
Abstract
Insomnia is linked to absenteeism, reduced productivity, and diminished job satisfaction. This study aimed to evaluate the comparative efficacy of different components of Cognitive Behavioral Therapy for Insomnia (CBT-I) on work productivity. PubMed, Cochrane Library, Web of Science Core Collection, MEDLINE, APA PsycINFO, APA PsycArticles, Embase, Wan Fang, and CNKI were searched from inception to October 8, 2024. Evidence quality was assessed using the GRADE approach. Seven randomized controlled trials involving 4751 participants were included. Moderate-quality evidence indicated that Full CBT-I significantly improved absenteeism and presenteeism; whereas evidence for work productivity loss and activity impairment was of low quality. For Sleep Restriction Therapy (SRT), low-quality evidence supported its efficacy for presenteeism, work productivity loss, and activity impairment, whereas evidence for its effect on absenteeism was very low. SRT combined with sleep hygiene education may serve as an efficient first-step intervention for work productivity, whereas Full CBT-I offers broader efficacy.
Keywords
Introduction
Insomnia is the most prevalent sleep disorder worldwide, affecting up to 50% of primary care patients (Perlis et al., 2022). According to the International Classification of Sleep Disorders, Third Edition (ICSD-3), insomnia is characterized by persistent difficulty initiating or maintaining sleep despite adequate opportunity and circumstances for sleep, accompanied by clinically significant daytime impairments (Riemann et al., 2023). The Three-Factor (3P) model provides a framework for understanding how acute sleep disturbance evolves into chronic insomnia, positing that predisposing traits (e.g. emotional reactivity), precipitating events (e.g. occupational stress), and – critically – perpetuating factors (e.g. conditioned arousal and dysfunctional sleep cognitions) interact to sustain the disorder and exacerbate daytime dysfunction (Spielman et al., 1987). This places a significant strain on individuals’ physical and mental well-being and adversely impacts their work performance (Baglioni et al., 2020; Kucharczyk et al., 2012), which is recognized as the second most impaired functional domain among individuals with insomnia (Kucharczyk et al., 2012).
In the workplace, the consequences of insomnia manifest primarily through two pathways: time lost from work and diminished effectiveness while at work. To capture these dimensions, work productivity is operationalized in occupational health research as a multidimensional construct comprising absenteeism (work time missed due to health-related issues) and presenteeism (reduced on-the-job performance or productivity while physically present despite experiencing health problems; Cancelliere et al., 2011). This is relevant to insomnia research, as the disorder’s daytime symptoms – including fatigue, reduced motivation, impaired concentration, and executive dysfunction – undermine an individual’s capacity to sustain optimal work performance, thereby translating sleep disturbance into measurable productivity loss (Fortier-Brochu et al., 2012; Swanson et al., 2011).
Studies have consistently reported that insomnia imposes significant economic costs on society and individuals due to absenteeism, reduced productivity, increased medical costs, and heightened utilization of healthcare services (Hillman et al., 2018; Uehli et al., 2014; Wickwire et al., 2016). Notably, the indirect costs related to lost productivity comprised the largest proportion – approximately 76.2% – of the total economic burden of insomnia (Daley et al., 2009a). Given this disproportionate impact, interventions that effectively target work productivity impairment among individuals with insomnia hold considerable clinical and economic significance, offering potential benefits not only for affected employees in terms of improved time management, work-life balance, and reduced workplace stress, but also for employers and healthcare systems seeking to mitigate productivity-related losses.
International guidelines recommend Cognitive Behavioral Therapy for Insomnia (CBT-I) as the first-line treatment for adults with insomnia (Riemann et al., 2023), which directly targets the perpetuating factors identified in the 3P model: Sleep Restriction Therapy (SRT) enhances homeostatic sleep drive; Stimulus Control Therapy (SCT) extinguishes conditioned bedroom arousal; and Cognitive Therapy (CT) restructures maladaptive sleep beliefs that maintain pre-sleep anxiety (Benz et al., 2020). Previous studies indicate CBT-I’s efficacy in working populations and its potential to reduce presenteeism (Reynolds et al., 2023; Takano et al., 2021, 2023). The Stepped Care Model (SCM) further highlights the need to identify the differential effectiveness of CBT-I components to optimize treatment costs (Baglioni et al., 2023). However, evidence regarding CBT-I’s impact on work productivity remains fragmented and has not been systematically synthesized.
Therefore, this study systematically evaluates all available Randomized Clinical Trials (RCTs) to compare the effectiveness of different CBT-I components in improving work productivity among individuals with insomnia. The findings will inform evidence-based decisions, ultimately reducing both the clinical burden of insomnia and productivity-related economic costs.
Methods
Study design and registration
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA) (Moher et al., 2009) and utilized data from previously published studies. The review protocol was prospectively registered with the International Prospective Register of Systematic Reviews (CRD42024591257).
Selection criteria
We formulated the following inclusion and exclusion criteria:
Population
Adults (⩾18 years) diagnosed with insomnia (First, 2013; Riemann et al., 2023; Sateia, 2014) based on Diagnostic and Statistical Manual of Mental Disorders (DSM), ICSD, International Classification of Diseases, or equivalent criteria for insomnia symptoms as measured by validated questionnaires with scores exceeding clinical cutoffs. Studies targeting shift workers were excluded.
Intervention
Included RCTs were required to feature at least one of the following components: SRT, SCT, CT, Relaxation Therapy (RT), and Sleep Hygiene Education (SHE). Combinations of these components were permitted. Studies combining CBT-I with other interventions (e.g. bright light therapy) was excluded.
For clarity and to facilitate interpretation of heterogeneity, the included components were operationally defined as follows: SRT – prescribed restriction of time in bed to approximate total sleep time, with weekly adjustment based on sleep efficiency; SCT – standardized behavioral instructions (e.g. go to bed only when sleepy, leave bed if unable to sleep, maintain consistent wake time); CT – structured identification and restructuring of maladaptive sleep-related beliefs; RT – formal training in techniques to reduce pre-sleep arousal; SHE – general recommendations regarding lifestyle and environmental factors conducive to sleep (Walker et al., 2022).
Comparator
Control conditions included SHE, Waiting List (WL), or Treatment as Usual (TAU).
Outcome
Work productivity measured by instruments including the Work Productivity and Activity Impairment (WPAI), Work Limitations Questionnaire (WLQ), Health and Work Performance Questionnaire, Valuation of Lost Productivity Questionnaire, or Institute for Medical Technology Assessment’s Productivity Cost Questionnaire (IPCQ; Peiyu Zhou, 2022). Different dimensions of the aforementioned scale, such as absenteeism, presenteeism, work productivity loss, and activity impairment, will be reported in the results.
Study type
Only RCTs were included (Schulz et al., 2010). Conference proceedings, case reports, reviews, meta-analyses, and studies with significant baseline imbalances were excluded.
Search strategy
A systematic literature search was conducted in PubMed, Cochrane Library, Web of Science Core Collection, MEDLINE, EBSCO (PsycINFO, PsycArticles), Embase, Wan Fang, and CNKI from inception to October 8, 2024. The search combined titles, abstracts, and keywords terms for core concepts (e.g. “sleep initiation and maintenance disorders,” “cognitive behavioral therapy”), with “efficiency”-related terms searched across all fields. The full search strategy for each database is provided in Table S1. Reference lists of included studies and relevant reviews were manually screened.
Two authors (NSY and ZYP) independently screened titles and abstracts, followed by full-text review against eligibility criteria. Discrepancies were resolved through consensus or by consulting a third reviewer (WJL). Authors were contacted for clarification when necessary. The selection process was documented per PRISMA guidelines.
Data extraction and management
Two reviewers (NSY and LZP) independently extracted data using a standardized form, including first author, participant characteristics, intervention components, productivity outcomes, and available employment and clinical data. Discrepancies were resolved through discussion or consultation with a third reviewer (ZH).
Quality evaluation and risk of bias assessment
Methodological quality was assessed using the Physiotherapy Evidence Database (PEDro) scale (Cashin and McAuley, 2020). This scale comprises 11 items covering internal validity and statistical reporting (item 1 does not contribute to the total score). A score above 6 indicates high-quality study, and less than 6 reflect greater potential for biases to affect the results of the trial (Cashin and McAuley, 2020).
Risk of bias was evaluated using the Cochrane Risk of Bias Tool version 2 (RoB 2; Puljak et al., 2020), assessing the following domains: randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selection of reported results. Each domain and the overall bias were rated as “low,” “some concerns,” or “high” (Hróbjartsson et al., 2013).
Two authors assessed the quality and risk of bias independently (NSY and ZYP). Discrepancies in assessments were resolved by consensus or consultation with a third researcher (ZP).
Quality of evidence
The quality of evidence for each outcome (absenteeism, presenteeism, work productivity loss, and activity impairment) was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) tool (Guyatt et al., 2011). Evidence quality was rated as high, moderate, low, or very low per GRADE guidelines (Brozek et al., 2009).
Data analysis
All analyses were conducted using STATA 17. Meta-analyses employed the Der Simonian and Laird random-effects model (Borenstein et al., 2010), with effect sizes calculated as Weighted Mean Difference (WMD) or Standardized Mean Difference (SMD) with 95% Confidence Intervals (CI), depending on outcome measures. Heterogeneity was assessed using the I2 statistic, with I2 > 50% and p-value < 0.1 indicating substantial heterogeneity. Under this condition, a random-effects model was used (Higgins et al., 2003). Subgroup analyses were performed by intervention components. Sensitivity analysis used the Jackknife method, and publication bias was assessed via funnel plots. Where quantitative synthesis was not feasible, findings were summarized narratively.
Results
Study screening and selection process
The initial search identified 2579 records. After removing 924 duplicates, 46 full-text articles were assessed for eligibility. Seven studies (Espie et al., 2019; Kalmbach et al., 2019; Kjørstad et al., 2022; Kyle et al., 2023; Okajima et al., 2020; Shaffer et al., 2021; Thiart et al., 2015) met the inclusion criteria, of which two (Kjørstad et al., 2022; Thiart et al., 2015) provided only follow-up data. The selection process is summarized in the PRISMA flowchart (Figure 1).
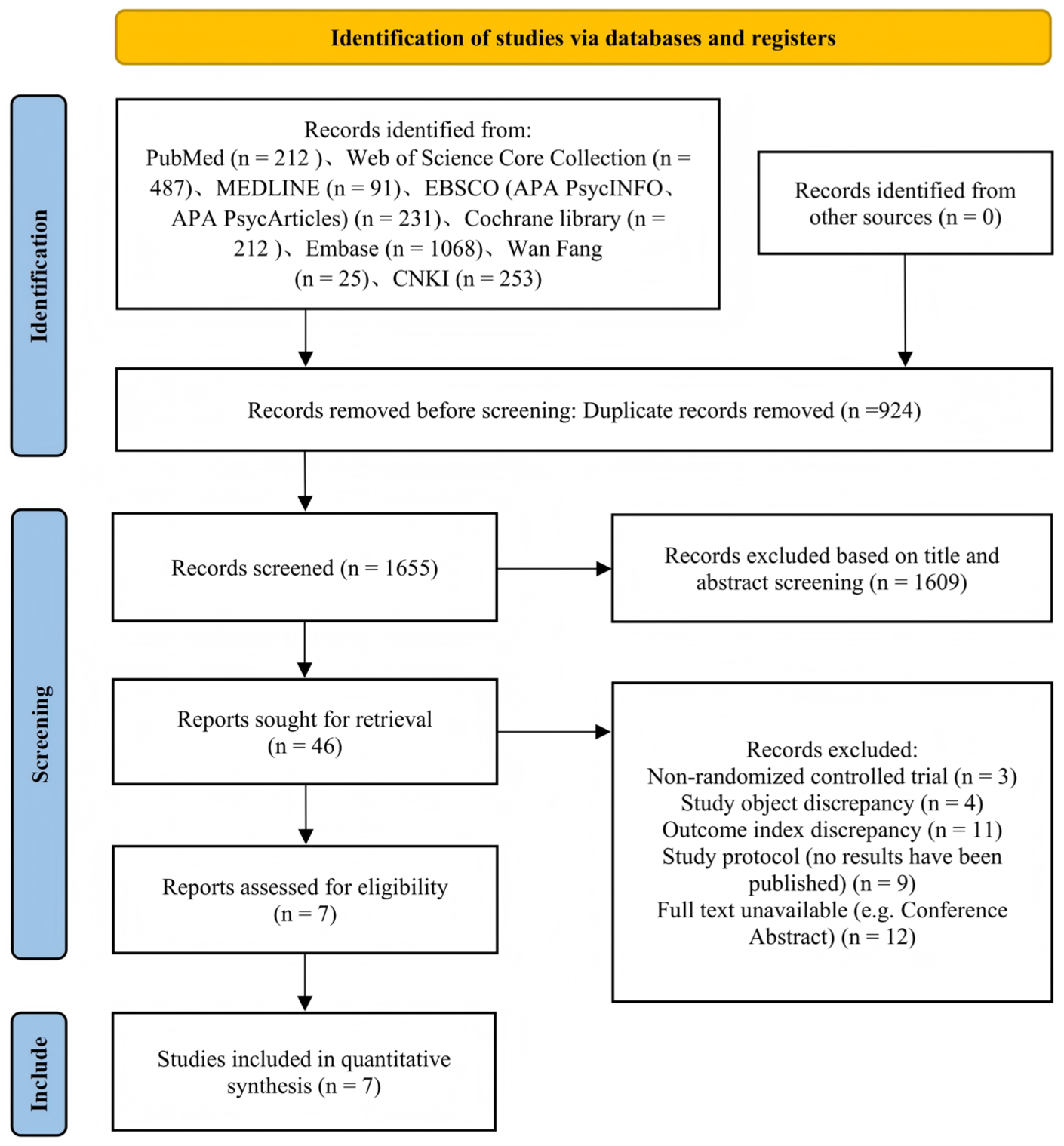
PRISMA flow diagram.
Characteristics of included studies
The seven included RCTs (Table 1) defined insomnia using DSM-5 criteria or the Insomnia Severity Index. The total sample comprised 4751 participants (Experimental Group (EG) = 2408, Control Group (CG) = 2343). Five studies employed digital CBT-I (dCBT-I; Espie et al., 2019; Kjørstad et al., 2022; Okajima et al., 2020; Shaffer et al., 2021; Thiart et al., 2015), including Behavioral Therapy for Insomnia (BBT-I; Combination of behavioral component and SHE; Okajima et al., 2020) and Full CBT-I (Interventions with at least one cognitive component, one behavioral component, and SHE; Espie et al., 2019; Kjørstad et al., 2022; Shaffer et al., 2021; Thiart et al., 2015). Two studies employed non-digital interventions: individual SRT (Kalmbach et al., 2019; Kyle et al., 2023) and individual Full CBT-I (Kalmbach et al., 2019). Outcome measures included the WPAI in five studies (Espie et al., 2019; Kalmbach et al., 2019; Kjørstad et al., 2022; Kyle et al., 2023; Shaffer et al., 2021), the WLQ in one study (Okajima et al., 2020), and the IPCQ in one study (Thiart et al., 2015).
Main characteristics of the included studies.
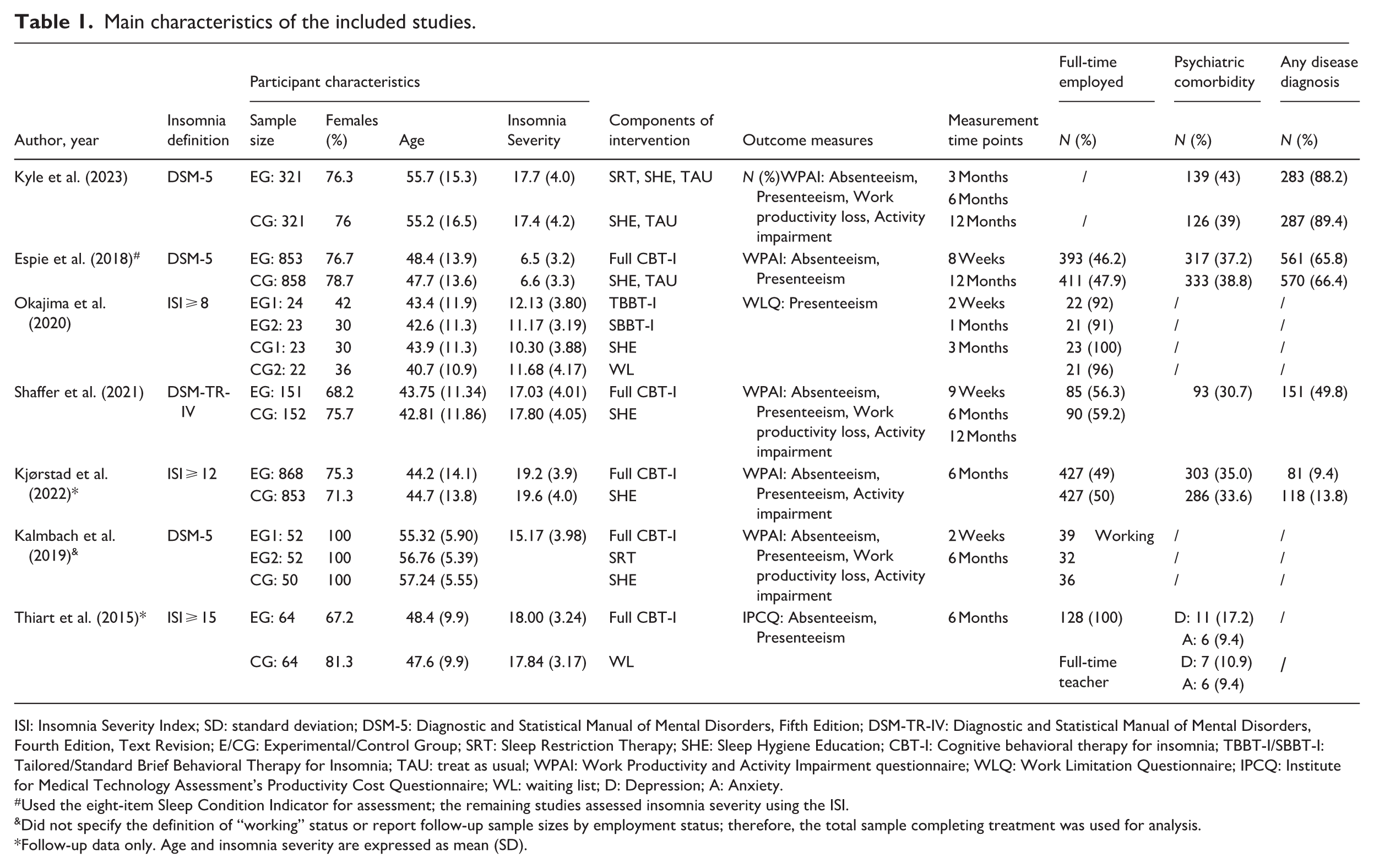
ISI: Insomnia Severity Index; SD: standard deviation; DSM-5: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; DSM-TR-IV: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision; E/CG: Experimental/Control Group; SRT: Sleep Restriction Therapy; SHE: Sleep Hygiene Education; CBT-I: Cognitive behavioral therapy for insomnia; TBBT-I/SBBT-I: Tailored/Standard Brief Behavioral Therapy for Insomnia; TAU: treat as usual; WPAI: Work Productivity and Activity Impairment questionnaire; WLQ: Work Limitation Questionnaire; IPCQ: Institute for Medical Technology Assessment’s Productivity Cost Questionnaire; WL: waiting list; D: Depression; A: Anxiety.
Used the eight-item Sleep Condition Indicator for assessment; the remaining studies assessed insomnia severity using the ISI.
Did not specify the definition of “working” status or report follow-up sample sizes by employment status; therefore, the total sample completing treatment was used for analysis.
Follow-up data only. Age and insomnia severity are expressed as mean (SD).
Employment status was reported in five trials (Espie et al., 2019; Kjørstad et al., 2022; Okajima et al., 2020; Shaffer et al., 2021; Thiart et al., 2015), with total full-time employment ranging from 47% to 100% and part-time from 3.5% to 20.3%. Occupation type was reported in two trials (teachers (Thiart et al., 2015) and office workers/Specialist (Okajima et al., 2020)). Psychiatric comorbidities were reported in five trials (total range: 9.4%–41.3%; Espie et al., 2019; Kjørstad et al., 2022; Kyle et al., 2023; Shaffer et al., 2021; Thiart et al., 2015). Any disease diagnosis was documented in four trials (range 11.6%–88.8%; Espie et al., 2019; Kjørstad et al., 2022; Kyle et al., 2023; Shaffer et al., 2021).
Quality and risk of bias assessment
PEDro scores of the studies ranged from 6 to 8 (mean = 6.86), indicating overall high quality. The most common limitations were insufficient blinding and inadequate follow-up (Table S2).
RoB2 revealed the following: one studies had some concerns and one had high risk for the randomization domain; four had some concerns and three had high risk for deviations from intended interventions; three had high risk for missing outcome datal and two had high risk for outcome measurement and selective reporting, respectively. Overall, six studies (Espie et al., 2019; Kalmbach et al., 2019; Kjørstad et al., 2022; Okajima et al., 2020; Shaffer et al., 2021; Thiart et al., 2015) were rated as high risk of bias (Figure 2 and S1).
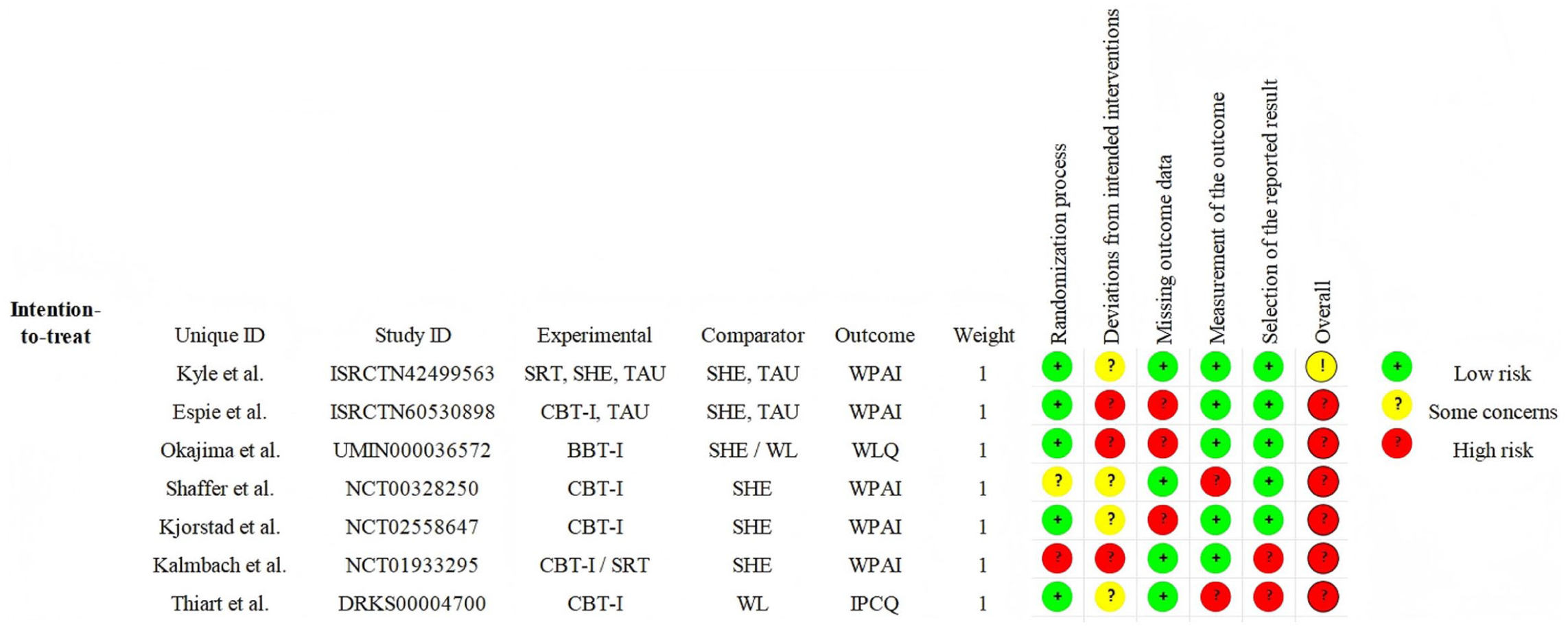
Risk of bias graph.
GRADE assessment indicated moderate-quality evidence for CBT-I in reducing absenteeism and presenteeism, but low-quality evidence for work productivity loss and activity impairment. For SRT, evidence was low quality for presenteeism, work productivity loss, and activity impairment, and very low for absenteeism. Evidence for BBT-I on presenteeism was very low (Table S3).
Effect on work productivity
Absenteeism
Six studies (Espie et al., 2019; Kalmbach et al., 2019; Kjørstad et al., 2022; Kyle et al., 2023; Shaffer et al., 2021; Thiart et al., 2015) assessed absenteeism using WPAI or IPCQ. Pooled analysis showed no statistically significant difference between groups WMD = −3.09, 95% CI: −6.73 to 0.54, I2 = 93.8%, p < 0.001; five studies, 1594 participants; Figure 3). Subgroup analysis indicated a significant effect for Full CBT-I, but not for SRT. Sensitivity analysis identified one study (Kyle et al., 2023) as the primary source of heterogeneity; its removal eliminated heterogeneity without altering the overall conclusion. No significant effect was observed at 6-month follow-up.
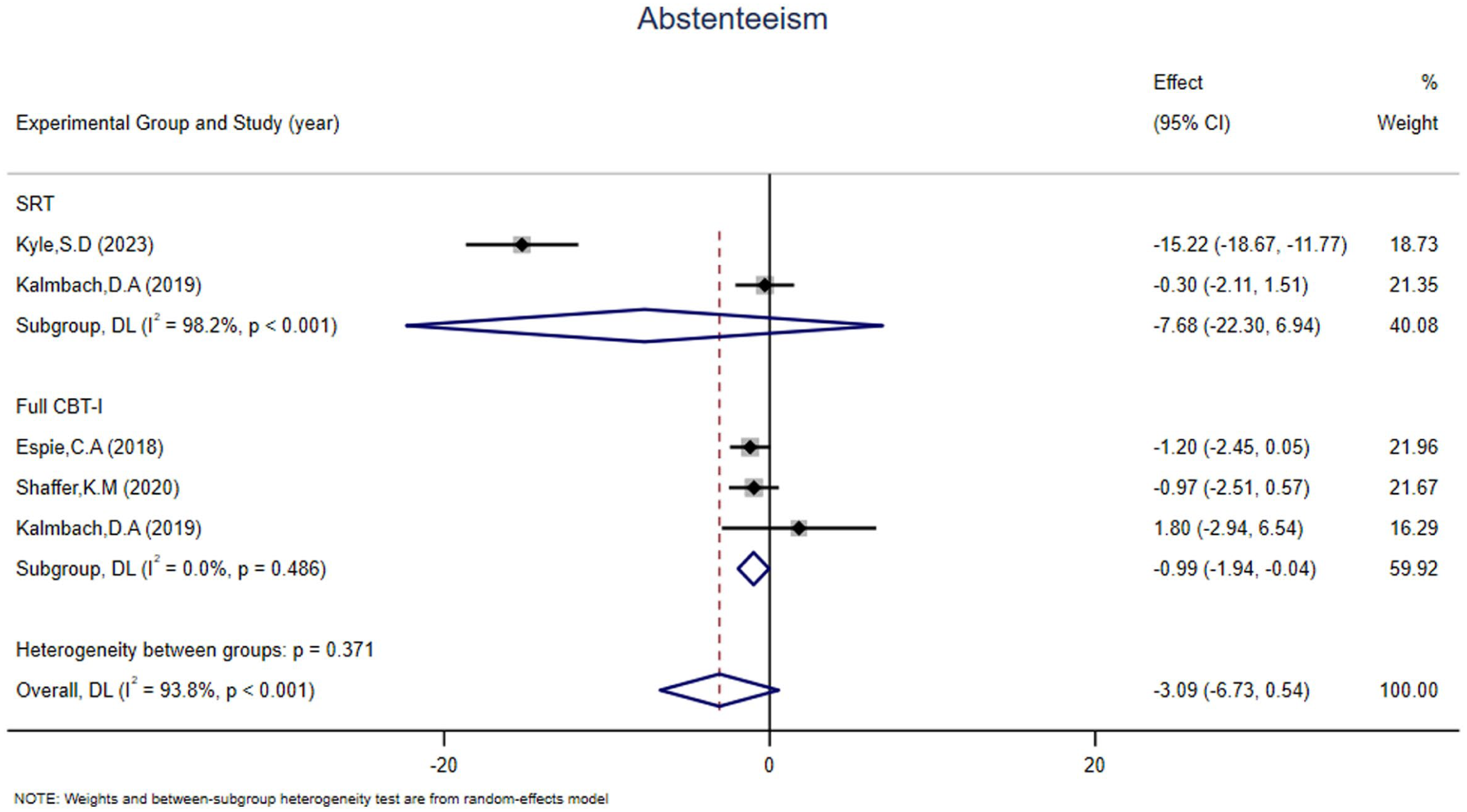
Forest plots of SRT and Full CBT-I (absenteeism).
Presenteeism
All seven studies (Espie et al., 2019; Kalmbach et al., 2019; Kjørstad et al., 2022; Kyle et al., 2023; Okajima et al., 2020; Shaffer et al., 2021; Thiart et al., 2015) assessed presenteeism using WPAI, WLQ, or IPCQ. The overall effect size was SMD = −0.41 (95% CI: −0.51 to −0.31, I2 = 0.0%, p = 0.868; nine comparisons, 1667 participants; Figure 4). Subgroup analysis showed a pooled SMD of −0.42 when the CG is SHE plus TAU or SHE. Both SRT and Full CBT-I demonstrated significant effects on presenteeism, except for BBT-I. Sensitivity analysis revealed no small-study effect, and funnel plots showed no evidence of publication bias. The effect remained significant at 6-month follow-up but not at 12 months.
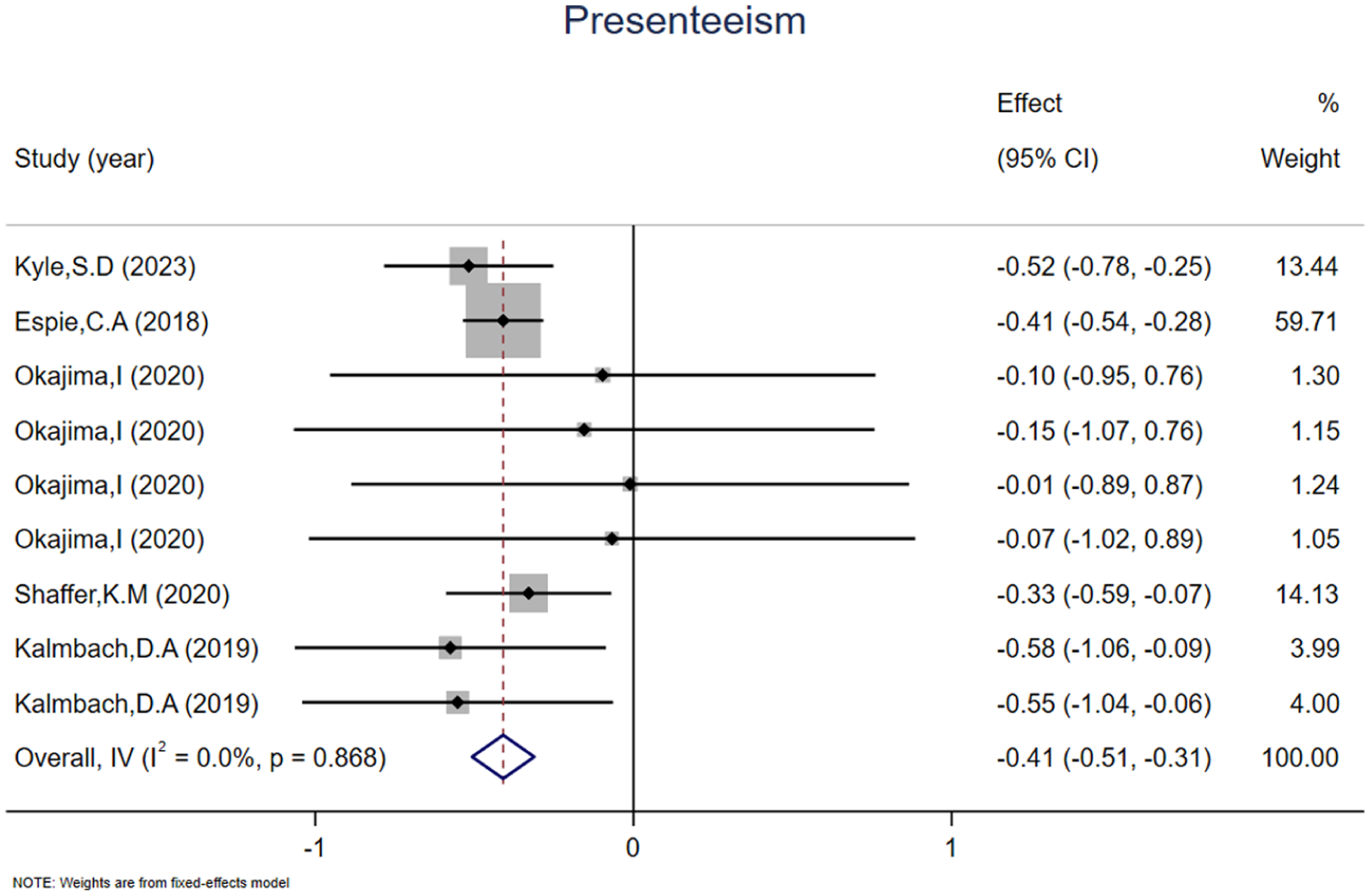
Forest plots of overall effects (presenteeism).
Work productivity loss
Four studies (Kalmbach et al., 2019; Kyle et al., 2023; Shaffer et al., 2021) assessed work productivity loss using WPAI. Both SRT and Full CBT-I significantly reduced work productivity loss (WMD = −10.03, 95% CI: −13.78 to −6.27, I2 = 0.0%, p = 0.727; four studies, 605 participants; Figure 5). No small-study effect or publication bias was detected. The improvement persisted at 6-month follow-up but was no longer significant at 12 months.
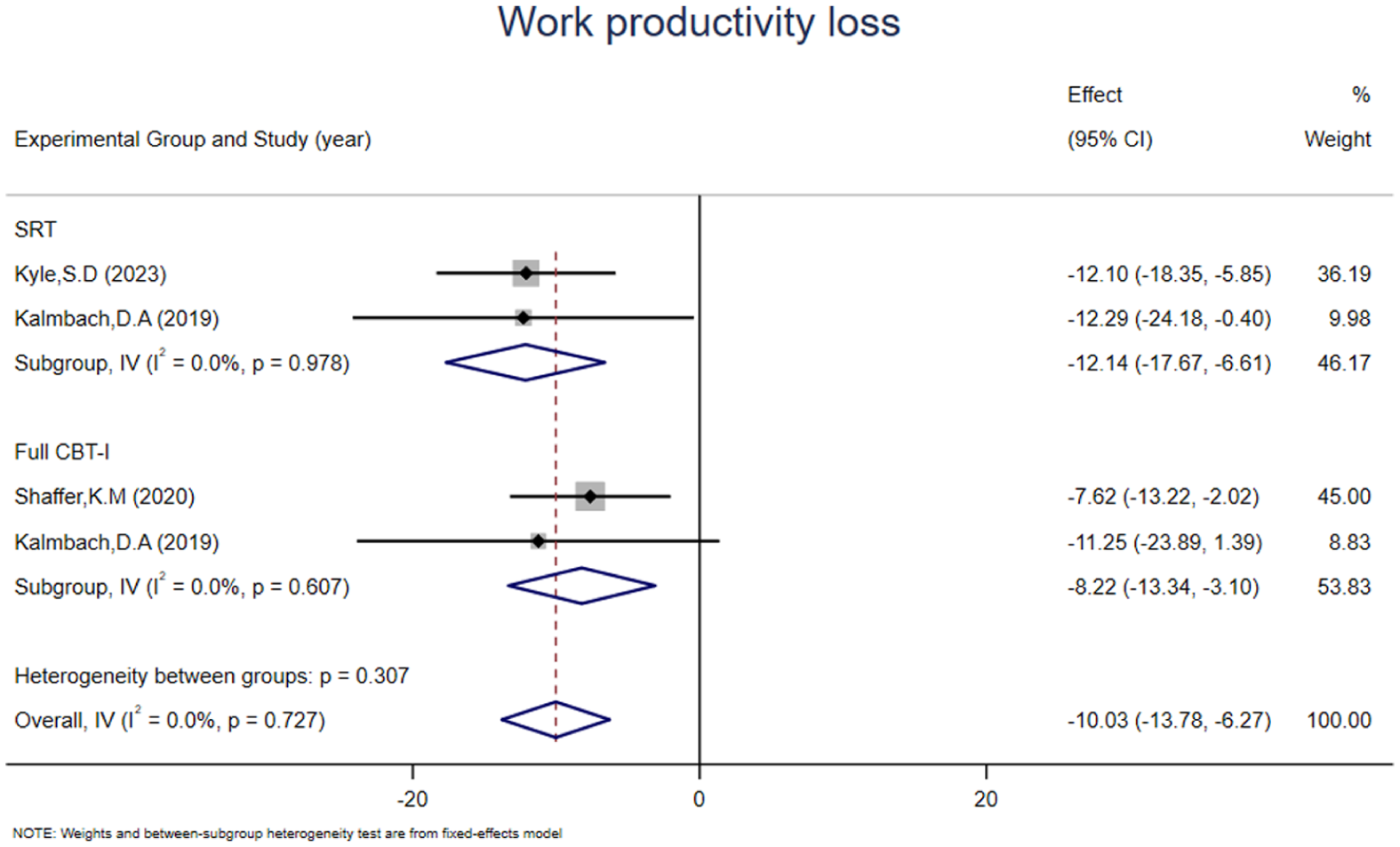
Forest plots of SRT and Full CBT-I (work productivity loss).
Activity impairment
Four studies (Kalmbach et al., 2019; Kyle et al., 2023; Shaffer et al., 2021) assessed activity impairment using WPAI. SRT and Full CBT-I significantly reduced activity impairment (WMD = −11.30, 95% CI: −14.45 to −8.14, I2 = 0.0%, p = 0.457; four studies, 957 participants; Figure 6). No small-study effect or publication bias was detected. Benefits were maintained at 6-month follow-up but not at 12 months.
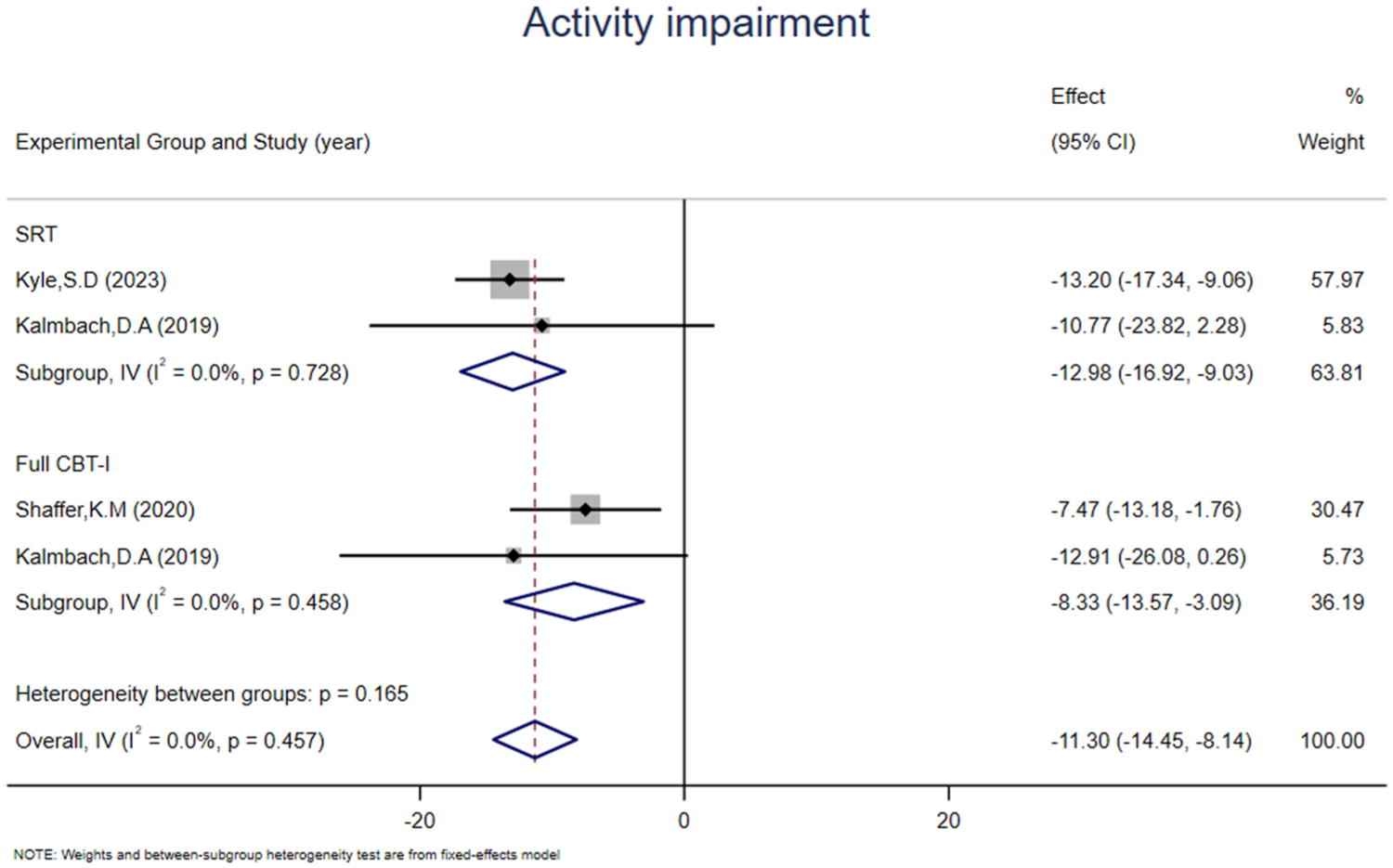
Forest plots of SRT and Full CBT-I (activity impairment).
Attrition rate and adverse events
Of 2408 participants assigned to the EG, 1635 completed post-treatment assessment (attrition: 32.1%). In the CG, 1623 of 2343 participants completed assessment (attrition: 30.7%). Adverse events reported in studies are used to assess the potential hazards of treatments. Reported in five studies, with nine adverse events in EG (eight from SRT) and eight in the CG (Espie et al., 2019; Kjørstad et al., 2022; Kyle et al., 2023; Okajima et al., 2020; Shaffer et al., 2021).
Discussion
Recent meta-analyses have confirmed CBT-I yields benefits beyond sleep, including improvements in daytime symptoms (Benz et al., 2020) and quality of life (Alimoradi et al., 2022). To our knowledge, however, this is the first meta-analysis to specifically examine the impact of different CBT-I components on work productivity. Our findings support the efficacy of both SRT and Full CBT-I in reducing presenteeism, work productivity loss, and activity impairment, with effects maintained at 6-month follow-up. For absenteeism, only Full CBT-I showed significant benefit. Notably, despite variation in study designs and potential biases, most studies demonstrated consistent intervention effects with overall high quality and low heterogeneity. This pattern suggests that adherence to treatment instructions, rather than the specific format or delivery mode, may largely drive observed improvements (Maurer et al., 2021).
Absenteeism
Evidence consistently links insomnia to elevated absenteeism (Espie et al., 2018), with affected individuals demonstrating over twice the absenteeism rate of good sleepers and markedly greater sleep-related work hour loss (Daley et al., 2009b). Our findings suggest that Full CBT-I, but not SRT, significantly reduces absenteeism. One possible explanation is that Full CBT-I addresses the broader cognitive and behavioral array maintaining insomnia-related functional impairment (Nakao et al., 2021; Takano et al., 2023) – including catastrophic worry about sleep and maladaptive coping behaviors (Harvey, 2002) – which may be necessary to alter persistent patterns of work absence. In contrast, SRT primarily targets sleep consolidation and may be insufficient to overcome the complex barriers to workplace attendance. These findings align with recent evidence suggesting that multifaceted interventions combining individual therapy with workplace adjustments are more effective in reducing sick leave than single-component approaches (Shiri et al., 2025).
Presenteeism
Presenteeism, though less visible than absenteeism, accounts for the majority of insomnia-related productivity losses, representing 66%–84% of total performance cost reductions across industries (Hemp, 2004; Mazzetti et al., 2019; Stewart et al., 2003). Our analyses indicate that both SRT and Full CBT-I yield significant and sustained reductions in presenteeism, with effects maintained at 6-month follow-up. The non-significant finding for BBT-I likely reflects the limited number of trials and small sample sizes rather than true inefficacy. Notably, a recent meta-analysis of dCBT-I trials similarly reported positive effects on presenteeism and work-related outcomes (Zettor et al., 2025). These results underscore the potential of both single-component and multicomponent CBT-I as practical workplace interventions.
Work productivity loss and activity impairment
Both SRT and Full CBT-I demonstrated significant efficacy in reducing work productivity loss and activity impairment, with benefits sustained at 6-month follow-up. Previous studies have established the effectiveness of these interventions in alleviating insomnia symptoms (Maurer et al., 2021; Mitchell et al., 2019; van Straten et al., 2018), and our findings extend this evidence to occupational outcomes. From a neurobiological perspective, insomnia is associated with chronic inflammation and oxidative stress (Palagini et al., 2022), which can impair neuronal function (Davinelli et al., 2024; Zhao et al., 2024). CBT-I may restore normative brain activity patterns, thereby optimizing cognitive processes essential for work performance (Marques et al., 2020; Miller et al., 2021; Sabot and Baumann, 2023).
Attrition rate and adverse events
Attrition rates were substantial in both the EG (32.1%) and CG (30.7%). Most studies (five of seven) employed digital delivery, which may limit timely feedback and therapist-participant interaction (Andersson and Titov, 2014), potentially reducing engagement (Blanchard and Markus, 2004; Christensen et al., 2009). Non-adherence to intervention schedules may also have contributed to dropout (Duan and Bu, 2019). Future research should prioritize strategies to enhance treatment adherence, including fostering motivation, self-efficacy, and positive treatment expectations (Matthews et al., 2013), and providing consistent feedback throughout treatment (Hebert et al., 2010). In two studies reporting adverse reactions, SRT was associated with more adverse effects than Full CBT-I and posed implementation challenges. To mitigate these issues, future applications of SRT should adopt a personalized, gradual approach (Garbarino and Bragazzi, 2024; Kyle et al., 2015) integrated with SHE. Specifically, SHE addresses behavioral and environmental barriers to adherence, establishing a supportive foundation for SRT implementation (De Pasquale et al., 2024; Matthews et al., 2012). This combined approach may enhance the acceptability of SRT while minimizing adverse effects.
Mechanisms underlying improvements in work productivity
An important question is whether the observed benefits of CBT-I components on work productivity are driven exclusively by sleep improvement, or whether other factors – such as enhanced mood, reduced daytime fatigue, or increased self-efficacy – play meaningful mediating roles. Prior research has demonstrated that CBT-I produces reliable improvements in depressive symptoms and fatigue (Ballesio et al., 2018; Xu et al., 2021), both of which are plausible contributors to occupational outcomes. Emerging evidence further suggests that CBT-I may enhance work productivity through the alleviation of both insomnia symptoms and daytime fatigue (Kieley et al., 2020; Kjørstad et al., 2022). However, the trials included in the present review did not consistently measure these potential mediators, precluding formal mediation analyses. Future trials should incorporate systematic assessments of hypothesized mediators to elucidate the pathways linking insomnia treatment to occupational outcomes.
Implications for stepped care
The differential effects observed across CBT-I components align well with the SCM, which advocates delivering the least resource-intensive intervention likely to confer benefit before escalating to more comprehensive treatments (Baglioni et al., 2023). Within this framework, SRT combined with SHE may serve as an efficient first-step option for addressing presenteeism and productivity loss in occupational settings, particularly when access to specialized therapists is limited. For absenteeism, which in our analyses responded significantly only to Full CBT-I, a comprehensive approach may be warranted. This stepped approach is especially relevant for workplace health programs, where accessibility and cost-effectiveness are important considerations. Notably, the ease of implementation of these interventions is further enhanced by digital delivery formats: recent evidence indicates that dCBT-I yields meaningful improvements in productivity, with estimated annual savings exceeding $12,000 per employee (Russell et al., 2026), underscoring the practicality of integrating such approaches into occupational health services.
Limitations
This review has several limitations. First, subgroups analysis by delivery format and control condition were unfeasible due to the limited number of included studies. Second, Second, none of the included trials were rated as having a low risk of bias, likely reflecting the inherent difficulty of blinding participants in CBT-I trials (Kjørstad et al., 2022). Finally, inconsistent reporting of demographic, occupational, and clinical characteristics across trials limited examination of potential moderators of treatment effects. Future studies should prioritize standardized collection of these data to enable more comprehensive moderator analyses.
Conclusion
Both Full CBT-I and SRT are effective in improving work productivity among individuals with insomnia, with benefits sustained at medium-term follow-up. Full CBT-I demonstrated efficacy across all productivity outcomes, whereas SRT was effective for presenteeism, work productivity loss, and activity impairment. These findings support the integration of CBT-I into workplace health programs, with SRT combined with SHE offering a resource-efficient first-step option and Full CBT-I reserved for cases requiring broader therapeutic coverage. Further large-scale RCTs are needed to confirm the differential effects of specific CBT-I components on work productivity and to clarify the mechanisms linking insomnia treatment to occupational outcomes.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261461928 – Supplemental material for Comparative efficacy of different components of cognitive behavioral therapy for insomnia on work productivity: A systematic review and meta-analysis
Supplemental material, sj-docx-1-hpq-10.1177_13591053261461928 for Comparative efficacy of different components of cognitive behavioral therapy for insomnia on work productivity: A systematic review and meta-analysis by Shuyi Nie, Yiping Zhao, Jialin Wang, Zhoupeng Lu, Hui Zou and Peng Zhao in Journal of Health Psychology
Footnotes
Acknowledgements
We confirm that every individual listed as an author has contributed to this work in accordance with the ICMJE guidelines and is prepared to take public responsibility for its content. We extend our sincere gratitude to Dr. Peng Zhao for his guidance and to our families and friends for their full support throughout this work.
Ethical considerations
Ethical approval was not required for this study as it is a systematic review and meta-analysis, which synthesizes data exclusively from previously published studies and does not involve direct human participant recruitment or intervention. All original studies included in this analysis have presumably obtained their own ethical approvals and participant consents in accordance with standard publishing guidelines and the Declaration of Helsinki.
Consent to participate
Consent to participate is not applicable to this review article as no data were collected from participants.
Consent for publication
Consent for publication is not applicable to this review article as no identifiable participant data are included.
Author contributions
Shuyi Nie and Yiping Zhao are the principal authors of this study, with full access to all research data and responsibility for the accuracy and integrity of the data analysis. Peng Zhao contributed to the conceptualization and study design. Shuyi Nie, Yiping Zhao, and Jialin Wang contributed to the article search and initial screening process. Shuyi Nie, Yiping Zhao, Zhoupeng Lu, and Hui Zou contributed to data collection and interpretation. Shuyi Nie and Yiping Zhao drafted the initial manuscript, conducted revisions, and provided final approval. All authors have reviewed and approved the final manuscript and meet the ICMJE criteria for authorship.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the 2025 Special Research Project on Sports for Persons with Disabilities (Project Number: 2025KFJS&003). The funder had no role in the study design, data collection, analysis, interpretation, or writing of this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data and materials supporting the findings of this systematic review and meta-analysis are available upon reasonable request. Researchers interested in accessing the data should contact the author, Shuyi Nie, at 17871635733@163.com.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.