
Abstract
This study examined Fear of Progression (FoP) trajectories among first-stroke patients from onset to 6 months post-stroke and identified predictors for different subtypes. A total of 314 eligible patients were recruited via convenience sampling, with FoP assessed at 1, 3, and 6 months post-stroke. Latent class growth models (LCGM) were employed to identify FoP trajectories patterns, and univariate and multivariate logistic regression analyses were conducted to explore associated factors. Three distinct patterns of FoP emerged among first-stroke patients, significantly associated with multiple factors including age, employment status, monthly income, health insurance coverage, Modified Rankin Scale (MRS), National Institutes of Health Stroke Scale (NIHSS), Brief Illness Perception Questionnaire (BIPQ), Perceived Social Support Scale (PSSS), dimensions of the Coping Style Questionnaire (confrontation, avoidance, acquiescence), and Post-Traumatic Stress Disorder (PTSD). This study contributes to understanding the heterogeneity of FoP patterns in this population, providing a theoretical basis for interventions aimed at alleviating their fear.
Keywords
Introduction
Stroke is defined as a syndrome characterized by acute neurological dysfunction caused by sudden disruption of cerebral blood circulation (Hilkens et al., 2024). With increasing incidence and mortality, heavy disability burden, high recurrence risk, and considerable socioeconomic costs, stroke represents a major global public health challenge (Sun et al., 2023).
Fear of Progression (FoP) refers to disease-specific apprehension related to potential biological, psychological, and social consequences, as well as fear of disease worsening or recurrence. Unlike general anxiety or depression, FoP is a targeted emotional response triggered by actual health threats (Dankert et al., 2003). Stroke is associated with a high risk of recurrence, with the likelihood of recurrence increasing over time. A systematic review (Lin et al., 2021) reported that the recurrence rates at 3 months, 6 months, and 1 year after stroke were 7.7%, 9.5%, and 10.4%, respectively. The progressive decline in partial or complete loss of self-care ability may also provoke a strong fear of disease recurrence among patients (Liu et al., 2024). Della Vecchia et al. (2019) conducted qualitative interviews with 24 stroke patients, revealing that this population commonly experiences cognitive distress due to the uncertainty surrounding disease recurrence and the unpredictable progression of the condition. This perceived loss of control over health management and the unknown trajectory of the disease can lead to psychological stress responses, which are often manifested as persistent anxiety and FoP.
According to the Psychological Stress and Coping Theory, stress reflects a dynamic cognitive–environmental interaction rather than a simple linear process (Folkman et al., 1986). Stress mediates the relationship between stressors and stress responses. After exposure to stressors, psychological stress reactions arise through interactions among cognitive appraisal, coping strategies, social support, personal experiences, and emotional status. Such stress responses reflect a dynamic imbalance in a multifactorial system and may impair patients’ physical and mental health (Wang et al., 2024). The onset of stroke introduces a continuous endogenous threat to patients. Prolonged psychological distress and/or inadequate social support may heighten patients’ perception of disease-related risks (Yang et al., 2025). If individuals employ maladaptive coping strategies in response to such conditions, it may further contribute to the development and progression of FoP. Post-traumatic stress disorder (PTSD) refers to a condition in which, following exposure to a threatening or severely traumatic event, intrusive thoughts prevent an individual from processing the trauma caused by the event. This manifests as recurring flashbacks of the traumatic event, efforts to avoid reminders of the event, and a state of heightened physiological arousal (Ryder et al., 2026). Building upon this theoretical framework, the present study incorporated sociodemographic and clinical characteristics, illness perception, social support, coping styles, and PTSD as potential predictors of changes in symptom trajectories over time.
FoP is not a static construct but rather demonstrates dynamic fluctuations over time. A meta-analysis study (Luigjes-Huizer et al., 2022) indicated that among 11,226 cancer patients and survivors, there was considerable heterogeneity in both the levels and incidence of fear of recurrence across different cancer types. Specifically, 59% of patients reported moderate or higher levels of FoP, while 19% experienced high levels, indicating a need for targeted interventions. Disease trajectories exhibit both individual and group-level variability. Latent class growth models (LCGM) accounts for temporal heterogeneity by identifying distinct developmental trajectories, and it has been widely applied in studies examining health trajectories across various populations (Herle et al., 2020). Currently, research on FoP among stroke patients remains limited, with most existing studies employing cross-sectional designs (Lei et al., 2025; Ning et al., 2025; Wang et al., 2024) and lacking longitudinal follow-up data. Therefore, this study applied LCGM to identify distinct trajectories of FoP and their associated factors among first-episode stroke patients. The goal was to clarify heterogeneity in the development of FoP and inform targeted clinical interventions.
Methods
Design and participants
A prospective cohort study was conducted at a tertiary hospital in Nantong City, Jiangsu Province. Participants were recruited using a convenience sampling method. This study was approved by the Research Ethics Committee of Nantong University Affiliated Hospital in June 2024, with approval number 2024-K051-01.
A baseline questionnaire was administered by the research team when the patients’ medical conditions had stabilized following their initial admission. Follow-up assessments were conducted via telephone interviews or outpatient visits at 1 month (T2), 3 months (T3), and 6 months (T4) post-discharge. Inclusion criteria were as follows: (1) patients met the diagnostic criteria outlined in the clinical guidelines of the Chinese Stroke Association and were confirmed by head CT or MRI; (2) age ⩾18 years; (3) first-ever stroke episode, having passed the acute phase with stable vital signs; (4) clear consciousness, normal cognitive function, and intact language expression ability; and (5) voluntary participation with signed informed consent; (6) patients with mild to moderate stroke with National Institutes of Health Stroke Scale (NIHSS) ⩽13. We excluded patients who had experienced other major medical conditions within the past 3 months, such as severe hepatic or renal insufficiency, severe arrhythmia, frequent angina pectoris, severe heart failure, myocardial infarction, or those who were unable to cooperate due to severe psychological trauma or significant disability.
Data collection procedure
The study was conducted from August 2023 to January 2025. Data collection was carried out by trained members of the research team, who administered paper questionnaires in a one-on-one setting or followed up via telephone. Standardized instructions were provided to explain the content of the questionnaire. For participants who encountered difficulties in reading or completing the questionnaire, researchers assisted by explaining each item and recording responses individually to ensure data accuracy. To facilitate the follow-up process, two contact methods were obtained from each participant during baseline data collection, and proactive contact was initiated 7 days prior to each scheduled follow-up. The data collection methods and timelines were adapted based on individual participant needs. The telephone follow-up only records relevant research data and does not record sensitive personal information. After all the data are entered, the names, phone numbers and identity identifiers are immediately deleted, and only the research numbers are retained. The sample size was calculated using G*Power 3.1 software, guided by the reference table for sample size estimation for single-group repeated measures. Based on an average intra-class correlation coefficient (ρ) of 0.05, an effect size (f) of 0.14, a significance level (α) of 0.05, and a desired statistical power (1−β) of 0.80, the minimum required sample size was determined to be 142 participants. Accounting for a projected attrition rate of 20%, the final target sample size was set at 170 participants. A total of 353 questionnaires were distributed, and 314 participants completed the follow-up process, resulting in an effective questionnaire recovery rate of 88.95%.
Measurements
Sociodemographic and clinical characteristics
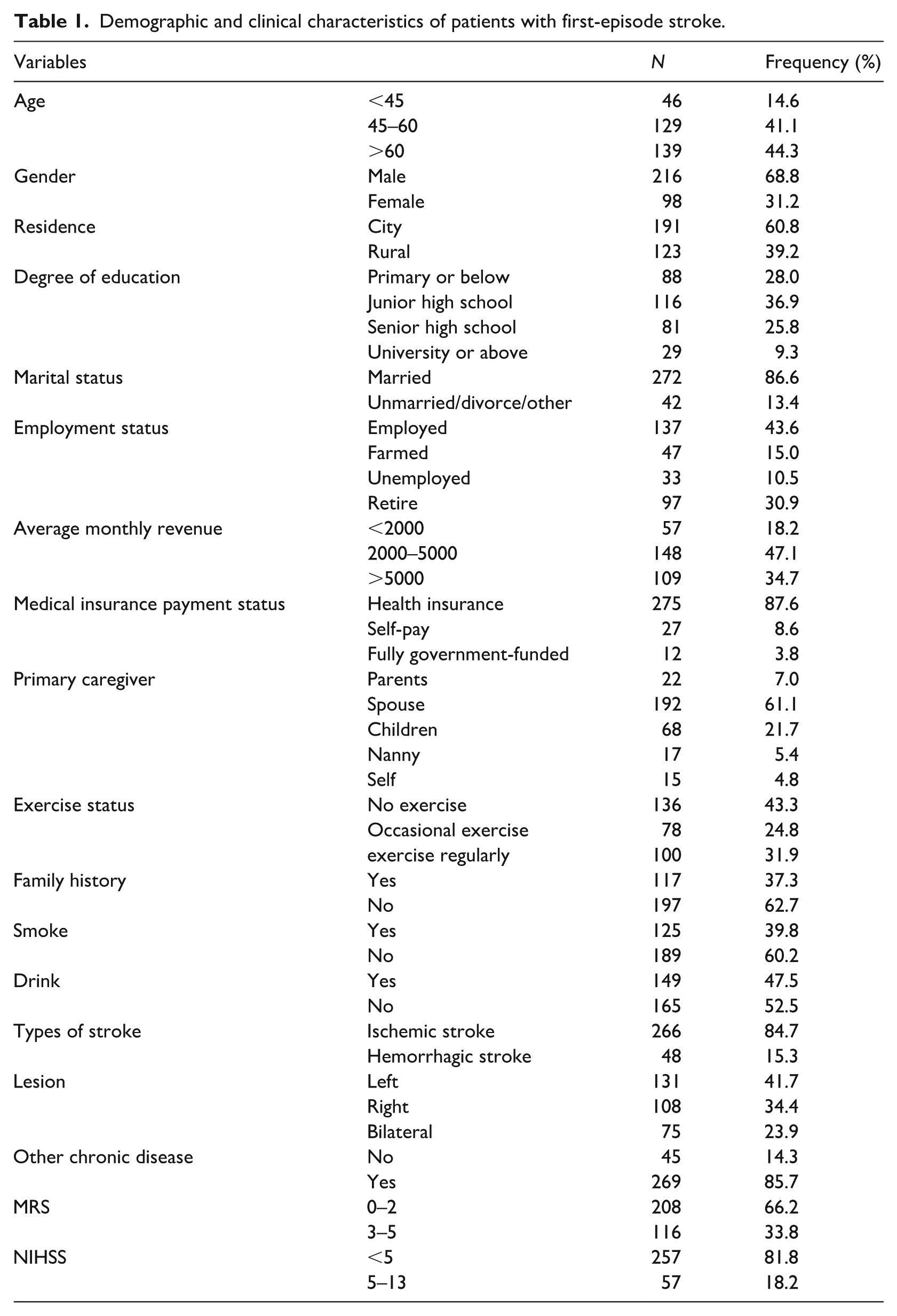
The questionnaire encompasses socio-demographic information and disease-related data. The socio-demographic section includes variables such as age, gender, residence, educational attainment, marital status, occupation, average monthly income, type of medical insurance, primary caregiver type, and physical activity levels of the respondents. Disease-related data comprise family history of stroke, history of tobacco use and alcohol consumption, stroke subtype, presence of comorbid chronic conditions, lesion location, and measures of physical disability, assessed using the Modified Rankin Scale (MRS), as well as neurological impairment evaluated by the NIHSS.
Fear of progression questionnaire-short form
This assessment tool was initially developed by the Mehnerts’ research team (Mehnert et al., 2006) in 2006. Subsequently, Chinese scholar Wu et al. (2015) conducted cultural adaptation in 2015 to localize it for Chinese populations, translating it into Chinese and applying it in clinical studies involving patients with primary liver cancer. The instrument comprises two sub-dimensions: physical health and social family. It contains a total of 12 items, with each dimension encompassing 6 items. Specifically, items 1, 2, 3, 5, 9, and 10 constitute the physical health dimension, while items 4, 6, 7, 8, 11, and 12 form the social family dimension. The questionnaire adopts a five-point Likert scale, with total scores ranging from 12 to 60. Based on this scoring range, the level of fear can be categorized into three tiers: low fear (12–22 points), moderate fear (23–36 points), and high fear (37–60 points). A total score of 34 or above is considered a clinical warning threshold, indicating the potential presence of psychological distress in patients. In this study, the Cronbach’s α coefficient for the scale was 0.85.
Brief illness perception questionnaire
The questionnaire was revised and compiled by Broadbent et al. (2006) and has since been widely adopted across numerous countries to evaluate patients’ perceptions of illness. The instrument comprises three dimensions: emotional response, cognitive representation of the disease, and perceived understanding. It consists of a total of nine items. The first eight items are rated on a 0–10 scale, where 0 indicates “no impact at all” and 10 indicates “extremely severe impact.” Item 9 is an open-ended question, while items 3, 4, and 7 require reverse scoring. The total score ranges from 0 to 80, with higher scores reflecting more pronounced negative perceptions of illness-related experiences. The Cronbach’s α coefficient for the questionnaire in this study was 0.83, indicating acceptable internal consistency.
Perceived social support scale
The scale was originally developed by Zimet et al. (1990), and the Chinese version was subsequently adapted by Chinese scholar Jiang (2002). This assessment instrument comprises three dimensions: family support, friend support, and other forms of support, encompassing a total of 12 measurement items. The scale adopts a seven-point Likert format (where 1 indicates strongly disagree and 7 indicates completely agree), with a total score ranging from 12 to 84. A higher total score reflects a higher level of perceived social support by the individual. In this study, the Cronbach’s α coefficient was 0.93.
Medical coping modes questionnaire
This questionnaire, developed by researcher Feifel et al. (1987), has been extensively utilized to evaluate coping strategies among patients with chronic illnesses. The scale comprises three dimensions: confrontation, avoidance, and resignation, encompassing a total of 20 items. The confrontation dimension consists of items 1, 2, 5, 10, 12, 15, 16, and 19, while the avoidance dimension includes items 3, 7, 8, 9, 11, 14, and 17. The resignation dimension comprises items 4, 6, 13, 18, and 20. All items are rated on a four-point Likert scale (ranging from 1 to 4 points), with 8 items requiring reverse scoring. The original scores for each dimension were standardized by dividing the actual score by the maximum possible score. The dimension yielding the highest standardized score indicates the individual’s predominant coping strategy. The Cronbach’s α coefficients for the three dimensions in this study were 0.73, 0.86, and 0.82, respectively.
Posttraumatic stress disorder check-list -civilian version
This scale is designed to assess the psychological stress responses of individuals following traumatic events (Ruggiero et al., 2003). The evaluation of PTSD symptoms encompasses three primary symptom clusters: re-experiencing, avoidance and emotional numbing, and hyperarousal. The scale comprises a total of 17 items, with 5 items measuring re-experiencing symptoms, 7 items assessing avoidance and numbing symptoms, and 5 items evaluating hyperarousal symptoms. A five-point Likert scale is used for scoring, where 1 indicates “no symptoms” and 5 indicates “extremely severe symptoms.” A total score of 38 is considered the threshold indicating the presence of PTSD symptoms (Dobie et al., 2002), with higher scores reflecting greater symptom severity. The Cronbach’s α coefficient for the scale in this study ranged from 0.86 to 0.89, indicating good internal consistency.
Statistical analysis
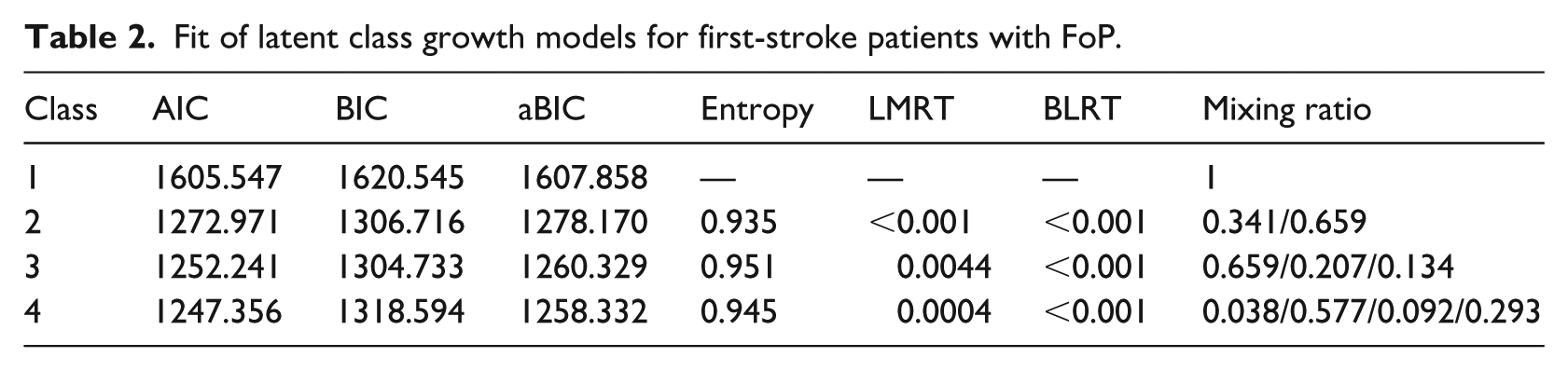
SPSS 26.0 and Mplus 8.3 statistical software were employed to process and analyze the research data. Count data were summarized using frequencies and constituent ratios. When the absolute value of the skewness coefficient of the variable is less than 2 and the absolute value of the kurtosis coefficient is less than 7, then the variable is regarded as meeting the standard of normal distribution (Kim, 2013). Data conforming to a normal distribution were expressed as mean ± standard deviation, whereas data with skewed distribution were reported using medians and interquartile ranges. Comparisons between groups were conducted using the chi-square test and analysis of variance. Variables that showed statistical significance in univariate analysis were selected for further analysis, followed by the construction of a multiple logistic regression model. Additionally, LCGM was developed and evaluated based on several model fit indices, including the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), sample-adjusted Bayesian Information Criterion (aBIC), Entropy, Lo-Mendell-Rubin likelihood ratio test (LMR), and Bootstrapped Likelihood Ratio Test (BLRT). Lower values of AIC, BIC, and aBIC, along with higher Entropy and statistically significant p-values (p < 0.05) for LMR and BLRT, indicated a well-fitting model.
Results
Participant characteristics
At time point T1, a total of 353 valid questionnaires were sent out. At time point T2, 337 people completed the follow-up, among whom 15 cases were lost to follow-up and 1 case relapsed. At time point T3, 325 people completed the follow-up, among whom 8 cases were lost to follow-up and 4 cases relapsed. At time point T4, 314 people completed the follow-up, among whom 9 cases were lost to follow-up and 2 cases relapsed. As shown in Figure 1. The demographic and clinical characteristics of the 314 patients who completed follow-up at all four time points are presented in Table 1. We used Missing Completely at Random (MCAR) to examine the pattern of missing data, and the results indicated that missing data in this study were randomly distributed (p > 0.05).Given the low attrition rate (11.05%) and random missing pattern, the potential bias caused by missing data was minimal. Although missing data may slightly reduce statistical power, the final sample size (n = 314) still exceeded the calculated minimum sample size (n = 142) and met the statistical requirement for power analysis.
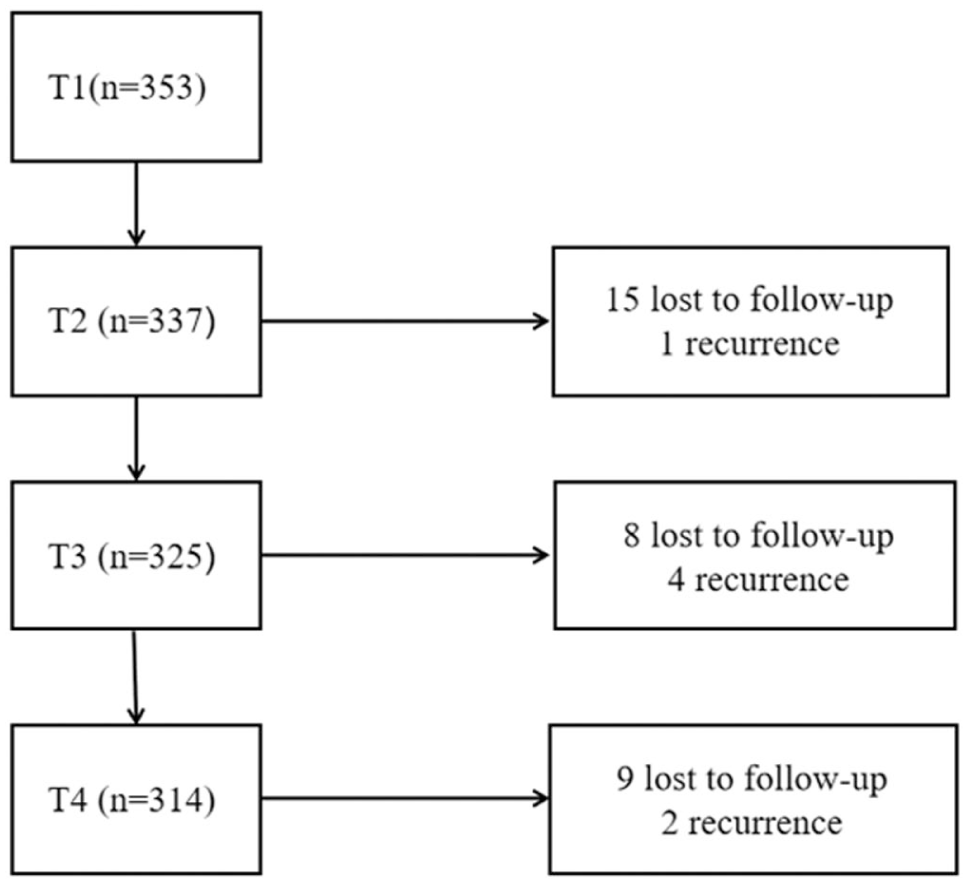
Sample loss flowchart.
Demographic and clinical characteristics of patients with first-episode stroke.
Identification of potential subcategories and naming of trajectories for first-stroke patients with fop
The heterogeneity in FoP trajectories among first-episode stroke patients was analyzed using LCGM, with FoP scores collected during the follow-up period serving as the primary variable. The model fitting results are summarized in Table 2. Model fit indices indicated that as the number of latent classes increased from 1 to 4, the AIC and aBIC values continuously decreased, while the BIC value reached its minimum at 3 classes. Additionally, the entropy value of the three-class model was superior to that of other models, suggesting better classification accuracy and model clarity. The LMRT and BLRT values for models with 2–4 classes were all statistically significant. However, when the number of classes increased from 3 to 4, the proportion of one class fell below 5%, which was considered insufficient for meaningful interpretation. At the same time, the BIC value is minimal when there are three categories. Based on a comprehensive evaluation of model fit indices and prior research, the three-class model was determined to best represent the data. Class 1 included 207 individuals (65.9%), who exhibited moderate FoP levels at T1 and a consistent decline in subsequent time points. This group was labeled the “Moderate-level decrease group.” Class 2 consisted of 65 individuals (20.7%), who initially showed high FoP levels. Although a decline was observed over time, FoP levels remained relatively high at the final time point. This group was termed the “High-level stable group.” Class 3 comprised 42 individuals (13.4%), who demonstrated a gradual increase in FoP levels throughout the follow-up period. This group was classified as the “Moderate-level increase group.” The trajectory patterns of each class are illustrated in Figure 2.
Fit of latent class growth models for first-stroke patients with FoP.
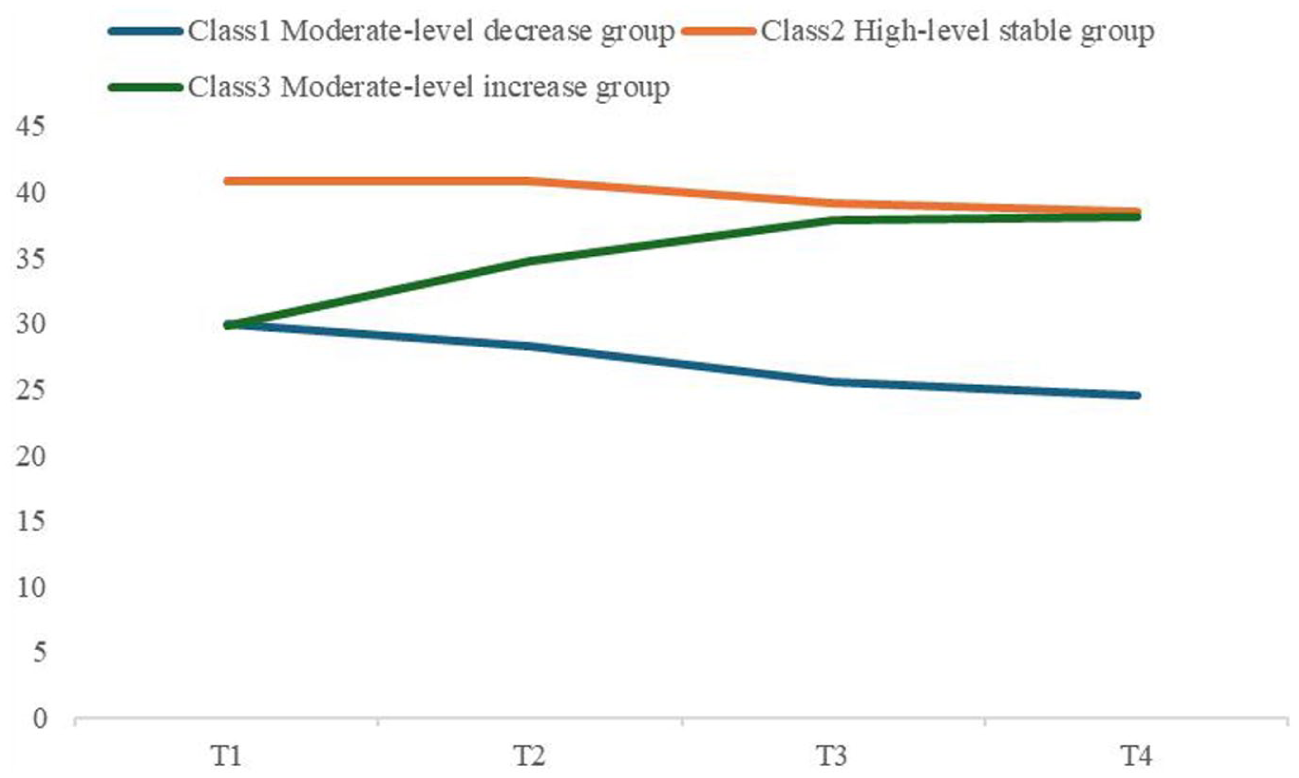
Growth model diagram for potential categories of first-stroke patients with FoP.
Univariate analysis of latent categories of functional oriented pathways trajectories in first-stroke patients
The distribution of raw scores for each variable falls within the normal range for skewness and kurtosis, meeting the criteria for normal distribution. Univariate analyses of the three potential categories of FoP in first-episode stroke patients with varying demographic and clinical characteristics are presented in Table 3. The results of the univariate analysis indicated statistically significant differences among the three groups in terms of age, employment status, average monthly revenue, medical insurance payment status, MRS and NIHSS (p < 0.05). Additionally, significant differences were observed across the three independent subgroups regarding illness perception, perceived social support, PTSD, and coping styles including confrontation, avoidance, and resignation (p < 0.05).
Univariate analysis of the development trajectory of fear of disease progression in patients with first-ever stroke.
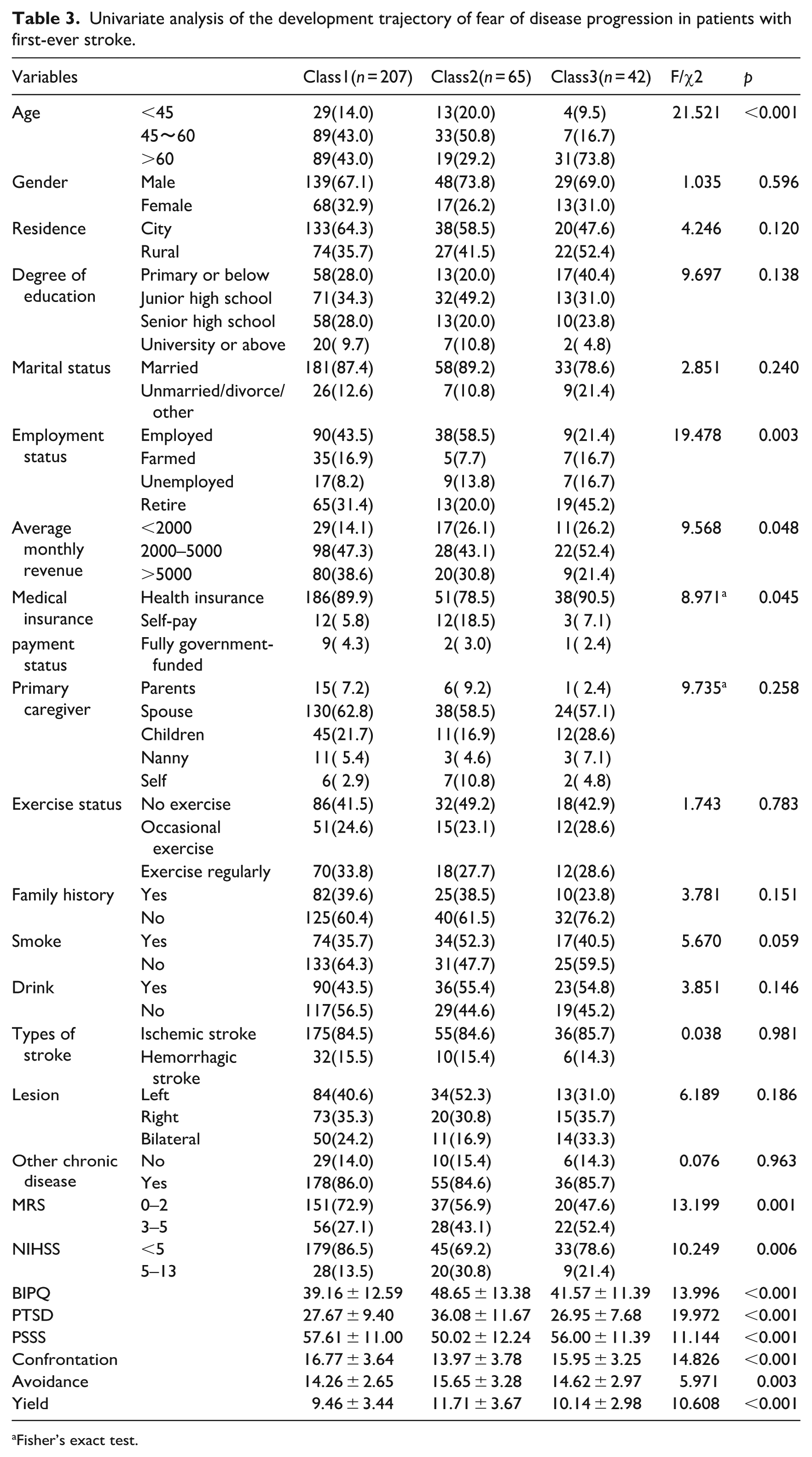
Fisher’s exact test.
Multivariate analysis of latent categories in the fear of disease progression trajectories of first-stroke patients
Predictors that demonstrated statistically significant differences in univariate analysis were selected for unordered multinomial logistic regression to identify independent predictors across different population subgroups. Using Class 2 (High-level stable group) as the reference category, the results indicated that PTSD and confrontation coping styles were independent predictors for Class 1 (Moderate-level decrease group) (p < 0.05). For Class 3 (Moderate-level increase group) in patients with first-ever stroke, PTSD, age (46–60 years), and MRS were identified as significant influencing factors (p < 0.05). Further details are presented in Table 4.
Multinomial logistic regression analysis of heterogeneous subgroup influencing factors of fop population in first-ever stroke patients.
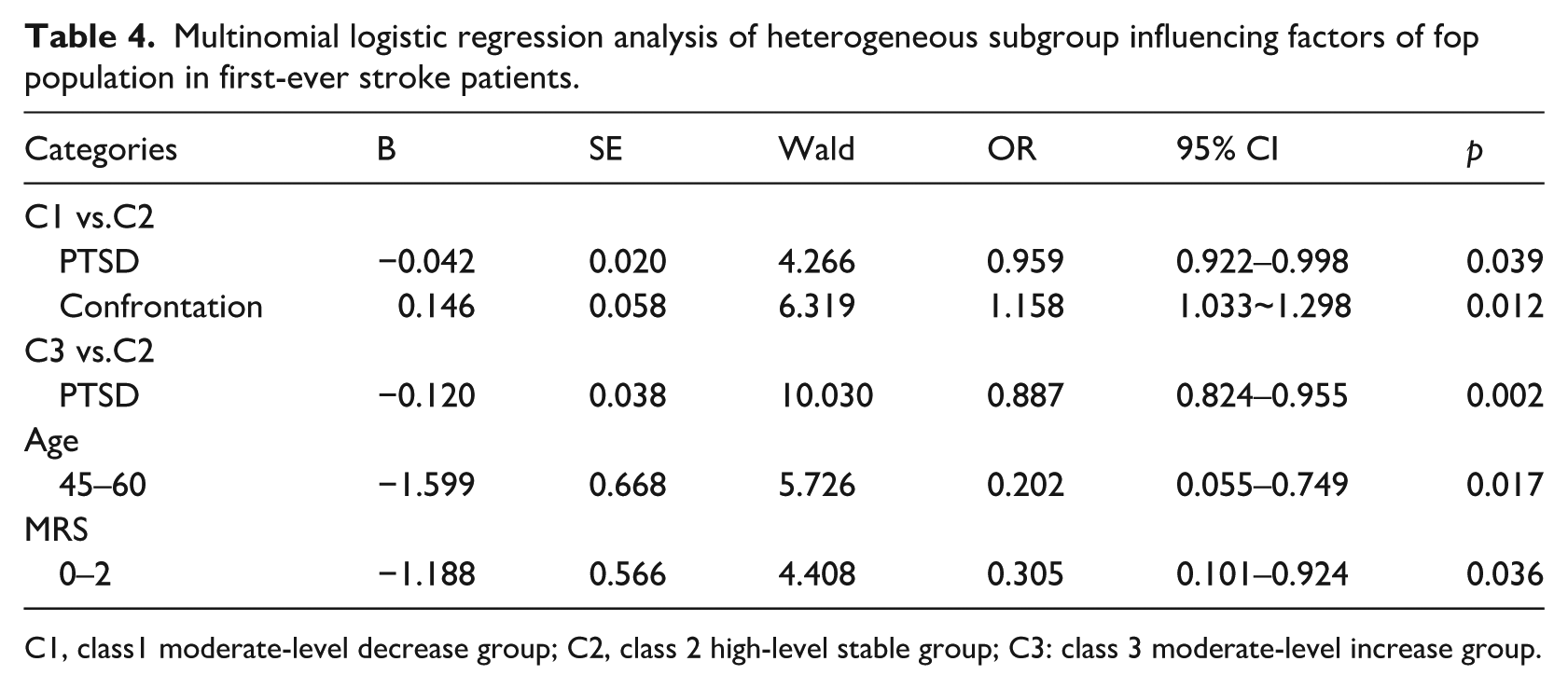
C1, class1 moderate-level decrease group; C2, class 2 high-level stable group; C3: class 3 moderate-level increase group.
Discussion
This study exclusively enrolled patients with mild to moderate stroke and excluded those with speech dysfunction. This exclusion was necessary because patients with severe stroke (NIHSS score >13) often present with significant neurological deficits, impaired consciousness, dysphagia, and high complication rates. Their pathophysiological mechanisms, treatment responses, and prognostic patterns differ markedly from those of mild to moderate stroke patients. Concurrently, severe stroke patients frequently require more complex emergency and supportive care. Some patients, due to their critical illness, may be unable to complete the assessment protocols established for this study, potentially leading to data loss, selection bias, and outcome bias during follow-up. Therefore, patients with severe strokes were excluded. However, this exclusion may also limit the generalizability of the study findings to some extent.
Using LCGM, we identified three distinct trajectories of FoP, which are comparable to those reported in FoP studies among cancer and chronic disease populations but remain under-investigated in stroke cohorts. We found that more than 60% of patients belonged to a moderate-level decreasing trajectory, suggesting that most stroke patients can gradually achieve psychological adaptation with standardized treatment and health education. This finding is consistent with previous research (Custers et al., 2020), which suggests that as patients gain access to information about their condition, reframe their perceptions, and adopt more effective coping strategies, their subjective perception of the threat posed by the illness gradually diminishes. Approximately 20% of patients exhibited a high-level stable FoP trajectory. Although scores declined slightly over time, they remained above the threshold for psychological distress throughout follow-up, indicating persistent maladaptation. This pattern mirrors the high stable fear trajectory observed among cancer survivors by Schapira et al. (2022), reflecting the long-term psychological impact of sudden-onset severe illness. Stroke is characterized by acute onset, uncertain prognosis, and high risk of motor, swallowing, and speech impairments (Dulay et al., 2023; Yusuf et al., 2020). Combined with insufficient disease-related knowledge and poor emotional regulation, these factors prevent some patients from recovering from acute stress, leading to sustained high levels of fear (Gu et al., 2026; Ning et al., 2025). About 13% of patients showed a moderate-level increasing FoP trajectory, especially during the transition from inpatient rehabilitation to home care. This highlights the unique challenges stroke survivors face during the critical transition period from inpatient rehabilitation to home care. Discharge often signifies a reduction in structured support, shifting responsibility for symptom monitoring and rehabilitation adherence to patients and caregivers (Morone and Pichiorri, 2023). For individuals with residual neurological deficits, the absence of ongoing medical supervision may cause heightened anxiety, as subtle symptom changes—such as transient weakness or fatigue—can be mistaken for signs of recurrence or deterioration (Huang et al., 2025).Our findings indicate that over 50% of patients experience a gradual decrease in FoP levels during the later stages of the disease. However, a portion of the group still exhibits elevated FoP levels, consistent with previous research (Schapira et al., 2022). This suggests that over time, FoP remains one of the common mental health issues affecting patients during their recovery phase. These findings suggest that establishing a dynamic screening system for high-risk individuals, implementing individualized psychological education interventions for those with positive screenings, shifting from reactive responses to proactive prevention, and focusing on enhancing patients’ role functioning, cognitive abilities, and emotional regulation skills could significantly improve their overall quality of life.
In this study, PTSD emerged as a significant factor influencing both the moderate decline group and the moderate increase group. This finding was unexpected and intriguing, despite prior research confirming PTSD as an independent predictor of FoP (Guo et al., 2025; Smith et al., 2018). This suggests that, from a long-term disease progression perspective, PTSD may not be a simple unidirectional risk factor but rather exhibits heterogeneity and bidirectional effects on FoP. PTSD encompasses symptoms such as heightened arousal, intrusive thoughts, and hypervigilance, as well as avoidance, emotional numbing, and denial. Patients primarily exhibiting avoidance, numbing, and passive coping actively reduce their perception of disease-related threats, manifesting as diminished subjective experience of FoP (Sumner et al., 2021). According to Horowitz’s stress response model (Horowitz, 1986) patients who avoid stressors psychologically and behaviorally may achieve temporary relief in their physical and mental states in the short term. If patients then employ active coping strategies, this may further promote a reduction in FoP. Meanwhile, due to the frequent outpatient follow-ups or revisit requirements associated with stroke, some patients repeatedly expose themselves to traumatic environments. Intrusive traumatic memories may alter their previous perceptions of the disease (Nguyen et al., 2025). Negative cognitions further erode individuals’ self-belief, amplifying the disease’s negative impact and leading them to become more prone to excessive focus on disease-related symptoms. Even minor symptoms are often overinterpreted. This cognitive bias not only diminishes trust in current treatment plans but may also trigger intense prognostic anxiety, thereby exacerbating FoP.
Coping styles, as key modulators of psychological stress responses, directly influence the intensity of physiological and psychological reactions during stressful states through their specific types and effectiveness. Positive coping strategies can effectively mitigate the impact of stressors on psychological well-being, maintaining stress responses within a manageable range. In contrast, negative coping strategies may exacerbate stress responses (Burnos and Wrzosek, 2021; Yuan et al., 2022). During the recovery phase of illness, patients can engage in cognitive restructuring and behavioral activation through adaptive coping mechanisms, thereby reframing disease-related threats as controllable challenges and reducing the FoP during follow-up periods.
Previous studies have confirmed that age is an adverse predictor for FoP in patients (D’Souza et al., 2026; Li et al., 2025; Liu et al., 2025; Zhu et al., 2025). However, some studies have also shown that age is not correlated with FoP (Goebel and Mehdorn, 2019; Luo et al., 2025). In this study, Age (45–60 years) serves as an independent predictor of elevated FoP. This may be explained by the fact that, following initial diagnosis and discharge, further disease progression among middle-aged patients can lead to significant disease-related stress and unfavorable prognostic outcomes. These factors may result in the loss of work capacity or disruption of career trajectories, thereby exerting a profound impact on household financial stability (Strilciuc et al., 2021). Individuals within this age group are typically the primary breadwinners and emotional anchors of their families, bearing substantial socioeconomic responsibilities. They are often tasked not only with caring for aging parents but also with supporting and raising children. Consequently, they are particularly vulnerable to the psychological and practical implications of income reduction and diminished social roles (Feigin and Owolabi, 2023). The dual burden of these familial and societal obligations may precipitate a breakdown in the family support system, thereby generating considerable psychological distress and contributing to heightened levels of FoP.
MRS is frequently utilized to assess neurological functional recovery following stroke (Saver et al., 2021). MRS score ranging from 0 to 2 indicates that the patient experiences either no disability or only mild disability, whereas a score of 3 or higher typically reflects a decline in physical function (Bazan et al., 2025), which is significantly associated with an increased risk of stroke recurrence and long-term care requirements (Sluis et al., 2025). Severe stroke often results in persistent disability, which may directly restrict the patient’s daily activities and hinder their reintegration into society. Patients may consequently develop a heightened awareness of the disease’s impact on their physical condition, leading to diminished happiness, reduced enthusiasm for daily life, and increased anxiety regarding disease progression. Furthermore, the economic burden associated with disability,such as reduced income or elevated caregiving costs, not only compromises treatment adherence but also exacerbates fears of uncontrolled disease progression due to cognitive misinterpretation.
Study limitation
Due to objective constraints in the research cycle and human resources, the sample collection for this study was limited to a single tertiary hospital in Nantong. As a single-center study may result in limited sample heterogeneity, future research should consider multi-center and larger-sample designs to enhance generalizability. Furthermore, since this study only followed patients for 6 months after their initial stroke, longitudinal studies with extended follow-up periods are recommended to capture better the dynamic changes in FoP levels among post-stroke patients.
Conclusion
In this study, LCGM was employed to identify three distinct trajectory patterns of FoP among patients who had experienced their first stroke: the medium-decreasing group, the high-stable group, and the medium-increasing group. Factors associated with these trajectory categories included age, MRS, PTSD, and Confrontation coping styles. These findings underscore the importance of early identification of stroke patients and conducting comprehensive psychosomatic assessments. Healthcare providers should pay close attention to the dynamic changes in patients’ FOP during clinical practice. For individuals at higher risk of FOP, targeted psychological support may be considered, which could potentially enhance the effectiveness of psychological interventions in clinical settings.
Footnotes
Acknowledgements
We would like to express our sincere gratitude to all the hospital staff for their support and help, as well as the patients who participated in this study. Trajectory Characteristics and Influencing Factors of Fear of Progression Among Patients With First-Ever Stroke: A Prospective cohort Study
Ethical considerations
The institutional ethics committee approval was granted (Affiliated Hospital of Nantong University Ethical Committee,2024-K051-01)
Consent to participate
All participants signed written informed consent forms.
Consent for publication
All participants provided written consent for the publication of anonymized data collected during the study. No identifiable information about participants will be disclosed in this publication.
Author contributions
Conceptualization, Methodology: GX, QH, ZQ, CJ, YH, WF; Data collection and collation: GX, ZQ, CJ; Data Statistical Analysis: GX, QH, ZQ; Literature retrieval and drafting: GX, QH; Revision of the manuscript: QH, YH, WF; Study supervision: QH and WF. All authors approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data are available from the corresponding author upon reasonable request*.