
Abstract
Postpartum depression (PPD) affects both parents, yet its association with multiple screen addiction (MSA) remains under-researched, particularly within family systems. To address this gap using a couple-based perspective, this study evaluated the relationship between PPD and MSA in 83 mother–father dyads recruited from a primary care setting in Türkiye. Participants completed the Edinburgh Postnatal Depression Scale and the Multiple Screen Addiction Scale (MSAS). Results indicated that mothers had higher PPD scores, while fathers exhibited higher MSA levels. Significant positive correlations were observed between PPD and MSA within individuals, and scores were also significantly correlated between partners. Multivariable linear regression analyses identified significant individual and inter-partner associations between depressive symptoms and screen addiction in both parents. These findings suggest that postpartum mental health and screen use behaviors may be interconnected within couples, highlighting the importance of evaluating both parents together to better understand inter-partner dynamics during the postpartum period.
Keywords
Introduction
Postpartum depression (PPD), typically defined as a major depressive episode occurring during the postpartum period, is a common and clinically significant mental health condition affecting individuals during the postpartum period, with well-documented consequences for maternal well-being, infant development, and family functioning (O'Hara and McCabe, 2013; Slomian et al., 2019; Stein et al., 2014). Maternal PPD has been associated with impaired mother–infant bonding, adverse cognitive and emotional development in children, and increased family stress. While the prevalence of PPD among mothers is estimated to be around 15% in high-income settings, prevalence estimates vary depending on assessment methods and populations (O'Hara and McCabe, 2013; Shorey et al., 2018). Emerging evidence also indicates that fathers may experience depressive symptoms during the perinatal period, with meta-analytic estimates suggesting paternal PPD rates of approximately 8%–10% (Cameron et al., 2016; Paulson and Bazemore, 2010). Importantly, postpartum mental health is increasingly conceptualized as a relational and family-level phenomenon rather than an isolated individual experience (Cameron et al., 2016; Goodman, 2004).
Recent research has emphasized the interdependent nature of parental mental health, demonstrating that depressive symptoms in one partner are associated with emotional and behavioral outcomes in the other (Goodman, 2004; Paulson and Bazemore, 2010). Dyadic and longitudinal studies have shown bidirectional associations between maternal and paternal depressive symptoms during the postpartum period (Cameron et al., 2016; Don and Mickelson, 2012). This interdependence may be explained by shared environmental stressors such as sleep disruption, financial strain, and increased childcare demands (Don and Mickelson, 2012). In addition, mechanisms such as emotional contagion and mutual emotional regulation within close relationships may contribute to cross-partner effects (Goodman, 2004; Hatfield et al., 1993). Despite this growing evidence, many studies continue to focus on mothers alone, potentially overlooking dyadic processes influencing postpartum adaptation.
In parallel, digital behaviors—particularly excessive use of screen-based devices—have emerged as an important public health concern (Elhai et al., 2017). Problematic engagement with smartphones, social media, and other digital platforms has been associated with sleep disturbances, reduced physical activity, and psychological distress (Alonzo et al., 2021; Elhai et al., 2017; Thomée, 2018). Several studies have demonstrated associations between problematic internet or smartphone use and depressive symptoms (Elhai et al., 2017). These relationships appear to be bidirectional, with depressive symptoms potentially increasing problematic screen use and excessive screen use contributing to mood disturbances (Alonzo et al., 2021; Elhai et al., 2017). However, most studies examining these associations have focused on individuals rather than couples or family systems (Thomée, 2018).
The postpartum period may represent a particularly vulnerable window for the interaction between mental health and digital behaviors. New parents experience substantial role transitions, increased caregiving demands, and changes in daily routines that may influence both emotional well-being and technology use (McDaniel and Coyne, 2016; Radesky et al., 2016). Individuals experiencing depressive symptoms may turn to digital media as a coping mechanism or for social support. Conversely, excessive screen use may exacerbate depressive symptoms through sleep disruption, reduced interpersonal interaction, and decreased social engagement (Alonzo et al., 2021; Elhai et al., 2017). However, the extent to which these associations operate within couples—and whether partners’ behaviors and mental states are interconnected—remains largely unexplored (Radesky et al., 2016; Thomée, 2018).
In addition to psychological and behavioral factors, several sociodemographic and parental–infant characteristics may influence postpartum mental health and screen use. Factors such as employment status, parity, pregnancy complications, and caregiving burden have been associated with PPD symptoms in previous research (Norhayati et al., 2015; Yim et al., 2015). Lifestyle factors such as alcohol use, sleep patterns, and family childcare dynamics may also influence both psychological well-being and technology use (Elhai et al., 2017; McDaniel and Coyne, 2016). Despite their potential importance, these variables are often inconsistently incorporated into dyadic analyses (Cameron et al., 2016; Don and Mickelson, 2012)
To address these gaps, the present study adopts a couple-based perspective to examine the associations between PPD symptoms and multiple screen addiction (MSA) in mothers and fathers simultaneously. By evaluating both within-individual (actor) and between-partner (partner) associations, this study aims to provide a more comprehensive understanding of how mental health and digital behaviors co-occur within families during the early postpartum period.
We hypothesized that: (1) PPD symptoms would be positively associated with MSA within individuals; (2) depressive symptoms and screen addiction would show significant inter-partner associations within couples; and (3) selected sociodemographic and parental–infant factors would be associated with both depressive symptoms and screen addiction outcomes.
Methods
Study design and setting
This study was designed as a single-center, community-based, cross-sectional study conducted between July and December 2024 in a family health center located in Trabzon, Türkiye. The center serves an approximately 18,000-person registered population and provides routine maternal, postpartum, and infant follow-up services within a primary care framework. In this setting, families are regularly invited for scheduled postpartum and infant monitoring visits, which provided an appropriate context for recruiting mother–father dyads.
The study was approved by the Scientific Research Ethics Committee of the University of Health Sciences Trabzon Faculty of Medicine (approval date: 13.08.2024; decision no: 2024/110). Written informed consent was obtained from all participants prior to data collection. The study was conducted in accordance with the Declaration of Helsinki and reported in line with the STROBE guidelines (von Elm et al., 2008).
Participants and recruitment
The study population consisted of mother–father dyads who presented to the family health center for routine infant follow-up visits during the first 6 months postpartum. Eligible participants were consecutively recruited during the study period.
Inclusion criteria were: (1) both parents attending the visit together, (2) both aged 18 years or older, and (3) cohabiting in the same household. Exclusion criteria included the presence of cognitive impairment, severe psychiatric disorder, or communication difficulties that could interfere with questionnaire completion.
A priori sample size calculation was not performed. Instead, all eligible dyads presenting during the predefined study period were included. This approach was chosen due to the exploratory nature of the study and the practical constraints of recruiting complete dyads within a primary care setting. The study period was determined based on feasibility considerations, including patient flow and time-limited access to the study setting.
Measures
Data were collected using a structured questionnaire administered separately to mothers and fathers through face-to-face interviews.
Sociodemographic and parental–infant variables included age, education level, employment status, number of children, duration of marriage, smoking and alcohol use, presence of chronic disease, and family history of depression. In addition, pregnancy- and caregiving-related variables were recorded, including whether the pregnancy was planned, presence of trauma or medical complications during pregnancy, primary caregiver status, and perceived difficulty in infant care. These variables were selected based on previous literature suggesting their potential association with postpartum mental health and behavioral outcomes.
PPD symptoms were assessed using the Edinburgh Postnatal Depression Scale (EPDS), a widely used screening instrument consisting of 10 items scored on a 4-point Likert scale (0–3), with total scores ranging from 0 to 30 (Cox et al., 1987). The validated Turkish version of the EPDS was used (Engindeniz et al., 1996). In this study, Cronbach’s alpha coefficients were 0.795 for mothers and 0.786 for fathers.
MSA was assessed using the Multiple Screen Addiction Scale (MSAS), which evaluates problematic use of various screen-based technologies (Sarıtepeci, 2021). The scale includes 15 items rated on a 5-point Likert scale. Both monothetic and polythetic criteria were considered in defining screen addiction. In this study, Cronbach’s alpha coefficients were 0.885 for mothers and 0.901 for fathers.
Statistical analysis
All statistical analyses were performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were presented as median [interquartile range] for continuous variables and as frequencies (percentages) for categorical variables. Normality of distributions was assessed using skewness and kurtosis values.
Comparisons between mothers and fathers were conducted using the Wilcoxon signed-rank test for continuous variables and the McNemar test for categorical variables, accounting for paired data structure. Between-group comparisons for independent variables were performed using the independent samples t-test or Mann–Whitney U test, as appropriate.
Spearman correlation analysis was used to examine associations between EPDS and MSAS scores within individuals and between partners.
To evaluate independent associations, separate linear regression models were constructed for maternal and paternal EPDS and MSAS scores. Variables that showed significant associations in univariate analyses were included in the multivariable models using a stepwise approach.
Given the dyadic nature of the data, partner variables (e.g. paternal EPDS and MSAS scores in maternal models and vice versa) were included in the regression models to partially account for interdependence between partners. However, formal dyadic analytical approaches such as the Actor–Partner Interdependence Model (APIM) were not applied. Therefore, the present findings should be interpreted as exploratory inter-partner associations rather than fully modeled dyadic effects.
Square root transformation was applied to EPDS and MSAS scores to improve normality of residuals. Statistical significance was set at p < 0.05. Given the number of comparisons performed, results were interpreted with caution, particularly for secondary analyses.
Use of Artificial Intelligence
Artificial intelligence-based tools were used for language editing and stylistic refinement of the manuscript. The AI tool (ChatGPT, OpenAI) was used to improve clarity, grammar, and academic tone of the text written by the authors. No AI tools were used in study design, data collection, statistical analysis, data interpretation, or figure generation. All analyses and interpretations were conducted by the authors, who take full responsibility for the content of the manuscript.
Results
Sample characteristics
The study included 83 mother–father dyads (n = 166 individuals). The median age was 29 years [IQR: 7] for mothers and 32 years [IQR: 8] for fathers (p < 0.001). Fathers were more likely to be employed, smoke, and consume alcohol, whereas mothers more frequently reported pregnancy-related trauma, medical complications, and difficulties in infant care. Detailed comparisons of parental characteristics are presented in Table 1.
Comparison of descriptive characteristics of mothers and fathers.
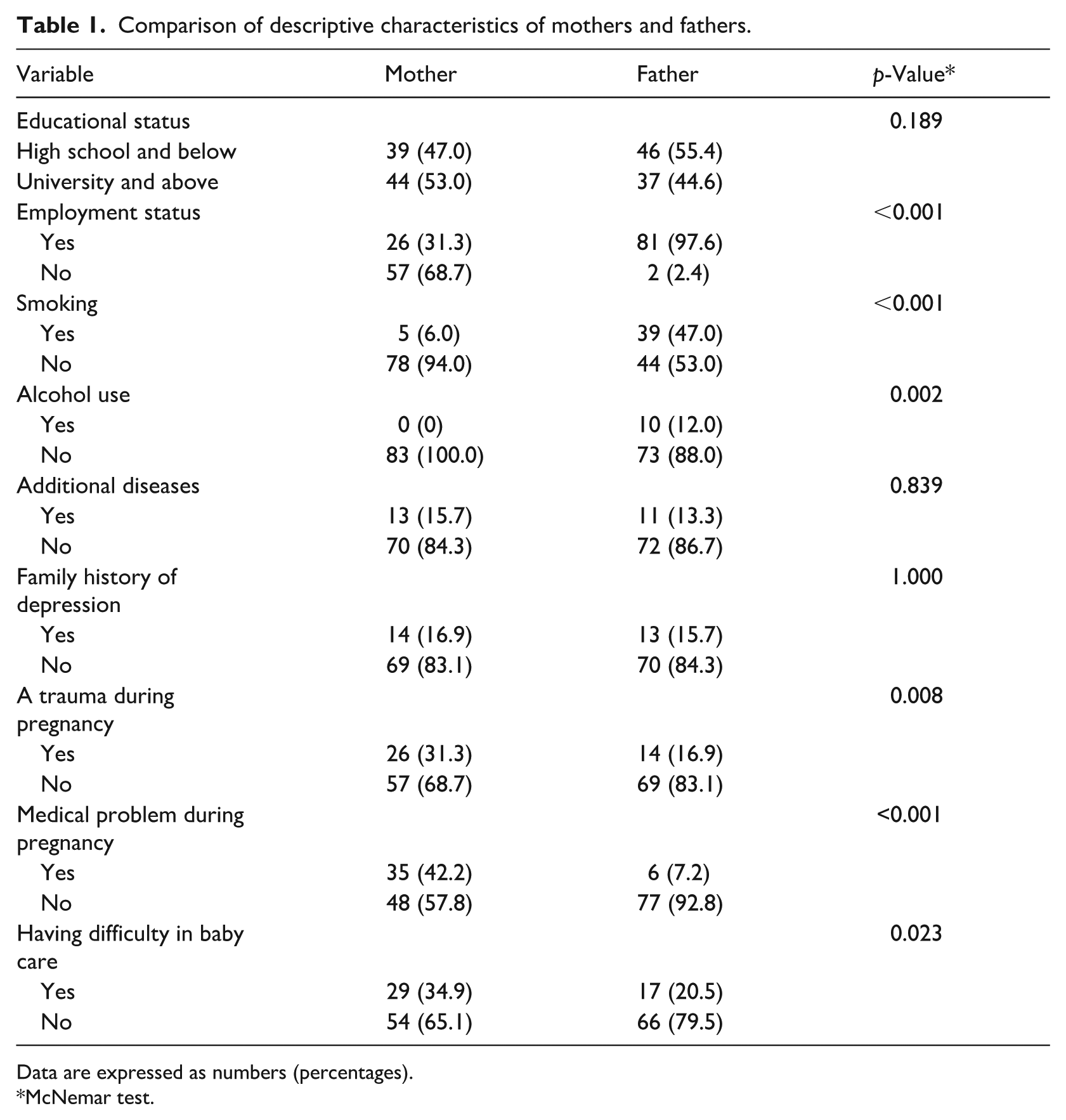
Data are expressed as numbers (percentages).
McNemar test.
Regarding shared couple-level characteristics, most couples were within the first 5 years of marriage (61.4%). The median number of children was 1 [IQR: 1], and the median infant age was 2 months [IQR: 3]. The majority of pregnancies were planned (72.3%), and in most cases, the mother was identified as the primary caregiver (66.3%).
EPDS and MSAS findings
The overall median EPDS score was 4 [IQR: 5], with 16.3% of participants scoring ⩾ 10, indicating at least mild depressive symptoms. Mothers had significantly higher EPDS scores and a higher prevalence of depressive symptoms compared to fathers.
For MSA, 18.7% of participants met the polythetic criteria for MSA. Although the prevalence of MSA did not differ significantly between mothers and fathers, fathers had higher median MSAS scores.
Detailed comparisons of EPDS and MSAS outcomes between mothers and fathers are presented in Table 2.
Comparison of EPDS and MSAS findings of mothers and fathers.
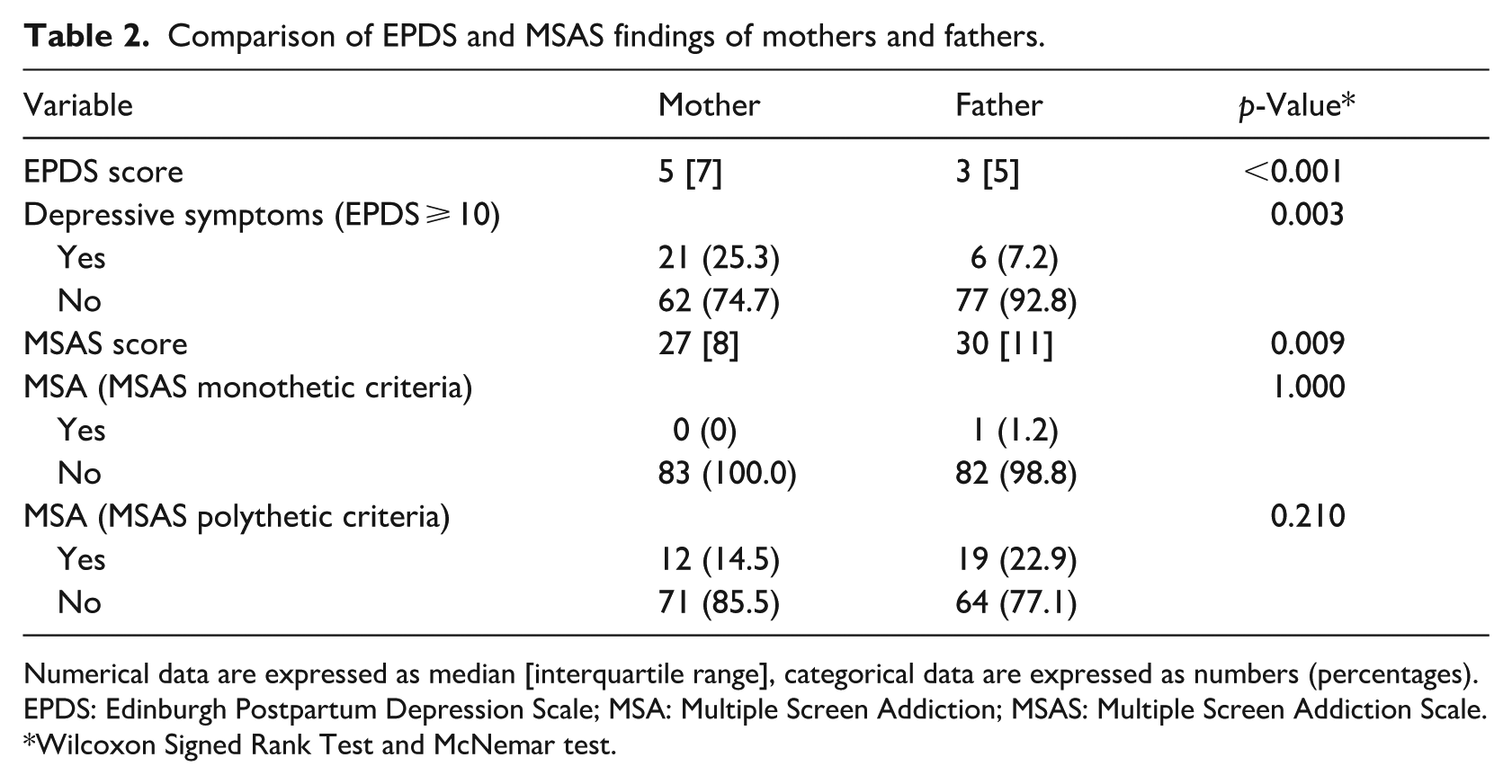
Numerical data are expressed as median [interquartile range], categorical data are expressed as numbers (percentages).
EPDS: Edinburgh Postpartum Depression Scale; MSA: Multiple Screen Addiction; MSAS: Multiple Screen Addiction Scale.
Wilcoxon Signed Rank Test and McNemar test.
Within-individual and between-partner associations
Correlation analyses were conducted to examine both within-individual (actor-level) and between-partner (partner-level) associations between depressive symptoms and screen addiction.
Within individuals, higher EPDS scores were positively correlated with higher MSAS scores in both mothers (r = 0.270, p = 0.014) and fathers (r = 0.262, p = 0.017). Between partners, significant positive correlations were observed for both EPDS scores (r = 0.333, p = 0.002) and MSAS scores (r = 0.352, p = 0.001). However, cross-domain associations (e.g. paternal EPDS with maternal MSAS) were not statistically significant.
Multivariable regression analyses
Multivariable linear regression analyses were conducted to identify independent factors associated with EPDS and MSAS scores in mothers and fathers, while accounting for both individual and partner-level variables.
For maternal depressive symptoms, higher EPDS scores were significantly associated with maternal employment, pregnancy-related medical complications, difficulty in infant care, shared caregiving, higher paternal EPDS scores, and higher maternal MSAS scores. For paternal depressive symptoms, higher EPDS scores were associated with trauma exposure and medical complications during pregnancy, as well as higher maternal EPDS scores (Table 3).
Linear regression results for EPDS scores.
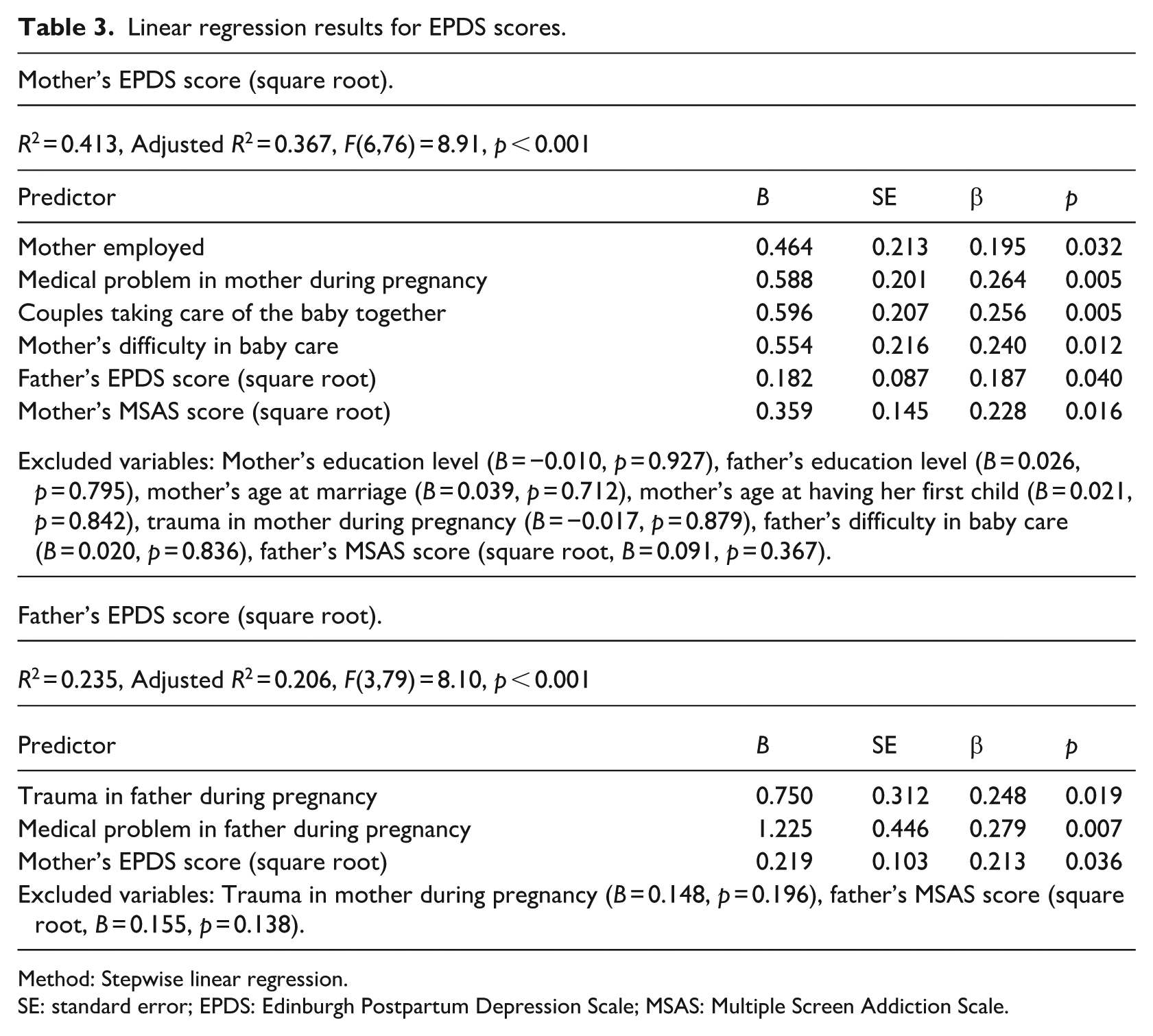
Method: Stepwise linear regression.
SE: standard error; EPDS: Edinburgh Postpartum Depression Scale; MSAS: Multiple Screen Addiction Scale.
In terms of screen addiction, higher maternal MSAS scores were associated with fewer children, higher maternal EPDS scores, and higher paternal MSAS scores. Similarly, higher paternal MSAS scores were associated with alcohol consumption, higher paternal EPDS scores, and higher maternal MSAS scores (Table 4).
Linear regression results for MSAS scores.
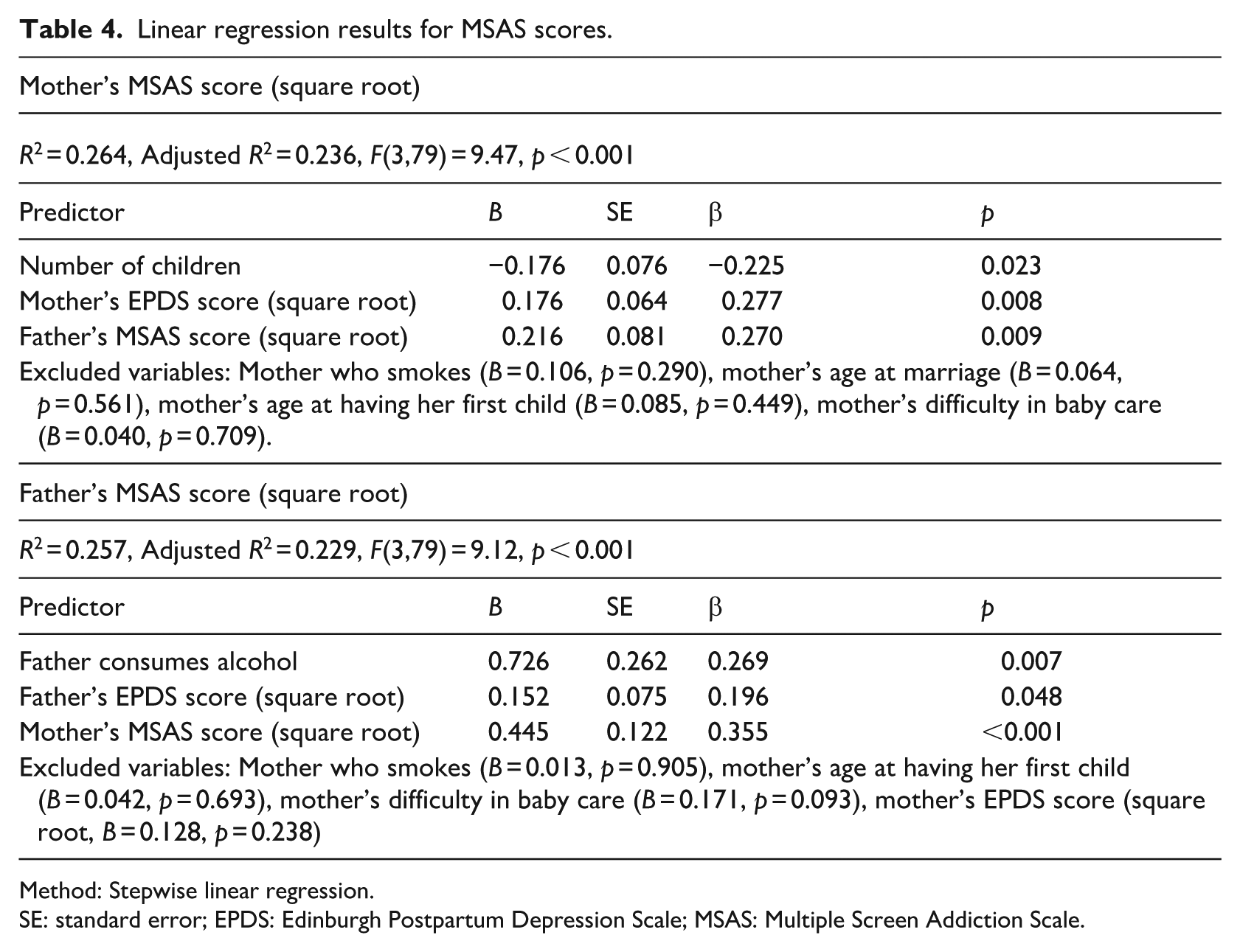
Method: Stepwise linear regression.
SE: standard error; EPDS: Edinburgh Postpartum Depression Scale; MSAS: Multiple Screen Addiction Scale.
Discussion
Our study identified a significant association between PPD symptoms and MSA in both mothers and fathers. These findings are consistent with previous studies showing a strong link between social media, internet, and gaming addiction and depression (Andreassen et al., 2016; Lin et al., 2016). Some studies suggest that individuals with higher levels of depressive symptoms may turn to digital platforms to cope with emotions and escape reality (Kircaburun et al., 2019). On the other hand, meta-analyses have reported that individuals with problematic smartphone or internet use are more likely to experience depression, potentially due to increased social isolation, disrupted sleep, and lack of interpersonal support (Li et al., 2020; Lozano-Blasco et al., 2022). Given the cross-sectional nature of the study, these findings should be interpreted as associations rather than causal relationships.
Several mechanisms may explain the observed association between MSA and PPD symptoms. The postpartum period introduces a new parental identity in addition to traditional individual and spousal roles and imposes significant responsibilities (Fowles, 1998). The psychosocial stress associated with this role transition is known to be an important trigger of PPD symptoms. According to Folkman and Lazarus (1985), avoidance behavior is one mechanism used to cope with stress, and screens may provide an easily accessible and low-cost form of distraction (Hasan and Jaber, 2019). Mothers may also use screens for informational purposes during infant care, which, when excessive, may contribute to health anxiety or cyberchondria. Additionally, prolonged screen exposure has been shown to impair sleep quality through delayed bedtimes, musculoskeletal discomfort, and disrupted melatonin secretion due to blue light exposure (Brautsch et al., 2023; Chinoy et al., 2018). Sleep disturbances, in turn, are known to exacerbate mood disorders, including depression. Furthermore, reduced face-to-face communication and weakened social support associated with excessive screen use may also contribute to depressive symptoms (Al-Kandari and Al-Sejari, 2021; Tateno et al., 2019).
Another key finding of this study was the association between PPD symptoms in mothers and fathers. This finding suggests that depressive symptoms may cluster within couples during the postpartum period. Shared stressors such as poor infant sleep, financial strain, and relationship dissatisfaction may contribute to this pattern (Atif et al., 2022; Goodman, 2004; Johansson et al., 2020; Thiel et al., 2020). Additionally, emotional contagion—where individuals unconsciously mimic and internalize their partner’s emotions—may help explain the observed inter-partner association (Ierardi et al., 2019; Prochazkova and Kret, 2017). However, given the cross-sectional design, the directionality of this association cannot be determined.
We also observed a correlation between screen addiction levels in partners. Research specifically addressing screen addiction within couples is limited; however, behavioral addictions share similarities with substance-related addictions, where exposure to addictive behaviors within close environments has been identified as a risk factor (Grant et al., 2010; Haller et al., 2010). Several theoretical frameworks may help explain this pattern. Social Learning Theory suggests that individuals model behaviors observed in close relationships (Bandura and Walters, 1977), while Social Network Theory emphasizes how behaviors spread through interpersonal connections (Liu et al., 2017). Additionally, Attachment Theory and Compensatory Internet Use Theory propose that individuals experiencing emotional distress or unmet attachment needs—such as during the postpartum period—may turn to digital platforms as coping mechanisms (Ainsworth et al., 2015; Kardefelt-Winther, 2014). These frameworks support the possibility that screen use behaviors may develop within shared relational contexts.
Our study found that working mothers had higher PPD symptom scores, which may reflect the challenges of balancing employment and childcare responsibilities, consistent with previous findings (Goker et al., 2012; Vaezi et al., 2019). Maternal medical complications during pregnancy were also associated with higher depressive symptoms, in line with prior research highlighting the psychological burden of pregnancy-related health problems (Durukan et al., 2011).
Interestingly, mothers who reported shared childcare responsibilities also demonstrated higher depressive symptom scores. One possible explanation is reverse directionality, whereby fathers may become more involved in infant care in response to maternal distress or increased caregiving burden. However, cultural and family-role dynamics may also contribute to this association. In more traditional family contexts, including some Turkish family structures, mothers are often expected to assume primary responsibility for infant care, while paternal involvement may still be perceived as “assistance” rather than shared responsibility (Erdem et al., 2021; Zhang et al., 2023). In such contexts, increased paternal involvement may not always be experienced solely as supportive and could, in some families, contribute to role ambiguity, perceived inadequacy, or stress related to shifting caregiving expectations. Therefore, this finding likely reflects a complex interaction between caregiving burden, family dynamics, and sociocultural expectations rather than a straightforward protective or harmful effect.
Furthermore, mothers who reported difficulties in infant care had higher depressive symptom scores, consistent with previous studies identifying childcare-related stress as an important contributor to PPD symptoms (Cutrona, 1984; Leung et al., 2005; Roomruangwong et al., 2016). These findings suggest that caregiving burden and perceived parenting difficulties may be associated with maternal psychological well-being during the postpartum period.
In our study, fathers who experienced health problems or trauma during pregnancy had higher depressive symptom scores. This finding is consistent with previous research indicating that stressors experienced during pregnancy or the early postpartum period may increase paternal depressive symptoms (Kothari et al., 2022). Potential explanations include exposure to traumatic events, increased perceived responsibility, and limited help-seeking behaviors influenced by traditional gender roles. Additionally, reduced social support during this transitional period may further contribute to paternal psychological distress.
In our study, an inverse association was observed between the number of children and maternal MSA. As the number of children increases, caregiving responsibilities may expand, potentially reducing the time available for screen use. This interpretation is consistent with the idea that increased parenting demands may be associated with reduced engagement in digital activities. However, alternative explanations, such as differences in parental experience or family structure, cannot be excluded.
Additionally, alcohol consumption in fathers was associated with higher levels of MSA. Previous studies have also reported associations between alcohol use and problematic internet use, suggesting that these behaviors may co-occur within broader patterns of reward-seeking or coping-related behaviors (Jain et al., 2020; Yen et al., 2009). These findings may indicate that certain lifestyle behaviors cluster together during the postpartum period.
Strengths
This study addresses an important gap in the literature by examining the relationship between PPD symptoms and MSA using a couple-based approach. Simultaneous evaluation of mothers and fathers allowed the assessment of inter-partner associations, providing a more comprehensive understanding of family dynamics during the postpartum period.
Furthermore, conducting the study in a primary health care setting may enhance the representativeness of the sample compared to hospital-based populations, where more severe cases are often overrepresented. The inclusion of both psychological and behavioral variables also enabled a broader examination of postpartum well-being within a real-world primary care context.
Limitations
Several limitations should be considered when interpreting the findings of this study. First, the cross-sectional design precludes conclusions regarding causality or directionality between PPD symptoms and MSA. Longitudinal studies are needed to better understand temporal relationships between these variables.
Second, the study was conducted in a single primary care center, which may limit generalizability to other populations and cultural contexts. Although primary care settings may improve representativeness, multi-center studies would provide more robust external validity.
Third, data were collected using self-report instruments, which may be subject to recall bias and social desirability bias. In addition, the EPDS is a screening tool rather than a diagnostic instrument and therefore does not establish clinical diagnoses of depression.
Fourth, although partner variables were included in regression models to partially account for interdependence between mothers and fathers, formal dyadic analytical approaches such as the Actor–Partner Interdependence Model were not applied. Future studies using formal dyadic analytical frameworks such as APIM may provide more comprehensive insights into actor and partner effects within couples.
Fifth, although all eligible mother–father dyads during the study period were included, the relatively modest sample size may have limited the precision and stability of multivariable regression estimates, particularly given the number of predictors included in the models.
Finally, given the number of comparisons performed, some findings—particularly secondary analyses—should be interpreted cautiously. Larger studies may help confirm the robustness of these associations.
Conclusions
This study identified significant associations between PPD symptoms and MSA in mothers and fathers attending primary care follow-up during the first 6 months postpartum. These findings suggest that postpartum mental health and digital behaviors may be interconnected within couples.
Maternal depressive symptoms were associated with employment status, pregnancy-related medical complications, difficulty in infant care, and shared caregiving responsibilities. In fathers, depressive symptoms were associated with trauma and medical complications during pregnancy. Additionally, fewer children were associated with higher screen addiction levels in mothers, while alcohol consumption was associated with higher screen addiction levels in fathers.
These findings suggest that evaluating both mothers and fathers may help improve postpartum mental health assessment. Incorporating assessment of screen use behaviors into postpartum follow-up may help inform future primary care screening approaches. Future longitudinal and multi-center studies are needed to further clarify these associations and explore potential mechanisms underlying these relationships.
Footnotes
Ethical considerations
The study was approved by the Scientific Research Ethics Committee of the University of Health Sciences Trabzon Faculty of Medicine (approval date: 13.08.2024; decision no: 2024/110).
Consent to participate
Written informed consent was obtained from all participants prior to data collection.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and analyzed during the current study are not publicly available due to privacy and ethical restrictions but are available from the corresponding author on reasonable request.