
Abstract
This article focuses on the everyday materialities of polycystic ovary syndrome (PCOS) (currently being renamed to polyendocrine metabolic ovarian syndrome). A PCOS is a combination of symptoms that vary from patient to patient, such as absent or irregular ovulation and menstruation, impaired glucose metabolism, excessive body hair or problems with fertility. This article adds to research on menstrual health and chronic disease, which has tended to prioritise tracking technologies and medical devices, by drawing attention to ordinary material objects. Drawing on Science and Technology Studies theorisations of disease and self-care, this article examines in-depth semi-structured interviews with people with PCOS to illuminate how materiality shapes everyday coping with this common yet diverse condition. The major finding of the analysis is that although medical professionals frame PCOS as a coherent whole, patients attend to their individual ‘packs’ of symptoms in their daily efforts to manage the condition.
Introduction
Polycystic ovary syndrome, abbreviated as PCOS, is a common condition. It affects 5–20% of women and persons assigned female at birth worldwide (Hachey et al., 2020). A PCOS is often connected to reduced fertility and a greater risk of developing health issues related to metabolism and blood sugar, such as prediabetes and type 2 diabetes. To receive a PCOS diagnosis, a patient needs to meet three criteria: elevated levels of androgens (‘male’ hormones including testosterone), missing or irregular menstruation, and the presence of ‘cysts’, or more precisely, antral follicles that did not reach the stage of ovulation, on the ultrasound image (Williams, 2016, 107–109). In addition to posing long-term health risks, PCOS affects the everyday lives of a significant portion of the world's population through symptoms such as excess body hair and facial hair, acne, dark patches on skin, balding, fatigue and gastrointestinal issues (Mousa et al., 2023).
A PCOS has been a subject of social science research for more than two decades. Medical sociologists, anthropologists and gender studies scholars have examined various aspects of living with PCOS, including stigma and the frustration of not conforming to normative femininity (Kitzinger and Willmott, 2002), the invisibility and fat shaming of people with PCOS (Fisanick, 2005, 2009); patients’ agency and expertise in contrast to health professionals’ neglectful attitudes (Ellerman, 2012), the ecological, social and economic contexts shaping PCOS prevalence (Pathak, 2015, 2018, 2020, 2021; Pathak and Nichter, 2015) and practices of self-care (Vleming, 2018). This article offers a new theoretical perspective by focusing on materiality. While scholars of medical humanities do not offer a uniform definition of materiality, they emphasise the interrelation of tangible qualities of bodies and various objects that interact with these bodies (Carroll and Parkhurst, 2019; Fox, 2016, 67). These tangible qualities, such as weight, texture, temperature, size or colour, affect social relations of the patients, their feelings and values (Carroll and Parkhurst, 2019). Rather than a background for a patient's lived experience, materiality is a constitutive part of this experience. This profound role of materiality is especially characteristic of chronic diseases that affect the patients’ lives beyond clinical settings.
Everyday uses of objects, substances and technologies for coping with chronic disease have been addressed in the literature in sociology, anthropology, Science and Technology Studies (STS), Human–Computer Interaction (HCI) and design research from the last two decades (Aarhus and Ballegaard, 2010; Arteaga, 2019; Berk, 2018; Binnie et al., 2021; Chamberlain et al., 2017; Craig and Chamberlain, 2017; Danholt and Langstrup, 2012; Horrocks, 2019; Langstrup, 2008; Nunes and Fitzpatrick, 2018; Paterson et al., 2017; Prendiville, 2017; Wada and Wallace, 2022; Wainwright, 2018; Weiner and Will, 2018). These studies showed that materiality can support patients’ emotional adaptation to their post-surgery limitations (Arteaga, 2019), shape patients’ agency through ‘intra-actions’ between bodies and medical devices (Berk, 2018) or enhance one's sense of safety and well-being despite pain and discomfort (Binnie et al., 2021). The view of materiality as interconnected with human feelings and relationships permits sidestepping the traditional dichotomy in medical sociology and anthropology that separates ‘disease’ (a biological reality) from ‘illness’ (subjective experience), or a tripartite model that adds ‘sickness’ (the social reaction to illness) (Eisenberg, 1977; Kleinman, 1978; Mol, 2002, 9–10; Fox, 2011, 365). Materiality interconnects bodily physical processes with emotions and social relations.
The materiality of PCOS is distinctive because it is not organised around a single, condition-specific medical object such as a stoma bag, an insulin pump or an oximeter. To date, there is no dedicated medical device or medication that directly targets the underlying biological processes of PCOS, although a PCOS-specific pharmaceutical is currently in clinical trials (Garcia-Beltran et al., 2023). Therefore, the treatment of this condition heavily relies on lifestyle interventions, including diet, physical activity, relaxation techniques and skincare. These interventions involve a variety of non-medical objects: from lunchboxes to fitness balls, from tweezers to hot bottles. While these objects are familiar to people without PCOS, those with the condition use them in distinctive combinations and for particular purposes. This article brings to light the uses of commodities by PCOS patients, focusing on tangible objects and substances, such as pharmaceuticals, rather than on mobile applications or social media. Although digital tools play an important role in the everyday lives of people with PCOS, and they have their own materiality (Clark and Lupton, 2023; Kragh-Furbo et al., 2018), I chose to address them in a separate article (Karpova, 2025).
In what follows, I introduce the theoretical premise of my fieldwork, namely, the multiplicity of PCOS profiles. Afterwards, I outline the scope of my fieldwork along with the theoretical framework and methodology used to analyse the data. I then introduce the three themes generated through the thematic analysis and examine each in detail. In conclusion, the article discusses how the findings show, first, that materiality is central to the varied lived experience of PCOS and, second, that people with PCOS use material objects with the focus on their specific sets of systems rather than on the diagnosis as a whole.
Before proceeding to discuss the theoretical background, a note about terminology is in order. Just when I received the final decision on the paper from the editor, The Lancet announced the official renaming of PCOS to PMOS: polyendocrine metabolic ovarian disorder (Teede et al., 2026). The renaming was a result of a long international and interdisciplinary consensus process involving clinical researchers, practising physicians, patients, policymakers and activists. A ‘PCOM’ more accurately reflects the complex nature of the syndrome, and it promises to optimise and shorten diagnostic procedures and bring forward the improvement of treatment and patients’ well-being (May et al., 2026). While appreciating the renaming as an important landmark, I chose to stay with the old name, as it was used in my fieldwork and my informants’ responses. The universal introduction of the new name will be a long process, and I will use ‘PCOS’ in this article for clarity and out of respect for my informants' life experience associated with this term.
Multiple symptom packs
Medical researchers suggested identifying different PCOS phenotypes according to the set of symptoms, such as irregularities of the menstrual cycle, insulin resistance (lowered sensitivity of the body's cells to insulin), body mass index or dermatological problems (Mumusoglu and Yildiz, 2020; Myers et al., 2023). The great variability of PCOS was the major inspiration for my fieldwork research, and I borrowed the concept of a ‘multiple body’ as a key theoretical tool. This concept originates from a landmark work by philosopher Annemarie Mol, in which she uses atherosclerosis of the lower limbs as a case study, demonstrating how medical practices can contribute to the development of diseases (Mol, 2002). Instead of arguing that atherosclerosis is a social construct, a product of different perspectives (the doctors’, the patients’, the Big Pharma's, etc.), Mol relied on the material semiotics approach, popular in STS (Law, 2008), which focuses on practices that shape, or ‘enact’, different realities, including social relations and material objects. Mol demonstrated how different forms of atherosclerosis are enacted in the hospital through practices such as interrogating the patients in a consultation room, surgery to widen arteries or ultrasound. Accordingly, atherosclerosis manifests as pain in the lower limbs, thickening of the innermost layer of arteries or reduced blood flow in the arteries. Different machines and instruments, such as a Doppler apparatus, surgical needles and catheters, enact ‘various atheroscleroses’ (Mol, 2002, 87). Likewise, different forms of PCOS are enacted through practices such as collecting a patient's blood at a GP office and testing the blood samples in a laboratory, evaluating the amount of facial and bodily hair by a GP or a gynaecologist, interrogation of a patient about their menstrual patterns and transvaginal ultrasound. As a result, in different clinical settings, PCOS appears as irregular menstrual cycle, excess hair on the body or face, elevated testosterone in the blood serum, multiple antral follicles (‘cysts’) visible on an ultrasound image of the ovaries or reduced fertility. At the same time, there are medical practices that aim at coordinating different versions of a disease into a more or less coherent whole. For example, professional medical organisations, by publishing diagnostic criteria, bring together different symptoms into a single diagnosis. In the case of PCOS, the three Rotterdam Criteria, accepted in 2003, brought together elevated testosterone, irregular menstruation and ‘12 or more follicles measuring 2–9 mm in diameter and/or an ovarian volume greater than 10 mL in at least one ovary’ under a single diagnosis (Mousa et al., 2023).
However, because only two of the three Rotterdam criteria are enough to give the PCOS diagnosis, people diagnosed with PCOS have different combinations of criteria and symptoms. One of my informants, Karolina, talked about different ‘symptom packs’ that people with PCOS get: for example, she does not experience fast weight gain and is therefore spared from weight stigma and body shaming but she had problems with fertility and dealt with excessive facial hair. A PCOS can be conceptualised as a ‘multiple disease’ not only within one patient's body (when it can be at once ‘follicles on an ultrasound’, ‘subfertility’ and ‘facial hair’) but also across bodies. The HCI scholar Sarah E. Fox and her colleagues relied on Mol's theorisation in presenting menstruation as a ‘multiple object’ that is constituted by concrete sensemaking practices of different people, such as attending to one's bodily experiences, tracking them in mobile apps, observing the diminishing frequency of menstruation during gender-affirming hormonal therapy or sharing the experience of menstrual pain on social media (Fox et al., 2020). A disease can also be multiple across bodies: Mol gave an example of atherosclerosis patients who did not feel any leg pain despite severe narrowing of their arteries, whereas other patients endured leg pain every day (Mol, 2002: 15–16; 65). When announcing the diagnosis, a doctor presents the disease as a coherent whole with clearly defined treatment recommendations. As a team of STS scholars drawing on Mol's work suggests, diagnostic procedures ‘prompt particular understandings of the body and delineate potentially problematic areas that require treatment, surveillance and management’ (Gardner et al., 2011: 844). Receiving the PCOS diagnosis can orient the patient towards everyday practices for treating symptoms, such as dieting or exercising. Hypothetically, however, the patients adjust these requirements to their specific ‘symptom packs’. I employ the notion of the multiplicity of diseases and bodies to better understand the roles of materiality in everyday lives with PCOS.
Apart from ‘multiplicity’, I employ two other concepts from STS, ‘self-care’ and ‘tinkering’: both were actively used by Mol and her colleagues in studies of disease, disability, elderly care and other areas of care (Mol et al., 2010). Furthermore, I rely on the studies of temporality in chronic disease and disability and the concepts ‘crip time’ (Kafer, 2013) and ‘endo time’ (Williams et al., 2025) to speak about ‘PCOS time’ and how materiality structures the rhythm of the everyday lives of my informants. In addition, I invoke phenomenological theorisations of chronic shame (Dolezal, 2015) and sensorimotoric perception (Arteaga, 2019; Warnier, 2001) in my analysis of coping with shame in PCOS.
Data and methodology
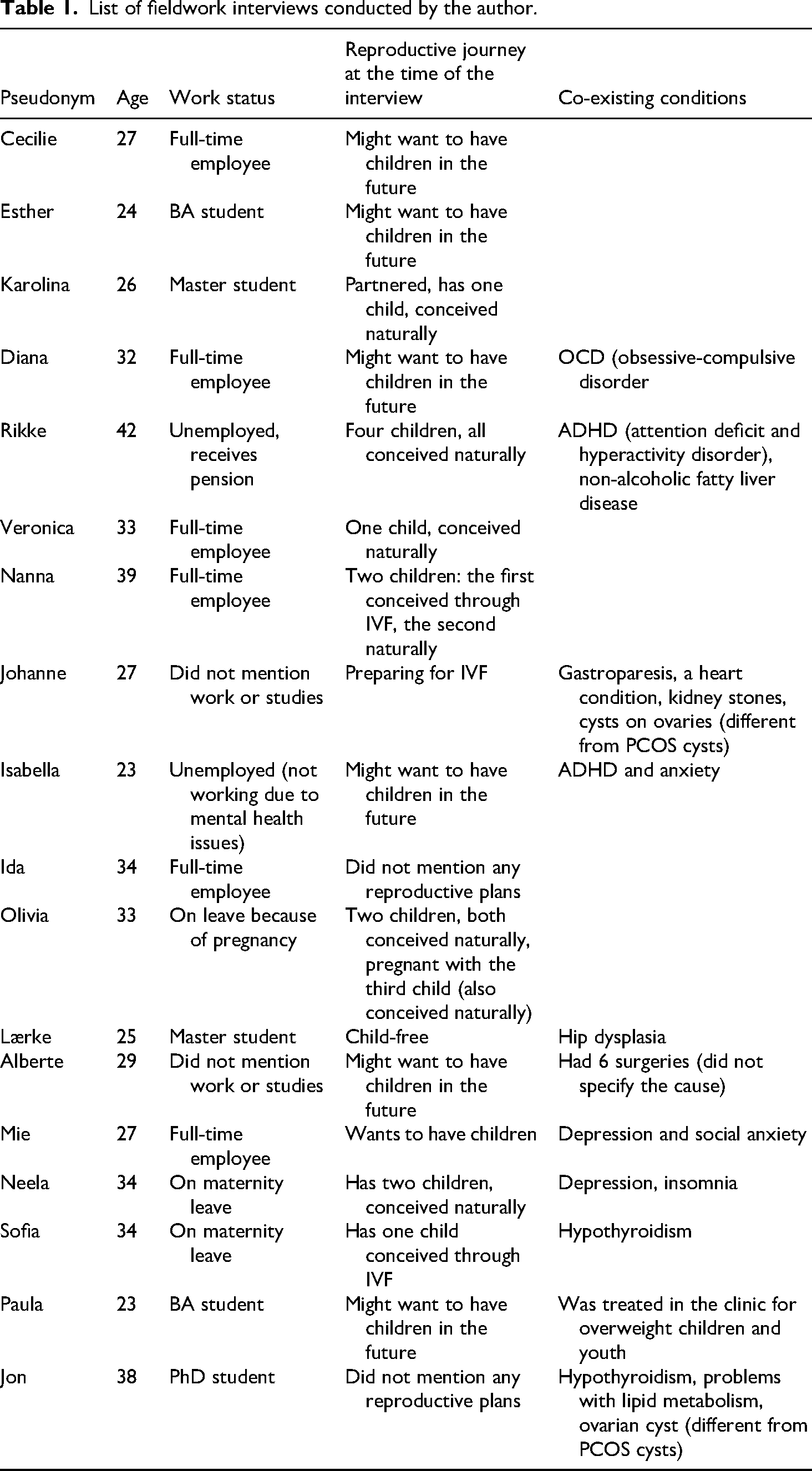
My empirical material consists of eighteen semi-structured in-depth interviews with people diagnosed with PCOS, aged 23–42: 17 women and 1 transgender man (see Table 1). The interviews with women were conducted from February to November, 2023. There were two criteria for selecting the respondents: having a PCOS diagnosis and experience with the Danish healthcare system in relation to this diagnosis. I recruited my respondents from Danish-language social media communities: a closed support group on Facebook and a closed community managed by an Instagram influencer. This made it possible to locate participants who are actively interested in knowing more about and managing their PCOS better. It also led to a relatively homogeneous sampling: all my participants at this point were middle-class cisgender women, all but two were white, and all but three were ethnic Danes. Sixteen interviews were conducted in person in different areas of Denmark, and one via a video call, all in English. Later, in the spring of 2025, I met a transgender man with PCOS through a personal contact. Although he lives in another Western European country and has never resided in Denmark, I chose to interview him because his experience shows both notable parallels and important contrasts with those of the other respondents, adding valuable nuance to my fieldwork data. I interviewed him via a video call, in Russian, in June 2025 (I translated the quotes from his interview myself). The fieldwork was approved by the Research & Innovation Organisation at the University of Southern Denmark, and all participants provided informed consent. The participants were pseudonumised. Table 1 presents the list of pseudonyms and personal details that can influence everyday life with PCOS: age at the time of the interview, employment status, reproductive plans or experience as well as comorbidities.
List of fieldwork interviews conducted by the author.
During interviews, I attentively listened to how my informants spoke about using pharmaceuticals, food-cooking utensils, sports equipment and other material items. Most of the interviews were conducted face-to-face in informants’ homes, which enabled them to discuss these everyday objects while looking at them and showing them to me. In this way, interviews became sensory events (Pink, 2015): informants could recall sensory experiences and tell stories about familiar objects in the comfort of their homes.
Upon completing the fieldwork, I transcribed the interviews verbatim and conducted a thematic analysis of the interview transcripts. I followed the guide on conducting thematic analysis proposed by Victoria Braun and Virginia Clarke: transcribing the interviews, coding the transcripts manually, collating the codes into themes, making a thematic map, checking the relevance of the themes against the entire data set and revising the thematic maps several times while re-reading the transcripts (Braun and Clarke, 2006). I used the theoretical approach to thematic analysis: while coding the transcripts, I proceeded from the conceptualisation of PCOS as a multiple object across bodies, outlined in the previous section. In other words, I coded for the specific research question: ‘How does materiality shape the lived experience of the multiple versions of PCOS?’ The resulting themes can be characterised as ‘latent’, that is, focused on the ideas and assumptions that shaped the semantic content of the data. Braun and Clarke suggest that an analyst should choose an epistemological position: whether essentialist or constructivist (Braun and Clarke, 2006: 83–85). In my analysis, however, I relied on new materialist premises about the interconnection and mutual configuring of reality and language, nature and culture, and therefore bypassed this choice. Instead of considering my informant's narratives as either directly reflecting their experience or produced by social context, I viewed the interviews as stories about multiple versions of PCOS that are enacted through the materiality of bodies and objects in everyday life.
In the latest revision of my thematic map, the following themes were generated: self-care, time and shame. These themes relate to different aspects of materiality, such as routine use of objects, wondering about the changes in the physical qualities of one's body over time or coordinating the material qualities of different objects to affect the biological functioning of the body. In the next sections, I will analyse each of the themes in detail.
Self-care
Care and self-care have been conceptualised across a wide range of scholarly disciplines, from moral philosophy to STS, and they play a central role in debates about both gender and health. Social policy scholar Lizzie Ward traces how the notion of ‘self-help’, originally advanced by feminists in the 1970s and 1980s to challenge the medicalisation of women's bodies, was later co-opted by restructured healthcare systems unable to provide adequate care. ‘Self-care’ as an individual responsibility for one's well-being emerged from this co-optation, a trend that became especially pronounced after the 2008 financial crisis (Ward, 2015). In this sense, ‘self-care’ aligns with Foucault's concept of the ‘care of the self’, a set of ascetic practices directed at achieving idealised states such as happiness or purity (Foucault 1997, 225). Yet self-care cannot be reduced to a forced adaptation to shrinking welfare states, and it retains a liberatory potential. As anthropologists Rosenbaum and Talmor (2022: 367) observed, self-care is ‘a polysemous term, capacious enough to hold multiple – often oppositional – worldviews and theories of the world’.
Although my interviewees did not explicitly use the term ‘self-care’, they frequently described everyday routines aimed at managing PCOS symptoms. These practices, such as preparing low-carbohydrate meals and snacks, training in a gym or plucking facial hair, can be understood as forms of self-care. To explore the materiality of such practices, I turn again to Annemarie Mol's work. Mol famously contrasted the logic of choice and the logic of care as two distinct ‘modes of thinking and acting’ in medicine: the former emphasises solutions and places responsibility for treatment on patients, while the latter centres on the ongoing adjustments and negotiations between medical professionals and patients needed to achieve ‘good enough’ outcomes (Mol, 2008). In relation to PCOS, Mol's theory of ‘two logics’ has helped me explain the role of different digital tools in patient experience (Karpova, 2025). Here, I draw on Annemarie Mol's further conceptualisation of care, as tinkering, the concept she first used in ‘The Body Multiple’ and then in ‘The Logic of Care’ and in her article for The Lancet (Mol, 2002: 177; 2008, 2009). She further developed this notion in her 2010 volume co-edited with Ingunn Moser and Jeanette Pols. Together they described tinkering as central to care: a set of ‘persistent’ and ‘adaptive’ practices that respond to the shifting needs and circumstances of carers and care recipients (Mol et al., 2010: 13, 15).
Tinkering often involves material objects: for example, Winance explored the ‘shared work’ of people and wheelchairs to adjust to each other (Winance, 2015: 95). Danholt and Langstrup wrote about self-care and tinkering in the context of everyday use of medication in chronic disease. They presented tinkering as ‘the negotiation of trade-offs’ when deciding when and how to take medication, depending on the changing circumstances of one's everyday life and social relations (Danholt and Langstrup, 2012: 525–527). In the recent special issue on care in STS, Eidenskog argued that conceptualising ‘care as tinkering steers the focus away from the traditional connection between care and the warm relationships between humans to a broader scope where the interweaving of technology and everyday practices is in focus’ and highlighted the importance of tinkering in urban planning (Eidenskog, 2021: 28). Building on this argument, one can think of tinkering as a useful analytical tool for highlighting material aspects of care and self-care.
Tinkering with nutrition and exercise is a common thread of several interviews. The material qualities of food and its components, such as vitamins and macronutrients, affect the secretion and activity of hormones such as insulin, leptin and testosterone (Szczuko et al., 2021). These hormonal shifts, in turn, alter physical processes including glucose metabolism, ovulation, menstruation and skin oil production, and sometimes cause bodily sensations such as fatigue or bloating, and mental states such as stress or anxiety (Dewani et al., 2023). To cope with these symptoms, my informants modified their diets, usually by trying to reduce the consumption of sugar and other simple carbohydrates and reorganising their cooking and meal prepping routines. At the same time, physical exercise improves insulin sensitivity and therefore helps improve glucose metabolism and makes the menstrual cycle more regular (Woodward et al., 2020). The recommendation to modify diet and be physically active typically comes from doctors who focus on ‘excess weight’ and body fat as key elements in the pathophysiology of PCOS. Weight stigma and fat shaming are common problems faced by PCOS patients. When the doctors, to use Mol's terminology, enact the ‘excess body fat’ version of PCOS, the patients sometimes resist, openly objecting to the weight loss recommendations or seeking body-positive attitudes towards PCOS in online support groups (Karpova, 2025). When telling me about their food choices, my informants usually described their motivation not as weight loss in pursuit of an ‘ideal’ body but as improvement of glucose metabolism, lowering of testosterone levels, and thus making menstruation more predictable or less heavy, and preventing the development of type 2 diabetes and cardiovascular diseases in the future. They tinkered with food, cooking appliances and lunchboxes to find optimal daily routines fitting their work schedules, emotional needs, fertility plans or parenting duties. I will now zoom in on several examples.
Ida received her PCOS diagnosis at the age of 20, when she lived with her parents in a small city. Her gynaecologist did not give her any advice apart from taking birth control pills to regulate her menstruation. In search for more information, Ida attended meetings of the Danish ‘PCO Foundation’, a support organisation for people with PCOS. One meeting included a presentation by a dietitian, who recommended meticulously counting macronutrients and calories, weighing plates and reducing simple carbohydrates. Ida started following this diet together with her parents. She bought a kitchen scale to weigh plates and printed out charts with caloric and nutritional values of different foods that she found on the Internet. The whole family followed this diet, but after a while, Ida became ‘fed up’ with weighing food and counting calories and nutrients, so she switched to a version of a ‘low-carb, high-fat diet’ that does not require tracking. Now, at 34, she intuitively feels what feels good and what makes her bloated and her heart rate increase (e.g., starchy products). When she wants a snack, she opts not for something not sweet but rather fatty and salty, ‘like snack sausages or little pieces of cheese’. Ida showed me a snack pack with lettering and the logo of the popular supermarket chain Rema 1000 and the inscription ‘Flæskesvær’ (see Figure 1). I did not know what it meant, and she explained: ‘It's actually quite disgusting: dried pigskin’, and laughed. Explaining her snack choice to someone not familiar with it made Ida recognise that the material qualities of dried pigskin can provoke disgust. For Ida, however, the choice of pork scratchings over sweet snacks is a matter of tinkering: she traded off taste for positive mental and physical sensations and long-term health benefits. While Ida cannot give up snacking altogether, pork scratchings serve as a compromise. After she stopped tracking calories and nutrients, her attention shifted to the materiality of different foods: taste, texture and the impact on her digestion and overall well-being.

A package of pork scratchings that Ida uses as a snack. Photographed by the author.
For Rikke, a 42-year-old mother of three, tinkering with food means attending to the needs of the entire family. Rikke turned to her GP at 23, when trying for her second child with no success, only to hear that she was ‘too young to have PCOS’. She nonetheless insisted on being referred to a gynaecologist and received her diagnosis. Rikke followed the gynaecologist's recommendation to take a glucose-regulating medication, Metformin and lose weight through dieting. This helped normalise Rikke's menstrual cycle and conceive her third child. Now she is struggling to maintain her weight because she is afraid of developing type 2 diabetes, and she cannot keep taking Metformin because of an unpleasant side effect, a bad stomach. Over the years, Rikke tried different diets and exercises, lost weight and regained it again. At 29, she received a diagnosis of attention deficit hyperactivity disorder (ADHD), a condition which is marked by difficulty maintaining routines: ‘You have to do it, but you cannot get to do it’. It has been easy for Rikke to avoid sugary drinks, but cooking PCOS-friendly meals (with lower carb content and a lot of fibre) is more difficult because two of her children are autistic and have their own nutritional restrictions due to sensory sensitivities to certain textures and tastes. Rikke explained: ‘And it's not, as it's not so easy when you have PCOS, and it's a life-changing lifestyle you have to do. And you have to see all the factors in a person's life to see if it's going to work or not. And in my household, it's very difficult to change the meals, because (…) two of my children (…) are autistic. So we have to eat special things, so everyone in the house can get food’. While in Ida's case, her family adjusted to her changing routine, Rikke had to adjust to her family's needs and prepare different meals for everyone.
Now Rikke tinkers with meal preparation in several ways: by being less restrictive about her diet and eating the same as other family members, by delegating cooking to her husband and by ordering cooking meal kits from HelloFresh. It is an imperfect solution. Rikke would like to have clear guidance on nutrition, something that would make meal planning easier while also ensuring that she eats healthily enough to prevent type 2 diabetes: ‘I would have loved it if there was a specific cookbook, or something that could help people with PCOS, [distributed by] the hospitals or the gynaecologist’. A cookbook could serve as a material object with concrete recipes to hold on to everyday, when you are burdened by caring about other family members. Rikke added, ‘I think I would benefit from having a health coach who could help me with the exercise, my food, and could help me manage all the things’. Without such a coach, she has to continue tinkering with more or less burdensome options.
When planning and practising physical activity, one can tinker with choosing the type and intensity of exercise, and whether to do it in a group, in a company or alone. A 24-year-old Esther, similarly to Ida and Rikke, did not receive any detailed lifestyle advice from her doctor when receiving her diagnosis. She searched for information herself and learned that Metformin can help, but lifestyle interventions are also necessary. Esther uses nutrition and exercise to mitigate the irregular menstrual cycle, pain during ovulation and menstruation as well as constant hunger. She described her routines: ‘I go to the gym 3–4 times a week, at least try to do it. I combine cardio and weight lifting. And then I am more mindful of how many sweets I eat, or the combination of carbs and sugars on my plate. I think I tend to eat more greens than before, because they keep you full longer, and they have great benefits. But it's not something I thought about before. In the summertime, I would think, ‘I eat an ice cream, it's okay’. I just need to look at the option, do I really need this ice cream, does it need to be a vanilla ice cream or can I do with a sorbet, just because it's hot and I need to cool down, or because I really need this sweet? So I want to be more mindful’. Here, tinkering appears in the form of combining different types of exercise in a gym, tracking nutrients or swapping vanilla ice cream for sorbet in summertime. When I asked Esther to provide more details on her gym visits, she explained that her exercise routine depends on whether she does it alone or accompanied by her boyfriend. Alone, she likes attending dance classes at her gym. ‘But it's also fun to lift weights with my boyfriend. So it depends on whether he is there or not. I cut down my weight lifting if he is not there, and then maybe run [longer] on a treadmill. But if he is there, I’m more likely to cut down on the treadmill and lift more weights’. Tinkering with exercise serves the purpose of maximising joy from exercise: the weight feels better in Esther's hands when she shares this experience with her boyfriend, while the treadmill under her feet is more enjoyable when she trains alone. This way, the materiality of the gym equipment interconnects with social relations.
As these examples show, tinkering is the shared work of patients’ bodies, nutritional properties of food, shapes and technical affordances of cooking utensils as well as weight and speed of the gym equipment. Patients tinker differently depending on their PCOS symptoms, co-existing mental and physical conditions and social obligations. One particular characteristic of tinkering is its engagement with time: it takes time, while it often aims at saving time by simplifying or rescheduling certain tasks. The next section focuses on the role of time in everyday life with PCOS.
Time
Temporality is frequently emphasised in studies of care and of disease. In their introduction to a special issue on ‘materialities of care’, Buse et al. suggest that ‘materialities and practices of care’ are ‘folded within a multiplicity of intersecting temporalities’ (Woodward, 2016; Buse et al., 2018: 248). Likewise, Shove et al. emphasised the ‘material, emotional, moral and political dimensions’ of time (Shove et al., 2009: 2). The temporality of disease is related not only to the routines of monitoring and treatment of symptoms or the schedules of medical appointments but also to the futures that the disease forecloses, or, on the contrary, opens. Materials can facilitate ‘processes of “material imagining”’ (Buse et al., 2018: 249), for example, when, by learning to use medical devices, a patient hopes for the future with less pain or anxiety and more comfort (Arteaga, 2019; Berk, 2018). In PCOS, the future is often uncertain, especially at the time of receiving the diagnosis. Several informants described their emotional reaction at the announcement of the diagnosis by the doctor as confusion, stress or loneliness due to not knowing anyone else with the condition. As a chronic and incurable condition, PCOS becomes an element of the future: as my informant Isabella phrased it, ‘it is a forever disease’.
The future with PCOS can mean never having regular menstruation. Some people with PCOS have regular periods, like, for example, my informant Olivia, but most of them will either have an irregular menstrual cycle (oligomenorrhea) or no menstruation at all (amenorrhea) (Harris et al., 2017). Inability to predict the start of the next menstruation requires what Fox et al. call ‘material preparedness in the form of carrying a pad’ (Fox et al., 2020: 2). A few informants told me that they would necessarily carry a pad or a menstrual cup when going outside. This constant anticipation of a sudden bleeding becomes a routine. Alberte, a woman in her mid-30s, always carried a pad just in case, because she found it the most convenient sanitary product: ‘Take it out of your bag, and then you’re good to go’. She tried to listen to her body to predict the approaching period, but was often mistaken: ‘There were actually a lot of times where I felt like I was about to have my period, it felt like my body was going there. And then I didn’t have my period. I don’t know if it's just the cysts doing that thing [laughs] or whatever’. Alberte implied that she could mistake the sensation of having enlarged follicles in her ovaries for pre-menstrual discomfort. The temporality of the physical processes in her body was difficult to grasp, so the constant presence of a material object, a pad, in her bag mitigated this uncertainty. A few months before the interview, Alberte had a non-gynaecological surgery, and after that her menstrual cycle became regular for a reason she cannot quite understand. This new timing of her period turned out to be uncomfortable: she feels that she menstruates ‘too often’. The disappearance of one of the common PCOS symptoms produced a new rhythm that required adjustment.
Hunger and satiation are also rhythmic, cyclical sensations. Six of my informants reported being hungry either before the period starts or when missing a period. Some talked about frequent hunger or never feeling quite full. Overcoming this feeling was one motivation for dietary changes. Esther, whose tinkering with different snacks I discussed in the previous section, managed her appetite through careful timing of meals. ‘Before I had a big appetite [laughs], because I didn’t feel I could… no matter how much I ate, it didn’t fill me up. And now I eat breakfast, then a snack at 10:00, then a big lunch, then a small snack at 15:00–16:00, and then I don’t need a lot of food for dinner, because I have eaten regularly throughout the day. It just works better for me than three big meals. I find that even though I went to the gym, I do not need as much food for dinner, because I feel full already’. When I asked her how she managed this meal when in the university, Esther explained that she packed her lunch in a lunchbox with several sections, and bananas and crispbread for a snack in a one-section container. And when I wondered how she carries all this to the university, she pointed to her big black backpack: ‘So I just put it there, or have a little reusable net with me over the shoulder. I don’t consume plastic on the way. You know what I mean, with plastic bags (…) When I have overnight oats with me, I also have them in old jam jars’. Esther's daily tinkering is oriented towards saving time, contributing to saving the environment from waste, and also saving money by packing reasonably priced lunch and snacks. In other words, the temporality of Esther's PCOS materialises through tinkering with different objects – filling meals and snacks, reusable containers such as glass jars, and her capacious backpack.
The temporality of menstruation and hunger in PCOS can be compared with the temporality of chronic diseases and disabilities. Alison Kafer, who works within crip theory, introduced the notion of ‘crip time’ that ‘involves an awareness that disabled people might need more time to accomplish something or to arrive somewhere’. Disabled people need time to get on and off the bus in a wheelchair, or adjust hearing aids, or wait for the accompanying caregivers who may be running late (Kafer, 2013: 26.) People with mental illnesses and neurodevelopmental disorders may have a different perception of time: for example, people with ADHD have difficulty adopting to the rhythms of their workplaces and everyday chores (Nielsen, 2019). While menstrual disorders are not considered disabilities, they affect people's relations to bodily rhythms and pose challenges to keeping daily schedules. Williams and her colleagues, in their study of work routines of women with another common gynaecological condition, endometriosis, reconceptualised Kafer's notion of ‘crip time’ as ‘endo time’. Like PCOS, endometriosis is a condition with variable symptoms and unpredictability related to menstruation. However, unlike PCOS, where menstruation is not necessarily accompanied by pain, endometriosis is characterised by unpredictable pain that can be debilitating enough to disrupt work schedules and place affected people in a precarious position (Williams et al., 2025). Relying on my interview data, I suggest thinking of ‘PCOS time’ as not necessarily falling outside of work schedules, dictated by capitalism, but as fragmented into different rhythms facilitated by materiality: the irregular rhythm of menstruation and preparing sanitary products, the rhythm of hunger and satiation regulated by meal prepping and packing snacks, the rhythm of exercise dependent on the level of tiredness, the proximity of the gym and availability of comfortable workout clothes. These rhythms connect to the ‘material imagining’ of the future (Buse et al., 2018; Woodward, 2016), that is, using materials and their properties to achieve a more desired future: without diabetes or cardiovascular diseases, with more predictable menstrual cycles, or, not least, with the possibility of conceiving, carrying a pregnancy and giving birth.
Reduced fertility, or sub-fertility, is usually the first aspect of PCOS that doctors mention when announcing the diagnosis. For some of my informants who were diagnosed at a young age, this information felt irrelevant because they had not thought about having children, and family planning felt like a remote prospect. For others, it was sad and shocking news. For example, Karolina wanted to future-proof her fertility. When her gynaecologist said that PCOS cannot be cured, she asked about her fertility prospects. She was 21 at the time and wanted to start trying to conceive in the near future: ‘So, it was a subject that I thought a lot about. And he [the gynaecologist] said, “When this time occurs, you should go and talk to your own doctor [the GP]” (…) And the nurse on the side was friendly and said, “I understand what you’re concerned about, but you’re so young and so thin, and I wouldn’t be concerned about it”. And I had to ask if there is anything I can do to improve fertility when the time occurs. And he was like, ‘what do you mean?’ ‘Well, is there anything I can eat or exercise?’ ‘Exercise is always good’, he said, and I felt like I wasn’t being taken seriously, because I wasn’t a typical PCOS patient’. The medical professionals perceived Karolina's worries about the future as not well-grounded due to the materiality of her body: it fits the medical definition of ‘healthy weight’, and her young age implied that she had enough time to wait before starting a family. While Karolina's thinness and youth gave her the privilege of not being pathologised by the doctors, she received no assistance in imagining her future fertility. Therefore, she turned to ‘material imagining’ through tinkering with eating and storing food, hydration and exercise: I heard that the process of conceiving with medical help is painful, stressful, can be almost like a full-time job for some women, with a lot of tests and going in and out of the hospital. So, I wanted to avoid that and tried to somewhat cut out caffeine. I said, okay, one cup of coffee is enough if I need it. And then I tried to minimise sugar, added sugar. But I was also aware that if I ban everything, it will be a hard tryout for me. So, I allowed myself some things every day. And then I started not to exercise hard, but tried strength training, muscles. We went for a lot of walks.
Karolina was able to conceive without assisted reproductive technologies. Several other informants had had long journeys through fertility treatment or were about to start their IVF (in vitro fertilisation) protocols at the time of their interviews. Fertility treatment unfolds as a temporal experience, characterised by extended waiting periods and continually shifting horizons of future pregnancy (Payne et al., 2025). For Sofia, who meets all three PCOS criteria (irregular period, cysts on an ultrasound and high testosterone), the journey towards a successful pregnancy proved to be relatively long. After going through one round of intrauterine insemination and two rounds of IVF with no success, Sofia and her boyfriend took a break in treatment due to tiredness and the stress from the sudden onset of illness in an older relative. Meanwhile, Sofia discovered that she had an under-functioning thyroid and needed to start taking a synthetic thyroid hormone, L-thyroxine. Then, after two more unsuccessful IVF rounds, Sofia got pregnant. She took a lot of different medicines to support her pregnancy, including
Sofia used a mundane object for her material imagining during her long-awaited pregnancy: a little notebook. When I asked what she wrote down in there, Sofia clarified: ‘Ups and downs during pregnancy. Like, for example, at the start, I had a little bleeding. And I was super scared. I just wrote stuff like that: positive things, negative things’. She also recorded what kind of medicine she was taking in that notebook rather than in a digital tracker. Sofia did not buy the notebook specifically for this purpose; she found it at home and decided to start ‘kind of like a pregnancy diary’. She told me she was still using it, but as a diary of her child's growing up: ‘It's about my son, how he has ups and downs as well, and how he's walking, how he's eating’. When I asked Sofia whether she would give the notebook to her son to read when he was older, she replied, ‘Yeah, sure’. The notebook connected the sensory experiences of different time periods: fertility treatment, pregnancy, breastfeeding and observing the child hitting his milestones and having different moods. Sofia's story contains a lot of tinkering with medication, with her bodily processes (thyroid function, glucose metabolism, milk glands in preparation for breastfeeding), with note-taking by hand and, ultimately, with time.
The analysis of these few case studies demonstrates how the everyday experience of PCOS is shaped by waiting: for a period to start, for the appetite to normalise, for the pregnancy to happen, for the treatment to take effect. But my data reveals another aspect of PCOS temporality: repetition or circularity. Tinkering with medication, food and consumer objects from backpacks to notebooks is a routinised, repetitive practice. In my next section, I will argue that the circularity and persistence of tinkering in PCOS can help cope with shame.
Shame
Philosopher Luna Dolezal, combining phenomenological and social constructivist visions of shame, suggests that women are especially susceptible to systemic, ‘chronic’ shaming. She argues that events that cisgender women's bodies typically go through, such as menstruation, menopause, and, for some, pregnancy, are positioned by societies and medical communities as anomalies. Especially in Western societies, the female body is structurally defined as in constant need of perfection and becomes ‘a central cog in the neoliberal consumer capitalism’. The multi-billion dollar beauty, cosmetic surgery industry and fitness are based on this structural shaming of women's bodies (Dolezal, 2015: 108). A PCOS body that deviates from the medical norm and from the social standards of beauty and femininity – ‘too fat, too hairy, too invisible’, as scholar and activist Christina Fisanick (2005) phrased it – can be an easy target of structural shaming. Yet even people whose PCOS symptom packs do not include fatness or facial hair still experience shame, for example, due to irregular or absent menstruation or fertility challenges (Kitzinger and Willmott, 2002). My data, however, showed examples of actively refusing to be ashamed and speaking up against shaming. I will dwell on a few of them.
Alberte struggles with excess body and facial hair. She got a referral to a dermatologist for laser hair removal, but discontinued the sessions due to being too busy: ‘Life just happens, and then you’re like, whatever, I look the way I look’. When she removes her hair at home with a combination of shaving, waxing and plucking with a tweezer, depending on the length and thickness of hair in different areas of her body and face, she still experiences pain. Therefore, she needs to ‘psych up’ every time to do the removal, and she does it only once a month. Alberte's acceptance of her body can be viewed as strategic in justifying her reluctance to minimise painful and time-consuming hair removal procedures. However, she herself describes this acceptance as a result of changing priorities. Her anxiety about her skin lowered as she reached her late 20s: ‘Not that I want the beard, and I am removing it, but it's more like: this is my body. This is how it works. It's not nice. It's not what I wanted, but this is how I am, and I think that's been nice for me getting older’. This explanation sounds like tinkering with feelings about one's body: not a full acceptance but a compromise. Tweezers, wax strips and shavers are still part of Alberte's everyday life, as is the pain they cause. Growing a beard is still not an option she considers. But she chose to trade off skin smoothness for having less pain in her everyday life.
A 23-year-old Isabella, who lives with her husband in a house in the countryside, is more outspoken about her body acceptance. She felt comfortable telling her husband about her PCOS and possible fertility problems just as they met. Now, she often talks about PCOS with others: I'm really not the best at wearing clothes. That sounds really awful. But I always just like to wear, you know, a long T-shirt or something, and especially because his friends always come over at night, they used to see me in just my sleepwear. And sometimes I have hair on my legs, and one day we spoke about it, oh, why I have that and why I do not shave and stuff like that. So most of his friends know about this, too. I'm not really… I'm not the one to hold it back from people.
If falling outside the medical and social standard of femininity is a major source of shame in PCOS, what is a place of shame in the experience of gender-non-conforming people with PCOS? For Jon, a 38-year-old transgender man, bodily hair causes not shame but, on the contrary, some comfort in his transition journey. Jon has not had access to gender-affirming hormonal therapy. He has only been through a social transition – a set of non-medical activities, such as changing personal style in clothing and hair, coming out as transgender to selected people and groups and using a new name and pronouns. While Jon admits that he does not completely ‘pass’ (i.e., he is not perceived by others as a man yet), having bodily and facial hair helps him look less feminine. In addition, being in a larger body has the same effect: he believed that if he were skinny, others would more likely see him as a ‘girl’. Before his transition, Jon experienced a lot of body shaming and experimented with dieting, which resulted in significant weight fluctuations. That, in turn, caused his problems with liver functioning and impaired his lipid metabolism. Like the informants in the two previous examples, Jon learned to accept his body over the years, but for him, social transition played a decisive role. By changing his style of clothing and hair and choosing a more masculine social presentation, Jon released himself from what he calls ‘the gender box’. At the same time, he does not yet feel the pressure of any social standards of masculinity and male fitness. Jon uses the terms ‘fat’ and ‘plump’ neutrally: ‘Yes, I am plump, but not everyone can be Apollo. I still have charisma and beautiful hair’.
Body acceptance allowed Jon to break his long-term association of exercise with shame. When doctors in his home country fat-shamed Jon and recommended physical activity, he would feel shame and guilt for not exercising enough and not losing weight fast. After his emigration and social transition, Jon chose walking as his preferred exercise that is good for health and enjoyable: I've always been told that I need to move more, a lot, to lose weight. Here [in the Western European country where Jon lives] they [the GP] told me that I just need to move more, without thinking about weight, because movement prevents dementia, protects against cancer and a whole bunch of other things (…). And there is no need to connect to weight and tell yourself, ‘Well, if I go for a walk today, I'll burn that many calories’. It's better to say that I should go for a walk today, and I'm doing a good job because my body will get oxygen and overall become healthier, and walking is simply fun (…) When you do something not out of guilt or fear or self-hatred, you get to know yourself better with every step.
In all three cases, adaptive tinkering allows sidestepping or confronting bodily shame. This tinkering differs in length and the type of material objects involved, depending on one's symptoms and needs. Bodily shame in PCOS is tightly related to medical and social gender norms, and Jon's case reveals that gender non-conformity can itself be a form of adaptive tinkering. However, the lengthiness of one's experience of PCOS is not a guarantee of overcoming shame. According to my data, shame, like any other emotion, can still accompany the changing reality of PCOS, when, for example, one starts a fertility treatment and does not succeed, or has a recurrence of a mental health crisis. My interviews demonstrated that a person with PCOS can deal with episodes of shame as they come, through tinkering.
Conclusion: multiple materiality?
This article employed a medical STS framework to examine the everyday lives of people with PCOS, a condition that is both widespread and markedly diverse. It argued that attending to materiality is essential for understanding the routines, emotions and social relations that shape patients’ experiences. I illustrated this claim with examples from my interviews, in which participants with PCOS showed me various objects and described how they used them. The thematic analysis of the data yielded three interconnected themes: self-care, time and shame. These themes overlap: self-care, practised through tinkering, helps people adjust to bodily rhythms and cope with uncertain futures; bodily shame often diminishes over time; and the repetitive practices of self-care/tinkering can foster greater acceptance of one's appearance, including weight and body hair. Tinkering, a key concept in care studies in STS (Mol, 2008; Mol et al., 2010), appears to be effective in characterising the everyday materialities of PCOS: all the analysed interview fragments reveal the stories of adapting cooking, eating, exercising, taking medication and skincare to one's physical and emotional needs and external circumstances such as caring for families. Tinkering is my informants’ reaction to the scarcity of guidance from their medical providers. It allows managing uncertainty, imagining futures (Buse et al., 2018) and caring about one's physical and emotional needs and cravings. Tinkering is material: it is focused on textures (smooth or hairy skin), tastes (sweet or salty, lean or fatty foods, sticky wax stripes or sharp rasors), weight (sports equipment) and speed (running on a treadmill, walking) and physical effects of the chemicals in medications.
Tinkering analysed in this article may appear ordinary and not unique to PCOS. Practices such as going to the gym or dance classes, avoiding sugary drinks and preparing meals in advance or plucking facial hair are common among many people who pursue a healthy lifestyle and seek to look conventionally attractive. However, in the context of PCOS, these practices take on specific orientations and purposes. People with PCOS tinker with particular goals in mind: making menstrual cycles more predictable; gaining access to gender-affirming hormone therapy; trying to conceive naturally to avoid fertility treatment or to improve the likelihood of success with IVF; balancing family members’ dietary needs while preventing diabetes; and removing bodily hair or deliberately showing it to educate others about the condition.
People with different ‘symptom packs’ may tinker in similar ways. For instance, Karolina, who had always had a small body, and Alberte, who aimed to lose weight, both reduced simple carbohydrates and cooked diverse meals in order to regulate their menstrual cycles. Conversely, people with similar ‘symptom packs’ may tinker in similar ways but towards different ends. Most of my informants used physical exercise and balanced eating to lower their testosterone levels, whereas Jon adopted the same practices to qualify for testosterone therapy and continue his gender transition. Yet, like many others, Jon was also motivated by the desire to prevent type 2 diabetes and cardiovascular diseases.
The analysis presented in this article shows that while people with different ‘symptom packs’ of PCOS often engage in similar patterns of tinkering, they direct these practices towards different goals. As a result, distinct ‘symptom packs’ are linked to different materialities, yet these materialities frequently overlap in meaningful ways. John Law, in his contribution to the abovementioned volume on care as tinkering, characterised tinkering as ‘a set of constantly unfolding and only partially routinised practices for holding together that which does not necessarily hold together’ (Law, 2015: 69). Ordinary practices, analysed in this article, can be described as holding PCOS together and simultaneously revealing the diversity of this syndrome. While health professionals in different clinics and hospital departments work on coordinating different versions of PCOS, patients focus on the treatments relevant to their specific ‘symptom packs’. They tinker with specific material objects to manage their symptoms and address their everyday needs—rather than to treat PCOS as a unified syndrome.
This article focused on the individual, everyday tinkering practices of people with PCOS, shaped by the materialities of objects and social relations with family, friends and co-workers who do not experience PCOS themselves. Nearly all of my participants said they barely knew anyone else with the condition, apart from the occasional conversation with affected relatives. To find other PCOS patients, seek advice and build solidarity, they turn primarily to social media rather than to practices involving analogue objects, as I demonstrated elsewhere (Karpova, 2025). This does not mean that people with PCOS never meet or support one another offline. As noted earlier, the Danish PCOS Foundation (PCO Foreningen) once brought together patients and healthcare experts, although it is no longer active. Tracing the history of such organisations and identifying contemporary offline forms of PCOS patient activism would require extensive archival research and new forms of fieldwork and would be a valuable direction for future study.
Footnotes
Acknowledgements
The research for this article was part of the project ‘Design as Somatic Expertise: The User's Body and Well-Being in Design Today’, funded by the Carlsberg Foundation (Project number CF21–0231). The author thanks Harun Kaygan, Mette Kjærsgaard, Ida Kathrine Hammeleff and Luna Dolezal and three anonymous reviewers for their comments on the drafts of this article.
Author’s note
The fieldwork research for this article was approved by the Research & Innovation Organisation at the University of Southern Denmark. All the participants signed a consent form before being interviewed.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Carlsbergfondet, (grant number CF21-0231).
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.