
Abstract
Postpartum psychosis (PP) is a severe psychiatric disorder affecting 1 to 2 per 1000 births. While effective treatments are available, barriers to treatment and recovery persist. This analysis aims to deepen understanding of recovery support across sociocultural contexts. Participants were individuals enrolled in the Massachusetts General Hospital Postpartum Psychosis Project who completed an open-text follow-up survey on recovery experiences. Data included 131 responses to the question addressing how to best support those experiencing PP. A qualitative content analysis guided by the Socio-Ecological Model (SEM) was performed. Key themes, including the importance of self-acceptance, support systems, provider education, improved clinical practices, and reducing stigma, were mapped onto the levels of the SEM. Applying SEM to the analysis not only highlights individual experiences but also examines the systemic factors influencing PP recovery. Findings provide a framework for future multi-level, theory-driven approaches to facilitate recovery for individuals with PP.
Introduction
Postpartum psychosis (PP) is a severe perinatal psychiatric disorder affecting approximately 0.86 to 2.6 per 1000 births (VanderKruik et al., 2017). Typically presenting within the first 2 weeks postpartum, PP is characterized by a range of psychotic symptoms, including hallucinations, delusions, and an impaired sense of reality (Cohen et al., 2025). These symptoms can emerge abruptly and have profound consequences for the individual, their infant, and their broader support network. Without timely and adequate treatment, PP can lead to long-lasting psychological and social impacts, including strained relationships, impaired maternal-infant bonding, and increased risk of harm to self or infant (Alford et al., 2025).
The recovery process for PP is complex, often requiring pharmacological treatment and possibly hospitalization, as well as other psychosocial supports and information for the entire family unit (Heron et al., 2012; Roxburgh et al., 2023). Research indicates that individuals often face significant barriers to accessing timely and effective care, including logistical challenges such as childcare, transportation, and the stigma surrounding mental illness (Alford et al., 2025; Doucet et al., 2012). Many individuals report feeling unheard or misunderstood by healthcare providers who do not have a specialty in treating perinatal psychiatric disorders, further compounding feelings of isolation and mistrust of the healthcare system (Doucet et al., 2012). Facilitators of recovery, on the other hand, include strong social support networks, empathetic care from providers, and access to high-quality mental health services (Forde et al., 2020; Heron et al., 2012). Nonetheless, recovery experiences remain highly variable (Vanderkruik et al., 2024), underscoring the need for a deeper understanding of the factors that influence these trajectories.
Qualitative research offers a valuable approach to bridging this knowledge gap pertaining to a broader understanding of factors that could facilitate recovery from PP. By capturing the lived experiences of individuals affected by PP, qualitative methods can provide insights into the non-quantifiable aspects of the condition, such as emotional challenges, social dynamics, and cultural influences on care-seeking behaviors (Bhangu et al., 2023). Existing qualitative studies, primarily conducted in the United Kingdom (UK), have shed light on aspects of PP including barriers to care, strain on social networks, and effective care strategies (Holford et al., 2018). However, these studies have relatively small samples and are based in a country with a National Healthcare System (NHS) in contrast to our study population which assesses how the experience of PP can be affected in a country with a healthcare system that is predominantly privatized (Davis et al., 2019; Glover et al., 2014; Kobylski et al., 2024; Roxburgh et al., 2023). Mental health is a leading cause of maternal mortality and morbidity especially during postnatal care in the United States (US) and is critical to assess how recovery differs across contexts of different nations and healthcare systems (Davis et al., 2019; Papanicolas et al., 2024). This study addresses such barriers/facilitators in a much larger sample size than other studies and specifically addresses these barriers/facilitators in a geographically diverse population across the US. This study also addresses the generalizability gap when considering most studies occur in the UK which has a public health care system and by expanding the sample size to the US, we can better understand the differences in barriers/facilitators in a private healthcare system. (Davis et al., 2019; Kobylski et al., 2024; Roxburgh et al., 2023, 2025). There is an opportunity to expand on existing qualitative research on PP with the aim of understanding how to support recovery effectively while considering a range of sociocultural contexts.
The Socio-Ecological Model (SEM) provides a robust framework for deepening our interpretation of this qualitative research on PP. Widely utilized in public health, the SEM emphasizes the interplay of multiple levels of influence on health outcomes, including intrapersonal (microsystem), interpersonal (mesosystem), community (exosystem), and societal/policy (macrosystem) factors (Bronfenbrenner and Morris, 1998; Erickson et al., 2024). Although previous studies have demonstrated the utility of the SEM in capturing the multifaceted nature of mental health systems in adolescents and adults with untreated psychosis, to our knowledge, this is the first paper to apply to SEM as a model to the PP recovery process (Paquin-Goulet et al., 2023; Richie et al., 2023; Thorpe et al., 2025). By applying the SEM to the study of PP, researchers can explore not only individual-level experiences but also the broader social, cultural, and systemic factors that shape recovery. This approach can provide a comprehensive understanding of how to design, implement, and evaluate integrative care interventions that address socio-environmental factors that possibly moderate the effectiveness of treatment and sustained recovery (Moore et al., 2013). This current study builds on existing literature by pulling together the prior literature into one theoretical model to provide a deeper understanding of PP recovery from individuals with lived experiences. By mapping responses to a public health perspective with the SEM, this research seeks to provide a theoretical model that can be applied to future approaches designed to support those recovering from PP.
Methods
Design
The Massachusetts General Hospital Postpartum Psychosis Project (MGHP3), launched in 2018, enrolls an international cohort of individuals who experienced PP within 6 months of childbirth and during the 10 years prior to study participation, contributing to a greater understanding of the etiology, presentation, and treatment of postpartum psychosis (Cohen et al., 2023). Participants are recruited primarily through internet presence, PP advocacy networks, and physician referral. A one-time structured clinical interview is conducted with participants by phone to confirm PP diagnosis and capture lifetime psychiatric and medical history, including postpartum treatment information. A detailed description of the MGHP3 methodology has been previously reported (Cohen et al., 2023). This manuscript reports on a cross-sectional self-administered follow-up qualitative survey that was administered to all enrolled MGHP3 participants. All study procedures were conducted following the Declaration of Helsinki and with approval from the Mass General Brigham Institutional Review Board (protocol #2018P000886, approved August 2018). Privacy rights of human subjects were observed, and informed consent was obtained from all participants.
Measures
The self-administered follow-up survey contained six short written questions (see Figure 1) about influences, factors, and changes that would have been beneficial prior to, during, and after their PP episode.
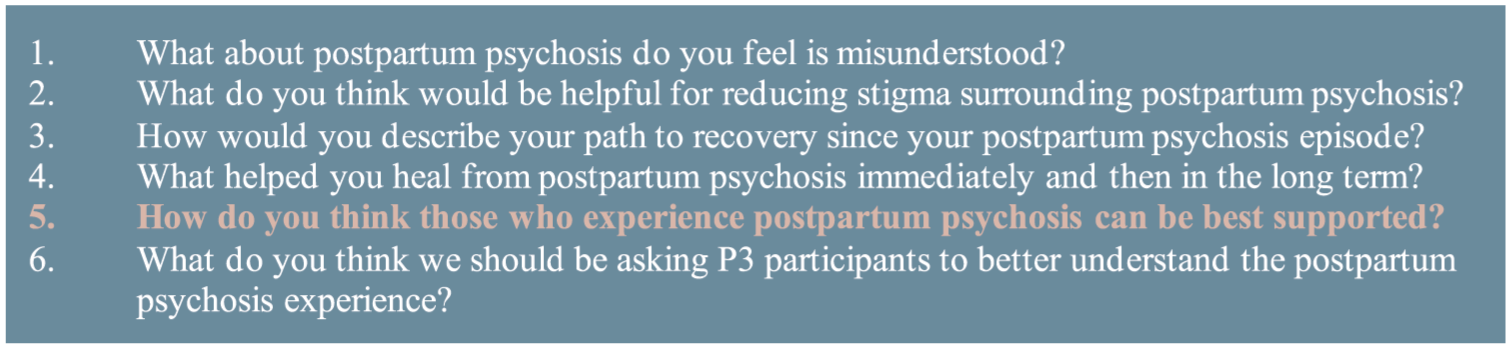
Survey questions. The six original questions posed in the self-administered follow-up qualitative survey, with question 5 being the focus of this analysis.
This analysis is of open-text responses to one question, “How do you think those who experience postpartum psychosis can be best supported?” The questions in this survey were developed based on clinical interest of the research team, input from MGHP3 advocacy partners, and to build on a qualitative analysis of PP narrative experiences from this study sample (Vanderkruik et al., 2024). The survey questions did not change over the course of the data collection period.
Participants
Participants were eligible if they completed the MGHP3 interview before October 1, 2023. The first six-question follow-up survey invitation was sent out on December 1, 2023, with a reminder sent in January 2024. Data were collected up until February 10, 2024. For more information on the eligibility criteria for MGHP3, see Cohen et al. (2023). Participant demographics were collected in the initial MGHP3 interview before the self-administered survey. A $25 Amazon gift card was provided to individuals who completed the self-administered qualitative survey.
Analysis
A content analysis approach was applied to identify major and minor themes (Elo and Kyngäs, 2008). We employed a combination of inductive and deductive coding to analyze survey responses. Initially, researchers familiarized themselves with the data by thoroughly reading the de-identified responses. An inductive approach was used to identify emerging codes. As codes developed and were refined over the analysis process, the coders recognized that emerging codes aligned with the SEM framework (Fereday and Muir-Cochrane, 2006). In the analysis process, initial codes were reorganized to be child code of each section of the framework. We applied a version of the SEM that was adjusted to specifically address mental health and well-being to guide deductively generated codes; the model shifted the narrative from mental illness as an individual’s responsibility to the impacts of social and environmental influences on the well-being of those diagnosed with a mental illness (Golden and Wendel, 2020; Michaels et al., 2022).
Within this SEM theoretical framework, participant responses regarding types of support from those with lived experience of PP were mapped at each of the levels of influence. As outlined in section 1 (introduction), there are six levels of the SEM: the intrapersonal level, the interpersonal level, the organizational level, the community level, the policy level, and the societal level. Each level is measured with a frame that focuses on improving mental health (Erickson et al., 2024). The intrapersonal level is measured based on the relationship one has with themselves. The interpersonal level measures the relationship between people. The organizational level is measured by participant suggestions for clinical care changes that range in complexity. The community level is measured in the relationships which occur in diverse settings (e.g. support groups or support for those within the participant’s social network; Bronfenbrenner and Morris, 1998). The policy level is measured by looking at how the individual is impacted by employment and/or governmental policies. Finally, the societal level is measured by the impact and influence society has on the individual.
Data were deidentified, cleaned, and manually coded using Microsoft Excel. Coders first familiarized themselves with the data by reading through each of the participants’ responses. The first round of coding was then conducted by reading through each of the participants’ responses to develop initial codes, and the last two rounds of coding were conducted with responses grouped by question rather than by participant to ensure consistency in coding across content areas. This choice may have affected the contextual or biographical coherence of the data, however, after the first two read throughs, coders felt comfortable with the flow of the narratives. Initial code generation was conducted collaboratively by four researchers with varying levels of expertise, two holding Bachelor of Arts degrees (HEY, MG), one holding a Bachelor of Science degree (PB), and one holding a Master of Public Health degree (AS). This team met regularly to discuss the coding process, compare interpretations, and resolve discrepancies. Reflexivity is an important cornerstone of qualitative research (Berger, 2015); therefore, researchers regularly questioned the impact of their backgrounds and beliefs on the interpretation of data and generation of themes. Disagreements were resolved through discussion to better refine code definitions. These results were collated and interpreted qualitatively. A fifth researcher contributed to decisions in cases of disagreement (RV).
A codebook was developed and iteratively refined throughout the analysis to ensure clarity and consistency of codes. After initial coding, each researcher independently analyzed specific survey responses. To ensure reliability, two researchers reviewed the others’ coding work, verifying alignment with the codebook. Once coding was finalized, codes were grouped into preliminary themes, focusing on question five of the survey to begin organizing the data. The themes were refined based on their prevalence across survey responses, ensuring they represented cohesive and meaningful patterns within the data set. The data extracted supporting each theme were reviewed to confirm their relevance and consistency. Researchers collaboratively reviewed and refined the themes, defining and naming the final themes to accurately capture the core ideas within the data. The standards of reporting qualitative research (SRQR) were used to guide the analysis and reporting of findings (O’Brien et al., 2014).
Results
As of October 1, 2023, a total of 390 women were enrolled in MGHP3. Of those, 75 did not complete their MGHP3 interview (withdrawn or lost to follow-up). There were 315 participants invited to take part in the follow-up survey, and 131 (42%) individuals who met the criteria for at least one episode of PP as established by the Mini International Neuropsychiatric Interview for Psychotic Disorders Studies (MINI-PDS) responded to the cross-sectional qualitative survey. Thus, the present sample comprises 131 women and 141 evaluable episodes of PP (some participants experienced more than one episode); see Figure 2 for participant study flow. A summary of demographic information is provided in Table 1.
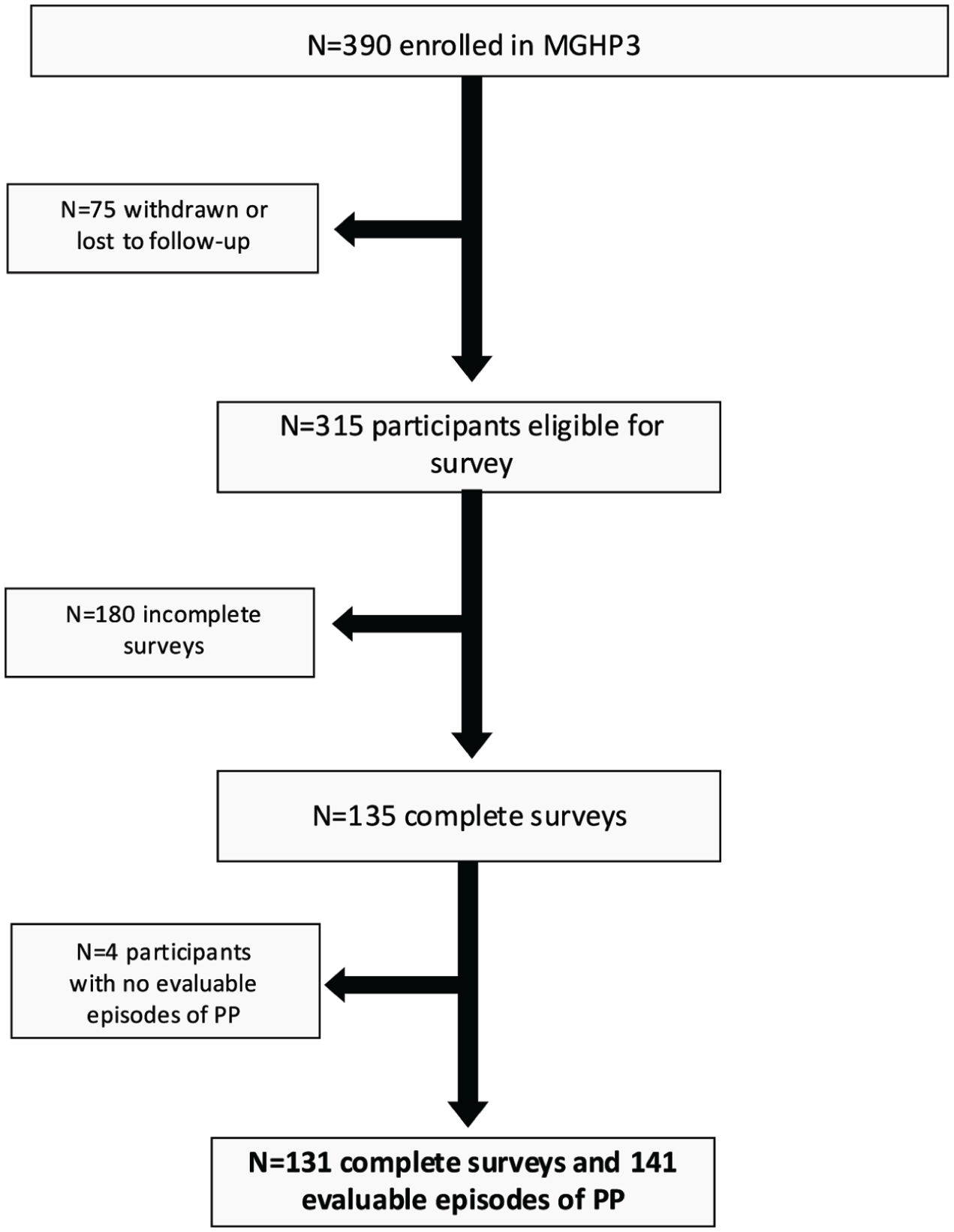
Participant enrollment. Flowchart illustrating study enrollment and selection of sample for analysis.
Demographics of study sample.
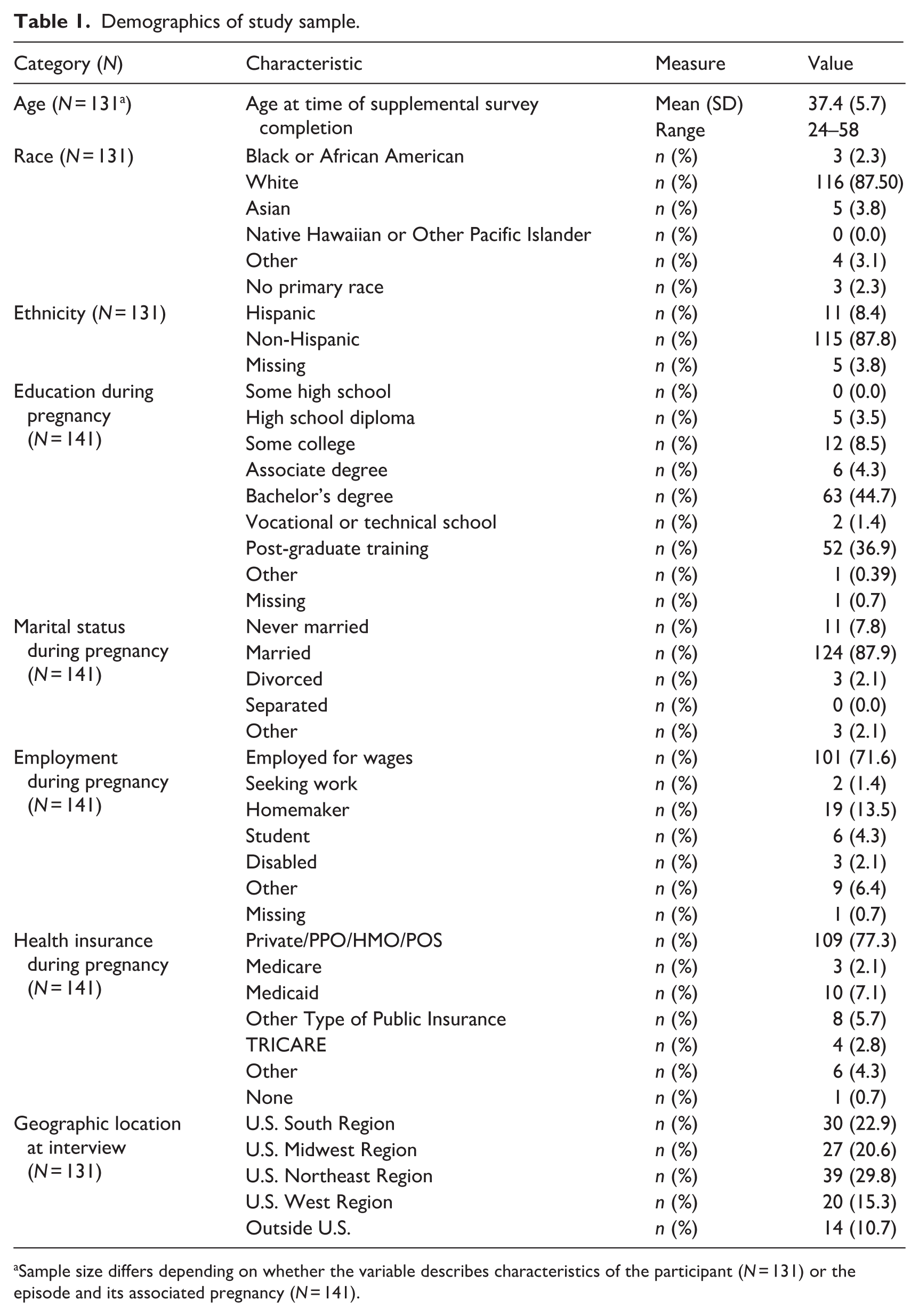
Sample size differs depending on whether the variable describes characteristics of the participant (N = 131) or the episode and its associated pregnancy (N = 141).
Findings are reported aligning with the levels of the SEM model, as displayed in Figure 3 and summarized in subsections 3.1–3.6.
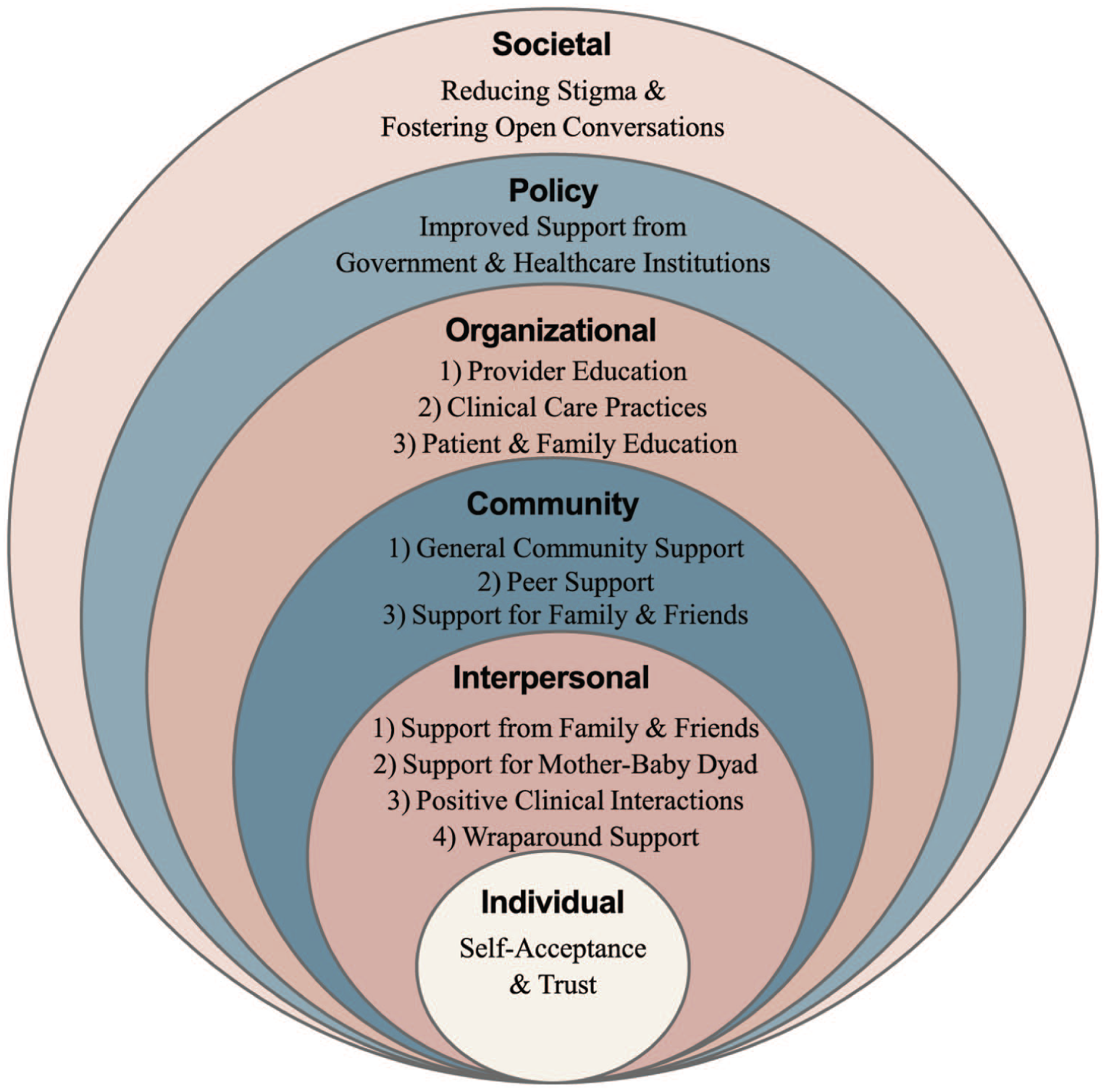
Findings mapped to the Socio-Ecological Model (SEM). Themes from qualitative analysis of participant responses mapped onto the six levels of the SEM model.
Individual level
At the intrapersonal level, a key theme that emerged was the importance of self-acceptance and trust for recovery. A participant emphasized, “She needs to know that it’s not her fault” (P1328). Participants discussed how repairing one’s self-concept and the ability to forgive oneself and have improved self-awareness influenced their experience of and recovery from PP. They emphasized that knowing that recovery is possible can empower individuals facing PP. One participant shared, “Being honest with yourself about how you’re feeling and not doubt[ing] yourself. Don’t be ashamed to take care of yourself . . . ” (P1004). Participants also underscored the importance of accepting support from others, emphasizing that seeking help should not be viewed as shameful or as a sign of failure, but instead as an important part of self-care and recovery.
Interpersonal level
Four themes emerged at the interpersonal level:
Support from family and friends. Participants described the critical role of immediate social support in recovery, often responding with variations of “family and friends” (P1382) as important for supporting those who experience PP. This support was linked to environmental and behavioral changes, such as encouraging and facilitating personal care and support for their children. This code was placed at the interpersonal level because the priority of this relationship is support from someone directly related to the mother and the impact those relationships have directly on the mother.
Support for mother-baby dyad. Many participants advocated for the importance of having the option to be with their baby throughout their recovery. One participant said, “There needs to be in patient places where women can be with their babies. I was separated from my baby for 4 weeks on a general psych ward and it was horrible” (P1278). Participants expressed the belief that having this time with their baby would be important for their recovery. This code was placed at the interpersonal level instead of the organizational level because the priority of this code was to highlight the relationship between mother and baby specifically and how their relationship is impacted by clinical care.
Positive clinical interactions. Participants highlighted the value of meaningful and trusted relationships with clinical providers. One participant stated, “I think having a psychiatrist that involves the support system of the affected person could be extremely beneficial for helping to set realistic expectations for families and determine best treatment plans for affected individuals” (P1285). Collaborative and supportive interactions with knowledgeable providers were highlighted as helpful for recovery. This code was placed on the interpersonal level instead of the organizational level because the narratives focused on the personal relationships between patient and provider instead of organizational level changes.
Wraparound support. Participants emphasized the importance of comprehensive support that validates their experiences and eases demands during the recovery period. As one participant noted, “Aside from medical management I think assistance with sleep and childcare would make a big difference” (P1208); another participant stated, “Having people help you maintain your sleep hygiene during recovery” (i.e. caring for the baby at night) (P1380). Support from others that specifically enables improvement of lifestyle behaviors was viewed as helpful for recovery.
Community level
At the community level, three themes arose:
General community support. Participants advocated for interventions to provide support when interpersonal networks were insufficient. For example, one participant suggested, “There must be some community volunteers or something like that to help. . . Even just help cleaning the house is very useful” (P1180).
Peer support. Many participants found solace and encouragement in peer communities, which provided a judgment-free space to share experiences and combat feelings of isolation. One participant remarked, “I think that knowing you aren’t alone in your experience goes a long way. Being able to easily connect with fellow survivors would be so helpful” (P1260). This code was categorized within the community level instead of the interpersonal level because the prioritized narratives in this code focused on group relationships that the mother encountered.
Support for family and friends. Participants emphasized the need for resources to help family members process the impact of PP. One participant described the perceived lasting effects on her son, who witnessed her psychosis: “I would love more support for siblings and family members. My, now, 16-year-old son. . .witnessed me get taken to the hospital and police come to the house. It must have been very scary for him” (P1135). This was categorized within the community level because the focus of this code was to capture how groups of people around the mother were supported.
Organizational level
At the organizational level, participants proposed three key areas for improvement:
Provider education. Participants advocated for better training for non-psychiatric healthcare providers to identify and manage PP. One participant noted:
OBGYNs need to be trained in warning signs and able to prescribe the medications needed to help with psychosis. Every doctor who wasn’t a [psychiatric health care provider] was terrified to prescribe me the anti-psychotics needed, and had I not gone to the ED and immediately been put in a program with access to a psych NP immediately, I would’ve had to wait 6 weeks for an appointment with a [psychiatrist] for medications and quite honestly, I wouldn’t have survived that long. They should be able to prescribe and be comfortable with that. Maybe additional training [options] for them. A certification or something. (P1023)
This participant highlighted the importance of practitioners being able to diagnose and treat the disease, which was a sentiment echoed by many other participants. Participants reported that the wait times to see a specialist were too long for a patient in crisis. Many advocated for training that would reach a wider set of practitioners to ease the barriers they faced in identification of PP and receiving treatment.
2. Clinical care practices. Many participants recommended changes to facilitate treatment while also keeping families together. As one participant expressed, “Give us [a] better chance to get treatment with[out] fear of losing our children” (P1327). Overall, the clinical changes recommended by participants were better screenings, care for mothers and babies together (e.g. mother and baby units), and increased access to treatment (e.g. antipsychotic medication). This differs from the interpersonal code of positive clinician interaction because the narrative prioritized in this code referred to larger systemic changes which could occur at the clinical care site instead of individual interactions between people.
3. Patient and family education. Participants emphasized the importance of transparency and education in the treatment process, stating it would empower families to provide better support. One participant explained, “If someone could have sat me down in the hospital and explained things to me more, it might have helped” (P1293). This participant was not alone in their desire for more transparency in how treatment is given. Secondarily, participants also wanted their families involved in the treatment discussions to better support the person experiencing PP. As another participant stated, “ . . . support from my spouse was also critical. He was present for every other meeting with the psychiatrist to give his perspectives on how things were progressing, and it was helpful for the psychiatrist and encouraging to me . . . ” (P1285). The narrative prioritized in this organizational code again emphasized larger systemic changes which could occur at the clinical care site instead of between individuals.
Policy level
At the policy level, participants advocated for government and healthcare institutional changes to better support those experiencing PP. Suggestions included paid family leave, insurance coverage for postpartum doulas, and expanded access to therapy. One participant shared, “Time and space to heal which means childcare support and time off from work” (P1322). Another participant noted that, “Improvements to public health that provide better support for families and reduce stress around issues of reproduction and healthcare would make a huge difference as well” (P1208). Lastly, one participant requested, “Better maternal Healthcare in general–postpartum doulas covered by insurance, paid time off, insurance having to cover all follow up care including therapy . . . ” (P1320). These requests speak to the vital policy changes which could be made at the company, state, or federal level to improve the pathway to recovery.
Society level
At the societal level, participants highlighted the need for reducing stigma and fostering open conversations about PP. Participants reported that societal norms or lack of awareness often hindered recovery, with one participant stating: “It would be helpful if the general public were aware, and the stigma of psychosis and mental illness were lessened, because that could encourage women to seek help without fear of judgement or ridicule” (P1086). Many participants emphasized the importance of sharing stories with more positive outcomes to challenge stigma and increase public awareness and knowledge of the illness.
Discussion
This study highlights the complex and multifaceted needs of individuals experiencing PP and provides insights into how to expand care and support for the recovery processes. Our findings largely align with a systematic review and meta-analysis of experiences with recovery from PP, which concluded that more integrative and individualized approaches are needed that incorporate long-term psychological and psychosocial support, and considers the needs of the family, to improve clinical outcomes (Forde et al., 2020). Thus, our findings contribute to the literature by empirically reinforcing and contextualizing established priorities leveraging the voices of a large sample of individuals with lived experience of PP. This is particularly important in PP, where evidence-based recommendations are often inconsistently implemented or deprioritized in practice. Our findings reinforce that well-established factors are repeatedly identified by patients themselves as central to recovery. In addition, our study advances the literature by situating these themes within a socio-ecological framework, demonstrating how commonly cited factors operate across multiple levels (e.g. interpersonal, healthcare system, societal), and by highlighting their real-world salience, interconnections, and implications for multi-level intervention. While the underlying concepts appear similar, their mechanisms, responsible actors, and intervention strategies differ meaningfully across levels. Lastly, although the sample population was international, the majority of participants are from the US, indicating that these needs are found both in countries with nationalized healthcare and privatized healthcare. Furthermore, the indication that needs of mothers in both types of care environments have similar needs suggests the fundamental need for change within society.
By framing findings through the SEM, this analysis conceptualizes PP as a public health issue, emphasizing the importance of interdisciplinary and multi-level approaches to support recovery (Golden and Wendel, 2020). Key recommendations emerging from participants’ lived experiences in this analysis include: (1) Encouraging and fostering support networks at interpersonal and community levels; (2) Improving elements of clinical care, including provider training and integrated care models; (3) Implementing policies to enhance care access and support for new mothers; (4) Increasing societal awareness of PP to combat stigma and foster timely intervention. While findings are aligned with existing evidence-based practices for postpartum mental health support, recommendations for PP support are often dismissed as the illness is considered “rare” or “uncommon.” The current study’s large, international sample highlights the number of individuals, communities, and organizations touched by PP, demonstrating a need for closer alignment between evidence-based findings and real-world clinical practice. Moreover, given the severity of PP, including risk of infanticide and heightened suicidal ideation, clear guidelines to support PP treatment and recovery are crucial (Brockington, 2017; Feingold and Lewis, 2025; Sharma et al., 2022). A multi-level and interdisciplinary care approach for addressing PP based on the SEM, such as engaging peer and community support systems and enhancing societal awareness, can enhance current clinical care practices to treat the illness.
As recovery from PP does not follow a linear path (Forde et al., 2020), services should address not only acute episodes but also the long-term recovery process (Vanderkruik et al., 2024). Findings from our analysis emphasize impactful supports occurring at the interpersonal and organizational levels. Participants stressed the importance of positive relationships with family, friends, and clinical providers, advocating for integrated care approaches such as improved care coordination, role clarity within clinical teams, and structured inclusion of support persons in care planning and psychoeducation. (Ruffell et al., 2019). Similarly, recurrent descriptions of gaps in provider knowledge highlighted participant recommendations for standardized training in PP recognition and management across obstetric, psychiatric, and primary care settings. Additionally, community-level peer support groups, policy-level initiatives, such as paid family leave, and societal-level public awareness campaigns were identified as critical resources for sustained recovery. Finally, participants note at both the interpersonal and organizational level the desire for further support for the mother-baby dyad, including access to mother-baby units, which aligns with findings from other qualitative research on PP experiences (Roxburgh et al., 2023). While many participants expressed the difficulty of being separated from baby and the desire to have contact with baby during the recovery process, other research has found that some mothers appreciated having time away from their baby to focus on getting healthy (Plunkett et al., 2017). Thus, it may be important to have options for separation from, or contact with, baby depending on a given patient’s situation and preferences.
Expanded awareness and education about PP is needed. Participants highlighted the detrimental impact of stigma and a lack of understanding, which often delays help-seeking until crises occur (Forde et al., 2020). Education for families and the public on the signs and symptoms of PP is essential to facilitate early recognition and appropriate care (Plunkett et al., 2017). These efforts can help reduce the emotional and logistical burdens on immediate family networks, enabling a broader community-based support system (Heron et al., 2012). This study builds upon findings from UK-based research and fills a gap by incorporating a theoretical framework (i.e. SEM) into qualitative research on postpartum psychosis. The SEM framework may provide a foundation for designing future interventions and clinical practices, addressing PP at multiple levels to alleviate the overwhelming responsibility often borne by individuals and their families (Golden and Wendel, 2020).
Strengths and limitations
Strengths of this study include a large, geographically diverse sample from five countries, 33 US states, and Washington DC, as well as rigorous diagnostic confirmation using structured interviews in MGHP3. Additionally, the use of the SEM framework enhances the interpretive depth of findings, providing a structured lens for understanding the layered complexities of PP recovery. However, several limitations exist which should be considered when interpreting our findings. The sample lacked racial and socioeconomic diversity, with 87% identifying as white, 83% holding at least a bachelor’s degree, and 77% reporting private insurance during their perinatal period. The homogeneity of the sample impacts the generalizability to other racial/ethnic and socio-economic groups. Retrospective reporting may also introduce recall bias, although evidence suggests recall of traumatic experiences like PP is typically reliable (Doucet et al., 2012). Furthermore, the qualitative data were derived from short-answer, written survey responses, restricting the ability to probe deeper into participant experiences. The range of experiences and factors that individuals with lived experience of PP recovery were described in this content analysis, rather than a more interpretive thematic analysis that typically relies on in-depth interviews and richer narrative data. Finally, the 42% response rate to the supplemental survey invitation may have introduced response bias.
Future directions
Given the severity and complexity of PP, there is a need to expand awareness and multilevel supports for providers, patients, and families. Incorporating the voices of individuals with lived experience is crucial in designing patient-centered interventions. Future research could build on these reported findings and explore strategies to develop and implement comprehensive support services. Furthermore, the SEM was used as a framework to guide the analysis only; future research could consider using the SEM to guide qualitative inquiry during the development of an interview guide or survey, to intentionally explore constructs in the model. This study provides a preliminary mapping of patient-identified support needs which may contribute to a framework for future interventions. Findings underscore the importance of multi-level, theoretically grounded approaches to improving outcomes for individuals recovering from PP.
Footnotes
Ethical considerations
All study procedures were conducted following the Declaration of Helsinki and with approval from the Mass General Brigham Institutional Review Board (protocol #2018P000886, approved August 2018).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Author contributions
Ariel L. Scalise: Conceptualization, Methodology, Data curation, Writing – Original Draft, Writing – Review & Editing, Visualization, Project administration. Hannah E. Yoon: Investigation, Data curation, Writing – Original Draft, Writing – Review & Editing, Project administration. Peri E. Barest: Data curation, Writing – Original Draft, Writing – Review & Editing. Margaret L. Gaw: Investigation, Writing – Review & Editing. Marlene P. Freeman: Conceptualization, Methodology, Writing – Original Draft, Writing – Review & Editing, Supervision, Funding acquisition. Lee S. Cohen: Conceptualization, Methodology, Writing – Original Draft, Writing – Review & Editing, Supervision, Funding acquisition. Rachel C. Vanderkruik: Conceptualization, Methodology, Investigation, Writing – Original Draft, Writing – Review & Editing, Visualization, Supervision, Project administration.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Jeanne and Gerhard Andlinger Research Fund for Innovative Science at Massachusetts General Hospital and The Rosalie Katz Family Foundation.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lee S. Cohen, MD – Research Support: Dr. Cohen is an employee of Massachusetts General Hospital and works with the MGH National Pregnancy Registry. MGH National Pregnancy Registry: Current Sponsors: Alkermes, Inc. (2016–Present); Bristol-Myers Squibb Company (2025–Present); Eisai Inc. (2022–Present); Otsuka America Pharmaceutical, Inc. (2008–Present); Sage Therapeutics (2019–2023, 2024–Present); Supernus Pharmaceuticals (2021–Present). Past Sponsors: Forest/Actavis/Allergan (2016–2018, declined to sponsor: 2018–Present); Aurobindo Pharma (2020–2022, declined to sponsor: 2022–Present); AstraZeneca Pharmaceuticals (2009–2014, declined to sponsor: 2014–Present); AuroMedics Pharma LLC (2021–2022, declined to sponsor: 2022–Present); Johnson & Johnson/Janssen Pharmaceuticals, Inc (2019–2023, declined to sponsor: 2024–Present) ; Ortho-McNeil-Janssen Pharmaceuticals, Inc (2009–2014, declined to sponsor: 2015–Present); Pfizer, Inc. (2009–2011, declined to sponsor: 2012–Present); Sunovion Pharmaceuticals, Inc. (2011–2023, declined to sponsor: 2024–Present); Teva Pharmaceutical Industries Ltd. (2018–2025; declined to sponsor 2025–Present); Dr. Reddy’s Laboratories, Inc. (2023–2025, declined to sponsor 2025–Present). Updated sponsors can be found at: ![]() . As an employee of MGH, Dr. Cohen works with the MGH CTNI, which has had research funding from multiple pharmaceutical companies and NIMH. Other research support: National Institutes of Health; SAGE Therapeutics, The Marriott Foundation, NEDA. Advisory/Consulting: JDS Therapeutics LLC; Luminous Minds LLC. Speaking/Honoraria: None.
. As an employee of MGH, Dr. Cohen works with the MGH CTNI, which has had research funding from multiple pharmaceutical companies and NIMH. Other research support: National Institutes of Health; SAGE Therapeutics, The Marriott Foundation, NEDA. Advisory/Consulting: JDS Therapeutics LLC; Luminous Minds LLC. Speaking/Honoraria: None.
Marlene P. Freeman, MD – Research Support: Dr. Freeman is an employee of Massachusetts General Hospital and works with the MGH National Pregnancy Registry. MGH National Pregnancy Registry: Current Sponsors: Alkermes, Inc. (2016–Present); Bristol-Myers Squibb Company (2025–Present); Eisai Inc. (2022–Present); Otsuka America Pharmaceutical, Inc. (2008–Present); Sage Therapeutics (2019–2023, 2024–Present); Supernus Pharmaceuticals (2021–Present). Past Sponsors: Forest/Actavis/Allergan (2016–2018, declined to sponsor: 2018–Present); Aurobindo Pharma (2020–2022, declined to sponsor: 2022–Present); AstraZeneca Pharmaceuticals (2009–2014, declined to sponsor: 2014–Present); AuroMedics Pharma LLC (2021–2022, declined to sponsor: 2022–Present); Johnson & Johnson/Janssen Pharmaceuticals, Inc (2019–2023, declined to sponsor: 2024–Present) ; Ortho-McNeil-Janssen Pharmaceuticals, Inc (2009–2014, declined to sponsor: 2015–Present); Pfizer, Inc. (2009–2011, declined to sponsor: 2012–Present); Sunovion Pharmaceuticals, Inc. (2011–2023, declined to sponsor: 2024–Present); Teva Pharmaceutical Industries Ltd. (2018–2025; declined to sponsor 2025–Present); Dr. Reddy’s Laboratories, Inc. (2023–2025, declined to sponsor 2025–Present). Updated sponsors can be found at: ![]() . Other Research Support: Other research support through MGH: Sage, NIA, NIMH. Advisory/Consulting, Data Safety Committees/Independent Data Safety and Monitoring Committees: Consulting through CTNI through MGH, Janssen (Johnson& Johnson), Novartis, Neurocrine; Eliem, Sage; Brainify; Everly Health; Tibi Health; Relmada; Beckley Psytech; Brii Biotech; Reunion; Vistagen. Speaking/Honoraria: MGH Psych Academy, WebMD, Medscape, Pri-Med, Postpartum Support International, PRIME, HMP Global, CME Institute.
. Other Research Support: Other research support through MGH: Sage, NIA, NIMH. Advisory/Consulting, Data Safety Committees/Independent Data Safety and Monitoring Committees: Consulting through CTNI through MGH, Janssen (Johnson& Johnson), Novartis, Neurocrine; Eliem, Sage; Brainify; Everly Health; Tibi Health; Relmada; Beckley Psytech; Brii Biotech; Reunion; Vistagen. Speaking/Honoraria: MGH Psych Academy, WebMD, Medscape, Pri-Med, Postpartum Support International, PRIME, HMP Global, CME Institute.
Rachel Vanderkruik, PhD, MSc – Research Support: Dr. Vanderkruik is an employee of Massachusetts General Hospital and works on projects funded by The J. Willard and Alice S. Marriott Foundation and the National Eating Disorder Association.Advisory/Consulting: World Health Organization. Speaking/Honoraria: MGH Psych Academy.Ariel L. Scalise, MPH, Hannah E. Yoon, BA, Peri E. Barest, BS, Margaret L. Gaw, BA have no conflicts of interest to disclose.
Data availability statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.*