
Abstract
Differences in joint attention are prominent for some children with autism and are often used as an indicator of the disorder. This study examined the joint attention competencies of young children with autism who demonstrated joint attention ability and compared them to children with developmental delays. A total of 40 children with autism and developmental delays were matched pairwise based on mental and chronological age. Videos of children engaging in play were coded for the frequency and forms (eye contact, gestures, affect, etc.) of joint attention. Additionally, concurrent language was compared among children with autism (N = 32) by their joint attention ability. Children with autism spectrum disorder entered into joint attention significantly less often than children with developmental delays, but once engaged used the forms of joint attention similarly. For the matched pairs, there were no differences in language, but the children with autism who used joint attention had significantly better language than children with autism who did not (even after controlling for mental age). There is a group of young children with autism who can use joint attention but do so at lower frequencies than children with developmental delays. Possible reasons include difficulty disengaging attention and limited intrinsic social motivation to share. Adult persistence is recommended to encourage joint attention.
Young children with autism spectrum disorders (ASD) have well-documented deficits in joint attention (JA) (e.g. Mundy et al., 1990; Sigman and Ruskin, 1999; Stone et al., 1997). JA involves two people paying attention to the same object or event and monitoring one another’s attention to that focus (Jones and Carr, 2004). During JA, a pair coordinates their gestures, eye gaze, and other behaviors as they attend to a shared interest. For instance, when a toddler points excitedly to an airplane flying overhead and then glances over at his mother to ascertain that she sees that same plane in the sky, he is initiating joint attention (IJA). IJA refers to the “ability to spontaneously create or indicate a shared point of reference by the use of gestures, or more frequently, alternating gaze between objects or events and other people” (Mundy et al., 2009: 3). When the child’s mother spots the plane above, she will nod and make a comment to show she understands what he is pointing out; this is an example of responding to joint attention (RJA). RJA refers to the “ability to follow the direction of gaze, head posture or gestures of other people and consequently share a common social point of visual reference” (Mundy et al., 2009: 3).
JA skills typically emerge in young children between the ages of 9 and 18 months (Mundy et al., 2007) as they strive to share the world around them. In children with ASD, the development of JA has been found to be absent or delayed (e.g. Mundy et al., 1990; Sigman and Ruskin, 1999; Stone et al., 1997). As a group, these children comment and use JA significantly less often than typically developing children and children with other developmental delays (DD) (Mundy et al., 1990; Stone, et al., 1997; Wetherby et al., 2007), and many young children with the disorder do not engage in JA at all (Watson et al., 2013; Wetherby et al., 2004). Although this is a common deficit, variability has been observed demonstrating that some children with ASD use some manner of JA during play and when interacting with adults (Naber et al., 2008). This capacity to use JA, and the ways in which children with ASD who do use it compared to other children of similar developmental levels, has not been well explored and is the focus of this article.
One of the reasons that JA is clinically important for individuals with ASD involves its relationship to language. JA skills have been found to be associated with children’s language abilities both concurrently and as they age (e.g. Dawson, et al., 2004; Mundy et al., 1990; Murray et al., 2008; Sigman and Ruskin, 1999). This association has been found to be true for typically developing children, children with ASD, and children with other disabilities. Beuker et al. (2013) studied JA in typically developing children. They followed a sample longitudinally from 8 to 24 months of age and found that early JA predicted later language skills, but that early language skill did not predict later JA. Also, children who directed attention with gaze alternation earlier showed greater early growth in vocabulary. Mundy et al. (2007) also looked at typically developing children and found their use of RJA and IJA at 12 and 18 months, respectively, predicted their 24-month language scores and that RJA developed earlier than IJA.
Children with ASD, who tend to engage less in JA than do typically developing children, have the same association between JA and language. Children with ASD who begin with poorer JA have worse language outcomes over time than those who begin with stronger JA abilities (Charman, 2003; Sigman and Ruskin, 1999; Thurm et al., 2007). For children with DD other than ASD, Sigman and Ruskin (1999) looked at children with autism, Down syndrome, other DD, and typical development. They found that both RJA and IJA had a concurrent association with language skills for the children with Down syndrome and other DD, and that RJA (but not IJA) had a significant association with current language skills for the typically developing group.
This association with language is likely because the nonverbal communication skills that are used to share attention play an important role in the later development of verbal comprehension (Thurm et al., 2007). Children who participate in fewer JA bids have correspondingly fewer opportunities to take part in social communication events or to get practice in language interaction. In contrast, those who use JA more frequently have increased opportunities for adults to describe and verbally expand on their shared interests. For example, a child who frequently points things out to an adult is likely to get responses that are attuned to his or her focus of attention (e.g. a parent might say, “It’s an airplane. Yes, I see the airplane flying up in the sky. It’s making a lot of noise …”), providing a language-rich interaction for the child.
JA is so vital to early language learning that it may be a pivotal skill needed for language to develop normally (Mundy and Crowson, 1997). A pivotal skill is one that, when improved, causes positive changes in other areas of functioning (Koegel et al., 1999). Recent intervention studies support this pivotal skill theory. By teaching young children with ASD to use JA, researchers have seen downstream improvements in their language (Jones et al., 2006; Kasari et al., 2008; Schertz et al., 2012).
JA ability is used to differentiate children with ASD from other disabilities. The American Academy of Pediatrics recommends observing JA at early well-child visits because they state, “Deficits in JA seem to be one of the most distinguishing characteristics of very young children with ASDs” (Johnson et al., 2007: 1191). It is used in both early screening tools like the Checklist for Autism in Toddlers (CHAT, Baron-Cohen et al., 2000) and the Modified Checklist for Autism in Toddlers (M-CHAT, Robins et al., 2001) and in more in-depth diagnostic tools like the Autism Diagnostic Observation Schedule (ADOS, Lord et al., 1999; ADOS-2, Lord et al., 2012). The children who fail the JA questions are considered to have an elevated risk of ASD.
Utilizing the JA deficit as an indicator of ASD in young children works because, by and large, only children with autism fail the JA items, whereas typically developing children and those with other DD usually pass them. The CHAT and other early screening tools that depend on JA probes (in combination with other key items like imitation and pretend play) have excellent specificity, that is, the children who fail these screens are very likely to have an ASD (Baird et al., 2000). Therefore, failing JA or imitation probes uniquely discriminates children with autism from other groups (Sullivan et al., 2007). On the other hand, there are some children with ASD who pass the JA probes who are missed by early screening tools and may be somewhat masked on the diagnostic tools. Although an early JA deficit is a good indicator of ASD, the observation that a child engages in JA should not rule out the diagnosis.
This seemingly dichotomous nature of JA in ASD can be clarified by noticing that children with the disorder acquire JA at different rates and competency levels. Some of the children who initially lack JA may develop skills as they mature. Mundy et al. (1994) found that children with autism were initially delayed in their JA development, but by 30 months their RJA skills were similar to those of typically developing children. Similarly, Naber et al. (2008) reported that at 24 months, children with ASD used significantly less JA than a comparison group of children with DD, but by 48 months, the two groups had very similar levels of JA use. Paparella et al. (2011) found that children with autism developed JA skills later than typically developing children, and those who learned to use JA followed a different developmental sequence. What is still unknown is what the JA is like for the children with ASD who acquire the skill. When they begin to use JA, is it in the same ways as other children or do children with ASD use JA distinctively?
The main purposes of this study were to explore whether children with autism use JA in a syndrome-specific way when compared to children with DD of similar developmental levels and to see whether the language of young children with autism is impacted by their JA ability. For this study, we took a careful look at the JA abilities of children with autism, with particular interest in those who did respond to JA. We had three hypotheses. We hypothesized that children with autism would (1) use JA differently than children with DD and at much lower frequencies; (2) have inferior language skills than the children with DD, in association with the less frequent JA use; and (c) we surmised that some young children within the diagnosis of autism would use JA and correspondingly would have better concurrent language than their peers who did not use JA. We hoped to find out whether there was an autism-specific pattern of JA use and suggest reasons why children with ASD might use JA differently than their peers.
Methodology
Participants
This study involved a subset of data collected for a larger study that focused on patterns of responses to sensory stimuli. For the larger study, 2- to 7-year-old children with ASD were recruited along with comparison samples of children with DD not associated with autism and children with typical development. This study included only the children with autism and those with DD.
To be included in this study, the children with autism had a clinical diagnosis of an ASD and met strict criteria for a diagnosis of autistic disorder on both the Autism Diagnostic Interview–Revised (ADI-R; Lord et al., 1994) and the ADOS (Lord et al., 1999). Consistent with the larger study from which these participants were drawn, children who met the lower cut-off for ASD or other variant of autism like Pervasive Developmental Delay–Not Otherwise Specified (PDD-NOS) were not included in the autism group in this study.
The children with DD had a clinical diagnosis of intellectual disability or developmental delay, including an overall cognitive score that was 2 or more standard deviations below the mean in one area or scores that were at least 1.5 standard deviations below the mean on two separate areas of development. These children had no clear symptoms of autism, spectrum disorders, as confirmed by not meeting autism spectrum cut-offs on the ADOS or the Childhood Autism Rating Scale (Schopler et al., 1988). Examples of the children in the DD group included children with Down syndrome, children with other genetic syndromes with no known association with autism (e.g. Williams syndrome), and children with non-specific developmental disabilities including idiopathic intellectual disability.
Because the focus of this study was on JA, only children assessed with the ADOS Modules 1 and 2 were considered for inclusion in the analyses because these two modules include specific activities designed to assess JA. For the purposes of our analyses, RJA ability was determined for each child (see section “Procedure” for more details on this process). Once RJA ability groups were identified, two analyses were undertaken.
Analysis 1
Analysis 1 was a video analysis that included 40 children. These children consisted of 20 with autism and 20 with DD. The sample size was determined based on a power analysis, which indicated that 20 matched pairs would provide a power level of 0.70 for detecting an effect size of d = 0.5. All of the children demonstrated RJA ability on two tests of JA. The 20 pairs were created to be as closely matched as possible based on nonverbal mental age (NVMA) scores and chronological age. Resulting pairs were on average within 2 months of one another on NVMA and within 12 months of each other on chronological age. Table 1 shows a description of the children included in Analysis 1.
Demographics for participants in Analysis 1.
SD: standard deviation.
The nonverbal mental age score is from the Mullen Scales of Early Learning Visual Reception scale.
Analysis 2
Analysis 2 examined the concurrent language of the children with autism. This study examined 32 children with autism, which included all of the children from the larger study sample with NVMA scores below 30 months. The NVMA cut-off of 30 months was chosen for this analysis, because at NVMAs of more than 30 months, all children with autism demonstrated RJA, whereas below a NVMA of 30 months, there was within-group variability in whether children demonstrated RJA or not. The children were grouped by their RJA ability; half of the children demonstrated RJA (N = 16) on two tests of JA and half did not. Table 2 has demographic information describing this sample.
Demographics for children with autism in Analysis 2, by responding to joint attention (RJA) ability.
SD: standard deviation.
Measures
With the exception of the ADI-R (Lord et al., 1994), which was only administered for children with a clinical diagnosis of ASD, children in both groups were assessed with each measure.
ADOS
The ADOS is a semi-structured direct assessment measure that employs a series of probes called “presses,” which are planned interactions designed to elicit and observe autism symptoms (Lord et al., 1999). The ADOS Modules 1 and 2 (used in this study) include several JA probes. In particular, this study utilized the RJA probe to classify children into JA ability groups. This probe involves an examiner gaining the child’s attention by calling his or her name. Then the examiner says, “Look!” and turns his or her head deliberately toward a new object across the room. The bid can be repeated up to three times, adding a point toward the object if the child does not initially respond. The RJA is scored as 0 or 1 when the child responds to a JA bid (when the child follows just the examiner’s eyes/gaze without needing a point they get a score of 0; when the examiner uses a point and the child follows it, they get a score of 1). If the child does not respond to either the examiner’s gaze or point, they get a score of 2 or 3. On the ADOS, a higher score on any item indicates more impairment.
ADI-R
Those that met criteria for an ASD were also evaluated with the ADI-R (Lord et al., 1994). (Children with other DD were not assessed with the ADI-R.) The ADI-R is a caregiver interview that provides a diagnostic algorithm based on lifetime history of symptoms as well as an algorithm score for current symptoms. Research staff administering the ADOS and ADI-R obtained research-appropriate levels of reliability with a University of Michigan Autism and Communication Disorders Center (n.d.)–certified examiner, and reliability of scoring was checked by the certified examiner on a minimum of 20% of assessments throughout the study.
Mullen Scales of Early Learning
The Mullen is a standardized, examiner-administered measure of cognitive functioning for children from birth up to 68 months of age (Mullen, 1995). A NVMA score was determined for each participant using the Visual Reception (VR) scale of the Mullen. The VR scale primarily tests visual discrimination and visual memory skills. We utilized the VR age equivalent (AE) scores as an estimate of NVMA.
Preschool Language Scale, 4th edition
The Preschool Language Scale, 4th edition (PLS-4) is a standardized language test composed of two subscales: Auditory Comprehension and Expressive Communication (Zimmerman et al., 2002). The Auditory Comprehension subscale includes items tapping attention, understanding of gestures, vocabulary, concepts, grammatical markers, syntactic structures, and narratives, as well as phonological awareness. The Expressive Communication subscale includes items assessing a child’s vocal development; use of gestures; ability to name objects; express concepts (e.g. descriptors, quantity); use prepositions, grammatical markers, and syntactic structures appropriately; and narrative production as well as phonological awareness. The specific items administered to a child will depend on his or her language development level. The PLS-4 is designed for use with children from birth through 6 years, 11 months. The language scores that we used as an outcome measure were taken from the Total Language-AE score from the PLS-4.
Attention Following and IJA protocol
The Joint Attention Protocol (Watson et al., 2003) examines RJA and IJA directly and repeatedly. It was developed based on JA tasks used by other investigators (Brady et al., 2005; Leekam et al., 1998; Mundy et al., 2003; Stone et al., 1997) with four goals: (1) a specific focus on measuring response to and initiation of JA; (2) reliable and efficient scoring during administration rather than requiring later video coding; (3) interaction contexts that would appeal to children across a range of ages and functioning levels; and (4) measurement of variability in performance within and between groups of children. Although based largely on previously developed measures, no single previous measure of JA met all of these criteria, so this measure combines and extends them to meet the four goals mentioned above. The Joint Attention Protocol includes an Attention Following subscale that includes eight trials that directly assess RJA. Children are asked eight times to respond to the examiner’s bid for shared attention, alternating between directing attention to the left and right of the child, and using increasing prompts on every second trial (i.e. the examiner silently looks to an object in the first set of trials, looks with a point on the second set of trials, looks with a point and says, “Look!” on the third set of trials, and then looks with a point and says, “Look (NAME OF OBJECT)” on the last set of trials). The Attention Following trials are interspersed with eight trials to provide contexts for IJA.
The reliability and concurrent validity of the Joint Attention Protocol are strong (Watson, in preparation). Inter-rater reliability (N = 53) between two raters was substantial (Total JA Score: 87.9% exact agreement and kappa = 0.749; Attention Following: 91.3% exact agreement and kappa = 0.831; IJA: 82.8% exact agreement and kappa = 0.666). Internal consistency is also high, with Cronbach’s alpha = 0.99 for the Attention Following subscale and 0.98 for the IJA subscale. Also, despite the limited range of scores for JA items on the ADOS, a Spearman correlation between the Attention Following score on the Joint Attention Protocol and the RJA item on the ADOS yielded a rho (98) = −0.744, p < 0.001, and similarly, the correlation between the IJA subscale score and the ADOS combined scores for the spontaneous initiation of JA item and the showing item was rho (103) = 0.89, p < 0.001.
Procedure
Identifying RJA ability
Two tests of JA were administered to identify children who engaged in RJA. The scores from (1) the ADOS’ RJA probe and (2) the Attention Following subscale from the Joint Attention Protocol (see section “Measures” for additional information regarding these assessments) were used to classify children into RJA ability groups. The children who responded to RJA bids on these measures were placed in the Yes-RJA group and the children who did not respond were placed in the No-RJA group. There was a high agreement in grouping between the Joint Attention Protocol and the RJA score from the ADOS; there was only one child from each JA ability group who met criteria on one of the measures but not on the other. In these two cases, the RJA score from the ADOS was used for the purposes of classification.
Using RJA to differentiate JA groups was done for three reasons. First, in RJA the child needs only to respond to what is being asked of him and not originate a behavior (as he or she would in IJA). Second, all of the children in this study who had IJA skills also had RJA skills, but the converse was not always true, that is, many children with autism who were able to respond to JA did not initiate. Finally, RJA was relatively straightforward to test in that they either looked or reacted in some way when asked to follow an adult’s attentional bid or they did not.
Analysis 1
Analysis 1 was a video analysis designed to compare the JA skills of children with ASD to children with DD.
Power and effect size
For Analysis 1, a power analysis was completed to determine how many participants would be needed if the data were analyzed by matched pairs. Pairwise matching eliminates some of the variability between groups that might affect outcome measures and thus provides a gain in power. To detect a medium effect size of 0.5 (with an alpha of 0.05 and a one-tailed test) at a power level of 0.7, 20 matched pairs were required. Thus, 40 participants (20 from the autism group matched with 20 from the DD group) were included in the video analysis.
Matching
There were a total of 38 children with autism and 34 children with DD who exhibited RJA skills and could be considered for inclusion in matched pairs for Analysis 1. None of the children with autism with NVMAs above 50 months had a potentially close match in the DD group based on a reasonable similarity in both NVMA and chronological age. This left 27 children with autism, and 28 with DD, all with NVMA scores below 50 months. Four children had problems with their videos (e.g. there was an error in the taping or an obstructed view of the child) and could not be included. Based on the power analysis above, 20 matched pairs were created from this pool, with children matched as closely as possible in terms of both NVMA and chronological age.
Matching was done initially on NVMA because mental age is correlated with JA ability and language (Charman et al., 2003). A total of 17 children from the autism group were matched to children from the DD group who had NVMA scores within 3 months of one another. The remaining three pairs were matched within 4–6 months of one another. Most matches had chronological ages within 12 months of one another (16 of the 20 pairs). Additionally, each girl with autism (N = 3) was matched with a girl from the DD group who had the most similar NVMA and chronological age. The remaining girls with DD (N = 5) were matched to boys from the autism group. The remaining children did not have suitable matches.
Video analysis
Trained doctoral students coded two video clips of children engaged in semi-structured play designed to elicit JA; the video clips were drawn from scenes from the ADOS, during which a parent and an examiner were present. These play scenarios were designed to provide contexts to press for RJA and IJA from the children (the Bubble Play and the Mechanical Bunny scenarios). During each scenario, the children were able to move freely around the room and interact with the play items. This allowed opportunities for spontaneous IJA, which can be difficult to tap in a structured testing setting. The ADOS protocol also allowed children to choose to initiate to their parent or to the examiner. Although there is flexibility in the timing and technique of how probes are administered, the examiner uses a specific set of items and prompts for all children, thus providing contexts for comparing JA across children.
Video coding procedures
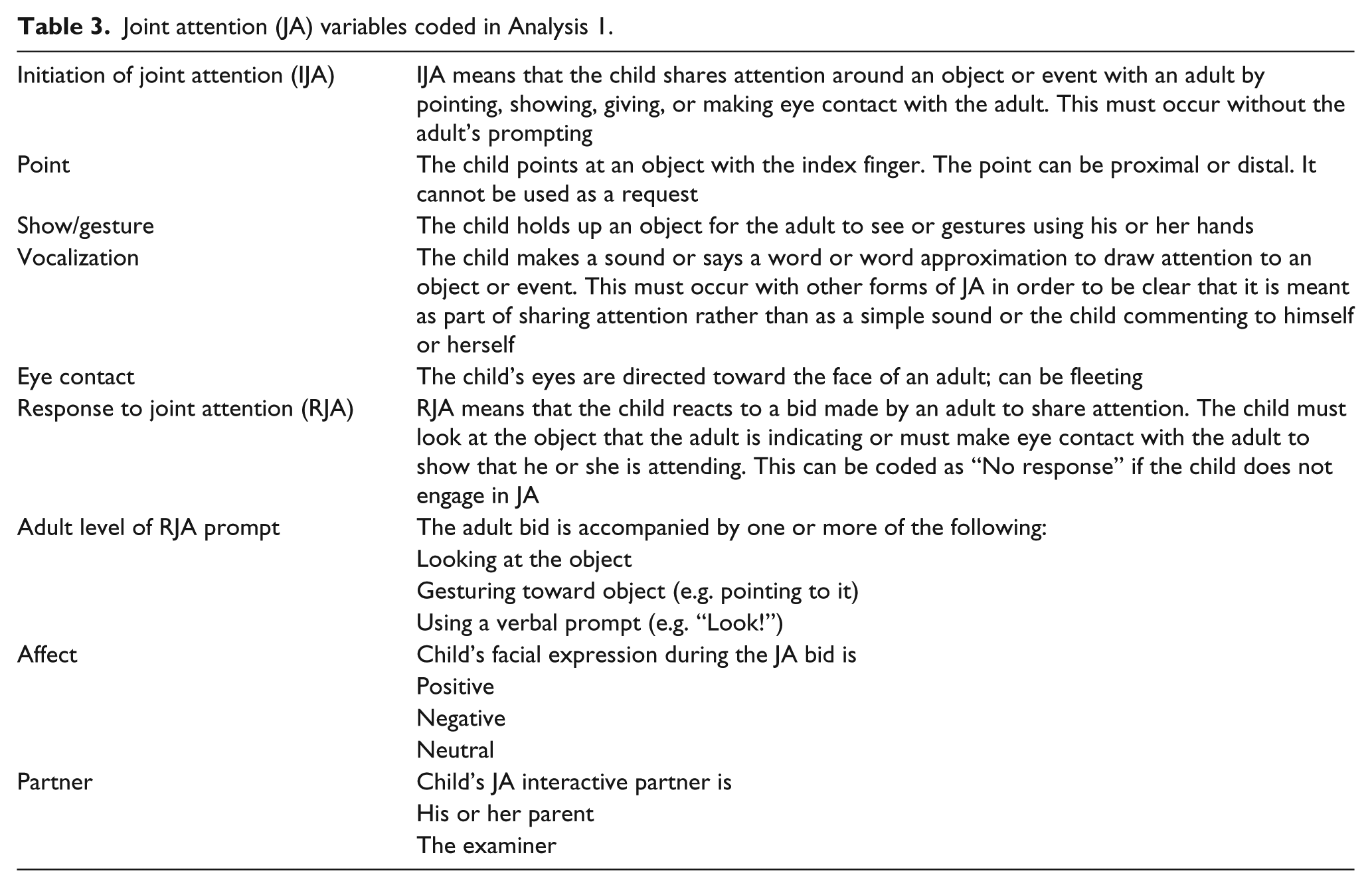
For the children’s videos, each instance of RJA or IJA was coded. Every time a JA bid was initiated by either the child (IJA) or an adult (providing an opportunity for RJA), the video was stopped, the event and time recorded, and then that part of the video replayed so that the details of the bid could be examined. Of particular interest were the following: if gestures, eye contact, or vocalizations were used, what facial affect the child exhibited during the bid, and the adult partner with whom the child interacted (i.e. the parent or the examiner). Table 3 describes some of the JA characteristics coded in this study. A coding manual providing details about the coding procedure is available from the first author.
Joint attention (JA) variables coded in Analysis 1.
The start and end time for each scenario was recorded to provide a total time for each coded session. There could be variation in the length of the video clips depending on whether the child was very engaged, if he or she showed disinterest or fatigue, how quickly the examiner got the required information, and other related factors, and this time variation was taken into account during the analysis of the data.
Inter-rater agreement
After establishing reliability of at least 80% exact agreement on three consecutive practice tapes with the first author, a research assistant coded 100% of the videos. The research assistant, a doctoral student in education, was hired to perform this analysis and did not participate in any of the original data collection. She was blind to diagnosis and did not know which cases constituted the matched pairs. She was provided with a list of ID numbers, in no particular order, to code. The first author coder coded 20% of the videotapes for reliability purposes. The tapes to be coded by both people were chosen at random, and diagnostic group membership of the children was not accessed before coding the tapes.
Intraclass correlations (ICCs) were used to document reliability between observers (Osterling et al., 2002). The ICCs for variables of interest were as follows: RJA bids offered by adult (0.94), RJA no response by child (0.88), RJA look by child (0.79), RJA eye contact (0.97), RJA gesture (0.63), RJA vocalization (0.85), RJA affect neutral (0.88); IJA bids initiated by child (0.95), IJA point (0.96), IJA show/give (0.83), IJA eye contact (0.97), affect positive (0.93), affect negative (0.80), partner parent (0.91), and partner examiner (0.94).
Statistical analyses
The matched pairs were analyzed to see how the groups compared in three main areas: (1) the broad RJA levels and the forms of RJA used, (2) the broad IJA levels and the forms of IJA used, and (3) the associations with children’s concurrent language. To determine whether matched pairs from the two diagnostic groups used RJA in different ways, a repeated-measures logistic regression was used. For the broad IJA examination, the IJA bids made over time were analyzed using a repeated-measures log-linear Poisson regression that adjusted for time (the log of time was used as an offset to account for the varying lengths of time children were observed).
All statistics were run in SPSS 16.0 for the Mac.
Analysis 2
Analysis 2 was designed to compare the concurrent language of children with autism who used RJA to children with autism who did not. Children with autism were grouped by RJA ability, and their concurrent language scores were compared. We chose to limit this analysis to children with NVMA scores below 30 months because above this age coordinating attention and symbol use are typically consolidated (Adamson et al., 2009) and many children have learned to use JA, meaning there is much less variability.
In order to compare the two RJA ability groups, t-tests were conducted with concurrent language as the outcome measure. Language scores were taken from the Total Language-AE score from the PLS-4.
In addition, after seeing that there were slight differences in NVMA, we ran an analysis of covariance (ANCOVA) to control for the potential effects of NVMA.
Results
Analysis 1
RJA grouping and matching
Out of the original sample of 55 children with autism, 38 (69%) met criteria to be included in the RJA subgroup. Out of our original sample of 37 children with DD, 34 (92%) met criteria to be included in the RJA subgroup. In all, 20 matched pairs of these children were made. There were no significant differences in NVMA or chronological age for the pairs of children with autism and DD. Due to the pairwise matching and resulting close comparability of the groups on these variables, neither NVMA nor chronological age was used as covariates in the subsequent analyses.
Broad RJA analyses
Based on the video analyses, the pairs of children did not significantly differ on their RJA ratio scores, which represented the number of bids they responded to divided by the number of bids that were offered by an adult, χ2(1, N = 40) = 1.416, p = 0.234. It is likely that ceiling effects impacted these results, because 29 of the 40 children had RJA ratios of 1.00 (i.e. they responded to every bid that they were offered).
A further examination of RJA revealed two interesting points. First, the adults offered the children with autism significantly more RJA bids than they did to children with DD, group means of 3.65 bids (SD = 1.84) and 1.95 bids (SD = 1.05), respectively, t(38) = 3.58, p = 0.001. To examine this relationship within the matched pairs, a repeated-measures logistic regression was run with “JA bids offered by adult” as the outcome. Adults offered significantly more JA bids to children with autism than to their matched partners with DD, χ2(1, N = 40) = 15.17, p < 0.001. To be specific, in 16 of the 20 pairs, the adults made more attempts to engage children with autism in JA than children with DD; for two pairs, an equal number of JA bids were made, and for two pairs, adults made more bids to the children with DD than to the children with autism. Figure 1 depicts the number of JA bids offered by adults.
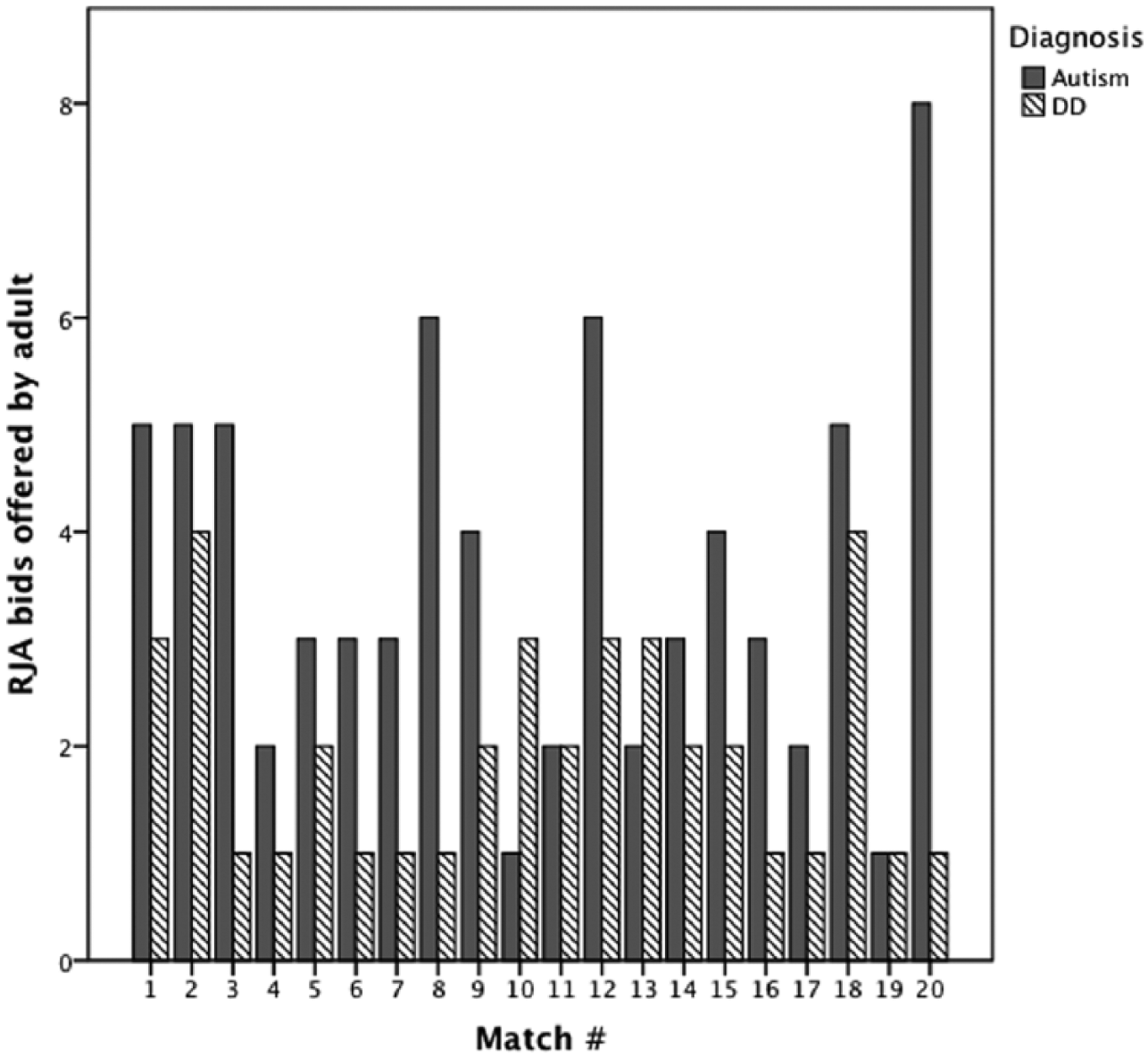
Number of JA bids offered by adults to each child in Analysis 1, grouped by matched pairs.
Second, although all of the children in this analysis responded to at least one of the JA bids made by an adult, 45% of the children with autism failed to respond to some RJA bids. In contrast, only 10% of the children with DD failed to respond to some RJA bids. There was a significant difference for “No response” to a RJA bid, based on a repeated-measures logistic regression, χ2(1, N = 40) = 4.43, p = 0.035. To summarize, children with autism were offered significantly more JA bids than those with DD and many of the children with autism did not respond to one or more of those bids.
Examination of RJA characteristics
The forms of RJA children used when they were engaged in a bid were examined. Children were compared on whether they made eye contact, where they looked, what gestures they used, whether they vocalized during the bid, and their facial affect. Facial affect was overwhelmingly neutral for both groups with only a few smiles seen (from five children in the autism group and only two in the DD group). Negative affect was rare (seen on fewer than four children in each group). The only area of significant difference in the RJA profiles of the two groups was that the children with autism vocalized significantly more than their matched pairs with DD, χ2(1, N = 40) = 7.46, p = 0.006. Otherwise, once children were engaged in RJA, there were no significant differences in the amount of eye contact children used, in their facial affect (positive or negative), or in the use of looks or gestures.
Broad IJA analyses
The IJA scores for the children with autism were compared to the children with DD. Children with autism initiated JA significantly less frequently per minute than those with DD, χ2(1, N = 40) = 4.434, p = 0.035. Figure 2 depicts the number of IJA bids made per minute by each child in the study.
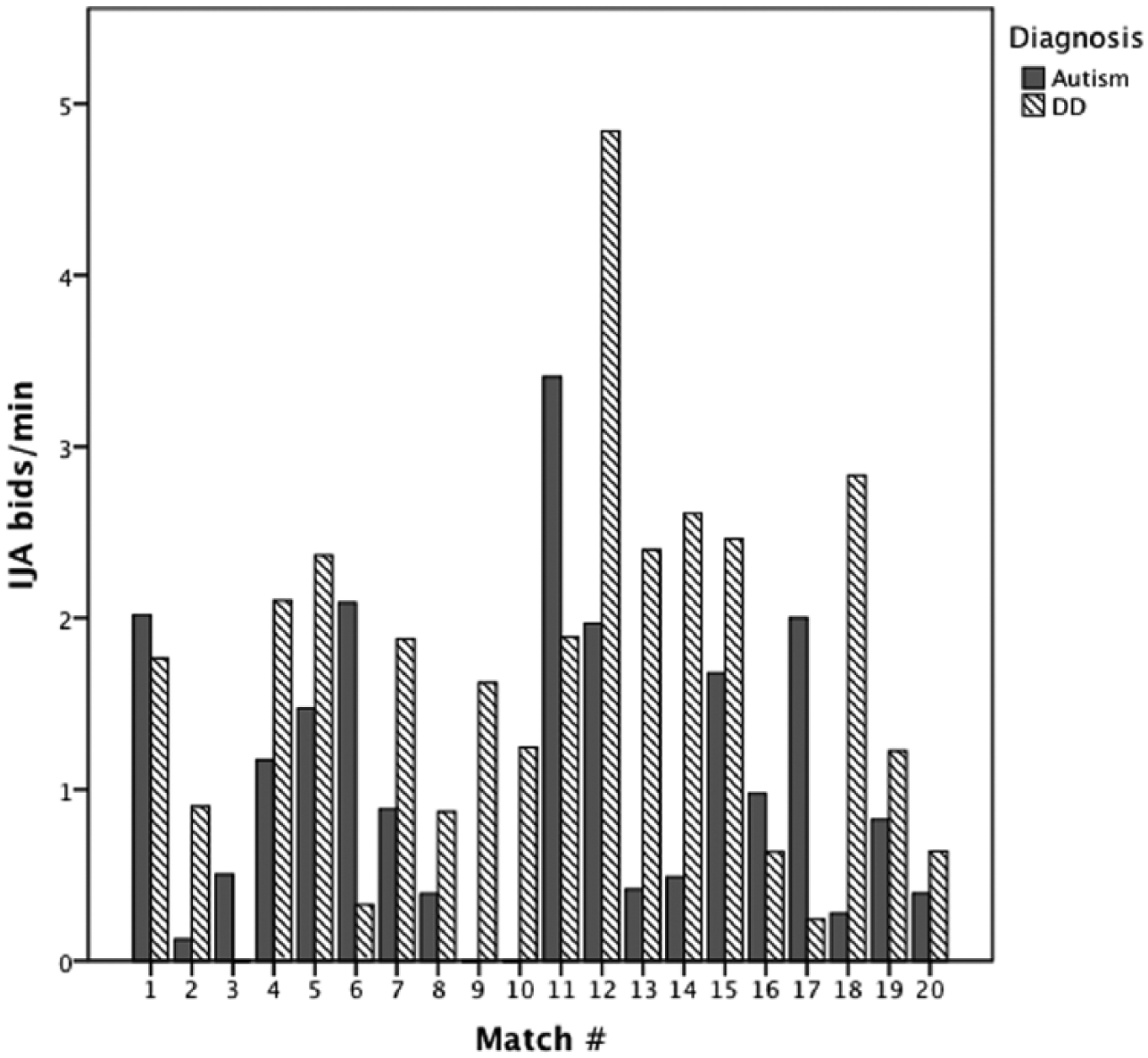
Number of JA bids initiated by each child in Analysis 1, grouped by matched pairs.
Examination of IJA characteristics
The forms of IJA that children used when they were engaged in an IJA bid were examined. There were no significant differences in the type, or variety of bids, or the rate with which children with autism and children with DD used different forms of IJA. To be specific, when children initiated a bid, those with autism were equally likely to point, show, or use other gestures as those with DD and their levels of eye contact, and type of facial affect was all similar. Only a few children from either group pointed (five from each group), although almost all of the children made eye contact with an adult (17 with autism and 19 with DD) and many did so repeatedly. Affect was more positive during IJA bids than it was during RJA, as children appeared excited about the activity they were sharing. Most children showed positive affect (13 from the autism group and 15 from the DD group) and only three children from each group had negative affect during an IJA bid. There was no significant difference between the groups regarding whom bids were directed to (i.e. toward the parent or examiner).
A note regarding vocalizations: during IJA bids, children from both groups used vocalization similarly (15 of the children with DD and 11 children with autism vocalized), in contrast to greater use of vocalizations to accompany RJA by the children with autism.
Association with concurrent language scores
The concurrent language scores were compared for the matched pairs of children. The average language scores were not significantly different for the two groups; for children with autism, the mean language score was 24.10 (SD = 11.29, range: 11–50) months, and for children with DD it was 27.40 (SD = 13.41, range: 12–54) months, χ2(1, N = 40) = 3.07, p = 0.080.
Several correlations were examined. The NVMA scores and concurrent language scores were highly correlated with one another, r(38) = 0.78, p < 0.001. Finally, both of the scores from the Joint Attention Protocol (the Attention Following score that measures RJA and the Initiation score that measures IJA) were correlated with concurrent language. The correlation between Attention Following score from the Joint Attention Protocol and language, by group, was as follows: autism, r(18) = 0.51 p = 0.023; DD, r(17) = 0.46 p = 0.047. The correlation between the Initiation score from the Joint Attention Protocol and language, by group, was as follows: autism, r(18) = 0.46, p = 0.039; DD, r(17) = 0.53, p = 0.020.
Analysis 2
The language among children with autism, separated by their RJA group, was analyzed. From the original sample of 55 children with autism, 32 children had NVMA scores below 30 months, and half of them demonstrated RJA (N = 16). All of the children with autism who had NVMA scores above 30 months (N = 23) demonstrated RJA ability.
The average chronological age for the group of children with autism who used RJA was the same as for those who did not (chronological age approximately 43.00 months for both subgroups). The average NVMA was 13.25 for those who did not use RJA and 17.75 for those who did. This was not significantly different for the groups, but the significance value was just above the 0.05 cut-off, NVMA = t(30) = −1.98, p = 0.057 (Cohen’s d = 0.70 and r = 0.33, indicating a medium effect size).
The language scores for children with autism with NVMA below 30 months were compared based on their RJA ability. The language scores differed significantly between the two groups (Figure 3 depicts this comparison). The mean Total Language-AE score for the group that did not show RJA ability was 9.25 (SD = 3.86), and the mean for the group that demonstrated RJA ability was 17.06 (SD = 5.26). To begin, t-tests were run with language scores as the outcome measure. The RJA ability group had significantly higher language scores than the group that did not show RJA, t(30) = −4.79, p < 0.001 (Cohen’s d = 1.69 and r = 0.646, which represents a large effect size). Since the NVMA could have had an impact on the outcome, the analysis was re-run using an ANCOVA to control for the potential effects of mental age on language. Mental age significantly affected the model, F(1, 29) = 13.20, p = 0.001. After controlling for NVMA, the groups still differed significantly on language, F(1, 29) = 21.51, p < 0.001 (effect size r = 0.43).
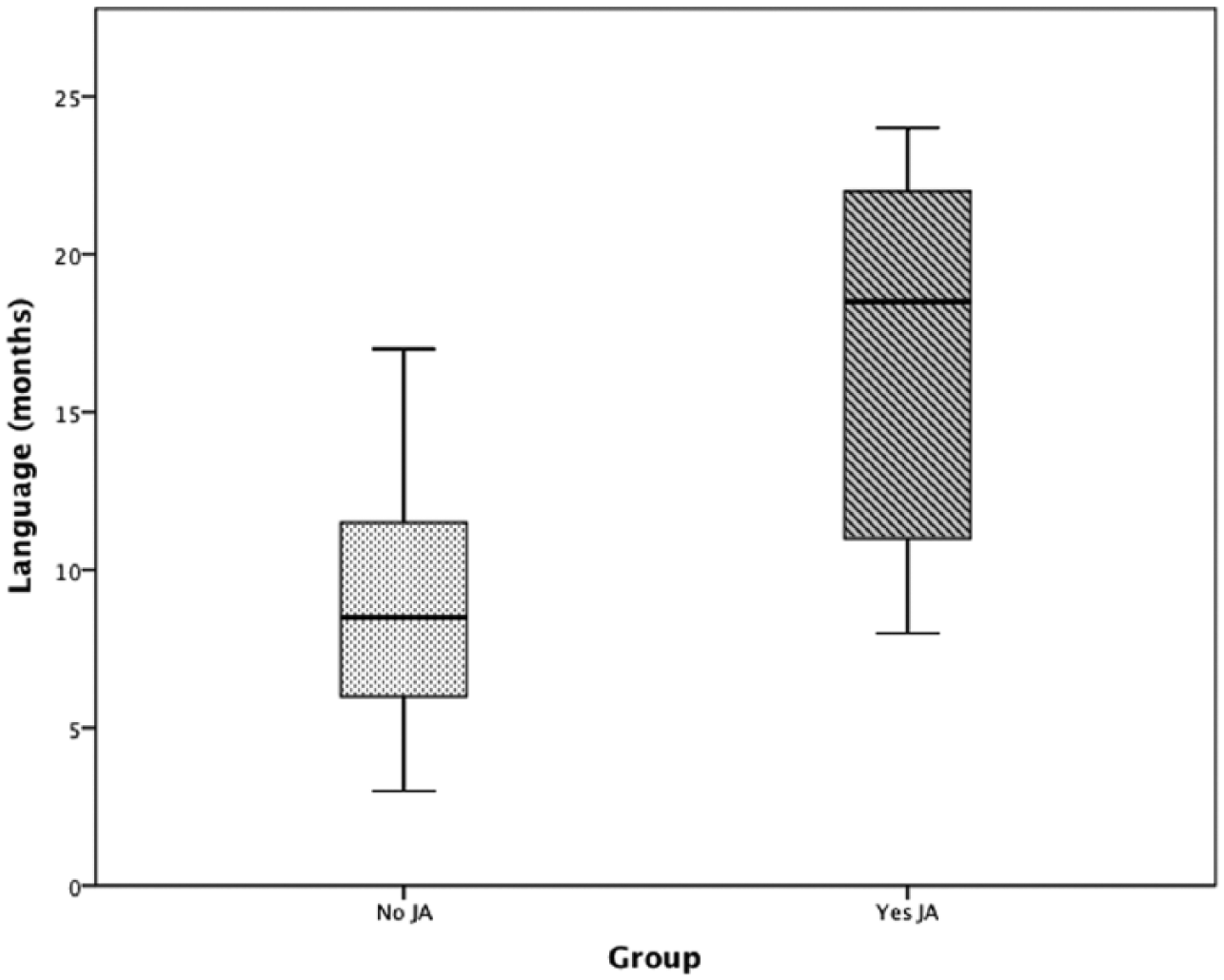
Language scores for children with autism in Analysis 2, by RJA use.
Discussion
The purpose of this study was to compare the JA abilities of children with autism who use this skill to children with DD to identify whether there were differences in frequency or form and to see how JA use related to concurrent language. The emphasis of much previous research has been on the JA deficits among many children with ASD; this investigation extends the earlier work by focusing on their JA competencies. Our main finding is that there is a significant subgroup of children with ASD who can appropriately use JA. They do so at significantly lower frequencies to children with DD, but when engaged in a bid, they use the forms of JA similarly. This has important implications for differential diagnosis and language development.
It is not clear why some children with ASD use JA while others do not. In our sample, the more developmentally advanced children, who had NVMA scores of 30 months or above, all demonstrated the ability to use RJA. This is supported by earlier research showing the delayed but eventual development of JA in some children with ASD (Carpenter et al., 2002). On the other hand, only half of the children with autism in our sample with NVMA scores below 30 months demonstrated the ability to respond to RJA. Although alone these numbers appear to imply that children with autism can use JA relatively well, they seem less impressive when compared to our sample of children with DD, more than 90% of whom demonstrated RJA ability.
While children with autism in this study were found to engage in JA, they did so at significantly lower frequencies than their matches with DD. This has been seen occasionally in the literature, for example, Paparella et al. (2011) did note that some children with ASD in their study were capable of using preverbal JA skills but that they too only did so infrequently. One explanation for lower RJA rates might be related to another issue that children with ASD have: a difficulty disengaging their attention from whatever they are focused on and shifting it to something new (Landry and Bryson, 2004). This overly focused or “sticky” attention (Ibanez et al., 2008) may be one reason why adults had to ask them repeatedly to look across the room at something novel, many more times than they asked children with DD. The difficulty disengaging has previously been studied using non-social stimuli (e.g. pictures on a video monitor), so examining the effects of sticky attention during social interactions might be an interesting direction for future study.
The lower frequencies of IJA use found among the children with autism fits with what we know about their general disinclination toward social engagement. Some believe that children with ASD are less motivated to use social communication because they do not find sharing attention with others to be intrinsically rewarding (Stone et al., 1997). The frequency of IJA use “may be more affected by social motivation rather than a social-cognitive process” (Mundy et al., 2007: 13). This theory supports the idea that although they know how to, children with ASD may choose not to engage in JA or to do so less frequently than children who enjoy interacting socially. They are more likely to use social communication in the form of a request for a desired toy or a snack because a request results in tangible reinforcement, whereas JA does not, its main function being social sharing (Jones and Carr, 2004). In research, children have been motivated to increase their IJA frequency by getting to engage in their highly preferred interests as a reward, thereby demonstrating that JA can be improved using non-social incentives (Jones and Carr, 2004; Vismara and Lyons, 2007).
It was notable that the children with ASD in this sample used the same forms of JA as their matched-peers with DD. Once engaged in a JA bid, they were able to use gestures and eye contact at comparable rates and had similar (mostly neutral) facial affect. Previous research on toddlers with ASD had a similar finding. In Shumway and Wetherby’s (2009) study, toddlers with ASD who engaged in JA were similar to children with DD on the proportion of coordinated gestures, vocalization, and eye gaze that they used.
Contradictory to our expectations, being able to use JA but doing so at lower frequencies did not appear to have a negative impact on concurrent language in this sample. The language scores for each matched-pair of children were very similar, a fact that can be partially attributed to the fact that children were initially matched on their NVMA and there is a high correlation between mental age and language. However, JA skills have been associated with language above and beyond mental age (e.g. Murray et al., 2008; Toth et al., 2006), and in the second analysis of this study, when we grouped children with autism by their ability to respond to JA, we found that language scores were much higher for the children who used JA, even when controlling for NVMA.
Perhaps there is a threshold level of JA use that is sufficient to facilitate language acquisition. It is possible that using JA, even at lower frequencies, is enough to attain basic language skills, and then more sophisticated levels of language can be acquired through other routes. For example, using alternative strategies like imitation (Carpenter et al., 2002) or non-direct means, such as observing other dyads as they use the words in context (Akhtar and Gernsbacher, 2007), could help “make up” some of the differences in learning opportunities missed from not participating in JA episodes. This might also explain some of the peculiarities (e.g. echolalia, rote phrases, and peculiar word usages) seen in the language of children with ASD. On the other hand, it may be that periods of more sophisticated joint engagement are important for teaching children how to participate in the increasingly complex conversations that occur as language demands grow with age (Adamson et al., 2009), and the long-term impacts of less frequent JA engagement would be seen only later in language development. The longitudinal impact of threshold levels of JA use on language development in ASD is a potentially interesting area for future research.
Like others (e.g. Murray et al., 2008), we found that young children with autism who used RJA had better concurrent language than children who did not. The important impact that using JA early has on language development makes it a worthy therapeutic focus for families. To engage children with ASD in JA, persistence on the part of parents and caregivers may be an enormously valuable trait. In this study, adults had to repeat bids, sometimes several times, before successfully engaging children with autism in JA. The adults were permitted to repeat the bid up to three times, first by calling the child’s name and then adding a point toward the object if the child did not initially respond. Many times the child with ASD did not respond the first time but finally did look (or make eye contact) as the adult repeated the call for attention and added more overt gestures (i.e. pointed and turned their head to clearly face the item that they hope to share). By the adult providing them with repeated chances, these children ended up with opportunities to see new things, map new language, and practice being part of a social dyad that they would have missed if they were interacting with a less persistent person. Adults are recommended to persevere in providing children with ASD opportunities to be part of social-communicative dyads through which they can practice their early language skills.
Finally, several teams have been able to successfully implement JA interventions with children with ASD (e.g. Kasari et al., 2010; Landa et al., 2011; Whalen et al., 2006). For young preverbal children, targeting JA appears to be a good treatment option that may improve downstream language development. For older children though, it may be more effective to focus intervention on language and social skills directly (Schertz and Odom, 2004). In a longitudinal follow-up to their JA intervention, Gulsrud et al. (2014) found that teaching preschool-aged children with ASD to point improved their later development of expressive language, but once the children were using spoken language, there was less need to point, so teaching that skill was no longer a priority. There are many routes to learning for children, and the best intervention choices will likely involve a customized approach; employing a goodness-of-fit between child characteristics like existing JA ability, age, and developmental level; and matching them to the most appropriate treatment model (Ingersoll et al., 2001).
Implications for future research
Drawing attention to the verity that there are young children with autism who use JA may have implications for early screening tools. Typically, screening tools use dichotomous (e.g. “yes” or “no”) responses to questions, and if the response indicates a child performs a critical item, their autism risk score is diminished. Although the sample in this study included mostly children older than the early screening tool range of 18–30 months, it would be excellent to extend the examination to focus on younger children. If the findings remain similar for young children, a follow-up question on assessments may be warranted. It could be useful to ask more about the children who pass JA items regarding the frequency of their sharing, showing, or responding to JA. Tools like the CHAT have high positive predictive value, but their sensitivity is only moderate (Charman, 2003). This low level of sensitivity means that a significant proportion of children who are later diagnosed with ASD pass the early screen, many because they could use JA. Differential diagnosis might be aided by knowing, for example, that a child only engages in RJA after repeated requests from an adult or that the child gets excited by new things and occasionally, but infrequently, shows them to another person. By getting more detail on JA items, children with ASD who employ JA might still be identified as at-risk on these critical factors.
Limitations
This study has several limitations. Like many other studies involving children with ASD, the sample size was relatively small, although the power analysis indicated that it was large enough to detect medium effects with good power. Looking at JA variability among a bigger sample would have improved the study. In addition, there remains the possibility that differences seen in the frequency of JA could be attributed to the later development of the skill rather than reflecting a syndrome-specific pattern of the way children used JA. This concern would be alleviated by looking at children’s JA skills over time, preferably beginning when they were young.
Missing from this study were qualitative measures, which might have helped to describe the individual situations. A qualitative component could have provided information on the personalities of the participants and perhaps could have lent insights into why some children employed JA in particular contexts while others did not engage in JA at all. It would have been interesting to know what the children were doing when the examiner was repeatedly calling their name, and it might have helped to explain why they did not look up even when the adult was purposefully trying to gain their attention. A qualitative element would be a worthwhile component for future JA research projects.
Conclusion
In summary, there is a subgroup of children with ASD who can appropriately use the forms of JA in similar ways to children with DD, but who engage in JA at significantly lower frequencies. These children may understand how to use JA, but due to factors like sticky attention and less motivation to interact socially, they may employ JA less often. There was a difference in concurrent language scores between the children with autism who employed JA and those who did not, highlighting the role that JA may play in early language acquisition. Adult persistence is recommended to encourage very young children to participate in JA and thereby build their concurrent, and potential downstream, language skills.
Footnotes
Funding
This research was made possible through grants from the National Institute for Child Health and Human Development to the University of North Carolina at Chapel Hill (R01-HD042168, P30HD03110).