
Abstract
Social support, especially from healthcare workers, arises as an anxiety potential relieving factor for people living with HIV (PLWH). This study explored how different types and sources of social support are associated with anxiety among HIV-infected inpatients in Vietnam. A cross-sectional study was conducted in 392 PLWH, approached through convenience sampling, at Nhan Ai hospital in Vietnam, using a questionnaire that included the Generalized Anxiety Disorder 7-item (GAD-7) scale and the Medical Outcomes Study Social Support Survey (MOS-SSS). Anxiety prevalence was 27.04%. Tangible support (OR = 0.91; 95% CI: 0.85–0.97; p = 0.005) and positive social interaction (OR = 0.91; 95% CI: 0.85–0.98; p = 0.011) were significantly associated with a lower likelihood of anxiety. Participants receiving support from both friends and healthcare workers showed the strongest association with lower odds of anxiety (OR = 0.07, 95% CI: 0.02–0.23, p < 0.001). This study suggests an inverse association between social support and anxiety among PLWH, especially in inpatients with limited family support.
Introduction
Compared with the general population, PLWH face a higher risk of experiencing mental health issues, which negatively affects their access to and adherence to antiretroviral treatment (ART) as well as their prognosis (Collins et al., 2021; Nguyen et al., 2021). Anxiety disorder is among the most common mental health conditions in PLWH (Hu et al., 2025). The estimated anxiety prevalence among PLWH was 29%, significantly higher than the general population (4.05%; Hu et al., 2025; Javaid et al., 2023). A variety of factors influence anxiety in PLWH. Sociodemographic characteristics, including gender, age, marital status, economic status, education, and substance use, are associated with anxiety (Ahmed et al., 2021; Beer et al., 2019; Camara et al., 2020; Mannes et al., 2021). HIV clinical staging and opportunistic infections are among the clinical factors related to anxiety (Tesfaw et al., 2016; Yousuf et al., 2020).
Within the stress–coping framework (Biggs et al., 2017), anxiety among people living with HIV can be conceptualized as a psychological response to chronic illness-related stressors and disease progression. HIV represents not only a medical condition but also an ongoing source of stress requiring continuous cognitive and emotional adjustment. From this perspective, stress arises not solely from the illness itself but from individuals’ cognitive appraisal of its demands and their perceived resources to cope. Consistent with the buffering hypothesis (Cohen and Wills, 1985), social support may attenuate the psychological impact of these stressors by shaping primary and secondary appraisals, enhancing perceived control, reducing internalized stigma (Ahmed et al., 2021; Liu et al., 2013; Scardera et al., 2020), and facilitating adaptive emotional regulation. In institutional contexts such as long-term hospitalization, the salience and availability of specific support sources may further influence how stress is appraised and managed, thereby being associated with variations in anxiety levels.
Among PLWH, a low level of social support has been associated with higher levels of anxiety (Ahmed et al., 2021). Higher social support is correlated with lower levels of anxiety, with psychological resilience serving as an important mediating role (Liu et al., 2013; Sun et al., 2023). Family support, in particular, has shown a strong association with lower anxiety and has been associated with lower psychological burden in PLWH (Sun et al., 2023). In a cultural context such as Vietnam, where familial cohesion is highly valued, the family often serves as the principal source of support. However, in long-term inpatient settings, daily interactions with healthcare workers and fellow patients may make these sources of support more psychologically salient than family support due to prolonged separation from the broader social environment and sustained contact with fellow patients and healthcare workers. In these settings, daily interactions with healthcare workers and fellow patients may become especially influential. Support from friends has been recognized as an important source of social support and has been associated with better mental quality of life in HIV patients during treatment (Lifson et al., 2017). Although healthcare workers may significantly influence patients’ mental well-being and treatment adherence, few studies have explored their role as a source of social support for hospitalized PLWH. Similarly, supportive engagement with healthcare workers may shape patients’ sense of trust and perceived control in treatment processes (Schneider et al., 2004). Despite these plausible mechanisms, limited research has examined healthcare workers as a distinct source of perceived social support among hospitalized PLWH.
However, in Vietnam, while most current evidences focus on outpatients (Matsumoto et al., 2017; Nguyen et al., 2025; Thai et al., 2025), the role of social support in promoting the mental health of HIV-positive inpatients remains poorly understood. Notably, while the roles of family and friends have been widely studied (Oppong Asante, 2012; Seffren et al., 2018), the specific impact of healthcare workers as a source of social support—and its impact on anxiety among hospitalized HIV patients—remains underexplored.
Against this background, the present study was conducted to examine the prevalence of anxiety and its association with social support among PLWH, focusing on inpatients and the unique role of healthcare professionals. The cross-sectional survey was conducted at Nhan Ai hospital in Vietnam that provides comprehensive HIV/AIDS care, including treatment for advanced cases, long-term inpatient care and support, and hospital- and community-based activities. The study aimed to identify patterns of social support among inpatient PLWH in Vietnam.
Methods
Research design
This is a cross-sectional study conducted at Nhan Ai hospital. The hospital, located on a mountainside, is the largest hospital providing inpatient care for socioeconomically disadvantaged PLWH in Vietnam, including those living in poverty, without health insurance or identification documents, experiencing homelessness, lacking family support, or with a history of drug use. Patients are treated in separate wards that are physically isolated from one another; only patients and healthcare workers are permitted to reside long-term in these wards, and family visitation is restricted. Due to these circumstances, most patients reside in the hospital for long-term care and treatment, to a much greater extent than in other healthcare settings, and remain relatively isolated from the outside world. The hospital offers specialized HIV/AIDS support and treatment programs, greenery space, and hospital- and community-based support activities. Annually, patients in the hospital also receive support and supplements from a variety of organizations.
Given the hospital’s limited inpatient capacity and the specific characteristics of patients treated at Nhan Ai hospital, a convenience sampling approach was used to recruit 392 PLWH receiving inpatient care from March to April 2025. Once the visit is complete, patients are provided with a clear explanation of the study’s aims. Patients who agree to participate will be further guided to fill out a consent form before beginning a face-to-face interview. Trained interviewers administered the structured, pre-designed Vietnamese language questionnaire. The interviews were conducted in a private setting, with each lasting approximately 20–30 minutes. Based on a pre-designed questionnaire, the participants were asked to provide information on their social background and experiences with social support, anxiety symptoms, and social support activities. Data collected was supplemented by relevant clinical information extracted from patients’ medical records.
This study included PLWH receiving inpatient treatment in Nhan Ai hospital, who were aged at least 18 years old, willing to consent to our study, and capable of participating in a face-to-face interview. Individuals who did not complete the full questionnaire were excluded from the analysis.
Measurements
Anxiety
Anxiety was evaluated with the Generalized Anxiety Disorder 7-item (GAD-7) scale. The questionnaire consists of seven items on anxiety symptoms over the previous 2 weeks, each scored on a 4-point Likert scale, rated from 0 (“not at all”) to 3 (“nearly every day”), with a combined total score ranging from 0 to 21. Scores were categorized as no anxiety (0–4), mild (5–9), moderate (10–14), and severe (15–21; Spitzer et al., 2006). Although a lower statistically optimal cut-off (⩾3) has been reported in a Vietnamese validation study (Mughal et al., 2021), we defined anxiety as a GAD-7 score ⩾5 to align with the established severity thresholds of the instrument and to enhance clinical interpretability and consistent with prior HIV-related studies in the world as well as in Vietnam assessing anxiety burden(Johnson et al., 2025; Nguyen et al., 2022; Nyongesa et al., 2020; Phan et al., 2025). GAD-7 is a reliable measure of anxiety symptoms (Löwe et al., 2008), and the Vietnamese version used in this study showed good internal consistency (Cronbach’s alpha = 0.91; Mughal et al., 2021).
Social support
Types of social support were measured using the Medical Outcomes Study Social Support Survey (MOS-SSS). This self-administered instrument comprises 19 items and assesses four distinct dimensions: tangible support (4 items), emotional/informational support (8 items), affectionate support (3 items), and positive social interaction (4 items). Each item was evaluated on a 5-point Likert scale, ranging from 1 (“none of the time”) to 5 (“all of the time”). The Vietnamese version of the MOS-SSS has been validated and demonstrated good internal consistency (Cronbach’s alpha = 0.97; Khuong et al., 2018; Sherbourne and Stewart, 1991). Subscale scores were used for descriptive and analytical purposes.
Additional questions on sources of social support were appended to the MOS-SSS. Based on prior research and the characteristics of long-term inpatients, sources were measured as a multiple-response nominal variable and categorized into family, friends, healthcare workers, and others (Harrison et al., 2023; Oppong Asante, 2012). Given the hospital context and patient population, “friends” primarily referred to other PLWH receiving treatment in the same ward. Each social support source was reported descriptively, whereas analyses were performed according to the combinations of sources received by participants.
Demographics, social, and HIV-related factors
Demographic variables included gender and sex (⩽25, 26–50, >50 years). HIV-related variables comprised duration since HIV diagnosis and ART initiation (⩽5 and >5 years), opportunistic infections (pulmonary tuberculosis, extrapulmonary tuberculosis, others), WHO clinical stage (I–II, III, IV), substance use history (illicit drugs, tobacco, alcohol, antidepressants/anxiolytics), disclosure status, and chronic comorbidities, assessed dichotomously where applicable.
Social factors included residence, marital status, educational attainment, financial support, duration of hospitalization, patient visitation, participation in support activities, physical activity, and sexual orientation. Residence was classified as Ho Chi Minh City or other provinces. Marital status was categorized as married, not married, and others (including divorced or widowed). Educational attainment was grouped as no formal education, primary (1–5 years), lower secondary (6–9 years), higher secondary (10–12 years), vocational training, and college/university or higher (⩾13 years). Financial support was dichotomized as ⩽500,000 VND or >500,000 VND. Duration of hospitalization (months) and participation in support activities (number of events in the past year or since admission) were treated as continuous variables. Patient visitation was assessed by whether patients were visited in the past month and the average monthly frequency. Physical activity was categorized as <150, 150–300, or >300 minutes per week. Sexual orientation was classified as heterosexual, homosexual, or other.
Data analysis
The prevalence of anxiety (GAD-7 ⩾5) was examined by types of social support, sources, and their combinations, as well as other variables. Logistic regression analysis was performed to investigate the associations between anxiety and social support.
Univariate logistic regression was conducted to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for each type of social support as well as demographic, social, and HIV-related variables. Multivariate logistic regression was then performed using a stepwise approach, with all four types of social support entered a priori and variables with p < 0.20 included as potential confounders. Variables with p < 0.05 were retained. In a separate analysis, combinations of support sources received by participants were incorporated into the model alongside the four types of social support.
Analyses were conducted in RStudio (version 2025.05.1). Two-sided tests with p < 0.05 were considered statistically significant. Model fit was assessed using the Hosmer–Lemeshow test. No problematic multicollinearity was observed in either analysis (mean VIF = 2.49 and 3.13, respectively), although slightly higher VIFs were noted for age groups (5.59 and 5.57) and two combined source categories (5.65 and 5.42), remaining within acceptable limits.
Ethics approval
The study was approved by an institutional ethics committee of the University of Health Sciences, Vietnam National University Ho Chi Minh City, Vietnam. Ethical clearance was also obtained from Nhan Ai hospital in January 2025. All participants provided informed consent to participate in this study.
Results
Table 1 presents the socio-demographic characteristics and HIV-related factors of 392 PLWH surveyed. Participants were predominantly male (88.52%), and most were in the 26–50 age group (82.40%). Most participants resided in HCMC (83.93%); about two-thirds received financial support exceeding 500,000 VND (33.42%). Regarding educational attainment, 90% had at least a primary school level. Only 18.11% of participants were married. In terms of sexual orientation, 75.77% identified as heterosexual. Median duration of hospitalization was 9 months (IQR 4, 13), and 37.50% received patient visitation. Most participants spent less than 150 minutes per week on physical activities. The median participation in support activities was 3 times (IQR 1, 5). Among the participants, the median duration since HIV diagnosis was 11 years (IQR = 6, 16.5), with 75.77% having been diagnosed for more than 5 years. Mean durations since ART initiation were 10 years (IQR 5, 14). Opportunistic infections were reported in 10.71% of patients, and pulmonary tuberculosis in 8.16%. Overall, 96.17% of participants reported a history of substance use, mainly illicit drugs (84.18%), tobacco (57.40%), alcohol (38.27%), and antidepressant/anxiolytic (13.27%). Moreover, 89.54% were at WHO HIV clinical stage I and II. Nearly half of the patients (46.43%) had at least one chronic comorbidity, and 83.67% of patients reported disclosing their HIV status.
Socio-demographics and HIV-related factors.
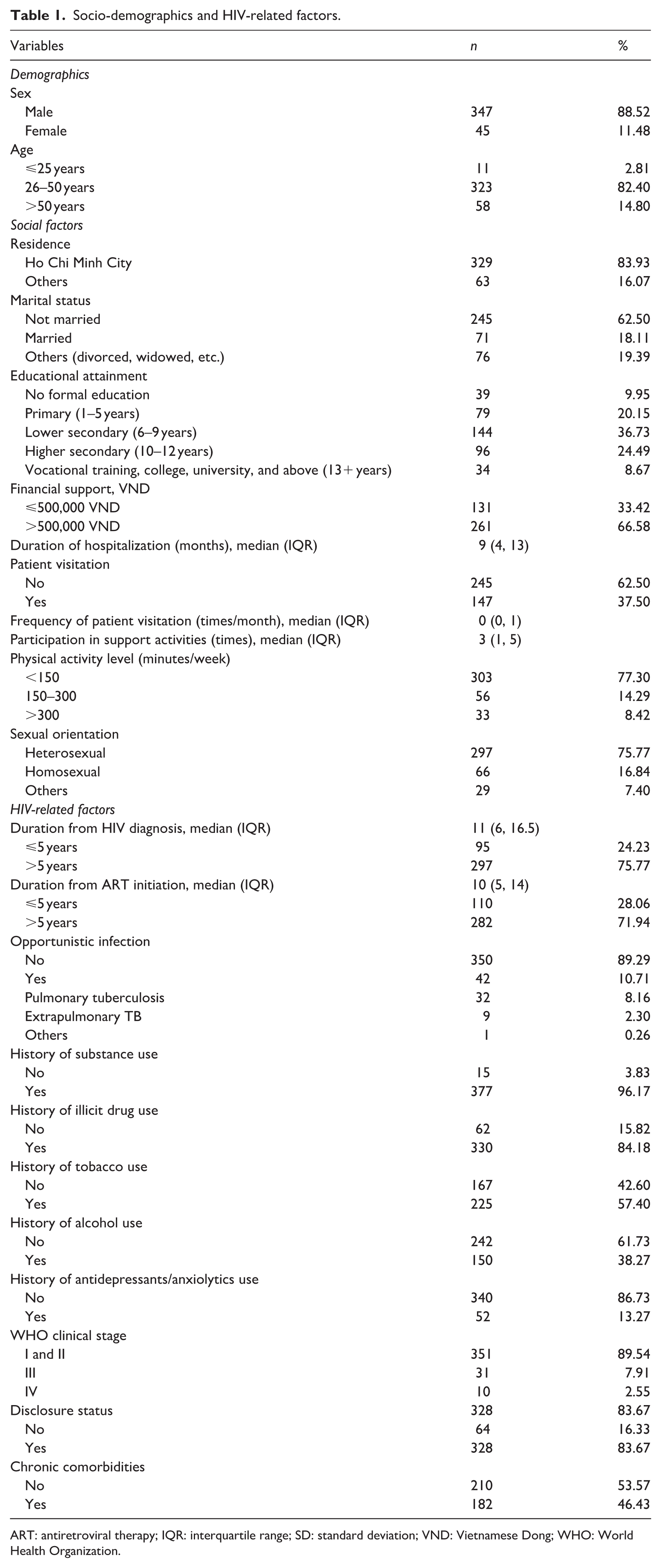
ART: antiretroviral therapy; IQR: interquartile range; SD: standard deviation; VND: Vietnamese Dong; WHO: World Health Organization.
Figure 1 shows the prevalence of the participants. In general, 27.04% of the participants had anxiety. Mild anxiety was reported by 17.09% of respondents, followed by moderate (6.38%) and severe anxiety (3.57%).
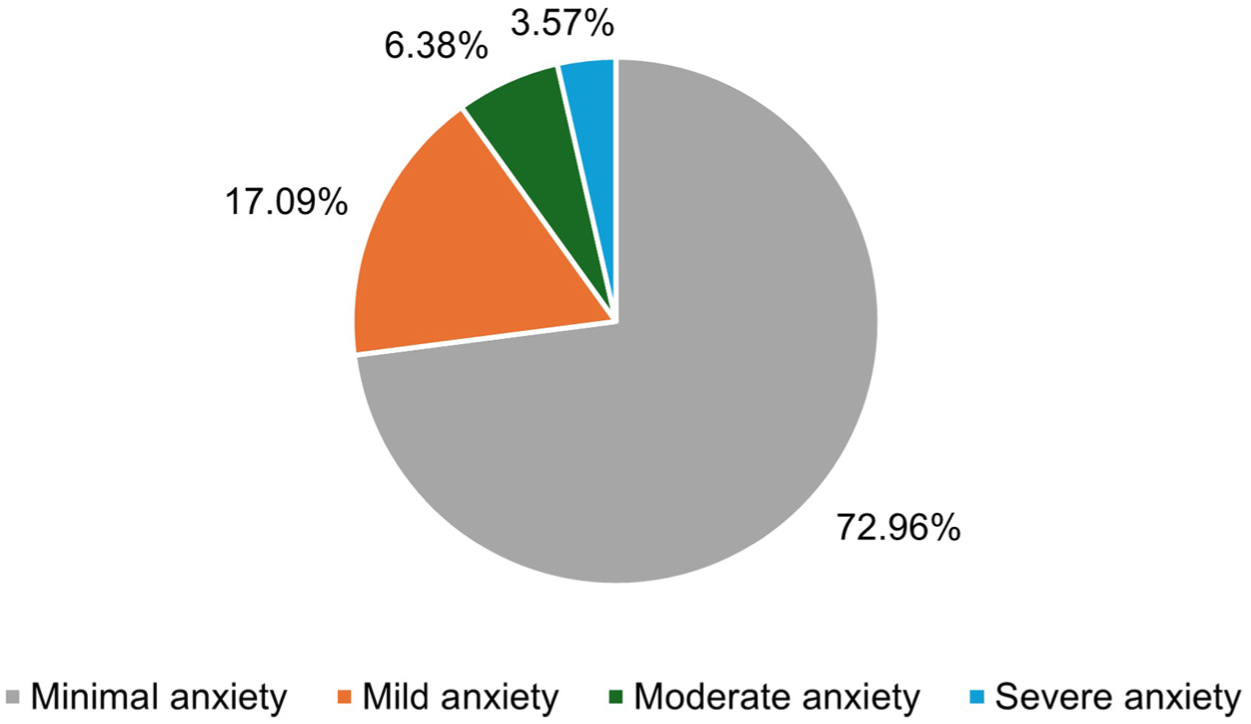
Prevalence of anxiety among participants according to GAD-7 score.
Table 2 illustrates the prevalence of anxiety (GAD-7 ⩾ 5) according to types and sources of social support that the participants perceived. Overall, the prevalence of anxiety in this population was 27.04%. Across the different levels of each social support type, the prevalence of anxiety showed fluctuations without a consistent linear pattern. Moreover, nearly 80% of patients were receiving social support from friends, followed by healthcare workers (70.66%) and family (60.2%). Only a minority of patients (<1%) derived social support from all three sources of social support.
Prevalence of anxiety by types and sources of social support.
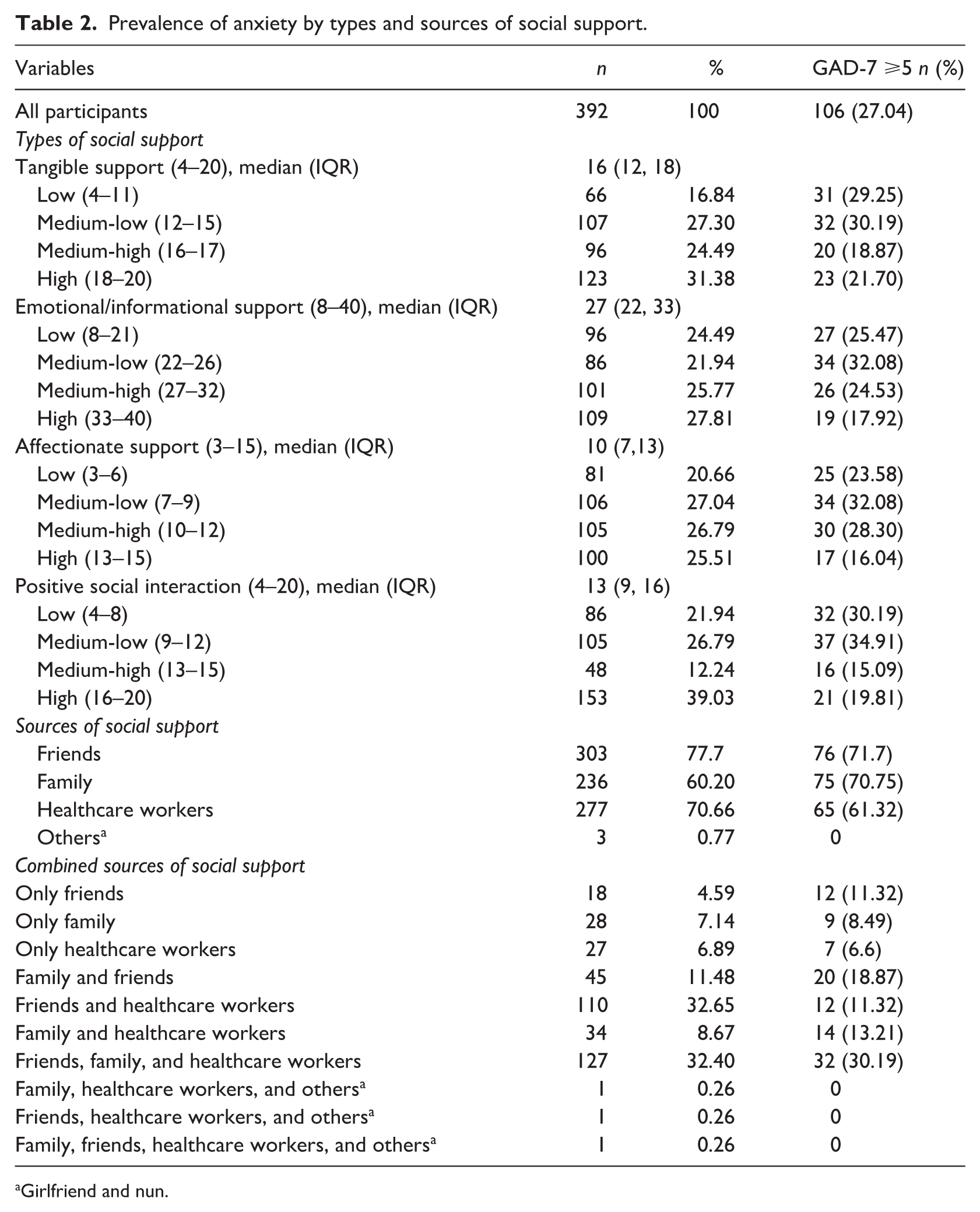
Girlfriend and nun.
Types of social support were evaluated using the aforementioned Vietnamese version of MOS-SSS. Using this scale, we first investigated the statistical association between four types of social support and GAD. Table 3 shows the results from univariate and multivariate logistic regression models. The univariate logistic regression analysis identified several factors associated with GAD among PLWH, including age group, participation in support activities, duration from HIV diagnosis, duration from ART initiation, opportunistic infection, pulmonary tuberculosis, history of illicit drug use, clinical stage, and four types of social support (tangible, emotional/information, affectionate, positive social interaction). The final model was constructed with the following factors: age, participation in support activities, history of illicit drug use, WHO clinical stage, tangible support, emotional/informational support, affectionate support, and positive social interaction. Multivariate logistic regression analysis revealed that age remained independently related to anxiety, with participants aged 26–50 having significantly lower odds of anxiety compared to those aged ⩽ 25 (OR = 0.14; 95% CI: 0.03–0.60). Similarly, a significant association was found for the >50 age group (OR = 0.14; 95% CI: 0.03–0.68). Participation in support activities (OR = 0.91; 95% CI: 0.84–0.99), tangible support, and positive social interaction (OR = 0.91; 95% CI: 0.85–0.97; p = 0.005; OR = 0.91; 95% CI: 0.85–0.98; per one-point increase in MOS-SSS score, respectively) were linked to lower odds of anxiety. Notably, the history of illicit drug use was also inversely associated with anxiety (OR = 0.53; 95% CI: 0.28–1.00). The analysis also indicated that the WHO clinical stage had a significant relationship with anxiety. Specifically, patients in clinical stage III had 2.32 times the odds of GAD compared to those in stages I and II (OR = 2.32; 95% CI: 1.03–5.20).
Univariate and multivariate logistic regression outcomes for determinants of anxiety in the study sample (n = 392).
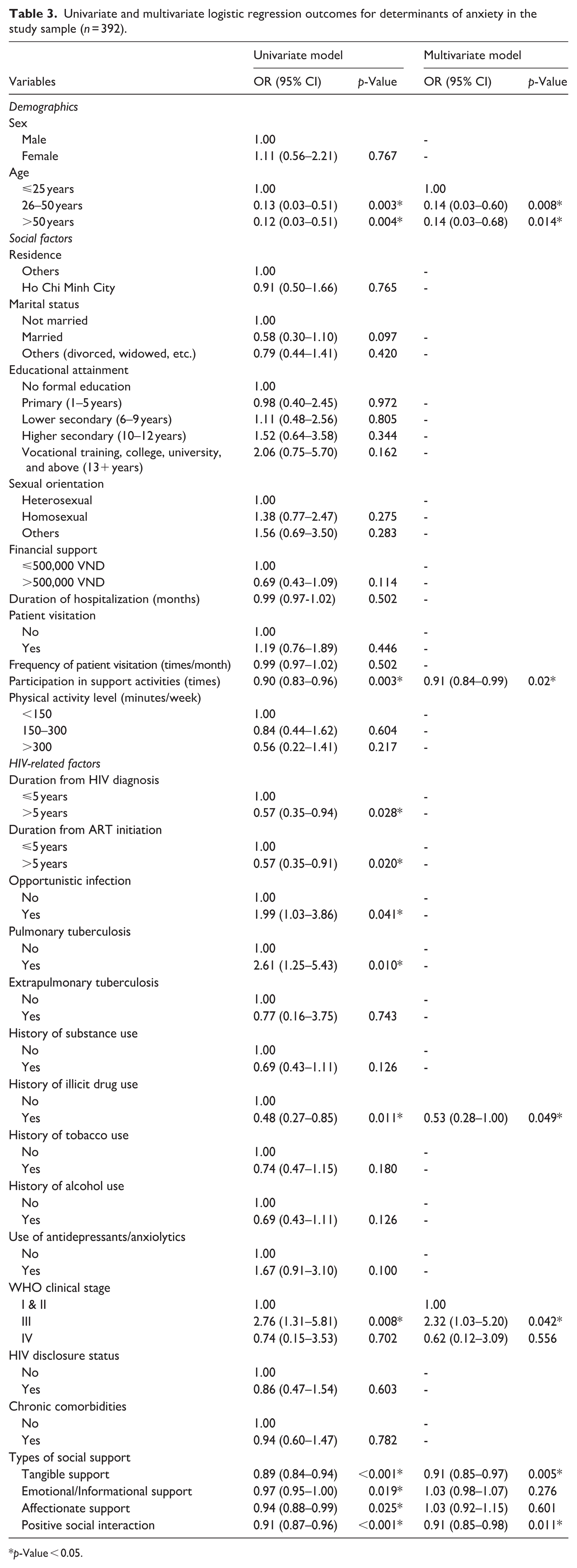
p-Value < 0.05.
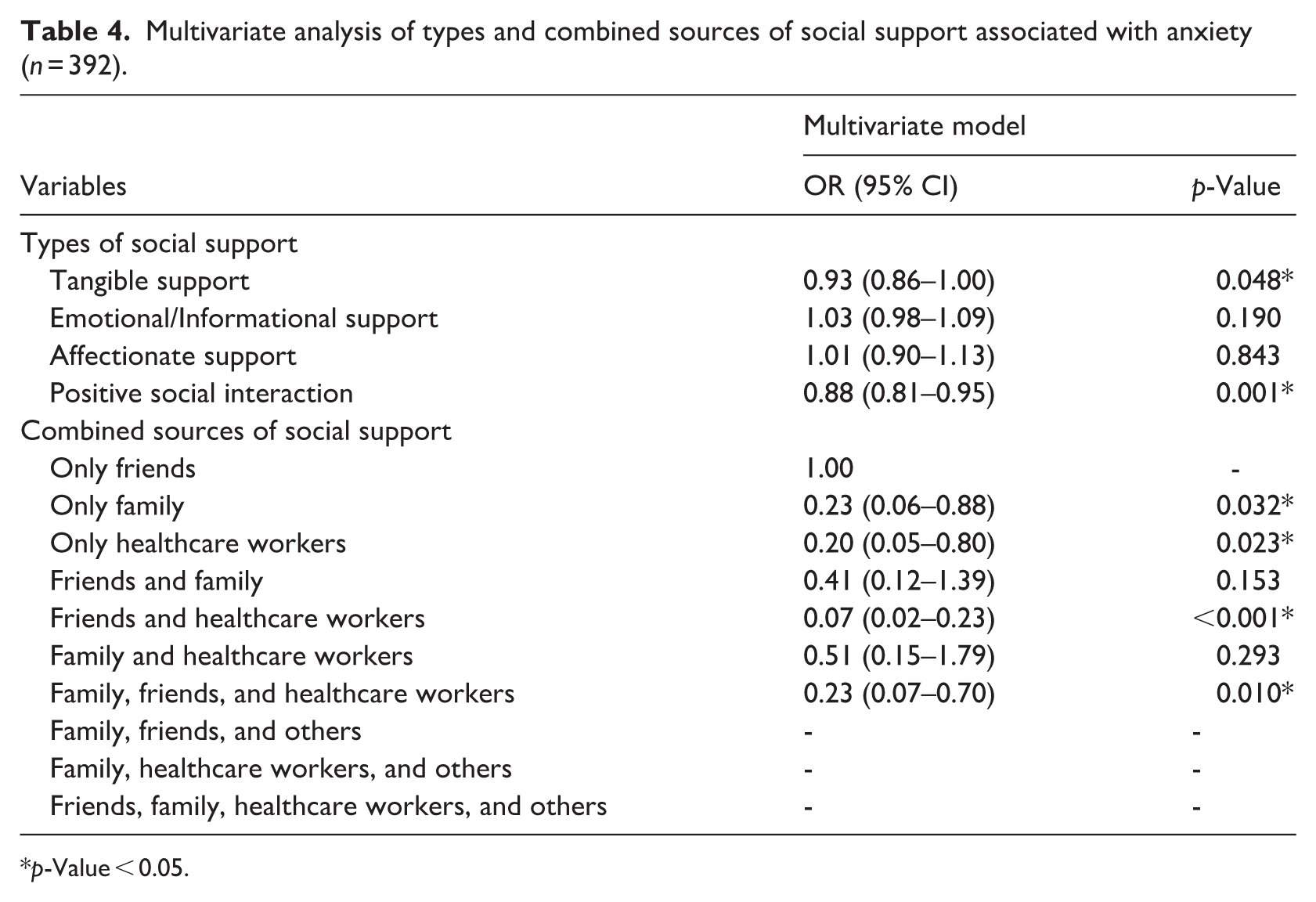
Finally, we analyzed the association between sources of social support and the presence of anxiety. As shown in Table 4, we utilized both social support types and sources in a multivariate logistic regression model. The four types of social support showed a similar pattern to the previous model (Table 3), where tangible support and positive social interaction were associated with reduced odds of anxiety. Compared to receiving support solely from friends, individuals receiving support exclusively from family (OR = 0.23, 95% CI: 0.06–0.88) and those receiving support exclusively from healthcare workers (OR = 0.20, 95% CI: 0.05–0.80) had a significantly lower probability of experiencing anxiety. The strongest inverse association was among participants receiving support from both friends and healthcare workers (OR = 0.07, 95% CI: 0.02–0.23), indicating that this combined source was associated with the lowest odds of anxiety. Furthermore, the group receiving support from family, friends, and healthcare workers also showed a significantly lower odds ratio (OR = 0.23, 95% CI: 0.07–0.70).
Multivariate analysis of types and combined sources of social support associated with anxiety (n = 392).
p-Value < 0.05.
Discussion
The prevalence of anxiety in this study was 27.04%, which was relatively similar to that in general HIV populations (29%; Hu et al., 2025). Meanwhile, the figures in other previous studies targeting Vietnam’s HIV populations ranged from 16.1% to 32.3% (Nguyen et al., 2022; Phan et al., 2025; Thai et al., 2017). This discrepancy can stem from the use of various assessment tools employing different thresholds for anxiety severity, as well as the diverse social and clinical contexts of PLWH in inpatient settings compared with those outside.
Our study demonstrated a significant inverse association between social support and anxiety levels, even after controlling for potential confounders. These findings align with previous literature identifying social support as a key factor linked to lower anxiety risk (Ahmed et al., 2021; Liu et al., 2013; Scardera et al., 2020). Particularly, our study is novel in examining how different types of social support affect anxiety among a specific, understudied population: inpatients in Vietnam, with an average hospital stay of 9 months. Multivariable analysis indicated that only tangible support and positive social interaction remained significantly associated with lower odds of anxiety in the fully adjusted model. This finding may be explained by participants’ concurrent financial and health-related challenges, highlighting the potential role of tangible assistance and meaningful social engagement in mitigating anxiety symptoms.
Our findings reveal that participation in hospital- and community-based support activities is significantly associated with lower odds of anxiety, with each additional activity linked to a 9% decrease in these odds. This inverse association may be explained by the buffering nature of positive social interactions, which likely mitigate loneliness, foster community connection, and serve as an effective coping strategy for PLWH confronting stigma and isolation (Ahmed et al., 2021; Nguyen et al., 2025; Tesfaw et al., 2016). Notably, this is the first study in Vietnam to identify the potential protective role of such hospital- and community-based support activities, underscoring a promising intervention pathway within the inpatient care setting that warrants further investigation.
Key demographic and clinical correlates of anxiety were also identified. Consistent with previous research, age is an associated factor, with older participants (>25 years) demonstrating substantially lower odds of anxiety compared to the youngest cohort (⩽25 years; Ahmed et al., 2021). This may reflect the development of more resilient coping mechanisms and psychological maturity over time, in contrast to the specific, future-oriented pressures that younger individuals often face post-diagnosis. Regarding clinical severity, stage III emerged as a significant correlate of anxiety. This finding is clinically plausible and consistent with previous research, as this stage typically signifies increasing physical symptom burden and heightened concern about disease progression (Alemayehu et al., 2024). Overall, these findings suggest that younger patients and those in more advanced disease stages represent particularly vulnerable subgroups warranting targeted screening and clinical intervention for anxiety.
One of the more unexpected findings of this study was the inverse association between a history of illicit drug use and anxiety symptoms. Our findings differ from earlier research, which reports that a history of substance use is a significant risk factor for psychiatric disorders, including anxiety (Ahmed et al., 2021). Possible explanations include selection effects, differential access to psychosocial or addiction-related services, and reporting bias. Due to the cross-sectional design, directionality cannot be established. Therefore, this result should be interpreted cautiously and considered hypothesis-generating. Longitudinal studies are needed to further examine this relationship.
In this study, friends and healthcare workers were the most common sources of social support among hospitalized PLWH, and their combined support demonstrated the strongest association with lower odds of having anxiety. This finding diverges from established literature, which identifies family support as a factor in correlation with reduced odds of anxiety among community-dwelling PLWH (Oppong Asante, 2012; Seffren et al., 2018). In our sample, family support appeared less influential. This might be due in part to patients’ shared experiences, which create empathy and naturally lead to peer support. Additionally, healthcare workers’ social support—possibly a result of their professional expertise and wealth of experience in HIV/AIDS care—could help to promote less stigmatizing attitudes (Aziz et al., 2023; Dong et al., 2018). Together, these factors create a comfortable and safe care environment, which correlates with a lower level of developing anxiety (Ahmed et al., 2021; Harrison et al., 2023; Lifson et al., 2017; Zhang et al., 2023). These results suggest a new direction for developing social support and mental health interventions. Especially in settings where family support is unavailable, connections with peers and healthcare workers become particularly important.
To the best of the author’s knowledge, this is the first investigation in Vietnam to evaluate the association between social support and anxiety in HIV inpatients. Our study suggests that hospital- and community-based support activities and support from healthcare workers are associated with lower levels of anxiety among HIV patients, thereby suggesting a potential direction for future research within the inpatient care setting. The findings in the study could provide valuable information for further mental health management strategies for HIV patients, especially in contexts that are resource-limited and family-oriented. Social support may be an integral part of a patient’s comprehensive care. Anxiety screening for all HIV patients may warrant consideration to support mental health disorder prevention, quality of life, and improving overall outcomes. Our study has several limitations. First, as this is a cross-sectional study, causality between social support and anxiety cannot be established. Second, since GAD-7 and MOS-SSS are self-reported tools, responses may be subject to recall bias. Thirdly, this study used convenience sampling at a single specialized hospital on PLWH with predominantly male patients, prolonged hospitalization, and a high prevalence of substance use history. Therefore, selection bias may have occurred, and the findings are most applicable to a specific subgroup of hospitalized PLWH rather than to the broader HIV population. Replication across multiple settings is needed to enhance external validity. Finally, our study evaluated anxiety prevalence using a screening tool. Such drawbacks are a starting point for the conduction of further research relating to the clinical diagnosis and interventions of anxiety disorders in inpatient PLWH.
Conclusion
In conclusion, anxiety prevalence in this study was comparable to previous reports on HIV outpatients. Higher levels of tangible support and positive social interaction were associated with lower odds of anxiety. Notably, despite the isolation of hospitalization, support from both family and non-family members (healthcare workers and peers) remained significantly linked to better mental well-being. Future multicenter, longitudinal, and/or intervention research is required to investigate a deeper understanding of this population. These findings provide preliminary evidence that may inform future research on strengthening social networks among hospitalized PLWH, particularly those with limited family support.
Footnotes
Acknowledgements
We acknowledge first and foremost the people living with HIV in Nhan Ai Hospital who contributed their valuable time to participate in our study. We are grateful to the National University of Ho Chi Minh City, Vietnam, for funding our research. We wish to thank the staff of Nhan Ai Hospital who supported us during data collection. Lastly, we also thank Le Van Hang, MD, MSc, for his valuable suggestions during the revision.
ORCID iDs
Ethical considerations
The study was approved by the University of Health Sciences, Vietnam National University, Ho Chi Minh City (reference: 01/QD-HDDD). Ethical clearance was also obtained from Nhan Ai Hospital in January 2025.
Consent to participate
All participants provided informed consent to participate in this study.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
Van Thanh Ngo, Dang Quang Le, Chau Ngoc Nguyen, and Huy Anh Tran contributed equally to this work. Van Thanh Ngo, Chau Ngoc Nguyen, Dang Quang Le, Huy Anh Tran, An Huynh Bao Nguyen, and Anh Thi Duyen Nguyen conceived and designed the study. Van Thanh Ngo, Chau Ngoc Nguyen, Dang Quang Le, Huy Anh Tran, and Anh Thi Duyen Nguyen developed the methodology. Van Thanh Ngo, Chau Ngoc Nguyen, Dang Quang Le, Huy Anh Tran, and An Huynh Bao Nguyen conducted the formal analysis and investigation. Van Thanh Ngo, Chau Ngoc Nguyen, Dang Quang Le, and Huy Anh Tran drafted the first version of the manuscript. Dung Hoang Nguyen, Anh Kim Tran, An Huynh Bao Nguyen, and Anh Thi Duyen Nguyen revised the manuscript for important intellectual content. Dung Hoang Nguyen and Anh Thi Duyen Nguyen acquired the funding. Anh Kim Tran and An Huynh Bao Nguyen provided resources. Dung Hoang Nguyen, Anh Kim Tran, An Huynh Bao Nguyen, and Anh Thi Duyen Nguyen supervised the study. All authors contributed to the interpretation of the findings, discussed the results, and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by Vietnam National University, Ho Chi Minh City, Vietnam (VNUHCM), under grant number 86/QD-DHQG
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.