
Abstract
Given the high co-occurrence of tobacco, marijuana use, and mental health disorders, we explored behavioral health providers’ perceptions of patient mental health and substance use during the COVID-19 pandemic. We conducted semi-structured interviews with 21 Ohio providers randomly sampled from state licensure records, analyzing data using constructivist grounded theory. Providers perceived broad increases in substance use and mental health symptoms, attributing these to isolation, reduced support access, and pandemic-related stress. Providers consciously de-prioritized tobacco and marijuana to focus on “more acute” concerns. Substance use providers emphasized “riskier” substances while mental health providers prioritized severe psychiatric symptoms. Tobacco was often excluded from abstinence frameworks due to its normalization in recovery settings. These findings highlight the need for targeted provider training, organizational policy reform, and educational interventions to address the systematic deprioritization of tobacco and marijuana in behavioral health settings, with implications extending beyond the COVID-19 pandemic to future public health crises.
Introduction
Tobacco use in the United States remains the leading cause of preventable deaths despite declines in cigarette smoking, with half a million deaths each year attributable to cigarette smoking (U.S. Department of Health and Human Services, 2020). Persons with mental illness and substance use disorders (SUD) bear a disproportionate burden of tobacco-related disease. The proportion of cigarette smoking among persons with any mental illness was 67% higher than those without and approximately 40% of all tobacco-related deaths occur among those with a mental health condition (Loretan et al., 2022; Prochaska et al., 2017). Though cigarette smoking has declined among those with SUD, the prevalence of smoking is notably higher (35.8%) compared to those without SUD (16.8%; Han et al., 2022). SUD treatment facilities often have high proportions of persons smoking tobacco products, estimates ranging from 63% to 93% (Guydish et al., 2011, 2019).
Despite the burden of disease, tobacco use is frequently undertreated in behavioral health settings; fewer than half of mental health and SUD treatment facilities offer evidence-based cessation (Marynak et al., 2018). The American Society of Addiction Medicine recommends integrated tobacco use disorder into SUD care, yet this guidance is often unimplemented (American Society of Addiction Medicine, 2022). Clinicians may perceive tobacco to be a lower priority than other concerns, harboring misconceptions that cessation may harm other treatment outcomes or that patients lack motivation to quit (Iyahen et al., 2023; White et al., 2023).
Marijuana use is more common among people who smoke cigarettes (Weinberger et al., 2016). Tobacco and marijuana are two of the most commonly used substances in the United States, and co-use of these substances is increasingly common, with 6.38% of U.S. adults reporting past-month co-use (Rubenstein et al., 2024). The use of multiple substances, referred to as polysubstance use, including alcohol, tobacco, and marijuana, is associated with worse mental health outcomes, including depression and anxiety (Khan et al., 2026). The policy context surrounding marijuana use has also shifted considerably in recent years; as of 2023, 24 states and Washington D.C. had legalized recreational marijuana, including Ohio, where recreational use was approved by voters in November 2023 (Bryan, 2024). These regulatory changes have implications for how providers perceive and prioritize marijuana use in clinical settings. Effective treatment of co-occurring substance use and mental health concerns can be challenging due to a historically fragmented system with separated mental health and substance use care (Knickman et al., 2016). Current treatment guidelines encourage the simultaneous treatment of both mental health and substance use disorders (Substance Abuse and Mental Health Services Administration, 2020). Despite this, only approximately 44% of adults with co-occurring disorders received any mental health care, while only 13% received substance use treatment, and only 9% received treatment for both disorders (Han et al., 2017); more recently, only 14.9% of adults with SUD received treatment in 2022 despite increasing prevalence (Liu et al., 2025).
While extensive research has examined healthcare providers’ adherence to treatment guidelines and perceptions of the harms of tobacco (Grech et al., 2020; Kilgore et al., 2021; Price et al., 2019), only limited research has explored healthcare providers’ perceptions of the harms of marijuana use. Within this small body of research, most has been conducted among oncology, obstetrics, and family medicine physicians (Braun et al., 2018; Holland et al., 2016; Kondrad and Reed, 2022). These studies have largely focused on whether providers consider marijuana harmful, rather than identifying specific aspects of those harms. Comparatively little research has explored how behavioral health providers, whose specialty encompasses both substance use and mental health treatment, prioritize addressing tobacco and marijuana use in substance use and mental health treatment settings. Understanding how these providers conceptualize treatment priorities is critical to designing further integrated care approaches for substance use and mental health concerns.
The COVID-19 pandemic affords a unique opportunity to explore how behavioral health providers address substance use and mental health concerns under conditions of widespread psychological distress. Nearly 41% of the U.S. population reported adverse mental health or behavioral health conditions during the pandemic (Czeisler et al., 2020), and even those without a psychiatric history experienced heightened levels of psychological distress (Holingue et al., 2020), resulting in unmet needs for psychiatric care (Coley and Baum, 2022). While COVID-19 was a singular event, the conditions it created, such as elevated stress, disrupted services, and sudden increases in patient need, are not unique to pandemics. Research has documented similar patterns of worsening mental health and substance use following other large-scale crises, including natural disasters, mass casualty events, and economic disruptions (Alexander and Ward, 2018; Substance Abuse and Mental Health Services Administration, 2024).
We draw on the self-medication hypothesis (Khantzian, 1997) as a sensitizing concept to orient our analysis, interpreting providers’ accounts through the lens of substance use as a response to psychological distress. The self-medication hypothesis is a widely applied framework for understanding the co-occurrence of mental health and substance use disorders (Turner et al., 2018). Treating the self-medication hypothesis as a broad sensitizing concept rather than a formal hypothesis to be tested is consistent with the inductive nature of constructivist grounded theory, allowing us to acknowledge the pre-existing nature of this theoretical idea while also utilizing our data to generate novel insight about the phenomena under study. An alternative explanation for co-occurring mental health and SUD is the common liability model, which proposes that overlapping genetic, environmental, and neurobiological factors can explain their co-occurrence (Vanyukov et al., 2012).
We employ a qualitative approach with inductive methods to address multiple gaps in the literature, examining how behavioral health providers perceive changes in mental health and substance use during a time of elevated psychological distress. Given the high prevalence of tobacco and marijuana use among this population, we also seek to understand how providers who specialize in treating mental health and substance use disorders perceive the importance of addressing these concerns. Findings from this study may inform how behavioral health systems anticipate and respond to future public health crises and other contexts of elevated psychological distress.
Methods
Design overview
Our research approach draws on constructivist grounded theory methodology (Charmaz, 2014, 2017). Constructivist grounded theory is an inductive approach rooted in the idea that reality is socially constructed, consistent with our view that providers interpret patient behaviors and make clinical decisions within the context of their individual and social experiences. This study is based on 21 original semi-structured interviews with licensed or certified community behavioral health providers within Ohio. The final sample size was determined by reaching theoretical saturation, which we assessed through the process of concurrent data collection and analysis consistent with constructivist grounded theory methodology. Recruitment continued until no substantively new dimensions of the core analytic categories were revealed through further interviews.
Study population and sampling
We recruited participants using a census of Ohio-based behavioral health providers from the Ohio Department of Mental Health and Addiction Services (OhioMHAS). Licensure information was stratified by type of license as defined by OhioMHAS: community behavioral health, opioid treatment programs, hospital-based, and three levels of residential facilities. Due to the small number of providers in the three classes of residential facilities, we combined these into one category.
Within each type of license, providers were randomly selected and contacted via phone and email. After three unsuccessful attempts, we attempted recruitment through front-desk associates, ceasing efforts after three additional attempts or direct refusal. A $50 gift card was provided as an incentive after interview completion. Demographic information for recruited participants is provided (Table 1). Our sampling strategy ensured that each licensed provider had an equal probability of being contacted; however, the final sample overrepresents community-based social workers relative to other provider types.
Descriptive characteristics of the study population (N = 21).
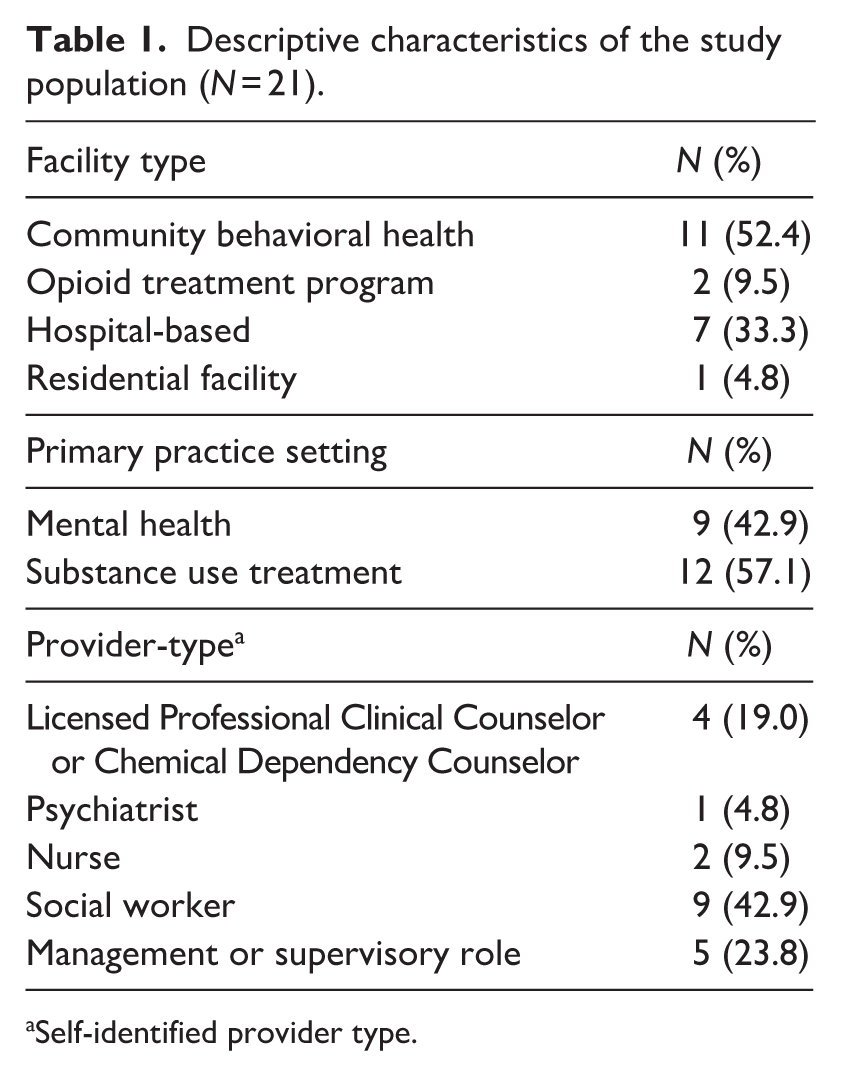
Self-identified provider type.
Data collection
We conducted semi-structured interviews to solicit providers’ experiences and perceptions in their own words. The semi-structured interview protocol (Supplemental Information) guided participants through discussions of perceived changes in their patients’ mental health, substance-related coping behaviors, and perceptions of the harms of both tobacco and marijuana. Probing questions were used throughout to elicit deeper discussion. All interviews were conducted by the first author using teleconferencing software (Zoom) and recorded. Interviews were conducted between August 2023 and January 2024. Participants were asked to reflect on their clinical experiences during the pandemic, with a primary focus on the period spanning from approximately 2020 to 2022.
Data analysis
We analyzed transcripts using a constructivist grounded theory approach (Charmaz, 2014, 2017) through an iterative coding process (Figure 1). We first generated line-by-line codes that closely captured the content of each interview segment, then we organized these into broader thematic categories. The formation of thematic categories represented the first major level of abstraction.

Model of the grounded theory analytic process.
From this process, we generated a list of focused codes (Supplementary Information). Focused codes represented ideas stemming from the thematic categories of line-by-line codes and were often more conceptual in nature. At this stage, we pared down groups of codes to focus on those that were conceptually more related to our research questions and appeared more frequently. Thematic categories containing line-by-line codes that were retained in the analysis comprised our focused codes
We re-analyzed all interviews using the focused codes, leading to further abstraction into analytic categories encompassing multiple concepts Patterns were explored using comparative tools and analytic memos. We employed constant comparative techniques, which involved generating concepts and theories through comparisons of increasing levels of abstractions (e.g. comparing data from one interview with data from another, and comparing content across analytic categories). We devoted specific attention to whether providers primarily engaged in mental health or substance use treatment in our comparisons.
We strengthened the analysis using abductive methods, developing hypotheses, rooted in the data and related to unexpected findings, and exploring these hypotheses through systematic analysis of variation across the interviews (Tavory and Timmermans, 2014; Timmermans and Tavory, 2022). An example of this would be seeking out “negative cases” or observations that challenged hypotheses developed at prior analytic stages.
The analysis process described above began while data were being collected. The simultaneous data collection and analysis allowed for a dynamic approach, through which we were able to probe novel findings. We used NVivo software (version 14) for qualitative research to organize data, maintain codes, and foster comparisons between data elements. Participants are identified using pseudonyms. Demographic characteristics were not collected and are not provided. Brackets within quotes summarize removed content or clarify referents.
Ethics
This study was determined exempt by the Ohio State University (Protocol #2023E0512). IRB Review Exemption was based on criteria that disclosure of responses outside of the research context would not reasonably place participants at risk of legal, financial, or reputational harm. Questions focused on clinical perceptions and practice experience; no individually identifiable data were collected. All participants provided informed consent prior to enrollment.
Results
Analysis revealed common core ideas about how providers perceived changes in mental health and substance use during the COVID-19 pandemic, and their approach to substance use concerns during the initial phase of the pandemic. Abductive analyses highlighted that substance use treatment providers and mental health providers conceptualized changes in different ways. Both groups appeared to perceive a hierarchy of importance of addressing various substances, with tobacco and marijuana often being less important than primary mental health or “riskier” substance use. Notably, providers appeared to categorize tobacco use separately from other substances. While informants alluded to a conscious de-prioritization of tobacco use, this phenomenon extended beyond the pandemic. Providers described abstinence-only models of treatment, but their conceptualization of abstinence-only did not include cessation of tobacco use. It is important to note that providers’ perceptions and clinical beliefs do not always align with current research evidence; where relevant, such discrepancies are noted throughout. The following sections describe patterns and core theoretical ideas that emerged from the analysis of transcripts, the synthesis of which is represented in a conceptual model (Figure 2).
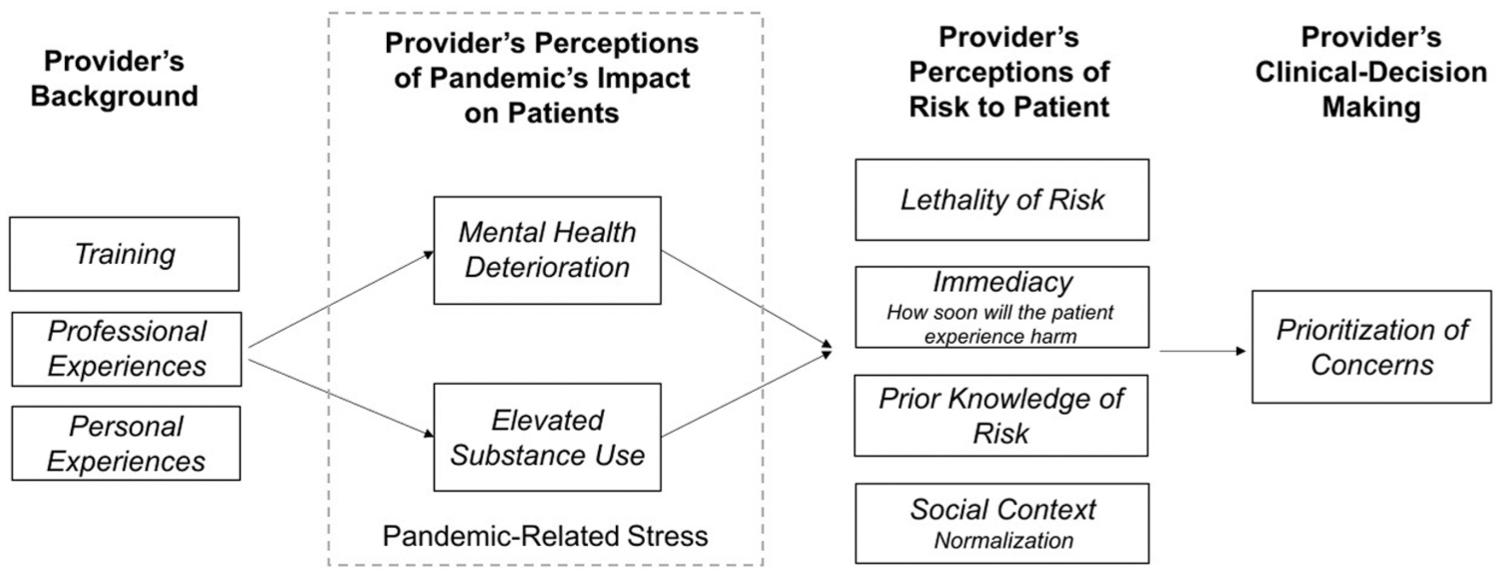
Conceptual model of how behavioral health providers made clinical decisions to prioritize or de-prioritize patient concerns in response to elevated stress from the COVID-19 pandemic.
The COVID-19 pandemic worsened mental health
All 21 providers witnessed declines in their patients’ mental health during the COVID-19 pandemic, blaming this on pandemic effects. Informants observed worsening symptoms, including elevated depression, anxiety, suicidal ideation, and increased stress from unmet care needs across their entire patient population.
Providers worried that isolation from stay-at-home orders worsened mental health. Compounding this, patients experienced challenges in accessing treatment services. Providers felt unprepared for the sudden shift to telehealth, citing a lack of resources and training. Providers also emphasized harm to patients’ interpersonal relationships. Kyle, a substance use treatment provider, described this: We saw a lot of isolation amongst our patients. . .[patients] didn’t realize how much they relied upon those relationships of going out to the grocery store . . .when everything switches over to electronic or to online, I think it takes a toll on folks’ mental health.
Substance use increased during the COVID-19 pandemic
Informants highlighted changes in substance use during the COVID-19 pandemic, describing increases in use of tobacco, marijuana, methamphetamine, alcohol, and opiates. However, providers gave limited responses and expressed an unwillingness to discuss specific changes, citing unfamiliarity with literature and statistics. The brevity of responses prevented a robust inductive analysis.
Analysis of why informants understood substance use to have increased revealed common rationales. First, patients used substances to cope with pandemic stress. Specifically, patients were using substances to alleviate depressive and anxious feelings. Most of those who described this phenomenon explicitly invoked the language of “self-medication.” Jessica, a mental health provider, articulated this concept in the context of pandemic-related substance use, [Substance use] definitely increased. . .like a self-medicating thing or a coping skill that people were using to deal with the worsening mental health . . . and uncertainty about the future. . .I think a lot of people coped with that by turning to substance use, whether they had previously been using substances. . . or. . .turning to it for the first time.
Like many providers, Jessica did not appear to conceptualize this dynamic in the context of specific substances.
Informants further attributed patients’ increase in substance use to their inability to access support services. As treatment centers and community support groups closed during the initial phase of the pandemic, providers became concerned that patients were at a higher risk of relapse during this time. Substance use providers focused on closure of recovery support groups; mental health providers described loss of connection with case managers and group sessions. Madison, a mental health provider, asserted that patients struggled with their mental health due to these changes, Throughout the pandemic, and especially early on, [there were] challenges with some of our patients . . . getting their medications, attending follow-up appointments. . .case managers were not allowed to transport them. . .[Patients] started falling off with missing appointments. . .which resulted in the influx into the inpatient units.
While informants expressed optimism that telehealth options helped meet a need for care, they did not see it as equivalent to an in-person connection. Emma, a substance use provider, worried patients didn’t benefit from online substitutes: “changes to the meeting formats [were detrimental] . . .there were meetings available virtually, [but] it still wasn’t the same. People who had been in live meetings. . .before would say. . . it doesn’t feel the same. . .I feel disconnected.”
A further rationale was that patients lost external motivators that helped them regulate consumption of substances during the pandemic. Providers normally receiving court-mandated referrals noted census decreases as fewer patients were required to seek treatment. One stated, The majority of the clients we see in substance use [are] court ordered and because people were in their homes, and they weren’t out committing crimes. . .[Court referrals] really went down. . .there was less motivation, because people [weren’t] self-selecting (Amber, mental health provider).
Further, providers noted that the shift to remote work allowed patients to use substances more discreetly, particularly alcohol and marijuana, as they were not required to be physically present in their workplaces.
Substance use, particularly alcohol consumption, was normalized during COVID-19
Informants witnessed a normalization of substance use during the pandemic, focusing on the use of marijuana and alcohol, and vaping of nicotine products. However, providers differentiated increased acceptance of substances that they ascribed to the pandemic from increased acceptance that occurred as part of broader trends.
For example, participants seemed to tie the normalization of marijuana use to legalization efforts. One provider, Sarah, described the changes she saw, I think I have seen a slow increase in marijuana. . . I see that slow transition in marijuana in Ohio from when medical [marijuana]. . .came into play. And now, with the passage of the legalization of marijuana. . .Everyone saw the world did not fall apart. You just saw the increase in use, and now it is just acceptable. . . people’s perceptions of it have changed.
Sarah’s account reflects a broader policy context that was actively shifting at the time of data collection, as Ohio’s evolving marijuana legalization landscape contributed to changing social attitudes and perceptions of the substance among both patients and providers. Similarly, other providers viewed vaping as more socially acceptable in the context of the pandemic, part of a broader trend predating COVID-19.
In contrast to marijuana and vaping, providers considered patients’ normalization and increased use of alcohol as specific to the pandemic. As Kyle described, “there were several times where we had patients trying to drink on camera from their basement or from wherever [. . .] on Uber Eats you can have alcohol delivered right to your house, so I think that accessibility factored in a ton.” Kyle’s account illustrates not merely an increase in alcohol consumption, but a broader shift in its social acceptability, as alcohol became more accessible and more openly consumed in contexts where it previously would not have been.
Interestingly, informants seemed to root their ideas about the normalization of alcohol not only in changes they saw in their patients but also in their own personal experiences during the pandemic. For example, one provider described, At least once or twice a month [we] started doing Zoom happy hour. We would all sit at home and get on Zoom calls. . .[the calls] would be around drinks and my one girlfriend would be [saying] ‘I’m already done my first bottle of wine’ [and] in a normal time. . .she would be at home, just getting off work and making dinner” (Sarah, substance use provider).
Sarah’s account illustrates how pandemic conditions shifted the social context of alcohol consumption, with behaviors that would previously have been considered atypical becoming socially accepted. Across their personal experiences, providers tied the normalization of alcohol consumption to feelings of elevated stress and a pervasive sense of uncertainty. One provider described, “a lot of friends . . . a lot of coworkers. . . would say the same thing. . .it was like World War Three, we didn’t know what was going to happen.” Providers framed the normalization of alcohol to worsening stress that they saw not only among their patients, but also among themselves.
Consciously deprioritizing tobacco and marijuana during COVID-19: “It felt like the least of my concerns.”
During the pandemic, providers needed to adapt to sudden shifts in the mental health and substance use of their patients. Providers felt they could only meet the most pressing concerns facing their patients – their experiences of depression, anxiety, and suicidal ideation. While providers still felt that treating tobacco use was important, they acknowledged deprioritizing it during the pandemic. Interestingly, substance use providers tended to focus on patients’ use of “riskier” substances, while mental health providers appeared more concerned about patient’s deteriorating mental health.
During the pandemic, mental health providers prioritized treating more severe mental illnesses over addressing patients’ tobacco and marijuana use, “I think we were more concerned with keeping our severely depressed. . .severely mentally ill population alive. We need to keep them medicated. I think [smoking cessation] took a back burner” (Rachel, mental health provider). Mental health providers appeared to prioritize primary mental health concerns over not just tobacco, but also other substances, including marijuana. Britney, a mental health social worker, described a conscious decision to shift attention away from substance use toward a focus on mental health, “it felt like [tobacco and marijuana were] the least of my concerns in the pandemic. . .it’s not that they’re not relevant, or they don't deserve to be treated, but if those are the only things that people are using . . .I wasn’t as concerned about that.”
Similar to those in mental health, substance use treatment providers also described a conscious de-prioritization of tobacco and marijuana use during the pandemic. Substance use providers focused on addressing substances other than tobacco or marijuana. As Hannah described her thought process, Tobacco use is something that is important for us to address . . .[but] if there was a higher priority of something a little bit more urgent, we would maybe not prioritize it above something else. So [if] somebody is using opiates or somebody is smoking cocaine, we would tailor it to what is more harmful. . .the more acute need (Hannah, substance use provider).
Substance use providers focused on what they referred to as “more harmful” substances over tobacco; these included opiates, alcohol, cocaine, and methamphetamine. They feared that patients could die if their use of these harmful substances was not addressed, highlighting the immediacy and potential lethality of potential overdoses. Informants approached patients’ use of marijuana similarly. One described, “At least [marijuana] is not fentanyl or alcohol. . . we know there has never been any marijuana overdoses” (Chelsea, substance use provider). When confronted with the possibility of lethal harm from patients’ substance use, providers deliberately chose to focus on other concerns aside from tobacco or marijuana.
Providers weigh the physical health consequences of tobacco with the mental health harms of marijuana
Providers were acutely aware of the harms of tobacco smoking, highlighting the fact that they treat many patients with chronic diseases caused by tobacco use. Informants framed tobacco’s harms in terms of the physical sequelae of chronic use: COPD, emphysema, and lung cancer. In contrast, providers conceptualized the harms of marijuana use primarily in terms of its mental health consequences. John, a substance use provider, explained, [Tobacco and marijuana] are both very different. When you are talking about the dangers to your primary health. . . you may want to look a bit more at what disadvantages tobacco offers. When you are talking about beginning to become needy and dependent on something. . .the number of other substances [marijuana] opens you up to its more dangerous when you are looking at the side of marijuana.
Informants expressed that the most salient concern with tobacco was cancer risk. Tyler, a substance use provider, felt that tobacco’s physical health consequences outweighed the harms of marijuana: Most people think that tobacco is going to cause a lot more problems. . .than marijuana [will] . . . I think about the number of clients we have had who get lung cancer and die, who have emphysema. . .and other kinds of vital organ problems. Then, I think about the people who had just smoked pot and I do not think they have the same kind of problems.
While informants framed tobacco’s harms around long-term physical illness and lethality, providers felt that marijuana’s harms were primarily mental health consequences. Informants often felt that patients did not understand the potential consequences of using marijuana to cope with psychological distress. For example, Britney described, “people know that marijuana can make you kind of paranoid, but I do not think they realize that if you have any sort of underlying genetic predisposition for an acute mental illness like bipolar or schizophrenia; if you use marijuana, it can trigger that” (Britney, mental health provider).
Providers did feel marijuana could cause physical harm as well but seemed to lack the confidence to make definitive assertions. Emma, a substance use provider, expressed, “I know even among professionals, there’s a mixed point of view about [marijuana being] good or bad. I think, ultimately, the jury is still out because they are still doing a lot of different research on it.” Like many providers, Emma felt the scientific evidence on marijuana’s harms remained unsettled. Informants predicted that they would have a better understanding after more research is conducted, but were uncertain about how long this would take, “Marijuana is new now that it is fully legal. I think it is going to have that. . .20, 30, 40-year impact before it is going to have those negative ramifications and going to have research that shows this” (Sarah, substance use provider).
Gateway drugs: Framing the harms of tobacco and marijuana in the context of other substances
Both substance use and mental health providers framed tobacco and marijuana as “gateway drugs.” Providers recognized that patients’ use of tobacco was deeply intertwined with larger substance use concerns, “they have shown a lot of studies about nicotine enhancing the effects of other substances, which causes higher propensity for addiction to other substances, so nicotine is the true gateway drug” (Emma, substance use provider).
Similar to tobacco, providers tended to view a patient’s possibility of progressing toward “more dangerous” substances as an integral harm of marijuana: Certainly, when people start using marijuana, they start using other drugs. . .The gateway. I don’t think it is an automatic gateway that people start using marijuana and then they start using pills and they start shooting drugs. . .I do think that when you are in that environment and run with people who use a lot of marijuana, you are frequently going to use other substances. . .Most people do not start by using heroin or an opioid. They have frequently used alcohol and marijuana first (Tyler, substance use provider).
Informants witnessed many patients inadvertently using other substances, such as fentanyl, because they had obtained marijuana that was adulterated. Notably, providers framed marijuana’s physical harms not through its intrinsic effects but through its association with adulterated or co-used substances. It should be noted that the gateway drug hypothesis, while reflected in providers’ accounts, is a contested concept in the literature.
Acceptance of tobacco use by substance use providers: Prioritizing other substances at the expense of tobacco cessation
Substance use treatment providers discussed tobacco use in a substantially different way from mental health providers. While substance providers were aware of the harms of tobacco smoking, they appeared to accept it, even describing it as a substantial part of the culture of treatment. In recovery settings, not only did patients routinely use tobacco products – but staff members did as well. Angela, a clinical social worker at a community-based substance use treatment facility, asserted, “our population is heavy smokers, just in general, and we are an agency that allows [smoking]. We do offer [smoking] cessation for folks who want to work on that. But it is part of the culture of our organization that [smoking] is what people do on breaks. . .They go outside and have a cigarette.”
Informants working in substance use settings appeared hesitant to promote greater tobacco cessation initiatives. Darren, the director of a substance use treatment facility, confidently asserted that allowing patients to continue to smoke and access tobacco products improved their recovery. He began, “cigarettes are harm reduction. . .if our clients don't buy cigarettes on our campus, they'll go up to the corner store and the corner store is exactly where the drugs are. . . I would rather them stay with us. . .and lower their relapse potential.” He elaborated that giving patients the opportunity to purchase cigarettes at the facility prevented them from leaving the facility and experiencing triggers that could cause them to relapse. For Darren, allowing patients to smoke tobacco resulted in higher engagement in treatment and helped people quit using other substances, such as opiates. He stated, We have this very intentional approach. . .when you look at a lot of organizations or hospital systems that. . .run outpatient behavioral health, they typically do not have a high census. It is because . . . they cannot permit cigarette smoking on their campus. So, you usually see people go more to these community-based health centers because they have access to [cigarettes]. . .cigarette choice is a huge factor whether people seek out treatment.
Darren’s description was not unique – substance use providers felt that patients seeking treatment for substances other than tobacco might disengage from treatment entirely if they were encouraged to quit tobacco products. It should be noted that this perception is not supported by the research literature, which indicates that tobacco cessation does not reduce treatment engagement and is associated with improved SUD outcomes.
Where providers differ: How do informants develop their perceptions of harms?
Informants emphasized the diversity in backgrounds of behavioral health workers as a key element underlying the differences in how providers address substance use, particularly tobacco and marijuana use. In contrast to the differences between mental health and substance use providers detailed in previous sections, which emerged from the abductive analytic process, informants themselves divided behavioral health providers differently, grouping them as medical providers or counselors. As Jessica articulated, “I do think the medical side approaches [substance use] a bit differently. . .I do not think it is necessarily in a negative way, but I think they focus a lot more on the diagnostic criteria associated with substance use.” She contrasted this with how she perceived social workers to focus on addressing the underlying reason that patients are using a substance. She then continued to describe how this difference might impact substance use treatment, “I think that sometimes the medical providers can encourage the cessation or abstinence more than [counselors] do. Because again, of the difference between the psychological aspect versus the medical aspect of substance use.” She concluded that she does not see a difference in patient outcomes based on these approaches.
Informants attested that their personal experiences treating patients were crucial in developing their approach to addressing substance use and its harms. Reflecting on his own experience in the field as a substance use counselor, Tyler said: When you listen to clients over years and years. . .you start to have a different perspective. . . and over the years, my attitudes about this [has] changed somewhat because I hear what [patients] are going through. And I hear their voice and the anxiety . . .and so I do think the longer you’re at it, the more likely you are going to be able to have a full world view.
His perspective, shaped by years of direct clinical experience, was echoed by other providers with a counseling background. Among mental health practitioners, psychosis treatment providers appeared to hold a unique outlook. Even providers outside this specialty noted that psychosis specialists likely hold distinct views given the strong links between tobacco, marijuana, and psychosis. For example, Madison described her experience working as a psychosis treatment provider, I think the other colleagues that worked on the inpatient unit during the pandemic that did not specialize in psychosis probably would. . .probably see smoking tobacco is the least of their worries if they have got other things going on. And often marijuana is a more harmless drug as well. I think it is really more a unique perspective of people working with psychosis sometimes that the focus is a little bit more on those [tobacco and marijuana] than other areas.
Madison’s psychosis background informed her view of tobacco and marijuana as clinical priorities.
Another unique division that emerged from multiple interviews was between harm-reduction models and abstinence-only models for treating substance use disorders. Among those who promoted an abstinence-based approach, some rooted that decision in their own lived experiences. Kyle, articulated, “We started out abstinence-based. . .just based off of the fact that three out of the four of our co-founders are in recovery and abstinence is what worked for us. But we quickly realized that it is not what works for the majority of people. If we can help somebody not stick a needle in their arm tonight. . ..let’s start there” Kyle further described his own experience in recovery and how that has informed his practice, “I have been through withdrawals and I have experience with Suboxone. . .I can tell you that it can help tremendously. . .We started out with no MAT [Medication-Assisted Treatment], . . .we were not going to help folks long if we don’t really open our mind to there being multiple pathways to recovery.”
Providers who promoted an abstinence-based approach appeared to exclude tobacco from their definition of abstinence. Darren, describing the workforce at his facility, said, “90 percent of our workforce is in recovery, and they are probably smoking too [. . .] because most are in recovery. . .. there’s a higher rate of tobacco use in the recovery population as well as the active using population. . .I would say [tobacco] is probably less likely to be treated the way it needs to be treated.” Darren acknowledged that tobacco use was not as likely to be addressed, stating that providers tend to presume that quitting tobacco is not a necessary part of abstinence. Informants repeated that even in abstinence-based treatment centers, patients routinely smoked, as it was part of the facility’s culture. One provider, Shana, anchored her personal philosophy of abstinence in the idea that no substance is more harmful than another, “[I] remember that they are all-inclusive and no one drug is more powerful or less than the next. Again, a drug is a drug is a drug. . .I strive not to compare them. . .because the only thing I know is that they all lead to death.” Interestingly, Shana, like many substance-use providers, appeared to exclude tobacco from her conceptualization of substance use treatment.
Discussion
The inductive and abductive analyses conducted in this study produced a conceptual model (Figure 2) that illustrates how providers prioritized tobacco and marijuana concerns during COVID-19. Pre-pandemic, providers’ opinions were shaped by training, clinical, and personal experiences, through which they understood the pandemic’s effects on patients. As pandemic-related stress was associated with worsening psychological distress, providers described this as contributing to elevated substance use. Providers described addressing concerns based on perceived severity and urgency; for example, suicidal ideation posed an immediate risk, whereas smoking’s harms would manifest years later. Providers further rooted their understanding of harm in their knowledge and social context of the harm. For example, the normalization of tobacco in substance use recovery may alter how harmful a provider perceives it to be. Specific mental health or substance use concerns were then prioritized or de-prioritized based on how harmful a provider perceived the concern to be for the patient. Across our sample, we found that informants consciously de-prioritized tobacco and marijuana use.
The conceptual model suggests that providers’ prioritization decisions are shaped not only by clinical training but by perceived risk, social normalization, and the broader context in which care is delivered. Prior research has documented that tobacco use is deprioritized in behavioral settings and that providers hold misconceptions about harms of addressing tobacco use (Goodwin et al., 2021; Rogers et al., 2018), but has not articulated the underlying cognitive and social processes by which these clinicians reach these decisions. The four-stage pathway from background through risk perception to clinical-decision making identifies specific leverage points, where targeted interventions may shift clinician behavior. The model offers a foundation for future research examining clinical-decision making and intervention development in behavioral health settings. Notably, the process we present is not necessarily specific to the COVID-19 pandemic; the same pathway may operate in settings where providers face elevated patient need and competing clinical demands.
The language and concepts described by behavioral health providers are consistent with the self-medication hypothesis (Khantzian, 1997). Providers framed the pandemic as a stressor that exacerbated psychological distress, which was associated with increasing substance use. Providers’ perceptions diverged from the self-medication hypothesis, however, in describing the social factors that contribute to substance use: external pressure such as employers or the criminal justice system, the social normalization of substances, and the presence or absence of social support. The prominence of social and structural factors in providers’ accounts suggests that alternative frameworks such as the common liability model, which emphasizes shared environmental vulnerabilities rather than a unidirectional causal pathway, may also help explain these patterns (Vanyukov et al., 2012). How a provider perceives the patient’s use of substances, particularly within a provider’s social context, influences whether the use is normalized or pathologized. Providers exhibited this phenomenon when describing patients’ tobacco use in recovery settings, where providers normalized patients’ smoking in keeping with the social and historical context of frequent tobacco use in treatment settings.
Tobacco’s unique status in behavioral health providers’ conceptualization of substance use emerged as a central finding. Substance use providers in particular distinctly deprioritized tobacco, consistent with prior research conducted outside the pandemic context (Rogers et al., 2018). Organizational factors, including limited managerial support for cessation and lack of training, have been identified as persistent barriers to implementing tobacco cessation services (Knudsen et al., 2012, 2013). High rates of tobacco use among both clients and staff in SUD treatment settings have been well documented and are suggested to influence the patient’s receipt of tobacco services (Guydish et al., 2022; Pagano et al., 2016). Taken together, these findings suggest that tobacco deprioritization in behavioral health predates the pandemic and reflects persistent structural and cultural barriers to addressing tobacco use in these contexts.
The historical context of tobacco use in mental health and substance use treatment continues to hinder tobacco cessation. Behavioral health providers often hold erroneous beliefs due to historical norms: opinions that it will harm recovery, concerns that a smoke-free environment will lead to treatment disengagement, and an exclusion of tobacco from an abstinence-paradigm (Goodwin et al., 2021; Ouellet-Plamondon et al., 2014). Research demonstrates that quitting smoking is associated with improved SUD treatment outcomes, including reduced relapse (McKelvey et al., 2017). Despite this evidence, these misconceptions persist among providers. Notably, some providers framed allowing patients to continue smoking as a form of harm reduction that supports engagement in treatment. This perception is not supported by the research literature (McKelvey et al., 2017).
Addressing these misconceptions may assist in counteracting the historical normalization of tobacco in behavioral health settings. Targeted training programs can dispel specific falsehoods, such as fears that cessation interferes with treatment or that patients are not interested in quitting. Research highlights that patients in substance use treatment are interested in quitting tobacco, and those who quit smoking are more likely to abstain from other substances (Goodwin et al., 2021). Further, training programs could improve provider comfort with prescribing cessation pharmacotherapy, as limited familiarity with treatments has been posited as a persistent barrier to addressing tobacco use (Iyahen et al., 2023; Rogers et al., 2018). Beyond education, organizational mandates, such as smoke-free facility policies, can support cessation efforts; facilities in states with stronger smoke-free laws are more likely to provide cessation services (Shi and Cummins, 2015). Together, training programs and organizational policies may shift norms and reduce the tobacco-related disease burden in this population.
Research on how healthcare providers address marijuana use is limited. Surveys suggest that while providers recognize risks, many are uncertain as to what these risks entail and lack confidence in conveying them to patients (Brooks et al., 2017). For example, obstetrics providers perceived marijuana as less harmful than other substances and did not consider it a treatment priority (Holland et al., 2016). Providers’ uncertainty about marijuana’s harms may also reflect the rapidly evolving policy and social context surrounding marijuana in Ohio, where recreational legalization had only recently passed at the time interviews were conducted. As patients rely on their healthcare team as a trusted source of information, providers must be able to effectively counsel their patients on marijuana use.
Few studies compare provider perceptions of marijuana use with tobacco. One qualitative study found that providers viewed marijuana as a gateway drug with harms similar to those of tobacco (Bascombe et al., 2016). In contrast, providers in our study noted unique harms from tobacco and marijuana, with providers noting psychological risks for marijuana and carcinogenic concerns for tobacco. It should be noted that the gateway drug hypothesis is highly contested; alternative frameworks, such as the common liability model, better account for patterns of co-occurring substance use (Vanyukov et al., 2012).
The inclusion of a broad range of behavioral health providers, spanning both mental health and substance use treatment backgrounds, offers important context for interpreting our findings. Though behavioral health encompasses both substance use and mental health, these domains have historically operated separately (Grella, 2003). Research indicates a lack of integrated dual-diagnosis training; social workers report greater training in mental health, while chemical dependency counselors are trained in substance use treatment (Fisher et al., 2014). This may partly explain our findings, where providers trained in substance use emphasized addictive substances, and mental health providers focused on other psychiatric concerns.
To our knowledge, our research is among the first to examine how behavioral health providers prioritize tobacco and marijuana during a time of widespread psychological distress. These findings have direct training implications, highlighting the need to educate behavioral health providers on the importance of addressing tobacco and marijuana use among their patients. Alongside provider education, organizational policy represents a critical lever for change; however, only 14 states require tobacco-free grounds for most mental health or substance use facilities as of July 2023 (Public Health Law Center, 2023), underscoring the need for continued advocacy. Importantly, the conditions that shaped provider decision-making in this study are not unique to the COVID-19 pandemic, and findings may therefore inform behavioral health practice and preparedness for future public health crises.
Limitations
This research has several limitations. First, despite a sampling strategy designed to ensure equal probability of contact across provider types, the final sample overrepresents community-based social workers, which may limit generalizability to providers in hospital-based or residential settings and preclude systematic comparisons by professional role or educational background. Information on whether participants’ facilities implemented smoke-free policies or formal tobacco cessation programs was not systematically collected. While providers’ treatment approach, including abstinence-based or harm-reduction approaches, was not recorded as a study variable, it emerged organically in several interviews. Future research should systematically examine variation by professional role, treatment setting, and facility-level policy context. Additionally, the study design did not allow us to assess whether deprioritization of tobacco and marijuana was unique to the pandemic period or whether clinical practice returned to pre-pandemic patterns following the acute phase; future research should examine these temporal dynamics directly.
Second, some analytic categories remained unsaturated, which we identified through abductive methods. For instance, many providers speculated that psychosis specialists would approach substance use differently, but only one was interviewed.
Lastly, our findings may be affected by recall bias, as interviews referenced events from approximately 3 years before interviews were conducted. Recall of emotionally challenging events is particularly susceptible to memory degradation and post-hoc sense-making over time, and the pandemic unfolded across multiple phases with varying levels of restriction and distress, making precise temporal recall especially difficult. Social desirability bias is also possible, as providers may have been unwilling to contradict accepted treatment guidelines. However, this is unlikely as informants spoke candidly about how tobacco and marijuana were not prominent concerns. Future research might also consider alternative theoretical frameworks for understanding provider decision-making, such as the Health Belief Model, which could offer a complementary lens for examining how providers assess perceived susceptibility, severity, and benefits when prioritizing patient concerns.
Conclusion
Behavioral health providers systematically deprioritized tobacco and marijuana when confronted with competing clinical demands, with differences emerging between mental health and substance use treatment providers. Tobacco held a unique status in recovery settings, where social norming reinforced its exclusion from abstinence frameworks. Targeted provider training and smoke-free facility policies may help address these persistent patterns, with implications extending to future public health crises.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261461883 – Supplemental material for Behavioral health providers’ prioritization of tobacco and marijuana concerns during the COVID-19 pandemic: A grounded theory analysis
Supplemental material, sj-docx-1-hpq-10.1177_13591053261461883 for Behavioral health providers’ prioritization of tobacco and marijuana concerns during the COVID-19 pandemic: A grounded theory analysis by Geoffrey J. Carney-Knisely, Amy K. Ferketich, Parvati Singh, Tamar L. Gur and Tasleem J. Padamsee in Journal of Health Psychology
Footnotes
Acknowledgements
The authors would like to thank Siddarth Dasari for his assistance with transcribing interviews.
Author note
All authors meet the International Committee for Medical Journal Editors (ICMJE) criteria for authorship. Geoffrey Carney-Knisely was involved in the conceptualization, data collection, analysis, and writing of this manuscript. Amy Ferketich was involved in conceptualizing the research question, the validation, and the approach of the research. Parvati Singh and Tamar Gur both were involved in critically evaluating the research approach, investigation, and review of the research. Tasleem Padamsee was involved in the conceptualization, data curation, analysis, validation, and writing of the manuscript. All authors participated in the drafting and revisions of the manuscript. All authors approved of the manuscript before submission.
Ethical considerations
The Ohio State University Institutional Review Board (Protocol #2023E0512) determined that this study is exempt from IRB review. All participants provided informed consent prior to enrollment.
Consent to participate
All participants provided written informed consent prior to enrollment.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ohio State University Graduate School’s Alumni Grants for Graduate Research and Scholarship.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data used in this study are not publicly available due to privacy concerns. Participants provided detailed accounts of personal and professional experiences related to mental health and substance use that are included in verbatim transcriptions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.