
Abstract
Medication nonadherence is common among patients diagnosed with schizophrenia and is associated with poor clinical outcomes. The effectiveness of adherence therapy (AT) in improving adherence remains debated, particularly in community settings. This systematic review evaluated the impact of AT on medication adherence among individuals with schizophrenia. Following PRISMA guidelines, eight databases were searched for randomized controlled trials (RCTs) published in English between 2010 and 2023. Study quality was assessed using CONSORT criteria, and risk of bias was evaluated independently by two reviewers using the Cochrane RoB 2 tool. Ten RCTs met the inclusion criteria. Findings indicate that AT is significantly associated with improved medication adherence and positive patient outcomes. Despite these promising results, further high-quality, double-masked RCTs involving diverse populations across different geographic and ethnic backgrounds are required to strengthen the evidence base and support the generalizability of AT in community-based mental health care settings.
Keywords
Introduction
Schizophrenia, a persistent psychiatric disorder, has shown an apparent increase in its global burden in terms of absolute prevalence, incidence, and disability-adjusted life years (DALYs; Solmi et al., 2023). The Global Burden of Diseases, Injuries, and Risk Factors Study reported that between 1990 and 2019, the absolute prevalence of schizophrenia increased by more than 65% (from 14.2 to 23.6 million), incidence by over 37% (from 941,000 to 1.3 million), and DALYs by over 65% (from 9.1 to 15.1 million) (Solmi et al., 2023; Vos et al., 2020). Over the same period, the global population increased by approximately 45%, contributing to substantial rises in the absolute prevalence, incidence, and DALYs of schizophrenia, which underscores the growing global burden of the disorder over time; however, age-standardized rates remained relatively stable, indicating that the underlying risk of schizophrenia has not markedly changed.
The sex distribution of the burden of schizophrenia has remained consistent in the general population over the past three decades, with a ratio of 1.1 males to females. However, this ratio decreases from younger to older age groups (Solmi et al., 2023; Vos et al., 2020). Interestingly, after the age of 65, the prevalence of schizophrenia is higher in females compared to males. Additionally, males tend to experience an earlier onset of the disorder, while females have a longer life expectancy. Those findings suggested that the sex ratio of schizophrenia changes throughout the lifespan, indicating variations in age of onset and survival based on sex (Solmi et al., 2023; Vos et al., 2020).
Medication adherence is often suboptimal in chronic conditions, as shown by low treatment adherence for cardiovascular disease and its association with factors such as smoking, marital status, and comorbid illnesses (Guo et al., 2023; Subih et al., 2023). Schizophrenia’s incidence, prevalence, and disability-adjusted life years (DALYs) have increased since 1990, and it remains underdiagnosed, particularly in developing nations; projections indicate a continuing rise (Charlson et al., 2018; Vos et al., 2020). These patterns highlight an urgent need for mental health services in the community, including adherence support and follow-up, to reduce relapses and improve outcomes. Although many interventions to improve patient compliance have been explored (Alizioti and Lyrakos, 2021; Bäuml et al., 2016; Cahaya et al., 2022; Chien et al., 2015; Staring et al., 2010; Uslu and Buldukoglu, 2020), no systematic reviews have assessed adherence therapy for individuals with schizophrenia. Thus, there is a need for a comprehensive, qualitative narrative summary to synthesize the available evidence, identify gaps, and evaluate adherence therapy across diverse contexts.
Recent guidelines urge the use of maintenance therapy with antipsychotics for a minimum duration of 5 years for individuals diagnosed with schizophrenia who experience recurring episodes (Barnes et al., 2020; Gaebel et al., 2020). Relapses occurred despite the administration of antipsychotic medication during the outpatient phase, primarily attributable to patient noncompliance (Barnes et al., 2020; Gaebel et al., 2020). Therefore, the focus should be on enhancing compliance, which entails acknowledging the heightened susceptibility to adverse effects, including tardive dyskinesia (Stahl et al., 2021); patients must undergo thorough training to effectively identify their side effects in a timely manner and adjust their treatment regimen in close collaboration with their psychiatrists (Stahl et al., 2021).
Nonadherence to treatment among patients diagnosed with schizophrenia has been associated with an increased risk of relapse (Kareem and Mahmood, 2022) and a higher likelihood of suicide and suicide attempts (Álvarez et al., 2022). A systematic review reported that the prevalence of suicide attempts was 20.3% in schizophrenia (SZ), 46.8% in schizoaffective disorder (SZAF), 11.1% in delusional disorder (DD), and 12.5% in first-episode psychosis (Álvarez et al., 2022). The review further indicated that higher rates of suicide attempts were observed in outpatient samples compared to inpatient populations, highlighting the potential vulnerability of individuals receiving community-based care. Medication adherence has been shown to reduce the likelihood of psychiatric hospitalization, utilization of emergency services, and legal involvement related to substance use (Baryakova et al., 2023). Conversely, noncompliance with medication in the first year has been shown to be associated with unfavorable outcomes like emergency department visits, leading to increased recidivism (Stewart et al., 2023; Tsikada, 2020).
Previous studies have used randomized controlled trials (RCTs) to examine the effectiveness of adherence therapy (AT) in improving adherence to antipsychotic medication among patients diagnosed with schizophrenia (Alizioti and Lyrakos, 2021; Bäuml et al., 2016; Chien et al., 2015; Staring et al., 2010; Uslu and Buldukoglu, 2020). While adherence related factors may differ between inpatient and outpatient populations, for example due to the level of supervision, structure of care, or access to community support, both groups are critical to understanding the overall effectiveness of AT. Therefore, examining evidence across these diverse care settings allows for a more comprehensive synthesis of interventions and their applicability in real world clinical practice. Despite several studies investigating adherence interventions, no systematic review has specifically evaluated AT across both inpatient and community based populations (Curto et al., 2021). Accordingly, this systematic review aims to evaluate the effectiveness of AT in enhancing medication adherence among patients diagnosed with schizophrenia in both inpatient and outpatient settings. The results of this study could contribute to the development and implementation of strategies, policies, and protocols to prevent and manage medication nonadherence among patients diagnosed with schizophrenia.
Aim
The purpose of this systematic research was to assess effective adherence therapy in improving medication adherence among patients diagnosed with schizophrenia in both inpatient and community settings.
Methods of review
Search strategy
This systematic review followed the guidelines established by PRISMA (Page et al., 2021) and was registered in the PROSPERO database (ID: CRD420261416466). Using the PICOS framework (P-population, I-intervention, C-comparison, O-outcomes, S-study design), research questions and eligibility criteria for inclusion were defined. A three-step search strategy was employed to identify published and unpublished studies published in English from 2010 to 2023:
(i) Step 1: Database Search
(ii) Step 2: Reference List Screening—The reference lists of all included articles were checked for additional relevant studies.
(iii) Step 3: Search for Unpublished Studies and Dissertations—The search also included unpublished studies, conference proceedings, and dissertations to help reduce publication bias. A detailed description of the search strategies for each database, including search syntax, subject headings, and the number of results retrieved, is provided in Supplemental Table S1.
Inclusion criteria
Studies were included in this review if they met the following criteria: (i) participants were adults aged 18 years and older diagnosed with schizophrenia spectrum disorders; (ii) the primary objective of the study was to investigate the effectiveness of adherence therapy (AT) in improving medication adherence; (iii) participants were either hospitalized (inpatients) or living in the community (outpatients) ; (iv) the study design was a randomized controlled trial (RCT) examining medication adherence among patients with schizophrenia; (v) the intervention specifically involved any modality of adherence therapy aimed at enhancing medication adherence; and (vi) The study was published in English between 2010 and 2023. Opinion pieces, literature reviews, and editorials were excluded from this review.
Screening and selection of included studies
The screening procedures involved two authors who independently evaluated all relevant search results based on titles and abstracts. Articles meeting the predetermined inclusion criteria proceeded to full-text review, during which the same authors independently assessed complete publications using a standardized template adapted from the Cochrane Review data collection form. Any disagreements between the two authors were first addressed through careful discussion and consideration. If consensus could not be reached, a third author was consulted to resolve the differences. Duplicate articles and studies not meeting the inclusion criteria were excluded from the analysis.
Quality assessment of included studies
Two reviewers independently assessed the quality of the included randomized controlled trials (RCTs). The reporting quality of the RCTs was evaluated using the Consolidated Standards of Reporting Trials (CONSORT) checklist to ensure transparency and completeness in reporting key trial elements. To assess the risk of bias in the RCTs, the Cochrane RoB 2 tool was applied, as recommended by the Cochrane Handbook (Sterne et al., 2019). This tool evaluates potential sources of bias across five domains: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Each study was assigned an overall risk of bias judgment based on these assessments. Disagreements between reviewers were resolved through discussion or consultation with a third reviewer.
Data extraction
Studies that had previously been identified for this review were used to extract data, which was done using a specifically designed electronic data extraction sheet. Included in the extracted data were identifying information on the study (title, year published), where the study was performed (country), what primary and secondary outcomes were measured, what instruments were used to collect data, what study design was employed, what intervention(s) were delivered and for how long, the size of the population/sample in the study, limitations identified in the study, and the study findings related to the review questions and specific objectives. The authors of the primary literature were contacted to help us find out whether they could provide additional information or clarify any unclear information. We selected a total of ten RCTs that met our pre-established criteria. A systematic research methodology has been employed to collect articles for the present study. This methodology can be found in Figure 1 (the PRISMA Flow Diagram), which illustrates the process of identifying and selecting research. Each of the selected studies was evaluated against specific, predetermined inclusion criteria (i.e. relevance) before it was included in the subsequent analysis. Therefore, it is necessary to evaluate your own research against these criteria when developing your analysis. Researcher 1 was assigned the task of performing the first assessment of each of the studies identified as potentially relevant to the present study. A total of 480 studies were identified as possibly relevant to the present study by this process. Of these, ten studies were ultimately selected for inclusion in the final review of the current research due to their appropriateness. A summary of the included studies is presented in Table 1.
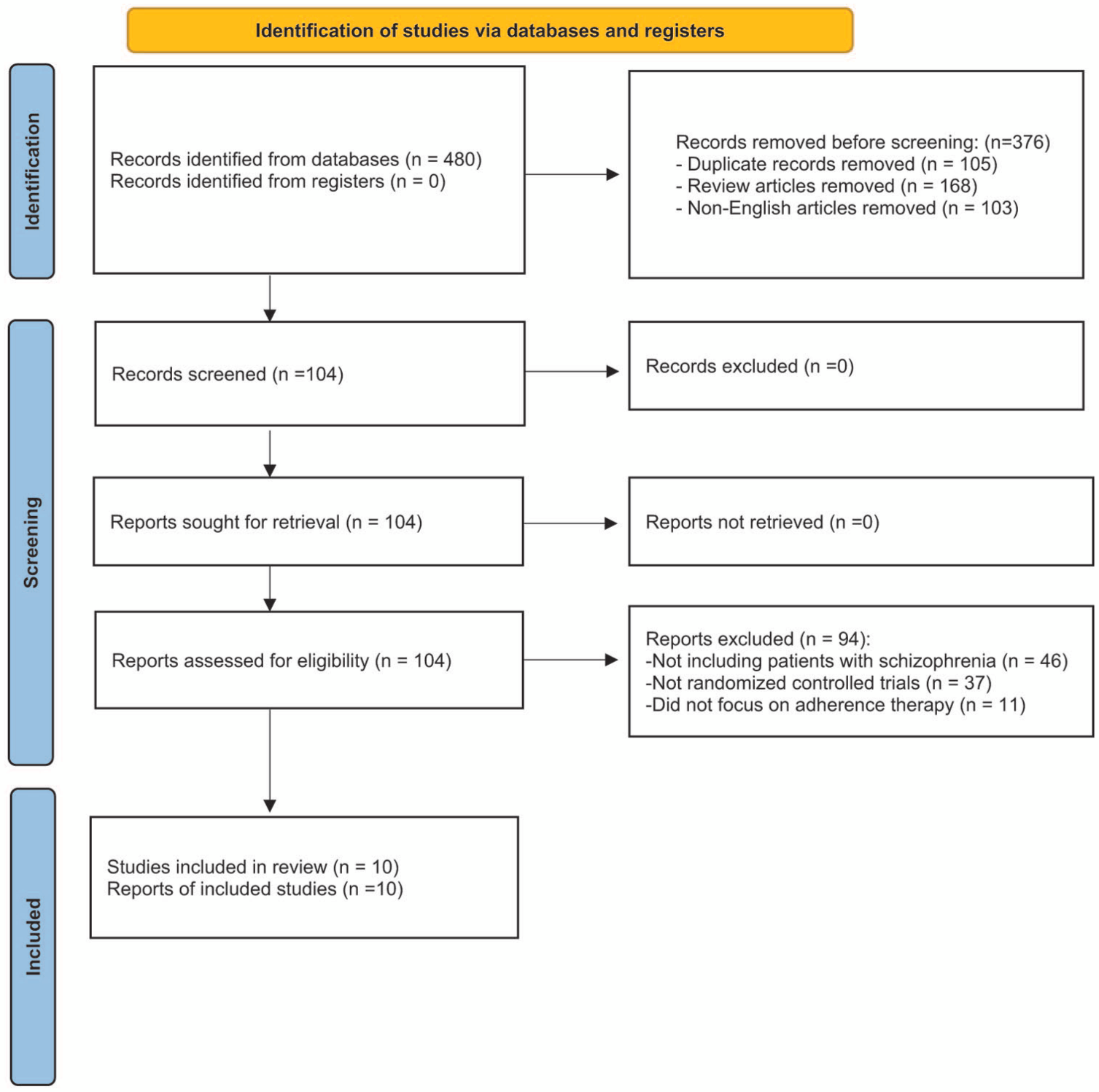
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources.
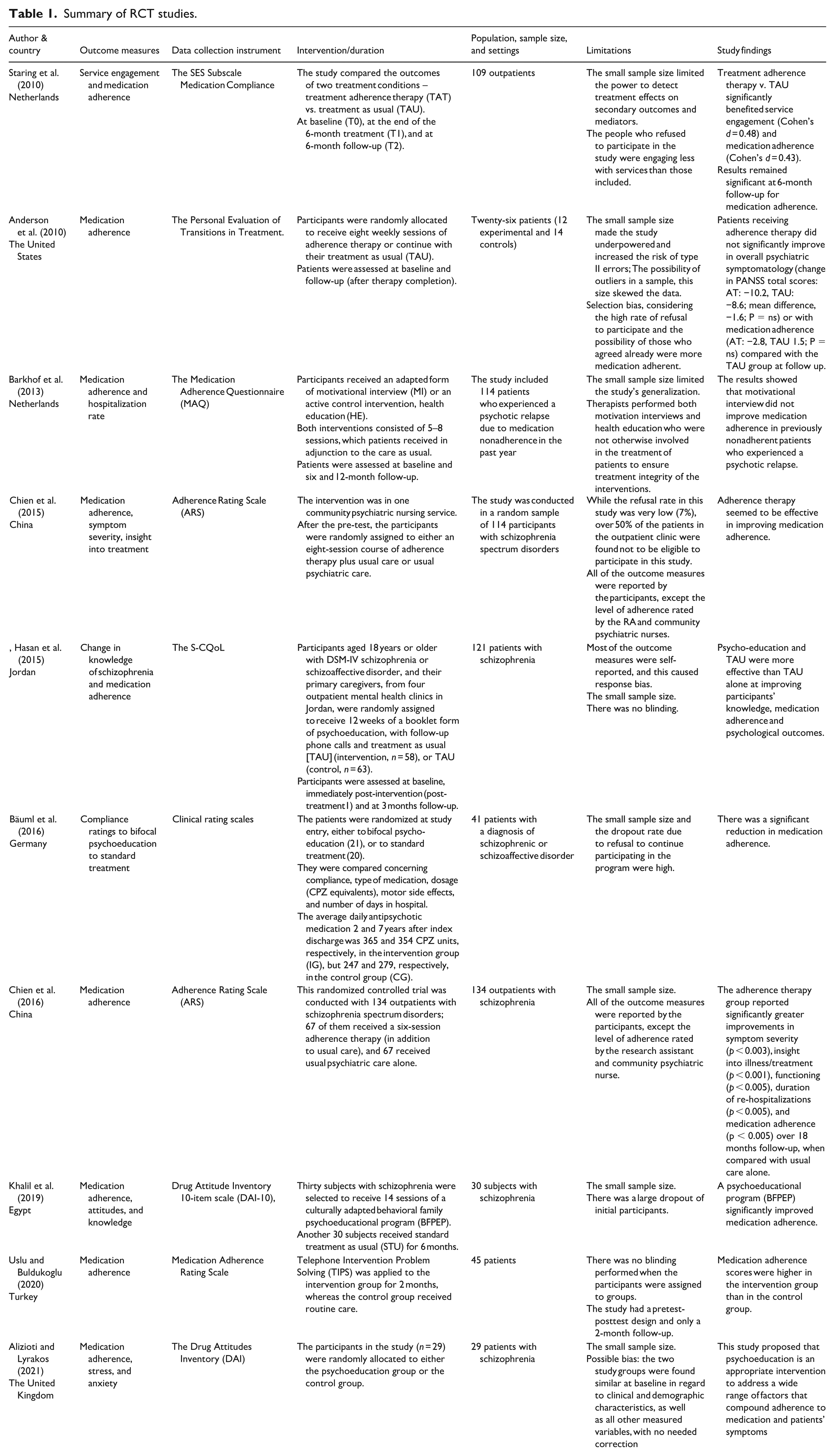
Summary of RCT studies.
Outcome measures
Medication adherence was measured using a variety of instruments across the included studies, including self-reported scales, clinician assessments, and objective indicators. No restrictions were placed on the method of adherence measurement to allow for a broader inclusion of studies and to reflect variability in clinical practice. Due to this heterogeneity in outcome measures, a qualitative systematic review approach was adopted.
Results
Study selection
The research methodology of this study included a systematic strategy to extract articles. The process of locating and selecting research is depicted in Figure 1, which showcases the PRISMA flow chart. The collected studies were assessed for their relevance using predetermined inclusion criteria. The researchers conducted an initial assessment separately to determine if they met the criteria for inclusion or exclusion. A total of 480 research publications were identified as potentially relevant to the current topic. Ten papers were chosen for inclusion in the comprehensive review based on their appropriateness. The inquiry was conducted by considering three stages of data evaluation. In phase I, databases were queried to identify studies that met the predetermined criteria. The investigation focused on scientific research articles published from 2010 to 2023. A grand number of 480 papers were obtained throughout the initial phase of the project. In the second part of the investigation, the initial selection of publications was conducted by removing duplicate articles (n = 105), deleting review articles (n = 168), and excluding research articles published in languages other than English (n = 103). During Phase III, the manuscript underwent scrutiny in 94 research journals. A total of 46 studies were excluded from the analysis due to their primary focus on populations that differed from patients diagnosed with schizophrenia. Additionally, 37 articles that did not employ RCTs were excluded from the study. Furthermore, the current study used a stringent selection criterion by removing research that did not solely examine AT. As a result, ten RCTs met the established criteria for eligibility. The study selection process is presented in Figure 1.
Study characteristics
This systematic review included a total of ten randomized controlled trials (RCTs) published between 2010 and 2023 (Alizioti and Lyrakos, 2021; Anderson et al., 2010; Barkhof et al., 2013; Bäuml et al., 2016; Chien et al., 2015, 2016; Hasan et al., 2015; Khalil et al., 2019; Staring et al., 2010; Uslu and Buldukoglu, 2020). The majority of included studies (n = 9) utilized a control group receiving standard psychiatric care without additional intervention, thereby allowing for direct comparison with adherence therapy interventions. In contrast, one study employed a health education intervention as an active control condition (Barkhof et al., 2013).
Medication adherence was the primary outcome in most of the included trials, although it was assessed as a secondary outcome in a minority of studies. Notably, considerable heterogeneity was observed across studies in terms of outcome measurement tools, with no single standardized instrument consistently applied across all trials. This variability limits the direct comparability of findings and represents a key source of methodological heterogeneity within the review (Alizioti and Lyrakos, 2021; Barkhof et al., 2013; Bäuml et al., 2016; Chien et al., 2015; Khalil et al., 2019; Staring et al., 2010; Uslu and Buldukoglu, 2020).
There are multiple validated tools to assess adherence to medications prescribed. The three studies utilized the Adherence Rating Scale (ARS; Chien et al., 2015, 2016; Uslu and Buldukoglu, 2020). Additional studies utilized various self-reporting and clinician-reported tools, such as the Drug Attitudes Inventory (DAI; Alizioti and Lyrakos, 2021; Khalil et al., 2019), the compliance rating scale developed by Bäuml et al. (2016), the Medication Adherence Questionnaire (MAQ; Barkhof et al., 2013), and the Personal Evaluation of Transitions in Treatment scale (Anderson et al., 2010). Also, the study by Hasan et al. (2015) used the Schizophrenia Quality of Life Scale (S-CQoL) to assess the impact of adherence on quality of life. Additionally, the SES subscale from the Staring et al. (2010) study was also utilized to assess adherence in this trial. Overall, the diversity of outcome measures and assessment tools underscores the lack of standardization in evaluating medication adherence in schizophrenia research, which may contribute to variability in reported outcomes across studies. The characteristics of the included studies are summarized in Table 1.
Risk of bias assessment
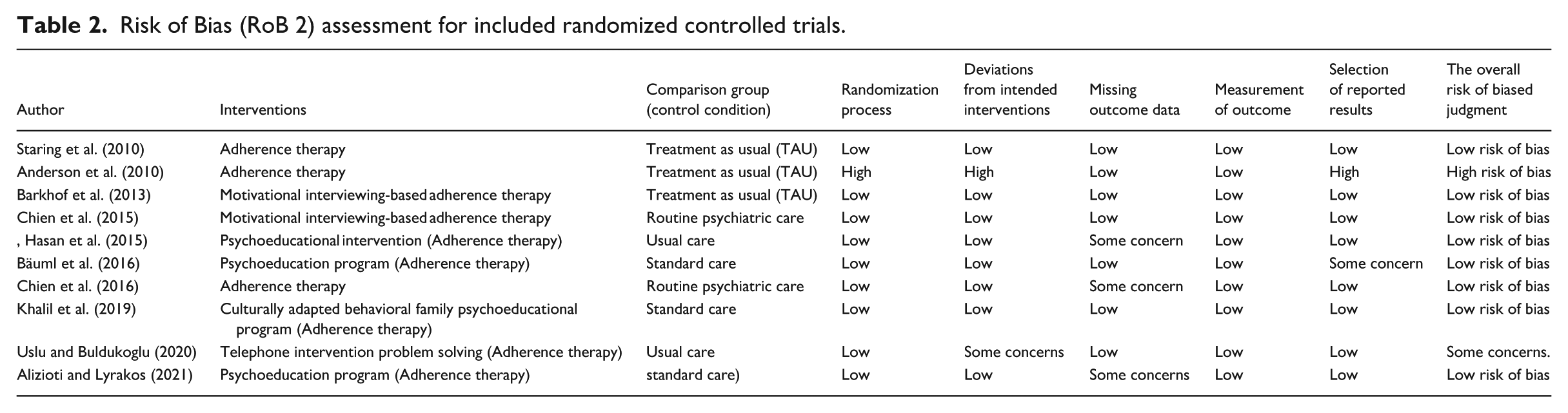
Overall, the majority of studies exhibited a low risk of bias across all domains assessed for randomization and outcomes. A few studies had a higher risk, as indicated by Anderson et al. (2010), which was due mostly to risk in randomization and deviation from the intervention. Likewise, the study by Uslu and Buldukoglu (2020) indicated deviation from the intended intervention as a source of concern.
Most studies explained how they concealed allocation, although Anderson et al. (2010) were less clear about this. Due to the psychosocial nature of adherence therapy, no study was able to blind participants. Most studies used patient self-reported outcomes, but some used objective outcomes (Chien et al., 2015). The risk of bias assessment of the included randomized controlled trials is summarized in Table 2.
Risk of Bias (RoB 2) assessment for included randomized controlled trials.
Effectiveness of adherence therapy
A meta-analysis was not conducted due to significant heterogeneity among the included studies in terms of intervention formats, outcome measures, and follow-up durations. Specifically, variations were observed in the delivery of adherence therapy (e.g. motivational interview-based, psychoeducational, or telephone-based interventions), differences in adherence measurement tools, and inconsistencies in follow-up periods. Therefore, a narrative synthesis was the most appropriate approach.
Findings based on intervention characteristics
The various methods of delivering adherence intervention were different across the included RCTs. Several studies employed motivational interview-based adherence therapy, which focused on enhancing the patient’s intrinsic motivation to adhere to the prescribed regimen of treatment through collaborative and patient-centered communication techniques. Improvements in patients’ insight and motivation to engage with treatment were documented via these techniques (Barkhof et al., 2013; Chien et al., 2015).
In contrast, other studies employed psychoeducation as an intervention means by trying to enhance and improve patient knowledge about, and understanding of, schizophrenia and the importance of taking medications as intended. Psychoeducational treatment was often delivered in the form of structured education, sometimes built into the sessions with family to support adherence. Such approaches were used extensively in the literature, with the majority of studies providing support for improved adherence-related outcomes (Alizioti and Lyrakos, 2021; Bäuml et al., 2016; Hasan et al., 2015; Khalil et al., 2019).
Additionally, several studies incorporated behavioral or structured adherence therapy approaches, targeting the modification of patient attitudes and behaviors regarding medication using structured therapeutic techniques. The main focus of these interventions was producing and maintaining behavioral changes through problem-solving, goal-setting, and addressing barriers to adherence (Anderson et al., 2010; Staring et al., 2010). Furthermore, a separate study used a telephone-based nursing intervention and identified that continuous follow-up and remote assistance helped to improve medication compliance for patients diagnosed with schizophrenia (Uslu and Buldukoglu, 2020).
Despite these variations in intervention modalities, a common underlying objective across all studies was to enhance patients’ understanding, motivation, and active engagement in medication adherence, suggesting that different therapeutic approaches may achieve similar outcomes through distinct mechanisms (Alizioti and Lyrakos, 2021; Barkhof et al., 2013; Bäuml et al., 2016; Chien et al., 2015; Hasan et al., 2015; Khalil et al., 2019; Staring et al., 2010; Uslu and Buldukoglu, 2020).
Findings based on outcome measures
Across the ten included randomized controlled trials, the majority of studies reported positive effects of adherence therapy on medication adherence outcomes. Specifically, eight studies demonstrated statistically significant improvements in adherence among participants receiving adherence therapy compared to those receiving usual care or control interventions. These findings suggest that adherence therapy is generally effective in enhancing medication-taking behaviors among individuals diagnosed with schizophrenia (Alizioti and Lyrakos, 2021; Bäuml et al., 2016; Chien et al., 2015, 2016; Hasan et al., 2015; Khalil et al., 2019; Staring et al., 2010; Uslu and Buldukoglu, 2020).
However, not all studies yielded similar results due to differences in study designs, populations, and other variables. Two studies exhibited either a limited effect or no significant effect of adherence therapy interventions on medication adherence outcomes. The variability among studies was likely due to differences in intervention characteristics and adherence measures used to determine adherence. Overall, discrepancies among study results emphasize that measuring medication adherence is complex and may be affected by contextual differences or methodological differences between studies (Alizioti and Lyrakos, 2021; Barkhof et al., 2013).
Findings based on study settings and follow-up
The included studies were conducted across a range of clinical settings, including community-based, outpatient, and inpatient environments, reflecting the diverse contexts in which individuals with schizophrenia receive care. This diversity enhances the generalizability of the findings but also introduces variability in how adherence therapy is implemented and evaluated across settings (Alizioti and Lyrakos, 2021; Hasan et al., 2015; Uslu and Buldukoglu, 2020).
Moreover, the duration of follow-up varied considerably across the included trials, ranging from 3 months to 7 years. However, it is important to note that in most randomized controlled trials, the primary effectiveness outcomes were assessed at the end of the intervention period or within short-term follow-up (typically up to approximately 6 months), with fewer studies incorporating long-term follow-up assessments. Therefore, differences in longer follow-up durations are less likely to have substantially influenced the primary effectiveness comparisons across most included studies. Nonetheless, longer follow-up periods, where available, provide additional insight into the sustainability of intervention effects over time (Bäuml et al., 2016; Chien et al., 2015).
This variability in study settings and follow-up durations may partially explain differences in reported outcomes, as short-term improvements may not necessarily reflect sustained adherence over time. Therefore, caution interpretation is warranted when considering the overall effectiveness of adherence therapy across heterogeneous study designs and follow-up periods (Bäuml et al., 2016; Staring et al., 2010).
Overall effectiveness
Overall, the majority of included RCTs demonstrated that adherence therapy has a positive effect on improving medication adherence among individuals with schizophrenia. However, due to heterogeneity in intervention design, outcome measurement, and study duration, the magnitude and consistency of this effect vary across studies. Therefore, findings should be interpreted with caution.
Discussion
The systematic review analyzed the role of Adherence Therapy (AT) in improving medication adherence in patients diagnosed with schizophrenia. The literature demonstrates that the topic of AT and how it impacts medication adherence in this population is poorly studied, although the importance of adherence to medication in this group is well established (Dikec and Kutlu, 2016; Gray et al., 2016; Nyanyiwa et al., 2022). This review included ten (10) randomized controlled trials (RCT’s) on AT and provided evidence suggesting that AT will likely improve the adherence to medication for the majority of patients receiving AT; however, there was no complete agreement among the outcomes of the 10 studies.
Of the ten RCTs in this review, eight studies found statistically significantly improvements in medication adherence; whereas two did not detect statistically significant effects in their individual analyses (Anderson et al., 2010; Barkhof et al., 2013). A future meta-analysis that statistically pools data from all eligible trials is likely to give a more precise estimate of the total intervention effect that is likely to be found across settings. Combining results may yield greater statistical power and offer clearer guidance about whether adherence therapy can be expected to have a consistent benefit across settings and populations. Such an analysis of individual participant data would undoubtedly be helpful in future work. Several factors may also help explain the differences observed between study findings. Methodological issues may exist with the interventions in Barkhof et al.’s (2013) study; in particular, their method of intervention (i.e. motivational interviewing) primarily utilized a lower intensity of intervention, and their study had relatively short follow-up periods, so it may have lacked sufficient time to see any changes in adherence to medication. The authors of this study mentioned that Anderson et al. (2010) limited their sample size (which was also relatively small), which would also limit the statistical power of any detected effects. Another potential factor might be that outcome measures were affected by differences in the populations studied across RCTs. For example, in the study conducted by Barkhof et al. (2013), the participant’s history of being nonadherent (due to having had many previous episodes of schizophrenia) limited any improvement from short-term intervention. However, most of the other RCTs studied population groups that had been diagnosed with either generalized anxiety disorder or hypomania and, as such, may have benefited more from behaviorally-based interventions than patient groups in the Barkhof et al. study (Alizioti and Lyrakos, 2021; Bäuml et al., 2016; Chien et al., 2015, 2016; Hasan et al., 2015; Khalil et al., 2019; Staring et al., 2010; Uslu and Buldukoglu, 2020). Differences in the outcomes of the studies were likely influenced by differences in intervention intensity, delivery, or components. For example, Khalil et al. (2019), Barkhof et al. (2013), and Uslu and Buldukoglu (2020) assessed various intensive intervention methods, including family involvement and therapist-directed intervention. In contrast, some studies assessed less intensive interventions over shorter durations, likely leading to lower benefits of the intervention. In addition, although some of the studies used standardized scales for assessing adherence such as the Adherence Rating Scale (Chien et al., 2015, 2016; Uslu and Buldukoglu, 2020), many other studies used various assessment instruments, thus decreasing comparability across the various outcome measures used in the studies.
Despite these variations, the overall pattern of evidence suggests that AT can positively enhance medication adherence, particularly in patients with moderate adherence levels or positive attitudes toward their medications. Accordingly, international evidence has confirmed the effectiveness of AT in several countries, including the United states (Alizioti and Lyrakos, 2021; Barkhof et al., 2013; Khalil et al., 2019; Staring et al., 2010; Uslu and Buldukoglu, 2020), the Netherlands (Barkhof et al., 2013; Staring et al., 2010), China (Chien et al., 2015, 2016), the United Kingdom (Alizioti and Lyrakos, 2021), Jordan (Hasan et al., 2015), Germany (Bäuml et al., 2016), Egypt (Khalil et al., 2019), and Turkey (Uslu and Buldukoglu, 2020).
Clearly, these findings indicate that ATs have considerable potential for widespread implementation, though cultural and health system differences may moderate their effectiveness.
Evidence from different service settings including inpatient and outpatient psychiatric facilities shows better medication adherence among people with schizophrenia (Alizioti and Lyrakos, 2021; Barkhof et al., 2013; Chien et al., 2016; Hasan et al., 2015; Khalil et al., 2019; Staring et al., 2010). Similar improvements were reported in community mental health centers (Anderson et al., 2010; Chien et al., 2015). In addition, a few studies remarked the beneficial effect of AT on medication adherence in psychiatric hospitals (Bäuml et al., 2016; Uslu and Buldukoglu, 2020).
Numerous RCTs evaluated the outcomes of measuring medication adherence, employing a variety of assessment tools. The Adherence Rating Scale (ARS) was one of the primary and frequently used instruments for evaluating adherence (Chien et al., 2015, 2016; Uslu and Buldukoglu, 2020). Different types of intervention have also been trialed to assess potential ways to improve medication adherence in the clinical setting (e.g. educated, behavior-based, and technologically-assisted interventions; Loots et al., 2021). The most commonly found components of adherence interventions were, but not limited to: patient education (Alizioti and Lyrakos, 2021; Bäuml et al., 2016; Hasan et al., 2015; Khalil et al., 2019), therapist-assisted sessions (Barkhof et al., 2013), family involvement in therapeutic interventions (Khalil et al., 2019) and telephone follow-ups (Uslu and Buldukoglu, 2020). Different methods of enhancing patient adherence were used in some studies, such as motivational interviewing and blended therapy (Barkhof et al., 2013; Chien et al., 2015; Staring et al., 2010).
Although there are numerous studies showing that AT has a positive effect, additional research using larger sample sizes and rigorous RCT methodologies is needed to enhance the evidence base and improve treatment methods for diverse patient populations.
Potential biases in the review process
The quality of RCTs included in this review was generally satisfactory. Most RCTs had a low risk of bias related to randomization processes and outcome assessments, although several studies demonstrated methodological limitations. For example, Anderson et al. (2010) was judged to have a high risk of bias related to the randomization process. Likewise, Uslu and Buldukoglu (2020) had some methodological flaws. Small sample sizes, short follow-up periods, and high rates of treatment refusal or non response may have reduced levels the internal validity and generalizability of the findings.
In contrast, Chien et al. (2015) demonstrated greater methodological rigor than the other included studies. Participants were recruited using a rigorous methodology, and sa clear protocol was implemented to manage missing data during the trial. In addition, the study showed a low risk of selective reporting bias due to the adequate descriptions of participants allocation, randomization concealment, and blinding procedures for outcome assessment, where applicable in psychosocial adherence therapy interventions.
In reporting the results and making sense of the implications, the limitations in methodologies particularly the use of patient-reported outcome measures in quasiexperimental studies should be borne in mind. On the positive side, several studies used objective measures (e.g. medication adherence rates and rehospitalization) which were reassuring. There is promise associated with adherence therapy for those with schizophrenia to support better adherence. With more RCTs, of better quality, and with more poorer quality studies, the evidence will gain more weight and be more persuasive.
Limitations
This systematic review has some limitations, including the low number of RCTs found, and considerable variation in follow-up time points across studies, which may lessen the applicability of the results. In addition, different RCTs used different methods to measure patient-reported outcomes for similar clinical endpoints, therefore limiting the ability to compare the results of those studies to one another. Also, one of the studies had a sample size that was not large enough to have adequate power, potentially increasing the chance of Type II error. Furthermore, by focusing on a qualitative narrative approach, this review is limited in its ability to quantify the overall effect of adherence therapy on medication adherence while controlling for variations in interventions.
Implication for practice and research
In order to empower patients and enhance their sense of control over their illness, it is advisable to incorporate AT into their treatment plan by using the cognitive behavioral therapy (CBT) and motivational interviewing (MI) therapeutic techniques, as these approaches are integral to AT (Gray et al., 2016). The implementation of CBT and MI may lead to an improvement in patients’ overall functioning, with the emphasis on adherence becoming less significant (Gray et al., 2016; Lin et al., 2022). Further studies are needed to elucidate the mechanisms underlying the effectiveness of AT, thereby ensuring its optimal application in various contexts and identifying which sociodemographic groups may be most receptive to this intervention.
Conclusions
The available RCTs examining the impact of AT on medication adherence in patients diagnosed with schizophrenia were limited, indicating the need for further investigation. This systematic review provides evidence suggesting that AT may be effective in improving medication adherence among patients diagnosed with schizophrenia. The review suggested that patients diagnosed with schizophrenia, particularly those with moderate adherence or positive attitudes toward their medications, could benefit from receiving AT as an adjunct therapy. However, patients with negative attitudes toward medications or low baseline adherence may represent a higher-risk group, and future research should investigate the effectiveness of AT specifically within this population.
Footnotes
Acknowledgements
The authors would like to acknowledge all researchers whose studies were included in this systematic review. The authors also appreciate the support provided by colleagues and academic staff who contributed to the development and completion of this work.
Author note
The manuscript has been seen and approved by all authors involved and is being published nor being considered for publication elsewhere.
Ethical considerations
This systematic review used published literature and did not involve primary data collection; therefore, formal ethical approval was not required.
Consent to participate
Consent to participate is not applicable to this review article as no data were collected from participants.
Consent for publication
Consent for publication is not applicable to this review article as no identifiable participant data are included.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data generated or analyzed are included in this article. Additional data are available from the corresponding author on reasonable request.*