
Abstract
This study analyzed co-occurrence patterns of negative aging perceptions and psychosocial symptoms among adults aged 60 and older across stages of the pandemic using repeated cross-sectional Health and Retirement Study data (2018: n = 5688; 2020: n = 4587; 2022: n = 4377). Although cynical hostility, pessimism, and hopelessness were higher during the pandemic, overall symptom prevalence remained relatively stable, with stress and loneliness being the most common. Association rule mining showed that co-occurrence patterns were more prevalent, diverse, and complex during the pandemic and persisted afterward. Women exhibited consistently higher prevalence and greater complexity, with patterns more sensitive to pandemic stressors and primarily centered on depressive symptoms. Findings suggest lasting pandemic effects on older adults’ psychosocial well-being. Interventions should target persistent loneliness and stress and prioritize evolving symptom co-occurrence, particularly among older women.
Keywords
Introduction
Increased life expectancy reflects significant advances in public health and social development. However, ensuring that these added years are accompanied by optimal psychosocial well-being remains a central challenge for aging societies (Trtica Majnarić et al., 2021). Ideally, late life should be a period of fulfillment, as empirical evidence supports the well-being paradox wherein many older adults report stable levels of loneliness (Mund et al., 2020) or even high levels of life satisfaction (Hansen and Blekesaune, 2022) despite physical declines. Nevertheless, growing evidence indicates that aging populations face significant challenges related to psychosocial distress that coexists with this broader pattern of resilience (Wang et al., 2021). The World Health Organization estimates that approximately 14.1% of older adults live with a mental disorder such as depression or anxiety (World Health Organization, 2025), and subclinical psychosocial issues, including loneliness, cynical hostility, and community disorientation, occur at even higher rates and demonstrate notable persistence over time (Huxhold and Henning, 2023; Kotwal et al., 2021). Additionally, these symptoms tend to co-occur (Li and Bressington, 2019; Segel-Karpas and Ayalon, 2020). Recent evidence suggests that between 23% and 64% of older adults report two or more psychosocial symptoms, with higher rates observed among those with physical concerns (Polak-Szabela et al., 2025), a profile associated with more severe negative outcomes.
This nuance is particularly important in the context of public health crises, such as the Coronavirus disease (COVID-19) pandemic. Using the prevalence or severity of psychosocial symptoms as indicators, existing studies have suggested that the impact of the COVID-19 pandemic on older adults’ psychosocial well-being is either nonsignificant or notable. Research focusing on adaptive capacity proposes that pandemic-related disruption was moderated by older adults’ lifelong crisis-coping experiences, yielding unaltered mental well-being during the pandemic (Röhr et al., 2020) or rapid recovery after the pandemic, despite a temporary increase in symptoms (Carbone et al., 2021; Schäfer et al., 2023; Wettstein et al., 2023). In contrast, studies focusing on vulnerability suggest that heightened health anxieties and pandemic-related restrictions may have disrupted older adults’ adaptive strategies for emotion regulation and social integration, thereby exacerbating symptom severity (Dong et al., 2020; Klasen et al., 2025) during the pandemic, with symptoms either persistently deteriorating (Zaninotto et al., 2022) or only partially recovering (López et al., 2022) post-pandemic. However, evidence regarding the co-occurrence of these symptoms remains sparse and inconclusive. One study estimated that the prevalence of psychosocial symptoms increased to 70% in high-risk groups, with more than half reporting multiple co-occurring issues (Dong et al., 2020), but little is known about the post-pandemic situation. Whether the crisis was associated with a lasting reconfiguration of psychosocial well-being among older adults may have significant implications for long-term health trajectories and intervention strategies, warranting further investigation.
Generally, older adults’ psychosocial well-being is closely linked to their perceptions of aging, a construct comprising two interconnected dimensions: aging attitudes and perceived ageism (Allen et al., 2022; Freeman et al., 2016). Aging attitudes represents internalized perceptions of the self-aging process; negative aging attitudes may undermine motivation and resilience, thereby compromising psychosocial well-being (Lyons et al., 2018). Conversely, perceived ageism reflects the perception of external prejudice, stereotyping, or discrimination, which can exacerbate social disconnection and adversely affect psychosocial outcomes (Marquet et al., 2019). Previous studies have reported increases in negative aging perceptions and concurrent psychosocial symptoms during the pandemic (Seifert, 2021; Wahl et al., 2022), exacerbated by ageist narratives framing older adults as burdensome and uniquely vulnerable (Brinkhof et al., 2023). Accordingly, interventions targeting aging perceptions are regarded as a vital non-pharmacological approach to enhancing psychosocial well-being (Kang and Kim, 2022). However, whether the combination of internalized negative beliefs and heightened perceived ageism persists post-pandemic remains unclear. Furthermore, the relationship between these perceptions and psychosocial symptoms has yet to be fully elucidated, representing a significant gap in crisis management research regarding the utility of an aging-perception lens for psychosocial intervention.
Specifically, the relationship between aging perceptions and psychosocial well-being may shift across different phases of the pandemic. The Strength and Vulnerability Integration (SAVI) model posits that aging involves a dynamic integration of accumulating emotional strengths alongside increasing physiological and cognitive vulnerabilities (Charles, 2010). Under stable, low-stress conditions, older adults typically utilize cognitive-behavioral emotion regulation skills to maintain well-being (Sliwinski et al., 2021), often successfully leveraging emotional strengths despite negative aging perceptions. However, during sustained, high-arousal stressors, these vulnerabilities can override regulatory capacities (Charles and Piazza, 2024). Under such conditions, negative aging perceptions as a critical cognitive-emotional vulnerability may undermine the effective integration of age-related strengths, thereby amplifying multiple psychosocial symptoms (Freeman et al., 2016) or triggering the onset of novel, complex symptom clusters (Banerjee et al., 2020). While a return to lower-arousal conditions post-pandemic might facilitate recovery (Charles and Piazza, 2024), individuals with entrenched negative aging attitudes may fail to reintegrate strengths, resulting in the persistence of complex co-occurrence patterns of psychosocial symptoms (Losada-Baltar et al., 2021). One study observed a shift toward more negative aging perceptions but relatively stable psychosocial well-being among older adults during the pandemic (Wettstein et al., 2023). However, empirical evidence capturing how these co-occurrence patterns evolve across and after the pandemic remains limited.
Furthermore, the co-occurrence patterns of aging perceptions and psychosocial symptoms across the pandemic may vary by gender. The SAVI model acknowledges that vulnerabilities and strengths are shaped by socio-contextual factors (Charles, 2010). While both men and women experience ageism, the manifestations and psychological reactions differ significantly due to the interplay of gendered stereotypes and societal expectations (Chopik and Giasson, 2017). Older women often internalize ageism as self-devaluation, intensifying their risk for internalizing symptoms such as depression and anxiety. Conversely, men may perceive ageism as a threat to competence, reinforcing ties to externalizing symptoms like cynical hostility. Beyond these psychological reactions, women typically maintain larger, more diverse social networks for emotional support, whereas men often rely primarily on immediate family (Antonucci and Akiyama, 1987). Pandemic stressors may have disrupted these gendered coping strategies differently, yielding divergent symptom clusters (Vlachantoni et al., 2022). Despite growing evidence documenting gender differences in the onset of negative aging perceptions and psychosocial symptoms (Hossain et al., 2020; Moradi et al., 2021), along with one study noting a more diverse and intense symptom overlap for older women during the pandemic (Dlamini, 2021), few studies have tracked how these patterns actually shifted across different phases of the crisis. It is essential to uncover these dynamics to develop gender-sensitive interventions that effectively foster psychosocial resilience during and after public health crises.
Aims and hypothesis
This study aims to systematically investigate the dynamic linkage patterns between negative aging perceptions (comprising negative aging attitudes and perceived ageism) and nine psychosocial symptoms among older adults across different phases of the pandemic, with a particular emphasis on potential gender differences. The findings are expected to enhance our understanding of the role of aging perceptions in shaping psychosocial well-being and inform the development of more context-specific, gender-sensitive interventions for crisis management.
Grounded in the SAVI model, we hypothesize that the co-occurrence of negative aging perceptions and psychosocial symptoms will be more diverse and complex during the pandemic. In the post-pandemic phase, these patterns may either persist, return to pre-pandemic levels, or become even more complex. Additionally, we hypothesize that older women and men will differ in how these perceptions and symptoms cluster, with women showing more complex psychosocial patterns anchored by negative aging perceptions.
Methods
Data sources and sample design
Data for this study were drawn from the Health and Retirement Survey (HRS), a nationally representative longitudinal survey that conducts biennial interviews with approximately 20,000 individuals aged 50 and older in the United States. Since its inception in 1992, the HRS has comprehensively assessed health conditions, physical functioning, and psychosocial traits, including attitudes and preferences. In 2006, the HRS expanded its protocol to include a self-administered psychosocial and lifestyle questionnaire following enhanced in-person interviews. Notably, this psychosocial questionnaire employs a rotating panel design in which a random 50% subsample of the longitudinal panel is surveyed in each wave (Weir, 2017). Rather than surveying the same individuals in consecutive biennial waves, this design rotates the subsample, meaning that psychosocial measures for specific individuals are collected every 4 years. Consequently, this study utilized data from before (2018), during (2020) and after (2022) the pandemic, treating these waves as repeated cross-sectional samples. This analytical approach facilitated the identification of shifts in co-occurrence patterns at the population level, allowing for an examination of how these patterns varied across distinct historical contexts rather than tracking individual symptom trajectories over time.
The response rates for the psychosocial assessments were 61.8%, 64.7% and 61.9% for the 2018, 2020, and 2022 waves, respectively. After excluding individuals with incomplete assessments or those below the age limits, the final sample consisted of 5688 individuals in 2018, 4587 in 2020, and 4377 in 2022. All participants provided written informed consent prior to enrollment. The HRS was approved by the University of Michigan Health Sciences Institutional Review Board (HUM00061128). Because this study utilized publicly available, de-identified data, additional ethical approvals were waived.
Measures
Psychosocial symptoms include nine items selected based on the Stress and Coping Paradigm (Lambert and Lazarus, 1970), which distinguishes between immediate stress responses and enduring susceptibility factors that influence long-term adaptation. Following established literature (Endler, 1997; Roberts et al., 2007; Wolters et al., 2023), anxiety, depressive, and stress symptoms serve as primary stress response indicators, representing immediate emotional and physiological reactions during times of crisis. Stress susceptibility indicators are further divided into cognitive and attitudinal patterns (e.g. cynical hostility, pessimism, hopelessness, and loss of control) that reflect internal cognitive schemas that can exacerbate distress, and social/environmental perceptions (e.g. loneliness and community disorientation) that reflect disruptions in social connectedness. Collectively, these constructs provide a comprehensive assessment of how individuals experience and navigate acute or chronic stressors.
Depressive symptoms were measured using the modified 8-item Center for Epidemiological Studies Depression Scale (CES-D), which identifies individuals at risk of depression and has psychometric properties comparable to the original 20-item version (Steffick, 2000). The total score ranges from 0 to 8, with a cut-off of ⩾4 used to indicate the presence of depressive symptoms (Turvey et al., 1999). The Cronbach’s α for the CES-D was 0.795 for the 2018 sample, 0.793 for 2020, and 0.791 for 2022.
Anxiety was assessed using a five-item subscale from the Beck Anxiety Inventory (BAI), featuring items such as “fear of the worst happening” and “nervous.” Participants rated symptom frequency from 1 (never) to 4 (most of the time). Total scores were summed, with a cut-off of ⩾12 indicating elevated anxiety (Gould et al., 2015). Internal consistency was robust across all waves (2018: Cronbach’s α = 0.815; 2020: Cronbach’s α = 0.814; 2022: Cronbach’s α = 0.823).
Stress symptoms were evaluated using the 10-item Perceived Stress Scale (PSS; Cohen et al., 1983). Respondents rated both negative (e.g. “felt nervous and stressed”) and positive (e.g. “felt things were going the way”) feelings from 0 (never) to 4 (very often). After reverse-coding positive items, total scores were computed. A score of ⩾14 identified individuals with elevated stress (Cohen et al., 2019). Cronbach’s α were 0.851, 0.846, and 0.844 for 2018, 2020, and 2022, respectively.
Cynical hostility was assessed with five items from the Cook-Medley Hostility Inventory (Costa et al., 1986). Statements (e.g. “people would lie to get ahead”) were rated from 1 (strongly disagree) to 6 (strongly agree). In accordance with standard protocols, data were treated as missing if three or more items were unanswered; an index was then created by averaging the scores, with a threshold of ⩾4 indicating cynical hostility (Hackett et al., 2015). Internal consistency ranged from Cronbach’s α = 0.780 (2018) to 0.807 (2020) and 0.797 (2022) across waves.
Pessimistic outlooks were evaluated with a 6-item version of the Life Orientation Test (Scheier et al., 1994). Participants rated three optimism and three pessimism items from 1 (strongly disagree) to 6 (strongly agree). Following the reverse-coding of optimism items, scores were averaged to represent overall pessimism. A cut-off of ⩾4 defined a pessimistic outlook and missing value were set if more than one item was unanswered (Scheier and Carver, 2018). Cronbach’s α for this scale was 0.714 for the 2018 sample, 0.715 for 2020, and 0.704 for 2022.
Hopeless feeling was assessed using a 4-item scale combining measures from Everson et al. (1997) and Beck et al. (1974). Items (e.g. “impossible to reach the goal”) were rated from 1 (strongly disagree) to 6 (strongly agree). Averaged scores of ⩾4 identified elevated hopelessness (Mitchell et al., 2020). The scale demonstrated high internal consistency across waves (2018: Cronbach’s α = 0.859; 2020: Cronbach’s α = 0.846; 2022: Cronbach’s α = 0.847).
Loneliness was assessed with the 3-item revised UCLA Loneliness Scale, which measures feelings of being left out, isolated, or lacking companionship (Perissinotto et al., 2012). Participants were categorized as experiencing elevated loneliness if they reported these feelings “Some of the time” for at least two items, or “Often” for one or more items. Cronbach’s α for this scale was 0.809 for the 2018 sample, 0.796 for 2020, and 0.801 for 2022.
Community disorientation describes social distrust toward one’s neighborhood using four items (e.g. “feel part of this area”; Robinette et al., 2018). Response (on a 1-to-7 scale) were reverse-coded and averaged, and scores of ⩾4 denoted community disorientation. The scale demonstrated high internal consistency across waves (2018: Cronbach’s α = 0.858; 2020: Cronbach’s α = 0.866; 2022: Cronbach’s α = 0.850).
Loss of control was measured with five items (e.g. “feeling helpless in dealing with the problems of life”) assessing perceived personal mastery and constraint (Lachman and Weaver, 1998). Agreement was rated on a 6-point scale, and averaged scores of ⩾4 identified an elevated sense of loss of control (Crosswell et al., 2020). Cronbach’s α were 0.855, 0.867, 0.853 across the three waves.
Negative aging attitudes was assessed using an 8-item scale combining five items from the Philadelphia Geriatric Center Morale Scale (Lawton, 1975) and three items from the Berlin Aging Study. Participants rated their agreement with four negatively framed statements (e.g. “the older I get, the more useless I feel”) and four positively framed statements (e.g. “I have as much as pep as I did last year”) on a 6-point scale (1 = strongly disagree to 6 = strongly agree). After reverse-coding positive items, a mean score was computed, with higher scores representing more negative attitudes. Following Sargent-Cox et al. (2012), a cutoff of ⩾4 was used to identify individuals with negative aging attitudes. Data were treated as missing if more than four items were unanswered. Internal consistency was acceptable across all waves (2018: Cronbach’s α = 0.723; 2020: Cronbach’s α = 0.716; 2022: Cronbach’s α = 0.720).
Perceived ageism was assessed using a 6-item scale designed to capture experiences of age-based discrimination (Williams et al., 1997). Respondents reported the frequency of daily discrimination (e.g. being “treated with less courtesy”) on a scale from 1 (almost every day) to 6 (never). After reverse-coding, individuals were categorized as having experienced discrimination if they reported such occurrences “a few times a month” or more for at least two items, or “at least once a week” or more for at least one item. Among these respondents, only those who specifically attributed these experiences to age were classified as perceiving ageism (Williams et al., 1997). Cronbach’s α for this scale was 0.823 for the 2018 sample, 0.826 for 2020, and 0.830 for 2022.
Covariates in this study included several sociodemographic and health-related variables, based on their established associations with aging attitudes and psychosocial well-being (Velaithan et al., 2024; Zach et al., 2021). Sociodemographic variables included gender (male/female), age, race (White/Black/Others), marital status (married or partnered/single) and education level (less than high school vs higher school or above). Household wealth was categorized into three tiers: relatively poor, medium and relatively rich. Additionally, physical limitations were assessed via difficulties in Activities of Daily Living (ADLs), including bathing, eating, dressing, walking across a room and getting in/out of bed. ADL disability was treated as a binary variable (none vs one or more difficulties).
Statistical analyses
Descriptive statistics were calculated for each wave, with categorical variables presented as percentages and continuous variables reported as means with standard deviations (SD). The prevalence of negative aging attitudes, perceived ageism, and psychosocial symptoms was estimated alongside 95% confidence intervals (CIs). To assess differences in sample characteristics across the pre-pandemic (2018), pandemic (2020), and post-pandemic (2022) periods, Pearson’s chi-square (χ2) tests were employed for categorical variables, using Cramer’s V as the measure of effect size. For continuous variables, one-way analysis of variance (ANOVA) was used, with eta-squared (η2) reported as the effect size. Following established conventions (Kim, 2017; Lachenbruch and Cohen, 1989), Cramer’s V < 0.1 and η2 < 0.01 were utilized to identify negligible associations. These criteria were applied to ensure that any observed shifts in psychosocial co-occurrence patterns were not primarily driven by compositional changes in the repeated cross-sectional samples.
To explore the interrelationships among the studied variables, association rule mining (ARM) was employed. ARM is an exploratory, data-driven analytical technique designed to identify frequently co-occurring patterns within large datasets without imposing a predefined dependent-independent variable structure (Agrawal et al., 1993). In health and social science research, ARM is increasingly used to uncover complex symptom clusters and multimorbidity patterns that traditional regression-based approaches may not adequately capture. Unlike hierarchical methods, ARM treats symptoms and perceptions symmetrically, reflecting the reality that psychosocial experiences and aging perceptions often develop and interact concurrently among older adults. Specifically, the estimation used the Apriori algorithm, evaluating association rules through three key indicators: support, confidence and lift. Support represents the joint probability of both the antecedent (A) and the consequent (B) appearing in the dataset. Confidence denotes the conditional probability of B occurring given the presence of A. Lift measures the strength of the association by comparing observed co-occurrence with the expected frequency by chance. A lift value > 1.0 indicates a positive association between the items.
In the first step, ARM was conducted for the pre-pandemic, pandemic, and post-pandemic samples. As universal thresholds for these metrics are not established, parameters were refined iteratively. We initially set the minimum support at 10%, minimum lift at 1.0, and minimum confidence at 30%. To ensure the reliability of the associations and exclude potential pseudo-rules, the minimum confidence threshold was increased in 5% increments to a final level of 70% (Wang et al., 2021). Furthermore, the minimum support threshold was adjusted to 15% to prioritize the most prevalent and clinically relevant itemset. In the second step, the analysis was stratified by gender, utilizing the finalized thresholds (support ⩾ 15%, lift > 1.0, confidence ⩾ 70%).
All descriptive and comparative analyses were performed using SPSS version 17.0, while ARM was executed via SPSS Modeler utilizing the Apriori algorithm.
Results
Table 1 shows the descriptive characteristics of the study samples across the three pandemic phases. Overall, the samples exhibited high comparability in demographic, socioeconomic, and functional characteristics. Gender composition remained stable across periods (χ2 = 0.23, p = 0.890), with women making up approximately 60% of each sample. Similarly, no significant differences were observed in racial composition (χ2 = 1.84, p = 0.764) or the prevalence of ADL difficulties (χ2 = 2.60, p = 0.107). Although mean age varied significantly across waves (2018: M = 67.97; 2020: M = 68.99; 2022: M = 68.76; F = 12.24, p < 0.001), the associated effect size was negligible (η2 = 0.002). While marital status, educational attainment, and household wealth reached statistical significance (all p < 0.05), their effect sizes were also very small (Cramer’s V ⩽ 0.02), reflecting minimal variation across periods.
Descriptive characteristics of the surveyed sample before, during and after the pandemic.
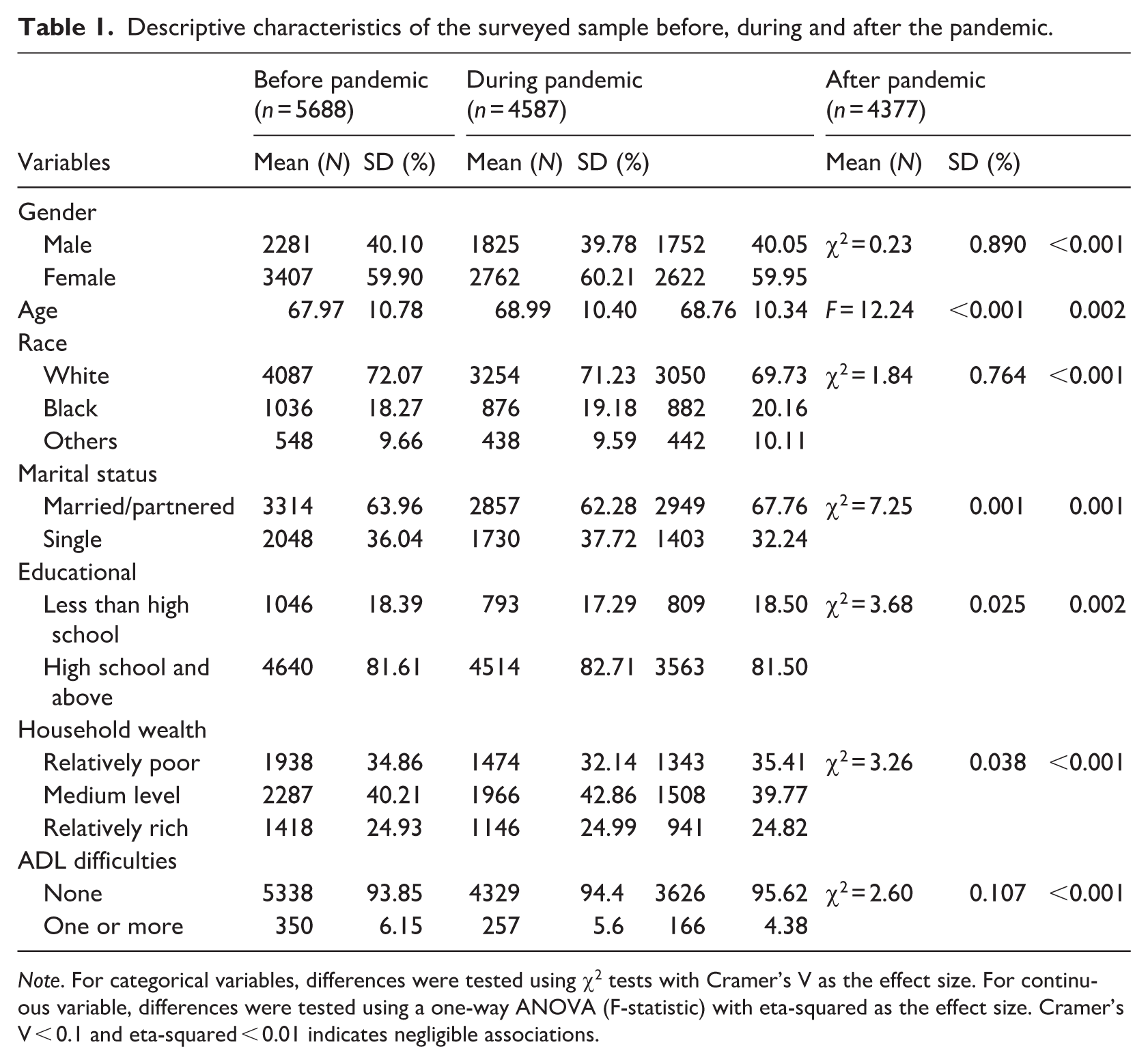
Note. For categorical variables, differences were tested using χ2 tests with Cramer’s V as the effect size. For continuous variable, differences were tested using a one-way ANOVA (F-statistic) with eta-squared as the effect size. Cramer’s V < 0.1 and eta-squared < 0.01 indicates negligible associations.
Figure 1 illustrates the stability of symptom prevalence among older adults across the pandemic. Loneliness and stress were the most common challenges, consistently affecting approximately 40%–55% of the sample, respectively. Notably, internalized negative aging attitudes (20%–22%) were substantially more prevalent than the perception of external age-based discrimination (5%–7%). While several symptoms including cynical hostility, pessimism outlooks, and hopeless feelings showed detectable increases during the pandemic followed by a post-pandemic decline, other indicators such as anxiety, loss of control and community disorientation remained relatively stable.
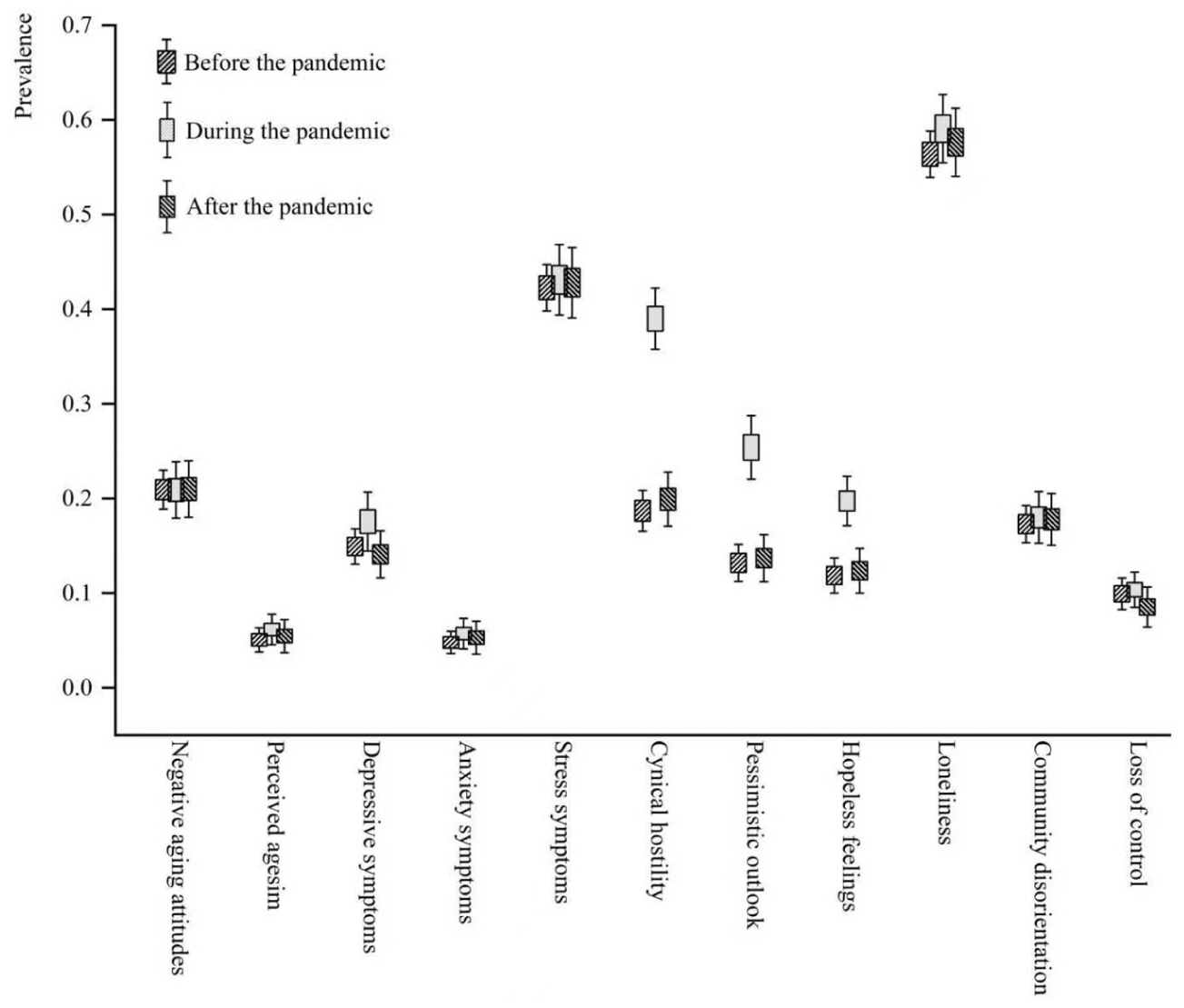
Prevalence of negative aging thoughts and mental health symptoms among older adults before, during, and after the pandemic (95% CI).
Figure 2 illustrates the association rule mining results for psychosocial symptoms and aging perceptions before, during and after the pandemic, indicating that while overall symptom rates remained stable, these symptoms intertwined in increasingly numerous and complex ways during and after the pandemic. Prior to the pandemic, co-occurrence patterns were relatively sparse (n = 13) and primarily involved isolated symptoms with limited cross-domain clustering. During the pandemic, these structures became more diverse (n = 20) and complex. Stress and loneliness emerged as central nodes around which multiple psychosocial symptoms and negative aging perceptions clustered. Notably, depressive symptoms, pessimistic outlook, hopeless feelings, and community disorientation appeared as isolated experiences in pre-pandemic data but were identified as frequently co-occurring clusters during the pandemic. In the post-pandemic period, stress and loneliness, particularly their joint occurrence, remained embedded in co-occurrence structures alongside negative aging perceptions and emotional symptoms (n = 23). This sustained structural complexity indicates a shift toward a wider variety of ways in which negative aging attitudes and psychosocial symptoms cluster, a pattern established during the pandemic and maintained afterward.
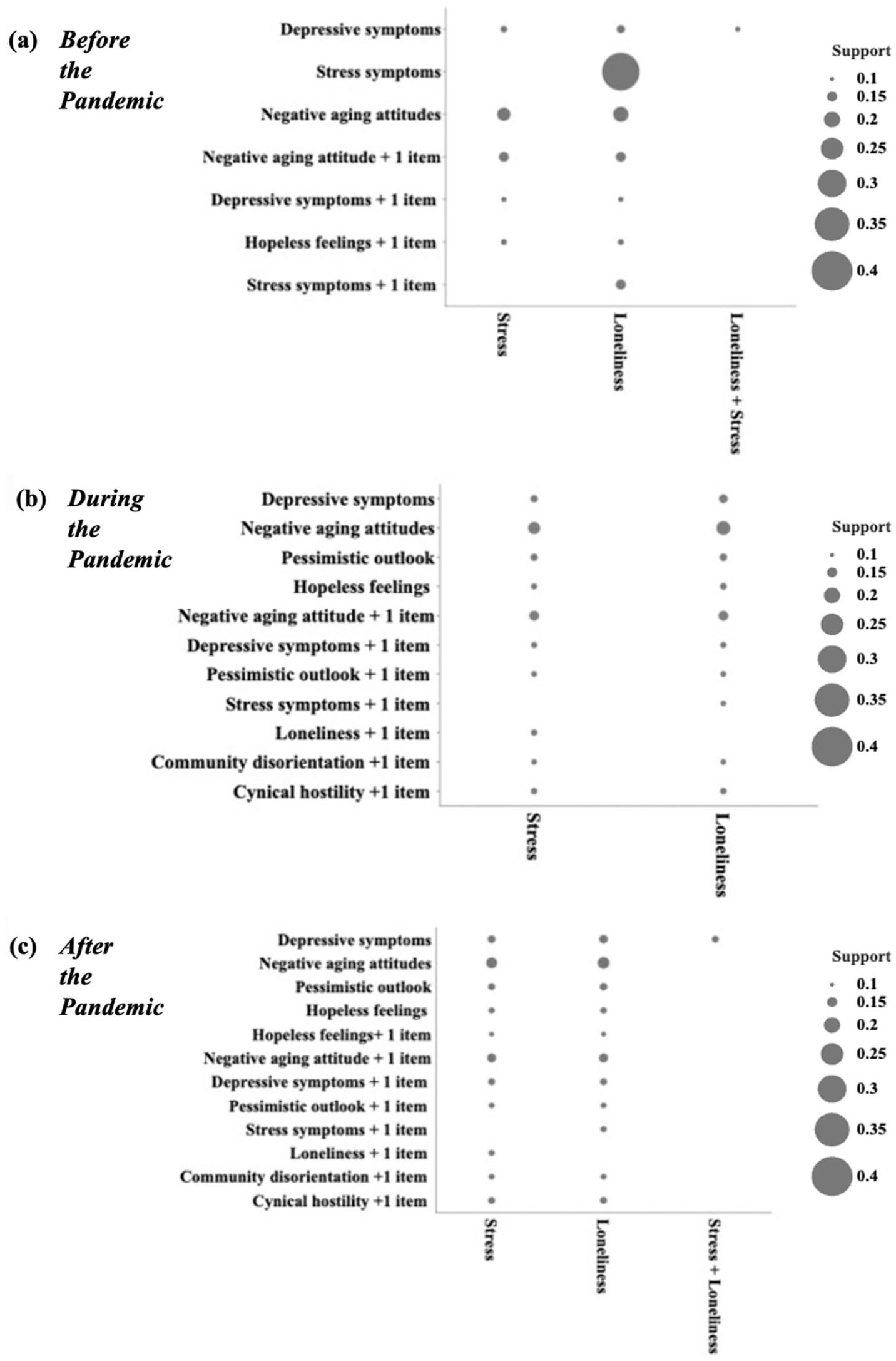
Associations between aging attitudes and mental health symptoms of older adults before, during and after the pandemic (Support > 0.1, Coefficient > 0.7).
Table 2 details the high-impact association rules, highlighting an intensification and stabilization of the linkages between negative aging attitudes and psychosocial symptoms across the study period. Before the pandemic, negative aging attitudes associated significantly with both stress symptoms (support = 0.238; lift = 1.487) and loneliness (support = 0.185; lift = 1.218). These associations typically involved single-item rules, reflecting relatively simple co-occurrence structures. During the pandemic, these patterns became more complex. In addition to stable dyadic associations, multi-item rules emerged wherein negative aging attitudes, in combination with either stress or loneliness, frequently co-occurred with the other symptom. These rules exhibited high confidence and elevated lift, suggesting strong interconnectedness among these factors during the pandemic phase. After the pandemic, these multi-item patterns remained evident, highlighting the positioning of negative aging attitudes as a central node in psychosocial symptom networks. Furthermore, depressive symptoms emerged as a novel co-occurring factor associated with loneliness, suggesting a post-pandemic pattern wherein prolonged distress and depressive symptoms co-occurred alongside social isolation for a subset of older adults.
Association rules showing aging attitude and mental health relationships among older adults before, during, and after the pandemic (Support > 0.15, Coefficient > 0.7).
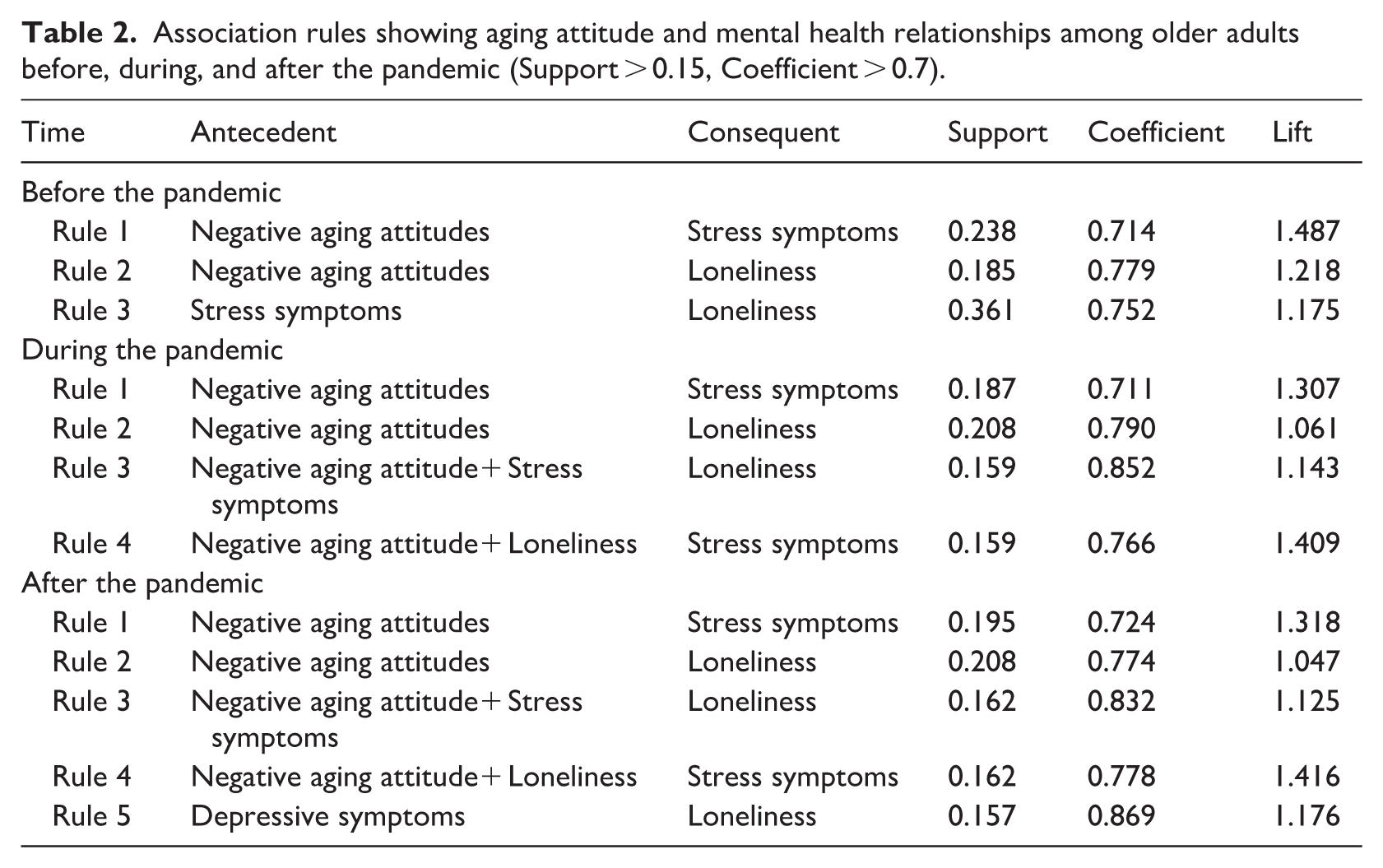
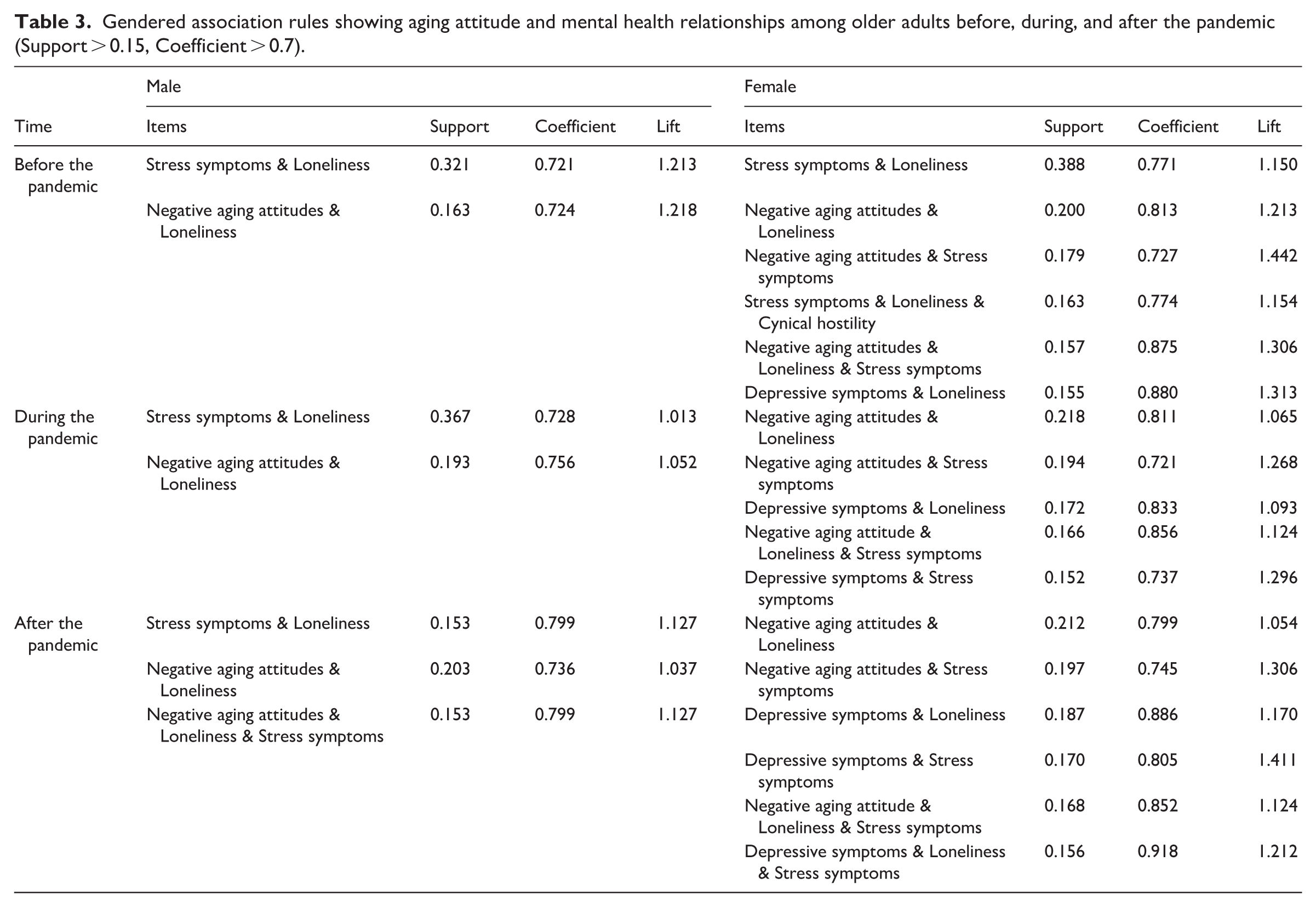
Figure 3 illustrates the gender-specific ARM results, revealing consistently greater complexity and more diverse symptom clusters among older women than men across all pandemic periods. Notably, depressive symptoms emerged as a central, highly connected node within women’s networks during and after the pandemic. While women’s symptom patterns exhibited substantial restructuring in response to the crisis, men’s patterns remained relatively stable and sparse. Table 3 further details the specific rules for both groups, confirming that older women experienced more frequent and diverse co-occurrence patterns linking negative aging attitudes and psychosocial symptoms. Before the pandemic, women’s profiles included six significant rules, whereas only two were identified for men. During the pandemic, women exhibited complex, multi-symptom clusters (e.g. three-item combinations) that were absent in the male profiles. Meanwhile, a critical distinction emerged regarding the role of internalizing symptoms. Rules featuring depressive symptoms in combination with loneliness or stress were present for women across all three periods, demonstrating high confidence (0.737–0.918) and meaningful lift (1.093–1.411). Conversely, depressive symptoms did not appear in any significant association rules for men. These results suggest that for older women, negative aging attitudes are more deeply integrated into a multifaceted network of emotional and social distress, a pattern that became more pronounced during the pandemic.
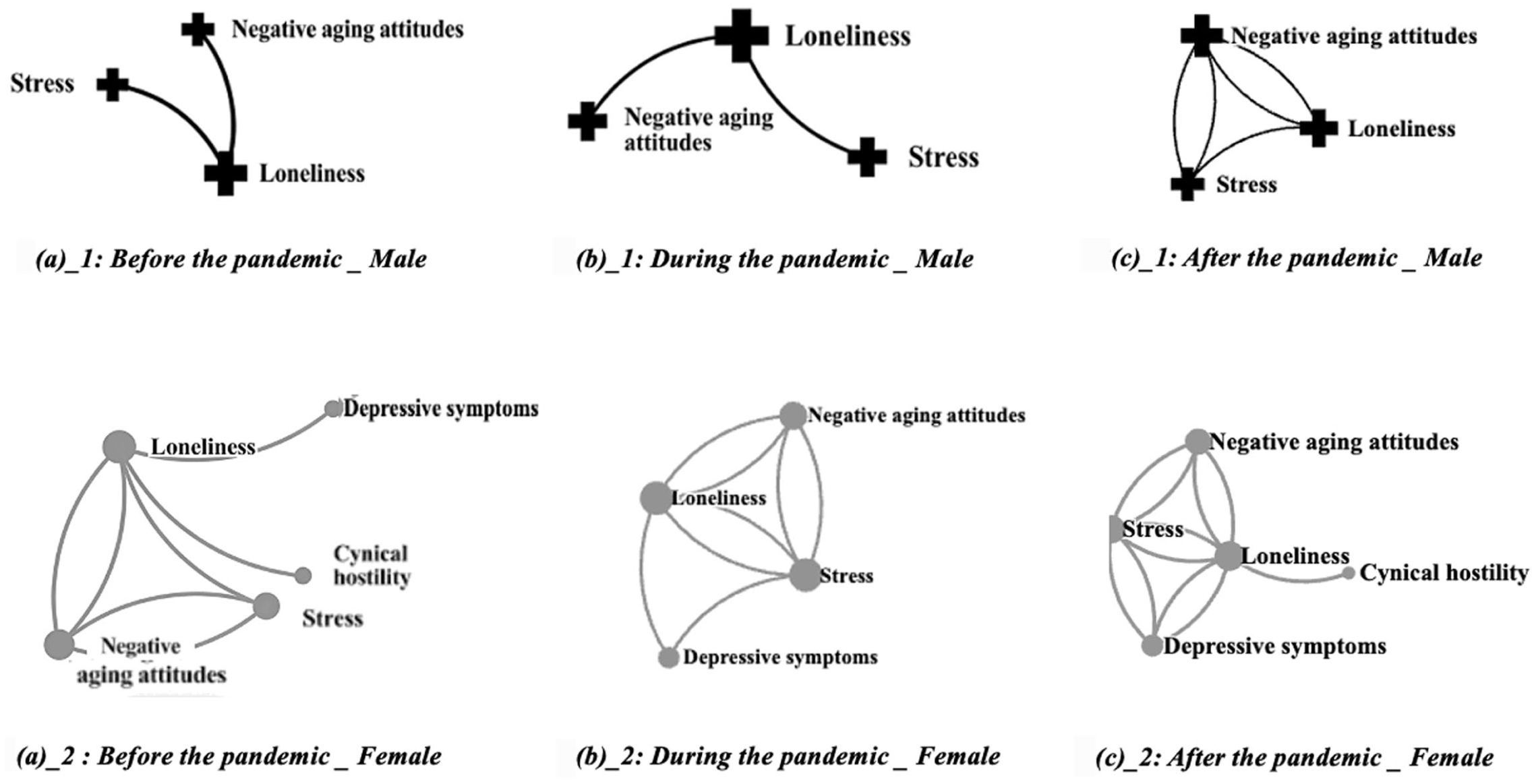
Gendered associations between aging attitudes and mental health symptoms among older adults before, during and after the pandemic (Support > 0.15, Coefficient > 0.7).
Gendered association rules showing aging attitude and mental health relationships among older adults before, during, and after the pandemic (Support > 0.15, Coefficient > 0.7).
Discussion
This study is among the first to investigate the co-occurrence patterns of negative aging perceptions and psychosocial symptoms among older adults throughout the pandemic, with a particular focus on gender-specific variations. Utilizing repeated cross-sectional data from over 13,000 observations, the findings indicate that despite a temporal increase in cynical hostility, pessimism, and hopelessness during the pandemic, the overall prevalence of negative aging perceptions and psychosocial symptoms remained relatively stable, with stress symptoms and loneliness being the most prevalent. However, the co-occurrence patterns demonstrated significant structural changes. During and after the pandemic, older populations exhibited more diverse and complex patterns, with negative aging attitudes evolving into a central node within psychosocial networks in the post-pandemic stage. This shift was particularly pronounced among older women, who showed higher prevalence of such co-occurring negative aging attitudes and psychosocial symptoms than their male counterparts, with patterns that frequently centered on depressive symptoms. By employing ARM, this study moves beyond traditional single-symptom prevalence analyses to capture how negative aging perceptions and psychosocial symptoms cluster synergistically. This configuration-based perspective offers a novel understanding of psychosocial vulnerability in the aftermath of crises. Several findings warrant further discussion.
First, this study reveals a notable pattern of psychosocial resilience among the older adult population. While symptoms including cynical hostility, pessimism outlooks, and feelings of hopelessness showed a temporary increase during the acute phase of the pandemic, their prevalence largely returned to pre-pandemic baseline levels by 2022. This finding underscores the robust adaptive capacity of older adults and aligns with theories of emotional resilience in later life (Diehl et al., 2014; Wettstein et al., 2023). However, this general recovery stands in contrast to the persistent and pervasive loneliness and stress symptoms. As noted, loneliness consistently affected nearly 60% of participants, while stress remained elevated (over 40%) across all three waves. These estimates align with recent large-scale surveys (Ansari and Kang, 2019; Cigna, 2020) and highlight that these two symptoms are not merely transient responses to a crisis but enduring systemic challenges. Moreover, as central nodes in psychosocial symptom clusters, loneliness and stress may act as foundational elements for the exacerbation of more severe comorbidities, increasing the long-term risk of physical and mental health decline. In addition, our findings highlight the acute emerge of cynical hostility, pessimistic outlooks, and feelings of hopelessness during the height of the pandemic. While prior studies have typically focused on disorders like depression or anxiety (Rosenberg et al., 2021; Webb and Chen, 2022), our study suggests that these subclinical affective states represent critical markers of vulnerability. Therefore, we advocate for the integration of subclinical monitoring into emergency response protocols. Routine screening for hostility and pessimism during public health emergencies could facilitate early intervention, mitigating the erosion of well-being and preventing potential escalation. Moreover, given the enduring loneliness and stress challenges, public health policies should shift from reactive crisis management toward sustained community programs designed to foster social connectivity and reduce chronic stress.
Second, this study reveals that the co-occurrence of negative aging attitudes and psychosocial symptoms became more prevalent, diverse and complex during the pandemic, and persisted post-pandemic. In line with prior research (Campagne, 2019), we identified predominant concurrent loneliness and stress symptoms before the pandemic, but found negative aging attitudes emerged as a frequently co-occurring element within broader symptom clustering in later phases. This pattern is consistent with the SAVI model (Charles, 2010), which posits that negative aging attitudes may serve as a cognitive-emotional vulnerability factor. Under the weight of a sustained crisis, this vulnerability may disrupt the integration of age-related strengths, neutralizing the regulatory processes that older adults typically use to maintain emotional well-being. This disruption could initiate a self-reinforcing cycle of distress, preventing individuals from restoring their psychosocial well-being and regaining a functional strength-vulnerability balance post-crisis. Interestingly, our findings suggest a divergence between internalized and externalized aging perceptions. Contrary to prior research (Ribeiro-Gonçalves et al., 2023), perceived ageism as an external stressor exhibited weaker associations with psychosocial clusters than internal negative aging attitudes. This suggests that external ageism may be cognitively appraised differently; it may mobilize compensatory coping efforts or protective social identification rather than being internalized (Kahlor et al., 2002). Conversely, the prolonged stress of the pandemic appears to coincide with weakened internal emotional regulation, allowing internalized negative aging attitudes to dominate the psychosocial symptom networks. Consequently, it is reasonable to conclude that prolonged pandemic stress coincided with more complex co-occurrence patterns between negative aging attitudes and psychosocial symptoms, suggesting that interventions addressing both negative aging attitudes and psychosocial distress simultaneously may be beneficial for older adults’ well-being during and after crises.
Third, this study indicates that older women exhibited higher prevalence and complexity in the co-occurrence of negative aging attitudes and psychosocial symptoms, with these patterns shifting more frequently across the pandemic. This aligns with evidence documenting gendered differences in psychosocial distress profiles (Pinquart and Sorensen, 2001; Zuckerman et al., 2017), and extends it by showing that the co-occurrence structure of negative aging attitudes and psychosocial symptoms became particularly dense for older women under pandemic threats. Specifically, while contemporary societal attitudes toward aging may appear virtually equivalent for men and women (Shakeri and North, 2025), older women remain more likely to internalize these perceptions as a threat to self-concept and experience concurrent psychosocial distress (Johnson and Whisman, 2013). Notably, depressive symptoms were a central, highly connected node exclusively within the female group, particularly during and after the pandemic. This is consistent with prior evidence that internalizing tendencies, including depressive symptoms, are more commonly observed among older women under stress (Shrira et al., 2020). Therefore, our findings suggest that interventions aimed at post-crisis psychosocial recovery should be gender-sensitive, with a prioritized focus on identifying and addressing depressive symptoms in older women who present with negative aging attitudes.
Strength and limitations
This study, utilizing novel empirical evidence collected before, during, and after the pandemic, reveals that the co-occurrence of negative aging attitudes and psychosocial symptoms became more prevalent, diverse, and complex during the pandemic and persisted afterward, with loneliness and stress symptoms being the most dominant elements. Additionally, older women were exposed to more diverse and intense concurrent symptoms across the pandemic, with depressive symptoms being frequently observed. These findings shed light on the dynamics of the co-occurrence of negative aging attitudes and psychosocial symptoms, offering valuable insights for promoting psychosocial well-being in public crisis contexts.
However, several limitations should be acknowledged. First, the use of repeated cross-sectional data allowed for population-level comparisons across pandemic stages but precluded the assessment of within-person change. Although sociodemographic characteristics remained consistent across waves, unobserved heterogeneity including personality traits and cognitive abilities may have influenced aging perceptions and psychosocial outcomes. Furthermore, utilizing a single pre-pandemic wave (2018) as a baseline limits the ability to distinguish whether the shifting co-occurrence patterns in 2020 and 2022 were uniquely triggered by the pandemic or represented an acceleration of longitudinal trends already in motion. Future research incorporating multiple pre-pandemic data points and a broader array of control variables is necessary to establish a more robust trajectory of these effects. Second, the study focused exclusively on adults aged 60 and older, without a younger comparison group. Consequently, we cannot determine whether the observed co-occurrence patterns are age-specific phenomena or reflect general stress reactions prevalent across the life span. Comparative designs across different age cohorts would help elucidate the extent to which these configurations are unique to the developmental context of later life. Finally, the assessment of psychosocial symptoms relied on short forms of self-reported measures, which may be subject to recall and social desirability biases. Future research incorporating clinical evaluations or multi-informant assessments would enhance the psychometric validity of these findings and provide a more nuanced understanding of the symptom clusters identified.
Conclusion
This study explored the co-occurrence patterns of negative aging perceptions and psychosocial symptoms among older adults across the pandemic, identifying significant gender differences. The findings indicate that the pandemic was associated with a restructuring of older adults’ psychosocial well-being, offering valuable insights for public health crisis management. We urge public health practitioners and policymakers to recognize the increasingly prevalent, diverse, and complex co-occurrence of negative aging attitudes and psychosocial symptoms during and after such crises, with older women being prioritized in targeted interventions.
Footnotes
Ethical considerations
All respondents gave written informed consent prior to participation, and the survey was approved by the University of Michigan Health Sciences Institutional Review Board (HUM00061128). As this study utilized publicly available, de-identified data, additional ethnic approvals were waived.
Consent to participate
For the 2018 and 2022 wave of the HRS, all respondents gave written consent. For the 2020 wave of HRS, all respondents gave oral consent due to pandemic restrictions.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Author contributions
Mingqi Fu: Methodology, Formal Analysis, Writing—original draft; Hao Kang, & Xiaorui Huang: Writing—review and editing; Jing Guo: Conceptualization, Writing—review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Hunan Federation of Social Sciences (XSP24YBZ031).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The original data was from Health and Retirement Survey at https://hrs.isr.umich.edu/data-products. Data and codes particularly used in the current study was reposited in ![]() . All information is available through request to the corresponding author.*
. All information is available through request to the corresponding author.*