
Abstract
Epilepsy can profoundly influence children’s psychological functioning, yet the contextual factors shaping this experience remain insufficiently understood. Using data from 104 children with epilepsy, their parents, homeroom teachers, and 1829 classmates, this study examined factors affecting children’s psychological functioning. A range of diagnostic, psychological, and social variables were assessed, and structural equation modeling was used to analyze relationships. The results showed that both epilepsy-related factors (presence of comorbidities, non-verbal intelligence, seizure freedom, and number of antiepileptic medications) and social influences significantly contributed to psychological functioning. Key social influences linked to the school environment included teacher support and attitudes, classmates’ awareness of the child’s epilepsy, stigma among classmates, and the child’s sociometric position. On the parental side, a significant role was played by parental depression and discrepancies between parent and child quality-of-life assessments. Notably, social influences were as impactful as medical factors, underscoring the need for holistic, multi-level interventions.
Introduction
Childhood epilepsy as one of the most common neurological disorders has a global incidence ranging from approximately 33–82 cases per 100,000 individuals annually (Fine and Wirrell, 2020). Over 8 million children and adolescents worldwide were living with epilepsy (Su et al., 2025) which has consequences that extend beyond clinical symptoms, profoundly affecting the psychological functioning of children with epilepsy (CWE). Accordingly, CWE experience markedly reduced quality of life (QoL) and a higher prevalence of depression and anxiety compared to the general pediatric population and children with other chronic conditions (Idowu et al., 2025; Reilly et al., 2011), with roughly one-third experiencing depressive symptoms and nearly half anxiety symptoms (Rodenburg et al., 2005).
The influence of epilepsy-related factors—such as seizure type, frequency or severity, and duration of epilepsy—has been extensively studied, with the number of antiepileptic medications and poor seizure control emerging as the most detrimental predictors of mental health and QoL in CWE (Ferro, 2014; Reilly et al., 2011). Beyond these medical variables, clinical characteristics such as comorbidities and intellectual abilities also show consistent associations with psychological outcomes, whereas demographic factors like gender and age yield more inconsistent effects, suggesting they may interact with medical and psychosocial influences rather than operate independently (Buelow et al., 2003; Fayed et al., 2015; Ferro, 2014; Reilly et al., 2011).
In contrast, psychosocial factors are the most robust correlates of QoL and mental health in CWE (Fayed et al., 2015; Reilly et al., 2011; Temple et al., 2023). Among these, parental mental health problems—commonly reported in parents of CWE—are associated with disruptions in parenting that foster feelings of rejection and weaken parent–child relationships (Ferro and Speechley, 2009; Jones and Reilly, 2016; Rodenburg et al., 2005). In this respect, parent–child discrepancies in QoL assessments may serve as indirect indicators of the quality of parent–child interaction. Although some degree of divergence between self- and parent reports is common in pediatric chronic illness, research shows that these discrepancies are less attributable to the child’s demographic or clinical characteristics and more closely related to parental psychosocial functioning and the broader family context. Specifically, poorer parental mental health, lower parental QoL, and elevated caregiving burden are associated with greater parent–child disagreement, whereas cohesive, low-conflict, and emotionally expressive family environments tend to promote higher agreement between reports (Eiser and Varni, 2013; Radicke et al., 2021; Silva et al., 2015). Taken together, these findings suggest that parent–child (dis)agreement in QoL assessments may mirror the level of emotional availability, empathy, and communication between parent and child.
Epilepsy-related stigma constitutes another major psychosocial risk factor, reported by nearly half of CWE (Aydemir et al., 2023) and recognized as one of their most significant concerns (Webster, 2020). It frequently manifests through negative interpersonal experiences such as bullying, to which CWE are more often exposed than peers with less stigmatizing chronic conditions (Emick et al., 2025). Interpersonal stigma may further internalize, reinforcing self-stigmatization associated with diminished perceived social support and self-efficacy (Fiest et al., 2014). Ultimately, stigma contributes to lower self-esteem and poorer mental health and QoL (Akca and Akca, 2026; Jacoby and Austin, 2007; Temple et al., 2023).
Given the central role of psychosocial factors in shaping psychological functioning in CWE, the school environment constitutes a key context where teachers and classmates play a crucial role in their daily experiences and development. CWE often experience peer difficulties, partly due to limited social interactions resulting from increased school absenteeism (Aguiar et al., 2007). Some are excluded from peer groups (Baker et al., 2005), while others deliberately withdraw out of fear of negative reactions to potential seizures (McEwan et al., 2004). Nevertheless, support from peers and classmates appears to play a pivotal role in shaping QoL in CWE—possibly even exceeding the impact of parental support (Fayed et al., 2015; Ferro et al., 2017). While peer relationships are central to the social experiences of CWE, teachers also represent critically important figures for students with chronic health conditions, including epilepsy. Their support is particularly needed in managing school absences, facilitating participation in school activities, fostering positive peer relationships, explaining the condition to classmates, and serving as trusted adults with whom children can discuss health-related concerns (Mukherjee et al., 2000).
In this context, a significant issue involves teachers’ perceptions and attitudes toward epilepsy. Research consistently indicates notable gaps in their knowledge and generally negative attitudes (Jones et al., 2018). Teachers may underestimate the academic abilities of CWE (Katzenstein et al., 2007), are less accepting than of children with other chronic conditions, and provide less encouragement for social interaction with peers (Chiou and Hsieh, 2018). Such attitudes can hinder both the academic performance and social development of CWE. Academic self-concept—reflecting children’s self-perceived competence and confidence in their academic abilities—has been shown to be significantly lower in CWE than in their peers without epilepsy (Brabcova et al., 2015; Buršíková et al., 2025; Scatolini et al., 2017). CWE tended to perceive themselves as clumsy, socially isolated, and academically underperforming, reporting difficulties at school and frequent feelings of unhappiness (Scatolini et al., 2017). The diminished academic self-concept observed in CWE may be partly attributable to their lower academic achievement, which largely depends on the severity of the condition (Huberty et al., 2000), as well as to the higher prevalence of specific learning disabilities (SLD) and/or attention deficit hyperactivity disorder (ADHD), both of which further undermine academic self-concept in this group (Buršíková et al., 2025; Ekinci et al., 2016). Interestingly, the correlation between academic achievement and academic self-concept was markedly weaker in CWE than in their peers without epilepsy, while the proportion of children with very high self-concept was comparable across groups. This suggests that, in CWE, academic self-concept is affected to a lesser extent by academic performance or epilepsy-related factors, and more strongly by psychosocial aspects (Brabcova et al., 2015; Ekinci et al., 2016). Taken together, these findings suggest that the psychosocial experiences of CWE are shaped not only by family influences but also by the broader school environment and its key actors.
Most existing studies on the psychological functioning of CWE have focused on isolated determinants, examining only a limited set of variables and thereby restricting a comprehensive understanding of the key factors shaping the lives of individuals with this condition. Although a few structural models have attempted to capture the interplay between medical and psychosocial factors, they provide only a partial picture—either by offering a limited perspective from CWE themselves (Fayed et al., 2015) or by combining children’s perspectives with those of their parents (Mitchell et al., 1994). A major gap in the literature thus remains: the absence of an integrative framework that situates CWE within the broader ecological context of their lives. In particular, the school environment—where children spend much of their time and face unique social and academic challenges—has been largely overlooked.
To address this gap, the present study adopts a holistic approach by developing a structural model of psychological functioning in CWE. This model is theoretically anchored in the conceptual models of Ronen et al. (2003) and Lach et al. (2006) as well as on the structural model developed by Fayed et al. (2015). It is based in line with these studies on the triad of medical factors (biomedical status/level of impairment), psychosocial variables (family and community) and functioning of CWE which includes quality of life, mental health and related concepts. It integrates medical and psychosocial variables across multiple perspectives—those of CWE, their parents, teachers, and classmates—to capture the complex interplay of factors shaping children’s daily experience. Specifically, the study examines the relative contribution of epilepsy-related factors and psychosocial aspects—such as those arising from the family and school environments—to the psychological functioning of CWE, conceptualized as a composite construct encompassing mental health, QoL, and academic self-concept. The hypothesis is that both epilepsy-related and psychosocial factors significantly predict the psychological functioning of CWE, with psychosocial aspects exerting effects comparable to or greater than those of medical variables. Despite the primarily theory-driven approach used in this study, an empirical specification of the model described below was needed due to the complexity of the issue and the limited sample size.
Method
Participants
The study included CWE (n = 104), their parents/guardians (n = 104), their homeroom teachers (n = 104), and their classmates (n = 1829). The inclusion criteria for CWE required them to be aged between 8 and 15 years, as the measurement instruments were appropriate for this age category and to attend a regular elementary school or its equivalent offering a more extended curriculum (Gymnasium). Children outside the specified age range and those attending practical schools were excluded. The study was conducted in accordance with the 1964 Helsinki Declaration and its later amendments. Ethical approval was obtained from the institutional ethics committee (approval no. GJ16-02453Y). All participants provided informed consent to take part in the study. In the case of underage participants, written informed consent was obtained from parents/guardians, accompanied by the assent of the children themselves. In the classroom sessions, only children from whom consent and assent had been obtained participated in the study.
Recruitment of CWE and their parents/guardians was conducted through two networks: collaborating child neurologists and principals of elementary schools in the Pilsen, South Bohemian, and Karlovy Vary districts in the Czech Republic. These contacts informed parents/guardians of eligible children about the possibility of participating in the research. Once parents/guardians expressed willingness to participate, the consent of the school principals where the child attended, as well as the child’s homeroom teachers, was sought. Additionally, the parents/guardians of classmates of CWE were asked for consent for their children to participate. A total of 125 parents/guardians of CWE meeting the inclusion criteria were contacted, and 104 ultimately participated. Non-participation was primarily due to parental/guardian refusal, often because they did not disclose the child’s epilepsy diagnosis to the school and were unwilling to participate in research involving school settings, or due to failure to submit the required forms. In two instances, school principals declined to participate.
The demographic characteristics of CWE are illustrated in Supplemental Table 1, with the type and frequency of seizures being presented in Supplemental Table 2. Characteristics of parents/guardians, homeroom teachers, and classmates of CWE are displayed in Supplemental Tables 3–5, respectively.
Measures
Since the present study is part of a larger project investigating the specific challenges faced by Czech CWE and their families, including broader aspects of psychosocial functioning and factors facilitating their adjustment, only a subset of variables relevant to the current analysis is described in more detail here.
Background variables
Background information for CWE included gender and age; for parents/guardians, type of relationship to the child, age, and highest level of education; for teachers, gender, age, length of pedagogical experience, specialization, prior teaching experience with a student with epilepsy, exposure to epilepsy during studies, and interest in information about epilepsy; and for classmates, gender, prior introduction to epilepsy, and acquaintance with a person with epilepsy. For parents, teachers, and classmates, this information was self-reported; for CWE, it was reported by parents/guardians.
Diagnostic information
The epilepsy-related diagnostic variables relevant for the analysis were comorbidities, namely ADHD and SDL, seizure freedom in the past 12 months, and the number of antiepileptic medications. Other diagnostic variables used to characterize the sample included type and frequency of seizures, mother’s age at the time of the child’s birth, mean duration of epilepsy, age at epilepsy diagnosis, and any change in treatment within the past 2 months. A diagnostic questionnaire was completed by the parents in collaboration with a pediatric neurologist.
Non-verbal intelligence of CWE
Non-verbal intelligence in CWE was assessed using the Standard Progressive Matrices (Raven et al., 1991). The test consists of five sets of 12 items each, totaling 60 non-verbal reasoning tasks. Respondents select the missing piece that best completes a visual pattern from several alternatives, with difficulty increasing progressively across sets. Each response is scored dichotomously (1 = correct, 0 = incorrect), yielding a total raw score (0–60) that is converted to age-normed percentiles. Higher scores indicate better non-verbal reasoning ability.
Depressive symptoms in CWE
Depressive symptoms in CWE were assessed using the Children’s Depression Inventory (CDI; Kovacs, 1992) in the Czech validated adaptation (Preiss, 1998). Children completed the self-report measure consisting of 27 items grouped into five subscales: Negative Mood, Interpersonal Problems, Ineffectiveness, Anhedonia, and Low Self-Esteem. Each item is rated on a three-point scale reflecting symptom severity (0 = absent, 1 = mild, 2 = severe). Scores are summed to yield a total score, with higher scores indicating more severe depressive symptoms. The CDI demonstrates good internal consistency, with Cronbach’s α values ranging from 0.71 to 0.89 (Preiss, 1998). Analyses in the present study used the total CDI score.
Absence of anxiety in CWE
The absence of anxiety in CWE was assessed using the 14-item Absence of Anxiety subscale of the Piers-Harris Children’s Self-Concept Scale – Second Edition (PHCSCS-2; Piers and Herzberg, 2002) in the Czech adaptation (Obereignerů et al., 2015). Each item is rated dichotomously (“yes” = 1, “no” = 0), and scores are summed, with higher values indicating lower anxiety. The Czech version demonstrated high internal consistency, with Cronbach’s α = 0.90 for this subscale (Obereignerů et al., 2015).
Self-concept of academic success of CWE
Self-concept of academic success in CWE was assessed using the Student’s Perception of Ability Scale (SPAS; Boersma et al., 1979) in the Czech validated adaptation (Matějček and Vágnerová, 1992). The scale comprises 48 dichotomous items (“yes” = 1, “no” = 0) covering six areas: General Abilities, Mathematics, Reading, Spelling, Writing, and Self-Confidence. Higher scores indicate a more positive academic self-concept. The Czech version demonstrates strong reliability (Cronbach’s α = 0.89–0.95). Analyses in the present study used the total SPAS score, obtained by summing all items and converting the result to sten scores according to the manual norms.
Perceived teacher support from the perspective of CWE
Perceived teacher support in CWE, defined as the teacher’s interest in the student and willingness to help when the student faces difficulties, was assessed using the five-item Teacher Support subscale of the Czech Climate of a School Class questionnaire (Mareš and Ježek, 2012). Items are rated on a five-point scale (1 = strongly disagree, 5 = strongly agree), with higher scores indicating greater perceived support. The subscale demonstrated strong internal consistency, with Cronbach’s α = 0.90.
QoL of CWE from the perspective of CWE and parents/guardians
QoL in CWE was assessed using a modified Czech version of the Children’s Quality-of-Life Measure for Children with Epilepsy (CHEQOL-25; Brabcova et al., 2014) originally developed by Ronen et al. (2003). The Czech version comprises 23 items rated on a four-point Likert scale (1 = not at all, 4 = very much) covering four domains: Interpersonal and Social Impacts of Epilepsy, Worries, Concerns, and Interests, Intrapersonal and Emotional Impacts, and Epilepsy as a Child’s Secret and the Quest for a Normal Life. Scores are summed within domains to produce subscale scores, and their total represents overall quality of life, with higher values indicating better quality of life. The subscales demonstrated satisfactory internal consistency, with Cronbach’s α ranging from 0.78 to 0.83. The questionnaire was completed independently by both CWE and their parents or guardians, with parents evaluating the child’s quality of life from the child’s perspective. Analyses in the present study used the total CHEQOL-25 score.
Depressive symptoms in parents/guardians
Depressive symptoms in parents or guardians of CWE were assessed using the eight-item Depression subscale of the Middlesex Hospital Questionnaire (MHQ; Crown and Crisp, 1966) in its validated Czech adaptation (Čepelák, 1982), which demonstrated acceptable internal consistency (Cronbach’s α = 0.71). The subscale includes both dichotomous and three-option items, scored 0–1 and 0–1–2, respectively. Total scores were calculated as the sum of all items (range 0–12), with higher scores indicating more severe depressive symptoms.
Teachers’ attitudes toward individuals with epilepsy
Attitudes toward people with epilepsy were measured using the Czech version of the Attitudes Toward Persons with Epilepsy Scale (ATPE; Antonak, 1990; Brabcová et al., 2016). The instrument consists of 21 items rated on a six-point Likert scale ranging from strongly disagree to strongly agree, with higher scores indicating more positive attitudes. It includes both negatively worded items (e.g. “Schools should not integrate persons with epilepsy into mainstream classes”) and positively worded items (e.g. “Persons with epilepsy are just like any other people as long as their seizures are controlled by treatment”); negatively worded items were reverse-scored prior to analysis. Analyses used the total ATPE score, computed as the sum of all items. The Czech version demonstrated satisfactory internal consistency, with Cronbach’s α = 0.82 in freshmen and 0.79 in senior teacher trainees.
Sociometric position of CWE
The sociometric position of CWE was assessed using the L–J test originally developed by Long and Jones (1960, as cited in Musil, 1977) and adapted into Czech by Musil (1977). The questionnaire was completed by the child’s classmates. Each student nominated their three most and three least favored peers, assigning three points for the first choice, two for the second, and one for the third. Popularity and unpopularity scores were calculated based on the total points received. The overall sociometric position was defined as the difference between the popularity and unpopularity scores.
Epilepsy-related stigma among classmates
Epilepsy-related stigma was assessed using the Czech version of the Stigma Scale of Epilepsy (SSE; Brabcová et al., 2018; Fernandes et al., 2007). The scale includes 23 items for children and adolescents rated on a five-point scale (1 = strongly disagree, 5 = strongly agree) measuring attitudes and emotional reactions toward epilepsy. Internal consistency was high (Cronbach’s α = 0.86), with higher scores indicating stronger stigma. Analyses used the total SSE score expressed as a percentage, which can be computed even with some missing responses. Only respondents familiar with the term “epilepsy” completed the questionnaire, and they were instructed to skip items they did not fully understand.
Class awareness of a child’s epilepsy
Class awareness of a child’s epilepsy was assessed based on responses to a question asking whether classmates knew someone with epilepsy and, if so, whom. The proportion of classmates who indicated awareness of the child’s epilepsy was then calculated. If at least 50% of classmates were informed about the child’s condition, class awareness was scored as “yes” (the class is aware); otherwise, it was scored as “no” (the class is not aware).
Procedure
All participants completed the questionnaires in a paper-and-pencil format. CWE and their parents/guardians filled out the forms at home following detailed written instructions and returned them to the research team either by mail or in person. The Standard Progressive Matrices were administered individually to CWE by a collaborating child psychologist, following the standardized administration procedures outlined in the test manual. Testing took place in the school environment, in a quiet room provided by the participating school, to ensure minimal distractions and standardized conditions. The assessment was conducted before regular school hours to allow children to attend their usual classes without interruption and to minimize potential fatigue associated with afternoon testing.
Homeroom teachers and classmates completed their forms during a single class session in the presence of a trained research assistant (a teacher education student), who provided detailed instructions to participants and offered individual assistance to those who had difficulty understanding particular items. Completing the questionnaires took approximately 15 minutes for parents, 60 minutes for CWE, 10 minutes for teachers, and 20 minutes for classmates. Parents were instructed to assist their children by guiding them through the questionnaires intended for CWE if needed, while refraining from influencing their responses, and to ensure that the forms were completed at the child’s own pace, with breaks taken whenever fatigue occurred and resumed later as needed. Similarly, during the classroom session, children were encouraged to take short pauses to minimize fatigue and maintain concentration while completing the questionnaires. All questionnaires were completed anonymously and labeled with numeric codes known only to the research team. These codes were used only to link data from CWE, their parents, teachers, and classmates, without recording any personal identifiers.
In the classroom settings, CWE completed a similar set of questionnaires as their classmates to maintain confidentiality and avoid drawing unwanted attention. In approximately 25% of cases, the parents/guardians of CWE requested that the research purpose be masked. In these instances, classmates were asked to complete additional questionnaires on other chronic illnesses (diabetes and asthma), with the explanation that the research focuses on children’s knowledge and attitudes toward various chronic diseases. This approach served to ethically safeguard the privacy of children whose parents did not wish their epilepsy diagnosis to be disclosed at school. This masking procedure minimized the risk of unintended identification and potential stigmatization of the child while enabling meaningful participation of classmates.
Statistical analyses
After transcribing the data from the paper-and-pencil format into an electronic database, scores for each variable were calculated (see Supplemental Table 6 for the operationalization of each relevant variable). Structural equation modeling was performed using the LISREL software. The model is theory-informed (see the last paragraph in Introduction) but empirically specified, given the complexity and novelty of integrating multi-informant data. The structural model development was specified by the conceptual framework developed by Buršíková et al. (2025) and a thorough analysis of inter-variable correlations. The process for building the structural model involved the following steps: (1) Conducting a detailed visual inspection of the inter-correlation matrix to identify clusters of variables that form latent constructs. To ensure parsimony, only variables demonstrating statistically significant associations with other variables were retained for inclusion. Conversely, variables lacking significant correlations with others were excluded from the model. This also applied to demographic variables, such as gender and age, which were independent of the other factors. Given the sample size and the number of potential indicators, this step was necessary to maintain an appropriate parameter-to-sample-size ratio and avoid model overfitting. The conceptual model indicated that a central category referring to the psychological functioning of CWE is shaped by both epilepsy-related factors and social influences (Buršíková et al., 2025). Accordingly, through a detailed visual inspection of the inter-correlation matrix, we identified clusters of variables corresponding to these overarching categories. To mitigate the potential impact of multicollinearity, variables exhibiting strong inter-correlations (r > 0.8) were excluded from the model. (2) Developing the measurement model, consisting of latent and observed variables, and evaluating its fit to the data. After excluding data from participants identified as outliers and those with missing values on any relevant scales, the model fit was assessed using data from 98 participants, employing the maximum likelihood estimation method. (3) Developing and assessing the structural model. Consistent with the measurement model, the structural model was tested using data from 98 participants, with parameter estimates obtained via the maximum likelihood estimation method, and (4) Creating alternative models and comparing their fit to the original structural model.
Results
The model comprised three latent factors: psychological functioning, epilepsy-related factors, and social influences, each represented by at least four observed indicators. The final set of observed variables associated with each latent factors is presented in Supplemental Table 6. The measurement model, constructed from a set of latent and observed variables, was developed to evaluate its fit to the data. The statistical significance of all parameter estimates within the model was examined alongside fit indices, which yielded the following results: χ2(87, n = 98) = 133.71; RMSEA = 0.073; CFI = 0.91; PGFI = 0.62. Although the fit indices approached the threshold values recommended by Hu and Bentler (1999), the model’s complexity and the multi-source nature of the data collection (involving children, parents, teachers, and classmates) support the conclusion that the fit is satisfactory.
Supplemental Figure 1 presents the standardized coefficients (β) for the measurement model and the correlations between latent constructs. For the observed indicators associated with the latent constructs social influences and epilepsy-related factors, negative coefficients reflect more positive outcomes. Conversely, for the latent construct psychological functioning, positive coefficients reflect more positive outcomes. The statistical significance of the coefficients is presented in Supplemental Table 7, indicating that all coefficients are significant at the 95% confidence level (α = 0.05). The final stage involved the development and evaluation of a structural model. In this model, social influences and epilepsy-related factors were specified as exogenous latent variables, while psychological functioning was designated as the endogenous latent variable. Model fit was evaluated using standard indices, yielding the following results: χ2(87, n = 98) = 134.26, RMSEA = 0.075, CFI = 0.90, PGFI = 0.61. These values indicate an acceptable model fit.
Two alternative models were also developed and assessed. In the first alternative model, the observed variable sociometric position was assigned to the endogenous variable psychological functioning. Fit indices for this model were as follows: χ2(87, n = 98) = 145.14, RMSEA = 0.096, CFI = 0.81, PGFI = 0.59. These results suggest a poorer fit compared to the original model. The second alternative model was informed by a structural framework proposed by Yeni et al. (2018), which examined relationships among knowledge, stigma, anxiety, depression, and QoL in adults with epilepsy. In this alternative model, the endogenous variable psychological functioning was replaced by two latent variables: psychological health (represented by the observed variables absence of anxiety and depression) and QoL (represented by the observed variables QoL and self-concept of academic success). Fit indices for this model were χ2(85, n = 98) = 181.33, RMSEA = 0.159, CFI = 0.56, PGFI = 0.47, indicating a substantially poorer fit compared to the original model. The comparison of model fit indices clearly demonstrates that neither alternative model provides a better fit to the data than the original model. Consequently, the original structural model is preferred over the alternatives.
Figure 1 illustrates the standardized coefficients for the structural model. The standardized coefficients for the paths from latent variables to observed indicators show minimal differences compared to the measurement model. In contrast, notable differences are observed in the standardized coefficients for the paths from the exogenous variables social influences, β = −0.50, p = 0.011, and epilepsy-related factors, β = −0.49, p = 0.011, to the endogenous variable psychological functioning. These results suggest that both exogenous variables exert a similar level of influence on psychological functioning, highlighting their comparable importance in explaining variance in the endogenous variable. Supplemental Table 8 presents the correlation matrix among continuous variables included in the final model.
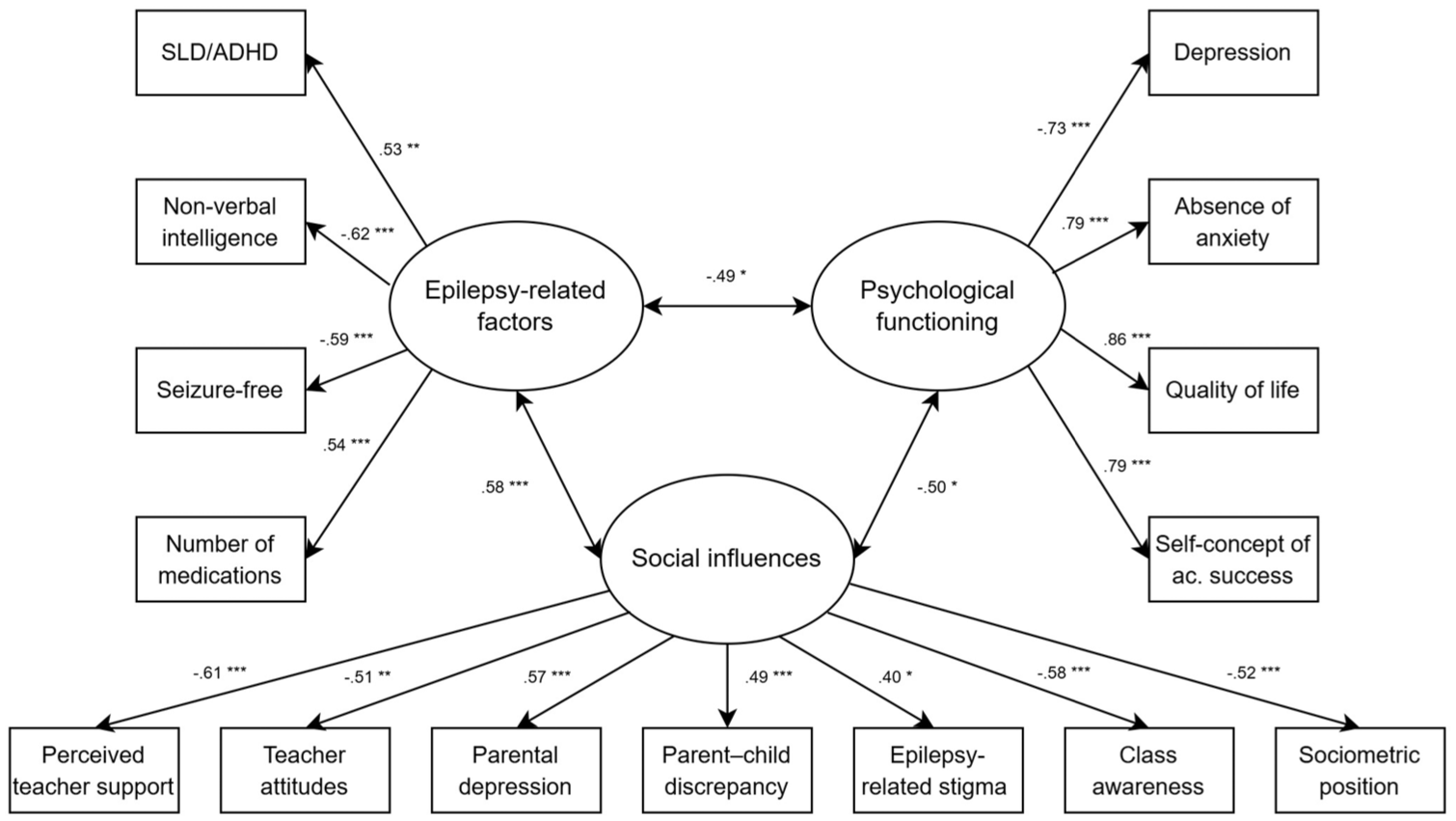
Standardized solution for the structural model.
Discussion
This study developed a structural model providing (despite its limited stability due to lower than optimum sample size) a comprehensive understanding of the experiences of CWE by integrating perspectives from children, their parents, homeroom teachers, and classmates. It tested the hypothesis that psychosocial factors exert effects comparable to or greater than epilepsy-related factors on the psychological functioning of CWE, encompassing self-reported depression, anxiety, QoL, and academic self-concept. The final model indicated a comparable effect of both factors on psychological functioning of CWE, highlighting the need for a holistic approach to better understand and promote their optimal psychological functioning. This finding is noteworthy, as it contrasts with previous literature often suggesting that social influences outweigh medical factors (e.g. Fayed et al., 2015). Our results suggest that both domains are equally important, underscoring that the impact of epilepsy-related and associated clinical variables should not be underestimated. In this respect, our research confirms the pivotal role of non-verbal intelligence, considered an epilepsy-related factor given that CWE generally exhibit lower IQ scores compared to their healthy peers (Park et al., 2013). This finding aligns with previous research demonstrating that IQ has a significant impact on mental health and self-concept in CWE (Buelow et al., 2003).
A second key domain influencing the psychological functioning of CWE involved social factors, particularly the influences of parents, teachers, and classmates. In this respect, a pioneering finding of our research is that factors linked to school environment, which were on a marginal side of research interest so far, may play a pivotal role, underscoring the importance of fostering an inclusive and supportive school environment. Within the broader category of social influences, perceived teacher support emerged as a key factor. The importance of teacher support for students with chronic health conditions is well established (Mukherjee et al., 2000) and particularly significant for younger school-aged CWE (Yang et al., 2022). Another pioneering finding that deepens our understanding of how social factors shape the psychological functioning of CWE is the key role of classmates’ awareness of the condition, which appears to act as a protective factor. Ragni et al. (2020) found that when described in sufficient detail, the diagnosis disclosure facilitated greater peer understanding and support. Thus, its positive role may arise from more accepting peer attitudes toward chronically ill children, fostered by better knowledge of their health needs (Brook and Galili, 2000), on one hand, and from greater social support, as having an ill peer can promote prosocial behavior—primarily manifesting as an increased willingness to help (Saija et al., 2025). A similar effect may stem from another contributing factor—better sociometric standing, which reflects stronger interpersonal relationships and higher levels of peer acceptance and likability. Since CWE often feel rejected and isolated (Ragni et al., 2020), maintaining positive peer relationships may not only benefit their overall psychological functioning but also enhance the frequency and quality of social support they receive. Nevertheless, as more anxious CWE also exhibited greater peer difficulties (Drewel et al., 2009), another possible interpretation could be based on a reverse—or more likely, dual—relationship, in which higher anxiety contributes to peer difficulties, while negative peer experiences, in turn, exacerbate anxiety levels.
Another important social influence was related to parental factors, which is in accordance with available literature (Jones and Reilly, 2016) Parent–child discrepancies in CWE QoL assessments which was identified as risk factor here, was previously linked to both worse parental mental health, and to dysfunctions in the family functioning, potentially mirroring decreased emotional attunement of parents toward CWE (Eiser and Varni, 2013; Radicke et al., 2021; Silva et al., 2015). Although the overall quality of the parent-child relationship often declines in families with chronically ill children (Pinquart, 2013), parents’ ability to empathize with their children’s negative emotions seems to be a crucial aspect of mental health and adjustment in these children (Main et al., 2022).
In addition, teachers’ attitudes toward epilepsy and the level of stigmatization among classmates emerged as significant contributors to the social influences cluster. It is, however, noteworthy that the relative contribution of stigma within this cluster was the lowest among the factors discussed above, despite the fact that stigmatization has traditionally been regarded as a major issue in epilepsy and a key factor negatively affecting psychological functioning (Baker et al., 2000). In this respect, our findings partially align with the conclusions of some authors who suggest that the role of perceived stigma in the development of mental health problems among individuals with epilepsy may be overestimated (Temple et al., 2023). Another possible interpretation could be that the relatively low contribution of stigma may indicate that stigmatization within the classroom plays a less prominent role—perhaps due to teacher mediation and classroom norms promoting inclusion—than that experienced in broader peer contexts, where it may persist in more subtle forms. Nevertheless, our findings still demonstrate the significant impact of stigma among classmates and teachers’ attitudes toward epilepsy, underscoring the need to continue efforts to minimize their negative effects—potentially by enhancing epilepsy-related knowledge, which has been shown to reduce stigma and promote more positive attitudes toward individuals with epilepsy (Caixeta et al., 2007; Jacoby et al., 2004).
Limitations
First, it is important to note that the developed structural model demonstrates marginal fit to the data, warranting further refinement and re-evaluation in future studies. Given the complexity of the model, replication with a larger sample would also enhance the stability of parameter estimates. According to Monte Carlo simulations by Wolf et al. (2013), structural equation models with three latent variables, four to eight indicators per variable, and factor loadings of 0.4–0.8 require approximately 200–250 cases for model stability. This estimate is consistent with the commonly used recommendation of 5–10 cases per estimated parameter (Bentler and Chou, 1987). Another limitation is that the structural model did not include demographic variables such as age and gender. Although their inclusion would be theoretically justified, their effects were insignificant, and including them would have unacceptably reduced model stability due to the lower number of observations per estimated parameter. Another conceptual limitation stems from the necessary compromise between theory-driven and data-driven approaches. Although the model was primarily theory-driven, it was also empirically specified based on detailed data analyses and a previously developed conceptual model, limiting the exploratory use of the data. However, a fully exploratory approach in such a complex field with numerous variables would require a substantially larger sample, which was not feasible for this study. Moreover, the study was conducted within a specific cultural and educational context, and the findings may not be directly generalizable to other populations. Further, while our model provides valuable insights into the interplay of medical and social factors, it is cross-sectional in nature and cannot establish causal relationships. Another limitation concerns the notable gender imbalance among parent participants, with mothers being strongly overrepresented, accounting for 93.3% of the sample. This asymmetry may limit the generalizability of the parent-reported data, as mothers and fathers can differ in their perceptions of a child’s functioning and in their emotional responses to their child’s chronic illness. The imbalance likely reflects caregiving patterns in Czech families, where mothers are typically the primary caregivers and more frequently communicate with schools and healthcare professionals. Lastly, despite its comprehensive approach, our model does not account for all potential variables that may affect psychological functioning, such as family socioeconomic status or peer support outside the school setting.
Directions for future research
Future research is warranted to replicate these findings across diverse cultural contexts to assess their broader applicability. Ideally, longitudinal studies should be conducted to examine the temporal dynamics of epilepsy-related and psychosocial factors influencing the psychological functioning of CWE. As this study included several variables that are more indicative of underlying mechanisms rather than self-explanatory in themselves, future research should build on these findings to identify the specific processes driving these associations. In particular, the results concerning classmates’ awareness of a child’s epilepsy and the parent–child discrepancies in quality-of-life assessments warrant closer examination to clarify their underlying mechanisms. Moreover, future studies should aim to recruit a more balanced parental sample to capture the perspectives of both mothers and fathers, for example through explicit invitations addressed to both parents.
Practical implications
The findings highlight key priorities for supporting the psychological functioning of CWE through targeted action in educational, familial, and clinical contexts:
1.
2.
3.
4.
5.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261458621 – Supplemental material for Psychosocial experiences are as important as medical factors in influencing the psychological functioning of children with epilepsy
Supplemental material, sj-docx-1-hpq-10.1177_13591053261458621 for Psychosocial experiences are as important as medical factors in influencing the psychological functioning of children with epilepsy by Dana Buršíková Brabcová, Ivana Mašková, Jiří Kohout, Adéla Otáhalová and Pavel Kršek in Journal of Health Psychology
Footnotes
Acknowledgements
The authors would like to thank Michala Suleková for her valuable assistance with data collection.
Ethical considerations
Ethical approval for this study was obtained from Ethical Commitee of University of West Bohemia under number GJ16-02453Y.
Consent to participate
Written informed consent for participation was provided by the participants.
Consent to publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting this study are available upon reasonable request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.