
Abstract
Stoma surgery can bring significant physical and psychological changes to an individual’s life. This study explored the experiences of living with a stoma and body image. 12 semi-structured interviews were conducted with women who underwent permanent stoma surgery due to either colorectal cancer, Crohn’s disease or ulcerative colitis. Thematic analyses revealed three key themes: (A) Adjusting to a new reality; (B) Lack of representation; (C) Moving forward. Results indicated that women with a stoma face an array of life changes, particularly surrounding struggles with body image post-surgery. All participants expressed that the presence of a stoma has had a negative impact on body image, with more pronounced concerns among colorectal cancer patients. The need for a more integrated approach for assessing and supporting those with stoma-related psychological symptoms is highlighted.
Introduction
The creation of a stoma is a common therapeutic intervention applied to a variety of chronic and acute conditions of the colon including colon cancer, ulcerative colitis and Crohn’s disease (Stavropoulou et al., 2021). A stoma is a surgically formed opening in the bowel, which is created to assist with the elimination of waste from the body (Sharpe et al., 2011). There are three main types of stomas and, depending on the extent of the disease and patients’ health, stomas may be temporary or permanent. A colostomy is a type of stoma where an opening is created in the large intestine and is a common procedure for patients of bowel or colorectal cancers. An ileostomy stoma creates an opening in the small intestine and is more common for patients with Crohn’s disease, ulcerative colitis and Inflammatory Bowel Disease (IBD). Finally, a urostomy stoma diverts the ureters to the abdomen. While colorectal cancer and IBD may present with similar gastrointestinal symptoms, colorectal cancer is characterised by progressive symptoms such as weight loss and anaemia while IBD can give rise to severe, long-lasting symptoms such as vomiting, diarrhoea and abdominal pain (Polidano et al., 2020). Stoma surgery aims to reduce debilitating symptoms such as chronic pain caused by inflammation in the bowel and improve overall health quality (Black, 2004). Furthermore, stoma surgery can reduce the impact of symptoms, such as constant pain or diarrhoea, which may have interfered with one’s work, hobbies and social activities (Petersén and Carlsson, 2021). Currently, there are no national statistics for stoma surgery in Ireland; however, it is proposed that there are approximately 2500 ostomy creations annually for the treatment of colorectal cancer, ulcerative colitis, Crohn’s disease and other inflammatory bowel diseases (Walsh, 2023). Given that colorectal cancer is now the second most common cancer in Ireland for both men and women (National Cancer Registry Ireland, 2024), for many individuals this intervention can be lifesaving.
Circumstances for needing a stoma can vary depending on each patient and can profoundly influence the initial thoughts and feelings experienced following the surgery. For those with cancer, stoma surgery may occur unexpectedly and can be a profound shock; conversely, for patients with chronic inflammatory diseases, stoma surgery may be a more positive experience and make life more predictable with reduced pain (Mørkhagen and Nortvedt, 2023). Post-surgery, increased control over the body may be experienced by those with inflammatory bowel disease (IBD) whereas for most cancer patients, stoma surgery stops the progression of the disease. While the physiological benefits of stoma surgery are clear, the psychological impact of stomas is profound and often complex.
Psychological impacts of stoma surgery
Living with a stoma can give rise to many challenges resulting from both physical changes to one’s body and psychological adaptations (Knowles et al., 2017). In recent years, researchers have begun to explore the psychological implications that arise following stoma surgery (Capilla-Díaz et al., 2019; Di Gesaro, 2016; Jayarajah et al., 2016). Several studies report that reduced social functioning, difficulties with intimacy, anxiety, embarrassment and body image issues are experienced by those who live with a stoma, and over time have a detrimental impact on the patient’s overall quality of life (Black, 2004). Ross et al. (2007) compared a stoma group versus a non-stoma group and found differences in social functioning and sexual issues between the two groups. Depression and anxiety levels were significantly higher among the stoma participants.
Several factors contribute to a poorer psychological outcome following stoma surgery such as poor preoperative preparation (White and Hunt, 1997) and complications relating to the stoma itself (Pittman et al., 2009). Despite evidence of poor psychological outcomes following stoma surgery, these issues are often overlooked by medical professionals (Di Gesaro, 2016). Some researchers have suggested that the psychological issues experienced by individuals with a stoma outweigh the physical issues (Mørkhagen and Nortvedt, 2023). The existence of a stoma is associated with several unfamiliar changes, both bodily and psychological (Honkala and Berterö, 2009). However, the circumstances that lead to someone needing a permanent stoma can greatly impact one’s perception of it and the extent of psychological problems associated with the stoma. Polidano et al. (2020) showed that psychological problems in patients with IBD following stoma surgery were present; however, the patients also reported positively about living with the stoma particularly regarding their liberation from IBD symptoms. Conversely, for those who received a stoma following a diagnosis of cancer, the diagnosis itself can be an extremely distressing time for the patient. Thus, the addition of a stoma can exacerbate these feelings of distress, leading to a heightened sense of loss and discomfort (Smith et al., 2017).
Body image
The formation of a stoma involves breaching body boundaries and can significantly change how one’s body looks and functions (Taylor, 2015). One of the most common negative psychological effects noted by women living with a permanent stoma was that of an altered body image (Redeker et al., 2025). Body image is an umbrella term used to describe perceptions, cognitions, behaviours and subjective evaluations of one’s body (Frederick et al., 2022). It is a complex multifaceted construct, involving perceptions and evaluations of one’s body with many positive and negative subcomponents such as body dissatisfaction, body-esteem, shame, body acceptance and appreciation (Thompson et al., 1999). Disturbances in body image have been defined as a persistent report of dissatisfaction, concern and distress associated with an individual’s physical appearance and is associated with impairment in social functioning and activities (Jayarajah et al., 2016). One’s body image is constantly changing during different stages of life and can be influenced not only by physical (e.g. body shape) or psychological factors (e.g. low self-worth, perfectionism) but also social (e.g. unrealistic beauty standards, social media) and personal circumstances (McLean et al., 2011). Historically, research has focused on the limited notion that body image issues solely involve body weight and shape, yet it is essential to look beyond this limited scope and examine the rich diversity of human experience and how it can influence body image. This includes challenges faced by individuals who have undergone significant physical changes, such as those who have undergone stoma surgery.
Body image following stoma surgery
An ostomate is an individual who has undergone a surgical procedure to create a stoma. People with bodies that are changed dramatically and at times irreversibly must adapt to a new bodily reality, which can be extremely difficult (Manderson, 2005). Much literature has highlighted these difficulties in relation to physical alterations from medical treatments such as surgery that has involved reconstruction such as mastectomy (Przezdziecki et al., 2013). To date, there is only a small body of literature exploring the impact of a stoma on body image; however, the existing literature indicates that individuals, particularly women, living with a stoma often experience significant disturbances in body image. In a study by Sharpe et al. (2011), women living with a stoma reported much higher body image disturbances than women who did not. Jayarajah et al. (2016) reported that women with a stoma experienced lower value as a woman compared to ‘healthy women’, and that the presence of the stoma on their body made them feel uncomfortable and unclean. As suggested by Black (2000), coming to terms with a new body image after a life-altering surgery is an interpersonal experience for ostomates and the way in which people respond depends on their attitudes, thoughts and feelings they have towards his or her own body.
According to Benedict et al. (2016), 40% of colorectal cancer patients experienced clinically meaningful body image problems in their first-year post treatment. In a similar study, disturbances in body image among colorectal patients was an independent predictor of depression, anxiety and distress following surgery (Sharpe et al., 2011).
The body image impacts of stoma surgery extend beyond self-esteem and self-confidence and may significantly impair one’s sexuality and sexual functioning. Understandably, perceptions of reduced attractiveness following stoma surgery can also affect intimate relationships, with patients experiencing concerns regarding sexual functioning, activity and overall intimacy (Black and Notter, 2021). Common worries around sexual functioning include the visibility of the stoma, incontinence accidents, embarrassment and feelings of un-attractiveness (Sharpe et al., 2011). Davidson (2016) found that ostomy patients reported that the presence of the stoma significantly impacted sexual activity. These concerns were most reported by those with a permanent stoma or who had undergone colorectal surgery (García-Rodríguez et al., 2021). Sexual problems are another critical aspect of body image and, like other psychological impacts of stomas, are often overlooked.
A stoma also presents a unique challenge in the context of body image due its concealed nature, meaning that it is invisible to others and may only ever be visible to the person with whom it is connected to. The hidden aspect of the stoma contrasts with the profound presence it can have on an individual’s perception of their body. People who are coping with a significant body alteration such as receiving a stoma are likely to experience difficulties between their internal world and their new public identity (Black, 2012). The invisibility of the stoma to others demonstrates that body image disturbances are not only related to how other people perceive us but also how we perceive ourselves.
This study
At present, most studies in the field of stoma related body image research have suffered from an overemphasis on quantitative measures and fail to look at the importance of lived experiences. Given that females are more likely to be concerned with body image and tend to suffer with more body image disturbances, this study will be focusing solely on women living with a permanent stoma. Given the life altering nature of the procedure, this study further aims to explore how pre- and post-operative support may influence participants’ adaptation to an altered body image.
Method
Design
A qualitative research approach was used to provide a rich and holistic picture of women’s lived experience of body image following stoma surgery.
Participants
This study comprised 12 participants between the ages of 35–60 years of age. All participants were female and currently residing in Ireland. All participants met the following inclusion criteria: (1) women who are 18 years and older, and (2) currently have a permanent stoma. The duration of time each participant was living with the permanent stoma at the time of interview varied between 6 weeks and 12 years. Among the participants, seven received a stoma due to colorectal cancer, two due to Crohn’s disease and three because of ulcerative colitis.
A purposive sampling method was predominately used to recruit participants. Purposive sampling aims to recruit participants that are ‘most likely to yield appropriate and useful information’ (Kelly, 2010: 317). Participants were recruited based on predefined criteria that aligned with the research topic. Participants were recruited through an online support group for ostomates in Ireland, allowing access to a population with lived experience of stoma surgery. Snowball sampling also enabled the researcher to recruit participants as suggested by other participants. As the study population aimed to consist of women who have received a permanent stoma, online stoma support groups advertised it to members of the group.
Procedure
Data collection was performed through semi-structured interviews and took place between the months of April and June 2024. The use of semi-structured interviews allowed for the collection of rich data from the participants, who were given the opportunity to speak freely about the research topic. Prior to the interview, the participants were provided with an interview schedule containing a series of open-ended questions that invited the participants to describe their experiences living with a permanent stoma. Examples of questions to participants included the following: ‘Has your body image been impacted since receiving a permanent stoma and, if so, how?’, ‘How has your experience with the Irish Health System been in terms of support received?’, ‘Do you feel you have accepted the stoma as a part of your body?’, ‘In what ways do you think patients could be better supported following stoma surgery?’.
Basic demographic information (e.g. age and circumstances that led to needing a stoma) were also collected. All interviews were conducted online via Zoom. Following the interview, each participant was emailed a debriefing sheet that contained relevant psychological support services should they need to avail of them. Once data saturation had occurred, the data collection phase was then complete. In this study, data saturation was reached once 12 interviews were completed. The recorded data was then transcribed verbatim for analysis and pseudo-anonymised, meaning that all identifiable information was removed from the transcript to safeguard participant’s privacy.
Data analysis
Data analysis was carried out under the principles of thematic analysis developed by Braun and Clarke (2006). An inductive, bottom-up approach was taken which meant that the development of codes and themes were directed by the data itself (Braun and Clarke, 2021a). This was a recursive process, following the six-step framework as outlined by Braun and Clarke (2006).
Researcher positioning
Data were interpreted from a critical realist epistemological standpoint. Participant experiences were considered approximations of reality, underpinned by existing social and psychological constructs (Willig, 2013). This approach was chosen over alternatives following reflection by the lead investigator on her own theoretical approach to research. She adopted an anti-authoritative role as an interviewer, with participants positioned as experts on their own condition; the researcher assumed the outsider role when clarifying health or medical terminology (Braun and Clarke, 2021b).
Ethical considerations
This study received ethical approval from the University on the 28th of March 2024.
Results
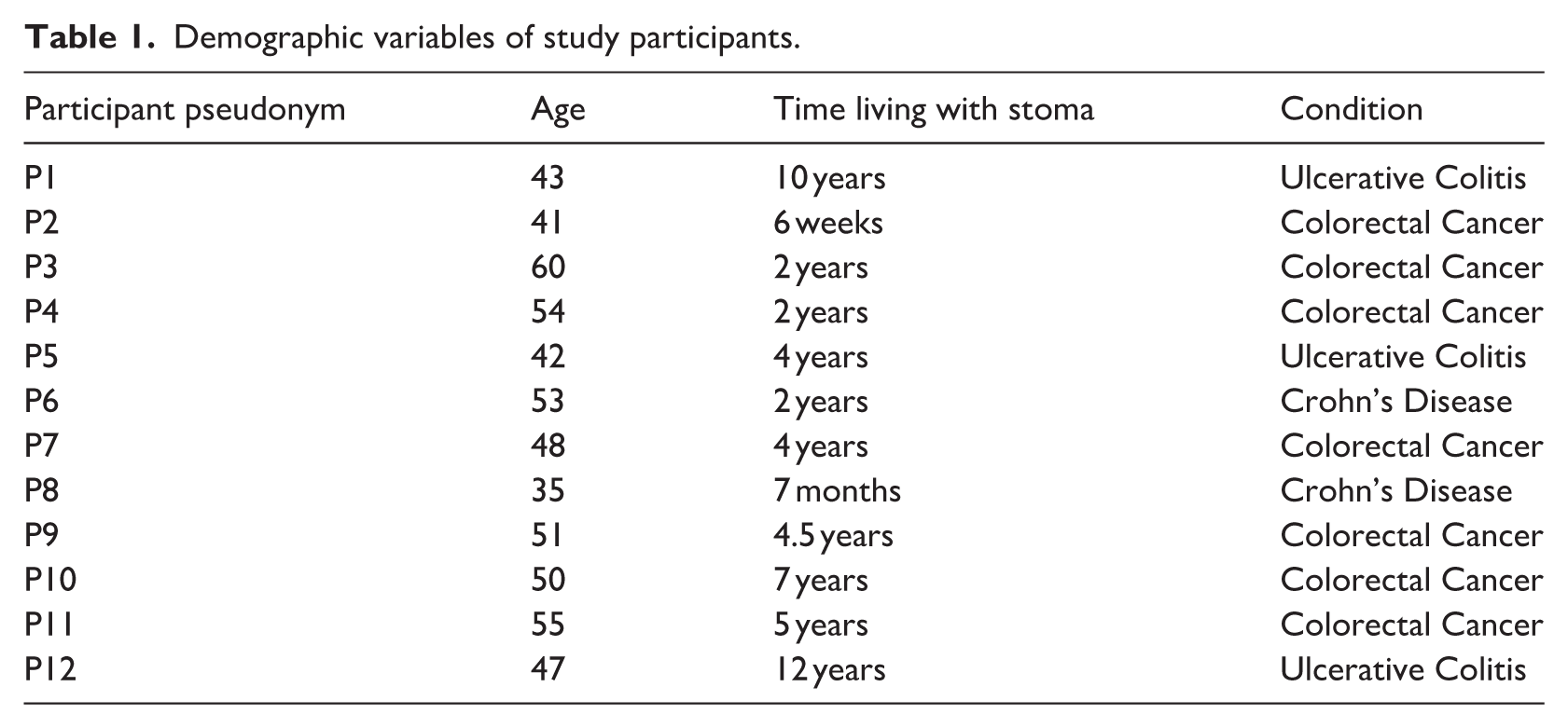
Demographic information for each participant is provided in Table 1. All participants had a permanent stoma and either a condition of Crohn’s disease, ulcerative colitis or a previous diagnosis of colorectal cancer.
Demographic variables of study participants.
The main overarching themes were identified: (1) Adjusting to a new reality, (2) Lack of representation and (3) Moving forward. Six relevant sub-themes were identified within the data, namely: A changed body, Coping through concealment, The need for support, Stigma and silence, Path to acceptance and Prioritising health. The relationships between themes and subthemes can be viewed in Figure 1 below.

Relationships between themes and subthemes.
Adjusting to a new reality
All participants spoke about their experiences with an altered body image post stoma surgery. Participants who received a stoma as a result of a diagnosis of colorectal cancer expressed far greater disturbances in body image and overall, more psychological impacts than those who received the stoma either due to Crohn’s disease or ulcerative colitis. Each participant shared their difficulties and ways of coping with the stoma and alterations in body image, which are identified through two sub-themes: (i) A Changed Body and (ii) Coping through Concealment.
A changed body
A recurrent theme in the interviews was a sense among the participants that the presence of a permanent stoma had significantly impacted how they perceive their body image, and over all sense of self. Extreme emotions were expressed by participants in relation to how their body looked following surgery, with the majority of participants expressing that adjusting to an altered body image was the hardest challenge of all.
I think it’s the body image bit of it is what I struggle with the most, like the practical side of it I could do in my sleep (Participant 9)
Physical changes such as weight-gain, scars and lumps were also discussed as side effects that emerged following surgery: I’m not very comfortable at all if I could change my body back to what it was I would in a heartbeat. . . My whole body is very scarred and there’s lumps and bumps now where there never were before (Participant 2)
Participants who received a stoma following a diagnosis of colorectal cancer highlighted their concerns about the functionality of their bodies following such an aggressive illness, fearing it no longer works as it used to: I’m very conscious that it (body) is broken and that it’s weak. . . I don’t feel like me in this body but a defective stranger. (Participant 4)
Coping through concealment
A predominant concern among participants was feeling uncomfortable looking at their own body. Consequently, some participants admitted to covering or hiding the stoma as a way of coping. In order to minimise its visibility for themselves and others, participants expressed ways in which they would conceal the stoma from view by wearing specific types and coloured clothing. Anxiety and fear over trying to disguise the stoma from the view of others undoubtedly seemed to overwhelm the participants’ daily routines.
I mean now I always have something there that I have to disguise. . . I always try to cover this area of my body or stand in a way where it wasn’t obvious. You have to be careful of things and adjust what you wear. . . you’d have to think carefully of colours, darker colours, maybe. . .. (Participant 5)
The creation of the stoma affected many individuals’ lifestyle and the things they enjoy doing. Participants discussed their concerns about feeling embarrassed about people seeing their stoma and choose to avoid some social situations. One participant spoke about the extent she would go to prevent someone from seeing the stoma on her body: “I’m very conscious that it is very visible underneath my leggings. So, I don’t go to an ordinary gym with other people. I just go to a person trainer on my own, and I make sure that I’m the only person in the room there.” (Participant 4)
It was clear from the interviews that by concealing the stoma, some participants feel more comfortable with their bodies, particularly in social situations, allowing them to maintain a sense of normality.
The need for control over ways to hide the stoma and prevent who sees it is evident among the participants as a way of coping. Many explained how they no longer wear jeans as they are too restrictive and make the stoma more visible. One participant commented on their love for fashion and retro clothing prior to stoma surgery but has since had to discard many pieces of clothing as they are no longer suitable for her or her body: “My body has really changed, so retro dresses that I had before my surgery that I loved, I can’t wear now . . .. If you want to wear a dress, you’d have to really try to hide it . . .. I would feel like people could see the shape of it. You’re always looking at clothes that will actually hide it and not make it stand out” (Participant 9)
Participants who concealed their stoma appeared to experience greater levels of body image disturbances, whereas those who adopted a more open approach tended to express greater acceptance.
A lack of representation
A clear theme that emerged from the interviews was the lack of support and representation for female ostomates. Many participants expressed feeling stigmatised given the lack of conversation and support surrounding body-image, intimacy and femininity following stoma surgery.
The need for support
A common viewpoint among participants was that their only form of psychological support was either through online Facebook group chats or an occasional visit from a stoma nurse. Stoma nurses were mentioned throughout most of the interviews as a positive channel of support following stoma surgery; however, these nurses were only able to assist in the physical adjustment to the stoma. While reflecting on the psychological support they received following stoma surgery, participants felt they were not supported when they needed it most and expressed desires for future support to be put in place.
My major problem with the Irish health system is that everything is based around your physical recovery. Nobody ever talks to you about the psychological turmoil you will go through accepting your stoma post-surgery. There should be counselling around this (Participant 2)
This view was echoed by another participant, who stated: . . . there needs to be a multidisciplinary team approach to something as life altering as stoma surgery, because nobody looks after the psychological effects of it (Participant 4).
Participants overwhelmingly stressed the need for psychological support for all stoma patients both before and after surgery. Despite three Crohn’s and Ulcerative colitis patients highlighting that they personally did not need follow-up psychological support given the increased quality of life they received post-surgery, they too expressed concern over the lack of support provided to patients.
I don’t think there is enough support at all. . . for me personally, I didn’t need it. . .. but I don’t think there’s enough after care for people like support wise . . . because it is hugely life altering for so many people (Participant 1)
Many participants stated that the lack of support received following surgery further exacerbated body image struggles. Education and knowledge around suitable clothing were factors mentioned as ways to help at the beginning stages of adjusting to one’s body image post-surgery.
You’re left to your own devices . . . they don’t contact you. They don’t go through different clothes that would suit . . . you know the way if they had something where they might give you tips in the beginning when you’re a bit less confident in your body (Participant 11)
Looking ahead, one participant shared their hopes that the system will change in the future given the rise in numbers of people requiring stomas: . . .. it’s absolutely crazy that they’re not putting any resources in place to make sure that people are living happy and healthy lives with a stoma, because a lot of people are getting stomas at all ages, and they should really be putting the psychological supports in place now. . . hopefully in time (Participant 4)
Stigma and silence
Despite a rising number of individuals requiring stoma surgery in Ireland, many participants felt that the topic of stomas is still considered taboo. Some participants expressed feeling marginalised following stoma surgery given the prevailing public perception of stomas and the lack of conversation surrounding women with stomas. This silence and lack of representation has led to women feeling inadequate in terms of their own body image and what it means to be feminine. One participant highlighted this contrast between stomas and societal views of femininity.
. . . it’s just very unfamiliar and it’s quintessentially unfeminine. It’s just very unfeminine . . . I feel like women with stomas are unrepresented in this country. People don’t want to talk about women and bowel movements. It’s not like menstruation where 50% of the population are going to go through it. And every the other 50% of the population must get used to it. This is something very taboo and very stigmatizing (Participant 10).
The creation of a stoma also significantly impaired some participants’ intimacy and sexual life. Four participants shared the silence that surrounds living with a stoma, particularly when discussing topics such as intimacy and sexual confidence post-stoma surgery. As some participants struggle with integrating a new body image and intimacy post-surgery, the lack of discussion left some feeling extremely isolated.
. . .. But the whole thing about sexuality and stoma surgery is massive and it is really, really difficult and there is nobody to talk to about that nobody and nobody ever discusses it, not even on the Facebook pages. So, you are left completely alone and I’m only 50. I’ve got another 20 or 30 years of marriage ahead of me . . . and so where do you go with that? I don’t know . . . (Participant 7)
Disturbances in body-confidence are evident in situations involving physical intimacy, as described by one participant who described how this drop in body-confidence experienced following stoma surgery has had an impact on her sexual life.
I think my confidence has dropped with regard to being intimate with people and people seeing my body in that way. At the minute I don’t feel comfortable with people seeing me naked (Participant 8)
Moving Forward
The majority of participants spoke to their experiences of moving forward with their lives following stoma surgery.
Path to acceptance
The sub-theme of acceptance emerged prominently: each participant spoke about her journey towards accepting the stoma as a part of their body. It was evident that participants who received a stoma following a diagnosis of Crohn’s or ulcerative colitis were more accepting of the stoma. Although a handful of participants who had a previous diagnosis of colorectal cancer had not fully accepted the stoma at the time of their interview, they acknowledged that acceptance would come with time. Many highlighted the life-saving nature of the stoma, which helped lessen the burden of the psychological and body image impacts it has had.
. . .Well, I probably don’t have a choice. If I look at the bigger picture of it saved my life so I just have to accept it as a part of me now even when it doesn’t feel normal or natural (Participant 2).
Similarly, another participant spoke about the interplay between their gratitude and body image concerns. This participant felt that although the stoma saved her life, grappling with an altered body image and stigma associated with stomas was a struggle at times.
It’s just . . . It’s not pink and it’s not pretty like other things and it makes you feel un-pretty, but it’ll be fine eventually . . . it’ll usually improve our lives a lot and for me it saved my life, so I just need to put up with not always liking how I look (Participant 10)
The level of acceptance felt by the participants was influenced by the individual experiences that led to them requiring stoma surgery. For some colorectal patients, the stoma is a constant reminder of their cancer diagnosis whereas for Crohn’s patients, the stoma serves as a symbol of relief from previous pain and discomfort. One participant who had Crohn’s for most of her life recognised the unique circumstances surrounding each stoma patient’s journey towards acceptance by stating: I accepted my stoma the day I got it because I had no alternative. My path to it was different so, therefore, my outlook is just different (Participant 6)
Discussion
This study aimed to understand the experience of having a permanent stoma on body image and to examine how women cope and adapt to such changes. All participants expressed that their stoma has negatively impacted their body image. This is consistent with existing literature which highlights that body image struggles are one of the most frequent difficulties expressed by stoma patients (Stavropoulou et al., 2021). Difficulties in adjusting to such alterations in body image are prevalent among female ostomates. Patients’ efforts to adapt and cope with alterations in body image are evident through concealment of the stoma, acceptance and prioritising health. Lack of support from the health system and silence around topics such as intimacy and stomas in general led to increased struggles with body image and overall poorer psychological outcomes.
One of the main findings from this study was that although changes in body image were expressed by all participants, those who received a stoma as a result of cancer noted far more disturbances than those with IBD. Several of the colorectal cancer patients described the daily discomfort of looking at changes to their body, expressing how they no longer feel comfortable or confident in their bodies post-surgery. Honkala and Berterö (2009) similarly found that women feel as if they do not experience themselves as having a normal body anymore. Participants felt particularly uncomfortable in social situations or during sexual activity due to changes in body shape and weight, leading to a drop in self-esteem and confidence. This is in accordance with other studies (e.g. Petersén and Carlsson, 2021). As summarised by Black (2000), changes in body image post-surgery may result in ‘mourning’ for the body part that no longer works as it used to, which is evident among colorectal patients who feared their body was now a broken, weaker shell of what it was.
All participants strived adapt to alterations in body image, and to seek ways to gain a sense of control of their new life. As cited by Taylor (2015), finding coping strategies can help reduce the gap between body ideal and body reality. Concealment of the stoma was a strategy used as a way of coping with body image struggles and the negative emotions associated with the stoma. In order to cope with low self-esteem and a drop in body confidence, particularly in social situations, participants opted to conceal their stoma from the view of others. Thorpe et al. (2009) similarly highlighted that some stoma-patients felt the need to hide body image struggles when meeting people in social settings. A new sense of control emerges when coping strategies such as concealment are learned (Petersén and Carlsson, 2021). Due to their bodies looking differently, participants expressed worries about people seeing the stoma underneath their clothing, a finding which mirrors those of Danielsen et al. (2013) The sub-theme of concealment is consistent with data obtained by Palomero- Rubio et al. (2018), who found that daily life is both limited and complicated for stoma patients, as it involves constant planning.
Similar to findings from Simmons et al. (2007), those who had accepted their stoma were better adjusted. From the interviews, participants who had their stoma for a longer period of time and who had a more positive outlook appeared to be better adjusted to it. Higher levels of resilience have been associated with an overall more positive adjustment to a permanent stoma (Scardillo et al., 2016).
Body image is just one of the many psychological impacts of living with a stoma and at present, the psychological needs of stoma-patients are not being met. As highlighted by Polidano et al. (2021), despite stoma surgery being considered as a ‘life-changing’ event, there is currently a lack of attention dedicated to how stoma-related psychological concerns are addressed and treated by healthcare professionals. Participants in this study unanimously expressed the need for psychological support from the Health Service Executive (HSE) following stoma surgery. While the finding that stoma nurses act as a positive source of support for stoma-patients mirrored that of existing literature (Burch, 2017), participants in this study felt that stoma nurses were only there to provide support for the physical adaptation to life with a stoma, rather than the psychological.
Any support received by participants in this study was sought privately. Currently, the lack of access to psychological support is leading to poorer psychological outcomes, including those relating to body image, similar to the responses from participants in another study (Knowles et al., 2013). Furthermore, as seen from the demographics of the participants, younger women are needing stomas. As such, it is important that sufficient support and education is provided to ensure a smooth adjustment to life with a stoma and to minimise the negative impacts associated, such as body image disturbances.
Sexuality is closely linked to body image. In accordance with previous literature, participants in this study described the impact of body image post stoma surgery on sexuality and intimacy (Kelly, 1992; Manderson, 2005). Participants highlighted that they feel less sexually attractive and more self-conscious of their body naked post-surgery. These findings are in line with those of Salter (1992). Stigma and silence was an important sub-theme derived from the analysis, representing the isolation felt by women due to the lack of conversation surrounding not only sexuality, but stomas in general. As noted above, concealment was a strategy mentioned by most of the participants to minimise the stomas visibility. However, the challenge of concealment extends into intimacy and sexuality, where the stoma cannot be hidden. Similar to the responses in this study, Paszyńska et al. (2023) found that body image disturbances were a key element disrupting intimate relationships. In addition, some researchers have observed a loss of body-confidence among women in relationships, who may try to hide their bodies from their partners (Thorpe and McArthur, 2017).
The final theme of ‘moving forward’ incorporated acceptance as reflected in the responses provided by the participants. Participants in this study highlighted a range of emotions reflecting the contradictory nature of living with a stoma. The intense gratitude for having survived extreme illnesses such as cancer or years of pain due to IBD contrasts profoundly with the negative emotions associated with stoma, particularly surrounding body image. However, it was evident from the interviews that each participant continuously tries to remain positive and optimistic despite huge challenges and changes brought about by the stoma.
Acceptance of the stoma appears to be central to the process of moving forward and adjusting to alterations in body image. For many participants, particularly those who previously had a diagnosis of colorectal cancer, accepting the stoma as a permanent part of the body is an on-going and complex process. Acceptance was associated with better quality of life among Crohn’s patients and lower reports of body image disturbances. This finding is in accordance with recent results outlined by Szpilewska et al. (2018). Thorpe and McArthur (2017) further explored the contrasts in acceptance between those with colorectal cancer and individuals with IBD, highlighting that colorectal cancer patients are more likely to undergo surgery very quickly after their diagnosis due to the life-threatening nature of the condition. This quick turnaround can leave these individuals less time to accept what has happened. Whereas for most individuals with IBD, they have spent years living with a debilitating condition before stoma surgery which may allow for quicker acceptance given the positive changes it has provided them.
Strengths and limitations
The qualitative nature of the findings from this study adds new knowledge to the body image and stoma literature. This study identifies the factors that contribute to body image alterations in women post stoma surgery, providing an insight into how these women perceive their bodies and providing a possible explanation for some of the poor psychological outcomes following this intervention. This study also offers a strong basis of information onto which a more efficient psychological support system for ostomates in Ireland can be built.
Some limitations are also present in this research study. The first limitation pertains to the homogenous sample whereby all participants were female. While a female-only sample size provided rich insights, it made it impossible to note any gender differences with regards to how individuals perceive body image post stoma surgery. Cultural context is important for examining the varied impacts of living with a stoma. As the participants in this study were not from culturally diverse backgrounds, future research may analyse how cultural factors can influence body image. Secondly, as some of the participants in this study had only been living with a stoma for a very short period, a longer timeframe for data collection may have allowed for a deeper exploration of both adaptations to changes in body image and overall acceptance. A further limitation of this study relates to the relatively smaller sample size. Future research with larger samples may further contribute to the knowledge in this field. Finally, as the data was derived from self-reported accounts, the findings may be subject to response biases, such as social reliability bias.
Conclusions and implications
Disturbances in body image are highly prevalent following stoma surgery regardless of the condition that necessitated the surgery and can affect various domains of life. Those who received a stoma as a result of colorectal cancer expressed more profound concerns relating to alterations in their body image. The psychological impact of living with a stoma was highlighted, with participants emphasising the urgent need for a more integrated psychological approach for assessing and supporting those with stomas. Moreover, body image disturbances require greater attention and understanding among healthcare professionals in Ireland. In light of these findings, Irish healthcare systems should consider integrating psychological support as a core component of the stoma care pathway. This may include the provision of psychoeducation to increase awareness of possible psychological difficulties which may arise following stoma surgery. The development of integrating multidisciplinary care that incorporates psychological support alongside surgical and nursing care would further support adjustment. These findings support a shift towards a more patient-centred model of care and the development of evidence-based interventions aimed at improving access to psychological support for those living with a stoma. Dedicated access to professional psychologists should be included in routine care. Future research examining the differences in the psychological impact of stomas because of either cancer or IBD could support establishing more effective pre- and post-operative care which may further enhance psychological outcomes for ostomates.
Footnotes
Ethical considerations
The School of Psychology Ethics Review Committee at Trinity College Dublin approved our interviews (approval: SPREC032024-08) on 28th March, 2024.
Consent to participate
Respondents provided written consent for participation.
Consent for publication
Respondents gave written consent for publication.
Author contributions
Roisin Duffy contributed to the conceptualisation of the study, implemented the study, interviewed participants, conducted analyses and led the writing of the paper. David Hevey contributed to the conceptualisation of the study, the method, analyses, interpretation and writing of the paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability Statement
Data will be shared with researchers upon request.*