individuals with chronic diseases within a broader framework are limited. In this respect, the present study aims to contribute to the evaluation of pain beliefs from a more comprehensive perspective in the context of chronic illness. Finally, conducting experimental intervention studies to examine the effects of cognitive-behavioral training, nursing counseling, and belief-restructuring programs on pain beliefs would provide valuable contributions to future research.
Conclusion
This study found that pain beliefs among individuals with chronic illnesses vary according to demographic characteristics and pain experiences. Women exhibited higher psychological pain beliefs, while married individuals showed stronger organic pain beliefs. Frequent and lifelong pain experiences were associated with higher pain belief scores. Regression analyses confirmed that gender, marital status, and pain frequency significantly influence pain beliefs. These findings highlight the importance of considering pain beliefs in clinical assessments and tailoring pain management within a biopsychosocial framework.
Footnotes
Ethical considerations
Ethics committee and institutional permissions were obtained from the Bezmialem Vakif University Non-Interventional Research Ethics Committee (Date: 27.02.2025/Subject: 64) and the Bezmialem Vakif University Health Practice and Research Center (Date: 09.01.2025/Number: 178346). Permission to use the Pain Beliefs Scale, which was used to collect the research data, was obtained from the author. Written and verbal informed consent forms were obtained from the patients who agreed to participate in the study. The principles of the Declaration of Helsinki were adhered to throughout the study.
Consent to participate
All participants were informed about the purpose of the study, and written and verbal consent was obtained.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Author contributions
Study design: BD, ML, BT, DM, DÖ; Data collection: ML, BT, DM, DÖ; Data analysing: BD, ML; Conceptualization: BD, ML, BT; Writing back-ground & discussion sections: BD, ML, BT, DM, DÖ; Writing method & results sections; BD, ML, DM; Reviewing: BD, ML, BT, DM; Supervision: BD. All authors approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.