
Abstract
This systematic review synthesizes evidence on the prevalence of experienced and internalized weight stigma in general adult populations. A systematic search of PubMed, Scopus, ScienceDirect, and PsycINFO was conducted from inception to October 2025, following the PRISMA 2020 guidelines. Eligible studies included community-based, non-clinical adult samples (⩾18 years) reporting weight stigma using validated instruments. Eight cross-sectional studies (n = 18,335) from six countries met inclusion criteria. Both experienced and internalized weight stigma were consistently observed across populations, with generally higher levels reported among women. Estimates varied across cultural contexts and were influenced by differences in measurement tools, scoring approaches, and sample characteristics. Overall, findings suggest that weight stigma is a prevalent and measurable phenomenon in the general adult population. The development of standardized, culturally validated instruments is needed to improve global surveillance and enable robust cross-country comparisons.
Keywords
Introduction
Weight stigma is increasingly recognized as a significant public health and social concern, affecting individuals across diverse cultural, socioeconomic, and geographic contexts. It is characterized by negative stereotypes, social devaluation, and discriminatory practices directed toward individuals based on their body weight, and has been widely documented both in high-BMI groups and in the broader community (Emmer et al., 2020; Pearl and Puhl, 2018; World Health Organization, Regional Office for Europe, 2017), although BMI should be interpreted with caution as a simplified indicator of health. The World Health Organization (WHO) has identified weight stigma as a pervasive global phenomenon and a violation of human rights, underscoring its relevance beyond individual health outcomes to broader issues of social justice and health equity (World Health Organization, Regional Office for Europe, 2017). This global recognition highlights the importance of quantifying its prevalence at the population level.
According to the WHO, “weight bias” refers to negative attitudes and beliefs directed at individuals based on their body weight. Weight bias can lead to “weight stigma,” defined as the social devaluation of individuals because of their body weight, expressed through negative stereotypes, prejudicial attitudes, and discriminatory practices. Three primary forms are commonly examined: experienced (or enacted) stigma, referring to direct or perceived encounters with teasing, unfair treatment, or discrimination; internalized weight stigma, whereby individuals adopt and apply societal weight-based stereotypes to themselves; and anticipated stigma, which refers to the expectation of being treated unfairly because of one’s body weight (Hunger and Major, 2015; Papadopoulos and Brennan, 2015; Puhl and Heuer, 2009; World Health Organization, Regional Office for Europe, 2017).
The language used to describe body weight plays an important role in shaping how stigma is understood and experienced. Terms such as “overweight” and “obesity,” although widely used in public health and research contexts, are not neutral but reflect socially and culturally constructed values. These terms have been critiqued for their potential to reinforce stigma and the pathologization of higher body weight. Increasingly, researchers have highlighted the importance of using more neutral and respectful language when possible. However, such terminology is retained to remain consistent with existing measurement tools and the broader literature, while acknowledging its limitations (Meadows and Daníelsdóttir, 2016; Robbins et al., 2025).
In addition, body mass index (BMI) is widely used in public health research as a simple indicator of weight status. However, its suitability as a measure of individual health remains debated. Its application within weight-based classification systems may also shape how body weight is perceived and socially evaluated, with implications for the development and perpetuation of weight stigma. BMI is derived from a ratio of height and weight and does not directly account for body composition or fat distribution. Moreover, its relationship with adiposity varies across factors such as sex, age, and ethnicity. As a result, BMI provides only a partial representation of health and should be interpreted with caution, particularly when examining complex and socially embedded phenomena such as weight stigma (Byker Shanks et al., 2025).
Weight stigma has been consistently associated with adverse psychological and behavioral outcomes, including depression, anxiety, low self-esteem, elevated stress, disordered eating behaviors, overeating, and avoidance of physical activity (Emmer et al., 2020; Levinson et al., 2024; Papadopoulos and Brennan, 2015; Thedinga et al., 2021). It also undermines quality of life by mediating the relationship between excess weight and its negative physical, mental, and social consequences, due to reduced engagement in health-promoting behaviors (Kahan and Puhl, 2017; Papadopoulos and Brennan, 2015). Importantly, these harms occur across the weight spectrum, highlighting a need to understand the true population burden of stigma.
These outcomes are not uniform across all forms of weight stigma, as different dimensions of stigma may operate through distinct mechanisms. Notably, internalized and anticipated forms of weight stigma are thought to arise, at least in part, from prior experiences of weight-based discrimination (Hunger and Major, 2015; O’Brien et al., 2016), with evidence suggesting that internalized stigma may be more strongly associated with adverse health and well-being outcomes than experienced stigma (Pearl and Puhl, 2016). Studies have shown that both experienced and internalized weight stigma are significantly associated with a range of mental health outcomes, including higher levels of depression, anxiety, psychological distress, and disordered eating, as well as lower levels of self-esteem, well-being, quality of life, and life satisfaction (Emmer et al., 2020; Wu and Berry, 2018). In addition, anticipated weight stigma has been associated with disordered eating behaviors, including dietary restraint, eating concerns, body shape and weight concerns, binge eating, and unhealthy weight control practices (Hunger et al., 2020; Wetzel and Himmelstein, 2023).
Despite growing international research interest, existing evidence remains fragmented and often limited to specific populations such as students, patients, or healthcare professionals (Kapera et al., 2024; Panza et al., 2018; Sohier et al., 2025; Sonneville et al., 2024). As a result, the prevalence of both experienced and internalized weight stigma in community-based adult populations remains insufficiently quantified at a global level. A previous systematic review conducted by Spahlholz et al. (2016) examined weight discrimination exclusively among individuals with obesity, thereby limiting generalizability to the broader population. Consequently, the prevalence of both experienced and internalized weight stigma in community-based adult samples remains poorly quantified.
To address this gap, the present review synthesizes international evidence on the prevalence of weight stigma in the general adult population, across the full BMI range, and includes both experienced and internalized stigma. The aim of this systematic review is to synthesize and critically evaluate international evidence on the prevalence of experienced and internalized weight stigma among general adult populations, and to examine how estimates vary across cultural contexts, measurement approaches, and study characteristics.
Methods
The review process, including study selection, data extraction, and synthesis, adhered to the methodological standards outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines (Page et al., 2021). The protocol was registered in PROSPERO (CRD420251090726).
Search strategy
Two researchers (IS and KG) independently carried out a systematic search across four electronic databases, PubMed, Scopus, ScienceDirect, and PsycINFO, from inception to October 15, 2025. The search combined controlled vocabulary (e.g. MeSH terms) and free-text keywords related to weight stigma, internalized stigma, discrimination, and adult populations. The search strategy was applied to titles and abstracts only, in accordance with database search functionalities. Disagreements between reviewers were resolved through discussion until consensus was reached. The full search strategy for each database is provided in Appendix 1. No language or publication-status restrictions were applied. Gray literature, dissertations, and conference abstracts were not searched, which is acknowledged as a limitation.
Eligibility criteria
The selection of eligible studies was guided by the PECOS framework, which defined the characteristics of participants, exposure, comparison, outcomes, and study design. Participants were required to be adults aged 18 years or older recruited from community-based, non-clinical settings. Studies were required to include individuals across the full BMI spectrum rather than exclusively overweight or obese groups. The exposure of interest was weight stigma (experienced/enacted or internalized), assessed using validated psychometric instruments. In prevalence-based designs, the comparison group consisted of individuals within the same sample who did not report experienced or internalized weight stigma. The primary outcome was the assessment of weight stigma, reported either as prevalence estimates (proportions) or as severity indicators derived from validated scales (e.g. mean scores). Eligible study designs included quantitative observational studies, such as cross-sectional population-based surveys, nationally or regionally representative surveys, and community-based cohort studies.
Studies were excluded if they employed qualitative methodologies, intervention designs, case reports, opinion articles, or conceptual papers. Studies were also excluded if they did not provide a clear or valid measure of weight stigma prevalence, including those lacking adequate descriptions of assessment tools or procedures. Predictor-only studies were included only when relevant prevalence data could still be extracted. Additional exclusions applied to studies focusing on specific subpopulations (e.g. pregnant women, university students, or clinical populations), studies recruiting participants based solely on BMI (e.g. overweight or obese samples), studies conducted exclusively in clinical or healthcare settings, and studies involving individuals undergoing weight-loss treatment or bariatric procedures. Finally, studies using non-validated or inadequately described stigma measurement tools were excluded.
Study selection
All records identified through database searches were exported to Zotero (version 7.0.19). Duplicates were removed using automated detection with subsequent manual verification. After the removal of duplicates, titles and abstracts were screened for relevance by two independent researchers (IS and KG). Full-text articles were then assessed for eligibility by the same reviewers. Disagreements at any stage were resolved through consensus. The study selection process is summarized in a PRISMA 2020 flow diagram (Figure 1).
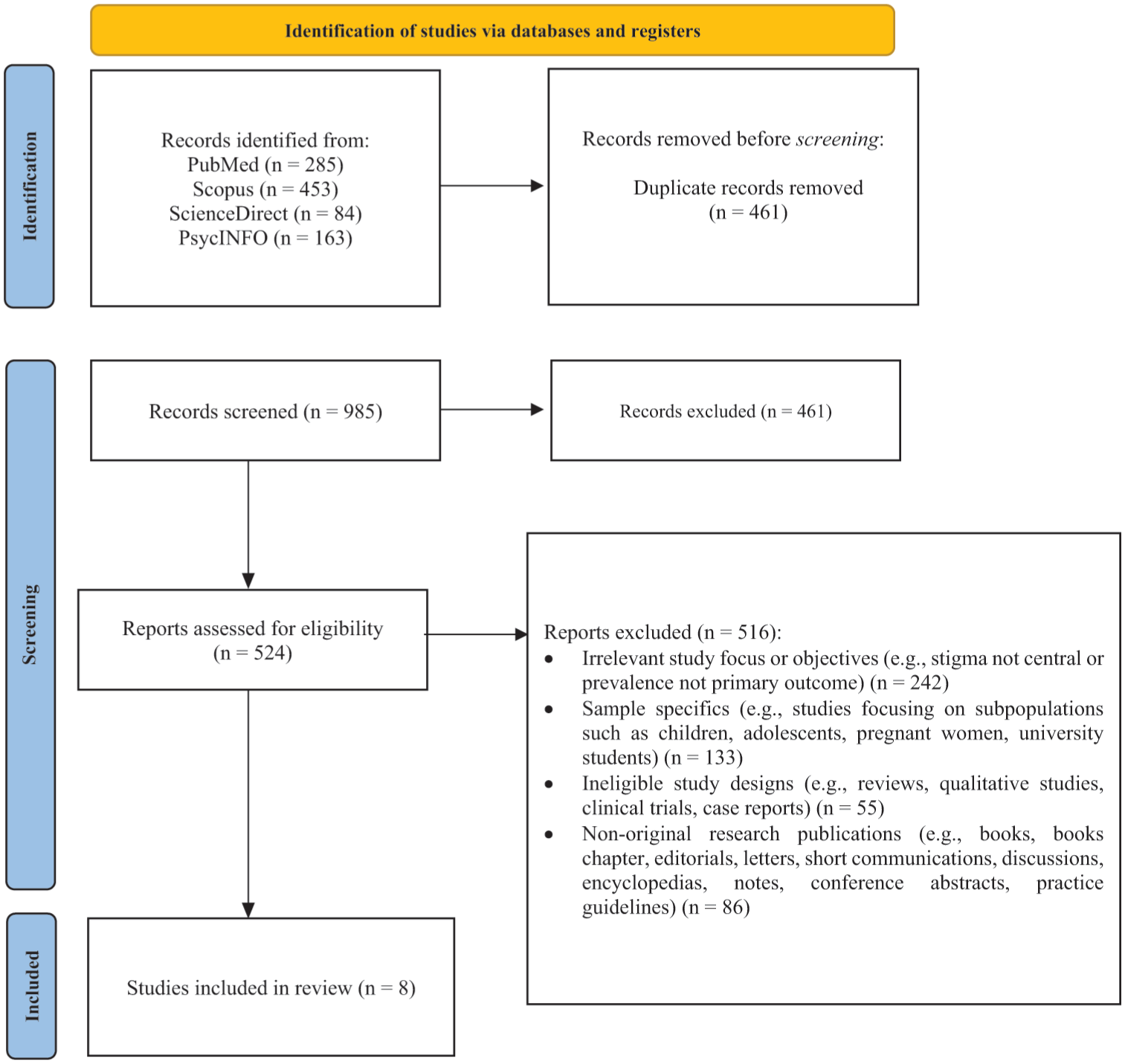
Flow diagram of the article selection process.
Data extraction
Data extraction was performed independently and systematically by two authors (IS and KG) using a standardized, pre-piloted extraction form. The following data were extracted: study details (first author, year, country, design), population characteristics (sampling method, sample size, age, gender distribution, BMI), type of weight stigma assessed (experienced/enacted vs internalized), measurement instrument used (WBIS, WBIS-M, WBIS-2F, SSI-B, WSSQ), prevalence metrics (percentages, mean scores, standard deviations, cut-off criteria where applicable). Any discrepancies in extracted data were resolved through discussion until consensus was reached.
Quality assessment
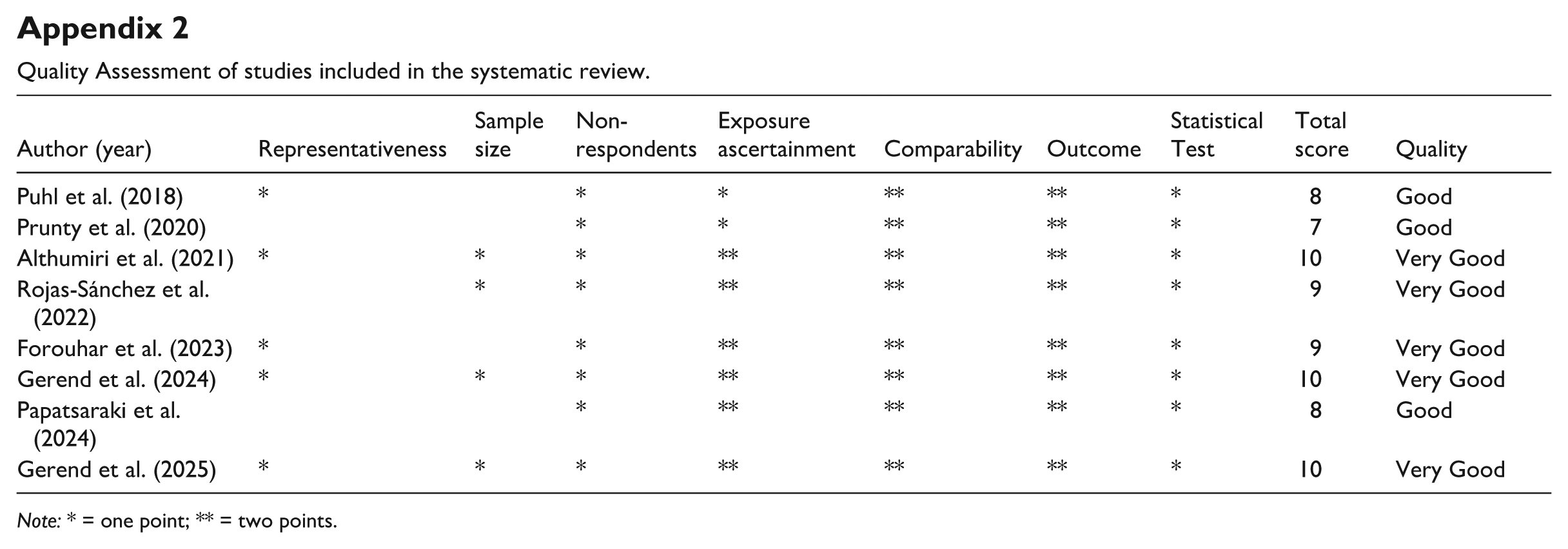
The methodological quality of the included studies was evaluated using the Newcastle–Ottawa Scale (NOS), adapted for cross-sectional studies (Herzog et al., 2013). Τhe NOS was selected due to its widespread use in assessing non-randomized studies and its suitability for observational designs commonly included in systematic reviews, providing a practical framework for evaluating methodological quality (Stang, 2010). The NOS assessed three domains: selection of study participants, comparability of study groups, and outcome assessment. These domains cover aspects such as sample representativeness, sample size, response rate, ascertainment of exposure, control of confounding factors, and the validity of outcome measurement and statistical analyses. Scores ranged from 0 to 10, and studies were classified as very good (9–10 points), good (7–8), satisfactory (5–6), or unsatisfactory (0–4). Two reviewers (IS and KG) independently performed quality assessments, and discrepancies were resolved through consensus.
Data synthesis
Due to substantial heterogeneity across studies, particularly in terms of study characteristics, measurement tools, scoring systems, and definitions of weight stigma, a formal meta-analysis was not conducted. Instead, a narrative synthesis was performed in accordance with PRISMA guidelines, summarizing findings by type of stigma and measurement instrument. To enhance comparability, studies were further grouped by geographic region to allow cross-cultural comparison. No statistical transformations or standardization of effect sizes were undertaken due to incompatible measurement scales.
Ethical approval
This review does not involve human participants or primary data collection; ethical approval was not required.
Results
Study selection
The initial search identified 985 articles. After removing duplicates, 461 articles remained for screening. During title and abstract screening, 225 studies were excluded, and a further 236 studies were excluded following full-text assessment. Eight studies met the eligibility criteria and were included, comprising a total of nine independent samples, as one study (Rojas-Sánchez et al., 2022) contributed data from two distinct populations (France and Mexico). The selection process is summarized in the PRISMA flow diagram (Figure 1).
Study characteristics
The eight included studies, published between 2018 and 2025, were conducted across six countries: the United States, Saudi Arabia, France, Mexico, Canada, and Greece. Across studies, samples included adults from the general population, with age ranges typically spanning young to middle adulthood. Gender distribution was relatively balanced in most studies, although some samples were predominantly female. BMI distributions varied across samples but generally reflected a mix of normal weight, overweight, and obesity categories. All studies employed a cross-sectional design and sampled adults from community-based, non-clinical settings. Most studies relied on non-probability sampling approaches, including convenience, quota, and snowball sampling. Only the study of Forouhar et al. (2023) used a probability-based panel, although participant selection within the panel was based on quota sampling. Sample sizes ranged from 153 to 4709. All studies reported gender distribution and used self-reported anthropometric data to calculate BMI. All studies used validated questionnaires to assess weight stigma, including the Weight Bias Internalization Scale (WBIS), the Modified Weight Bias Internalization Scale (WBIS-M), the Two-Factor Weight Bias Internalization Scale (WBIS-2F), the Stigmatizing Situations Inventory-Brief (SSI-B), and the Weight Self-Stigma Questionnaire (WSSQ). The WBIS and its modified versions (WBIS-M, WBIS-2F) assess internalized weight stigma and have shown acceptable to strong reliability and construct validity in prior research (Durso and Latner, 2008; Jenkins and Baysen, 2025; Meadows and Higgs, 2019). The SSI-B assesses experienced/enacted weight stigma and has demonstrated good reliability and convergent validity as a brief measure of stigmatizing experiences (Vartanian, 2015). The WSSQ assesses weight self-stigma, including self-devaluation and fear of enacted stigma, and has also shown satisfactory psychometric performance in validation studies (Lillis et al., 2010). These instruments typically use Likert-type response formats, with higher scores indicating greater stigma. Prunty et al. (2020), additionally used custom-designed items to assess enacted stigma. A detailed summary of study characteristics is provided in Tables 1 and 2.
Weight stigma measures and prevalence outcomes across included studies.
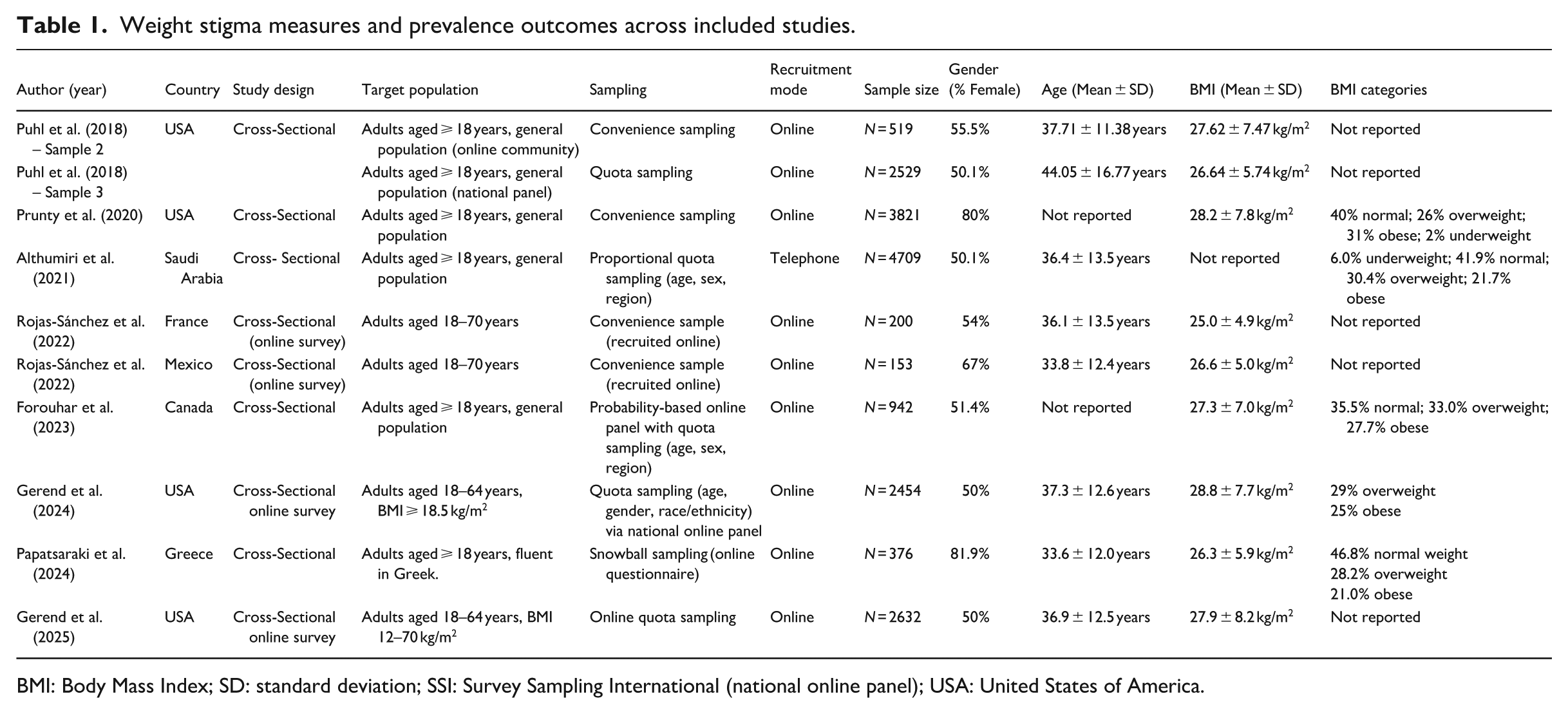
BMI: Body Mass Index; SD: standard deviation; SSI: Survey Sampling International (national online panel); USA: United States of America.
Assessment instruments and prevalence and severity estimates of weight stigma.
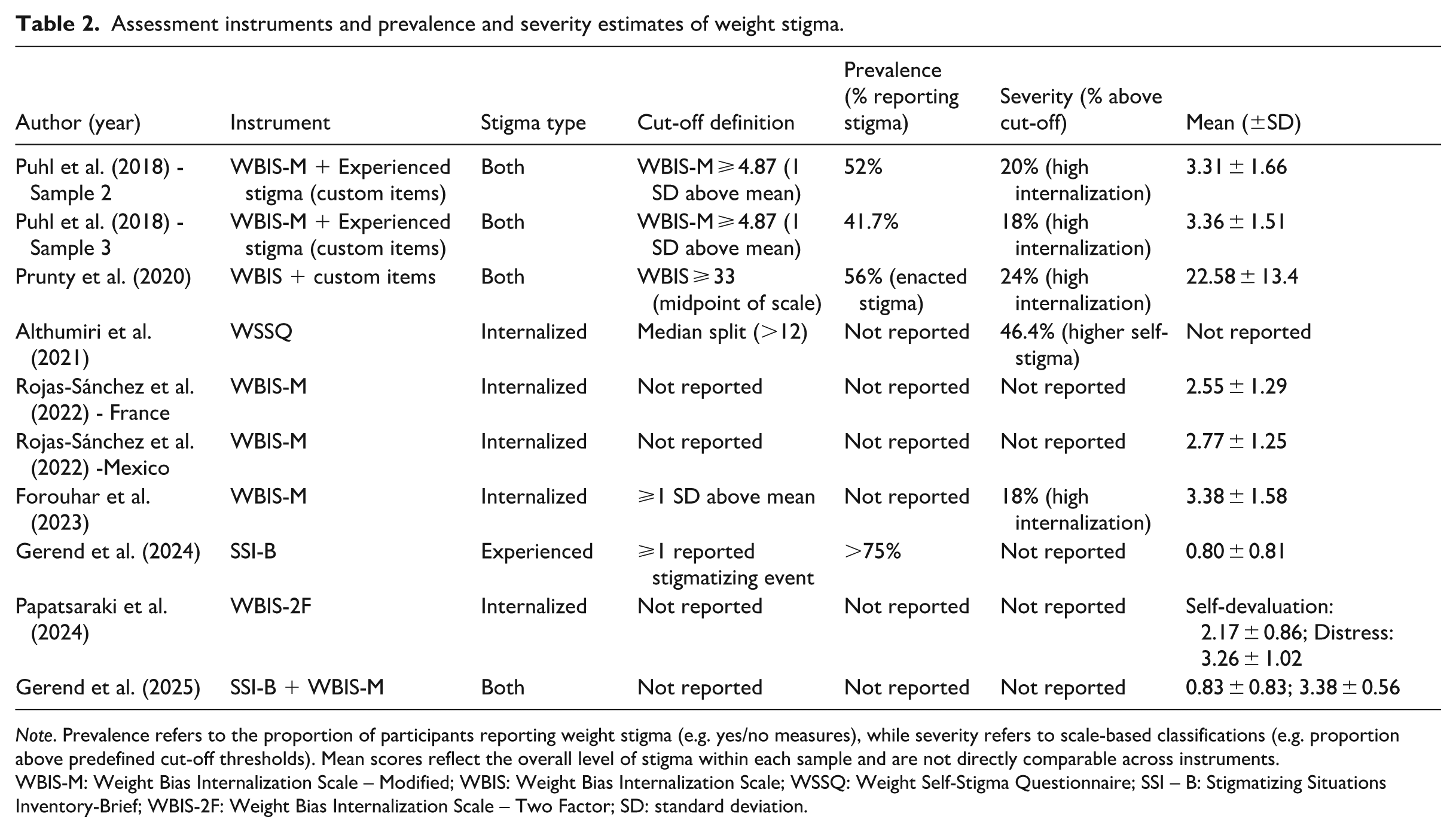
Note. Prevalence refers to the proportion of participants reporting weight stigma (e.g. yes/no measures), while severity refers to scale-based classifications (e.g. proportion above predefined cut-off thresholds). Mean scores reflect the overall level of stigma within each sample and are not directly comparable across instruments.
WBIS-M: Weight Bias Internalization Scale – Modified; WBIS: Weight Bias Internalization Scale; WSSQ: Weight Self-Stigma Questionnaire; SSI – B: Stigmatizing Situations Inventory-Brief; WBIS-2F: Weight Bias Internalization Scale – Two Factor; SD: standard deviation.
Prevalence and severity estimates
Studies reported weight stigma using both prevalence-based (proportion of participants reporting stigma) and severity-based (scale-derived scores or cut-off classifications) measures.
North America
Across studies conducted in North America, both experienced and internalized forms of weight stigma were commonly reported. In the United States, Puhl et al. (2018) assessed the internalized weight bias using the WBIS-M in two samples. The first sample reported in the original study was not included, as it comprised individuals with obesity at elevated risk for weight stigma and did not meet the inclusion criteria of the present review. Sample 2 was recruited from an online community platform (MTurk), whereas Sample 3 was derived from a large national panel designed to approximate general population characteristics. Experienced weight stigma was reported by 52% (Sample 2) and 41.7% (Sample 3) of participants. Mean WBIS-M scores were similar across samples (3.31 ± 1.66 and 3.36 ± 1.51), indicating comparable levels of internalized stigma, with approximately 60% of participants reporting moderate levels and 18%–20% reporting high levels of internalization. Consistent patterns were observed in other U.S. studies. Prunty et al. (2020) reported that 56% of participants experienced at least one instance of enacted weight stigma, while 24% met criteria for high internalized stigma (WBIS ⩾ 33). The mean WBIS score was 22.58 ± 13.4, reflecting the overall level (severity) of internalized stigma within the sample. Similarly, Gerend et al. (2024) found that over 75% of participants reported at least one stigmatizing experience, with mean SSI-B scores (0.80 ± 0.81) reflecting the severity of perceived discrimination. Gerend et al. (2025) also reported moderate levels of both experienced and internalized stigma, with mean WBIS-M and SSI-B scores of 3.38 ± 0.56 and 0.83 ± 0.83, respectively.
Comparable findings were reported in Canada, where Forouhar et al. (2023) observed a mean WBIS-M score of 3.38 ± 1.58, indicating moderate internalization, with 18% of participants classified as having high internalization. In Mexico, Rojas-Sánchez et al. (2022) reported mean scores of 2.35 ± 1.64 for weight stigma concerns and 2.77 ± 1.25 for WBIS-M, also indicating moderate levels of stigma severity.
Europe
Findings from European samples indicated moderate levels of internalized weight stigma across populations. The French subsample of Rojas-Sánchez et al. (2022) showed mean scores of 2.00 ± 1.40 for weight stigma concerns and 2.55 ± 1.29 on the WBIS-M. Similarly, in Greece, Papatsaraki et al. (2024) reported mean scores of 2.17 ± 0.86 for the self-devaluation and 3.26 ± 1.02 for the weight-related distress using the WBIS-2F, reflecting comparable levels of internalized stigma across European contexts.
Middle East
In Saudi Arabia, Althumiri et al. (2021) applied the WSSQ in a nationally representative sample (N = 4709). Using both a median-split classification and a cut-off score (>12), 46.4% of participants were classified as having higher levels of weight self-stigma, indicating a substantial proportion of the population experiencing elevated internalized stigma.
Gender differences
Across the included studies, gender differences were examined where data were available. Papatsaraki et al. (2024) reported no significant associations between gender and internalized stigma (p > 0.05), and Gerend et al. (2025) did not perform gender-stratified analyses. However, the majority of studies reported higher levels of weight stigma among women. For example, Puhl et al. (2018) found that women comprised 72.1% of individuals in the highest WBIS-M category. Prunty et al. (2020) reported higher prevalence of high internalized stigma among women (26%) compared to men (15%). Forouhar et al. (2023) also found significantly higher mean internalization scores among women (3.58 ± 1.65) compared to men (3.16 ± 1.48, p < 0.001). Similarly, Gerend et al. (2024) and Rojas-Sánchez et al. (2022) reported higher stigma scores among women, and Althumiri et al. (2021), in Saudi Arabia, reported higher prevalence of elevated weight self-stigma among women than men (50.2% vs 42.5%, p < 0.001). Overall, these findings indicate a general pattern of higher reported stigma among women across diverse settings.
Measurement tool differences
Across studies, differences in reported estimates were closely related to the measurement tools used and the type of stigma assessed. Studies using binary yes/no items generally reported substantial proportions of participants experiencing weight stigma, with estimates ranging from approximately 41.7% to 56% (Prunty et al., 2020; Puhl et al., 2018). Similarly, instruments such as the SSI-B, which assess the frequency of stigmatizing experiences, indicated high levels of experienced stigma, with over 75% of participants reporting at least one such experience (Gerend et al., 2024).
In contrast, studies using WBIS-based instruments (WBIS, WBIS-M, WBIS-2F) assessed internalized stigma using mean scores and scale-based classifications, which generally reflected moderate levels of internalization (e.g. mean scores ranging from 2.55 to 3.38). When cut-off thresholds were applied (e.g. ⩾1 SD above the mean or WBIS ⩾ 33), the resulting proportions (e.g. 18%–24%) reflected higher levels of internalization. Similarly, the WSSQ, which uses a median-split classification, identified 46.4% of participants as having higher weight self-stigma (Althumiri et al., 2021).
Stigma type differences
Across studies, both experienced and internalized forms of weight stigma were assessed. Measures of experienced stigma consistently indicated that a substantial proportion of participants reported at least one stigmatizing experience, often exceeding 40%. In contrast, internalized stigma, primarily assessed using WBIS-based instruments, was reflected in mean scores indicating moderate levels of internalization across samples (2.55–3.38). The WSSQ similarly identified a substantial proportion of participants as having elevated internalized stigma based on a scale-derived classification. Overall, these findings suggest that while exposure to weight-related stigma is widespread, the degree to which such experiences are internalized varies across populations and measurement approaches.
Methodological quality appraisal
All eight studies were evaluated using the NOS adapted for cross-sectional studies. Overall scores ranged from 7 to 10, indicating good to very good methodological quality. Most studies used validated psychometric instruments and applied appropriate statistical analyses. Common limitations included reliance on convenience sampling, limited reporting of sample size calculations, and the use of self-reported anthropometric data. No studies were classified as unsatisfactory. A detailed breakdown of NOS assessments is provided in Appendix 2.
Discussion
This systematic review provides evidence that weight stigma is present across general adult populations in multiple geographic regions. Overall, the findings suggest that both experienced and internalized forms of weight stigma are common, with moderate levels reported across diverse settings. Although estimates varied depending on the measurement instrument used, patterns were broadly consistent across studies. Given the substantial heterogeneity in measurement scales and scoring systems, direct numerical comparison should be interpreted with caution. Nevertheless, the consistent observation of moderate levels of stigma highlights the public health relevance of the phenomenon.
Across studies, women generally reported higher levels of stigma than men, and higher BMI groups showed greater internalization, consistent with prior research. These findings can be understood within the context of gendered sociocultural pressures surrounding body weight and appearance. In many social contexts, women’s bodies are subject to ongoing social evaluation, surveillance, and moral judgment, with thinness often framed as a marker of self-discipline, control, and social value. As a result, women may experience greater exposure to weight-related scrutiny and stronger pressures to conform to narrow body ideals (Cui et al., 2026; Selensky and Carels, 2021). These influences, reinforced through family, peer, and media environments, may contribute to increased vulnerability to both experienced and internalized weight stigma.
Regional differences were observed, with relatively lower stigma scores in European samples and higher levels in the Middle Eastern sample. However, these findings should be interpreted cautiously due to methodological heterogeneity and the limited number of studies per region. Cultural norms, social expectations, and the broader societal changes may partially contribute to these patterns, although the included studies did not directly assess these mechanisms (Galindo et al., 2026; Gerend et al., 2024). For example, rapid shifts toward Westernized beauty ideals in some regions may increase susceptibility to stigma, whereas settings with stronger body diversity acceptance may show lower internalization (Cui et al., 2026). However, these interpretations should remain tentative, as included studies did not directly measure cultural mechanisms. A key methodological observation is that differences in measurement instruments contributed substantially to variability across studies. WBIS-based tools consistently indicated moderate internalization, whereas SSI-B measures tended to capture high prevalence of experienced stigma. This variation underscores the need for standardized, cross-culturally validated instruments.
The findings of this review are broadly consistent with previous literature while extending existing knowledge by focusing on general population samples across multiple regions. For example, the review by Spahlholz et al. (2016), which focused on individuals with obesity, reported lower prevalence estimates, likely reflecting differences in study populations. Evidence from clinical and weight-loss settings has consistently shown higher internalized stigma, supporting the notion that stigma exists across the weight spectrum but may be more pronounced in clinical populations. Overall, the findings of this review are broadly consistent with prior literature, while extending existing knowledge by focusing on general population samples across multiple regions. No major contradictions were identified, however variability across studies highlights the influence of methodological differences.
Taken together, these findings indicate that weight stigma is a widespread phenomenon with important implications for public health. Educational interventions targeting healthcare professionals, including empathy-based and weight-neutral communication training, have demonstrated effectiveness in reducing implicit bias and improving care quality (Alberga et al., 2016; Paulus and Meinken, 2022). Similarly, school-based and university-level interventions have shown promise in reducing stigma (Levine, 2023; Ruck et al., 2025). Broader approaches, such as framing health beyond BMI, promoting media literacy, and supporting body-inclusive public health messaging, may further contribute to reducing stigma and its associated harms (Clark et al., 2021; Tylka et al., 2014). At a policy level, legal protections against weight-based discrimination may also play a critical role in promoting equity in healthcare, employment, and education.
This review has several strengths. It is among the first to synthesize prevalence estimates of experienced and internalized weight stigma in general adult populations across multiple regions. It also incorporates the use of validated measurement tools and follows established systematic review methodology. However, several limitations should be acknowledged. The small number of included studies limits the strength of conclusions. Substantial heterogeneity in study designs, measurement instruments, and reporting approaches precluded meta-analysis and limited comparability across findings. Most studies relied on non-probability sampling and self-reported anthropometric data, which may affect representativeness and introduce measurement error. Additionally, the cross-sectional nature of the included studies prevents causal inference. The search strategy was limited to titles and abstracts, which may have resulted in the omission of relevant studies. No attempts were made to contact study authors for missing or unclear data, which may have affected data completeness. Finally, variability in how weight stigma was operationalized (e.g. prevalence-based vs severity-based measures) further limits direct comparison across studies.
Future research should aim to strengthen the evidence base in this field. In particular, the development of standardized, cross-culturally validated instruments is essential to improve comparability across studies. Longitudinal research is needed to better understand the temporal relationships between weight stigma and health outcomes. Greater representation of underrepresented regions, including Asia, Africa, and South America, is also needed to enhance global generalizability. In addition, improved reporting of sampling strategies, psychometric properties, and the establishment of consistent cut-off thresholds would facilitate more robust synthesis and future meta-analytic work.
Conclusion
This systematic review indicates that weight stigma is present in the general adult population across multiple countries. Despite methodological heterogeneity, both experienced and internalized forms of stigma were consistently observed, highlighting its global relevance. Continued efforts to develop standardized measurement tools and expand research across diverse populations are essential for improving surveillance and informing effective interventions. Addressing weight stigma should be considered a key public health priority to promote population well-being and reduce health inequities.
Footnotes
Appendix 1. Search strategies for each database used in this systematic review
Appendix 2
Quality Assessment of studies included in the systematic review.
| Author (year) | Representativeness | Sample size | Non-respondents | Exposure ascertainment | Comparability | Outcome | Statistical Test | Total score | Quality |
|---|---|---|---|---|---|---|---|---|---|
| Puhl et al. (2018) | * | * | * | ** | ** | * | 8 | Good | |
| Prunty et al. (2020) | * | * | ** | ** | * | 7 | Good | ||
| Althumiri et al. (2021) | * | * | * | ** | ** | ** | * | 10 | Very Good |
| Rojas-Sánchez et al. (2022) | * | * | ** | ** | ** | * | 9 | Very Good | |
| Forouhar et al. (2023) | * | * | ** | ** | ** | * | 9 | Very Good | |
| Gerend et al. (2024) | * | * | * | ** | ** | ** | * | 10 | Very Good |
| Papatsaraki et al. (2024) | * | ** | ** | ** | * | 8 | Good | ||
| Gerend et al. (2025) | * | * | * | ** | ** | ** | * | 10 | Very Good |
Note: * = one point; ** = two points.
Ethical considerations
Ethics approval was not required for this review article as no data were collected from participants.
Consent to participate
Consent to participate is not applicable to this review article as no data were collected from participants.
Consent for publication
Consent for publication is not applicable to this review article as no identifiable participant data are included.
Author contributions
IS contributed to the conceptualization of the review, development of the search strategy, database searches, screening of titles and abstracts, data extraction, statistical analysis, data visualization, and drafting of the original manuscript. EH and IT contributed to methodological guidance, and writing – review and editing. KG contributed to the conceptualization, full-text screening, data extraction, risk of bias assessment, validation of analyses, methodological oversight, project administration, supervision, and drafting of the original manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data included in this review are derived from previously published studies and are available within the article.