
Abstract
This qualitative study explored the psychosocial experiences of individuals with type 1 and type 2 diabetes in underserved settings, focusing on suicidal ideation and coping mechanisms. Semi-structured interviews were conducted with 30 participants and analyzed using thematic analysis. Findings revealed substantial emotional distress, with some participants reporting suicidal ideation. Five core themes emerged: emotional burden, social support and resilience, spirituality, stigma and guilt, and financial strain with limited healthcare access. Participants with both type 1 and type 2 diabetes experienced psychosocial challenges; however, individuals with type 2 diabetes more frequently described hopelessness, stigma, and suicidal ideation related to disease progression and financial burden, whereas participants with type 1 diabetes emphasized lifelong disease management and misunderstanding of their condition. Social support and spirituality served as important coping resources. These findings highlight the need for culturally sensitive and integrated diabetes care that addresses both physical and mental health needs in underserved communities.
Keywords
Introduction
Diabetes, a chronic health condition affecting millions worldwide, has profound implications for both physical and psychological health (Duncan et al., 2025; Sun et al., 2022). Among its most challenging consequences is the high prevalence of psychological distress, including suicidal ideation, particularly among individuals with type 1 and type 2 diabetes (Fan et al., 2024). While the medical community has made significant strides in understanding the physiological management of diabetes, there is a growing recognition of the need to address the mental health burdens that accompany these conditions (Ceriello et al., 2022; Romadlon et al., 2024).
In this study, psychosocial experiences refer to the ways in which individuals perceive, respond to, and manage the interaction between psychological factors (such as emotions, distress, and coping) and social contexts (including family support, cultural beliefs, and community environments) in the course of living with diabetes (James et al., 2023; Upton, 2020). This concept encompasses psychosocial distress, suicidal ideation, coping mechanisms, social support, and the broader social and cultural influences that shape individuals’ lived experiences.
People living with diabetes, especially in rural and underserved regions, face unique challenges that exacerbate feelings of isolation, hopelessness, and despair (Foss et al., 2023; Romadlon et al., 2026a). These challenges include the demanding nature of daily self-management (e.g. blood glucose monitoring, medication adherence, and dietary restrictions), fear of acute and long-term complications, financial burden of ongoing treatment, and the cumulative psychological strain associated with managing a lifelong condition (Gupta et al., 2024). Rural areas often present additional barriers to mental health care, including limited access to healthcare services, cultural stigma surrounding mental health, and economic stressors (Coombs et al., 2022; Kavanagh et al., 2023). In such settings, the psychological impact of chronic conditions like diabetes may be underreported, leaving many individuals without adequate support or intervention (Kobo et al., 2022; Zhao et al., 2023).
Importantly, the experience of living with diabetes and its associated psychosocial distress is deeply shaped by cultural context. In many low- and middle-income countries, including Indonesia, health beliefs, social norms, and community structures strongly influence how individuals perceive illness, seek care, and cope with distress (Widayanti et al., 2019). Previous studies in similar cultural settings have shown that individuals often interpret chronic illness through a socio-religious lens, where health and illness are intertwined with spiritual meaning, moral responsibility, and communal expectations (Molla et al., 2025; Weber and Doolittle, 2023).
Research indicates that people with chronic health conditions, such as diabetes, are at heightened risk for mental health issues, including depression, anxiety, fatigue, and suicidality (Farooqi et al., 2022; Renaud-Charest et al., 2024; Romadlon et al., 2021). However, little is known about how these psychosocial challenges manifest in rural populations, where resources are limited and coping strategies are shaped by local cultural and religious practices. In the Indonesian context, spirituality and religion play a central role in daily life, particularly in rural communities where religious practices are closely integrated into social identity and support systems. Spiritual coping, such as prayer, religious rituals, and reliance on faith-based communities, has been identified as a key mechanism for managing emotional distress (Al Baqi et al., 2025). However, the meaning, expression, and impact of spirituality can differ significantly across cultural settings, making it essential to examine these factors within their specific sociocultural context.
Suicidal ideation, as a manifestation of profound psychological distress, remains a critical concern in diabetes care (Huang et al., 2022; Renaud-Charest et al., 2024). In rural settings, where the social fabric may be tight-knit yet secretive about mental health, individuals may experience a unique form of stigma that further isolates them and inhibits their ability to seek help (Foss et al., 2023). This is compounded by the cyclical nature of diabetes management, where physical health issues intersect with emotional struggles, creating a feedback loop of worsening health outcomes. Understanding the mechanisms by which individuals with diabetes cope with the challenges of their condition in rural settings is imperative for developing tailored interventions. Coping strategies, including social support, religious or spiritual beliefs, and community involvement, are critical factors that can mitigate the effects of mental health challenges associated with diabetes (Molla et al., 2025; Weber and Doolittle, 2023). However, the effectiveness and meaning of these coping strategies are likely influenced by cultural norms, belief systems, and local healthcare contexts, which remain underexplored in many rural and underserved populations.
Given these gaps, further research is needed to better understand how individuals in rural and underserved settings experience and cope with the psychological and social challenges of living with diabetes. This study aimed to explore psychosocial experiences, including suicidal ideation and coping mechanisms, among individuals living with type 1 and type 2 diabetes in rural and underserved areas. By situating this inquiry within the Indonesian cultural context, this study aims to provide culturally grounded insights into how individuals interpret and manage both the physical and psychological burdens of diabetes. By examining these lived experiences, the research aimed to illuminate the hidden burdens of managing diabetes in rural settings and to inform more effective, culturally relevant mental health interventions.
Methods
Study design and setting
A qualitative approach using semi-structured in-depth interviews was adopted to gain detailed insights into participants’ lived experiences. The study was conducted from February to November 2025 in several rural communities located in Java and Sumatra, Indonesia, where healthcare resources were limited, and cultural barriers to mental health support were prevalent. The study was conducted in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ; Tong et al., 2007).
Sample selection and sample size calculation
A total of 30 participants were included in the study, comprising 10 individuals diagnosed with type 1 diabetes and 20 individuals with type 2 diabetes. The distribution of participants was guided by the higher prevalence of type 2 diabetes in the general population, as well as the aim to capture a broader range of psychosocial experiences across different diabetes types. Eligibility for the study required participants to be adults aged 18 years and older, diagnosed with either type 1 or type 2 diabetes for a minimum of 1 year, and residing in rural or underserved areas with limited access to specialized diabetes care. Additionally, participants had to be willing to participate in in-depth interviews exploring psychosocial experiences, coping strategies, and suicidal ideation.
Participants were recruited using purposive sampling in collaboration with local healthcare providers, including primary care clinics and community health workers in rural and underserved areas. Recruitment was conducted through referrals and direct invitations to eligible individuals who met the inclusion criteria. This approach aimed to ensure variation in participant characteristics, including type of diabetes, age, gender, and socio-economic background.
Basic demographic and background information, including family support and healthcare access, were collected using brief structured questions prior to the interviews and categorized for descriptive purposes.
Individuals with severe cognitive impairments or those receiving active psychiatric treatment that could affect their ability to participate in the study were excluded. By using thematic saturation as the guiding principle for determining the sample size, a sample of 30 participants was deemed sufficient to capture the rich, in-depth data required for this qualitative study (Guest et al., 2006).
Data collection
Data collection was conducted through semi-structured in-depth interviews aimed at exploring participants’ lived experiences with diabetes, including their emotional and psychological responses, coping strategies, and experiences of suicidal ideation or self-harm. The interviews were guided by a structured interview guide (Supplemental Table 1) that was developed in consultation with diabetes care experts and psychosocial health experts to ensure clinical relevance and sensitivity to psychosocial issues.
The interviews were conducted by trained researchers (n = 2) with experience in qualitative research and psychosocial health. The guide included a combination of broad, open-ended questions and probing questions to facilitate an in-depth exploration of participants’ experiences. These questions were designed to encourage participants to reflect on both the emotional and practical aspects of living with diabetes in rural and underserved settings.
The interviews were conducted face-to-face by trained interviewers, ensuring that the participants felt comfortable and supported throughout the process. Each interview lasted between 45 and 60 minutes, and all interviews were audio-recorded with the participants’ consent. All interviews were conducted in Bahasa Indonesia, the native language of the participants, to facilitate comfortable communication and rich expression of experiences. The recordings were transcribed verbatim for analysis. In addition to the core interview questions, participants were encouraged to share any additional thoughts or experiences related to mental health, social support, or community involvement. The semi-structured nature of the interview allowed for flexibility, enabling participants to guide the conversation toward topics that they felt were most relevant to their experiences.
Data analysis
Data analysis was conducted using NVivo software (version 12), a robust tool designed for managing and analyzing qualitative data. The analysis followed the thematic analysis approach as outlined by prior guidelines (Braun and Clarke, 2006, 2024).
The transcription process was carried out by members of the research team (n = 2), and all transcripts were reviewed for accuracy before analysis. The researchers first familiarized themselves with the data by reviewing the transcribed interviews, which allowed them to gain an initial understanding of the content and context of the participants’ experiences. NVivo facilitated this process by helping organize the data into categories and subcategories.
All coding and theme development were conducted in Bahasa Indonesia to preserve linguistic nuances and cultural meanings embedded in participants’ narratives. Once the coding was completed, the researchers identified key themes that emerged from the data. These themes reflected common experiences and patterns regarding suicidal ideation, coping mechanisms, and psychosocial experiences in individuals with diabetes. The researchers interpreted these themes within the context of the rural setting, considering the influence of cultural, economic, and healthcare-related factors on participants’ experiences. Themes were selected based on their frequency, depth of discussion, and relevance to the study objectives.
For reporting purposes, selected participant quotations were translated into English by bilingual members of the research team. The translated excerpts were reviewed and discussed among the research team to ensure accuracy, consistency, and preservation of the original meaning. Any discrepancies were resolved through team discussion and consensus. This process also included member checking, where a subset of participants reviewed the preliminary results to confirm that the themes accurately reflected their experiences and that the findings resonated with them.
Data management and trustworthiness
To enhance the trustworthiness of the study, several strategies were implemented (Cypress, 2017; Guba and Lincoln, 1994; Lincoln and Guba, 1985). Data triangulation was conducted by comparing findings from the interviews with relevant literature and previous studies on diabetes and mental health, which supported the credibility of the results. Peer review was undertaken during the data analysis phase, whereby multiple researchers independently reviewed the coding and theme development to ensure consistency and reliability. An audit trail was maintained throughout the study, including detailed documentation of methodological decisions, data collection procedures, analytic steps, and interpretation processes. This approach ensured transparency and methodological rigor and allowed the research process to be systematically reviewed.
Ethical considerations
Ethical approval for this study was obtained from the Joint Institutional Review Board of the Ethical Committee of Medical Research at the Faculty of Dentistry, University of Jember (Approval No. 3633/UN25.8/KEPK/DL/2025). All participants gave written informed consent before taking part in the study, in full alignment with established ethical research standards. Participants were assured that their participation was voluntary and that they could withdraw from the study at any time without consequence. Additionally, all participants were provided with information about available mental health support services in case they experienced distress during or after the interview process. The confidentiality of participants was maintained throughout the study. All personal information and interview data were anonymized and stored securely to protect participants’ privacy.
Results
Demographic characteristics
Table 1 illustrates a diverse sample that captures the varied experiences of individuals living with diabetes in rural settings. The age range of participants spanned from 22 to 65 years, with both younger and older individuals included to provide a broader understanding of how age may influence the experience of managing diabetes. Participants with type 1 diabetes were generally younger (mean age of 47 years) compared to those with type 2 diabetes (mean age of 58 years), reflecting differences in current age at the time of data collection.
Participant demographics and background (N = 30).
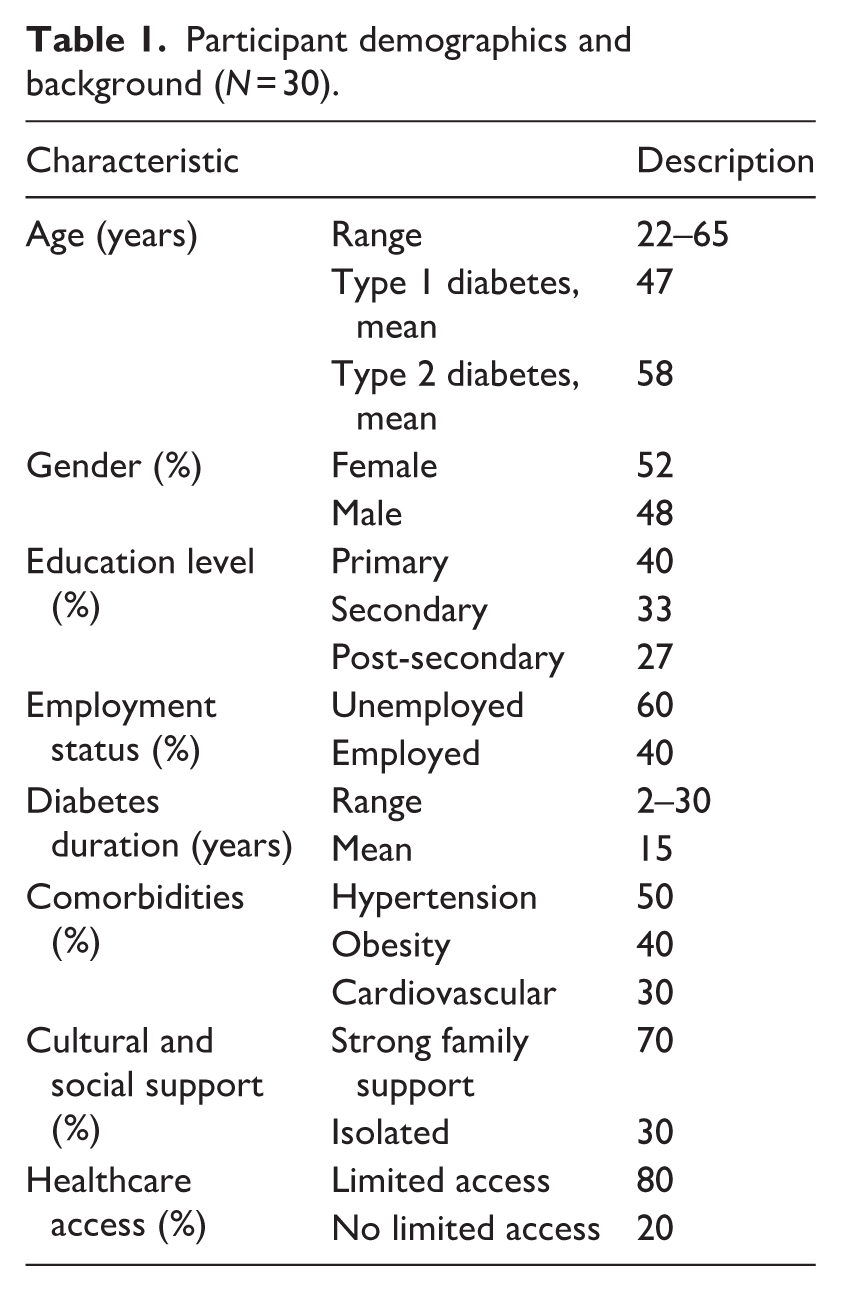
Gender distribution was nearly balanced, with 52% of participants identifying as female and 48% as male. Educationally, the majority had completed only primary or secondary education, which highlights the limited access to higher education in rural areas and potentially impacts their understanding of diabetes management and mental health. The sample revealed significant socio-economic challenges, with 60% of participants being unemployed or working in informal sectors, underscoring the economic hardships often faced in rural communities. Participants had been living with diabetes for a duration ranging from 2 to 30 years (mean = 15 years), indicating a substantial long-term disease burden.
Comorbidities, including hypertension (50%), obesity (40%), and cardiovascular conditions (30%), were commonly reported, with a greater burden observed among participants with type 2 diabetes, consistent with typical clinical patterns. Regarding social context, 70% of participants reported having strong family support, while 30% described experiencing isolation. In terms of healthcare access, 80% of participants reported limited access to healthcare services, highlighting structural barriers faced in rural and underserved settings. The purposive sampling strategy ensured diversity across diabetes type, gender, age, and socio-economic background, as reflected in Table 1.
Brief overview of psychosocial experiences
Participants described a wide range of psychosocial experiences related to living with diabetes in rural and underserved settings. Many expressed persistent emotional distress, including feelings of hopelessness, frustration, and loss of control, particularly when managing blood glucose levels and facing the risk of long-term complications. For some, these challenges were compounded by limited access to healthcare and support services, which intensified their sense of isolation. As one participant described, “Living with diabetes feels like a constant struggle every day” (Participant 1, Type 2 diabetes).
At the same time, participants highlighted various coping strategies and sources of resilience, including family support, spirituality, and personal adaptation to the demands of diabetes management. However, these experiences were shaped by broader social and structural factors, such as stigma, financial burden, and healthcare access. These initial patterns revealed the complex interplay between psychological, social, and contextual influences, which were further organized into the core themes presented below.
Core findings: Themes from participants’ lived experiences
The following core themes were identified as the most salient patterns across participants’ psychosocial experiences. These themes were derived inductively during the data analysis process and were selected based on their frequency, depth of discussion, and relevance to the study objectives (Table 2). Differences between participants with type 1 and type 2 diabetes emerged during analysis and are integrated within the themes where relevant. Each theme is presented with illustrative quotations to provide contextualized insights into participants’ lived experiences.
Core themes of psychosocial experiences among individuals with type 1 and type 2 diabetes in rural and underserved settings.
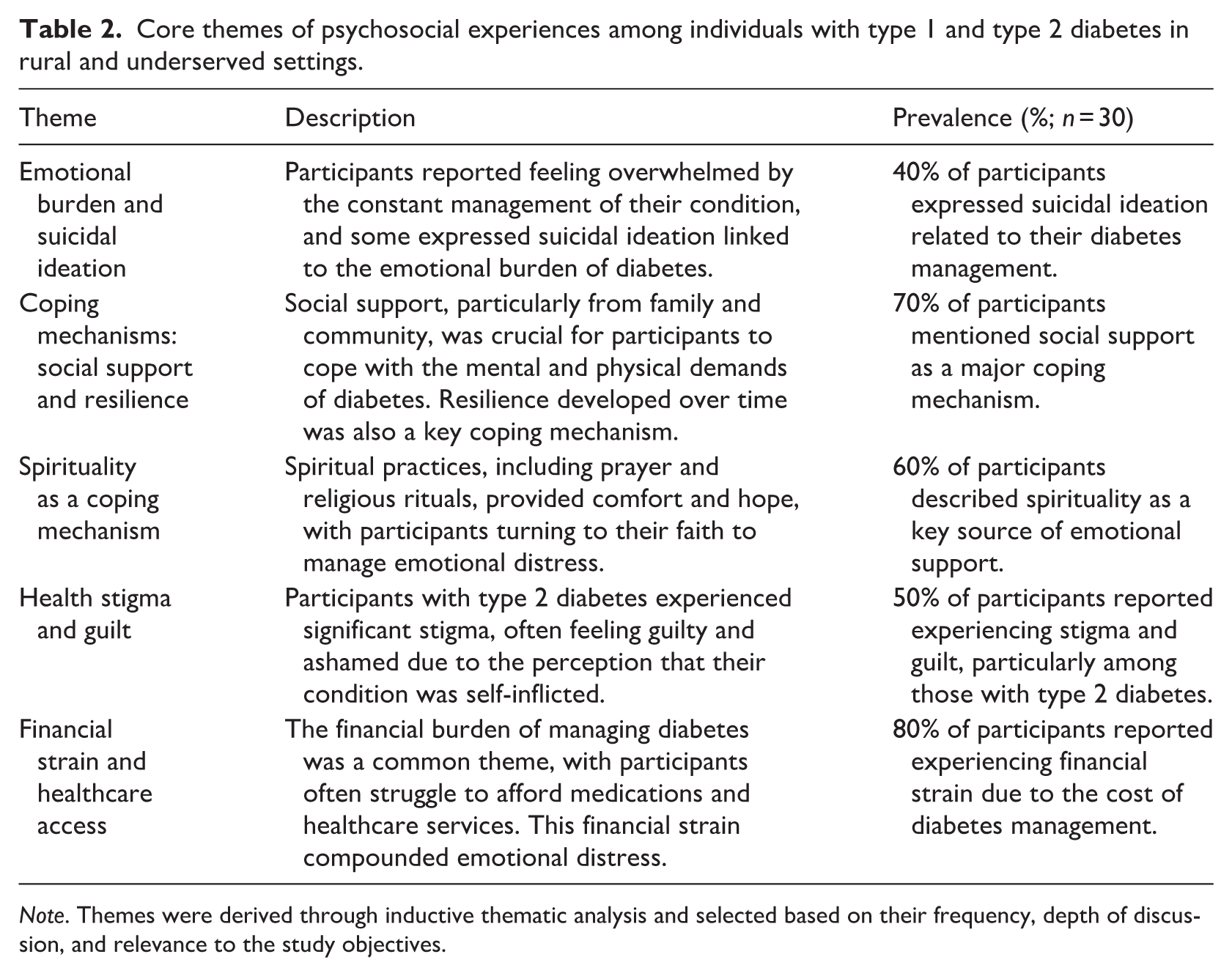
Note. Themes were derived through inductive thematic analysis and selected based on their frequency, depth of discussion, and relevance to the study objectives.
Emotional burden and suicidal ideation
A prominent theme was the emotional burden associated with managing diabetes, often leading to feelings of hopelessness and, in some cases, suicidal ideation. Emotional distress was reported by participants with both type 1 and type 2 diabetes. However, expressions of suicidal ideation and profound hopelessness were more frequently described among participants with type 2 diabetes, particularly those with longer disease duration, multiple comorbidities, and financial difficulties. Participants with type 1 diabetes more commonly described emotional exhaustion related to lifelong disease management and fear of future complications.
One participant shared, “When my blood sugar goes high, I feel like everything is out of control, and that makes me feel hopeless” (Participant 8, Type 2 diabetes).
Similarly, another participant expressed, “Sometimes I feel tired of fighting this disease every day. It feels like there is no end to it” (Participant 14, Type 2 diabetes).
A participant with type 1 diabetes also described the ongoing psychological burden of living with the condition: “Sometimes I feel mentally exhausted thinking that I will live with this condition for the rest of my life” (Participant 29, Type 1 diabetes).
For some individuals, particularly those with long disease duration and comorbidities, these feelings escalated into suicidal thoughts. As one participant described, “I feel like I’m just waiting for my body to give up on me, and I can’t see a way out” (Participant 19, Type 2 diabetes).
Coping mechanisms: Social support and resilience
Social support emerged as a key coping mechanism, particularly support from family and community members. Both participants with type 1 and type 2 diabetes emphasized the importance of family support in helping them manage emotional distress and maintain motivation for self-care. However, participants with type 2 diabetes more frequently described emotional dependence on family members due to worsening health conditions and financial burdens associated with long-term disease management. Participants with strong support systems reported greater emotional stability and motivation to manage their condition.
As one participant explained, “My family has always been my strength. They make sure I never feel like I’m alone in this fight” (Participant 3, Type 1 diabetes). Similarly, another participant noted, “When I feel weak, my family reminds me to keep going. Without them, I don’t think I could manage this disease” (Participant 11, Type 2 diabetes).
In contrast, participants with limited support described feelings of isolation and emotional exhaustion. One participant shared, “Sometimes I feel like I have to handle everything alone, and it becomes too overwhelming” (Participant 6, Type 2 diabetes). Over time, some individuals developed personal resilience through self-management strategies and adaptation to their condition.
Spirituality as a coping mechanism
Spirituality played a significant role in helping participants cope with emotional distress. Spiritual coping strategies were reported by participants with both type 1 and type 2 diabetes and appeared to provide emotional comfort regardless of diabetes type. In many cases, spirituality helped participants develop acceptance, hope, and emotional resilience in living with a chronic illness. Religious practices such as prayer and faith-based activities provided comfort and a sense of meaning. One participant stated, “Whenever I feel down, I pray, and it gives me strength to face another day” (Participant 15, Type 2 diabetes).
Another participant reflected, “I believe this illness is part of God’s plan, and that belief helps me stay strong” (Participant 9, Type 1 diabetes). This coping strategy was particularly prominent in rural communities, where religious beliefs are deeply integrated into daily life.
For some participants, spirituality also reduced emotional distress by fostering acceptance and hope in the face of chronic illness. This highlights the role of culturally embedded coping strategies in shaping psychosocial experiences in rural contexts.
Health stigma and guilt
Stigma was a major psychosocial challenge, especially among participants with type 2 diabetes. Many participants reported feeling judged or blamed for their condition, which contributed to guilt and reduced self-esteem. A participant noted, “People think diabetes is something I did to myself. . . it makes me feel ashamed” (Participant 21, Type 2 diabetes).
Another participant shared, “Sometimes I feel embarrassed to tell others about my condition because they might blame me” (Participant 17, Type 2 diabetes).
In contrast, participants with type 1 diabetes experienced stigma differently, often related to misunderstanding of their condition. As one participant explained, “People don’t understand that I didn’t cause this. They think all diabetes is the same” (Participant 4, Type 1 diabetes).
While both groups experienced stigma, participants with type 2 diabetes more frequently internalized blame and guilt associated with lifestyle perceptions and social judgment. In contrast, participants with type 1 diabetes more commonly described frustration related to public misunderstanding and lack of awareness regarding the nature of their condition. These differences highlight how stigma was experienced and interpreted differently across diabetes types.
Financial strain and healthcare access
Financial burden and limited healthcare access were significant challenges affecting both diabetes management and mental well-being. Participants with both type 1 and type 2 diabetes described financial difficulties related to ongoing treatment and healthcare access. However, participants with type 1 diabetes more frequently emphasized difficulties obtaining insulin and maintaining continuous treatment, whereas participants with type 2 diabetes more commonly discussed the cumulative economic burden associated with long-term complications, medications, and comorbid conditions. Participants reported difficulty affording medications and traveling long distances for care. One participant shared, “I sometimes have to choose between buying food and getting my insulin” (Participant 12, Type 1 diabetes).
Another participant noted, “The cost of treatment is very high, and it adds stress to my daily life” (Participant 23, Type 2 diabetes). Geographical barriers also limited access to healthcare services. As one participant explained, “The clinic is very far, and sometimes I cannot go regularly, even when I need help” (Participant 5, Type 2 diabetes). These structural challenges contributed to delayed care, emotional distress, and worsening health outcomes, particularly in rural and underserved settings.
Discussion
The findings of this study provide a nuanced understanding of the psychosocial experiences of individuals with type 1 and type 2 diabetes in rural and underserved settings. Consistent with the core themes identified in the Results, participants’ experiences were shaped by a complex interplay of emotional burden, coping mechanisms, cultural influences, stigma, and structural barriers.
A key finding of this study was the significant emotional burden and presence of suicidal ideation among participants with both type 1 and type 2 diabetes, although these experiences were more prominently expressed among individuals with type 2 diabetes and those with long disease duration. Participants with type 1 diabetes more commonly described emotional exhaustion related to lifelong self-management and fear of future complications, whereas participants with type 2 diabetes more frequently reported hopelessness associated with disease progression, financial strain, and comorbidities. These findings are consistent with existing research that underscores the profound psychological impact of living with a chronic illness like diabetes (Khunti et al., 2023; Sun and Li, 2023). The cyclical relationship between poor glycemic control, emotional distress, and hopelessness observed in this study highlights the need for integrated psychological support within diabetes care (Mashfufa et al., 2026; Pratama et al., 2026). In rural settings, where access to mental health services is limited, this burden may be further intensified (Prathiksha et al., 2024).
Social support emerged as a key coping mechanism, echoing findings from prior studies that emphasize the importance of familial and community-based support systems (Da Moura Semedo et al., 2023). Participants who reported strong social support networks, particularly from family, showed better emotional resilience and coping capabilities. Although social support was valued across both groups, participants with type 2 diabetes more frequently described dependence on family support due to worsening physical health and economic challenges associated with long-term disease management. However, this support was not universally available, with some participants feeling isolated and unsupported in their diabetes journey. The lack of structured mental health resources in rural communities also contributed to feelings of helplessness and despair, which aligns with prior research indicating that individuals with chronic conditions in rural areas often experience barriers to accessing comprehensive care (Zhao et al., 2023). This variation highlights the critical role of social environments in shaping psychosocial experiences and underscores the need for community-based support interventions.
In addition, spirituality emerged as an important culturally embedded coping strategy across both diabetes groups. Regardless of diabetes type, religious beliefs and practices provided participants with emotional comfort, acceptance, and hope in coping with chronic illness. In the context of rural Indonesian communities, religious beliefs and practices provided meaning, comfort, and emotional regulation for many participants (Al Baqi et al., 2025). This finding highlights the importance of integrating culturally sensitive and faith-informed approaches into psychosocial and diabetes care interventions, as spirituality can serve as both an emotional resource and a framework for coping with chronic illness.
In exploring the role of cultural beliefs and stigma, this study reinforces the significant impact that societal perceptions have on the management of chronic health conditions. Participants with type 2 diabetes, in particular, reported experiencing guilt and shame due to the stigma associated with their condition. This is consistent with previous findings, which noted that the perception of self-inflicted illness contributes to negative mental health outcomes, including depression and anxiety (Farooqi et al., 2022; McInerney et al., 2022). Differences between type 1 and type 2 diabetes participants further highlight how stigma is socially constructed and experienced differently across conditions. Participants with type 2 diabetes more frequently internalized blame associated with lifestyle-related assumptions, whereas participants with type 1 diabetes described frustration related to public misunderstanding and lack of awareness regarding their condition. The stigma surrounding both diabetes and mental health in rural settings compounds the psychological distress experienced by individuals, making it even more difficult for them to seek help or engage in diabetes management programs.
To address these challenges, several strategies may be considered to reduce stigma in rural and underserved settings. Community-based education programs that increase awareness of diabetes as a complex chronic condition, rather than a result of personal failure, may help shift public perceptions and reduce blame (Dietz et al., 2023). Integrating mental health services into routine diabetes care, particularly within primary healthcare settings, can also normalize psychological support and reduce barriers to seeking help (Sachar et al., 2023). In addition, peer support programs, including group-based interventions or community-led support networks, have shown promise in creating safe spaces for individuals to share experiences and reduce feelings of isolation and stigma (Romadlon et al., 2026b).
Importantly, culturally sensitive approaches are essential. In rural Indonesian contexts, where religion and community structures play a central role, involving religious leaders and community figures in health promotion efforts may enhance acceptance and effectiveness (Al Baqi et al., 2025). Faith-based initiatives and community dialogs can help reframe mental health struggles as common and manageable experiences, thereby reducing stigma and encouraging help-seeking behaviors. These approaches align with emerging evidence highlighting the effectiveness of culturally grounded and community-driven interventions in addressing stigma in low-resource settings. Addressing these cultural and social barriers is critical for reducing the stigma associated with both chronic illness and mental health, and for encouraging individuals to seek the support they need without fear of judgment.
Finally, the findings emphasize the role of financial strain and limited healthcare access as structural barriers shaping psychosocial experiences. Many participants struggled with the high cost of medications and healthcare services, although the nature of these financial challenges differed between groups. Participants with type 1 diabetes more frequently emphasized concerns regarding insulin access and continuity of treatment, whereas participants with type 2 diabetes described the cumulative burden of medications, complications, and comorbid conditions. This aligns with prior research highlighting how economic burden contributes to health inequities in rural populations (Butt et al., 2024). These findings suggest that addressing psychosocial challenges requires not only individual-level interventions but also systemic changes to improve healthcare accessibility and affordability.
Overall, while participants with both type 1 and type 2 diabetes shared common experiences of emotional distress, healthcare barriers, and reliance on social and spiritual coping mechanisms, important differences also emerged. Participants with type 2 diabetes more frequently described stigma, financial burden, and suicidal ideation associated with disease progression and social blame. In contrast, participants with type 1 diabetes more commonly emphasized the psychological exhaustion of lifelong disease management and frustration related to misunderstanding of their condition. These findings highlight the importance of considering both shared and condition-specific psychosocial needs when developing culturally sensitive interventions for individuals living with diabetes in rural settings.
Strengths and limitations
This study’s qualitative design provides a rich, in-depth exploration of the psychosocial experiences of individuals with type 1 and type 2 diabetes in rural and underserved areas. The focus on lived experiences offers valuable insights into the emotional and psychological challenges faced by participants, which are often not fully captured in quantitative studies. Furthermore, the inclusion of both type 1 and type 2 diabetes participants in rural settings, where healthcare access and social support are often limited, enhances the relevance of this study for informing care in similar underserved contexts. The use of in-depth interviews and thematic analysis also strengthens the credibility of the findings by allowing participants to express their experiences in their own words and enabling the identification of meaningful patterns across cases.
Several limitations should be considered. First, the study relied on self-reported data, which may introduce bias due to social desirability or recall inaccuracies. Second, the findings are context-specific to rural and underserved settings in Indonesia, and cultural factors may influence how psychosocial experiences are perceived and expressed. Therefore, caution is warranted when transferring these findings to other settings with different cultural or healthcare contexts.
Conclusion and implications
Living with type 1 and type 2 diabetes in rural and underserved areas presents significant psychosocial challenges, including both shared and condition-specific emotional burdens. Participants reported emotional distress, suicidal ideation, and difficulty coping due to the compounded impact of limited healthcare access and social stigma. While individuals with type 2 diabetes more frequently described hopelessness, stigma, and financial strain associated with disease progression, participants with type 1 diabetes more commonly emphasized the lifelong psychological burden of diabetes management and misunderstanding of their condition. The findings emphasize the crucial role of social support and spirituality in managing these struggles, while also underscoring the need for greater integration of mental health care into diabetes management. To improve outcomes, it is essential that interventions not only address the medical needs of individuals with diabetes but also provide psychological support and combat the stigma surrounding both chronic illness and mental health. Enhancing access to specialized care and building community-based support systems will be key to improving the overall well-being of individuals in these underserved settings.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261462452 – Supplemental material for Rural realities: Exploring suicidal ideation and coping mechanisms among people with type 1 and type 2 diabetes in underserved areas
Supplemental material, sj-docx-1-hpq-10.1177_13591053261462452 for Rural realities: Exploring suicidal ideation and coping mechanisms among people with type 1 and type 2 diabetes in underserved areas by Mario Pratama, Safiruddin Al Baqi, Rudy Kurniawan, Khalood Al-Abri, Emmanuel Ekpor and Debby Syahru Romadlon in Journal of Health Psychology
Footnotes
Ethical considerations
The study received ethical approval from the Joint Institutional Review Board of the Ethical Committee of Medical Research at the Faculty of Dentistry, University of Jember (Approval No. 3633/UN25.8/KEPK/DL/2025).
Consent to participate
All participants provided written informed consent before participating in the study.
Consent to publication
Participants provided consent for the anonymized publication of the findings in scientific journals.
Author contributions
MP: Writing – original draft, Writing – review & editing, Methodology, Formal analysis, Data Curation, Project administration, Funding acquisition, Conceptualization. SAB: Writing – review & editing, Methodology, Supervision, Data curation. RK: Writing – review & editing, Methodology, Supervision, Data curation. KAA: Writing – review & editing, Methodology. EE: Writing – review & editing, Methodology. DSR: Writing – original draft, Writing – review & editing, Supervision, Formal analysis, Data Curation, Project administration, Funding acquisition, Conceptualization.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This Research is funded by Thailand Science Research and Innovation Fund Chulalongkorn University (HEA_FF_69_217_3600_004) to DSR.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.*
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.