
Abstract
The COVID-19 pandemic disrupted physical activity behaviors and worsened mental health worldwide. This study synthesized observational evidence on relationships between physical activity and depression, anxiety, and stress in adults during COVID-19. A systematic review and multilevel random-effects meta-analysis (PROSPERO CRD42023491651) of observational studies published January 2020–May 2023 included 38 studies with 140,915 adults using validated measures. Physical activity showed significant inverse associations with depression (r = −0.18; p < 0.001) and stress (r = −0.14; p = 0.043), but not anxiety (p = 0.340). Heterogeneity was substantial. Findings suggest physical activity can serve as a low-risk adjunct to mitigate depressive symptoms and perceived stress during public health crises, though interpretation should be cautious given observational design and high heterogeneity. Clinically, brief assessment and promotion of regular physical activity—tailored to context and delivered in-person or remotely—may support psychological well-being, while anxiety may require combined approaches during emergencies.
Introduction
The COVID-19 pandemic substantially altered daily life and created major challenges for physical and mental health (Arabzadeh et al., 2023; Bohn et al., 2023; Chan et al., 2023). Following the World Health Organization pandemic declaration in early 2020, lockdowns, social distancing, and mobility restrictions disrupted routines and reduced opportunities for regular physical activity (Çerezci-Duygu et al., 2023; Hollingdale et al., 2022; Ju et al., 2023; Karpov et al., 2023). During the same period, population-based studies reported increased symptoms of depression, anxiety, and stress across diverse groups (Cruz-Ausejo et al., 2023; da Costa et al., 2022; Lardier et al., 2023; Odriozola-González et al., 2022; Ricci et al., 2023; Santana et al., 2023).
Physical activity is consistently associated with better mental health and psychological well-being (Heissel et al., 2023; Pearce et al., 2022; Wanjau et al., 2023; White et al., 2024). Pre-pandemic evidence suggests that regular physical activity is linked to lower levels of depression, anxiety, and stress through both biological and psychological pathways (Bhattacharya et al., 2023; Mu et al., 2024; Wilkialis et al., 2021). Proposed mechanisms include enhanced neurotransmitter function, increased brain-derived neurotrophic factor expression, and improved neuroplasticity, as well as psychological processes such as greater self-efficacy, improved emotional regulation, social connection, and more effective coping with stress (Bhattacharya et al., 2023; Mu et al., 2024; Wilkialis et al., 2021). From a health psychology perspective, physical activity may function as a behavioral resource that supports stress regulation, emotional coping, and perceived self-efficacy, while also helping to preserve routine, mastery, and social connectedness during periods of disruption (Hung et al., 2025; Ibáñez Román et al., 2023; Singh et al., 2023).
Although related, depression, anxiety, and stress represent partially distinct dimensions of psychological distress and may be associated with physical activity through overlapping but non-identical pathways (Liu, 2025; Pearce et al., 2022; Wanjau et al., 2023). Depression is often linked to behavioral withdrawal, reduced reinforcement (Wang and Feng, 2022); anxiety to uncertainty, hyperarousal, and emotion regulation difficulties (Brown et al., 2023; McElroy et al., 2020); and stress to perceptions of overwhelming situational demands (Brown et al., 2023; Liu, 2025). These distinctions suggest that the relevance of physical activity during the pandemic may not have been uniform across outcomes.
This perspective aligns with established health psychology frameworks. Stress and coping theory conceptualizes health behaviors as resources that shape appraisal and responses to challenging circumstances, while self-efficacy-based perspectives emphasize perceived control and agency in emotional adjustment (Abraham et al., 2024; Hagger, 2025). Behavioral activation concepts further explain why maintaining activity may be particularly relevant to depressive symptoms under conditions of isolation and disrupted routine. During the pandemic, physical activity may have buffered psychological distress by preserving coping resources, supporting mood regulation, and mitigating stress responses amid prolonged uncertainty (Koziel Ly et al., 2022; Shannon et al., 2023).
At the same time, the pandemic created conditions in which established relationships required re-evaluation. Reduced access to outdoor spaces and structured exercise opportunities coincided with elevated isolation, uncertainty, and psychological burden, affecting both physical activity and mental health simultaneously (Arora et al., 2022; Arora and Grey, 2020; Cruz-Ausejo et al., 2023; Shannon et al., 2023; Wut et al., 2023). Thus, the protective role of physical activity may differ under acute and sustained societal stress compared with pre-pandemic contexts.
Although individual studies have examined these associations, findings remain inconsistent. Some report protective associations (Açikgöz et al., 2022; Han et al., 2022; Lu et al., 2023; Rodrigues et al., 2023; Yasunobe et al., 2023), whereas others report weaker or null effects (Akçay et al., 2021; Arabzadeh et al., 2023; Duncan et al., 2021; Gierc et al., 2021; Lage et al., 2021; Stevens et al., 2021). This heterogeneity likely reflects differences in populations, measurement approaches, timing of data collection, and methodological quality, underscoring the need for systematic synthesis.
These questions are clinically and publicly relevant because physical activity may represent an important correlate of mental health when usual coping resources and support systems are disrupted (Bellicha et al., 2022; Tsekoura et al., 2023; Vally and Helmy, 2021; Zhu et al., 2022). Understanding these associations may therefore inform mental health planning, public health responses, and future research during periods in which access to usual services is limited or constrained (Shannon et al., 2023; Vuelvas-Olmos et al., 2023; Wut et al., 2023).
The current systematic review and meta-analysis synthesize observational evidence on the association between physical activity and mental health outcomes in adults during the COVID-19 pandemic. Specifically, we examined associations with depression, anxiety, and stress to clarify the magnitude and direction of these associations under pandemic conditions. By doing so, this review aims to determine whether associations observed before the pandemic were consistently maintained across distinct domains of psychological distress during a uniquely disruptive public health context.
Methods
Design and registration
This systematic review and meta-analysis followed the PRISMA guidelines (Page et al., 2021; Supplemental File S1), and was registered in PROSPERO (CRD42023491651).
Data sources and searches
Systematic searches were conducted in MEDLINE, EMBASE, Scopus, the Cochrane Library, and WOS, and EBSCOhost in English and Spanish, with no time restrictions. Search terms were based on MeSH headings and adapted for each database (Supplemental Table S1).
Study selection
Studies were included based on eligibility criteria covering:
Population: Studies were required to include adults (over 18 years) who had been active or inactive during the COVID-19 pandemic. Physical activity could be of any type or intensity.
Intervention/Exposure: Any form of physical activity, such as walking, running, cycling, or home workouts. Studies were required to include clear measurement definitions (e.g. self-report, use of fitness trackers).
Comparator: Physical inactivity or varying levels of physical activity.
Outcomes: Studies were required to consider the mental health of the participants (specifically depression, anxiety, or stress) measured using validated instruments.
Study Design: Only studies employing cross-sectional or longitudinal designs were included.
Context: Studies included in the review were required to have collected data during the WHO-defined COVID-19 pandemic period (January 30, 2020 to May 5, 2023). They could be from any geographical location and were required to consider the impact of lockdowns, social distancing measures, and other pandemic-related restrictions on physical activity and mental health.
Studies were excluded if they involved participants <18 years, lacked clear physical activity definitions, were non-original reports, were intervention trials without observational analyses, or did not provide sufficient data for effect-size computation. Reasons for exclusion are provided in Supplemental File S2.
Outcome measures
Primary outcomes were depression, anxiety, and stress, assessed using validated scales. The Patient Health Questionnaire (PHQ-9) and other self-reported scales were used to measure depression. The Generalized Anxiety Disorder Scale (GAD-7) and other scales were used to measure anxiety. The Perceived Stress Scale (PSS) and the Depression, Anxiety, and Stress Scale (DASS) were used to measure stress. Measurements from any phase (lockdown, easing of restrictions, or post-lockdown) were eligible, including studies examining changes in physical activity over time.
Data extraction
Three reviewers independently extracted study characteristics (country, design, sampling), participant demographics, physical activity instruments (e.g. IPAQ variants, device-based metrics), mental health measures (PHQ-9, GAD-7, PSS/DASS), timing within the pandemic, and effect estimates with precision. When multiple estimates were available, multivariable-adjusted results were prioritized using a prespecified covariate hierarchy. Authors were contacted for missing or unclear data.
Risk of bias assessment
Methodological quality was assessed using the Newcastle-Ottawa Scale for Cross-Sectional Studies (NOS-xS), specifically tailored for studies examining associations (Carra et al., 2025). This scale categorizes the risk of bias into three levels: low, moderate, and high, based on a 9-star system.
The assessment includes three criteria. First, Study Sample Selection awards a maximum of two stars for representativeness and adequacy of sample size. Second, the Assessment of Exposure(s) and Outcome(s) grants up to four stars, with evaluations of physical activity exposure and mental health outcomes. Both gold-standard assessments receive full stars, while acceptable and non-acceptable methods are scored accordingly. Lastly, Confounding Factors allows for up to three stars based on the degree of adjustment for confounding variables and the methodological rigor of their assessment. Overall, studies receive scores ranging from 0 to 9 stars, categorizing them as low risk of bias (7–9), moderate risk (4–6), or high risk (0–3).
Certainty of evidence assessment
Certainty of evidence was evaluated using GRADE (Grading, Development and Evaluation of Recommendations; Balshem et al., 2011; Guyatt et al., 2011). The GRADE methodology assesses confidence in the evidence in five areas: bias, inconsistency, indirectness, imprecision, and publication bias. Observational studies begin as low-certainty evidence quality, but particular criteria might increase or lower it (Schünemann et al., 2020).
Methodological constraints observed in individual research quality assessments, including convenience sampling selection bias, self-reported instrument measurement bias, and observational design confounding, were used to assess bias. Inconsistency was evaluated by using statistical heterogeneity (I2) and impact estimate variability. I2 values > 50% indicate substantial heterogeneity, requiring downgrading. Indirectness was assessed by whether study populations, interventions, and results directly addressed the research topic without substantial changes from the target population or setting. Sample size adequacy, confidence interval width, and clinically significant effects determined imprecision. Visual inspection of funnel plots and statistical tests assessed publication bias in meta-analysis of ⩾10 studies (Egger et al., 1997).
Large magnitude of effect (standardized mean difference >0.8), dose-response gradient, and instances where all probable confounding would lower the confidence. We rated each outcome’s evidence as high, moderate, low, or very low based on our confidence in the effect estimate and the possibility that more research would affect our results.
Two reviewers independently assessed GRADE, with discrepancies resolved through discussion and contact with a third reviewer. To make quality ratings transparent and aid clinical and public health interpretation, GRADE evidence profiles were created.
Data synthesis and analysis
Analyses were conducted in R software (Version 4.1.3) using the metafor package. A multilevel random-effects meta-analysis with restricted maximum likelihood (REML) accounted for multiple effect sizes per study (Viechtbauer, 2010). Heterogeneity was quantified using I2 statistics and tau2 estimates.
Given the observational nature of included studies, diverse statistical measures (correlations, regression coefficients, odds ratios, and prevalence ratios) were harmonized and converted to standardized effect sizes. All metrics were transformed to a common correlation metric (r) for pooling, following standard procedure implemented with metafor and custom code (Supplemental File S3).
Subgroup analyses examined association type, age group, physical activity instrument, mental health measure, geographic region, and methodological quality. A random-effects meta-regression evaluated publication year as moderator. Sensitivity analyses included leave-one-out, alternative effect size choices (adjusted vs unadjusted), exclusion of high-risk studies, and influence diagnostics (Supplemental File S3). Small-study effects were assessed using funnel plots and Egger’s tests when k ⩾ 10. Results are presented as pooled effect sizes with 95% confidence intervals, with statistical significance set at p < 0.05.
Ethical approval
This review used only published data; no ethical approval was required.
Results
Study selection
The study selection process is shown in Figure 1. The search identified 9133 records; after removing duplicates, 5245 remained for screening. Following title, abstract, and full-text assessment, 38 studies met the inclusion criteria. The full list of included studies is provided in Supplemental File S4.
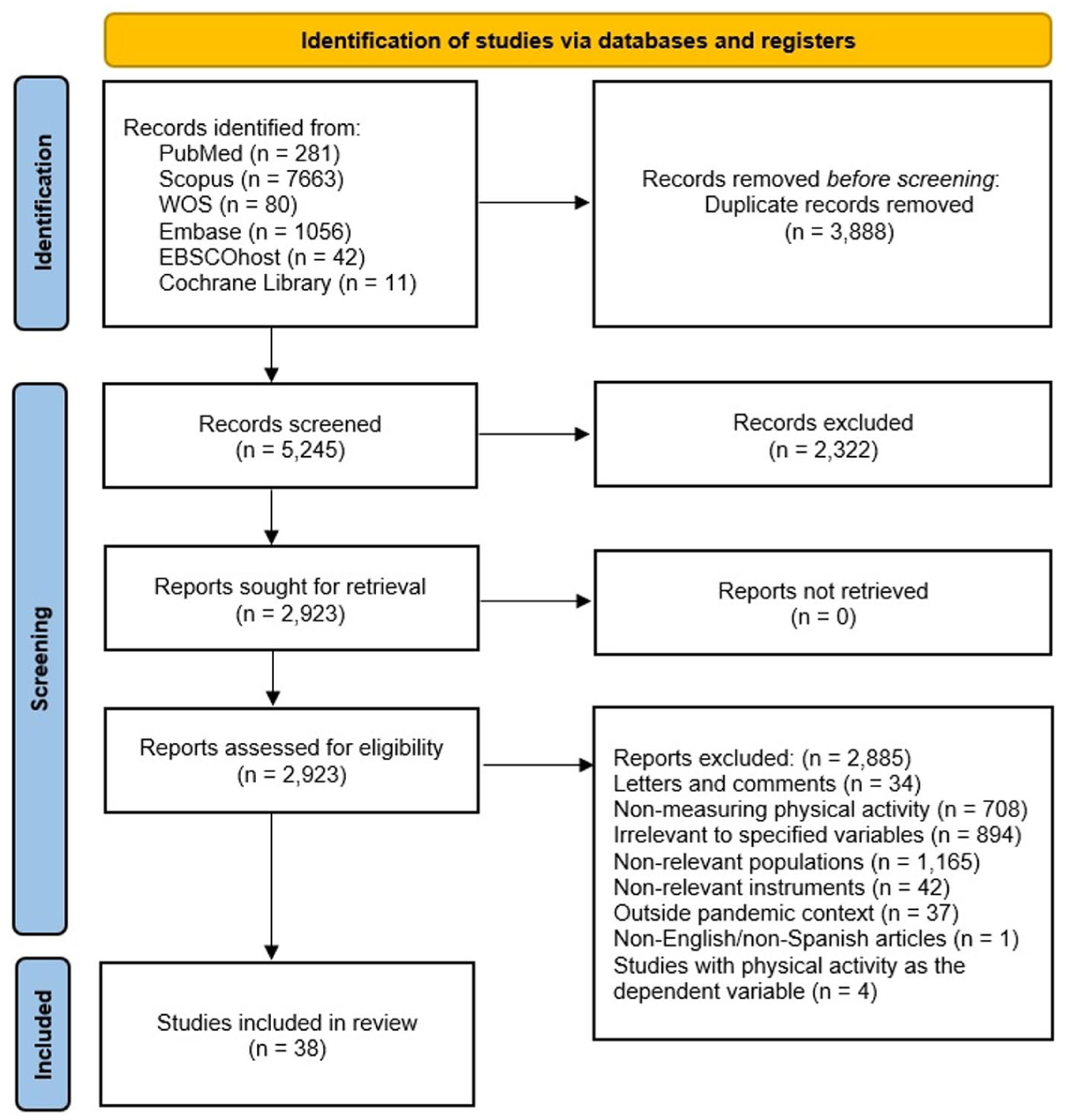
Flowchart illustrating the study selection process for studies examining the association between physical activity and mental health outcomes during the pandemic, following PRISMA guidelines.
Study characteristics
Characteristics of the included studies are summarized in Supplemental Table S2. Across 38 studies, 140,915 adults were included (59.3% women, n = 83,600; 40.7% men, n = 57,315). The mean age across studies was 41.64 years, with study-level means ranging from 19.5 to 76.1 years. Most studies were conducted in the Americas (42.1%, n = 16) and Asia (39.5%, n = 15). Of the 38 studies, 24 contributed data to at least one quantitative synthesis, while 14 were included only in the qualitative synthesis.
Populations included general adults (39.5%, n = 15), university students (28.9%, n = 11), older adults ⩾ 65 years (15.8%, n = 6), healthcare or hospital populations (10.5%, n = 4), and other specialized groups (5.3%, n = 2).
Physical activity was most commonly assessed using the IPAQ-SF (36.8%, n = 14). Depression was the most studied outcome (86.8%, n = 33), followed by anxiety (57.9%, n = 22), and stress (28.9%, n = 11). Depression was most often measured with the PHQ-9 (39.5%, n = 15); anxiety with the GAD-7 (31.6%, n = 12); and stress with the PSS and the DASS (each 13.1%, n = 5).
Methodological quality assessment
Using the NOS-xS, most studies demonstrated acceptable methodological quality. Of the 38 studies, 33 (86.8%) scored ⩾4 stars, 31 (81.6%) scored ⩾5, 16 (42.1%) scored ⩾6, and 17 (44.7%) were classified as low risk of bias (7–8 stars).
Quality was strongest for exposure and outcome assessment, as many studies used validated physical activity and mental health instruments. The main limitations involved sample selection, particularly representativeness and sample size justification, which reduced overall quality ratings. Overall, the methodological profile supported quantitative synthesis. Quality score distribution is shown in Figure 2.
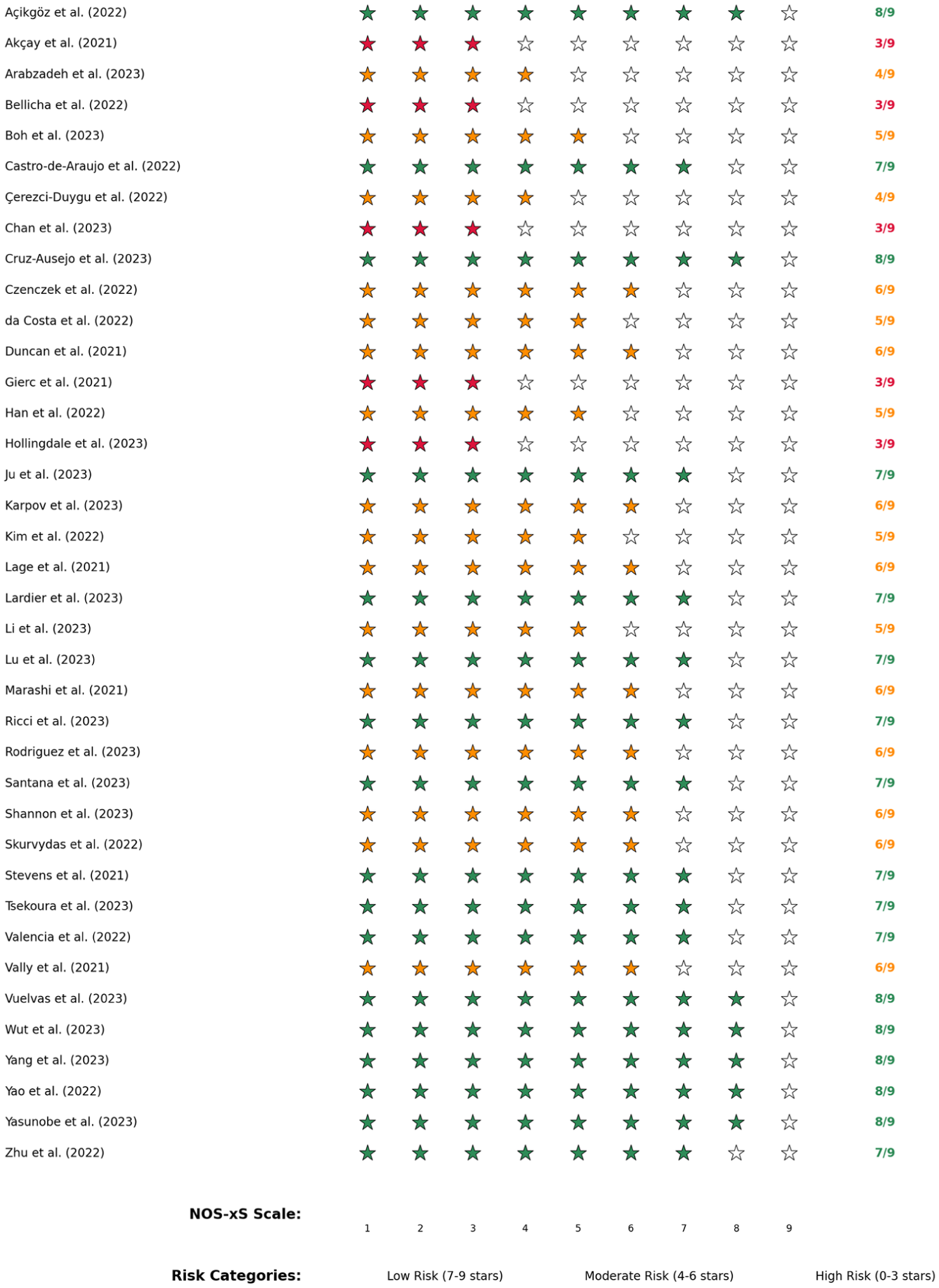
Newcastle-Ottawa Scale for Cross-Sectional Studies (NOS-xS) risk-of-bias assessment. Each study is represented by filled stars (★) indicating achieved quality points out of a maximum of 9 stars. Studies are color-coded according to the risk of bias categories: green indicates low risk of bias (7–9 stars), orange indicates moderate risk of bias (4–6 stars), and red indicates high risk of bias (0–3 stars). The numerical score (x/9) is displayed to the right of each rating.
Meta-analysis
Separate multilevel meta-analyses were conducted for depression, anxiety, and stress. For depression, 17 studies contributed 29 effect sizes from 54,972 participants. For anxiety, 13 studies contributed 21 effect sizes from 17,190 participants. For stress, five studies contributed seven effect sizes from 19,201 participants.
Publication bias assessment
Funnel plots (Figure S1—Supplemental File S5), Egger’s tests, trim-and-fill, and fail-safe N were applied to all outcomes. For depression, Egger’s test showed no asymmetry (p = 0.136), no studies were added via trim-and-fill, and the pooled effect remained unchanged (r = −0.18). Robustness remained high (Rosenthal fail-safe N = 6564; Rosenberg weighted N = 1330).
Anxiety showed no asymmetry (Egger’s p = 0.495), no added studies via trim-and-fill, and an unchanged effect size (r = −0.090), but limited robustness (Rosenthal = 269; Rosenberg = 35). Stress showed no asymmetry (Egger’s p = 0.468), no missing studies, preserved the effect (r = −0.14), and moderate robustness (Rosenthal = 111; Rosenberg = 121). Visual inspection of Figure S1 (Supplemental File S5) aligns with these patterns.
Leave-one-out sensitivity analysis
Excluding each study in turn did not materially alter pooled effects (Figure S2—Supplemental File S5). No single study drove the results. Robustness was highest for stress, moderate for depression, and lowest for anxiety.
Main meta-analytic results
Figure 3 presents the pooled associations. Physical activity was inversely associated with depression (r = −0.18, 95% CI: −0.299 to −0.062; I2 = 97.7%). For anxiety, the pooled association was small and non-significant (r = −0.09, 95% CI: −0.275 to 0.095; I2 = 99.4%). For stress, physical activity showed a significant inverse association (r = −0.14, 95% CI: −0.177 to −0.095; I2 = 29.2%).
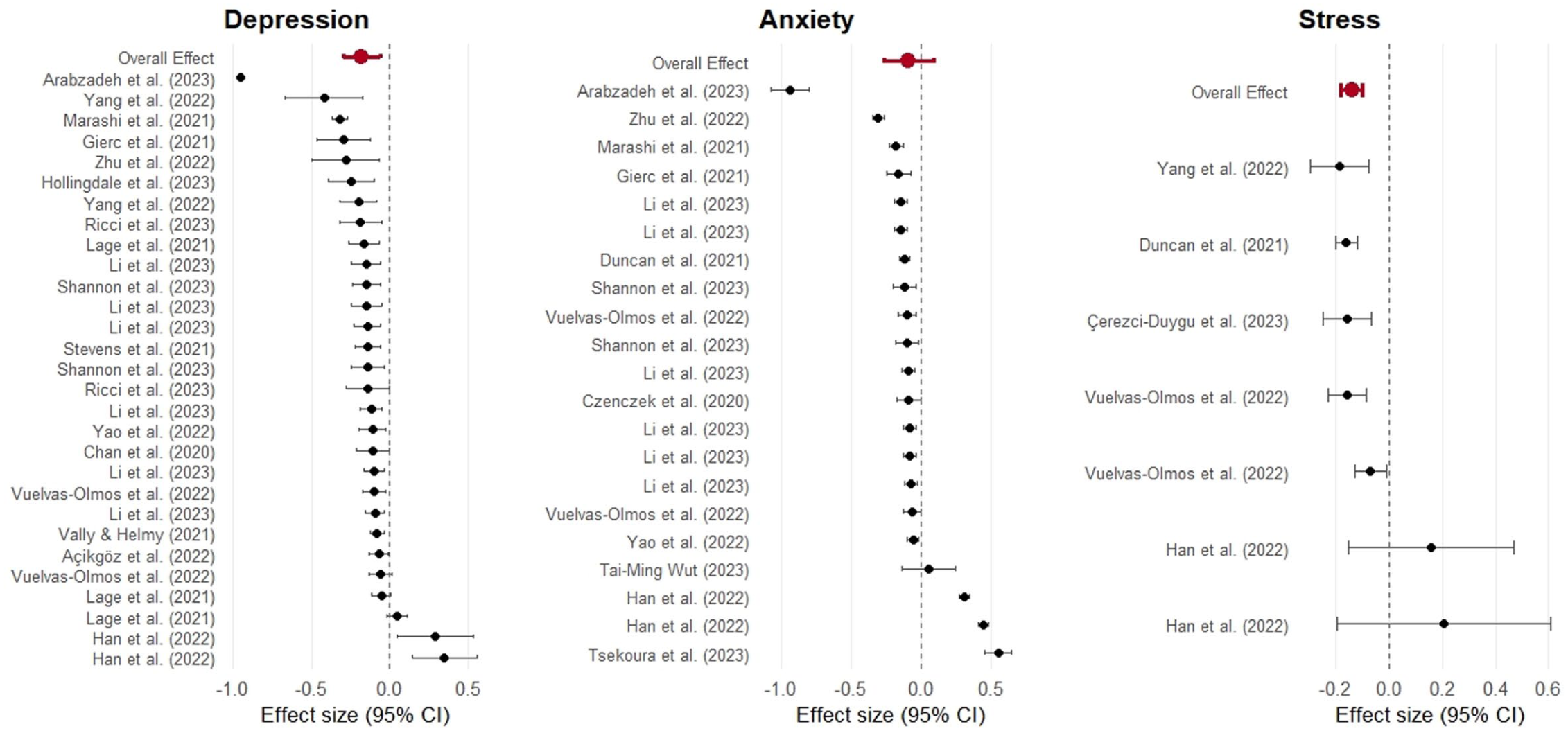
Forest plots show the association between physical activity and mental health outcomes: depression, anxiety, stress. Overall effects are shown as red round shapes; horizontal lines represent 95% confidence intervals for individual studies.
Subgroup analysis
Depression
As shown in Table 1, subgroup analyses for depression revealed significant heterogeneity across moderators. These findings are also illustrated in Figure 4, which presents the corresponding forest plots for each subgroup. First, association type significantly moderated the results (Q = 10.02, p = 0.04). Among the different association types, only studies using correlation analyses show a significant negative association between physical activity and depression (r = −0.243, 95% CI: −0.403 to −0.084). Physical activity measurement method also significantly influenced the results Q = 8.58, p = 0.013). Studies using standardized instruments to assess physical activity showed a significant negative association with depression (r = −0.195, 95% CI: −0.34 to −0.05), whereas studies using simple questionnaires did not show a significant effect (Figure 4).
Subgroup analysis of mental health outcomes in relation to physical activity during COVID-19.
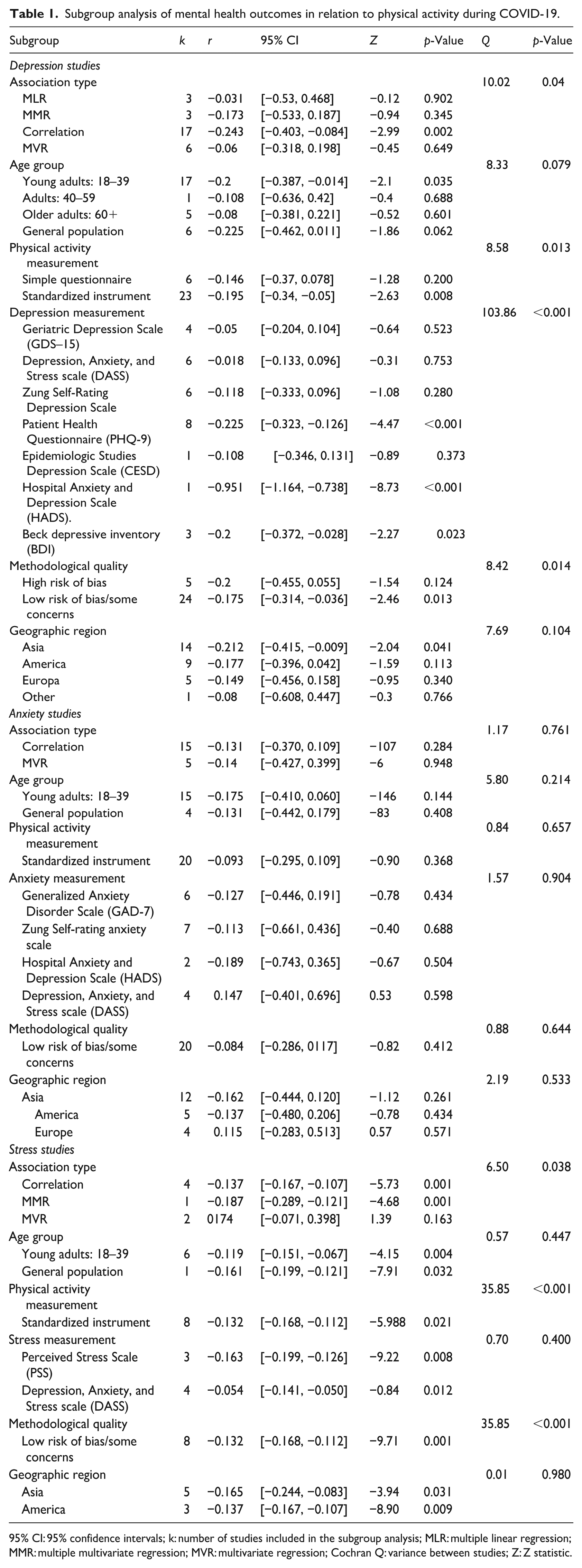
95% CI: 95% confidence intervals; k: number of studies included in the subgroup analysis; MLR: multiple linear regression; MMR: multiple multivariate regression; MVR: multivariate regression; Cochran Q: variance between studies; Z: Z statistic.
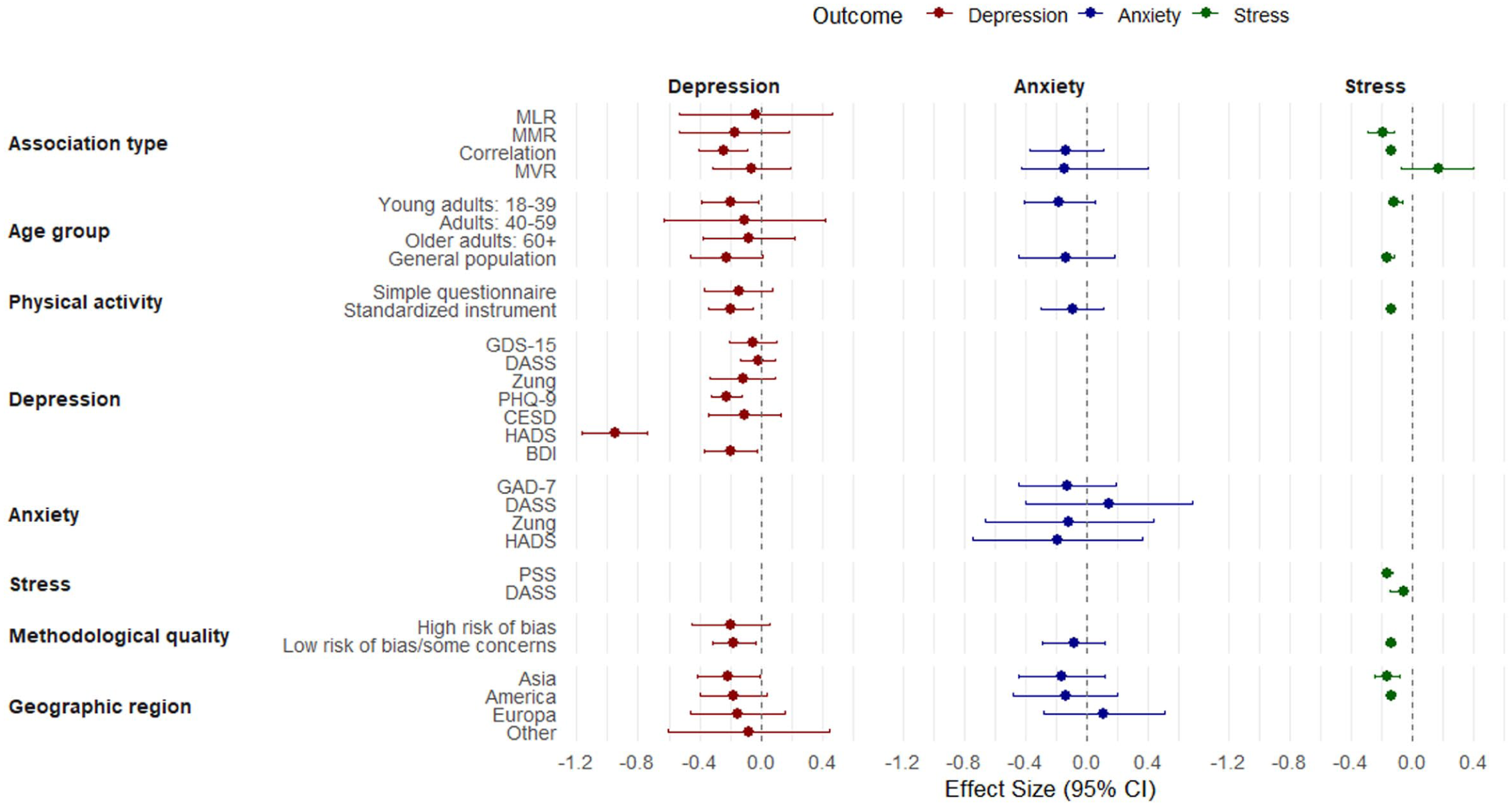
Combined forest plot of subgroup meta-analyses examining associations between physical activity and mental health outcomes (depression, anxiety, and stress). Effect sizes (with 95% confidence intervals) are shown for each outcome—depression in red, anxiety in blue, and stress in green—across key subgroup moderators such as association type, age group, and measurement methods.
Depression measurement type was a highly significant moderator (Q = 103.86, p < 0.001). As shown in Table 1 and Figure 4, the PHQ-9 (r = −0.225, 95% CI: −0.323 to −0.126), HADS (r = −0.951, 95% CI: −1.164 to −0.738), and BDI (r = −0.2, 95% CI: −0.372 to −0.028) showed significant negative associations. Other scales, including the GDS-15, DASS, Zung, and CESD, did not show significant effects. Methodological quality also significantly moderated the association (Q = 8.42, p = 0.014). Studies with low risk of bias or some concerns showed a significant negative association (r = −0.175, 95% CI: −0.314 to −0.036), whereas those with high risk of bias did not.
Anxiety
For anxiety, the available data presented in Table 1 and Figure 4 did not indicate significant moderation by association type or any other subgroup variable.
Stress
Analyses for stress identified association type as the strongest moderator (Q = 8.728, df = 2, p = 0.012). Studies using multiple mediation regression showed the strongest negative association (r = −0.207, 95% CI: −0.289 to −0.121) with no heterogeneity (I2 = 0.0%), whereas multivariate regression studies showed a non-significant positive association (r = 0.174, p = 0.1632). The remaining moderators did not significantly explain between-studies variance (See Table 1 and Figure 4).
Conversions by metric type
Results were robust across effect-size metrics. Stratified analyses (correlations vs ratios vs regression-derived) yielded consistent directions and overlapping confidence intervals for depression and stress; anxiety remained non-significant across metrics.
Cumulative meta-analysis by year
Cumulative analyses (Figure S3—Supplemental File S5) indicated that the association for depression strengthened over time, with fluctuations. Stress associations remained stable and became more precise, whereas anxiety associations weakened in more recent studies.
Certainty of evidence
Table 2 summarizes the GRADE assessment. The certainty of evidence was rated as very low for all three outcomes. For depression, 25 studies including 130,714 participants yielded a small but significant inverse association (r = −0.18, 95% CI: −0.299 to −0.062). The certainty of evidence was downgraded for risk of bias (−1) and very serious inconsistency (−2, I2 = 97.7%). For anxiety, 13 studies including 40,122 participants showed a non-significant inverse association (r = −0.09, 95% CI: −0.275 to 0.095), with downgrading for risk of bias (−1) and very serious inconsistency (−2, I2 = 99.4%). For stress, five studies including 11,627 participants showed a small but significant inverse association (r = −0.14, 95% CI: −0.177 to −0.095), with downgrading for risk of bias (−1) only.
GRADE evidence profile for the association between physical activity and mental health outcomes during the COVID-19 pandemic.
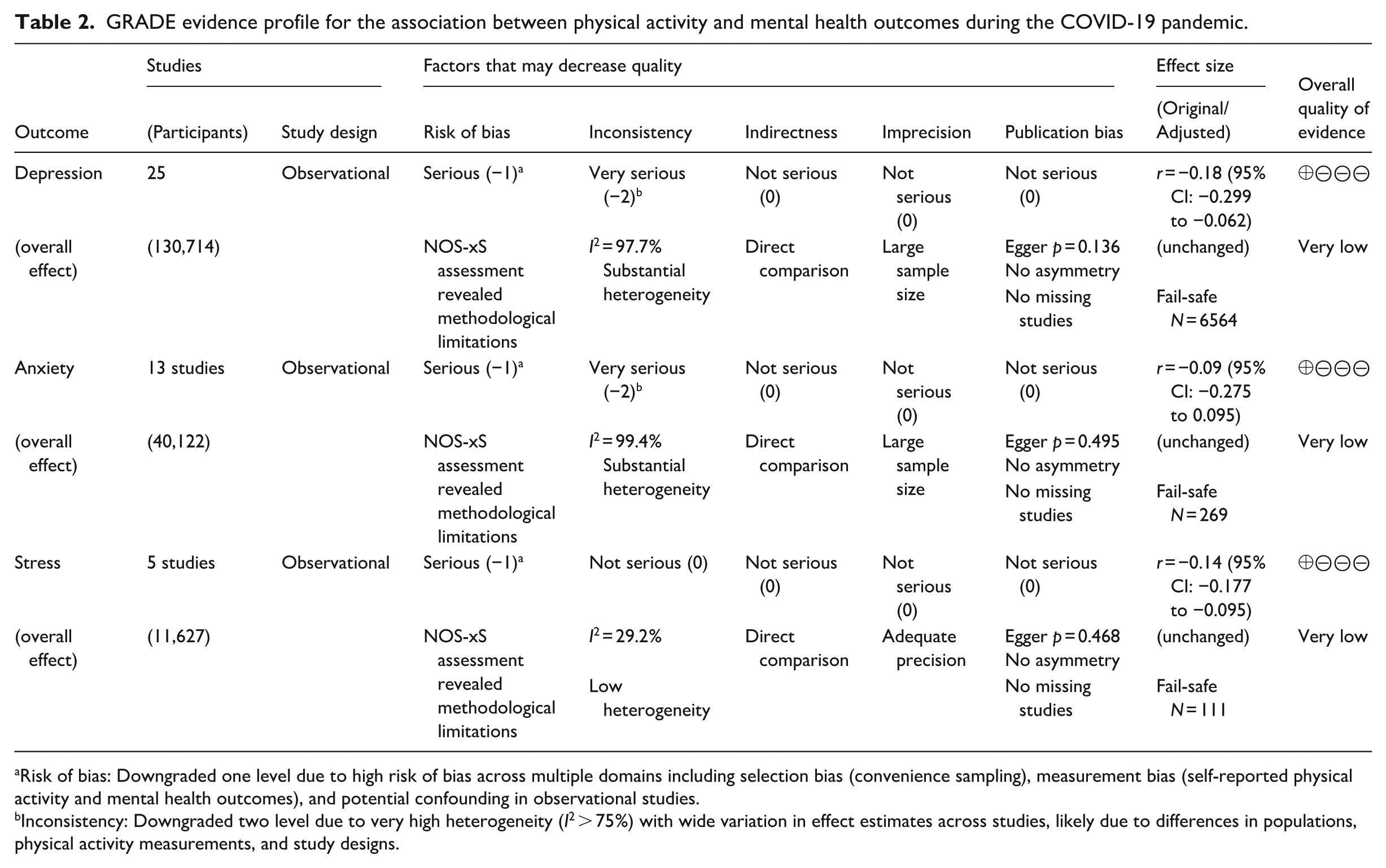
Risk of bias: Downgraded one level due to high risk of bias across multiple domains including selection bias (convenience sampling), measurement bias (self-reported physical activity and mental health outcomes), and potential confounding in observational studies.
Inconsistency: Downgraded two level due to very high heterogeneity (I2 > 75%) with wide variation in effect estimates across studies, likely due to differences in populations, physical activity measurements, and study designs.
Across outcomes, serious risk of bias reflected convenience sampling, self-reported physical activity and mental health measures, and residual confounding. Inconsistency was particularly pronounced for depression and anxiety, likely due to differences in populations, physical activity assessment, mental health instruments, and pandemic-related context. Indirectness, imprecision, and publication bias were not considered serious. Despite the very low certainty, the direction of effect was consistent for depression and stress.
Discussion
This multilevel meta-analysis of observational studies conducted during the COVID-19 pandemic provides evidence that higher physical activity was associated with lower depressive symptoms (r = −0.18, 95% CI = −0.299 to −0.062) and lower stress (r = −0.14, 95% CI = −0.177 to −0.095), whereas the association with anxiety was not statistically significant (r = −0.09, 95% CI = −0.275 to 0.095). Although these effects sizes are small according to conventional benchmarks (Cohen and Lea, 2004), they remain meaningful in the context of a prolonged global crisis, where even modest associations may translate to meaningful public health benefits when both exposure and outcome are highly prevalent (Matthay et al., 2021).
These findings are important not only as outcome patterns, but also as indicators of the psychological functions that physical activity may have served during the pandemic. Physical activity can be understood as a behavioral resource that supports coping, self-efficacy, mood regulation, stresss management, and daily structure (Bhattacharya et al., 2023; Mu et al., 2024; White et al., 2024). During COVID-19, these functions may have become especially salient because many individuals faced social isolation, disrupted routines, uncertainty, and reduced access to usual coping resources. In this context, physical activity may have supported mental health not only through physiological mechanisms, but also by providing an accessible means of emotional regulation and a sense of agency during a period of sustained disruption (Martín-Rodríguez et al., 2024; Vancampfort et al., 2025).
The inverse observed for depressive symptoms is particularly relevant. Depression during the pandemic was often linked to social withdrawal, reduced daily structure, inactivity, and diminished access to reinforcing activities. Physical activity may have helped counter these processes by maintaining behavioral activation, supporting self-efficacy, and promoting mood-regulatory effects even under restricted living conditions (Mu et al., 2024; White et al., 2024). Even modest increases in physical activity may therefore have provided psychological benefits during lockdowns by interrupting patterns of passivity closely linked to depressive symptomatology (Morse et al., 2021). In this sense, the observed association may reflect not only the well-established relationship between physical activity and mental health, but also the particular importance of movement as a coping behavior during a period marked by uncertainty and reduced everyday reinforcement (Samsudin et al., 2024; Wang et al., 2025).
The inverse association with stress is likewise consistent with a health psychology interpretation of physical activity as a stress-buffering behavior (Bhuiyan et al., 2022; Liu, 2025). During the COVID-19 pandemic, stress was shaped by uncertainty, confinement, financial strain, health fears, and major disruptions to work, family, and social routines. Under these conditions, physical activity may have helped individuals regulate arousal, reduce tension, preserve structure, and maintain a sense of control in everyday life (Bhattacharya et al., 2023; Mu et al., 2024; White et al., 2024). The observed association therefore suggests that physical activity may have functioned as a practical coping resource during widespread disruption, when many usual stress-management strategies were reduced or unavailable (Martín-Rodríguez et al., 2024; Vancampfort et al., 2025).
In contrast, the non-significant association with anxiety suggests that the mental health effects of physical activity were not uniform across outcomes. Anxiety during COVID-19 may have been more strongly shaped by fluctuating external threats —such as infection risk, uncertainty about the future, changing public health restrictions, and repeated exposure to alarming information (Wanjau et al., 2023; Wilkialis et al., 2021). These factors may have reduced the extent to which physical activity alone was sufficient to produce a stable association with anxiety across studies. It is also plausible that anxiety was more sensitive to contextual and methodological variation, including differences in pandemic phase, population characteristics, and measurement approach (Wanjau et al., 2023). Thus, the null anxiety finding should not be interpreted as evidence that physical activity is irrelevant to anxiety, but rather that its association may have been less consistent and more context-dependent under pandemic conditions.
Our findings align with and extend previous meta-analytic evidence from non-pandemic contexts (Heissel et al., 2023; Pearce et al., 2022; Wanjau et al., 2023; White et al., 2024). The depression effect size observed here (r = −0.18) is consistent with Pearce et al.’s (2022) comprehensive meta-analysis, which identified an inverse association between physical activity and depression risk and found that even minimal activity levels were associated with meaningful reductions in depression risk, with benefits plateauing at higher activity levels (Pearce et al., 2022; Schuch et al., 2018). However, the pandemic context adds specificity to this general finding. Unlike pre-pandemic studies, the included studies here were conducted under conditions of restricted mobility, disrupted routines, and reduced access to social and institutional coping resources. These conditions may have increased the relative salience of self-directed physical activity as a means of maintaining routine, managing mood, and buffering stress, potentially explaining why associations for depression and stress remained detectable even in an observational, cross-sectional literature (Heissel et al., 2023; Wanjau et al., 2023).
Physical activity may support mental health through multiple converging pathways: neurobiological pathways involving exercise-induced release of endorphins and neurotransmitter regulation (Bhattacharya et al., 2023); psychological pathways encompassing improved self-efficacy and mood regulation (Mu et al., 2024); social pathways through virtual fitness communities and outdoor exercise opportunities (Vella et al., 2023; Zhang et al., 2025); and behavioral pathways involving the maintenance of structure and routine during periods of widespread disruption (Martín-Rodríguez et al., 2024; Vancampfort et al., 2025). The relative contribution of each pathway is likely to vary across outcomes, populations, and pandemic phases, which may help explain some of the heterogeneity observed.
The substantial heterogeneity across outcomes highlights the importance of measurement quality as a moderator. For depression, significant associations emerged only when physical activity was assessed using validated instruments (r = −0.195), whereas studies employing dichotomous or brief self-report measures failed to demonstrate significant effects (Wang et al., 2025; Pearce et al., 2022). Similarly, studies with lower risk of bias showed more pronounced protective associations (r = −0.175 for depression), suggesting that methodological rigor enhances the ability to detect true associations while minimizing confounding (Schuch et al., 2018; White et al., 2024).
Temporal trends
Temporal trend analysis revealed evolving effect patterns across the pandemic. The strengthening of the physical activity-depression association over time may reflect the increasing importance of behavioral coping and routine maintenance as the pandemic shifted from acute to prolonged disruption (Samsudin et al., 2024; Wang et al., 2025). Stress-related findings appeared comparatively stable, suggesting that physical activity retained a relatively consistent role in stress regulation across phases of disruption. Anxiety associations were less stable, consistent with the possibility that anxiety was more strongly driven by changing external threats than by behavioral factors alone.
Clinical implications and limitations
These findings support the relevance of physical activity as a practical and scalable component of strategies to protect mental health during large-scale disruptions. For clinicians and public health practitioners, the results suggest that promoting feasible forms of physical activity may help support depression- and stress-related outcomes, particularly when usual services or routines are limited. However, these findings should be interpreted cautiously. The observational nature of the included studies precludes causal inference, and the substantial heterogeneity limits precision. Differences in measurement quality, study design, pandemic phase, and population characteristics likely influenced effect estimates. Reverse causation cannot be excluded, as individuals experiencing greater distress may have been less able to engage in physical activity. Even so, the consistency of the inverse associations for depression and stress across diverse study contexts suggests that physical activity may represent a meaningful component—though not a standalone solution—within broader mental health support strategies during crisis conditions.
Conclusion
This meta-analysis provides consistent evidence that physical activity was associated with lower depressive symptoms and stress during the COVID-19 pandemic, while its relationship with anxiety remained complex and requires further investigation. The findings extend pre-pandemic evidence by demonstrating that these associations persisted under conditions of restricted mobility, disrupted routines, and reduced access to usual coping resources. The importance of methodological rigor—particularly the use of validated measurement instruments—underscores the need for continued investment in high-quality physical activity and mental health research. Future work should examine the mechanisms and boundary conditions of these effects across different pandemic phases, population groups, and activity types to better inform mental health promotion strategies during future crises.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261460700 – Supplemental material for Mental health outcomes and physical activity during the COVID-19 pandemic: A systematic review and meta-analysis of observational studies
Supplemental material, sj-docx-1-hpq-10.1177_13591053261460700 for Mental health outcomes and physical activity during the COVID-19 pandemic: A systematic review and meta-analysis of observational studies by Rocío de las Nieves Pizarro Andrade, Yordanis Enriquez Canto, Roger Joaquín Angulo Salas, Claudia Rebeca Cahui Ramirez and Giovani Martín Díaz Gervasi in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053261460700 – Supplemental material for Mental health outcomes and physical activity during the COVID-19 pandemic: A systematic review and meta-analysis of observational studies
Supplemental material, sj-docx-2-hpq-10.1177_13591053261460700 for Mental health outcomes and physical activity during the COVID-19 pandemic: A systematic review and meta-analysis of observational studies by Rocío de las Nieves Pizarro Andrade, Yordanis Enriquez Canto, Roger Joaquín Angulo Salas, Claudia Rebeca Cahui Ramirez and Giovani Martín Díaz Gervasi in Journal of Health Psychology
Supplemental Material
sj-docx-3-hpq-10.1177_13591053261460700 – Supplemental material for Mental health outcomes and physical activity during the COVID-19 pandemic: A systematic review and meta-analysis of observational studies
Supplemental material, sj-docx-3-hpq-10.1177_13591053261460700 for Mental health outcomes and physical activity during the COVID-19 pandemic: A systematic review and meta-analysis of observational studies by Rocío de las Nieves Pizarro Andrade, Yordanis Enriquez Canto, Roger Joaquín Angulo Salas, Claudia Rebeca Cahui Ramirez and Giovani Martín Díaz Gervasi in Journal of Health Psychology
Supplemental Material
sj-docx-4-hpq-10.1177_13591053261460700 – Supplemental material for Mental health outcomes and physical activity during the COVID-19 pandemic: A systematic review and meta-analysis of observational studies
Supplemental material, sj-docx-4-hpq-10.1177_13591053261460700 for Mental health outcomes and physical activity during the COVID-19 pandemic: A systematic review and meta-analysis of observational studies by Rocío de las Nieves Pizarro Andrade, Yordanis Enriquez Canto, Roger Joaquín Angulo Salas, Claudia Rebeca Cahui Ramirez and Giovani Martín Díaz Gervasi in Journal of Health Psychology
Supplemental Material
sj-docx-5-hpq-10.1177_13591053261460700 – Supplemental material for Mental health outcomes and physical activity during the COVID-19 pandemic: A systematic review and meta-analysis of observational studies
Supplemental material, sj-docx-5-hpq-10.1177_13591053261460700 for Mental health outcomes and physical activity during the COVID-19 pandemic: A systematic review and meta-analysis of observational studies by Rocío de las Nieves Pizarro Andrade, Yordanis Enriquez Canto, Roger Joaquín Angulo Salas, Claudia Rebeca Cahui Ramirez and Giovani Martín Díaz Gervasi in Journal of Health Psychology
Supplemental Material
sj-docx-7-hpq-10.1177_13591053261460700 – Supplemental material for Mental health outcomes and physical activity during the COVID-19 pandemic: A systematic review and meta-analysis of observational studies
Supplemental material, sj-docx-7-hpq-10.1177_13591053261460700 for Mental health outcomes and physical activity during the COVID-19 pandemic: A systematic review and meta-analysis of observational studies by Rocío de las Nieves Pizarro Andrade, Yordanis Enriquez Canto, Roger Joaquín Angulo Salas, Claudia Rebeca Cahui Ramirez and Giovani Martín Díaz Gervasi in Journal of Health Psychology
Supplemental Material
sj-xlsx-6-hpq-10.1177_13591053261460700 – Supplemental material for Mental health outcomes and physical activity during the COVID-19 pandemic: A systematic review and meta-analysis of observational studies
Supplemental material, sj-xlsx-6-hpq-10.1177_13591053261460700 for Mental health outcomes and physical activity during the COVID-19 pandemic: A systematic review and meta-analysis of observational studies by Rocío de las Nieves Pizarro Andrade, Yordanis Enriquez Canto, Roger Joaquín Angulo Salas, Claudia Rebeca Cahui Ramirez and Giovani Martín Díaz Gervasi in Journal of Health Psychology
Footnotes
Author note
This review was registered with PROSPERO (CRD42023491651).
Ethical considerations
Ethics approval was not required for this review article as no data were collected from participants.
Consent to participate
Consent to participate is not applicable to this review article as no data were collected from participants.
Consent for publication
Consent for publication is not applicable to this review article as no identifiable participant data are included.
Author contributions
RNPA conceived the study idea and contributed to the development of the research question and conceptual framework. YEC led the project, designed the systematic review and meta-analytic methodology, supervised all stages of the study, and conducted the statistical analyses. RJAS contributed to data extraction, methodological quality assessment, and drafting of the Methods and Results sections. CRCR participated in screening, data extraction, and verification of extracted data, and contributed to the interpretation of findings. GDG supported literature searches, reference management, and contributed to the writing and critical revision of the manuscript. All authors reviewed and approved the final version of the manuscript. RNPA and YEC contributed equally to this work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data generated or analyzed during this study are included in this published article and its Supplemental Information files.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.