
Abstract
Autism Diagnostic Observation Schedule-2 is the ‘gold standard’ autism spectrum disorder observational assessment, and it is increasingly used in South Africa. However, its use is limited to English speakers, as it has not been translated into the country’s other 10 official languages. Moreover, the cultural appropriateness of this tool has not been explored in South Africa. The Autism Diagnostic Observation Schedule-2 was translated into Afrikaans and assessed for cultural appropriateness to the ‘coloured’ population from low-middle socioeconomic status backgrounds in the Western Cape Province. Using a mixed-methods approach, three components associated with method bias in the Autism Diagnostic Observation Schedule-2 were investigated: language used, social interactions and activities, and materials. An ethnographic investigation of play, social interaction and social activities was conducted in a community sample (n = 40), and the Afrikaans Autism Diagnostic Observation Schedule-2 was pre-piloted in a clinical sample (n = 7). Results highlighted unique aspects of the language (‘Kaaps’) that need to be considered during Autism Diagnostic Observation Schedule-2 administration. The social interaction demands of the Autism Diagnostic Observation Schedule-2 appeared appropriate, and sufficient familiarity with Autism Diagnostic Observation Schedule-2 materials and activities was found to support the use of the Autism Diagnostic Observation Schedule-2. Guidelines for administration of the Autism Diagnostic Observation Schedule-2 to this population were generated to improve cultural sensitivity and cultural appropriateness and to reduce method bias.
Keywords
Autism spectrum disorder (ASD) affects children worldwide across all demographic groups (Dyches et al., 2004), including racial and ethnic groups (Fombonne, 2003), and across different cultures (Daley, 2002). Socioeconomic status (SES) is not a risk factor for ASD (Fombonne, 2003), but may influence clinical diagnosis (Daley, 2002) and access to services (Durkin et al., 2010).
The prevalence of ASD in the United States is one in 68 (Christensen et al., 2016). In many countries, reliable and culturally appropriate ASD diagnostic tools are still not available. In South Africa, lack of such tools is a barrier to accurate ASD diagnoses and to determining the prevalence of ASD.
The ‘gold standard’ observational assessment for ASD diagnoses (Kanne et al., 2008) is Autism Diagnostic Observation Schedule-2 (ADOS-2; Lord et al., 2012). The ADOS-2 is a semi-structured, standardized assessment of social interaction, communication, play, imaginative use of materials, and restricted and repetitive behaviours. The ADOS-2 provides a standardized observation as part of a diagnostic work-up for possible ASD. The primary focus of the ADOS-2 is on the interactive social behaviour between the participant and one examiner. Any other person present in the assessment room should serve solely as an observer (Lord et al., 2012). Therefore, a translator/interpreter should not be used and the assessment should be conducted in the primary language spoken by both participant and examiner.
The ADOS-2 was developed in the United Kingdom and United States, but it has been used in many parts of the world, mainly in high-income countries, and administered to individuals from many different cultures. Given that South Africa lacked suitable ASD diagnostic tools, the ADOS-2 was imported from the ‘global north’, typically referring to the United States, United Kingdom and Western Europe.
When tools designed in the global north are used outside this context, cultural factors may present as challenges during tool administration. For example, these tools, like the ADOS-2, were predominantly designed in English. Outcome scores may be impacted when tools are administered in a language other than the mother tongue of the individual being assessed (Taliep and Florence, 2012). The ADOS-2 has, however, been translated into 18 languages (Western Psychological Services (WPS), 2015). Unfortunately, it has not yet been translated into any of South Africa’s 10 other official languages, thus limiting ADOS-2 assessments within South Africa to English-speaking individuals.
Furthermore, many diagnostic tools, including the ADOS-2, contain many different materials. Some materials may be unfamiliar to individuals being assessed (Norbury and Sparks, 2013) or be culturally inappropriate. Certain social interactions found in assessments, particularly between adults and children, may also be culturally inappropriate for individuals being assessed (Norbury and Sparks, 2013). The ADOS-2 assessment is structured so that an unfamiliar adult interacts with a child, often during play activities or social conversations, for the entire assessment.
In recent years, the ADOS-2 has become more widely used in South Africa. However, we have yet to ascertain whether it is appropriate for our local cultures. There is a risk that aspects of the ADOS-2, such as the language of the tool, the social interaction used or the materials, may be inappropriate for some South African cultures. These aspects are associated with method bias, that is, familiarity of tool materials and activities and appropriateness of tool administration (Van De Vijver and Tanzer, 2004).
South Africa is a multi-cultural country. When addressing the cultural appropriateness of a tool, the focus should be on one cultural group at a time. The ‘coloured’ population of the Western Cape Province of South Africa has a unique cultural heritage. ‘Coloured’ is the specific term used to refer to an ethnic category found in South Africa, which was derived from apartheid classification, but it is used in the modern South African census and will be used as such in this study (without the quotation marks). This category can be a positive assertion of identity and is the preferred term used by members of this ethnic group (De la Rey and Duncan, 2003).
In all, 76.5% of coloured people in the Western Cape speak Afrikaans (Statistics South Africa, 2012).‘Kaaps’ is a vernacular of Afrikaans, commonly spoken by coloured, Afrikaans-speaking people from low to middle SES backgrounds from the Western Cape (Devarenne, 2010; Martin, 2000). It differs significantly from standard Afrikaans, spoken by white and middle-class coloured people, in that the dialect is unique, and code-switching (using at least two distinct languages in the same conversation; Simango, 2011), particularly with English, is common (Van Der Waal, 2012). The dialect can be spoken at different ‘levels’ (‘… from the “respectable” language of the middle class, also frequently used by craftsmen and workers, to jail slang’; Martin, 2000: 111), and it varies according to situations, social company and impressions (Martin, 2000).
The literature on the coloured population of the Western Cape is limited. For example, there is no literature on the kinds of games coloured children in the Western Cape play, or the kinds of materials they play with. The limited literature often refers to ‘coloured communities’ (e.g. Devarenne, 2010; Martin, 2000; Van Der Waal, 2012), indicative of the sense of community shared by coloured people. They are a highly sociable group and share their life experiences, even if those experiences often include poverty and violence (Muyeba and Seekings, 2011).
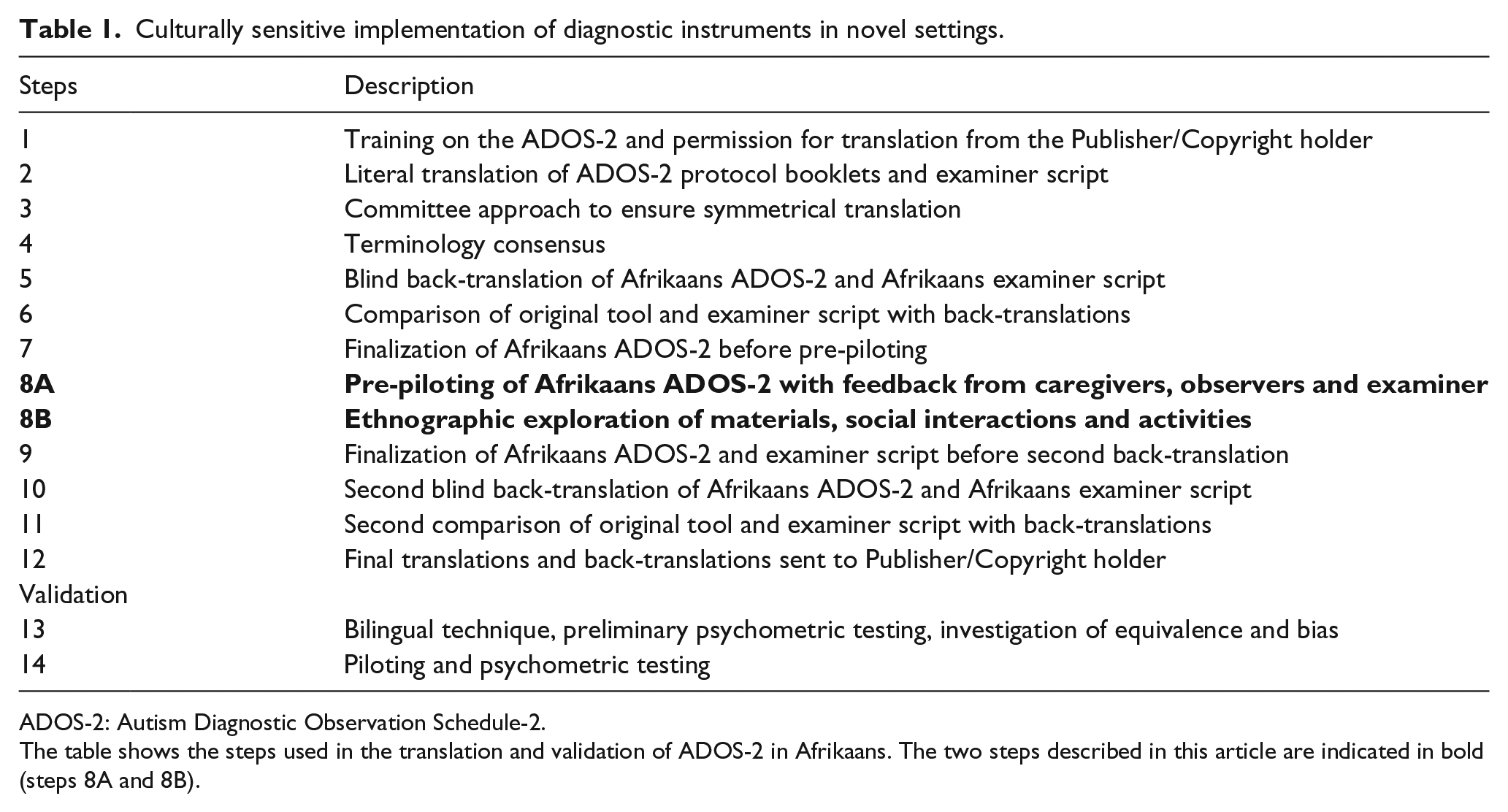
To ensure a culturally sensitive implementation of the ADOS-2 in a novel setting, we aimed for a rigorous and stepwise process as shown in Table 1. Steps 1–12 were executed in this study. Steps 13 and 14 are necessary to complete the full validation of the Afrikaans ADOS-2, which was not done in this current study. After training on the ADOS-2 and permission to translate the ADOS-2 was granted from the publishing company, the first task was to translate the ADOS-2 into Afrikaans. We elected to translate the examiner script, consisting of the verbal prompts required to administer the ADOS-2, as well as the full protocol booklets for Modules 1, 2, 3 and 4 of the ADOS-2. A symmetrical approach for translation (Sousa and Rojjanasrirat, 2011) was used, which warranted the faithfulness of meaning and colloquialism in the original English ADOS-2 and in the Afrikaans-translated version. The process of centring (Sousa and Rojjanasrirat, 2011) was applied, whereby the original English ADOS-2 and the Afrikaans-translated version were considered equally important. A committee approach (Brislin, 1970) was also used to work through the entire translation, and adaptations were made where necessary. The committee also ensured consensus on the terminology used and produced a pre-pilotable version of the Afrikaans ADOS-2.
Culturally sensitive implementation of diagnostic instruments in novel settings.
ADOS-2: Autism Diagnostic Observation Schedule-2.
The table shows the steps used in the translation and validation of ADOS-2 in Afrikaans. The two steps described in this article are indicated in bold (steps 8A and 8B).
This study aimed to investigate the cultural appropriateness of the ADOS-2 for Afrikaans-speaking, coloured families from the Western Cape (steps 8A and 8B as shown in Table 1). To ensure evaluation of families representative of the typical SES profile of our patient population, we were specifically interested in coloured families of low to middle SES (referred to as ‘low-middle SES’).
In order to achieve the study aims, we investigated three key components of method bias: (1) the appropriateness and accessibility of the language used in the Afrikaans-translated ADOS-2, (2) the appropriateness of the social interactions and activities in the ADOS-2 and (3) the appropriateness and familiarity of the ADOS-2 materials.
Methods
Ethical considerations
This study complied with the Declaration of Helsinki (2008). Ethical approval to conduct the study was granted by the School of Child and Adolescent Health at Red Cross War Memorial Children’s Hospital, the University of Cape Town Department of Psychology, and the Faculty of Health Sciences Human Research Ethics Committee. Permission was also obtained from WPS to translate the original English ADOS-2 into Afrikaans through a formal contract agreement with the senior author.
Participants
A total of n = 47 primary caregivers (who included parents and carers, referred to as ‘caregivers’ in the study) were recruited. Of these, n = 40 were from a community sample and n = 7 were from a clinical sample. The caregivers from the clinical sample had children who were referred to the Red Cross War Memorial Children’s Hospital Developmental Clinic, due to developmental concerns, including risk for ASD. Four of the seven children in the clinical sample had a known clinical diagnosis, including intellectual disability, global developmental delay (child of Participant 10A), attention deficit hyperactivity disorder (ADHD) and ectrodactyly–ectodermal dysplasia–cleft syndrome. The inclusion criteria stipulated that caregivers and their children needed to be coloured, Afrikaans-speaking and from low-middle SES backgrounds, and that the children needed to be between 12 months and 20 years of age. The community sample participants were recruited via word-of-mouth from a local cleaning company outsourced to the University of Cape Town and the clinical sample and their children were recruited from the Red Cross War Memorial Children’s Hospital Developmental Clinic.
Participants were divided into two groups based on the age of their children. Group A was defined as caregivers of children younger than 10 years old, and group B was defined as caregivers of children aged 10 years and older. A total of 20 participants from the community sample were in group A and 20 were in group B. Four participants from the clinical sample were in group A and 3 were in group B.
Measures
ADOS-2
The ‘pre-pilot’ version of the Afrikaans-translated ADOS-2 was used in the study (Lord et al., 2012; Afrikaans translation).
Language and cultural appropriateness questionnaire (available from authors)
The researchers generated this questionnaire to establish the appropriateness of the ADOS-2 activities and the language used in the Afrikaans ADOS-2 for the clinical sample. It was completed by the caregivers, the invited observers of the assessments (maximum 4) and the ADOS-2 examiner.
It asked whether any words used during the assessments were not understood by the caregivers/children and whether the language spoken during the assessments was similar in nature to the language spoken by the caregivers/children. It also asked whether any ADOS-2 activities felt uncomfortable and/or were culturally inappropriate.
Ethnographic questionnaire (Abubakar et al., available from authors)
This questionnaire was administered in an interview style and investigated play, social interaction and social activities for the community sample. An ethnographic questionnaire (EQ), developed by Dr Amina Abubakar Ali and colleagues, from the Kenyan Medical Research Institute was used. The questionnaire addressed natural play, activities of daily life and resources. It asked about the games children played and what toys they played with, whether the children had attended birthday parties and what happened at these parties. It asked whether participants had a ‘sink’ to brush their teeth at or what they used as an alternative. It also investigated the social routines children participated in. Furthermore, it questioned whether the caregivers had ever read and/or told stories to their children and whether their children had ever told them stories.
For the South African study, an additional question was added, addressing social interactions in daily life, and asked how often children played/socially interacted with their caregivers or other adults.
ADOS-2 materials questionnaire (available from authors)
This questionnaire was generated by the researchers to establish the appropriateness and familiarity of the ADOS-2 materials. A total of 28 materials from ADOS-2 kit were photographed. These materials were divided into two groups; materials from the toddler Module, Module 1 and Module 2 were grouped together and shown to caregivers of younger children (group A), and materials from Module 3 and Module 4 were grouped together and shown to caregivers of older children (group B). The remote-controlled bunny and toy frog were shown to both groups. Therefore, each group saw 15 materials, and each caregiver answered a total of 15 short questionnaires (one for each material) in an interview style.
The questionnaire asked the clinical and community sample participants whether their children had (1) seen the materials, (2) played with the materials and (3) whether they owned the materials. Where materials were not owned, participants were asked for a reason.
Socio-demographic questionnaire (available from authors)
This questionnaire was completed by the clinical and community samples. It recorded socio-demographic variables including age, sex, ethnicity and home language, as well as variables investigated by Myer et al. (2008), namely, highest level of education, annual household income and available material and financial resources. These socio-demographic variables were used to establish the SES of participants.
Procedure
Testing procedure
Community sample
Each caregiver was seen alone in a private room for approximately 45 minutes. They completed the socio-demographic questionnaire, EQ, and ADOS-2 materials questionnaire (AMQ). Participants were compensated with ZAR50 (~US$3) for participation, and all study-related expenses were reimbursed.
Clinical sample
One caregiver and his or her child were seen at a time in a private room with a camera for recording purposes. The Afrikaans ADOS-2 ‘pre-pilot’ version was administered to the participating child using standardized ADOS-2 administration procedures by the senior author (PJdV), who is fluent in Afrikaans and English. PJdV trained in the ADOS in 1998 and has been an international ADOS and ADOS-2 trainer since 1999. For lower modules, caregivers were present in the assessment room and a team of researchers (maximum of four) observed from behind a one-way mirror; for higher modules, the examiner and participant were in the assessment room, with the team of researchers in the observation room. Given that the purpose of this step was to evaluate the cultural appropriateness of the assessment, in a departure from standard ADOS-2 procedures, caregivers were also invited to be in the observation room with the research team. Caregivers, observers and the ADOS-2 examiner completed the language and cultural appropriateness questionnaire (LCAQ) during or immediately after the administration. After the assessments, caregivers completed the socio-demographic questionnaire and the AMQ. The testing procedure took approximately 2 hours in total. Participants were compensated with ZAR50 (~US$3) for participation and all study-related expenses were reimbursed.
Data analysis
First, detailed descriptive statistics were calculated to investigate sample characteristics. Second, data from the LCAQ (completed by the clinical sample caregivers, the observers and the examiner) were explored qualitatively to identify problematic language use, culturally inappropriate activities and suggestions for the improvement of the quality of Afrikaans ADOS-2 assessments. Third, a qualitative thematic approach was used to analyse the data from the AMQ and EQ. The researchers coded the data, uncovered common themes, extracted noteworthy quotes and translated the quotes from Afrikaans into English. Fourth, data regarding play materials from the AMQ and EQ were compared to determine the overlap between spontaneously reported play materials in the EQ and ADOS-2 materials (explored in the AMQ). The EQ was also analysed qualitatively to observe any overlap in spontaneously reported games played and games found in the ADOS-2. Fifth, the data collected from the EQ, AMQ and LCAQ were also analysed quantitatively to obtain proportions, percentages and frequencies in Microsoft Excel. Sixth, the notes on the ADOS-2 Modules made by PJdV during the pre-piloting assessments were used to adapt the final wording and layout of the Afrikaans-translated ADOS-2 Modules (not presented here).
Results
The characteristics of participants are shown in Table 2. Given the significantly discrepant income profiles in South Africa, two common definitions are used to describe the middle SES groups. The ‘actual’ middle class has an annual household income of ZAR18,240–ZAR54,720 (median = ZAR36,432), while the ‘relatively affluent middle class’ has an annual household income of ZAR67,200–ZAR480,000 (Statistics South Africa, 2012). Results therefore confirmed the low-middle SES profile of the sample. One child from the clinical sample (child of Participant 10A) was classified on the ‘autism spectrum’ by the Afrikaans ADOS-2. The remainder of the children were classified as ‘non-spectrum’.
Characteristics of the community and clinical samples.
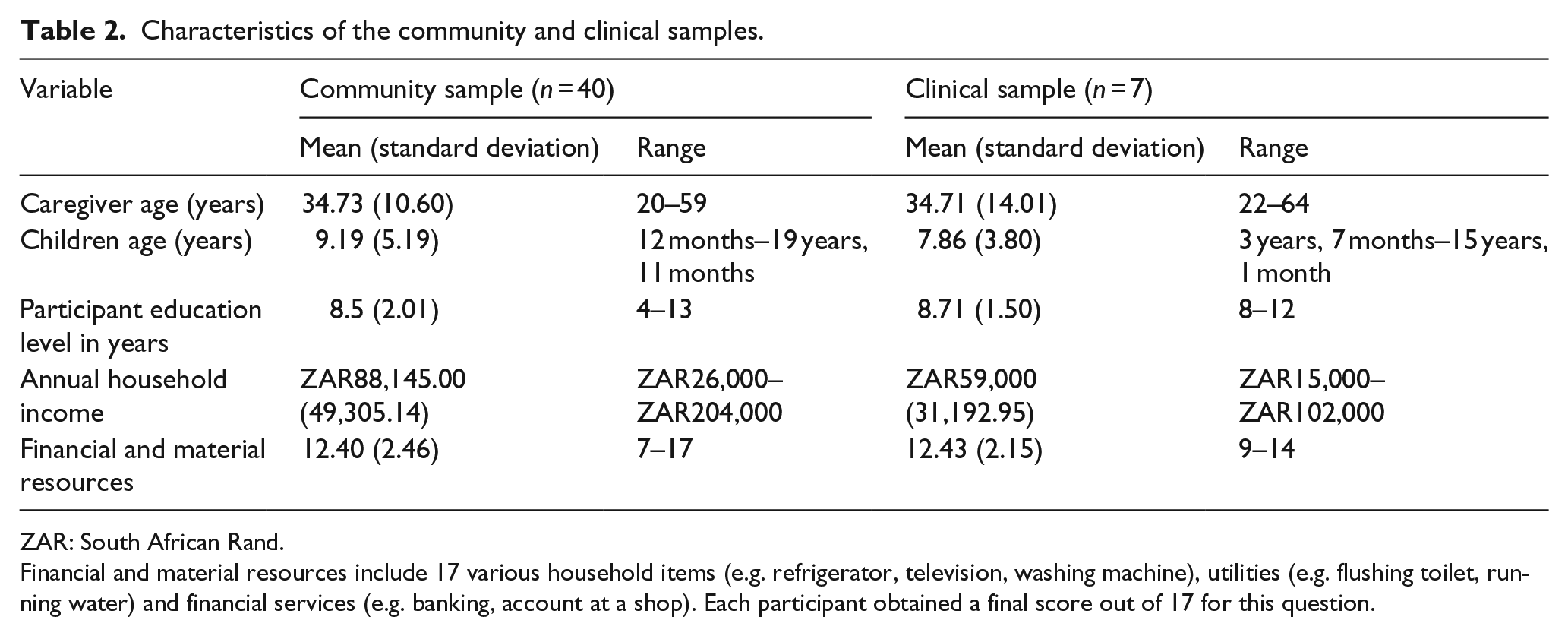
ZAR: South African Rand.
Financial and material resources include 17 various household items (e.g. refrigerator, television, washing machine), utilities (e.g. flushing toilet, running water) and financial services (e.g. banking, account at a shop). Each participant obtained a final score out of 17 for this question.
Language used during Afrikaans ADOS-2 assessments with the clinical sample
Pre-piloting a tool to observe language accessibility is well-established in research involving tool translation (Maneesriwongul and Dixon, 2004). A key goal here was observing the appropriateness of the language used from a cultural perspective. The language must be understood by, and accessible to, the target population and it must be culturally appropriate.
Dialect
A notable feature of the language used during the assessments was the difference in dialect used by the examiner and the children (noted by the examiner, observers, and Participants 10A and 12A). Whereas the examiner spoke with a more formal/precise Afrikaans dialect, children often spoke more slang or with a distinct Kaaps dialect (Van Der Waal, 2012).
Slang and informal language was produced more often during the Conversation and Reporting activity, the Demonstration Task, the Description of a Picture activity and the Telling a Story from a Book activity, where spontaneous language use was encouraged. When a strong Kaaps dialect was detected, the examiner made adjustments to certain words, in terms of pronunciation or accent, to facilitate rapport and promote understanding. Children acknowledged these attempts and the assessments felt more comfortable and culturally suited for the children.
Code-switching
Code-switching was another distinctive feature of the language used by the children during their assessments (noted by the examiner, observers, and Participants 10A, 12A and 29B). Children often switched between English and Afrikaans both within and between sentences. Accordingly, to match the children’s expressive language, the examiner made minor adjustments during the administration. For example, when necessary the examiner provided English words for infrequently used Afrikaans words, or clarified meaning with English words when Afrikaans words were not understood.
Terminology used by the examiner not understood by caregivers/children
A total of 20 words were identified by the caregivers, examiner and observers as words that either the children or caregivers did not understand during the assessments (Table 3). These words were predominantly about emotions or feelings. Many of these words were better understood in English or with further explanation in Afrikaans.
Guidelines for administration of the Afrikaans ADOS-2 to Afrikaans-speaking, coloured individuals from low-middle SES backgrounds.
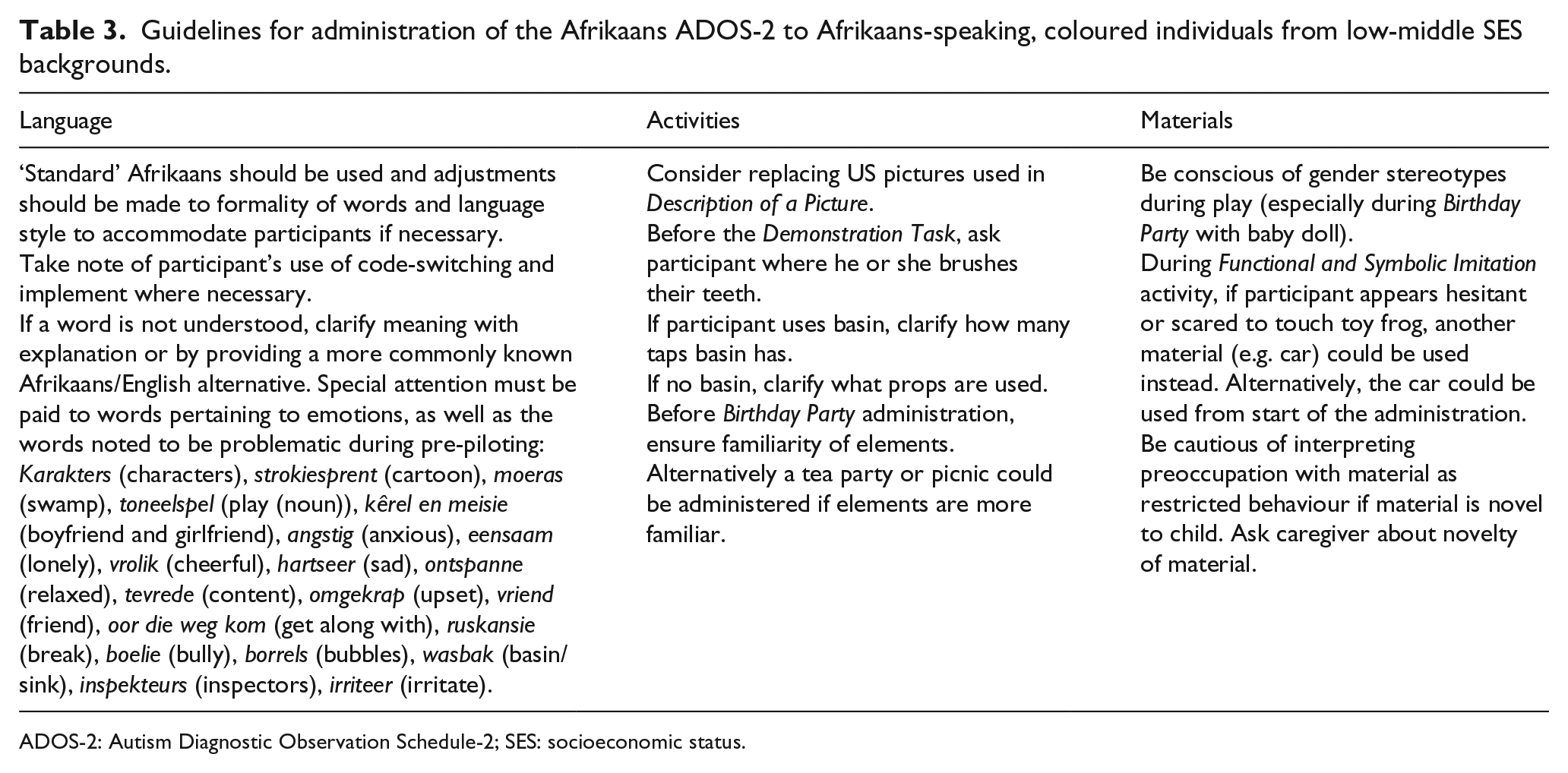
ADOS-2: Autism Diagnostic Observation Schedule-2; SES: socioeconomic status.
The appropriateness of the social interactions and activities in the ADOS-2
Social interactions
To determine the social appropriateness of a child interacting with an adult, we asked community sample caregivers how often their children socially interact with adults. The results are indicated in Figure 1. Almost 58% (57.5%) of participants reported regular, at least daily, adult–child interactions in their community, 20% described that this occurred seldom or never, and 17.5% described that this typically happened only at weekends. Most caregivers did, however, report that they had at some point in the past read story books (70%) and shared stories (72.5%) with their children and that their children had shared stories with them (85%). Furthermore, apart from the child classified as ‘autism spectrum’ on the ADOS-2, the social interaction observed between the children from the clinical sample and the examiner during the ADOS-2 assessments appeared to be socially appropriate.
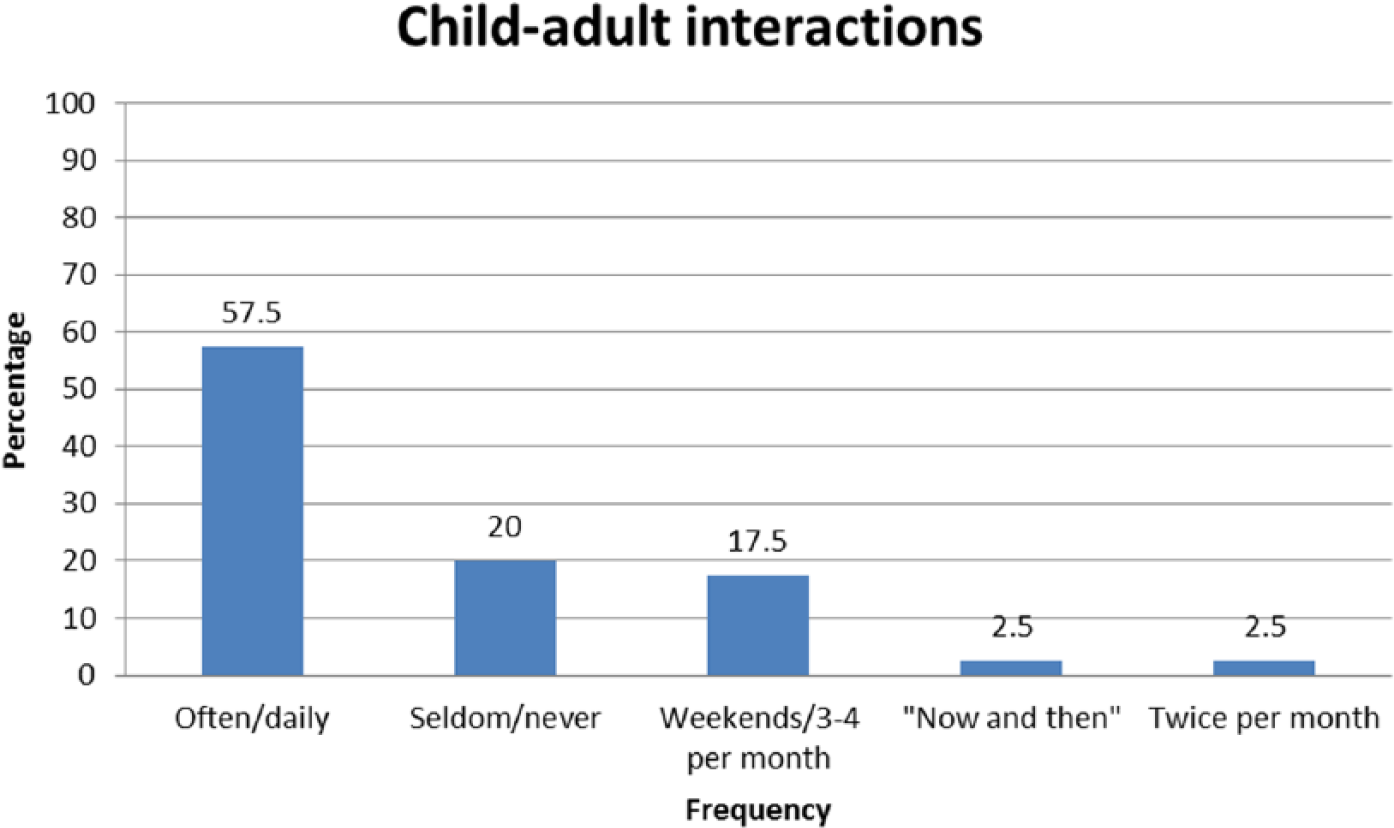
Frequency of child–adult interactions reported by the community sample caregivers (n = 40).
Inappropriate ADOS-2 activities
Given that the focus of the ADOS-2 is on observation of social behaviours and communication, activities are designed to provide comfortable and standardized, yet interesting contexts in which interactions can occur (Lord et al., 2012). It is important that these activities, however, are culturally appropriate for those being assessed.
Description of a picture
This activity was noted to be culturally inappropriate based on the responses on the LCAQ. Specifically, the US map scene picture was deemed inappropriate due to unfamiliarity.
Demonstration task
In the EQ, participants were asked whether their children were familiar with brushing teeth at a basin. In the community sample, 80% reported having a basin at home where they brush their teeth, 57.5% reported that their basin had warm and cold taps and 22.5% reported that their basin had a cold tap only. Of the eight participants who reported not having a basin at home, four used a cup, three used a bathtub and one used a baby bathtub when brushing teeth.
Birthday party
In all, 92.5% of the community sample reported that their children had attended a birthday party However, over three-quarters (77.5%) did not report a birthday cake at birthday parties, and only one-third (32.5%) reported that their children sang the Happy Birthday song at these parties.
No other activity raised concern about cultural inappropriateness.
Appropriateness and familiarity of ADOS-2 materials
In the community sample, 64.3% of the responses from the caregivers in group A confirmed familiarity of materials (see Figure 2). A total of 54.6% of the responses were that the materials had been played with, and 40% of the responses were that the materials were owned. All caregivers said that their children had seen balloons (owned by 55%), a baby doll (owned by 60%), and plastic cups, plates and utensils (owned by 100%). Most of the children who had seen these materials had also played with them (⩾80%). Participants reported that these materials were readily available and affordable in shops in their communities:
Dis ‘n baie common toy; die is iets wat jy onmiddelik kan kry in die winkel. (Participant 6A; regarding plastic cups, plates and utensils) Translation: It is a very common toy; it is something that you can get immediately in the shops. Dit kan ons bekostig. (Participant 14A; regarding balloons) Translation: We can afford this.
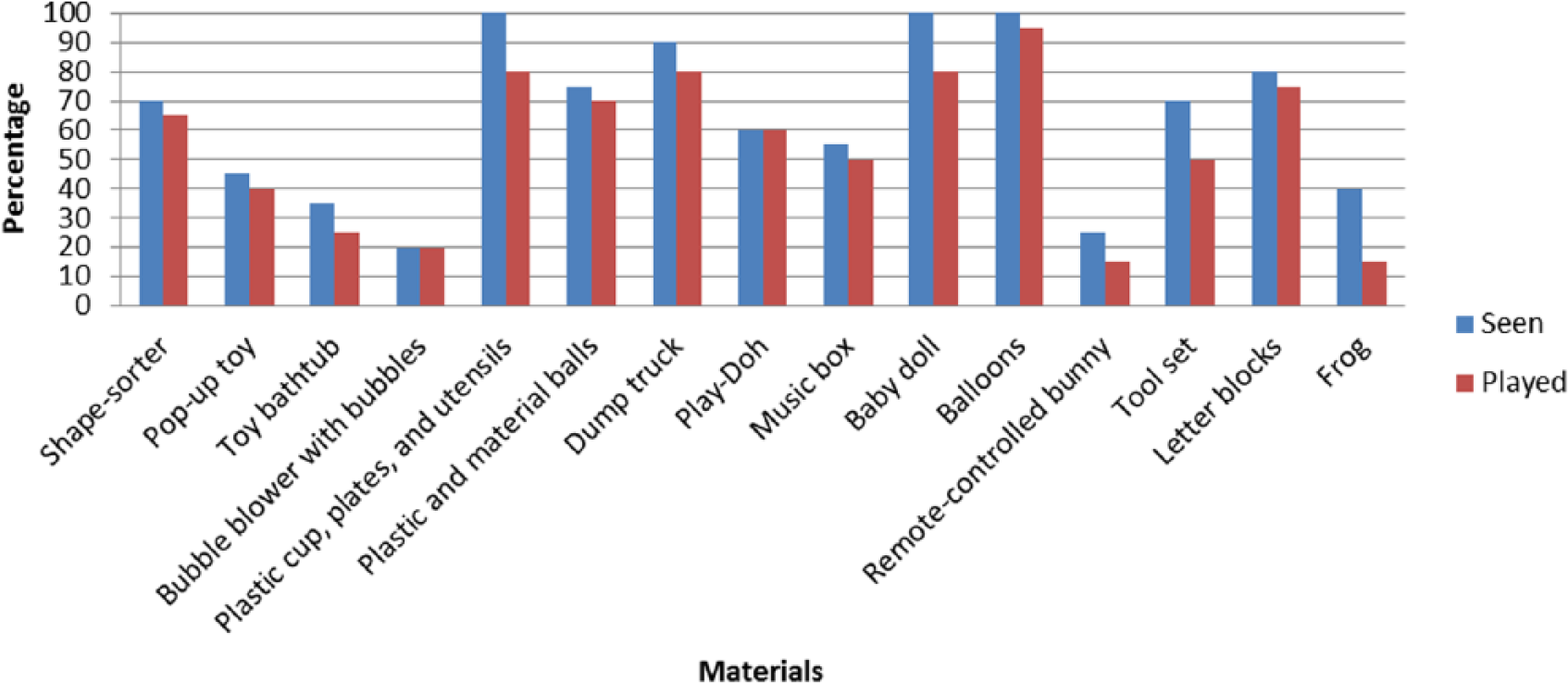
Percentage of participants from community sample group A who reported that their children had seen and played with ADOS-2 materials (n = 20).
The least familiar materials included the toy bathtub (owned by 15%), the remote-controlled bunny (owned by one participant only; 5%) and bubble blower (owned by 15%). All 16 caregivers (80%) who reported that their children had not seen/played with the bubble blower reported that their children had seen/played with ‘normal bubbles’ with a dipping stick.
In all, 73.3% of the responses from group B of the community sample caregivers were that the ADOS-2 materials had been seen, and 61% of the responses were that the materials had been played with (Figure 3). Nearly half of the responses were that the families (49%) had the materials at home. All of the participants reported that their children had seen marker pens (known as ‘koki-pens’ in South Africa; owned by all), the remote-controlled car (owned by 65%) and small toy cars (owned by 85%). Most of those who had seen those materials had also played with them (⩾80%).
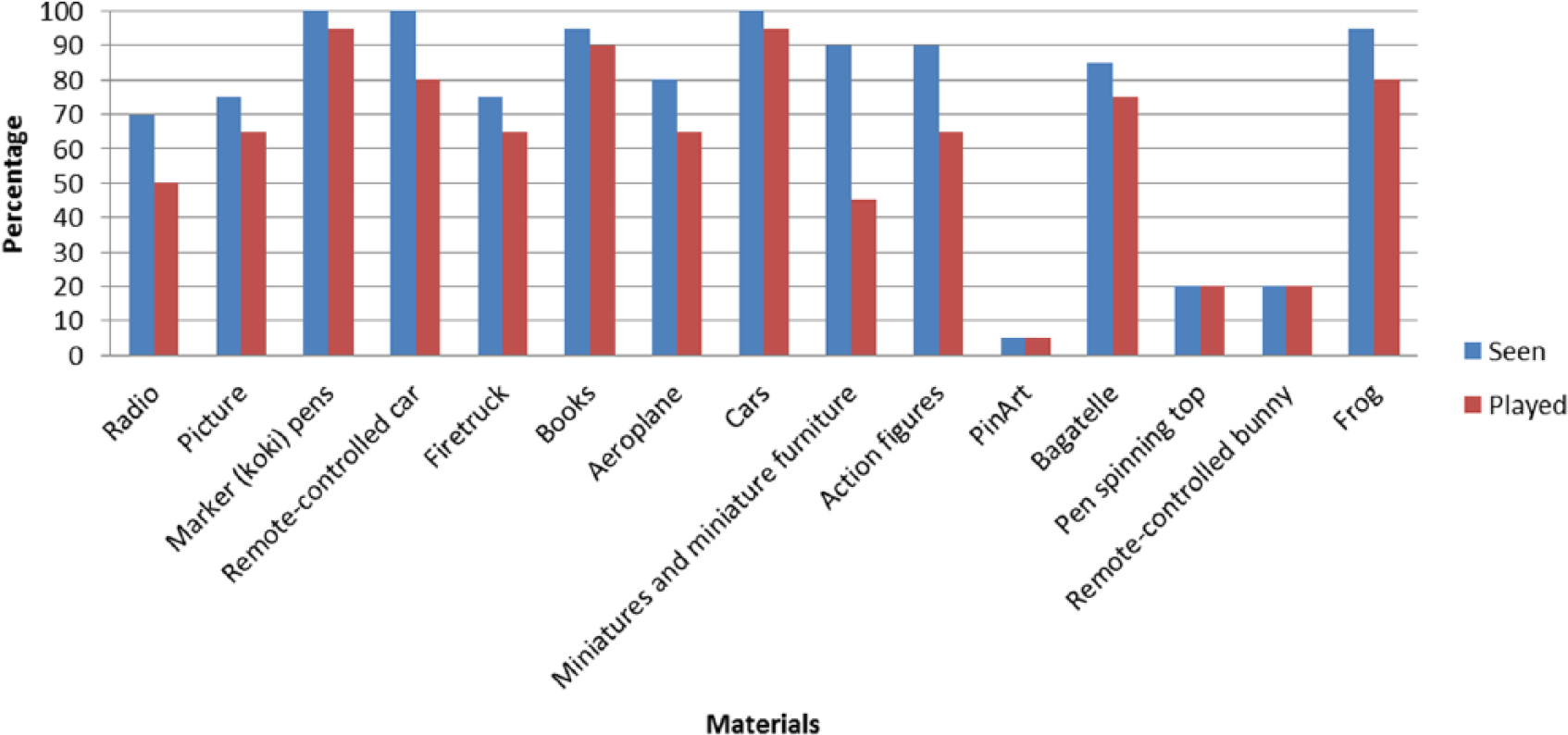
Percentage of participants from community sample group B who reported that their children had seen and played with ADOS-2 materials (n = 20).
The least familiar material, which no participant owned and only one child had seen and played with (5%), was the PinArt. Other unfamiliar materials included the remote-controlled bunny (seen and played with by 20%; not owned by any participant) and pen spinning top (seen and played with by 20%; owned by 10%). In total, 35% did, however, say that their children had played with a standard spinning top.
The findings were similar in participants from the clinical sample (n = 7), where all caregivers reported that their children had seen/played with some of the ADOS-2 materials. Clinical sample participants in group B commented on the unfamiliarity of the PinArt, the miniature figures and furniture and the remote-controlled bunny.
Common themes
Some common themes emerged from the AMQ when caregivers were asked why they did not own certain ADOS-2 materials.
Poverty and novelty
Caregivers often said that they could not afford certain ADOS-2 materials and that the shops in their communities do not stock unusual materials (e.g. PinArt and remote-controlled bunny).
Gender stereotypes
Stereotypical gender roles in use of materials were reported by caregivers at very high rates. In total, 71.4% (five of the seven) of caregivers in the clinical sample and 67.5% (27 of the 40) of caregivers in the community sample spontaneously commented on specific materials as intended for boys or girls only. Some caregivers very strongly indicated that their children did not or would not play with materials intended for the opposite gender:
Hy is ‘n boy man! Ons keer dit strictly boys/girls. (Participant 23A; regarding baby doll) Translation: He is a boy man! We keep it strictly boys/girls. Sy is ‘n girl. Ons kan nie vir haar boy toys koop nie! (Participant 43A; regarding dump truck) Translation: She is a girl. We cannot buy her boy toys! Hy het gesê hy is nie ‘n moffie nie! (Participant 46B; regarding miniature figures and furniture) Translation: He said that he is not gay!
Fear, violence and danger
A total of 55% (22/40) of the caregivers in the community sample and 3 of the 7 caregivers in the clinical sample mentioned elements within this theme.
Some participants in group A were concerned about whether the materials were safe for their children to play with. Specifically, concern was raised about children drinking the liquid used to blow bubbles, eating the Play-Doh and swallowing smaller objects.
The issues of ‘violent toys’ and materials promoting violence were also raised. Specifically, the toolset seen by group A and the action figures seen by group B evoked the most emotive responses. Many caregivers also mentioned that their children would be afraid of certain materials, especially the toy frog. In all, 37.5% (15 of the 40) of the community sample and one of the 7 caregivers in the clinical sample reported that their children would refuse to play with the toy frog. Participant 2A said,
Sy hou nie van hierdie goed nie. Sy sal nie aan slange, spiders en paddas vat nie. Die kinders is bang vir daai. Sy sal hysterical raak met hierdie goed. (Participant 2A) Translation: She does not like these things. She will not touch snakes, spiders and frogs. Children are scared of those. She will become hysterical with these things.
Participant 48A said,
Hierdie ding gat hy huil oor. Hy is bang! Hy sal nie naby hierdie ding kom nie! (Participant 48A) Translation: He will cry over this thing. He is afraid! He won’t come near this thing!
These responses likely stemmed from the culture which the participants were from. It may be culturally appropriate for this particular population not to play with materials associated with amphibians, reptiles and even insects. This finding would be consistent with the finding in KwaZulu-Natal, with the isiZulu-speaking population (Dr Lauren Franz, 2015, personal communication).
The theme of danger around play was also highlighted in a different way when caregivers spoke of the danger they face on a daily basis within their communities, which impacts their children:
Hulle skiet baie daar in ons gemeenskap. (Participant 11B) Translation: They often shoot there in our community. Buite is gevaarlik, daarom speel hulle in die huis. (Participant 35B) Translation: Outside is dangerous, therefore they play in the house.
Spontaneously reported play and play materials
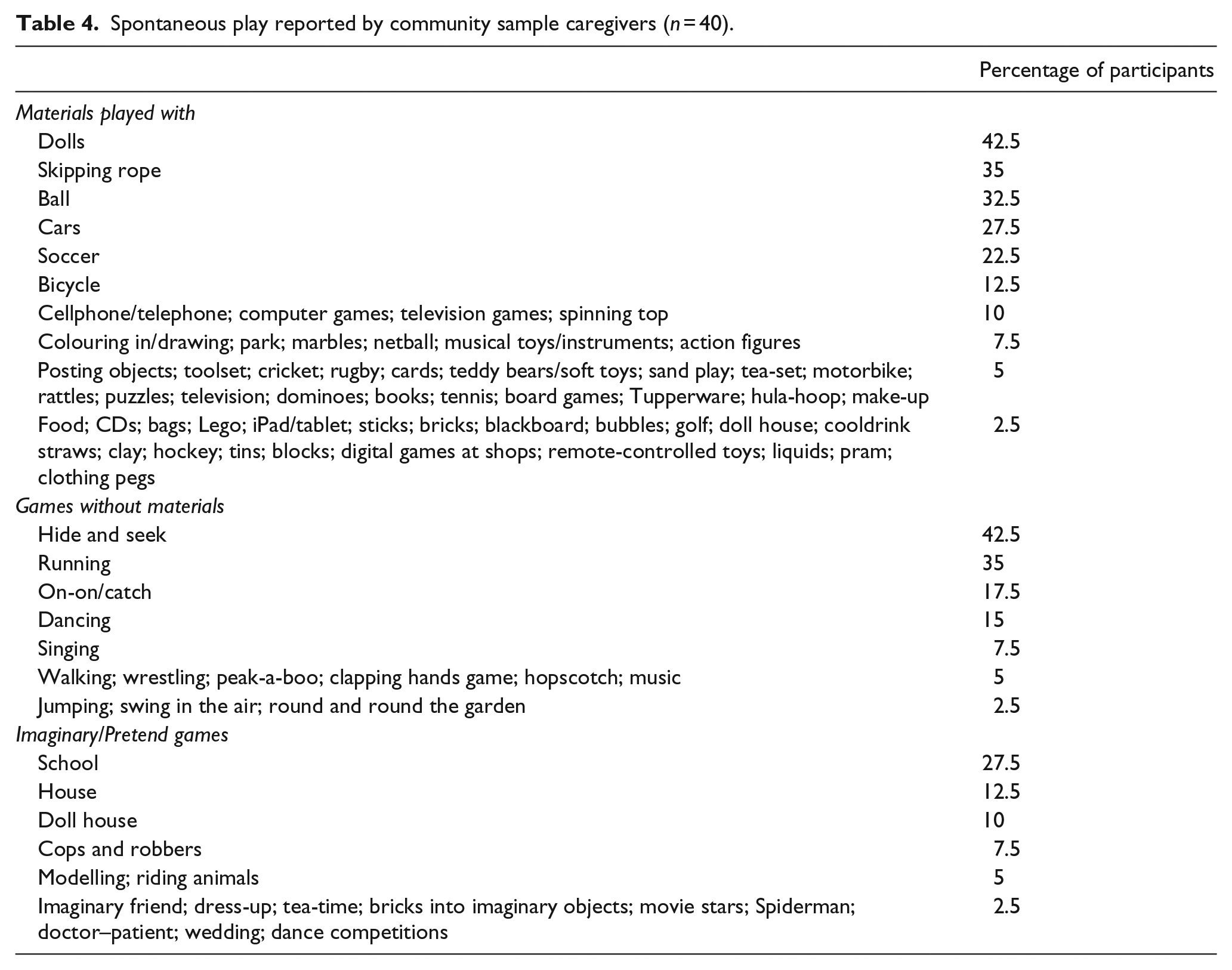
This ethnographic component was included given that there was no existing literature on the games played and play materials used by coloured children from this socio-cultural group. Results are summarized in Table 4.
Spontaneous play reported by community sample caregivers (n = 40).
Imaginary/pretend play
When community sample caregivers were asked what ‘pretend/imaginary games’ their children played, many provided games that include materials (e.g. tins, balls) and physical activity (e.g. running, kicking), but did not involve imaginary play. Nevertheless, 15 actual pretend games were mentioned. The most frequently listed pretend games included imaginary school (27.5%) and house (12.5%) play and imaginary play with dolls and doll house items (10%). The ADOS-2 provides opportunities for a range of imaginative play, including play with dolls.
Play without materials
A total of 15 games were mentioned spontaneously when the community sample caregivers were asked what games their children played without any materials. The most frequently listed games included hide and seek (42.5%), running games (35%), on-on/catch (17.5%), dancing (15%) and singing (15%). Singing is found in the ADOS-2 during the Birthday Party. The other frequently listed games can also be played if the child initiates the play, although it is not an actual game played during an assessment. Peek-a-boo (5%) and swinging in the air (2.5%), two activities in Anticipation of a Social Routine, were listed spontaneously, but at quite a low frequency.
Play with materials
A total of 56 different materials were listed spontaneously by the community sample when asked what materials their children played with, 21 of which are included in the ADOS-2. The most common materials included dolls (42.5%), skipping ropes (35%), balls (32.5%), cars (27.5%) and soccer items (22.5%).
Discussion
In this study, we set out to evaluate the cultural appropriateness of an Afrikaans translation of the ADOS-2 in a low-middle income group of Afrikaans-speaking coloured people in the Western Cape. We were particularly interested in three components of potential method bias, including language used, social interactions and activities, and materials used. Given that there was no pre-existing literature on typical play, social interactions and activities in children from the coloured community in South Africa, we were interested in collecting ethnographic information, in combination with empirical evaluation of live Afrikaans ADOS-2 administrations, in order to evaluate the cultural appropriateness of the tool in this setting.
Language used during Afrikaans ADOS-2 assessments
A discrepancy in the dialect used by the examiner and the children, as well as code-switching, was noted during ADOS-2 assessments with children classified as ‘non-spectrum’, as well as with the child classified on the ‘autism spectrum’. However, the dialect discrepancy and code-switching did not appear to impact the quality of the assessments. We therefore recommend that, for future Afrikaans ADOS-2 assessments with this population, ‘standard’ Afrikaans could be used, but that examiners need to be sensitive to the language used by participants and that adjustments should be made to the formality of the words or language to accommodate participants, as required. This implies that the examiner needs to be familiar with and responsive to the difference between a ‘standard’ Afrikaans dialect and the distinct Kaaps dialect.
The words not understood by the caregivers/children indicated that important terminology (especially words pertaining to emotions) used by ADOS-2 examiners may require particular caution to ensure fair coding. If an examiner thinks a word was not understood by a participant, the examiner may need to clarify meaning with explanation, or provide a more commonly known Afrikaans/English alternative.
The appropriateness of the social interactions and activities in the ADOS-2
Social interactions
The results confirmed that children from this population socially interact with adults. It was, however, interesting that only about two-thirds of the caregivers reported regular/daily adult–child interaction. While the social interaction between an ADOS-2 examiner and a child participant may therefore be deemed culturally appropriate for the majority of participants, it will be important for examiners to remain mindful that this may not be a high-frequency activity for all children. Although the impact of the gender of the ADOS-2 examiner on the social interaction was not explored in this specific cultural context, it may be interesting to explore in future cultural studies of the ADOS-2.
Inappropriate ADOS-2 activities
Many activities appeared appropriate in this setting, but a few cultural or contextual factors may be important to consider. For instance, the unfamiliar map of the United States used during the Description of a Picture task may benefit from substitution with a more familiar scene. Our results also suggest that examiners should, perhaps before starting the Demonstration Task, ask participants from this population where they brush their teeth, if they use a basin, and clarify how many taps the basin has. If the participant has one tap, the examiner should ‘draw’ one tap only. If the participant has a different strategy or props for brushing teeth, these should be used for the task. The alternative demonstration of washing their hands with soap may require similar adaptation.
The Birthday Party activity as a whole was familiar to members of this population. However, certain elements were unfamiliar. The birthday party routine may be jeopardized by unfamiliarity with elements, including singing the Happy Birthday song and blowing out the candles on the cake if the birthday cake is unfamiliar. We recommend that examiners ask caregivers before the task is administered how a birthday party is typically performed and then use the familiar routine in the ADOS-2 activity. Where the birthday party is completely unfamiliar (not seen in our study), other forms of ritualized social events, such as having a tea party or a picnic (Lord et al., 2012), can be used instead, with similar cultural caveats.
Appropriateness and familiarity of ADOS-2 materials
Clinical and community sample participants reported familiarity with most of the ADOS-2 materials, suggesting that the standard materials in an ADOS-2 kit would be appropriate to use, with a range of materials that would be novel for a proportion of children. A number of interesting common themes emerged.
Given that all families were from low to middle SES backgrounds, it appeared that lack of financial resources, rather than cultural factors, determined familiarity and/or access to these materials.
Novelty is of course not unwelcome in the ADOS-2. What is important is the way the participant behaves and communicates (Lord et al., 2012). Encountering novel materials may elicit a response from a participant that could provide important data in an assessment. However, when any child encounters a novel play material the child might become preoccupied with the material which may be coded as a repetitive activity or interest. If a child appears preoccupied with a material to the extent that it may be interpreted as a restricted interest, examiners may need to check with a caregiver whether the material is novel to the child and interpret the behaviour with caution.
An examiner administering the ADOS-2 to a child from this population should keep gender biases pertaining to play materials in mind to ensure the comfort of both the caregiver and the child during the assessment. Particularly, during the Birthday Party activity an examiner may need to pay careful attention to how a male participant responds to playing with the baby doll. If he appears highly resistant to engaging with the baby doll and an examiner is confident that the resistance is attributable to the gender stereotype attached to male children playing with dolls, another form of ritualized social events may be used (e.g. having a picnic or tea party) to elicit functional and symbolic play.
Caregiver concern regarding ‘violent’ play materials was also very relevant. Many participants were from communities where violence is rife. Playing outside was therefore not an option for many children. Hence, it is understandable why many caregivers said that they do not want their children owning or playing with materials which could promote more violence.
If a child from this population appears hesitant or scared to touch the toy frog during the Functional and Symbolic Imitation activity, another material, like the car, could be used instead. Alternatively, the car could be used from the start of the administration.
Limitations and future directions
We acknowledge limitations to the study. First, the sample size was small, particularly the clinical sample size (n = 7). However, this sample was used to evaluate the language of the Afrikaans translation in a ‘live administration’ setting. Two Module 1, four Module 3 and one Module 4 ADOS-2 assessments were administered. There is significant overlap in the examiner script across Modules 1 to 4. Given that all of the activities found in Module 2 are found either in Module 1 or 3, we deemed it unnecessary to administer Module 2 for the purpose of evaluating language. Furthermore, for each of the assessments, we had the examiner, participant, caregiver and one to four researchers contribute to the comments on language. In effect, we therefore received data from a minimum of n = 28 ‘participants’. Additionally, we felt that we had reached thematic saturation from 7 clinical sample participants and 40 community sample participants (n = 40).
Second, we selected an interview format, given the relatively low adult literacy levels in Sub-Saharan Africa (59%; United Nations Educational, Scientific and Cultural Organization, 2014). There are suggestions that research participants are more likely to disclose personal information during self-administration of questionnaires, rather than during face-to-face interviews (Bowling, 2005). Although adopting an interview style ensured questionnaire completion, this method may have led to an over-representation of desirable responses and an under-representation of undesirable responses. However, caregivers were quite forthcoming about gender, language and so on, suggesting that caregivers did disclose appropriately. We took care to ensure that the researchers were young, Afrikaans-speaking people who would not have been perceived of different social or cultural status from participants. We acknowledge that we used a clinical sample of children from a developmental clinic referred for a range of possible concerns, rather than just high risk for ASD. We selected to do this for ethical reasons to evaluate the appropriateness of the Afrikaans translation, before applying it to a higher risk for ASD group. Our subsequent use of the Afrikaans ADOS-2 in an extension study with a high risk group supports these findings.
Overall, our results suggest that the Afrikaans ADOS-2 can be culturally appropriate for Afrikaans-speaking, coloured individuals from low-middle SES backgrounds residing in the Western Cape. Most of the language used in the assessments, the social interactions and activities found in the ADOS-2, and the ADOS-2 materials were appropriate for the community and clinical samples (including a participant with a child classified on the ‘autism spectrum’ by the ADOS-2). ADOS-2 examiners need to be mindful about administering the tool in a way which is sensitive to the culture of this community. We propose some guidelines (Table 3) for administering this tool to this specific population in a culturally sensitive way, which should facilitate assessments and limit method bias.
We recommend a similar parallel process of translation and cultural appropriateness evaluation when translating the ADOS-2 into other languages spoken in South Africa, as well as a similar ethnographic exploration in other low- and middle-income communities where little is known about play, social interaction and social activities. Needless to say, some of the method biases explored in this study may exist even in languages and communities where the English and European language versions of the ADOS-2 are in use. We propose that a careful, systematic and culturally respectful approach to social-communication instruments may teach us much about the linguistic and cultural subtleties of social-communication around the globe.
Footnotes
Acknowledgements
The authors wish to thank the parents, carers, children and research colleagues who participated in the project. Thanks to Mariza van Wyk, Michelle Hoogenhout, Christelle Duckitt, Leon Smith, Vanesia Smith, Niel Hoogenhout and Annalene van der Merwe, who all contributed to the translation process to date.
Declaration of conflicting interests
P.J.d.V. is an accredited international trainer on the ADOS-2, but does not receive any direct payments or royalties relating to the instruments.
Funding
L.S. is supported by the National Research Foundation (NRF). P.J.d.V. is supported by the NRF, the University of Cape Town Programme for the Enhancement of Research Capacity and the Struengmann Foundation.