
Abstract
This study investigated the feasibility and preliminary effectiveness of a parenting training program designed for early intervention and early childhood special education (EI/ESCE) programs serving students with autistic spectrum disorders. Thirteen teachers representing three intermediate school districts implemented the intervention with 27 students and their parents. Eighty-nine percent of families completed the program. From pre- to post-intervention parents improved their use of the treatment strategies and children increased their rate of language during a parent-child interaction in their home. Parents and teachers reported significant gains in child mastery of social-communication skills and teachers, but not parents, reported a significant decrease in social impairment. Parents reported a significant decrease in parenting stress. Both groups rated the intervention highly in regard to treatment acceptability, perceived effectiveness, and usability. Findings suggest that this intervention can be feasibly implemented in public EI/ECSE settings, filling an important gap in services for intervention programs serving children with autistic spectrum disorders.
The importance of the direct involvement of parents in the education of children with autism spectrum disorders (ASD) has been widely recognized (e.g. National Autism Center, 2009; National Research Council, 2001). Parents can become active participants in their child’s education in a variety of ways. One approach, parent training, provides parents with direct instruction in intervention strategies to support their child’s development (Mahoney et al., 1999). The evidence base for parent training in ASD, either as a sole intervention or as a component of a more comprehensive program, is growing (e.g. McConachie and Diggle, 2007). A number of studies, including several recent randomized control trials, have demonstrated that parent training is an effective approach for improving social-communication development in young children with ASD (McConachie and Diggle, 2007). Research indicates that parents can learn developmental and behavioral strategies with a high degree of fidelity (e.g. Kaiser et al., 2000) and that use of these strategies results in increased language development (e.g. Kaiser et al., 2000) and social engagement in their child with ASD (e.g. Kasari et al., 2010; Mahoney and Perales, 2003).
Research also indicates that parent training is time- and cost-effective and leads to better generalization and maintenance than therapist-implemented intervention models (Brookman-Frazee et al., 2009). For example, one early study found increased generalization in children whose parents had been trained to use a behavioral intervention compared with children who received five times as many hours of intervention from a therapist (Koegel et al., 1982). A recent study conducted in Australia found that preschoolers with developmental delays including autism who were randomly assigned to center-based services plus weekly home-based parent training services made significantly greater gains in cognitive and behavioral functioning than children assigned to center-based instruction only (Rickards et al., 2007).
Parent training can also improve the quality of life for the family by reducing parental stress and depression (Tonge et al., 2006) and increasing parental leisure and recreation time (Koegel et al., 1982). This outcome is particularly important given the high rate of stress and depression found in parents of children with ASD (e.g. Estes et al., 2009). Furthermore, parents who participate in parent training programs report more optimism about their own ability to influence their child’s development (Koegel et al., 1982), which may help parents maintain their efforts with their child over time (National Research Council, 2001).
Although parent training is now considered an essential component of successful early intervention programs for children with ASD (National Autism Center, 2009; National Research Council, 2001), formal parent training programs are still the exception in community-based intervention programs for young children with ASD in the United States. For example, an Indiana survey suggested that parent training ranked 15th out of 19 possible interventions in rate of use and that only 21% of families with a child with autism aged 2–8 years had ever received parent training (Hume et al., 2005). The lack of available parent training services for younger children is even more striking; in a North Carolina survey, only 8% of parents of children with ASD 4 years and under reported receiving parent training (Thomas et al., 2007). This is particularly concerning as parent training ranked first of 19 interventions in terms of parents’ perception that the intervention was ‘efficacious and contributed to their child’s growth’ (Hume et al., 2005).
Given that the vast majority of young children with ASD in the United States receive intervention services through the public schools (Thomas et al., 2007), one way to increase access to parent training is to offer it as part of public Early Intervention (EI) and Early Childhood Special Education (ECSE) programming for children with ASD. This may be a particularly effective approach for increasing access to parent training, because the single strongest predictor of maternal involvement in the education of their child with autism is the extent to which public school teachers encourage and provide opportunities for their participation (Benson et al., 2008).
Despite its intuitive appeal, there are several obstacles that can prevent the inclusion of parent training in EI/ECSE programs. The first obstacle is that most empirically based parent training programs are conducted individually with the parent, child, and coach once to twice a week over many months (e.g. Kaiser et al., 2000; Mahoney and Perales, 2003). However, most EI/ECSE programs for children with ASD (especially those over three) in the United States are provided in classroom settings (Bitterman et al., 2008), which allow little time for teachers to meet individually with the parent and child. This can make it difficult for many special educators serving children with ASD to envision using these parent training models. A second obstacle is the lack of quality parent training materials for families of children with ASD. Many of the empirically based programs in the literature have developed materials for parent training; however, as they are typically conducted in a one-to-one setting, they lack many of the features necessary for providing training to a group of parents, such as slide presentations and video examples. A final obstacle is the lack of appropriate preparation for providers working with children with ASD and their families (McCollum, 1999). Most specialists, especially those working with children aged three and over, are not trained to understand how adults learn or techniques for teaching parents specific skills (Mahoney et al., 1999). Thus, the development of parent training curricula for children with ASD that can be easily adopted by EI/ECSE teachers is a high priority.
To address these issues, Ingersoll and Dvortcsak (2006) developed Project ImPACT, an evidence-based parent training curriculum whose format is compatible with a classroom-based intervention model and includes instruction for working with parents. Our initial evaluation of this program (Ingersoll and Dvortcsak, 2006) indicated that parents increased their understanding of the intervention techniques, were highly satisfied with the training format, and attributed gains in their child’s social-communication skills to the program. Participating teachers found the program to be appropriate for use in ECSE settings and user-friendly. They also reported a number of positive effects on the parents’ and children’s behavior, including improvements in parents’ ability to promote their child’s social communication and gains in child skills. Based on parent and teacher feedback, several changes were made to the curriculum, including increasing the length of the group sessions and adding one group session and two coaching sessions that focused on individualized goal development and strategies for teaching imitation and play. Materials were developed for the resulting 12-week program and the intervention techniques and the parent training procedures were manualized (Ingersoll and Dvortcsak, 2010).
The goal of this article is to examine the feasibility and preliminary effectiveness of the manualized parent training program in public EI/ESCE programs serving students with ASD. In particular, we were interested in assessing: 1) parent participation and treatment acceptability for parents and teachers; 2) parents’ ability to use the intervention techniques; 3) changes in child social communication; and 4) changes in parent stress.
Methods
Participants
This study was implemented in three intermediate school districts (ISDs) serving children with ASD. The three ISDs differed in terms of their program structure and services. In ISD A, all ECSE classrooms were ASD-only and EI services were delivered during weekly home visits. In ISDs B and C, ECSE classrooms were mixed-disabilities, and EI services for ISD B were provided in small toddler groups. Services also differed across programs and children within each ISD. For example, in ISD A, children receiving EI services received two 1.5-hour home visits per week, whereas children receiving ECSE services received 12 to 28 hours of intervention within a classroom setting.
Thirteen teachers who provided services to children with ASD were selected by their ISDs to participate based on their responsibility for educating students with ASD 1 . ISD program administrators made this decision without input from the research staff; thus, specific inclusion/exclusion criteria were not apparent to the researchers. All teachers had extensive experience working with young children with ASD and their families in various contexts prior to participation in this program; however, only one teacher had significant experience providing parent coaching prior to beginning the program. The teachers ranged in years of teaching experience from less than 5 to more than 20. Across programs, seven were classroom teachers in an ECSE classroom for children with ASD, three were ECSE classroom teachers for children with mixed disabilities, two were EI program teachers, and one was an autism consultant. Teachers received $200 for their participation in data collection.
Participating teachers invited families on their caseload to participate if their child was receiving services under an ASD eligibility or another eligibility if the teacher strongly suspected an ASD diagnosis. Twenty-six families representing 27 children (one family had two children) chose to participate in the parent program 2 . For each family, the primary caregiver participated in the training. In families in which more than one caregiver participated, only measures from the primary caregiver were collected. Pre- and post-treatment data were available for the 24 children whose parents completed the program. Parents received a $20 payment for data collection at each time point. See Table 1 for sample characteristics.
Demographic information.
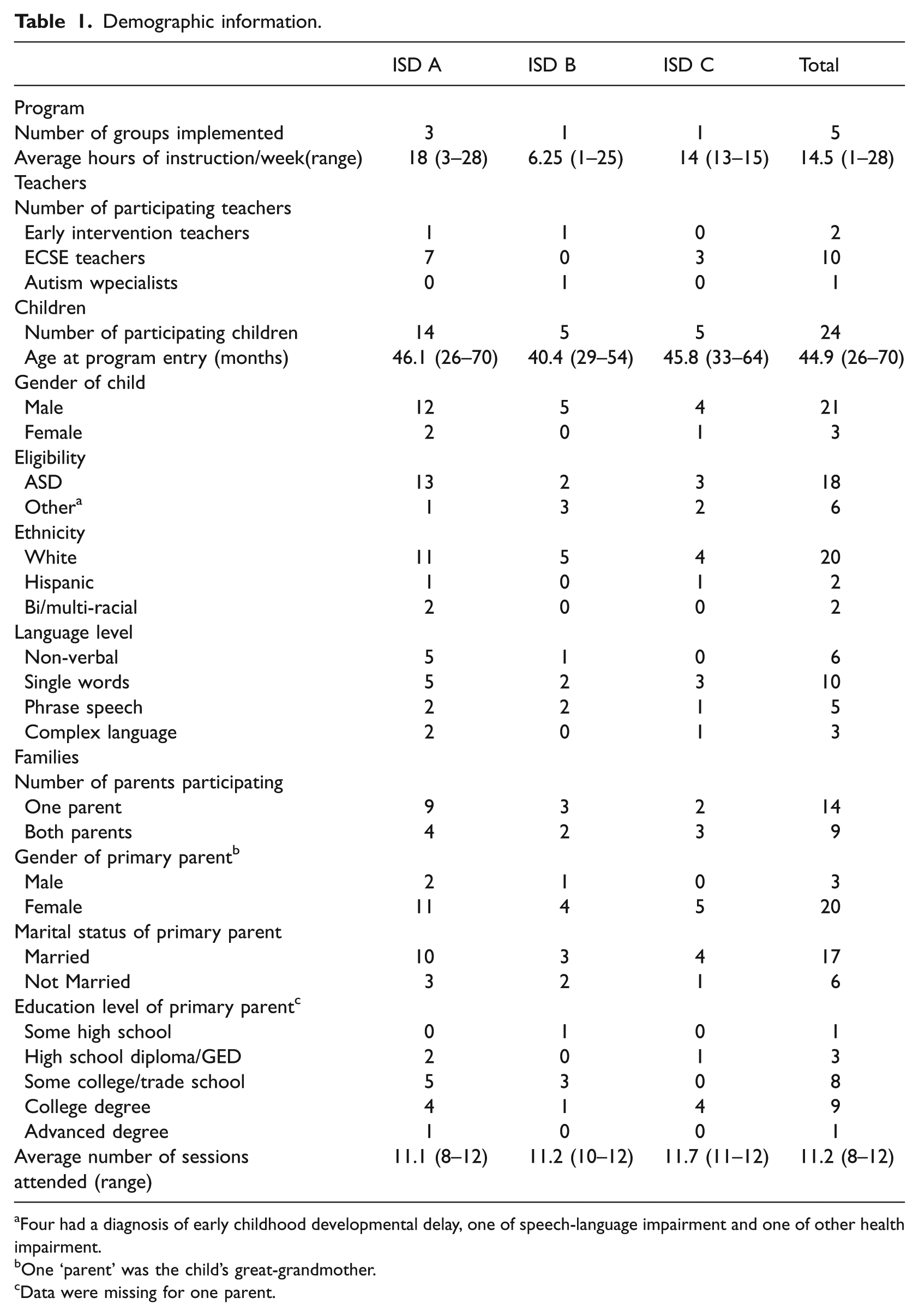
Four had a diagnosis of early childhood developmental delay, one of speech-language impairment and one of other health impairment.
One ‘parent’ was the child’s great-grandmother.
Data were missing for one parent.
Dependent measures
Social-Communication Checklist: Parents completed the Social-Communication Checklist (SCC; Ingersoll and Dvortcsak, 2010) for their child. Teachers completed the SCC for the students on their caseload. The SCC is a skills checklist that was developed to assist in goal setting as part of the program. It contains items that correspond to the skill areas targeted by the curriculum: Social Engagement (10 items), Language (24 items), and Imitation/Play (13 items). Respondents indicate whether the child uses each skill: at least 75% of the time; sometimes but not consistently; or rarely or not yet. Content for each scale was derived from the literature on social-communication development in autism (e.g. Loveland and Landry, 1986; Prizant and Wetherby, 1990; Tager-Flusberg et al., 2009; Ungerer and Sigman, 1981). Summary scores were obtained by summing the number of items for which the respondent indicated the child used the skill at least 75% of the time, and dividing by the total number of items for each content area. Cronbach’s alpha was .90 for Social Engagement, .96 for Language, and .87 for Imitation/Play.
Social Responsiveness Scale: Parents and teachers completed the Social Responsiveness Scale (SRS; Constantino, 2002) to measure changes in the children’s social impairment. The SRS is a reliable and valid parent- or teacher-report measure that assesses autistic social impairment in children appropriate for measuring response to treatment (Matson and Wilkins, 2007). A score of 60 or more is suggestive of clinically significant deficits in reciprocal social behavior.
Parent-child interaction: Parents were observed in their home with their child during free play and a home-based routine (e.g. meal, dressing, going outside). Free play observations averaged 9.81 minutes (range 4 to 17) and home-based routines averaged 3.18 minutes (range 1 to 11). Before each observation, parents were instructed to interact with their child as they typically did during that activity. Inter-rater reliability was obtained for 38% of the parent-child interactions by having two independent coders score the same observation. Reliability was calculated using Pearson’s product-moment correlations.
Parents’ fidelity of implementation was scored during the free play interaction using the ImPACT Fidelity Rating Scale to determine changes in the parents’ use of the intervention techniques. Parents were given fidelity ratings in four areas: Makes Play Interactive, Models and Expands Language or Play, Helps Increase the Complexity of Language, Imitation, or Play, and Paces the Interaction. An Overall Fidelity score was calculated by averaging scores across the four fidelity categories. Inter-rater reliability ranged from .89 to .95 across the five fidelity categories. Child language was coded from the free play and home-based routine interactions using frequency counts to determine changes in the children’s use of language with their parent. Child language was coded as contextually relevant and non-echolalic vocal verbal behavior used while looking at or moving in the direction of the parent or the item that corresponded with the child’s vocal behavior, and included all meaningful child utterances (word approximations, single words, phrases, and sentences). Rate of child language was chosen over a measure of language complexity, such as mean length of utterance (MLU), because it was more directly related to the intervention goal of increasing the number of communication opportunities that parents provide their child. Frequency was converted to a rate per minute by dividing the number of child verbalizations by the total number of minutes of the observation. Reliability for child language was .85.
Parent Stress Index: Parents completed the Parenting Stress Index, 3 rd Edition (PSI; Abidin, 1995) to assess changes in parent stress. The PSI is a 101-item self-report inventory designed to measure stress in the parent-child system. It has strong psychometric properties and has been used in a number of studies of autism and parent training. It contains 13 sub-scales that are grouped into a child domain and a parent domain. Items are rated on a 5-point scale from strongly agree to strongly disagree, with higher scores indicative of more stress.
Behavior Intervention Rating Scale: At post-treatment, parents and teachers completed the Behavioral Intervention Rating Scale (BIRS; Elliott and Treuting, 1991) to assess treatment acceptability of the Project ImPACT Curriculum. The BIRS is a well-validated measure that asks individuals to endorse items that assess the acceptability of a treatment’s procedures and its perceived effectiveness on a 6-point scale, ranging from 1 (highly disagree) to 3 (neutral) to 6 (highly agree). The BIRS was modified to better reflect the goals of the current intervention (acquisition of social-communication skills). Parents and teachers were also asked to rate 6–7 additional items that assessed the usability of the intervention and other potential benefits of the program using the same rating scale as the BIRS. Cronbach’s alpha was .94 for the Acceptability scale, .87 for the Effectiveness scale, .82 for the Parent Usability Scale, and .73 for the Teacher Usability scale.
Intervention
Techniques: Project ImPACT teaches parents to use a blend of developmental and naturalistic behavioral intervention strategies to promote their child’s social engagement, language, imitation, and play during daily routines and activities over the course of 12 sessions. See Ingersoll and Dvortcsak (2006; 2010) for a complete description of the intervention techniques.
Parent training procedure: Parents attended six group and six individual coaching sessions over the course of three to four months. The bi-weekly, 2-hour group sessions involved a didactic presentation of the intervention topics augmented by a slide presentation, video examples, and a written manual, along with group discussion and homework. The week following each group session, parents attended a 45-minute coaching session with their child conducted by the child’s teacher. During coaching sessions, the coach demonstrated the techniques from the previous group session with the child and parents practiced the techniques with their child while receiving feedback from the coach. For the homework, the parents selected a home activity in which to practice the techniques over the next week and answered reflection questions based on their experience (e.g. how they used the techniques, how their child responded). See Ingersoll and Dvortcsak (2006; 2010) for a more detailed description of the parent training procedure.
Four to six families participated in each parent group. ISD A conducted three separate groups, each led by different teaching staff. ISDs B and C each held one parent group. For each group, two to four teachers facilitated the group sessions at a central location at the ISD. Each teacher then provided coaching for their own students. Coaching was conducted either in the empty classroom or another empty room in the building. ISD A held the parent training sessions during the day on teacher preparation days. ISDs B and C held the training sessions in the evening.
Teacher training: Teachers attended a 2-day workshop that provided instruction in the intervention techniques and methods for training parents. Teachers were given the instructor materials, which included detailed instructions for conducting each session, slide presentations and video examples for use during the group sessions, and checklists for use during coaching sessions. One of the authors provided assistance with the first group session for each program and with one to four of the six coaching sessions. For ISD B, all group sessions were conducted by the first author; however, teachers were responsible for conducting the coaching sessions with assistance. Teachers in the same ISD were encouraged to collaborate with each other to conduct the group sessions. Information on teacher fidelity of implementation of the parent training procedure was not collected.
Results
Data analysis
Analyses were conducted using paired sample t-tests (two-tailed) unless otherwise noted. Only children whose families completed the program (n = 24) were included in the analyses 3 . Cohen’s d was used as a measure of effect size.
Treatment feasibility and acceptability
The majority of parents who began the program (89%) completed the training. Of these families, 87% missed two or fewer sessions and 13% missed three or four sessions.
At post-treatment, parents and teachers both rated the program as highly acceptable and effective on the BIRS (Table 2). Parents indicated that the program was highly usable and led to increased social support and improvement in the parent-teacher relationship. Teachers also rated the program as highly usable and indicated that they perceived that the parents learned the targeted skills and that the intervention led to improvements in other parent behaviors.
Treatment acceptability.
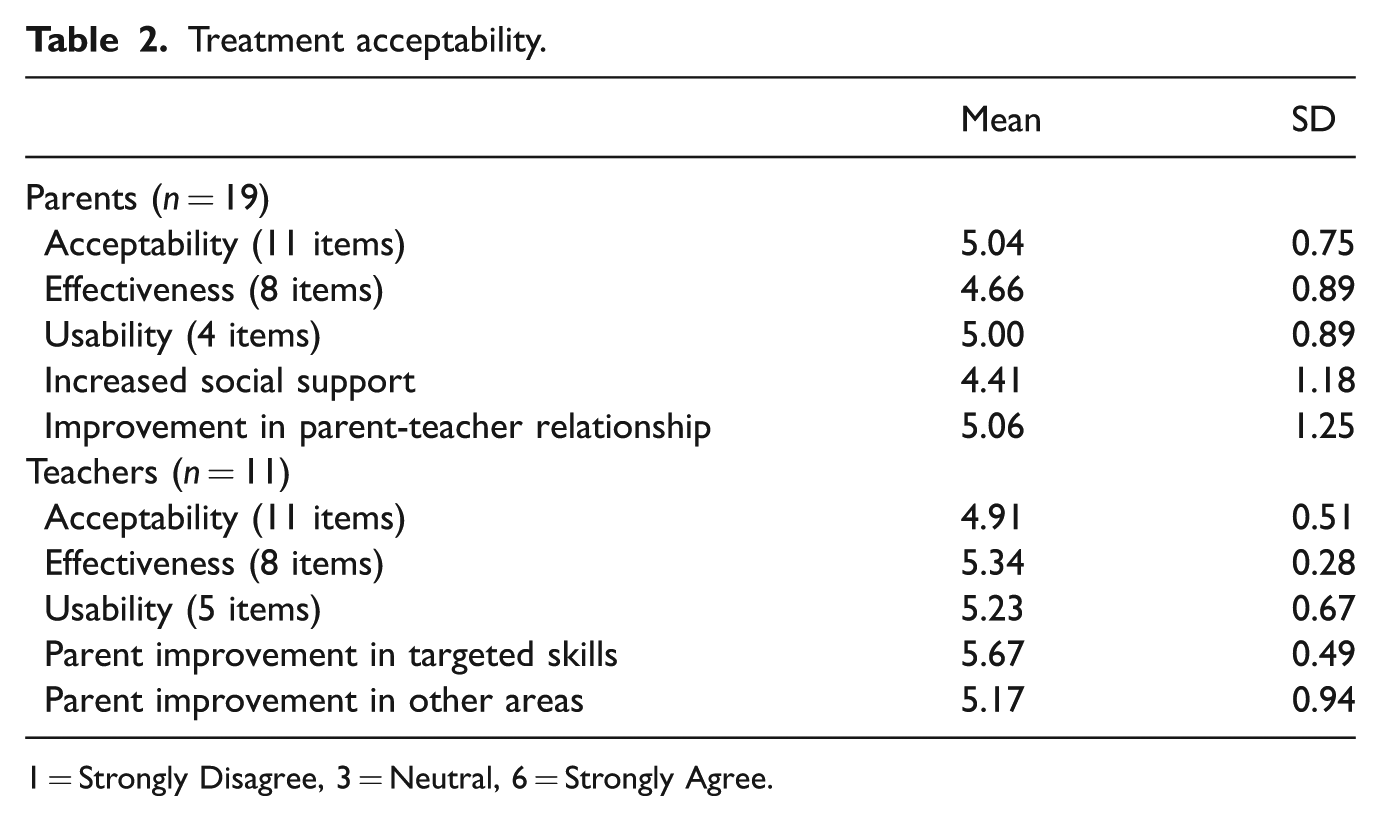
1 = Strongly Disagree, 3 = Neutral, 6 = Strongly Agree.
Parent fidelity
Parents significantly increased their accuracy of implementation of the intervention techniques, across fidelity categories, from pre- to post-treatment: Makes Play Interactive, t(22) = − 5.21, p < .001, d = − 1.09, Models and Expands Language or Play, t(22) = −6.65, p < .001, d = −1.39, Helps Increase the Complexity Language, Imitation, or Play, t(22) = −3.82, p < .001, d = −0.80, Paces the Interaction, t(22) = −4.34, p < .001, d = −0.91, and Overall Fidelity, t(22) = −7.88, p < .001, d = 1.64 (Table 3).
Dependent measures.
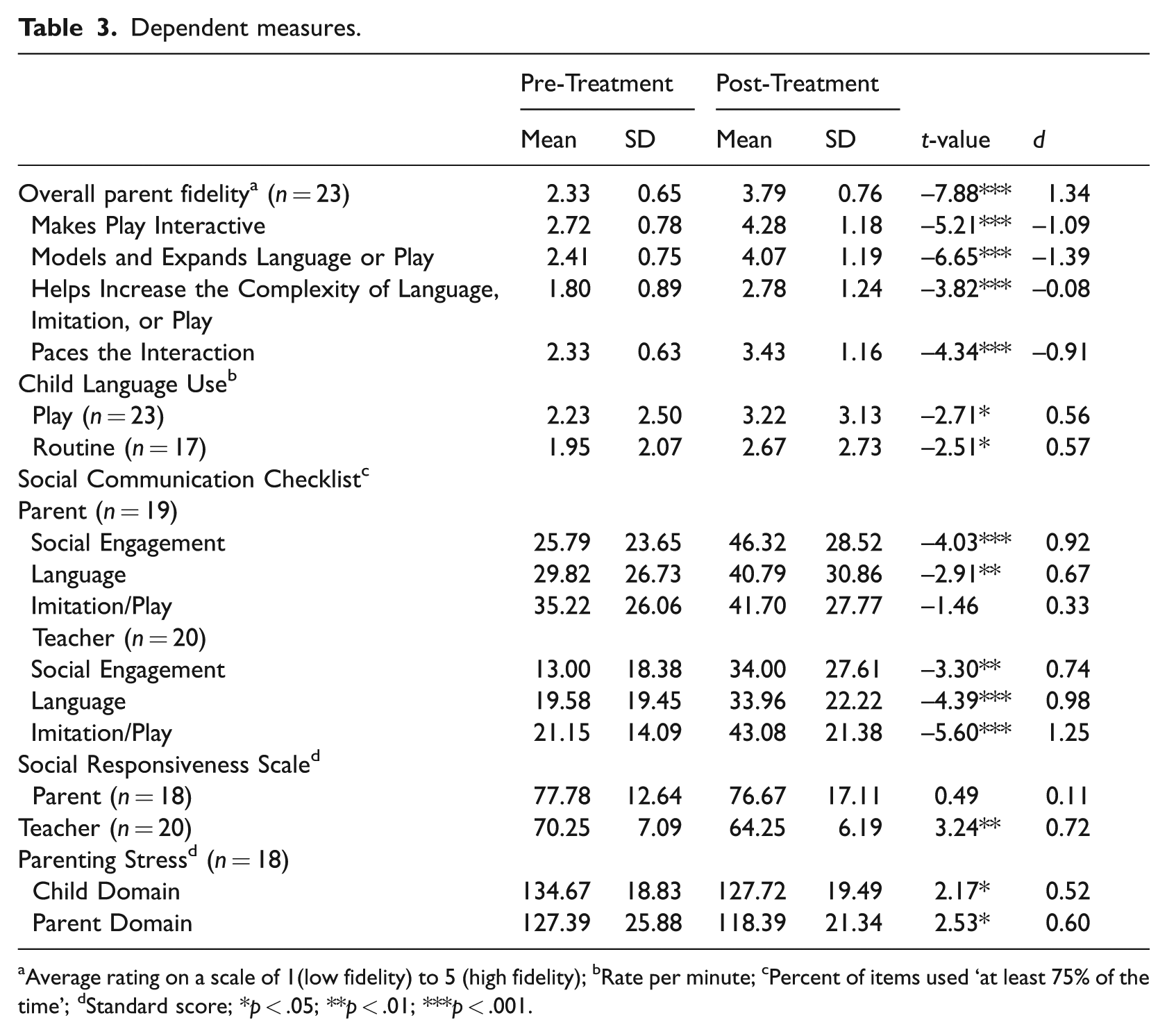
Average rating on a scale of 1(low fidelity) to 5 (high fidelity); bRate per minute; cPercent of items used ‘at least 75% of the time’; dStandard score; *p < .05; **p < .01; ***p < .001.
Child language use
The children used a significantly higher rate of language with their parent during free play, t(22) = −2.71, p < .05, d = .56 and during a home-based routine, t(16) = −2.51, p < .05, d = .57 at post-treatment than pre-treatment.
Social-communication skills
Parents reported that their children used significantly more skills at post-treatment than pre-treatment on the Social Engagement (t(18) = −4.03, p = .001, d = .92) and Language (t(18) = −2.91, p < .01, d = .67) scales of the SCC. There was not a significant difference on the Imitation/Play scale between pre-treatment and post-treatment (t(18) = −1.46, NS, d = .33). Teachers reported that the children used significantly more skills on all three of the SCC scales at post-treatment than pre-treatment: Social Engagement, t(19) = −3.30, p < .01, d = .74; Language, t(19) = −4.39, p < .001, d = .98; Imitation/Play, t(19) = −5.60, p < .001, d = 1.25.
Social responsiveness
Parents did not report a significant decrease in autistic social impairment from pre-treatment to post-treatment on the SRS (t(17) = .49, NS, d = .11). However, teachers reported significantly lower scores on the SRS at post-treatment than pre-treatment (t(19) = 3.24, p < .01, d = .72).
Parenting stress
Parents reported a significant decrease in stress on the child domain (t(17) = 2.17, p < .05, d = .52) and on the parent domain (t(17) = 2.53, p < .05, d = .60) of the PSI from pre-treatment to post-treatment.
Discussion
This parent training program was found to be highly feasible for teachers to implement in EI/ECSE settings. The program was implemented successfully across three separate ISDs, each of which was structured differently, both in terms of classroom composition (ASD only vs. mixed disabilities), number of staff per classroom, and average number of hours of instruction per student. Services also differed across programs within each ISD. Furthermore, 13 different teachers were involved in delivering the intervention, who differed in prior experience with autism interventions and parent training. Thus, our results suggest that this program can be successfully used in a variety of EI/ESCE settings by a variety of teaching staff.
Teacher ratings on the BIRS were positive, with most teachers indicating that they agreed or strongly agreed that that the program led to improvements in child social-communication skills. Most teachers also agreed that the program improved parents’ skills and led to improvements in other parent behaviors such as stress, depression, anxiety, and social support. Teachers also indicated the program was acceptable for use in EI/ECSE settings. Given that treatment acceptability and perceived effectiveness are necessary for long-term program adoption (Wolf, 1978), this finding is important. Teachers also indicated that the program structure, materials, and teacher preparation protocol were adequate to prepare teaching staff to implement parent training as part of the EI/ECSE curriculum.
This program was also highly feasible for parents. Eighty-nine percent of families who began the program completed it. This high rate of completion is comparable to that in laboratory-based studies of parent training for children with autism (e.g. Mahoney and Perales, 2003). Furthermore, the attendance rate, while not perfect, was relatively high, with 87% of families missing fewer than two sessions. In addition, for almost 40% of families, both parents attended at least some portion of the training. The high completion and attendance rates may have been due to the fact that the parents who chose to participate were particularly motivated, because not all parents offered the program chose to enroll.
Parents also rated the program highly in terms of perceived effectiveness and acceptability. The majority of parents reported that they received increased social support and that the program improved their relationship with their child’s teacher. Parents also rated the program highly in terms of usability; most agreed or strongly agreed that the training format was appropriate for learning the techniques, the materials were easy to understand, the amount of training they received was sufficient, and that they used the intervention regularly with their child.
One potential criticism of traditional parent training models for families of children with autism is that they may not be appropriate for many families, particularly those who are highly stressed or socioeconomically disadvantaged (Bernal, 1984; Robbins et al., 1991). Indeed, much of the parent training research with children with ASD has involved a majority of middle-class, well-educated parents participating in university-based training programs (e.g. Brookman-Frazee et al., 2009; Kasari et al., 2010). Although our sample was not particularly ethnically diverse (reflecting the demographics of the ISDs), it was diverse in parent education level, with more than half of the parents having less than a college degree. Furthermore, as the parent training program was implemented within the child’s education program, we had many families who participated who may not have accessed a university-based parent training program. These findings are encouraging and suggest that providing parent training through public EI/ECSE programs may be able to increase access to such services for families of children with ASD.
Parents increased their use of the intervention techniques during a play-based interaction with their child in their home. This finding is encouraging and suggests that group training plus coaching provided in the school setting can lead to improvement in parent use of the intervention in the home. However, many parents still had room for improvement. In particular, parents had the most difficulty mastering the naturalistic behavioral techniques aimed at increasing the complexity of their child’s language, imitation, or play skills. These techniques were introduced in the second half of the program; it is possible that parents struggled because they were still attempting to master the content from the first half of the program. Alternatively, parents may have found it challenging to incorporate more structured teaching strategies (e.g. prompting and reinforcement) into their interactions after practicing the more developmental techniques for several weeks. Finally, it is possible that the naturalistic behavioral techniques take more feedback and coaching than was provided to implement them with a high degree of fidelity. Coaching was provided in the school setting to facilitate the use of the program by classroom teachers who do not have time in their schedule for conducting multiple home visits. However, conducting at least some of the coaching sessions in the home might have improved parent mastery.
The children increased their rate of expressive language with their parent during a play-based interaction as well as a home-based routine (e.g. snack, dressing). Although suggestions were provided for implementing the techniques during daily routines, coaching sessions primarily focused on the use of the techniques during play. Again, these findings are encouraging and suggest that parents can generalize their use of the intervention strategies practiced during play to daily routines, children can generalize their use of language skills learned during play to other interactions, or both.
Improvements in the children’s social communication were also evident on parent- and teacher-report measures. On the SCC, parents and teachers reported an increase in the number of skills mastered in social engagement and language and teachers also reported increases in imitation/play. Furthermore, teachers, but not parents, reported significant decreases in social impairment on the SRS. These data suggest the children made gains in the specific social-communication skills targeted by the program and maybe social reciprocity more generally. It is unclear why teachers reported gains imitation/play on the SSC and social reciprocity on the SRS, but parents did not. It is possible that some child skills are less consistent across interaction partners or environments, leading parents and teachers to make different observations of child skill. Observational measures of child skills in both home and school contexts would help clarify this discrepancy.
In addition, parents reported a significant decrease in child- and parent-related stress over the course of the intervention. This finding is consistent with Tonge et al. (2006), who found a decrease in parenting stress as a result of receiving training in a behavior management intervention. Given the extremely high rates of stress reported by parents of children with ASD, this is an important finding and suggests that a school-based parent training intervention may have benefits that extend beyond the child. Future research that can examine ways in which parent training may influence parenting stress in families of children with ASD is needed.
Limitations
Several limitations of this study are acknowledged. First, the children in this study had an educational diagnosis of ASD and several of the children were receiving services under another eligibility. In these cases, teachers felt strongly that the child would meet criteria for an ASD eligibility, but an official evaluation had not been conducted through the ISD. This was most often the case for children under three. Although these inclusion criteria allow the possibility that some of the children in the sample may not have met DSM-IV diagnostic criteria for ASD, these are the children with whom the intervention is likely to be used in community settings. Therefore, including these children increases the ecological validity of the findings.
Second, although we categorized the children in terms of their functional language ability, we did not have standardized measures of child functioning. We also did not have follow-up data. Furthermore, for each dependent measure, there were missing data. Data were missing for a variety of reasons, including parent discomfort completing a particular measure, teacher discomfort completing measures on an unfamiliar student at intake, lost data, and lack of child cooperation during filming. Missing data did not seem to be systematic and the results were unchanged with imputed data. However, future studies of this program that use standardized and well-validated measures of child functioning and ASD diagnosis, and those that include follow-up data, are necessary. In addition, it would be interesting to examine the impact of this parent training program on different functions of child language use (e.g. requesting versus commenting).
Third, not all families chose to participate. Because the research team received information only from families who expressed interested in the program, it is unclear whether these families differed in meaningful ways from those that chose not to enroll. However, there were no systematic differences between program completers and non-completers in terms of demographic information, child characteristics, or parenting stress. Future research is needed to examine barriers to participation in parent training for families of children with ASD receiving community EI/ECSE services, in terms of both accessing services and completing training.
Fourth, teacher fidelity of the parent training procedure was not collected. This is because teachers implemented the procedures on their own only on days when research staff was not present. Given the parents’ increase in fidelity of implementation, we might assume that the teachers were able to carry out the training procedure as intended. However, additional research is needed on how accurately teachers can implement the parent training procedure after training.
Finally, the use of a pre-post design and parent- and teacher-report measures (which are more likely to be biased) limits the conclusions that can be drawn regarding the causal effect of the intervention on the parent and child outcomes. Both the teachers and parents attributed child gains to the addition of the parent training program, suggesting that some of the changes observed in the children and parents may have been due to the intervention. However, more controlled research using additional objective measures is needed to determine the effectiveness of this approach for increasing social communication in toddler and preschool children with ASD. In addition, given the potential benefit of this program to improve parent-child and parent-teacher relationships, future research should consider more objective and standardized measures of these constructs.
In summary, these data suggest that a parent training intervention targeting social communication can be feasibly implemented in public EI/ECSE programs serving students with ASD. Parents and teachers rated the program highly in terms of treatment acceptability and perceived effectiveness, and preliminary outcome data indicated gains in parent use of the intervention techniques, improvements in child social communication, and decreases in parent stress. These findings indicate that parent training programs for children with ASD can be developed for implementation in these settings and may improve child and parent outcomes when used in conjunction with traditional direct service models. Future research using randomized controlled trials, standard assessment batteries, and long-term follow-up is needed to determine the effectiveness of this program for improving both short-term and long-term outcomes for children with ASD and their families.
Footnotes
Acknowledgements
The authors would like to thank the teachers and families who participated in this project.
Funding
This project was supported by a Michigan State University FACT grant to the first author.