
Abstract
Research studies using existing samples of individuals with autism spectrum disorders have identified differences in symptoms between males and females. Differences are typically reported in school age and adolescence, with similarities in symptom presentation at earlier ages. However, existing studies on sex differences are significantly limited, making it challenging to discern if, how, and at what point in development females with autism spectrum disorder actually exhibit a different behavioral presentation than males. The purpose of this study was to gather impressions from a large group of clinicians to isolate specific areas for future study of sex differences. Clinicians were surveyed about their opinions and perceptions of symptom severity in females, as compared to males, at different points during development. They were also asked to provide open-ended responses about female symptom presentation. Consistent with previous literature, clinicians noted more sex-related differences in restricted and repetitive behaviors and fewer differences for social communication features. Differences were most commonly observed in school age and adolescence, suggesting this time period as a critical and particularly vulnerable window for females with autism spectrum disorder. The results are discussed in the context of other male/female differences across development so that more targeted investigations of autism spectrum disorder sex differences across development.
Keywords
Introduction
Questions about sex-specific behavioral manifestations of autism spectrum disorder (ASD) remain of great interest (Frazier et al., 2014; Frazier and Hardan, 2016; Halladay et al., 2015; Lai et al., 2014; Werling and Geschwind, 2013; Zwaigenbaum et al., 2012) despite findings from many studies suggesting that there are more similarities than differences (Anderson et al., 2013; Baron-Cohen et al., 2003; Lord et al., 1982; Volkmar et al., 1993).Per a recent meta-analysis (Van Wijngaarden-Cremers et al., 2014), sex differences in the behavioral phenotype are limited to repetitive behaviors, and even then, only during later childhood. Presumably, the ongoing interest in sex differences is driven, in part, by clinical observations that girls with ASD just seem different (Lai et al., 2015). This, in turn, has inspired researchers to carry out male–female comparisons in large data repositories (e.g. Frazier et al., 2014). However, analyses of existing datasets are limited by reliance on diagnostic measures that were not designed to detect subtle or nuanced differences between individuals with ASD. It is also possible that these measures are biased toward detection of “male” symptoms since much of what we know about ASD has been based on observations of males (Constantino et al., 2010). Thus, findings that females with ASDs, particularly those with higher cognitive and language abilities, are more likely than males to be under-identified or diagnosed later (Begeer et al., 2013; Giarelli et al., 2010; Wilson et al., 2016) may be, in part, due to reduced sensitivity of currently available diagnostic instruments or diagnostic constructs for detecting ASD symptoms in females. Identifying additional or alternative constructs that are specific to females could then be reflected in future generations of diagnostic tools and criteria.
Sex differences in typical development
Although some attempts have been made to examine sex differences in ASD phenotypes in light of typical development (Auyeung et al., 2009) and in the context of specific, socially valid behaviors (Bishop et al., 2016), the majority of research in this area has focused on between-group comparisons of males and females with ASD. This is problematic given that many aspects of social functioning in typically developing populations are known to vary as a function of sex. In fact, researchers have long argued that social competence is defined by different sets of behaviors in girls versus boys (see Crombie, 1988), with girls demonstrating greater skills and competencies early on. Thus, while researchers and clinicians have hypothesized that females with ASD have milder impairments (Lai et al., 2015) and particular compensatory skills (Mandy et al., 2012), these sex differences in the behavioral phenotype of ASD may simply represent a recapitulation of the sex differences in typical development and gender socialization patterns, which should be considered in future work on sex differences.
There is a large body of literature that has identified sex differences in language/communication, social behaviors, peer relationships, and play at various points in development (Barbu et al., 2011; Hankin et al., 2007; Maccoby, 2000; Rose and Rudolph, 2006). In the early years, female children, as compared to males, generally demonstrate a “more advanced” trajectory of social development. As early as 6 months of age, typically developing female infants show better emotion regulation than males (Weinberg et al., 1999), and in siblings of children with ASD, female infants have been reported to show greater attention to social stimuli (Chawarska et al., 2016). Sex differences in the toy preferences of typically developing children are also present in the first year of life; in a study of 3- to 8-month-olds, females demonstrated a visual preference for a doll versus a toy truck, while boys demonstrated the opposite fixation pattern (Alexander et al., 2009). During early childhood, girls attain associative and cooperative play skills at younger ages than boys (Barbu et al., 2011), while typically developing boys demonstrate greater repetitive play and unusual interests in objects (Leekam et al., 2007). This pattern of sex differences continues to favor females across social development. Emotion recognition and verbal abilities tend to be better in females, whereas males may demonstrate a greater interest in non-social stimuli. Together, these observations have formed the basis of Baron-Cohen’s “extreme male brain” hypothesis of ASD (Baron-Cohen, 2002).
In addition to the early sex-based differences in behavior, typically developing females may be held to different behavioral standards than their male counterparts. For example, in childhood, shyness is socially acceptable and even encouraged for girls, but is less tolerated in boys (Doey et al., 2014). These expectations are reversed in later development, however. As girls make the transition from childhood to adolescence, social interactions and friendships shift from play and turn-taking toward a greater emphasis on relationship-building (Bauminger et al., 2003). During this developmental period, female peer relationships are characterized by complex relational skills, with interactions focused more on conversation, shared emotions, and emotional support (Hannah and Murachver, 1999).
Implications for females with ASD
Recognizing and understanding these sex differences across development should inform hypotheses regarding sex differences in ASD and implications for diagnosis and clinical practice. For example, higher expectations for social skills in adolescence likely “widen the gap” between pre-adolescent/adolescent females with and without ASD, resulting in certain impairments becoming more apparent as females with ASD get older (Cridland et al., 2014; Rivet, 2011; Wilson et al., 2016). While both school-age girls and boys with ASD have fewer social relationships and are more likely to be excluded or overlooked than typically developing peers, these differences may be even more pronounced for girls with ASD when compared to typically developing girls (Dean et al., 2014). These important discrepancies in social experience are lost, however, if girls with ASD are not compared to appropriate controls (i.e. same sex and same-aged peers). In a small sample of males and females (aged 10–16 years) with and without ASD, researchers found that, on a measure of friendship, average scores for females both with ASD and without ASD were significantly higher than for males (Head et al., 2014). Thus, a female with ASD, who exhibits relatively mild social communication difficulties compared to others with the disorder, may not clearly demonstrate deficits until compared to same-aged female peers without ASD.
Increased impairments in social competence compared to typically developing peers, greater complexity in social norms and expectations, and elevated risk factors for internalizing symptoms (i.e. minimal peer support and low self-concept) may make adolescent and young adult females with ASD particularly vulnerable. For example, adult females with ASD secure jobs at the same rate as males with ASD, but do not maintain employment as well as males (Taylor and Mailick, 2014). It has been hypothesized that employers may be less tolerant of social faux pas and that females may gravitate toward professions that require more social skills.
Increased vulnerability as females with ASD grow older may also occur as a result of comorbid or secondary mental health problems. It is well established that typically developing females are at greater risk for depression and anxiety during adolescence as compared to males (Costello et al., 2003; Frazier et al., 2014; Galambos et al., 2003; Gotham et al., 2015; Hankin et al., 1998; May et al., 2014; Oswald et al., 2016), and recent studies suggest that the same may be true of females with ASD when compared to boys with and without ASD (Gotham et al., 2015; Solomon et al., 2012) or typically developing girls (Jamison and Schuttler, 2015; Solomon et al., 2012). High levels of internalizing symptoms may be especially problematic, and may appear primary, when they occur in females who are not identified until later in life and therefore do not have the benefits of interventions and supports to cope with their ASD-related difficulties.
Thinking beyond traditional diagnostic conceptualizations
To determine whether there are sex differences in ASD-related symptoms and behaviors and whether commonly used assessment measures appropriately identify and describe females, it is also necessary to look beyond established diagnostic constructs and tools and employ a bottom-up method to elicit contemporary symptom descriptions. Hiller et al. (2014) recently used such an approach and by means of teacher and clinician reports, found evidence of a female profile characterized by mild social impairments and subthreshold restricted and repetitive behaviors (RRBs). In their sample of “high-functioning” children with ASD, girls were less likely to meet the RRB criteria for fixated interests, and for those that did, these interests fell within the category which researchers defined as “seemingly random” rather than specific to “screens” or “characters.” This particular pattern may hold true across samples and may help explain some reported sex differences, but it is not possible to corroborate these findings using large, currently available data repositories due to insufficient details provided by standardized diagnostic measures.
As exemplified by Hiller et al.’s work, moving beyond diagnostic measures may yield additional clues about phenotypic sex differences (or lack thereof) without the constraints that result from simply examining scores on existing measures. Eliciting the perspectives of expert reporters could serve as a platform for designing future studies and developing new research questions. Observations from expert clinicians may be most important to refine diagnostic criteria, as clinicians have the most experience with a wide range of ASD phenotypes as well as non-ASD populations. Yet, while the literature includes several anecdotal reports from clinicians of sex differences in ASD, few studies have systematically asked clinicians to reflect on their observations of sex differences in patients with ASD.
This study
In this study, we asked clinicians to reflect on their own perceptions of symptom severity in females with ASD (compared to males with ASD) within core domains and across developmental time points. Although the evidence supports some sex differences in ASD, with recent literature suggesting females demonstrate greater social impairment later in development, significant variability is observed in terms of how and when these differences occur. We focused on Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria in order to gather information with potential implications for diagnostic impressions and examined perceived symptom severity across time to better understand whether and when clinicians perceive females differently from males. Although perspectives of other professionals and parents are important, this study focuses on symptoms directly related to diagnostic criteria and thus we narrowed our sample to include clinicians actively engaged in diagnosing ASD. Given previous literature on signs and symptoms of ASD in females in comparison to males, we did not have any a priori hypotheses about the direction of severity on different features of ASD. Outcomes are discussed within the context of sex differences in typically developing males and females, including suggestions for further study. Specific research questions include the following.
Do clinicians report using different methods for the ASD diagnostic evaluations of females versus males?
How do clinicians perceive ASD symptom severity in females as compared to males? Do females demonstrate greater or similar rates of comorbid conditions? How does this differ at different developmental time points?
What specific behaviors or characteristics influence clinician perspectives of females with ASD?
Materials and methods
Respondents
Given the study questions, sample recruitment focused solely on clinicians who are actively engaged in the assessment and diagnosis of ASD and related disorders. We did not recruit or sample clinicians who solely provide intervention, teachers, or parents to ensure a homogeneous sample that is familiar with ASD diagnostic procedures and criteria. Survey participants were recruited via an email sent by Autism Science Foundation to 116 clinicians in the United States, the United Kingdom, and Canada who conduct ASD evaluations. The message encouraged participants to circulate the survey to other clinicians and collaborators with similar assessment experience. It was also posted on the Autism Science Foundation social media outlets including Facebook and Twitter and on the Facebook page of a collaborating non-profit foundation. From these attempts, a total of 106 clinicians completed the survey (see Table 1 for respondent demographics).
Summary of respondent characteristics.
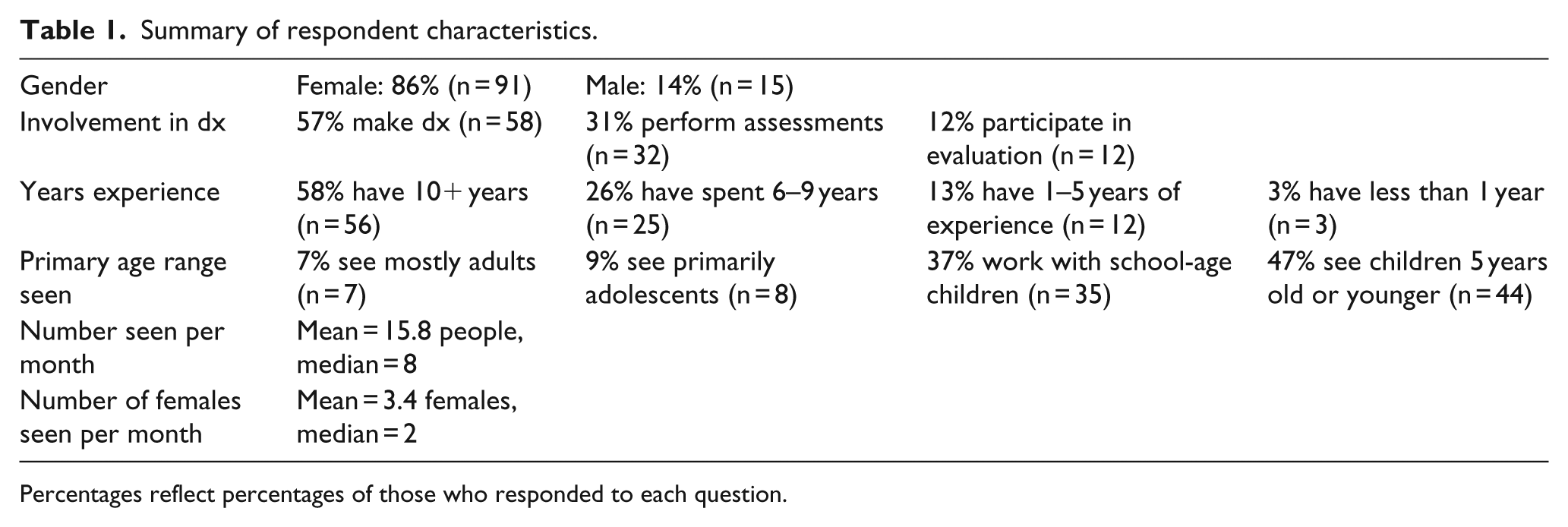
Percentages reflect percentages of those who responded to each question.
Survey questions
The study design is shown in Figure 1. Aside from respondent demographics and questions about clinician experience, the survey included questions about diagnostic methods and impressions. Respondents were asked to consider sex differences across the specific DSM-5 ASD criteria from diagnostic categories A and B as well as with respect to comorbid conditions (e.g. medical and other psychopathology). Additionally, clinicians were invited to provide qualitative information specific to their experiences of evaluating female children and adults.
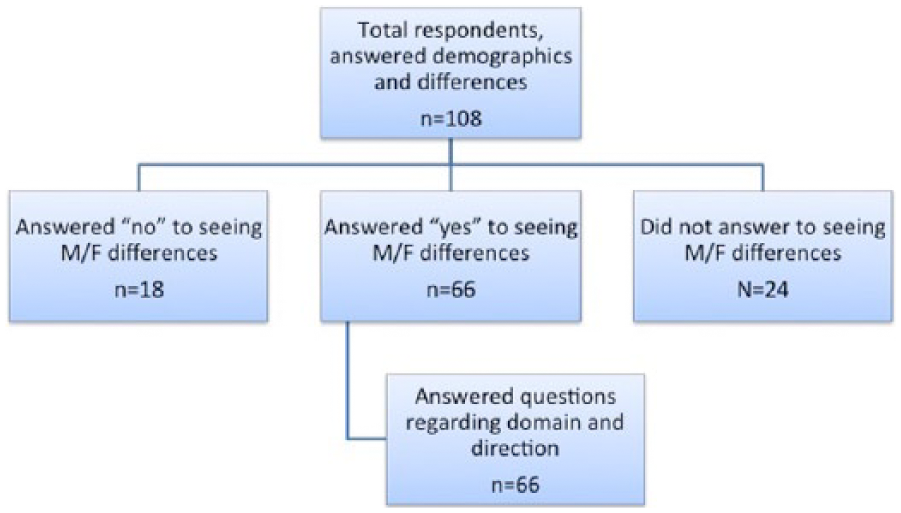
Study description.
For each behavioral dimension, respondents were asked to select one of the following: “females have less severe impairments,” “females are similar to males,” and “females have more severe impairments,” and within each identified age range: ages 0–5 years, labeled “early childhood”; ages 6–11 years labeled “school age”; ages 12–17 years labeled “adolescence”; and ages 18 years and above were labeled “adult.” These age groups were organized based on the National Health and Nutrition Examination Survey (NHANES) (Ogden et al., 2015).
Data analyses
The majority of findings are summarized utilizing descriptive statistics to reflect the proportion of clinicians making ratings within each severity category. We utilized a test of proportions to compare perceived severity for core ASD domains and associated symptoms. We did not make comparisons between criteria as this would result in a very large number of comparisons and thus significantly adjusted p values. In line with the purpose of the article, descriptive values allow for analysis of patterns of symptom severity within core domains of ASD and across time. Supplementary Table 3 summarizes perceived severity in DSM-5 symptoms at each identified age range, and Figures 2 to 6 illustrate perceived differences (less and more) and patterns over time. Qualitative findings were organized by theme in Supplementary Tables 3 and 4.
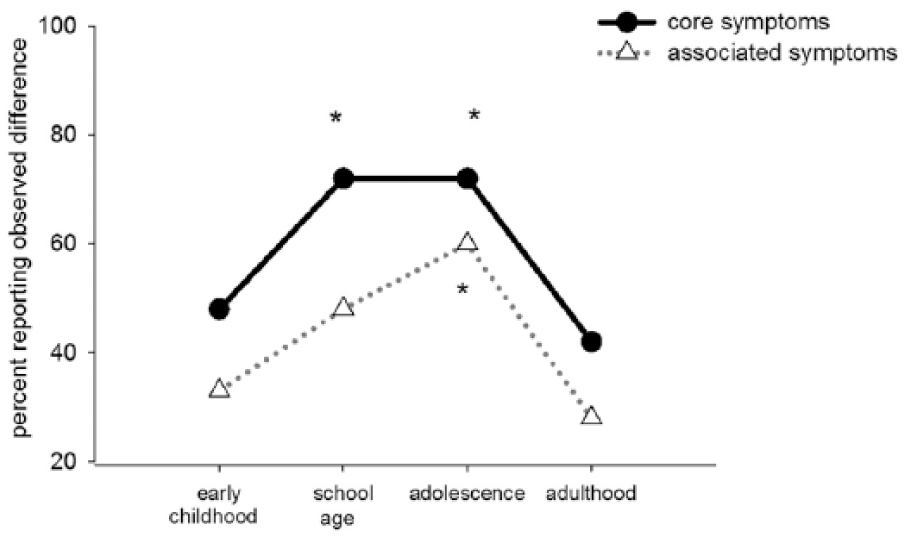
Percentage of respondents who noted differences in symptoms across time (core and associated symptoms).
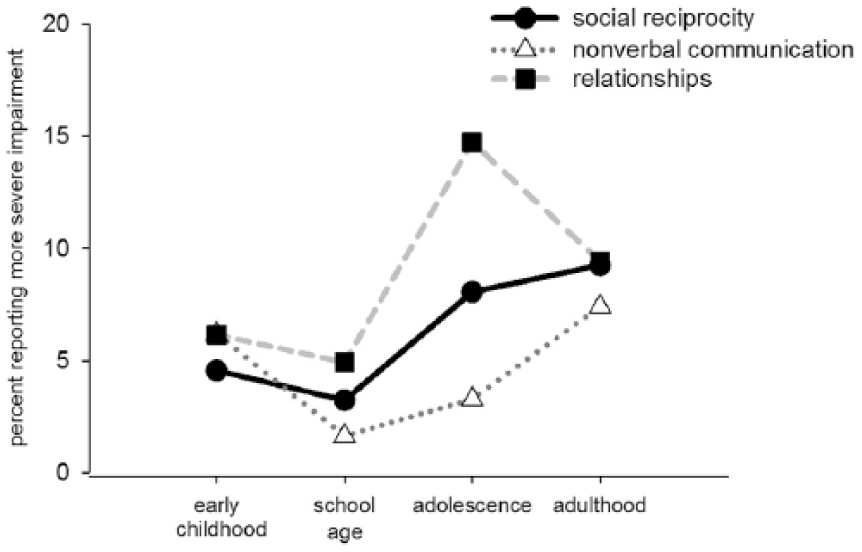
Percentage of respondents who responded that they observed more severe impairments in social communication behaviors across time (features from DSM-5 Part A).
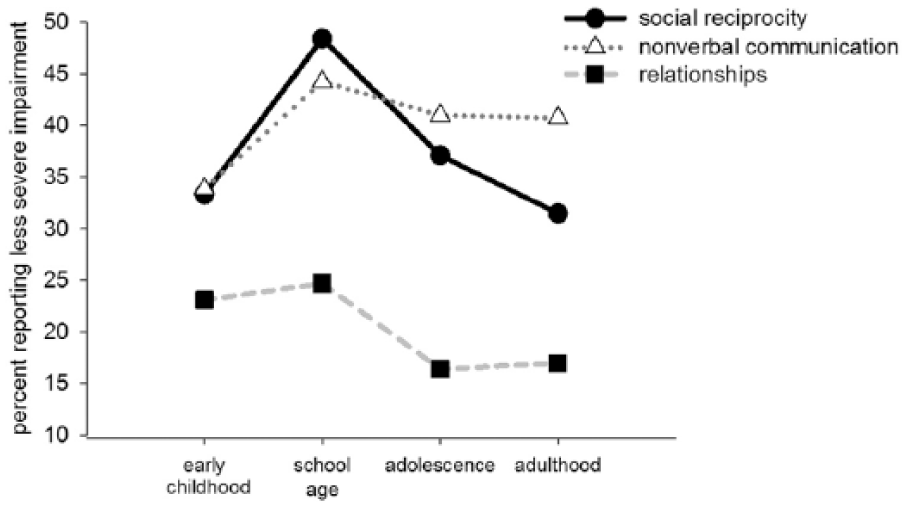
Percentage of respondents who responded that they observed less severe impairments in social communication behaviors across time (features from DSM-5 Part A).
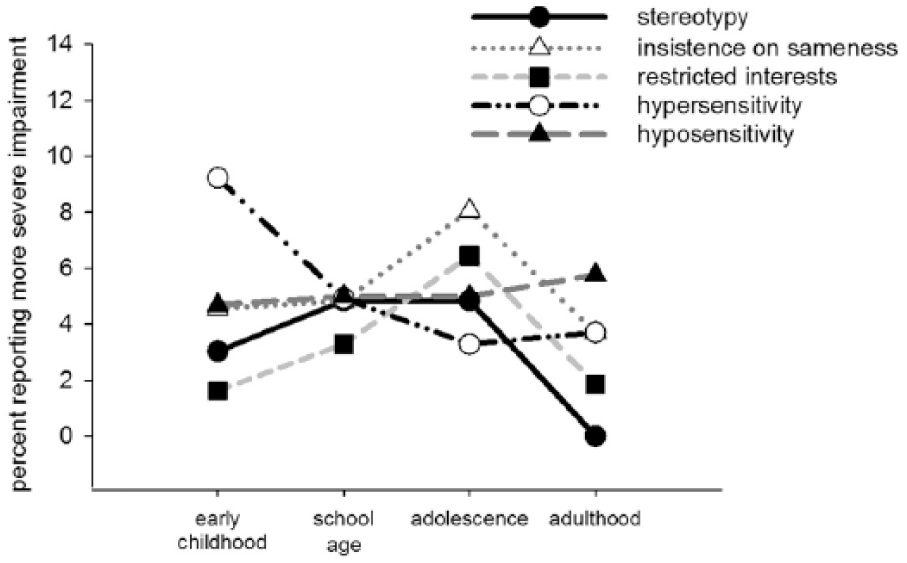
Percentage of respondents who responded that they observed more severe impairments in restrictive and repetitive behaviors across time (features from DSM-5 Part B).
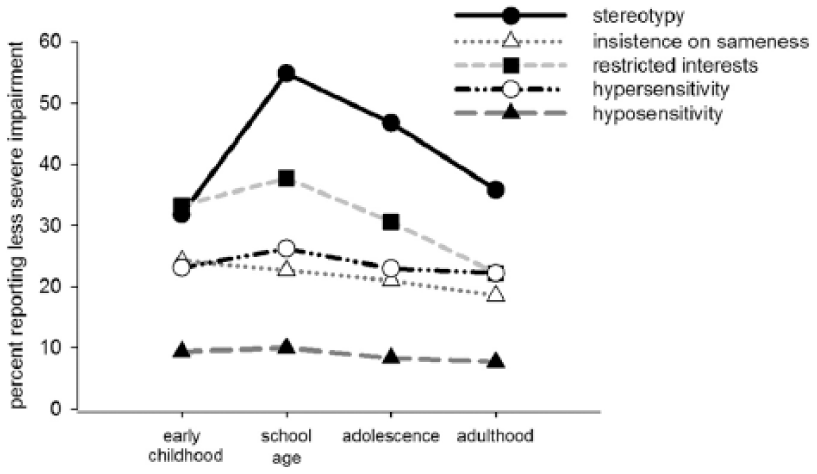
Percentage of respondents who responded that they observed less severe impairments in restrictive and repetitive behaviors across time (features from DSM-5 Part B).
Results
Respondent characteristics
Summary statistics of respondent demographics and characteristics are presented in Table 1. Most of the respondents were women (86%) and had over 10 years of clinical experience (58%). They reported seeing an average of 17 individuals with ASD per month, including approximately three females per month. Approximately half (47%) reported that the majority of their time is spent working with young children, while 37% work mainly with school-age children. Although a large percentage of clinicians reported spending a majority of their time with young children or those at school age, the sample represents expertise in ASD diagnosis and evaluations across development. Respondents were permitted to skip any question they considered out of the scope of their practice and expertise
Do clinicians report using different methods for the diagnostic evaluations of females versus males?
A large majority of the respondents (94%) indicated that they do not use a different methodology or instruments when making a diagnosis in males versus females. At the same time, 36% reported that when diagnosing females, they rely “more” on clinical impressions based on observational assessments. A minority of those polled (15%) indicated they rely on standardized instruments “less.”
How do clinicians perceive ASD symptom severity in females as compared to males?
Overall, 70% of clinicians reported perceived differences in the core symptoms of ASD. As noted in Figure 1, only those who reported differences in core symptoms were then asked to specify the type and direction in subsequent questions. Clinicians perceived substantially more differences in core symptoms during both the school age (72%) and adolescent (72%) time periods as compared to early childhood (49%) and adulthood (42%) (see Figure 2; z = −2.708, p = 0.007; z = −3.3925, p < 0.001; respectively). Results below are organized by developmental time point, as the pattern of male–female differences in specific symptom areas varied between age groups. Percentage of clinicians endorsing “more severe,” “less severe,” and “similar” are reported in Table 2 and graphically represented across development in Figures 3 to 6.
Direction of clinician responses in male/female differences in DSM-5 criteria across development.
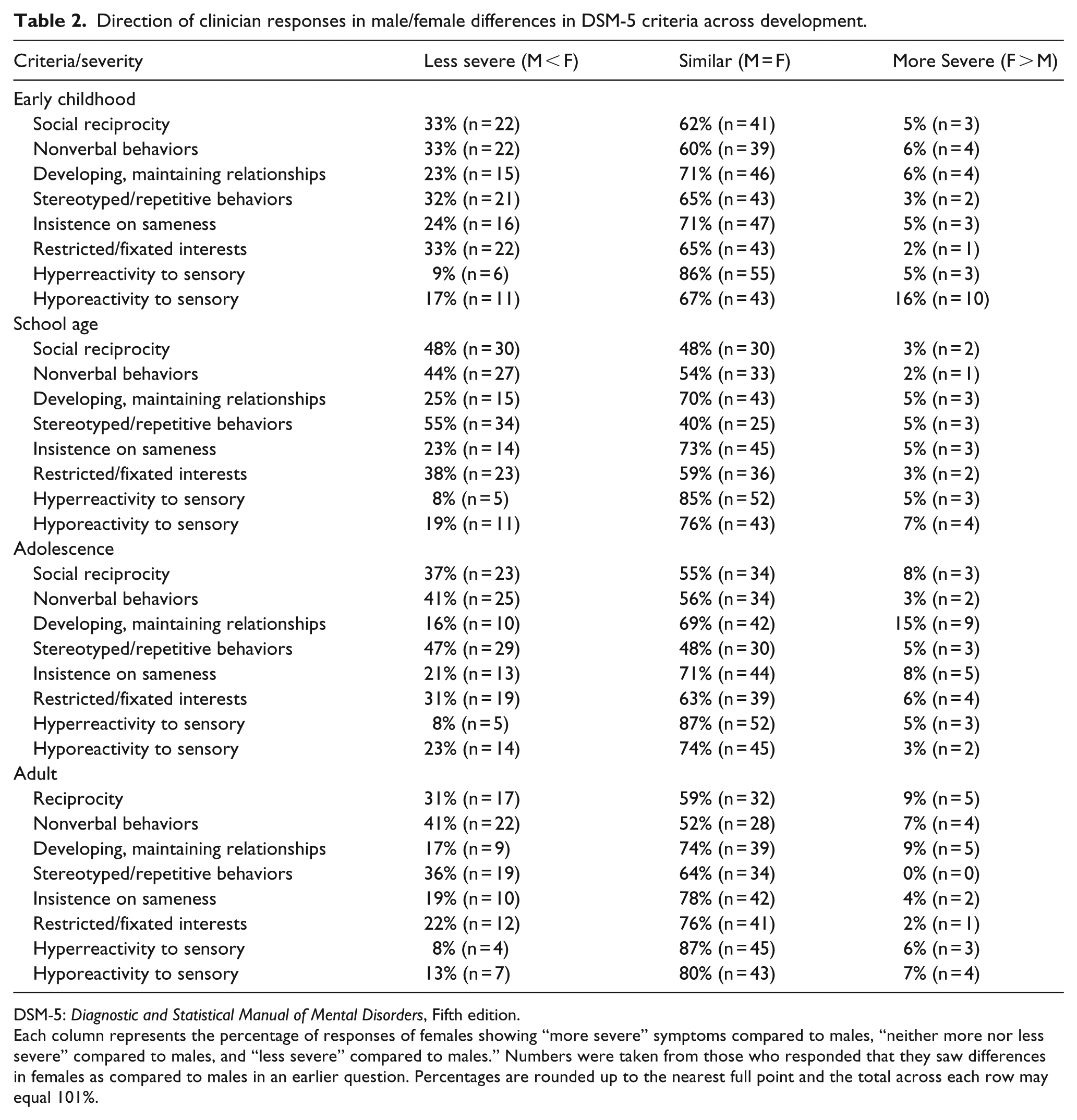
DSM-5: Diagnostic and Statistical Manual of Mental Disorders, Fifth edition.
Each column represents the percentage of responses of females showing “more severe” symptoms compared to males, “neither more nor less severe” compared to males, and “less severe” compared to males.” Numbers were taken from those who responded that they saw differences in females as compared to males in an earlier question. Percentages are rounded up to the nearest full point and the total across each row may equal 101%.
How (if at all) does perceived symptom severity differ across developmental periods?
Early childhood
In the Social Communication domain, clinicians most commonly responded that females were similar to males across all three subdomains, including Deficits in Social Reciprocity (62%), Nonverbal Communicative Behaviors Used for Social Interaction (60%), and Maintaining and Understanding Relationships (71%). The second most common response (23%–33%) was to rate females as having less severe impairments in comparison to males, with a higher proportion of clinicians (33%) reporting less severity in Deficits in Social Reciprocity and Nonverbal Communicative Behaviors compared to Deficits in Developing and Maintaining and Understanding Relationships (23%). Only a small percentage (5%–6%) of clinicians reported that females have more severe impairments in social communication behaviors during the early childhood period (Figure 3).
In the RRB domain, clinicians were again most likely to indicate that females in early childhood show similarly severe behaviors: Stereotyped or Repetitive Motor Movements (65%), Insistence on Sameness (72%), Highly Restricted, Fixated Interests (65%), Hyperreactivity to Sensory Input (68%), and Hyporeactivity to Sensory Input (86%). With the exception of Hyporeactivity to Sensory Input (9%), about one quarter to one-third of clinicians reported that females show less severe behaviors in the RRB subdomain, whereas only 1%–9% reported that females show more severe behaviors in any of the RRB subdomains (Figure 5). The largest proportion of clinicians (33%) reporting less severe symptoms in females was in the area of restricted and fixated interests (Figure 6).
For associated symptoms, the majority of clinicians indicated that females showed similar levels of medical (67%) and psychiatric comorbidities (83%) compared to males during the early childhood period. Approximately 59% indicated that females were equally likely as males to show deficits in intelligence quotient (IQ) during the early childhood period, but 26% reported that females were more likely to show deficits in IQ.
School age
The pattern for school age differed slightly, with a larger percentage of clinicians rating females as less severe for Deficits in Social Reciprocity and Nonverbal Communicative Behaviors Used for Social Interaction as compared to ratings in Early Childhood. That is, responses were more balanced between the categories of similar impairments as males (48% and 54%, respectively) and less severe impairments (48% and 44%, respectively) (Table 2). However, a similar pattern as seen in early childhood remained for Deficits in Developing, Maintaining, and Understanding Relationships with the most common response indicating similar severity in males and females (70%), followed by less severe in females (25%), and more severe in females (5%).
There is a pattern similar to early childhood in the RRB domain, showing that the most common response was that females were similar to males (59%–85%), with the exception of Stereotyped or Repetitive Motor Movements. For this criterion, 55% of clinicians reported that females have less severe behaviors during the school-age period, which is a significantly higher proportion when compared to the other RRB criteria (Figure 6). A small percentage of clinicians (3%–5%) rated any of the RRB criteria as being more severe in females during the school-age period.
Medical and psychiatric comorbidities were rated as being similarly common (75% and 73%, respectively) or less common (19% and 13%, respectively) in school-age females. Most clinicians reported that females are as likely as males to show Deficits in IQ during school age (66%), with the remaining responses split across less likely (16%) and more likely (18%).
Adolescence
Although the pattern of responses for social communication deficits during the adolescent period was generally similar to that observed for school age (i.e. most common response was females were similar to males), there is a significant shift with a greater percentage of clinicians rating females as having more severe impairments during adolescence than during school age and early childhood. This is especially apparent for Deficits in Social Reciprocity (8%) and Developing, Maintaining, and Understanding Relationships (15%). Figures 3 and 4 illustrate a decrease in the percentage of clinicians reporting less severity and an increase in clinicians reporting greater severity.
In terms of RRBs, clinicians indicated that females were most likely to show similar (48%) or less severe (47%) Stereotyped or Repetitive Behaviors (motor movements, language, and play) (Table 2). Again, response patterns suggest clinicians perceive females as less severed within this subdomain as compared to the other RRBs. The most common response across the other RRB subdomains was that females are similar to males, followed by females who show less impairment. Clinicians rarely indicated that females show more severe behaviors in the RRB subdomains during adolescence (3%–8%) (Figure 5).
Adulthood
Deficits in Social Reciprocity, Nonverbal Communicative Behaviors, and Developing, Maintaining, and Understanding Relationships were rated by most clinicians as being similar to (59%, 52%, and 74%, respectively) or less severe than males (32%, 41%, and 17%, respectively) in female adults. Again, Understanding Relationships has the lowest proportion of clinicians reporting females as less severe than males (Figure 4). Clinicians rated female adults as showing similarly severe or less severe behaviors than males across all of the RRB subdomains (64%–87%), and that Stereotyped or Repetitive Behaviors remain most likely to be rated as less severe compared to other subdomains. High levels of similarity in hyporeactivity to sensory input were also reported.
Associated symptoms
Approximately 54% of clinicians reported perceived differences in the associated symptoms (medical and psychiatric comorbidities, IQ) in females as compared to males (Figure 2). Clinicians indicated that these differences are most apparent during adolescence (59.72%) and school age (48.61%) as compared to early childhood (33.33%) and adulthood (27.78%). Follow-up tests examined the likelihood of specific associated symptoms to occur across age ranges. Although results show no differences in occurrence of medical comorbidities (χ2 = 4.7404, p = 0.578) or likelihood of IQ deficits (χ2 = 1.7972, p = 0.937) in females as compared to males, clinicians reported significant differences in the likelihood of psychiatric comorbidities (χ2 = 15.4116, p = 0.017). Furthermore, follow-up comparisons showed a significant peak at adolescence for more severe psychiatric comorbidities in females as compared to early childhood (Z = 3.40, p < 0.001) and school age (Z = 1.83, p = 0.067) with no changes in likelihood of “more severe” between adolescence and adults (Z = 0.55, p = 0.582).
Open-ended responses
Supplementary Tables 3 and 4 summarize the responses of clinicians for questions relating to challenges (Supplementary Table 3) and strengths (Supplementary Table 4) of girls and women with ASD. Participant responses were organized into themes. As seen in Table 4, many clinicians indicated that females tend to show relative strengths in particular social skills and nonverbal communication. However, common challenges observed in females include limited peer interactions, as well as social withdrawal or social anxiety (Supplementary Table 3). Some clinicians noted fewer RRBs, while others noted differences in presentation or interpretation. For example, clinician verbiage (Supplementary Table 4) described restricted interests as “typical,” “more socially acceptable,” or “often overlooked … because they are not always unusual in nature.” Future studies should include further inquiry regarding what clinicians perceive as typical or acceptable and consider how these perceptions may or may not influence diagnostic decisions.
Discussion
Unlike most researches on sex differences that compare scores on specific measures of ASD, this study examined the clinician perspective of symptom severity within core domains of autism and across different developmental time periods. Examining the perspectives of clinicians trained to diagnose ASD is essential given their expertise in both diagnostic differential and development; expert clinicians also have the experience of seeing a variety of ASD phenotypes.
This method also proved useful in identifying developmental periods where the most differences are observed. While results from this study suggest that overall, clinicians do perceive differences in females as compared to males, findings demonstrate variability in perceived severity and at what time point symptoms may be more or less severe or similar to their male counterparts. These data mirror some sex difference findings demonstrating that young females may present with less severe social difficulties and that social impairments become more apparent over time. Results are discussed within the context of core and associated symptoms of ASD, developmental trajectory, limitations of our sample and methodology, and implications for diagnosis and understanding females with ASD.
Clinician impressions
When asked to report about their own clinical experiences, approximately 70% of clinicians surveyed indicated that females appear different in core symptoms of ASD and 54% reported perceived differences in associated symptoms (e.g. sensory symptoms, medical comorbidities, and emotional difficulties). The magnitude of these perceived differences is large in comparison to sex differences reported within the extant literature and lends credence to continued efforts to understand sex differences. Clinicians also perceived these differences to be most apparent during school age and adolescence. Interestingly, when clinicians were asked to compare females to males on symptom severity within individual DSM-5 symptom domains and developmental periods, they most commonly responded that females were similar to males. For core symptoms, 48%–86% of clinicians rated symptom severity in females as similar to males. The second most common response (31%–55% of clinicians) was that females had less severe behaviors in these core symptom areas. These results were somewhat unexpected given that all respondents indicated perceived differences between males and females in the core domains of ASD. Although response options limit the potential variability in perceived severity, one would expect smaller proportions of clinicians to select the “similar” category. One potential explanation is that while clinicians perceive ASD as different in males and females, this may not equate to differences in severity but rather differences in the presentation or specific symptom profile of females and our qualitative results are consistent with this. Perhaps most important to consider, we did not ask clinicians to rate differences or symptom severity in comparison to expectations for typically developing females, which may well result in greater divergence in symptom severity when considering the male with and without ASD comparison.
Open-ended responses speak to the male–female differences and highlight the lack of consensus about differences symptom severity and variability across development. Responses suggest that some perceived differences in core symptoms may be driven by strengths exhibited by females, in particular social skills, such as increased joint attention skills and the ability to take another’s point of view or involve others in their interests. In addition, several clinicians reported that RRBs can appear more subtle in some females with ASD, which is one potential explanation for findings in some previous studies that demonstrated decreased RRBs in females with ASD (Van Wijngaarden-Cremers et al., 2014). Consistent with findings in recent studies of preschoolers with ASD (Harrop et al., 2016; Postorino et al., 2015), in this study, clinicians reported play skills, including imitative and imaginative play, as a common area of strength in females. This begs the question of whether the presence of these play skills may dampen reports of unusual behavior.
The disconnect between the clinician’s overall responses about perceived differences in females and their responses within each DSM-5 domain is notable; the gap suggests that clinician-observed sex differences may fall outside of our formal diagnostic criteria or that overall differences could be influenced by referencing typical development. Findings within the ASD sex differences literature often reveal limited differences in core characteristics, with greater differences reported based on observational measures (Dean et al., 2014; Harrop et al., 2015) or instruments capturing related features such as internalizing and externalizing symptoms (Frazier et al., 2014; Solomon et al., 2012), loneliness (Baldwin and Costley, 2015), and sex-dependent variation in adaptive behavior (Howe et al., 2015; Mandic-Maravic et al., 2015; Zwaigenbaum et al., 2012). However, our results also suggest that sex differences may exist and are limited to core ASD symptoms, with females showing relative strengths in use of certain basic social communication behaviors (e.g. eye contact and facial expression), with similar difficulties across sexes in interaction quality (Bishop et al., 2016).
Age and developmental level complicate examinations of sex differences in ASD and may help explain some of the inconsistent results across studies. A recent meta-analysis found that while several studies report that repetitive and stereotyped behaviors (RRBs) differ between males and females, differences in severity are clearest after the age of 6 years, but quite variable in early childhood (Van Wijngaarden-Cremers et al., 2014). Cognitive ability itself is also known to affect the presentation of RRBs. In ASD, a higher nonverbal ability is associated with milder RRBs over time, but only with respect to sensorimotor RRBs (Richler et al., 2010). For social communication behaviors, research similarly suggests that age and IQ interact with sex (e.g. Chawarska et al., 2016); yet, few studies include longitudinal designs or sufficiently large samples to adequately account for the effects of developmental level. Thus, even if sex differences do exist, our ability to detect differences could be obscured if they are only apparent during a particular developmental period or in a particular behavioral phenotype of ASD. Ascertainment issues further complicate such studies because, across the lifespan, referral and diagnostic trends may vary by sex and cognitive ability (Giarelli et al., 2010; Rutherford et al., 2016). Clearly, more research is needed to determine whether and how sex differences in ASD are affected by age and IQ.
Developmental changes
Results of this study also highlight the importance of considering developmental time period when examining potential sex differences. More clinicians reported perceived sex differences during adolescence and the school-age years. Nearly half (40%–50%) of clinicians reported Deficits in Social Reciprocity, deficits in Nonverbal Communicative Behaviors Used for Social Interaction, and stereotyped or repetitive behaviors as less severe in females within the school-age and adolescence categories. Results also demonstrated shifts toward greater similarity across development in some areas. These results could actually reflect an increase in social impairments across development for females as compared to males. For example, a peak in the frequency of more severe symptom presentation during adolescence within the social and communication criteria is consistent with findings demonstrating increased social impairments for females with ASD during this time period (McLennan et al., 1993; Rivet, 2011). The nature of social communication deficits during adolescence may be subtle and nuanced (Aggarwal and Angus, 2015). Thus, these findings are logical when considering the changes in social norms and expectations within adolescence and that sex differences in social behaviors suggest greater complexity for females in navigating relationships and communication styles. Existing research suggests typically developing adolescent females are at an increased risk for internalizing symptoms such as anxiety and depression as compared to males (Valla et al., 2010; World Health Organization (WHO), 2015). By adolescence, females are twice as likely to experience depression as compared to males (Bearman et al., 2003; Lewinsohn et al., 1998) and report lower levels of self-esteem (Puskar et al., 2010). Complexities in navigating and understanding social relationships, along with social impairments inherent in ASD, could lead to increased social impairments for adolescent females with ASD or a greater likelihood of receiving a diagnosis during the school-age or adolescent period. Peer rejection and limited friendships and social support, which are frequently experienced by individuals with ASD, may also increase the likelihood of developing internalizing disorders (Mazurek and Kanne, 2010). Peer relationship quality decreases with age (Orsmond et al., 2004), which along with sex as a risk factor increases the vulnerability of adolescent females with ASD. Peer social network centrality may be lower in later elementary school as compared to early elementary individuals with ASD (Rotheram-Fuller et al., 2010). In our data, clinicians were least likely to rate females as “less severe” on A3 (understanding relationships and reciprocal play) as compared to other criteria within the Social Communication domain. This pattern was consistent across age ranges, with fewer clinicians in the less severe category and an increased proportion reporting more severe within the adolescent and adult periods. Findings from our open-ended responses also support the notion that females become more impaired (or more impaired relative to typically developing females) during adolescence and have a high rate of co-existing psychiatric conditions as compared to males with ASD. Thus, while girls are less likely to be diagnosed or diagnosed later, they may be more negatively affected by ASD by the time they reach adolescence. This, in turn, leads to an increase in the number of girls being referred at certain ages, which then skews data in clinical databases and also colors clinicians’ perceptions. All of these problems clearly support the need for longitudinal research to examine sex differences in trajectories and outcome. As it is, ascertainment biases make it nearly impossible to use cross-sectional data to draw valid conclusions about sex by age interactions and phenotype.
Role of implicit bias
There may also be an implicit bias in diagnosing females with autism. Beyond individual factors, sex differences in the interpretation of female social behavior may explain why girls are diagnosed less frequently than boys. Such a bias is thought to exist across mental health disorders (WHO, 2015). This may also explain why girls often require additional symptomatology, such as intellectual disability and behavioral difficulties, over and above the symptoms of ASD to receive an ASD diagnosis. Other reports (Brereton et al., 2006; Dworzynski et al., 2012) similarly noted that females with ASD are just as likely as males with ASD to demonstrate disruptive behavior and attentional deficit and hyperactivity, a pattern different from that found in typically developing boys and girls. A recent study of adults reported that in a large clinic referred sample of adults, women were significantly less likely to receive a diagnosis of ASD after being referred for an evaluation (Wilson et al., 2016). The sum of these findings also mirrors conclusions from research on attention deficit hyperactivity disorder (ADHD). For example, in their review of sex differences in ADHD, Soffer et al. (2008) found that girls with ADHD require more severe behavior in order to be referred to a clinic. These authors also highlighted that girls demonstrate sex-specific symptoms; girls with ADHD demonstrated more internalizing symptoms and greater relational aggression, while boys demonstrate conduct disorder and other externalizing behaviors and peer aggression (Soffer et al., 2008). In fact, Keenan and Shaw (1997) have previously made the argument with respect to psychopathology in general; they propose that female children develop better adaptive skills and are socialized to internalize their psychopathology, both of which deter symptom expression. Our findings lend support to the former. Late diagnoses are a particularly problematic issue for girls with ASD (Aggarwal and Angus, 2015). On one hand, early in childhood, sex differences in socialization may make symptom detection difficult in girls, resulting in females underdiagnosed during this developmental period, and on the other hand, the onset of adolescence brings increased social expectations that create greater challenge and result in mood or anxiety symptoms that overshadow ASD symptoms. The result might be a more complex clinical picture by the time the affected female reaches a clinic evaluation.
Limitations
We interpret these data acknowledging potential limitations that may impact the validity of data and generalizability to a larger sample. Use of electronic mail and social media to recruit clinician respondents limited our ability to track and report a return rate for survey completion and could impact sample recruitment (e.g. clusters of clinicians with similar interests resulted from shared link via social media networks or email). These methods likely resulted in a high number of clinicians based in university settings with less representation of community-based clinicians. A limitation of this study is that most questions asked clinicians to compare males and females in terms of severity of impairments and did not clearly ask how females were different. It is possible that inconsistent findings may be at least partially attributed to differences in how “appropriate” behaviors are conceptualized by individual clinicians as a function of sex. That is, if clinicians are being asked to rate patient behavior compared to what would be “expected,” ratings may vary significantly depending on whom they select as their reference group. This raises the important question of how and against what data should be for compared on ASD-related symptoms in comparison to typically developing peers. In our survey, clinicians were asked to make severity ratings in comparison to males with ASD. However, it could be more informative to examine comparisons of social behaviors between females with ASD and their typically developing counterparts. We were unsure about clinician experience and exposure to typically developing females and therefore did not write questions in such a manner for this study. Sex differences in social behaviors and communication suggest same sex, typically developing individuals as the appropriate reference group for determining whether social behaviors are “decreased” or “impaired” and whether communication and other behaviors should be judged as “atypical” when making diagnostic impressions. This has implications for instrument development and normative samples and for a better understanding of social development, communication, and other behaviors expected across typical development, including variability between males and females and across time. Respondent characteristics could impact perspectives. Nearly all respondents were female, raising questions about how interpretations might differ between male and female clinicians. A large number of respondents reported a primary focus on the early childhood period, which may or may not limit their exposure to individuals across a variety of age ranges and thus their point of reference. Last, the small range of survey response options limits variability and thus ability to detect subtle changes in clinician’s perspective. Inquiring about general impressions regarding perceived differences in females with ASD may be qualitatively different from perceived severity of symptoms contributing to the unexpected proportions of clinicians reporting symptom severity as similar to males.
Future directions
A critical question arising from these data is where exactly we should go next with inquiries into phenotypic sex differences. These aggregate clinical impressions echo numerous one-off reports from individual clinicians suggesting that there “seems” to be something different about girls with ASD. However, quantitative analyses of large datasets have shown neither clear nor consistent differences. Inability to consistently detect differences may result from the use of tools that are not adequately fine-tuned to capture differences, or alternatively, what differences exist between one boy–girl pair may not exist between another, and thus differences may simply not exist at a group level. Given the growing consensus of changes in social behaviors and impairments across development, instruments and diagnostic criteria should consider age (or development) and socially valid comparison behaviors. Another possibility is that the clinicians responded by recapitulating what they have read in the literature. It is also possible that whereas clinicians see differences between females and males, these differences do not boil down to differences in severity per se, but in quality of impairments. The large proportion of clinicians in our study reporting perceived differences in core ASD domains in conjunction with limited variability in perceived symptom severity reiterates the inconsistencies within the literature. Anecdotal responses reflect changes in strengths and weaknesses across development. These data could aid in the interpretation of the existing literature and next steps in understanding sex differences. For example, researchers might shift focus from examining sex differences toward better understanding symptom expression within females and across development. The qualitative responses also provide some insight into next steps. For example, we could translate these qualitative responses into new questions or new measures that could be directly and systematically administered to large groups of girls and boys as a potential phenotypic measure.
Importantly, while these data still represent anecdotal reports, the ability to simultaneously evaluate anecdotal reports from more than 100 experienced clinicians is a strength of this study, and hopefully a step forward in understanding more about sex differences/similarities in ASD. Nevertheless, as long as we are limited to cross-sectional data from clinic-referral and convenience samples, the question of whether there are “really” differences will be difficult to answer.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.