
Abstract
The use of assisted reproduction technology has increased over the last two decades. Autism spectrum disorders and assisted reproduction technology share many risk factors. However, previous studies on the association between autism spectrum disorders and assisted reproduction technology have shown inconsistent results. The purpose of this study was to investigate the association between assisted reproduction technology and autism spectrum disorder diagnosis in a national birth cohort database. Furthermore, the results from the assisted reproduction technology and autism spectrum disorder propensity score matching exact matched datasets were compared. For this study, the 6- and 66-month Taiwan Birth Cohort Study datasets were used (N = 20,095). In all, 744 families were propensity score matching exact matched and selected as the assisted reproduction technology sample (ratio of assisted reproduction technology to controls: 1:2) and 415 families as the autism spectrum disorder sample (ratio of autism spectrum disorder to controls: 1:4). Using a national birth cohort dataset, controlling for the confounding factors of assisted reproduction technology conception and autism spectrum disorder diagnosis, both assisted reproduction technology and autism spectrum disorder propensity score matching matched datasets showed the same results of no association between assisted reproduction technology and autism spectrum disorder. Further study on the detailed information regarding the processes and methods of assisted reproduction technology may provide us with more information on the association between assisted reproduction technology and autism spectrum disorder.
Keywords
Introduction
The use of assisted reproduction technologies (ARTs), including in vitro fertilization, induced ovulation, and insemination, has increased over the last two decades (Andersen et al., 2007; Wright et al., 2007). The rate of conception using ART has increased from 1.0% in 2003 to 2.5% in 2013 (Ministry of Health and Welfare, 2014). In European countries, in vitro fertilization treatment accounts for an estimated 1.7%–5.9% of births in 2010 (Kupka et al., 2014); in the United States, the figure is 1.5% of births in 2013 (National Center for Chronic Disease Prevention and Health Promotion and Division of Reproductive Health, 2015). Therefore, safety measures and potential adverse effects related to these procedures need to be evaluated.
Besides the increased use of ART, the diagnosis of autism spectrum disorders (ASD) has also increased. The Centers for Disease Control and Prevention (2009) reported the prevalence of 1 in 110 for ASD in 2009 and 1 in 68 in 2014 in the United States (Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators and Centers for Disease Control and Prevention, 2014). Although the prevalence of ASD in Taiwan is much lower than that reported in the United States, the diagnosis of ASD has also increased annually. The Taiwan National Health Insurance database reported an annual incidence of 0.91 per 10,000 in 1997 to 4.41 per 10,000 in 2005 (Chien et al., 2011). Even with the dramatic increase in the incidence of ASD in Taiwan, an urban and education disparity between those screened out as being at high risk and those receiving the diagnoses of ASD still exists (Lung et al., 2016). A national birth cohort study in Taiwan found that children of mothers with higher level of education and living in the city had 2.37 times higher chance of being diagnosed with ASD compared to children of mothers with lower level of education and living in rural areas (Lung et al., 2016), showing that the uneven distribution of medical resources and the level of awareness of the parents may cause an under-diagnosis of ASD in Taiwan.
ASD and ART share the same risk factors: older parental age (Glasson et al., 2004; Idring et al., 2014; Sandin et al., 2012) and hormonal disturbances (Auyeung et al., 2009; Ingudomnukul et al., 2007). Furthermore, the use of ART leads to higher rates of preterm delivery and low birth weight (Lung et al., 2009), factors which have been found to be associated with ASD (Hultman et al., 2002; Larsson et al., 2005). Thus, the use of ART is a factor that potentially contributes to ASD. Three mechanisms linking ART with ASD have been proposed: first, parental infertility (such as hormonal disturbances) may be related to epigenetic changes leading both to an infertile state requiring ART and to ASD. Second, ART procedures may be related to ASD. Third, genetic susceptibility to ASD may be combined with the ART process (Zachor and Itzchak, 2011). However, previous studies on the association between ART and ASD have obtained inconsistent results (meta-analysis and systematic review: Conti et al., 2013; Hvidtjørn et al., 2009). It has been hypothesized that the heterogeneous etiology of ASD may explain why weak associations between ASD and ART are shown in larger samples (Coo et al., 2008). A large sample Finnish case–control study found no association between ASD and ART (Lehti et al., 2013). A Swedish population-based study found that the use of in vitro fertilization with intracytoplasmic sperm injection for paternal infertility was associated with a small increase in the relative risk of ASD (Sandin et al., 2013). Another Danish population-based study found that children conceived using ART had an increased risk of being diagnosed with ASD; however, this association disappeared after controlling for maternal age, educational level, parity, smoking, birth weight, and multiplicity of births (Hvidtjørn et al., 2011). Fountain et al. (2015) found similar results of the association between ART and ASD greatly reduced after the adverse prenatal and perinatal outcomes and multiple births are adjusted, showing the importance of controlling for confounding factors. Although population-based datasets can provide us with more information reflecting the population of interest, such large data also have a propensity of being sensitive in detecting statistically significant results which may not have clinical relevance. The Taiwan Birth Cohort Study (TBCS) was established with the intention of creating a sample that would be representative of children in Taiwan; a total of 20,095 children and families were sampled. To reduce the possibility of false positive caused by the large sample size, the exact matching approach of the propensity score matching (PSM) method was used. In this study, two different datasets were sampled: in one, variables associated with those being conceived using ART were controlled for, while in the other, matched by ASD diagnosis. Comparing the results from both datasets will provide us with more information regarding the association between ART and ASD.
Therefore, the purpose of this study was to investigate the association between ART and ASD diagnosis in a national birth cohort database. The PSM was used to control for the confounding variables associated with conception using ART and ASD diagnosis. The results from the ART and ASD PSM exact matched datasets were compared.
Materials and methods
Participants
This study used the TBCS database, which was established using a national household probability sampling method in order to create a sample that would be representative of children in Taiwan. All babies born between October 2003 and January 2004 in Taiwan were eligible for inclusion in the TBCS, with no exclusion criteria. The method of two-stage stratified random sampling was used. In the first stage, the primary sampling units were cities and towns; 85 townships were selected from among the total of 369 townships in Taiwan by systematic random sampling and then grouped into 12 strata according to four levels of size of the settlement in which the subjects were resident and three levels of total fertility rate. In the second stage, newborns were proportionally selected according to the rate of births from the 85 selected settlements (Lung et al., 2011). The initial sample selected for the TBCS was 24,200 families. The final sample at 6 months included 21,248 families (selection rate: 11.7%); 20,172 (94.94%) of these families agreed to remain in the study at 18 months, 19,908 (93.96%) at 36 months, and 19,721 (92.81%) at 66 months. In this work, the data collected at 6 and 66 months were used. Power calculation showed, with an odds ratio of 1.05 and power of 0.8, a sample of 20,616 is needed, which is close to our TBCS complete dataset.
Using the PSM method, participants were selected based on variables associated with ART. Cases conceived using ART and controls were selected at a ratio of 1:2; 248 children were conceived using ART, so 496 controls were selected, resulting in a final sample of 744. In another dataset, variables associated with ASD were controlled for using the PSM method. Children diagnosed with ASD and controls were selected at a ratio of 1:4; in total, 83 children diagnosed with ASD were matched with several variables, so 332 controls were selected, resulting in a final sample of 415.
At each stage of the study, after the parents had agreed to participate in the TBCS, a trained researcher would visit their homes and conduct a structured interview collecting data on variables that may affect the children’s health and development. Data on the demographics of the parents and children were collected when the children were 6 months old. The TBCS protocol was approved by the institutional review board of a teaching hospital in Taiwan and was conducted in accordance with the principles of the Declaration of Helsinki. After providing a detailed explanation of the study, written informed consent was obtained from the parents of all children at each stage of the study.
The structured interview at 66 months included a question asking the parents or main caregivers “Have a physician or special education specialist ever told you your child had autism or Asperger’s syndrome?” The answer to this question was used to indicate diagnosis of ASD in this study.
Statistical analysis
Demographic data on the children and their parents were analyzed using SPSS 21.0 software for Windows (Chicago, IL, USA). Bayesian analysis was used to produce data for missing points and for participants unable to be included in the follow-up process. Analysis of variance (ANOVA) was used to compare the age and level of education of the parents of those conceived using ART and those conceived spontaneously. Similarly, the age and level of education of the parents of those diagnosed with ASD and the controls were also compared.
Two datasets were sampled using the PSM exact matching method. The first dataset was matched by children conceived using ART, and the other was matched by those diagnosed with ASD. All variables collected were matched and controlled in the selection process. These variables included children’s characteristic of sex, having been breastfed or not, type of delivery, birth weight, gestational weeks at birth, single or multiple births, whether the child had been hospitalized previously; parental characteristics of parental age and level of education, place of residence (living in an urban or rural area), and living within 3 km from an incinerator. The PSM exact matching method provides a natural weighting scheme that yields unbiased estimates of the impact of treatment to yield an unbiased estimate of this impact. This can be achieved by controlling for the single propensity score, which encapsulates multiple characteristics relevant to the differences between any two units (King et al., 2011). The PSM implementation presented by Thoemmes (2012) is adapted in this study.
Logistic regression was used to investigate the associations of parental level of education, age, location of residence, conception using ART, sex of the child, being a twin, and being born prematurely with a diagnosis of ASD at 66 months. Both the ART and the ASD exact matching datasets were analyzed. The complete regression model and a parsimonious regression model are presented, meaning that only statistically significant variables (p < 0.05) are presented.
Results
The TBCS datasets from 6 and 66 months were combined, resulting in a final sample of 20,095 children and families in the complete dataset. The ART PSM exact matching dataset included 744 sets of data, while the ASD diagnosed exact matching dataset included 415. The demographic data of the three datasets are shown in Table 1. In the complete TBCS dataset of 20,095 children, approximately half were boys (52.5%), 88 (0.4%) had been diagnosed with ASD at 66 months, and 492 (2.4%) had been conceived using ART. In the ART PSM exact matched dataset, 6 (0.8%) were diagnosed with ASD; while in the ASD PSM exact matched dataset, 6 (1.4%) were conceived using ART.
Demographic data of the children and their parents.
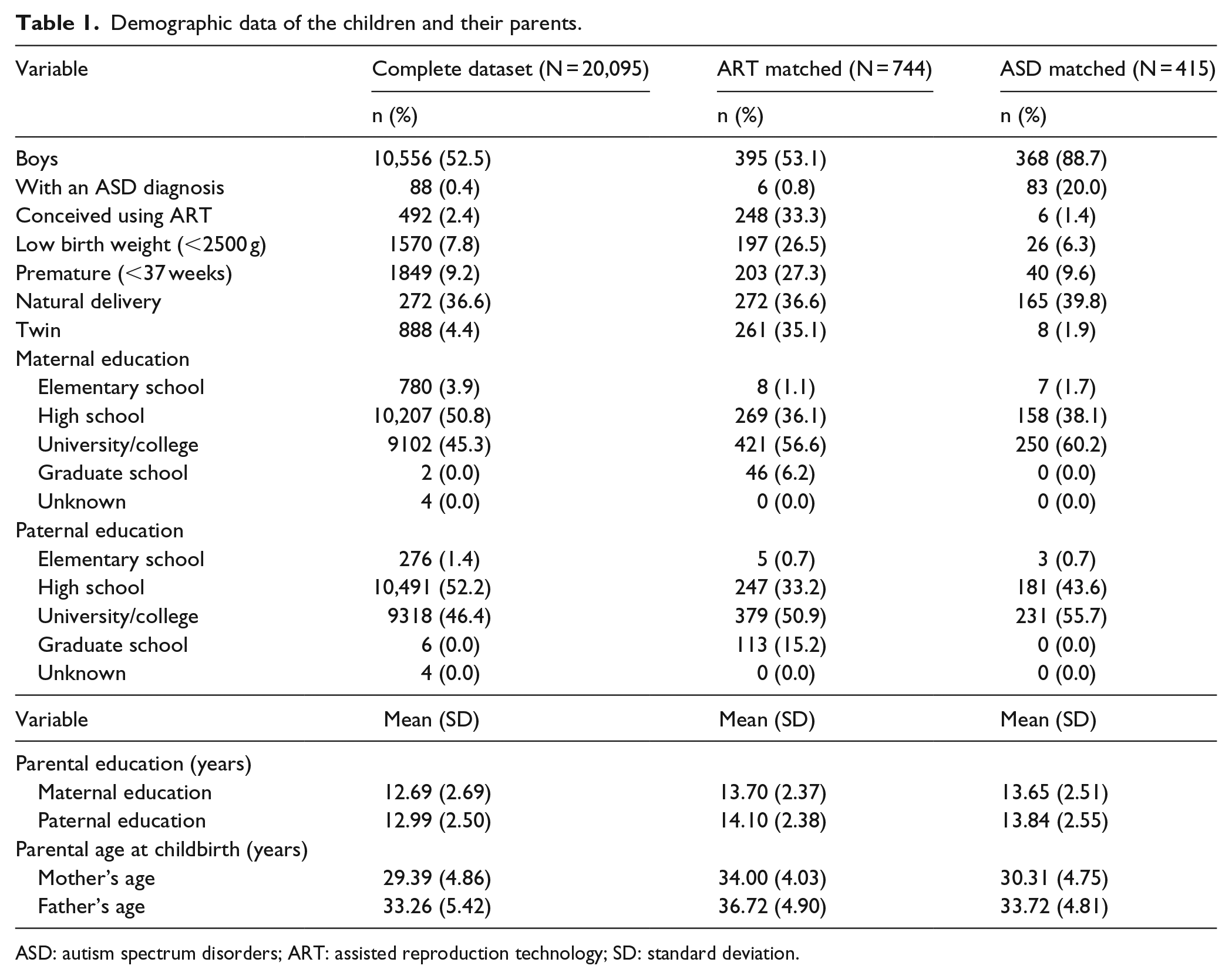
ASD: autism spectrum disorders; ART: assisted reproduction technology; SD: standard deviation.
With the complete dataset, analysis using ANOVA found that the parents of children conceived by ART were significantly older (maternal age: F = 281.53, p < 0.001; paternal age: F = 130.89, p < 0.001) and more highly educated (maternal education: F = 18.56, p < 0.001; paternal education: F = 32.73, p < 0.001) than those of children conceived spontaneously (Table 2). Similarly, mothers of children diagnosed with ASD were significantly older (F = 5.73, p = 0.017), and both parents were more highly educated than parents of children who had not received such a diagnosis (maternal education: F = 18.56, p < 0.001; paternal education: F = 32.73, p < 0.001).
Age and level of education of parents of children conceived using ART, diagnosed with ASD, and controls (N = 20,095).
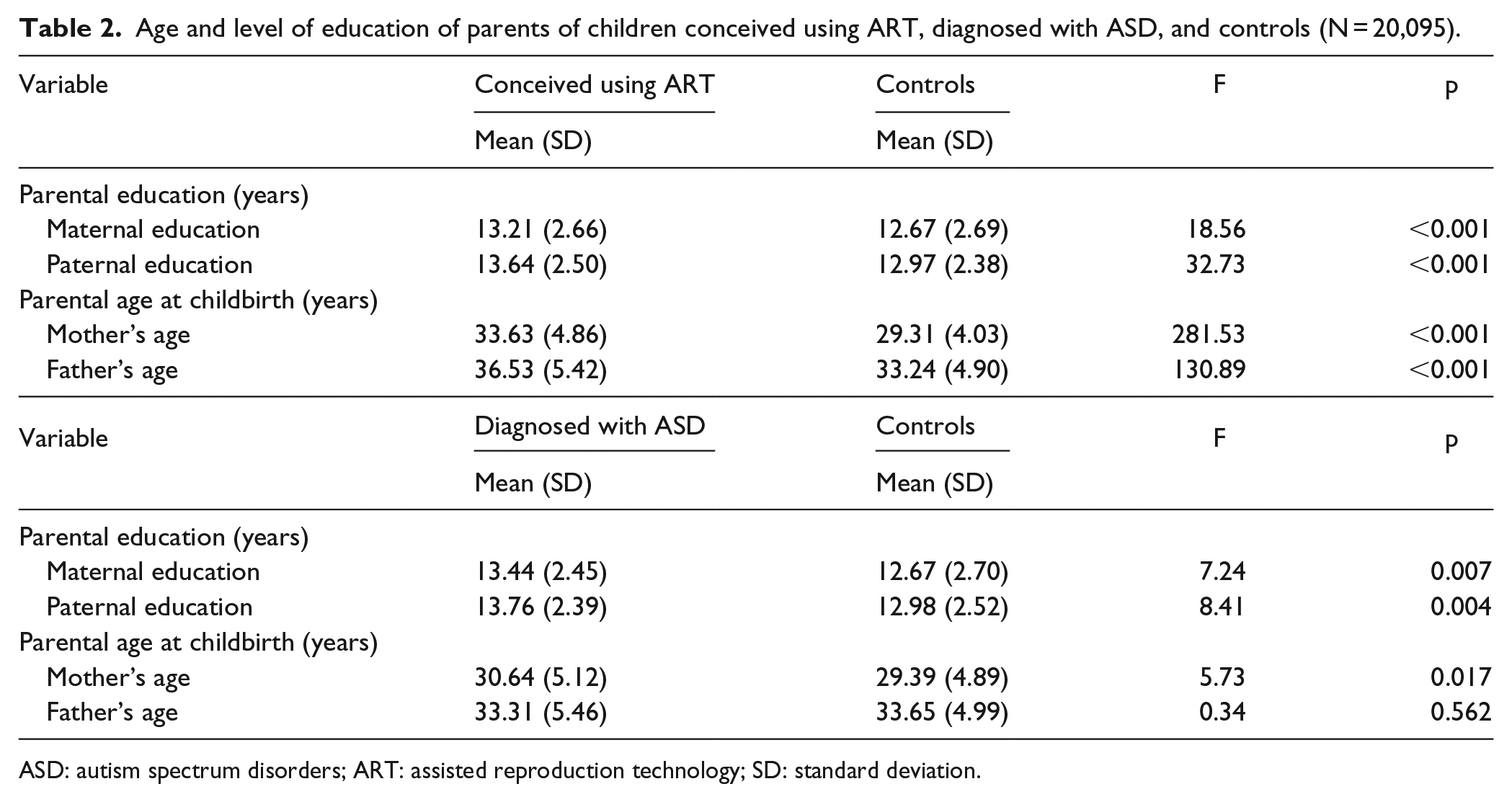
ASD: autism spectrum disorders; ART: assisted reproduction technology; SD: standard deviation.
Logistic regression was used to analyze the predictors of a diagnosis of ASD in the complete dataset, ART- and the ASD-matched datasets, as shown in Table 3. Parental level of education, parental age, location of residence, conception using ART, sex of the child, being a twin, and being born prematurely were analyzed as potential predictors of being diagnosed with ASD at 66 months. Paternal level of education, living in an urban area, sex, and low birth weight were found to be predictors for ASD (β = 0.10, p = 0.030; β = 0.63, p = 0.008; β = −1.86, p < 0.001; β = 0.65, p = 0.047). In the ART-matched dataset, the parsimonious regression model showed that the only predictor of a diagnosis of ASD was low birth weight (β = 1.73, p = 0.047). Similar results were found in the ASD-matched dataset, with only low birth weight being identified as a predictor of ASD diagnosis in the parsimonious regression model (β = 1.17, p = 0.005; β = 1.73, p = 0.047). Being conceived using ART was not associated with a diagnosis of ASD in the complete dataset, the ART-, or the ASD-matched datasets.
Parsimonious logistic regression results of the predictors of ASD diagnosis using the complete dataset, ART- and ASD-matched datasets.
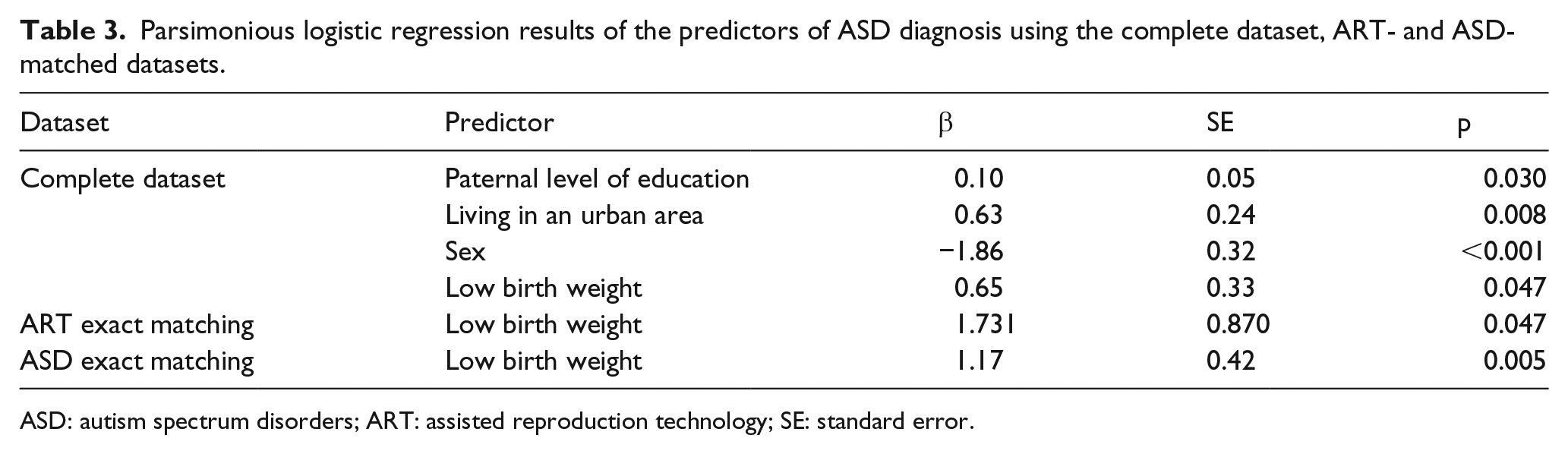
ASD: autism spectrum disorders; ART: assisted reproduction technology; SE: standard error.
Discussion
This study examined ART as a potential risk factor associated with ASD using a large national birth cohort dataset (TBCS). To reduce the possible significance caused by such a large dataset, two PSM samples were selected: one matched by those conceived using ART and the other by those diagnosed with ASD at 66 months. The PSM exact matching methods involve adjustment for demographic factors associated with ART and ASD, thereby reducing confounding bias. Our results showed no association between ART conception and ASD diagnosis at 66 months. However, low birth weight was associated with reported ASD diagnosis at 66 months in both the ART- and the ASD-matched datasets.
The TBCS dataset, which is representative of children and families in Taiwan, showed that among the 20,095 children, 492 (2.4%) were conceived using ART and 88 children (0.4%) had been diagnosed with ASD at 66 months. The rate of ART conception is consistent with the rate of 1.0%–2.5% births of children conceived using ART between 2003 and 2013 in Taiwan (Ministry of Health and Welfare, 2014). This is similar to the rate of 1%–4% of births conceived using ART reported for European countries (Andersen et al., 2007) and 3.06% in Israel (Zachor and Itzchak, 2011). However, the rate of children diagnosed with ASD is 0.4%, which is much lower than the recent finding of 1 in 68 found in the United States (Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators and Centers for Disease Control and Prevention, 2014). However, the prevalence of ASD in our study is still higher than the annual incidence of 4.41 per 10,000 found in the Taiwan National Health Insurance database in 2005 (Chien et al., 2011). From the TBCS pilot dataset at 36 months, it was found that 18% of children were identified as being at high risk of an ASD diagnosis using the Modified Checklist for Autism in Toddlers (M-CHAT; Lung et al., 2011). Another TBCS study found that at 66 months, an urban and education disparity was found in those screened out by the M-CHAT and those diagnosed with ASD (Lung et al., 2016). Children of mothers with higher level of education and living in the city had 2.37 times higher chance of being diagnosed with ASD compared to children of mothers with lower level of education and living in rural areas (Lung et al., 2016). This shows that due to the uneven distribution of medical resources and level of awareness of the parents, there is an under-diagnosis of ASD in Taiwan, which would explain the low prevalence found in our study. Besides the level of awareness of ASD in a particular society, the cultural influence of stigma associated with ASD (Chiu et al., 2013) may also affect the rate of diagnosis. Family stigma, a type of affiliate stigma, is the stigma experienced by family members as a consequence of being associated with a stigmatized relative (Larson and Corrigan, 2008). One study has shown that caregivers of children with developmental delay in Hong Kong show a higher level of affiliate stigma than those in Israel (Werner and Shulman, 2015). This may be associated with the fact that Chinese culture is characterized by collectivism, emphasizing the close links between individuals, in which the group is prioritized over the individual. Additionally, among parents of children with ASD, intellectual disability, and physical disability, caregivers of children with ASD have been reported to experience the greatest stigma (Werner and Shulman, 2015). Thus, although Taiwan has a universal healthcare system in which everyone should have equal access to healthcare, a lack of awareness among parents and the stigma associated with a diagnosis of ASD may have led to this spectrum of disorders continuing to be under-diagnosed in this country.
In this study, analysis of the complete dataset showed that the parents of those conceived using ART were significantly older and more highly educated than the parents of children conceived spontaneously. Similarly, the mothers of children diagnosed with ASD were older, and both mothers and fathers were more highly educated than the parents of children who had not received such a diagnosis. Parental age is an important confounding factor in the association between ART and ASD because the users of ART are more likely to be older and to have chromosomal abnormalities than fertile individuals (Agarwal et al., 2005). An association between advanced parental age and ASD has been found in previous studies (Idring et al., 2014; Sandin et al., 2012). Biologically, older mothers have an increased risk of obstetric complications (Cnattingius et al., 1992), which increases the risk of ASD (Gardener et al., 2011). On the contrary, older fathers are associated with ASD-linked de novo copy number variation (Kong et al., 2012; O’Roak et al., 2012). In terms of the level of education of parents, in accordance with the awareness hypothesis, older, more educated parents are more able to identify their children’s difficulties and to seek an appropriate medical diagnosis. Correspondingly, a previous study found that children from families with a higher socioeconomic status are more likely to receive a diagnosis of ASD than those from families with a low status (Thomas et al., 2012). The differences between the age and level of education of the parents of children diagnosed with ASD and the controls as identified in this study also emphasize the importance of parental awareness regarding children’s development and ASD for the diagnosis of this spectrum of conditions, supporting the validity of the awareness hypothesis in explaining the under-diagnosis of ASD in Taiwan.
In the ASD and ART PSM matched datasets, all variables associated with ASD and ART were controlled for, and in both datasets, no association between ART and ASD was found. This is consistent with the results of a systematic review and a population-based study of ART and ASD, which after adjustment for potential confounders, such as maternal age, multiplicity of births, parity, prematurity, and birth weight, found no significant association between ART and ASD (Conti et al., 2013; Hvidtjørn et al., 2011). In studies that did find an association between ART and ASD, the study design was of a lower quality or the sample size was smaller (Conti et al., 2013). A comparison of the genotype of ASD patients who had been conceived with and without the use of ART also showed no increase in the rate of ASD-associated genetic events in the former group (Ackerman et al., 2014).
In addition, both ART and ASD PSM matched datasets found low birth weight to be a risk factor for ASD. Both birth weight and ASD have been shown to be heritable (Clausson et al., 2000), increasing the possibility that shared genetic variants could act as confounders influencing both characteristics. Studies have found an increased prevalence of ASD in children with very low birth weight (1000–1500 g) and extremely low birth weight (<1000 g; Dudova et al., 2014), with a 3.2-fold higher risk of ASD in children with very low birth weight compared with that in normal controls (Singh et al., 2013). It has been suggested that there is a shared genetic mechanism involved in ASD and low birth weight, including a polymorphism in the gene for insulin-like growth factor-I, which was found to be associated with lower birth weight (Vaessen et al., 2002); this gene and others that are associated with a predisposition to a low birth weight may in part account for the association between low birth weight and ASD.
In the ASD PSM exact matched dataset, 368 (88.7%) selected cases were boys, and only 83 of 88 children diagnosed with ASD were matched. This may happen when matching for a rare event such as the diagnosis of ASD. In the process of performing the PSM, data balancing is performed in terms of the differences between the two groups that affect the dependent variable (in this case, ASD diagnosis; Guo and Freser, 2010). Since the children in the TBCS sample were randomly selected, but the children diagnosed with ASD are not randomly assigned to their family of origin, in the original TBCS dataset, when there are differences in the demographic data between the parents, this would certainly lead to statistically significant between-group differences (Neely-Barnes et al., 2014). Furthermore, frequency statistics is likely to happen in a large sample size like that of the TBCS dataset. Therefore, even though many cases were lost through the PSM matching process, this approach is still the best option to answer our research question in comparing ART conceived and spontaneously conceived with ASD diagnosis.
One of the limitations of our study was the failure to collect information regarding the applied method of ART. Different methods and processes of ART may have different prenatal effects, and previous studies have found a possible risk of ASD in mothers who underwent ovulation induction and were exposed to follicle-stimulating hormone (Hvidtjørn et al., 2011; Lyall et al., 2012). Furthermore, a population-based study found that the use of in vitro fertilization with intracytoplasmic sperm injection for paternal infertility was associated with a small increase in the relative risk of ASD (Sandin et al., 2013). Another limitation of our study is that the clinical diagnosis of ASD was based on parental reports, and no standardized ASD diagnostic assessment tool was used. Furthermore, no information regarding the details of the diagnosis or co-morbidity with other conditions (such as intellectual disability) was collected. However, the 0.4% incidence of ASD diagnosis is still higher than the annual incidence of 0.04% or the cumulative prevalence of 0.29% found in the Taiwan National Health Insurance database in 2005, which includes over 99% of the population in Taiwan (Chien et al., 2011). Furthermore, previous studies have found that nationally representative surveys of parents have produced ASD prevalence and demographic patterns that are comparable with estimates from population-based studies that relied on medical and special education record abstraction (Autism and Developmental Disabilities Monitoring Network Surveillance Year 2002 Principal Investigators and Centers for Disease Control and Prevention, 2007; Centers for Disease Control and Prevention, 2006). Therefore, the TBCS dataset used in our study is still representative of the ASD prevalence in Taiwan.
Using a national birth cohort dataset, controlling for the confounding factors of those being conceived using ART and having a diagnosis of ASD using the method of PSM exact matching, our results provide support that children conceived using ART were not at higher risk of being diagnosed with ASD. Further study on the detailed information regarding the processes and methods of ART, standardized assessment of ASD, or more information on the diagnosis of ASD may shed more light on the association between different methods of ART and the diagnosis of ASD.
Supplemental Material
AUT690492_Lay_Abstract – Supplemental material for Assisted reproductive technology has no association with autism spectrum disorders: The Taiwan Birth Cohort Study
Supplemental material, AUT690492_Lay_Abstract for Assisted reproductive technology has no association with autism spectrum disorders: The Taiwan Birth Cohort Study by For-Wey Lung, Tung-Liang Chiang, Shio-Jean Lin, Meng-Chih Lee and Bih-Ching Shu in Autism
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Bureau of Health Promotion (grant numbers DOH94-HP-1802, DOH95-HP-1802, DOH96-HP-1702, and DOH99-HP-1702).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.