
Abstract
Adults with low socioeconomic status (SES) experience profound tobacco-related health disparities. This paper describes the development of a mobile application, iQuit Mindfully 2.0, to provide accessible mindfulness training for smoking cessation for adults with low SES. In the initial usability study, adults with low SES who smoked (N = 16) used the app for 2 weeks and provided feedback through individual interviews, which were coded using NVivo. Participants appreciated that the app was simple and easy to use, relatable and personalized, and taught mindfulness practices for coping with stress and cravings. The app helped them reduce their smoking, develop greater confidence in their ability to cope with cravings, and recover from smoking lapses. Participants suggested ways to increase interactivity and social support, improve smoking behavior tracking, and enhance app esthetics. This feedback will be used to improve the app with the goal of providing accessible smoking cessation treatment for low-SES populations.
Introduction
Tobacco use is the leading preventable cause of morbidity and mortality (U.S. Department of Health and Human Services, 2014), with disproportionately high prevalence of smoking and associated health consequences among adults with low socioeconomic status (SES; U.S. National Cancer Institute, 2017). Although most U.S. adults who smoke want to quit and over half have tried to quit in the past year, less than 10% successfully quit, and adults with low SES have greater difficulty quitting (U.S. National Cancer Institute, 2017; VanFrank et al., 2024). Populations with poorer financial, structural and social resources face formidable day-to-day barriers, including societal (e.g. low healthcare access), community (e.g. tobacco advertising; neighborhood stress), interpersonal (e.g. social norms for smoking; low social support), and intrapersonal factors (e.g. high stress, low self-efficacy), that all collude to foster addiction and impede efforts to quit (Businelle et al., 2010; Hiscock et al., 2012; U.S. National Cancer Institute, 2017). There is a need for evidence-based smoking cessation interventions that are tailored to address barriers to cessation for adults with low SES.
Mindfulness is purposeful, present-focused attention with an attitude of acceptance and non-judgment (Kabat-Zinn, 1990). Mindfulness-based interventions (MBIs) are efficacious for improving a variety of psychological health outcomes (Goldberg et al., 2018; Khoury et al., 2015) and reducing substance use (Li et al., 2017). Growing research supports MBIs for smoking cessation. A meta-analysis of randomized controlled trials (RCTs) found that participants receiving mindfulness training were almost twice as likely to quit smoking than those receiving usual care (25.2% vs 13.6%; Oikonomou et al., 2017), although more research is needed to address inconsistencies across studies (Jackson et al., 2022). Mindfulness may also prevent early smoking lapses from transitioning to full-blown relapses (Heppner et al., 2016; Vidrine et al., 2016), which is critical given the prevalence of early lapses (Brown et al., 2005).
Most mindfulness research has focused on higher-SES and non-Latino White populations, although several studies support the promise of MBIs in low-SES and racially/ethnically diverse populations (Foale et al., 2024; Sun et al., 2022), including for smoking cessation (Brewer et al., 2011; Davis et al., 2014; Vidrine et al., 2016). Mindfulness practice (e.g. mindfully focusing on one’s breath) does not require socioeconomic resources. Mindfulness training directly targets stress and negative affect, which are critical barriers to smoking cessation for populations with lower SES (Cambron et al., 2020), who are more likely to experience stress associated with finances, housing, and other factors (Kraft and Kraft, 2021). Mindfulness training can weaken associations of both stress and craving with smoking (Brewer et al., 2013), such that people observe and accept these experiences without trying to cope by smoking. Studies indicate that mindfulness “decouples” links between negative affect/craving and substance use (Brewer et al., 2013; Elwafi et al., 2013). Given that negative affect and craving are potent smoking triggers, the potential for mindfulness to break these links is unique and promising.
MBIs that are delivered through weekly in-person sessions are not easily accessible for populations with low SES. In-person programs like Mindfulness-Based Addiction Treatment (MBAT; Vidrine et al., 2016) require substantial time (8 weekly 2-hour sessions) and resources (therapist time, facilities, travel, etc.). Adults with low SES often face challenges such as inflexible work schedules and limited transportation (Copeland et al., 2010) which severely limit access to in-person treatments.
Mobile health technology (mHealth) could be a cost-effective way to provide personalized, in-the-moment support for overcoming barriers to smoking cessation among adults with low SES (Businelle et al., 2024b). These interventions can reduce stigma associated with in-person treatment, encourage strategies in real-time (e.g. when stressed or craving), and standardize treatment in a way that is typically not possible with in-person services. Smartphone ownership has been rising rapidly among low-SES populations. In 2024, 84% of Americans with annual income <$30,000 and 87% of African Americans owned smartphones (compared to 91% smartphone ownership among American adults overall; Pew Research Center, 2025). Lower-income adults are more likely to rely on their smartphones for internet access (Pew Research Center, 2025). Although most apps have not been designed for or evaluated specifically among adults with low SES, recent research supports the promise of apps for smoking cessation in low-SES populations (Businelle et al., 2024b; Hébert et al., 2025). Smoking cessation apps that focus on mindfulness and acceptance have been developed for the general population with promising findings, such as “Craving to Quit” (Garrison et al., 2020), “SmartQuit” (based on Acceptance and Commitment Therapy (ACT) which includes mindfulness (Bricker et al., 2014, 2017)), and iCanQuit (also based on ACT (Bricker et al., 2020)), though these apps were not specifically designed for low-SES populations.
Through iterative feedback from adults with low SES, our team developed a text messaging program (iQuit Mindfully 1.0) that provides personalized, interactive messages to encourage mindfulness and other smoking cessation techniques in daily life. iQuit Mindfully 1.0 messages showed particular promise for enhancing smoking cessation among participants living in poverty (Spears et al., 2019a). However, a mobile app could provide more information and support than text messaging alone. Apps can provide a wider variety of content, including video and audio, and can allow users to access content even when cellular service or internet connectivity are limited. This paper describes the development of iQuit Mindfully 2.0 (i.e. MBAT + iQuit Mindfully 1.0, fully delivered through an app) and initial usability testing to examine acceptability and suggestions for improvement among a sample of low-SES adults.
App development
Overview
We took a user-centered design approach based on expert recommendations (Abroms et al., 2015; Bock et al., 2015) to elicit input from the target population throughout development. First, the app notification messages were developed based on iterative testing with a predominantly low-SES sample of adults who smoked. For more details, see (Spears et al., 2019a, 2019b). Next, the study team (with expertise in smoking cessation among adults with low SES, app development, mindfulness, and health disparities) collaborated to adapt MBAT content (Vidrine et al., 2016) for the app. The eight MBAT sessions were implemented through eight app modules. The intervention is grounded in theoretical models of mindfulness for treating addictions (Brewer et al., 2013). The app development process included hiring racially/ethnically diverse actors and partnering with a video production company to develop short videos. Overall, the content and format were designed to be clear, relevant and accessible. The app was programmed using Insight™ and tested internally before launching the usability study described below.
App features
Features are organized into the following options on the home screen: Tips, Guided Mindfulness, Nicotine Patches/Lozenges, Track My Progress, and Parts (i.e. app modules). See Table 1. The top of the screen also includes options to “Call Quit Coach” (to call the Tobacco Quitline) and “Call Staff” (to call the research team).
Features of iQuit Mindfully 2.0 App.
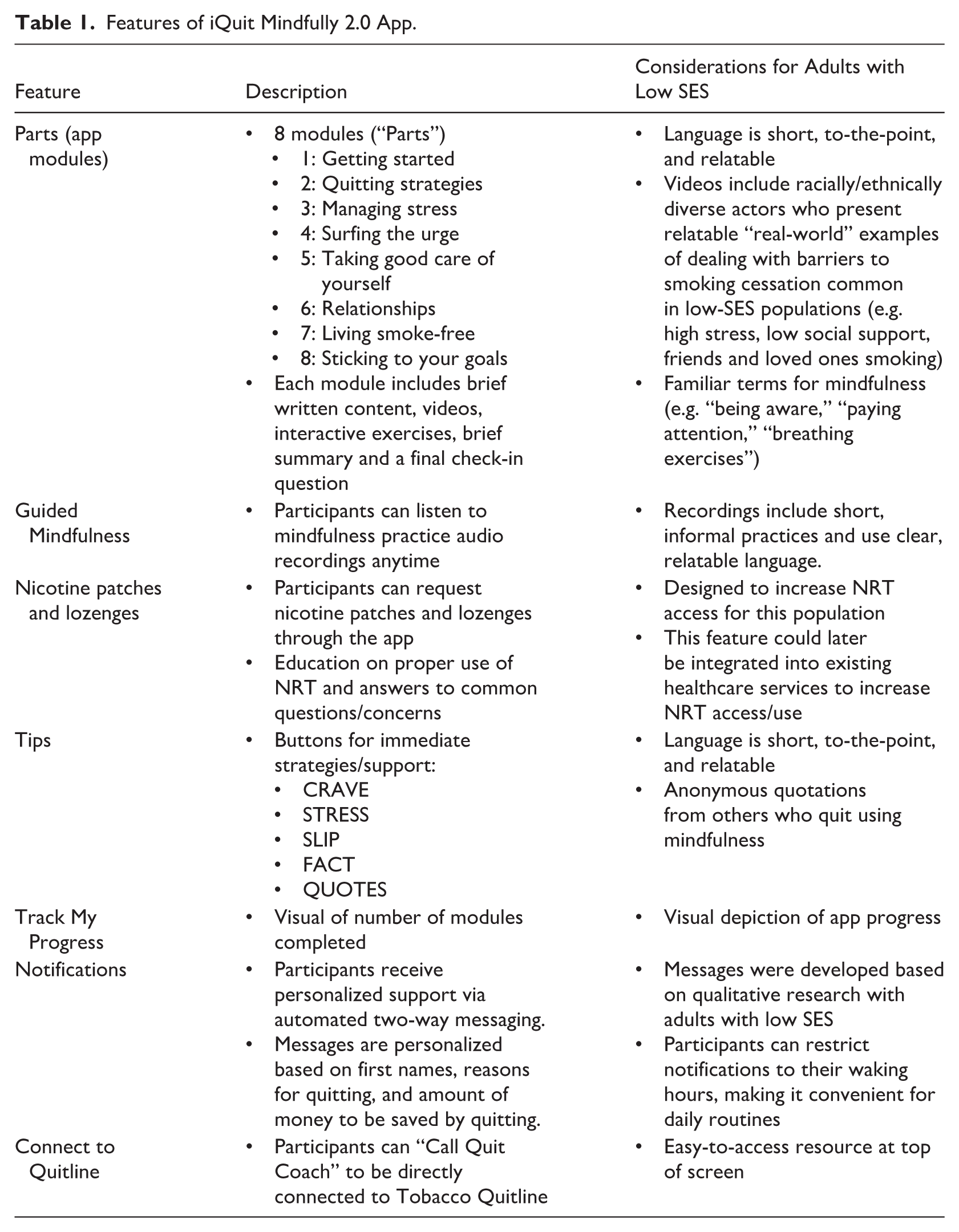
Within Parts, the eight modules developed based on MBAT naturally build upon each other. Participants need to complete each module before opening the next, but they can move through the modules at their own pace. Parts modules include brief written content highlighting key topics/strategies (e.g. “What is mindfulness?” “How can mindfulness help me quit?” “Tips for getting through urges to smoke,” “What to do if I slip?”). More familiar terms are used for mindfulness (e.g. “being aware,” “paying attention,” “breathing exercises”) based on previous qualitative work (Spears et al., 2017, 2019b). Each Parts module includes 1–3 videos (2–3.5 minutes each) showing the story of how the main character “Mike” quit smoking by practicing mindfulness, including his struggles with common challenges like stress, being around friends who smoke, and living with a partner who smokes. Each Parts module includes interactive exercises (e.g. “Try this: Mindful Pause”) as well as a brief summary and final check-in questions at the end. The number of modules completed is shown visually through the “Track My Progress” feature.
Within Guided Mindfulness, participants can listen to mindfulness practice audio recordings (e.g. mindful breathing, stretching, body scan) anytime. Recordings include short, informal practices and use clear, relatable language. These include 1–3-minute mindfulness practices like STOP (Stop–Take a Breath–Observe–Proceed) and Surfing the Urge.
Within Nicotine Patches/Lozenges, participants learn about the purpose and appropriate use of nicotine patches and lozenges, including answers to common questions/concerns (e.g. “Why would I put more nicotine in my body if I want to quit smoking?”). They can request nicotine patches and lozenges through the app, which are mailed by the research team.
Within Tips, participants can push the following buttons for in-the-moment strategies/support: CRAVE (coping with cravings), STRESS (coping with stress), SLIP (getting back on track after lapses), FACT (effects of smoking and benefits of quitting), and QUOTES. Within QUOTES, participants can choose “Hear from former smokers” to see anonymous quotations from people who quit smoking using mindfulness in our past studies, or “Get inspired” for other motivation.
Participants receive personalized motivation and support via automated messaging through the app’s pop-up Notifications, which encourage mindfulness and other techniques taught in the app. Notification messages are personalized based on first names, reasons for quitting, and amount of money to be saved based on individual smoking habits and price paid per pack (e.g. “[FirstName], say to yourself “By not smoking, I am taking control: I have less risk of cancer/disease, I save [personalized amount] a year, I smell better, & I’m proud.” Notifications encourage various mindfulness practices with links to guided audio recordings. Participants can choose their notification frequency (between 1 and 5 messages per day), and the messages are pushed between their normal waking/bedtimes. Participants receive a brief weekly in-app survey that allows them to change the number and timing of notifications.
Considerations for adults with low SES who smoke
First, iQuit Mindfully 2.0 targets factors that impede cessation for adults with low SES, including high stress, craving and withdrawal, and low self-efficacy and social support (Businelle et al., 2010; Cambron et al., 2020; Hiscock et al., 2012). Although these factors have been related to smoking regardless of socioeconomic background, they are critical in explaining the association between low SES and lower likelihood of smoking cessation (Businelle et al., 2010). The app includes examples that may be relevant for adults with low SES (e.g. high-stress environments, living with others who smoke).
Second, iQuit Mindfully 2.0 provides just-in-time support through messaging that appears to be particularly effective among adults living in poverty (Spears et al., 2019a). Messages were designed through several studies soliciting input from adults with low SES (Spears et al., 2019b). Third, the app videos feature diverse speakers in terms of race and sex, increasing likelihood that participants will “connect” and find the speakers to be credible. Fourth, the videos and written content use easily understandable language that does not require high literacy, and the app’s simple design does not require high technical literacy. Participants downloaded the smartphone app during their enrollment session so they could access most aspects without internet. Finally, participants were able to request mailed nicotine patches and lozenges through the app for free, thus increasing NRT access.
Usability study: Methods
Participants
Recruitment focused on print and digital flyers; social media (e.g. Craigslist, Nextdoor); and community outreach to local organizations serving adults with low SES. Inclusion criteria were: age 18 or older; currently smoking at least three cigarettes per day (confirmed with expired carbon monoxide (CO) >6 ppm); motivated to quit within next 30 days; home address in greater Atlanta, GA; able to speak, read, and write in English; marginal/adequate health literacy (>45 on Rapid Estimate of Adult Literacy in Medicine (Davis et al., 1991); and either less than 200% of the federal poverty threshold (according to 2022 US Census Bureau Guidelines) or education below high school diploma/GED or equivalent. Exclusion criteria were: contraindication for nicotine patch or lozenge; active substance abuse/dependence (based on Patient Health Questionnaire (PHQ)-Alcohol (Spitzer et al., 1999) and Severity of Drug Dependence Scale (Gossop et al., 1995); current use of tobacco cessation medications; current pregnancy, planning to become pregnant in next 3 months, or lactation; current suicidal ideation (PHQ-9 suicide screening item (Rossom et al., 2017)); or another household member enrolled in the study.
Procedures
After telephone or online screening, interested individuals scheduled an in-person session to finalize eligibility and provide written informed consent. Those who were ineligible were provided referrals. Enrolled participants downloaded the iQuit Mindfully 2.0 app through the Insight™ platform. They were given the choice of using their own smartphone or borrowing an Android smartphone. Staff provided hands-on guidance in using the app and gave participants the opportunity to use it and ask questions. Participants used the iQuit Mindfully 2.0 app on their own for 2 weeks before the final in-person follow-up session where they completed questionnaires and an interview. This study was approved by the Georgia State University Institutional Review Board (#H20729).
Interventions
Participants received self-help materials for quitting smoking (NCI’s “Clearing the Air” booklet (U.S. Department of Health and Human Services, National Cancer Institute, 2008); Tobacco Quitline referral; and 8-week regimen of nicotine replacement therapy (NRT), in addition to the iQuit Mindfully 2.0 app. Participants were given an initial 2-week supply of patches and lozenges at baseline, and then the additional 6 weeks at the follow-up session so everyone received a full 8-week NRT regimen. During the 2-week study period, participants could request different flavors/dosages through the app.
Measures
Participants completed baseline measures of sociodemographic characteristics and smoking behaviors. At follow-up, participants were asked, “In the last 2 weeks, did you make a serious attempt to quit smoking? That is, did you stop smoking for at least one day or longer because you were trying to quit?”(PhenX Toolkit, n.d.), and reported the number of cigarettes they smoked per day over the past 7 days. They completed program evaluations in which they rated the following four items from 1 (completely disagree) to 5 (completely agree): “The app gave me confidence that I can quit smoking”; “The app made me think that it was worthwhile for me to quit”; “The app made me feel that someone cared if I quit”; and “The app made me feel that I knew the right steps to take to quit” (Hoeppner et al., 2017). They were asked to “select the number that best represents whether you would recommend the iQuit Mindfully app for others who are interested in quitting smoking,” from 1 (would not recommend) to 10 (would definitely recommend). Next, they engaged in an individual audio-recorded interview (approximately 1 hour) starting with the prompt, “Tell me about your experience with the app over the past 2 weeks” and then asked about what was helpful and not helpful, usability, experiences with each of the app features, technical difficulties, experience learning/practicing mindfulness, and suggestions for improvement. The final number of interviews (N = 16) was determined based on the principle of saturation (the point at which similar responses and insights emerge without substantial new information; Hennink and Kaiser, 2022).
Data analysis
Interviews were transcribed verbatim and coded using NVivo software. Coding and analysis involved both inductive and deductive approaches (Ayres et al., 2003; Ryan and Bernard, 2003). A preliminary set of codes was developed based on the moderator guide, and additional codes were identified based on concepts emerging from the data. Three trained research staff members independently coded the transcripts, with regular group meetings with the senior author to resolve inconsistencies and refine the coding scheme. Once coding was finalized in NVivo, the combined quotes for each code were downloaded and split among the team to write memos summarizing the key findings. Material for each code was summarized in writing independently by two team members, followed by group discussion to finalize results.
Results
Participant characteristics
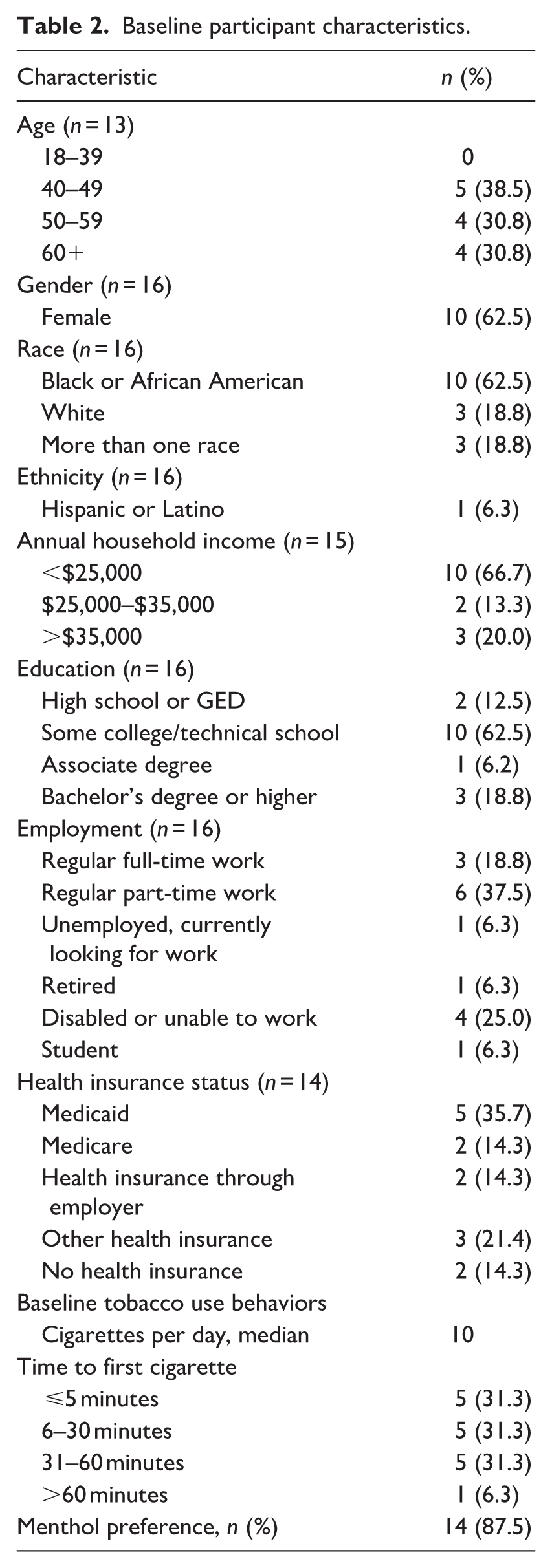
A total of 334 interested individuals completed telephone or online screening, and 154 were eligible. Of those, 102 scheduled an in-person eligibility appointment, 32 attended that appointment, and 16 enrolled. As shown in Table 2, participants (n = 16) were 63% female, 63% Black or African American, 54% aged 50 years or older, 12% having completed high school or GED, and 93% having an annual household income less than 200% of the federal poverty level.
Baseline participant characteristics.
Use of app features
Based on objective app data, 9 of 16 (56%) completed all eight Parts modules. Of those who did not complete all Parts, three people completed between 4 and 6 modules and four did 1–2 modules. All 16 participants used Guided Mindfulness, Nicotine Patches & Lozenges, Tips, and Track My Progress app features. Eleven of 16 (69%) completed the in-app weekly survey.
Quantitative results
On a 1–5 scale (1 = completely disagree, 5 = completely agree), 14 of 16 participants (2 missing) indicated the app gave them confidence to quit smoking (mean 4.4, SD 0.65), made them think it was worthwhile to quit (mean 4.6, SD 0.65), made them feel that someone cared if they quit (mean 4.5, SD 0.65), and made them feel they knew the right steps to take to quit (mean 4.4, SD 0.76). On a 1–10 scale of likelihood of recommending the app to others (1 = would not recommend, 10 = would definitely recommend), the mean rating among 12 of 16 participants (4 missing) was 9.2 (SD 1.4).
Although this pilot study was designed to gather feedback on the app and not powered to detect changes in smoking behavior, we report descriptive indicators of behavioral change. At the 2-week follow-up, 12 of 15 participants (80%; 1 missing) reported having made a serious attempt to quit smoking (i.e. stopped smoking for at least 1 day because they were trying to quit). At baseline, participants reported a median of 10 cigarettes per day (CPD; range 5–68, mean 15.2, SD 16.7). At follow-up, the median was 4 CPD (range 0–15, mean 5.6, SD 5.2). Among the 13 participants who reported CPD at both timepoints, 8 reduced, 1 remained unchanged, and 4 increased. All 8 who reduced did so by more than 50%: 2 reduced by 57%–67%, 4 by 78%–93%, and 2 reported complete cessation (100% reduction).
Qualitative results
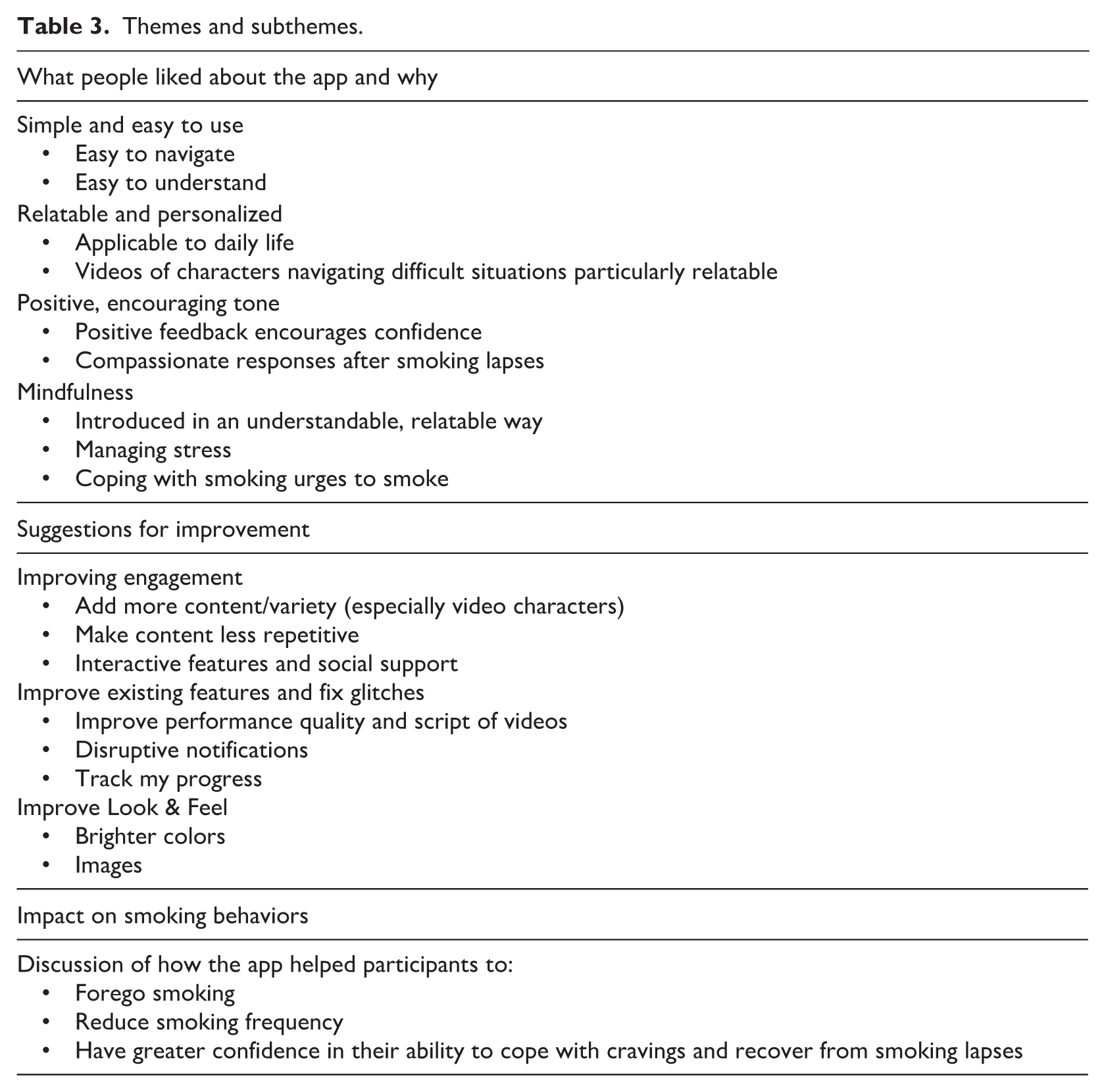
Qualitative results are described in three categories below, with quotes associated with pseudonyms: (1) what people liked about the app and why; (2) suggestions for improvement; and (3) impact on smoking behaviors. See Table 3.
Themes and subthemes.
What people liked and why
Participants provided positive feedback about the app (e.g. “The content is super useful. . . . I would recommend this app. I genuinely think it’s a great resource” [Brianna]). Key sub-themes were that it was simple and easy to use; relatable and personalized; had a positive, encouraging tone; and taught mindfulness for managing stress and smoking urges.
Simple and easy to use
Participants appreciated the ease of navigation and clear organization. One person said, “It wasn’t hard. It wasn’t complicated. That’s what I like most about it. There’s no difficulty. Anyone can use it. I like that.” (Kayla) Participants were able to get the information they needed through the app and described the “Tips” section as well organized and accessible. They appreciated being able to choose from a variety of “Tips” in the moment: “And because it’s not just like one tip. There’s the four, the craving, stress, slip, fact, quote. So you get a lot. You can pick what type of positive reinforcement you want.” (Brian)
Participants found the content easy to comprehend and appreciated the relatively simple, straightforward wording: I did like that it was short snippets of information on each screen. I like that because it doesn’t present you with a wall of text that you have to get through. . . Here are some manageable bullet points and when you have read and digested those, you can move on to the next thing. (Brianna)
Relatable and personalized
Participants said the app was personally relevant (e.g. “It matched my needs and preferences pretty well. I feel like it applied to me and touched on everything that I would need in my life, well in terms of quitting and coping with quitting” [Nicole]). People appreciated the relatable scenarios in the videos. They liked seeing examples of other people navigating difficult situations: It made me feel like, ‘Wow, there’s somebody going through this as well.’ It was very useful, especially in terms of where to start and the fact that all these hangups are not unique to me. Just feeling you’re not alone in this. . . was really, really reassuring. (Brianna)
Brittany explained: You truly feel this was their life situation, this really happened. She really quit and she really was trying to help him. . . I really put myself in his position like, wow, I’m not alone. . . . It’s gives you a visual, someone in your same situation. . . to see that you’re not alone. (Brittany)
The videos participants mentioned most often were those where the main character was interacting with friends and loved ones who also smoked but did not want to quit. For example: I like the situations that Mike was in. It seemed realistic and I could find myself in the situation. . . . It helped me with ideas of how to talk to family and friends, or when I’m in certain situations. . . . it gave me an idea of how I could come to [family member who smokes] and talk to her about it. (Nicole)
Positive, encouraging tone
Participants found the encouraging tone to be motivating (e.g. “gives you a little bit more strength and confidence to want to try to fight it and go through it,” Darius). Brian described, “I liked that because it was positive feedback, which, for somebody like me, I need a lot of that, especially for something like smoking.” Kayla explained the helpfulness of a compassionate response after a smoking lapse: Especially when you do slip, that part was extremely nice. I wasn’t expecting it to be so compassionate. . . . just keep going and just breathe throughout the whole thing. You were just being mindful of everything that you’re doing, how you’re feeling, this is your goal. Just stop for a moment and you got this.
Mindfulness
Many participants said the app exposed them to mindfulness for the first time and that mindfulness was introduced in an understandable, relatable way: The techniques for mindfulness and breathing, and mindful breathing and things like that, just meditation, are simple. People write entire books about how to do these things and make it way more complicated than it needs to be. So I like that it was simple. (David)
Kayla said, “[Mindfulness] changed my life. Definitely, just being aware.” Brittany explained, “Your app and your mindful breathing, who would’ve known that the way you think to breathe or just paying attention to your breathing could help you? I never would’ve known any of that if it wasn’t for the app.”
Participants commonly noted the benefits of mindfulness for managing stress: [Guided Mindfulness] makes you relax. It’s an immediate relaxation. . . You can do it any time of the day, there’s no, “I have to stand up,” or, “I have to be laying down.” You can do it anytime or anywhere. (Kayla)
They gave examples of practicing mindfulness to manage smoking urges: It’s helped me. . . to not react and grab a cigarette. Now I can just pause, take a minute, breathe. Breathing helps to relax me and have some awareness of what is really going on, opposed to just going and doing and reacting and all that. Just to sit and meditate. (Lauren)
Darius described using the mindful urge surfing he learned from watching “Mike” in the videos: I would just be so mad. I would just go grab a cigarette right now. . . . And then I thought about Mike riding the waves [of cravings]. I said, “You know what, I’m going to ride this wave today. I’m not going back.”
Suggestions for improvement
Participants’ suggestions involved improving three categories: engagement, existing app features/glitches, and the look and feel of the app.
Improving engagement
Participants suggested adding more content and variety; reducing repetition; and adding more interactive features. When asked if they would be interested in using this app for more than 2 weeks, all answered affirmatively, though some said more content is needed for longer-term use. The most common suggestion was to add more videos with varied characters and situations (e.g. “You could probably use different people, different age groups” [Nicole], “some more characters you could put in there” [Brandon]).
A few participants wished that app content was tailored to reflect various stages of quitting smoking (e.g. preparing to quit, on their quit date, maintaining abstinence after quitting). This was especially true among those who successfully quit or were close to it. To them, the app seemed like it would be less useful after they quit (e.g. “If I’m successful, I probably wouldn’t be using it that much,” Brian; “Well I’ve seen the videos and been through the parts, and gained a basic understanding of what’s there, so I feel like I’ve experienced it,” David).
Some participants said the content felt repetitive. Brittany explained, “The same information I had to keep reading, it just kind of felt like you’re in school and you don’t want to be in the class with the teacher because she keeps saying the same thing over again.” Participants suggested more varied messages in both the “notifications” and “tips” features.
Several said the app should be more interactive, such as adding games (e.g. “Just something to get that serotonin going. . .. video-gamify it. Just make it more fun to push buttons, I guess,” Brianna; “I just think more like interaction games,” Emily). Some wanted peer support features, such as: It would be great if they had a chatline where you could have a community of people that’s trying to quit smoking, they could maybe get together maybe on a Zoom or something. . . where you could just kind of encourage each other. (Darius)
Improve existing features and fix glitches
Participants suggested improving the performance quality and scripts of the videos; making notifications less disruptive; and fixing glitches. Although participants liked the videos overall, some said they seemed scripted or the actors did not seem like “real smokers.” Emily said “[the videos] just seemed fake to me,” and Brian said, “It might seem like they’re hired actors, and so it’s hard for me to identify them as real people.”
Several participants indicated issues with the notifications, including that they were disruptive, made the app crash, or made using other applications on their phones difficult. Brianna disliked “the fact that [clicking the notification] opens the app and cancels out everything that I’m doing on my phone” and said they were “not a fan of the loud notification. If it was a pleasant “Ding,” that’d be cute, but I keep my phone on vibrate most of the time. So it’s just like, “Blarrrr!”
When asked what they disliked, several participants mentioned the “Track My Progress” feature. Due to limited programming capabilities and technical glitches, participants could not tell what milestones were being recorded. Participants suggested that the app ask participants about their smoking behavior daily to track their progress and provide encouraging responses. Brittany suggested adding visual tracking of lapses: I thought there was going to be a way for me to put in a day or time that I had a slip, and I actually would’ve liked that. I only had two slips, but I can only imagine if I had more, it would’ve been nice to have a visual, to see a trend as to when I had a slip.
Improve look and feel
Participants suggested adding brighter colors and images, saying “Just the colors for me, make it more inviting” (Lauren) and “The color. Bring the colors out better. But the architecture, it came out real good though, designing and stuff. It’s designed real good.” (Brandon)
Impact on smoking behavior
Several participants reported smoking less over the 2-week period of using the app (e.g. “It helped me not to smoke; If I’m doing this, then my mind is not on cigarettes,” Ashley). They attributed successful smoking reduction to mindfulness practices and other strategies to manage smoking urges, as well as greater motivation, confidence, and accountability. Marcus described: They gave me the tools, man. They gave me good tips on how to cope with craving. . . . They was preparing me for what I could use in case of I had an urge to smoke. . . . I smoked a lot less, so it did work a lot. The breathing exercise what worked for me.
Jasmine explained, “It helped with the cravings and the desire to smoke.” Kayla described gaining greater confidence and hope from the videos and quotes: It did it with quotes for inspiration, saying the other former quitters. It gave you confidence, it gave you hope. If you did slip, it’s okay, especially that video, the way you spoke about it, and don’t give yourself up and just wait. It’s okay. It’s one step at a time.
Darius described using “Call Quit Coach” to connect to the Tobacco Quitline: I had a real strong urge to smoke. And instead of doing that, and even though I had the patch, I still wanted to smoke, but I didn’t. And what I did was there was a button on the app that said call our quit coach.
David explained that the accountability and feeling of accomplishment were key to his success, which felt different from their prior quit attempts: In the past, I would’ve gone back and forth and woke up, smoked two cigarettes and then put the patch on. [This time] I just didn’t go to the store. . . . The accountability, the reminder. It gives a little feeling of accomplishments, each day when you do another part and you still haven’t smoked. It’s like, okay, all right. Now I’m on day four. I’m on day five. . . . it gets a little easier each day. It’s like, okay, I just don’t smoke.
Discussion
This study supports the acceptability and feasibility of iQuit Mindfully 2.0, a mindfulness-based smoking cessation app designed to address common barriers to smoking cessation among adults with low SES. Participants appreciated the personalization, relatability, and simplicity of the app as well as the daily encouraging messages and tips. They perceived that learning and practicing mindfulness was beneficial for managing stress and coping with smoking urges. Participants commonly explained that the app helped them to reduce their smoking and build confidence in their ability to cope with cravings and get back on track after smoking lapses. Suggestions for improvement included adding features to track progress; enhancing visual esthetics; minimizing repetitiveness; and fixing technical glitches. These improvements were incorporated into the refined app for future trials and may also inform other digital health interventions for adults with low SES.
Extant studies have shown benefits of smoking cessation apps that teach mindfulness. Experience sampling data from an RCT of the Craving to Quit app showed that although there were no between-group differences in abstinence rates, mindfulness training via Craving to Quit weakened the association between craving and smoking (Garrison et al., 2020). Smart Quit 2.0, an app rooted in ACT, which promotes mindful acceptance of cravings without smoking, has produced strong quit rates (e.g. 21% 7-day point prevalence abstinence at 2-month follow-up; Bricker et al., 2017). However, these study samples were majority non-Latino White and had more than a high school level education (Bricker et al., 2017; Garrison et al., 2020). The iQuit Mindfully 2.0 app is unique as a mindfulness-based smoking cessation app designed for adults with low SES. Improving accessible smoking cessation services for this population is critical (U.S. National Cancer Institute, 2017). Adults with low SES and racially/ethnically minoritized groups have been underrepresented in MBI research (Waldron et al., 2018), which limits our ability to understand the effects of MBIs in diverse groups and identify tailoring strategies for underserved communities.
Results are promising because participants with low SES found the app content relatable and enjoyed applying mindfulness to manage cravings and cope with stress. Several participants appreciated the relatable scenarios portrayed in the videos. Videos that resonated particularly well were those in which the main character navigated conflicts with friends and loved ones who smoked. Indeed, given the higher smoking prevalence in low-SES communities, quitting can be difficult when people perceive that many people around them smoke, which can trigger smoking urges and lessen social support for quitting. The iQuit Mindfully 2.0 videos share strategies for avoiding smoking at home and social activities when others who smoke are nearby, regardless of whether those individuals wanted to quit.
Our qualitative results align with several findings from a recent review of users’ experiences with smoking cessation apps, although that review did not focus on mindfulness (Zhang et al., 2023). Participants across studies of various smoking cessation apps appreciated ease of use in addition to learning strategies to cope with unpleasant emotions and cravings, receiving motivational reminder messages and engaging with diverse content (e.g. video, audio, text; Zhang et al., 2023). Consistent with our findings, app users wanted interactive features and ability to track their smoking behavior.
This study provides suggestions for improving the iQuit Mindfully 2.0 app, including making the app’s tracking of smoking behavior more effective, improving the look and feel of the app, fixing glitches, and adding more content and variety including video characters of different ages. Participants highlighted the need for more interactive features such as games and peer support. These are important suggestions given the high rates of drop-out and non-adherence with mHealth apps (Baumel et al., 2019; Meyerowitz-Katz et al., 2020). Indeed, social and gamification features have been associated with higher mHealth app engagement (Jakob et al., 2022). Such features could be useful for improving engagement with iQuit Mindfully, particularly given that just over half of participants completed all eight Parts modules. Future studies with larger samples could examine how many modules need to be completed for a meaningful dose of the intervention. Examining the measurement of dose and response for digital smoking cessation interventions is an area of inquiry that deserves empirical attention (Ichimiya et al., 2022). All participants in our short pilot expressed interest in using the app for a longer period of time. Some suggested tailoring content to different stages of quitting. Although the app was designed for people who are motivated to quit, future iterations could be tailored to different stages of change including for those who are not yet ready to quit, as has been done with another smoking cessation app that did not involve mindfulness (Businelle et al., 2024a).
This usability study is limited by a small sample size and short timeframe as part of our iterative efforts to refine the app. The study lacked statistical power to examine quantitative changes and did not include a control group. Once the app is refined based on user feedback, a larger randomized trial with longer-term follow-up is needed to examine participants’ experiences over time and effects on smoking behavior, compared to other apps as well as non-digital interventions. Nevertheless, this study is strengthened by a focus on adults with low SES, who experience severe tobacco-related disparities, have lower access to smoking cessation treatment, and have been underrepresented in mindfulness research. Participants provided in-depth feedback that can be used to improve the iQuit Mindfully 2.0 app and perhaps other related mHealth apps for adults with low SES. Tailoring evidence-based mHealth apps that are accessible and meet the needs of lower-SES populations is critical for targeting health disparities.
Footnotes
Acknowledgements
The authors wish to acknowledge the contributions of the participants who shared their personal experiences and perspectives, which are invaluable for improving the iQuit Mindfully app.
Ethical considerations
This study was approved by the Georgia State University Institutional Review Board (#H20729).
Consent to participate
All participants provided written informed consent prior to enrollment in the study.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
CAS, DWW, MPE, MJH, and DEK conceived and designed the study. KCH coordinated and collected data. MMM, KCH, SA, TK, and CAS conducted data analysis. MMM and CAS drafted the manuscript. All authors reviewed and edited the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute on Drug Abuse (R34 DA049208, PI Dr. Claire Spears). The mHealth Shared Resource at the OUHSC and NCI-designated Stephenson Cancer Center developed the Insight™ mHealth platform (co-invented by Dr. Kendzor and Dr. Businelle and partially supported by grant #P30CA225520), through which the iQuit Mindfully 2.0 app was programmed. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Darla Kendzor and Dr. Michael Businelle are co-inventors of the mobile health platform (INSIGHT). They receive royalties when investigators outside of the University of Oklahoma (their home institution) use the INSIGHT platform. However, this monetary benefit is based on use of the platform and is not based on specific study outcomes. The other authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Data availability statement
Due to the sensitive nature of qualitative interview data, full transcripts are not publicly available but can be accessed from the corresponding author upon reasonable request.