
Abstract
We examined associations between child body mass index at 2–5 years and maternal pre-pregnancy body mass index, gestational weight gain, and rapid weight gain during infancy in children with autism spectrum disorder, developmental delays, or population controls. The Study to Explore Early Development is a multi-site case–control study of children, aged 2–5 years, classified as autism spectrum disorder (n = 668), developmental delays (n = 914), or population controls (n = 884). Maternal gestational weight gain was compared to the Institute of Medicine recommendations. Rapid weight gain was a change in weight-for-age z-scores from birth to 6 months > 0.67 standard deviations. After adjusting for case status, mothers with pre-pregnancy overweight/obesity were 2.38 times (95% confidence interval: 1.96–2.90) more likely, and mothers who exceeded gestational weight gain recommendations were 1.48 times (95% confidence interval: 1.17–1.87) more likely, to have an overweight/obese child than other mothers (P < 0.001). Children with autism spectrum disorder showed the highest frequency of rapid weight gain (44%) and were 3.47 times (95% confidence interval: 1.85–6.51) more likely to be overweight/obese as children with autism spectrum disorder without rapid weight gain (P < 0.001). Helping mothers achieve a healthy pre-pregnancy body mass index and gestational weight gain represent important targets for all children. Healthy infant growth patterns carry special importance for children at increased risk for an autism spectrum disorder diagnosis.
Introduction
Obesity rates among US youth have tripled in the last 30 years and have reached an all-time high, with 17.4% of youth having obesity (body mass index (BMI)-for-age ⩾95th percentile) in 2013–2014 (Skinner et al., 2016). Children with autism spectrum disorder (ASD) are disproportionately affected by overweight/obesity (Broder-Fingert et al., 2014; Curtin et al., 2010; Kral et al., 2015; Phillips et al., 2014). A recent analysis (Hill et al., 2015) compared overweight/obesity rates among children from the general population using data from the National Health and Nutrition Examination Survey (2007–2012) and children with ASD who were enrolled in the Autism Speaks Autism Treatment Network database (2008–2013). For children aged 2–5 years, 32.1% of children with ASD compared with 23.5% of typically developing children met criteria for overweight/obesity (BMI-for-age ⩾85th percentile) and 16.0% of children with ASD compared with 10.1% of typically developing children met criteria for obesity.
Several early life risk factors have been identified which pose an increased risk for childhood obesity. Maternal pre-pregnancy BMI is an important predictor of offspring weight status during childhood (Berkowitz et al., 2003; Woo Baidal et al., 2016). Data from a retrospective cohort study showed that maternal obesity during the first trimester of pregnancy more than doubled the risk of obesity in children aged 2 and 4 years (Whitaker, 2004). A higher maternal pre-pregnancy BMI was also strongly associated with exceeding the Institute of Medicine (IOM) recommendations for gestational weight gain (GWG) (Deputy et al., 2015), which has been identified as a risk factor for obesity in the offspring during childhood (Sridhar et al., 2014). Evidence also suggests rapid weight gain during infancy is a risk factor for childhood obesity (Druet et al., 2012; Stettler et al., 2003). While early life risk factors for childhood obesity have been extensively studied in children with typical development, data in children with developmental disabilities, including those with ASD and developmental delays and disorders, are scarce. If it is found that early life risk factors are associated with weight status during early childhood in children with developmental disabilities, this knowledge will shed light into possible mechanisms underlying the increased obesity risk in this population and offer targets for early intervention.
The aim of this analysis was to examine the associations of maternal pre-pregnancy BMI, GWG, and rapid weight gain during infancy with weight status in pre-school children classified as ASD, developmental delays or disorders (DD), and general population controls (POP). Data for this analysis are drawn from a large geographically diverse multi-site, case-control study that includes two distinct groups of children with developmental disabilities.
Patients and methods
Design and participant ascertainment
The Study to Explore Early Development (SEED) is a case–control study, implemented in 6 U.S. sites, with community-based ascertainment of children aged 2–5 years (born 2003–2006) classified as ASD, DD, or POP. Data were collected between 2007 and 2011. The original sample included 3899 children (ASD: N = 722; Possible ASD: N = 584; DD: N = 1304; POP: N = 1289). We excluded possible cases and children (N = 849) who had (1) missing infant or current anthropometric data, (2) biologically implausible values (months 0–6: weight-for-age z-scores <–5 or >5; ages 2–5 years: BMI z-scores <–4 or >5) (Centers for Disease Control and Prevention, 2016), or (3) mothers with a BMI < 14.5 kg/m2. The final sample included 2466 children (ASD: N = 668; DD: N = 914; POP: N = 884).
Details of the SEED methodology were previously published (Schendel et al., 2012). ASD and DD participants were identified from special education and clinical sources providing services to children with disabilities. Children had special education or International Classification for Disease codes indicative of autism/ASD or other developmental disabilities. POP participants were selected from random samples of birth certificates within each site’s defined geographic study area. All study groups completed an in-person general developmental assessment. Children with Social Communication Questionnaire (SCQ) scores ⩾ 11 were designated as potential ASD cases regardless of initial identification method. All children with a previous ASD diagnosis or special education classification were considered potential ASD cases regardless of their SCQ scores. Final ASD case classification was based on scores from gold standard evaluation tools, the Autism Diagnostic Observation Schedule and Autism Diagnostic Interview—Revised. Some children with ASD also had cognitive delays (e.g. developmental delay or intellectual disability), but they remained in the ASD group. Children designated as potential ASD cases not meeting research criteria as an ASD case, were classified as DD or POP, depending on how they were initially identified. Caregivers completed an interview about family sociodemographics, reproductive history, and index child pregnancy. The study was approved by the Institutional Review Boards at the Centers for Disease Control and Prevention (CDC) and all study sites.
Child weight and birth variables
Child weights and lengths from birth to 6 months of age were ascertained from neonatal and pediatric medical records. Child current weights and heights were measured by trained staff during an in-person clinic visit. Weight was measured on a digital scale and standing height on a stadiometer with children wearing light clothing and shoes removed. Child age- and sex-specific weight and BMI percentiles and z-scores were calculated using the World Health Organization Growth Charts (birth to 24 months) (World Health Organization, 2006) and the CDC Growth Charts 2000 (>24 months) (Ogden et al., 2002). Children were classified as underweight (BMI-for-age < 5th percentile), normal-weight (BMI-for-age 5–84th percentile), overweight (BMI-for-age 85–94th percentile), or obese (BMI-for-age ⩾95th percentile).
Rapid weight gain during infancy was defined as a change in weight-for-age z-scores from birth to 6 months >0.67 standard deviation (SD) (Monteiro and Victora, 2005). This 0.67 SD represents an increase in weight on a standard growth chart that would be equal to crossing upward by at least one weight centile band (Ong and Loos, 2006).
Several birth variables were selected based on clinical significance and were assessed for their effect on infant growth during pregnancy and early childhood: (1) birth weight from medical record, (2) gestational age categorized based on infants’ estimated date of delivery (maternal report) and converted to weeks of gestation, and (3) duration of breastfeeding (never, 0–3 months, 3–6 months, >6 months) from maternal interviews. Term was defined as 37 to ⩽41 weeks gestation and post-term as >41 weeks. Level of prematurity was defined as moderate to late preterm at 32 to <37 weeks and very or extremely preterm at <32 weeks gestation (World Health Organization, 2017).
Maternal weight variables, medical conditions, and smoking status
Maternal self-reported height and pre-pregnancy weight were derived from the maternal interview. Maternal pre-pregnancy BMI was calculated as weight (kg) divided by height (m) squared. Mothers were classified as underweight (BMI < 18.5 kg/m2), normal-weight (BMI 18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), or obese (⩾30 kg/m2) (Expert Panel on the Identification, Evaluation, and Treatment of Overweight in Adults, 1998). GWG was determined by subtracting mothers’ pre-pregnancy weight from their recorded weight at delivery. Maternal GWG adequacy was determined by comparing weight gain to the IOM guidelines for weight gain during pregnancy according to pre-pregnancy BMI (underweight: 12.5–18.0 kg; normal-weight: 11.5–16.0 kg; overweight: 7.0–11.5 kg; obese: 5.0–9.0 kg) and categorized as meeting or not meeting (above or below) the weight gain recommendations (Institute of Medicine et al., 2009).
Several maternal conditions were selected based on clinical significance and assessed for the effect on infant growth during pregnancy: (1) pre-pregnancy or gestational diabetes, (2) high blood pressure (BP) before or during pregnancy and pregnancy-related high BP conditions (eclampsia, pregnancy-induced hypertension, HELLP (hemolysis, elevated liver enzymes, low platelet count) syndrome), (3) eating disorders (bulimia nervosa, anorexia nervosa, or dieting during pregnancy), (4) intrauterine growth restriction (IUGR), and (5) smoking during pregnancy. Data for pre-pregnancy and gestational diabetes, pregnancy-induced hypertension, and IUGR were abstracted from medical records; data for eclampsia, HELLP syndrome, and high BP were abstracted from medical records and maternal interviews (if data from medical records not available); data for eating disorders were abstracted from medical records, maternal interviews, and medical history forms; and data for maternal smoking were abstracted from the maternal interview.
Statistical analysis
Data were analyzed using the SAS System for Windows (Version 9.3; SAS Institute, Cary, NC). Bivariate analyses assessed differences in demographic/anthropometric characteristics and maternal medical conditions by case status using analysis of variance (ANOVA), Kruskal–Wallis, independent t-tests, or Wilcoxon tests for continuous variables and chi-square/Fisher’s exact tests for categorical variables. A generalized linear model (PROC GENMOD) assessed the association between maternal pre-pregnancy BMI, GWG (met, above, or below IOM recommendation), rapid weight gain, and case status on child BMI status (overweight/obese vs underweight/normal-weight) at ages 2–5 years. The interaction between predictors and case status was tested for significance in all models. The influence of demographic, maternal, and birth variables on outcomes was tested by adding these variables as covariates to the models. Maternal and child demographic covariates included maternal education, race/ethnicity, poverty status, child age, and sex. Poverty status was determined using the U.S. Census Bureau 2015 Poverty Thresholds (United States Census Bureau, 2015). Maternal covariates included diabetes, high BP conditions, eating disorders, IUGR, and smoking status. Birth covariates included birth weight, prematurity status, and breastfeeding duration. Analyses related to the association between maternal GWG and child weight status excluded mothers with preterm infants (N = 414) to avoid misclassification of IOM status due to a shortened gestational period. P-values < 0.05 were considered statistically significant.
Results
Demographic, anthropometric, and medical characteristics of sample
At the clinic visit, children were, on average, 59 months of age across groups (Table 1). A significantly higher proportion of children with ASD were male (82%). Children with ASD showed the highest frequency of rapid weight gain (44.0%) during the first 6 months of life when compared with children in the DD (35.9%) and POP (33.3%) groups. Children with ASD showed higher overweight/obesity rates than children in the POP group (P < 0.001), but not the DD group (P = 0.247). A significantly smaller proportion of mothers in the ASD (P < 0.001) and DD (P < 0.001) groups than mothers in the POP group attended college; a higher proportion of mothers in the ASD group lived below the poverty level (P < 0.001); and a higher proportion of mothers in the POP group were White (P < 0.001). Mothers in the ASD and DD groups showed higher pre-pregnancy overweight/obesity rates than mothers of the POP group. There was a significant relationship between GWG adequacy and case status: the proportion of mothers not meeting the recommendations for GWG adequacy in the ASD and DD groups was higher (65%) than in the POP group (59%). Mothers in the ASD and DD groups showed higher prevalence of gestational diabetes, hypertension, and smoking during pregnancy and a greater proportion of them breastfed for <3 months compared to mothers in the POP group. Fewer mothers in the POP group delivered preterm babies (14%) compared to mothers in the ASD (20.8%) and DD (26.9%) groups, respectively.
Demographic and anthropometric characteristics of children and mothers and maternal medical conditions by group.
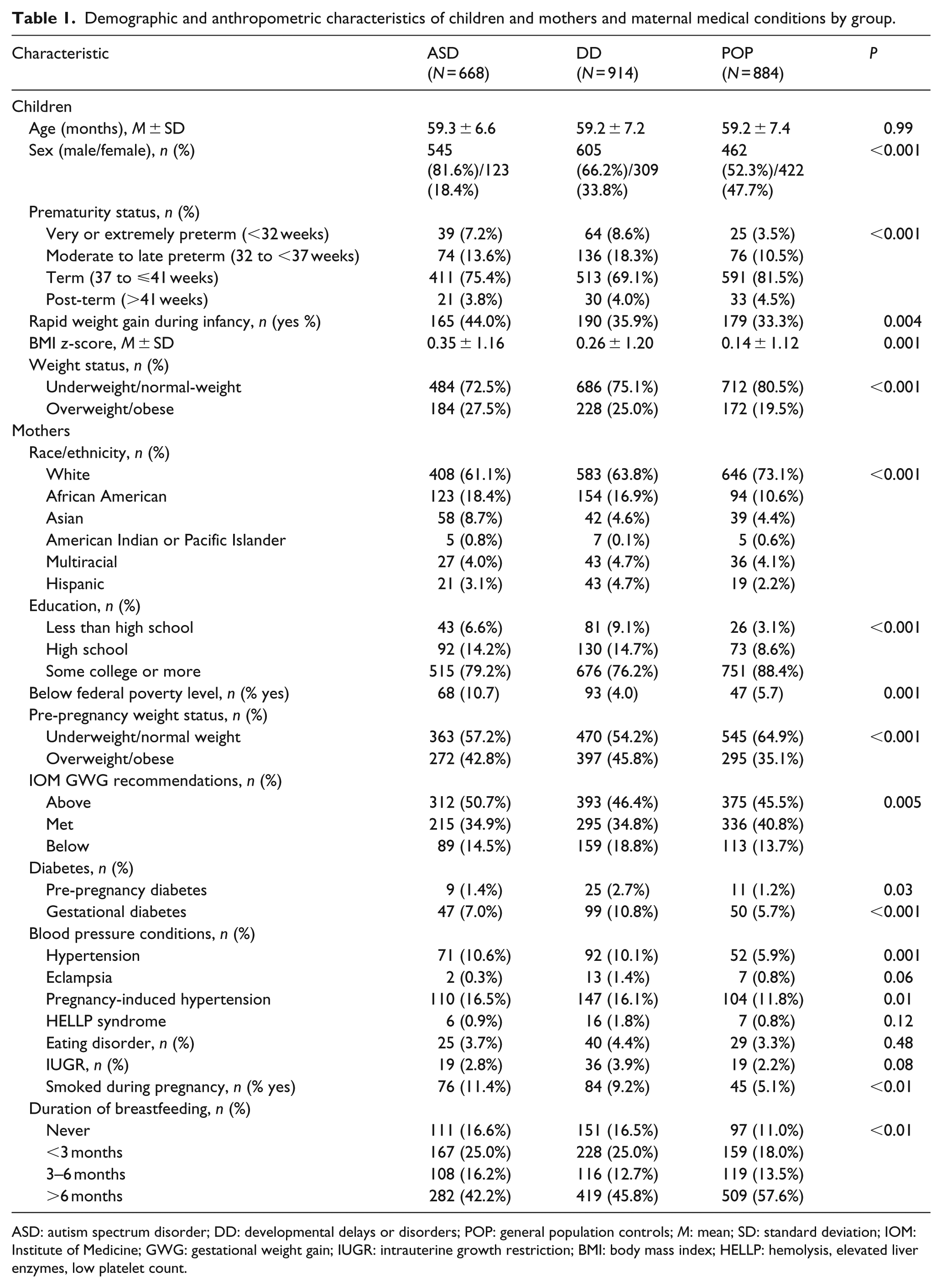
ASD: autism spectrum disorder; DD: developmental delays or disorders; POP: general population controls; M: mean; SD: standard deviation; IOM: Institute of Medicine; GWG: gestational weight gain; IUGR: intrauterine growth restriction; BMI: body mass index; HELLP: hemolysis, elevated liver enzymes, low platelet count.
Maternal pre-pregnancy weight status and child weight status
There was a significant main effect of maternal pre-pregnancy BMI on all children’s weight status (P < 0.001), but no significant interaction between children’s case status and mothers’ pre-pregnancy BMI (P = 0.25). This finding indicates that the association between maternal pre-pregnancy BMI and child weight status was consistent across groups. After adjusting for case status, mothers who were overweight/obese prior to pregnancy were 2.38 times more likely to have an overweight/obese child at the time of the clinic visit as compared to mothers who were underweight/normal-weight pre-pregnancy (P < 0.001; Table 2). Of the mothers who were overweight/obese pre-pregnancy, 33% had an overweight/obese child while 16.8% of the mothers who were underweight/normal-weight pre-pregnancy had an overweight/obese child (chi-square = 82.3; P < 0.001). The main effect of maternal pre-pregnancy BMI on child weight status remained statistically significant in adjusted analyses. After controlling for all covariates, mothers with pre-pregnancy overweight/obesity were two times more likely to have an overweight/obese child when compared to mothers who were normal-weight pre-pregnancy (95% confidence interval (CI): 1.57–2.53; P < 0.001).
Association between maternal pre-pregnancy weight status and child weight status at ages 2–5, adjusted for covariates.
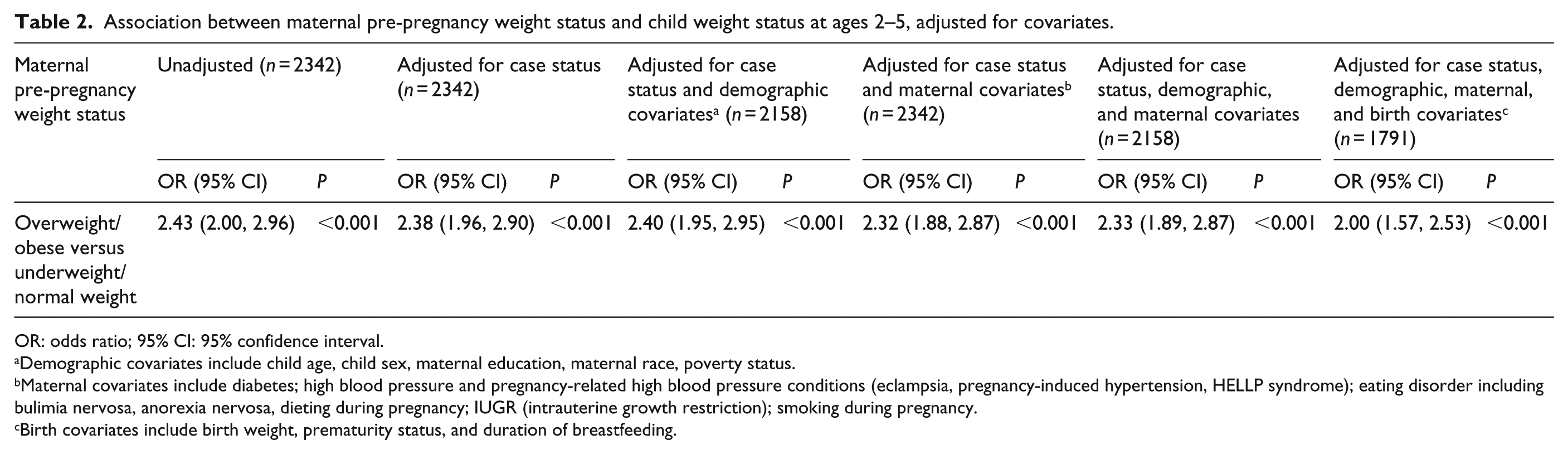
OR: odds ratio; 95% CI: 95% confidence interval.
Demographic covariates include child age, child sex, maternal education, maternal race, poverty status.
Maternal covariates include diabetes; high blood pressure and pregnancy-related high blood pressure conditions (eclampsia, pregnancy-induced hypertension, HELLP syndrome); eating disorder including bulimia nervosa, anorexia nervosa, dieting during pregnancy; IUGR (intrauterine growth restriction); smoking during pregnancy.
Birth covariates include birth weight, prematurity status, and duration of breastfeeding.
Maternal GWG and child weight status
When controlling for (1) case status and demographic covariates and (2) case status, demographic, and maternal covariates, mothers whose GWG fell below the IOM recommendations had (1) 34% (95% CI: 0.47–0.92) and (2) 31% (95% CI: 0.49–0.96) lower odds of having an overweight/obese child when compared to mothers who exceeded the recommendations, respectively. In addition, when controlling for case status, mothers who exceeded the GWG recommendations were 1.48 (95% CI: 1.17–1.87) times more likely to have an overweight/obese child as compared to mothers who met the weight gain recommendations (P = 0.001). This association remained statistically significant after adding demographic, maternal, and birth covariates (birth weight and breastfeeding) separately and simultaneously to the model (P = 0.033; Table 3). Sensitivity analyses showed a significant association between birth weight and adherence to GWG recommendations (P < 0.001). Infants whose mothers exceeded the recommendations had significantly higher birth weights (3302.2 ± 768.4 g) compared to infants whose mothers met (3203.5 ± 662.7 g) or gained less than the recommended amount of weight during pregnancy (2916.4 ± 824.3 g; P < 0.001). There also was a significant association between breastfeeding and adherence to GWG recommendations (P < 0.001). Infants whose mothers gained less than the recommended amount of weight during pregnancy were significantly less likely to have been breastfed (21.1%) than those whose mothers met (11.5%) or exceeded (12.2%) the GWG recommendations (P < 0.001).
Association between maternal gestational weight gain and child weight status at ages 2–5, adjusted for covariates.
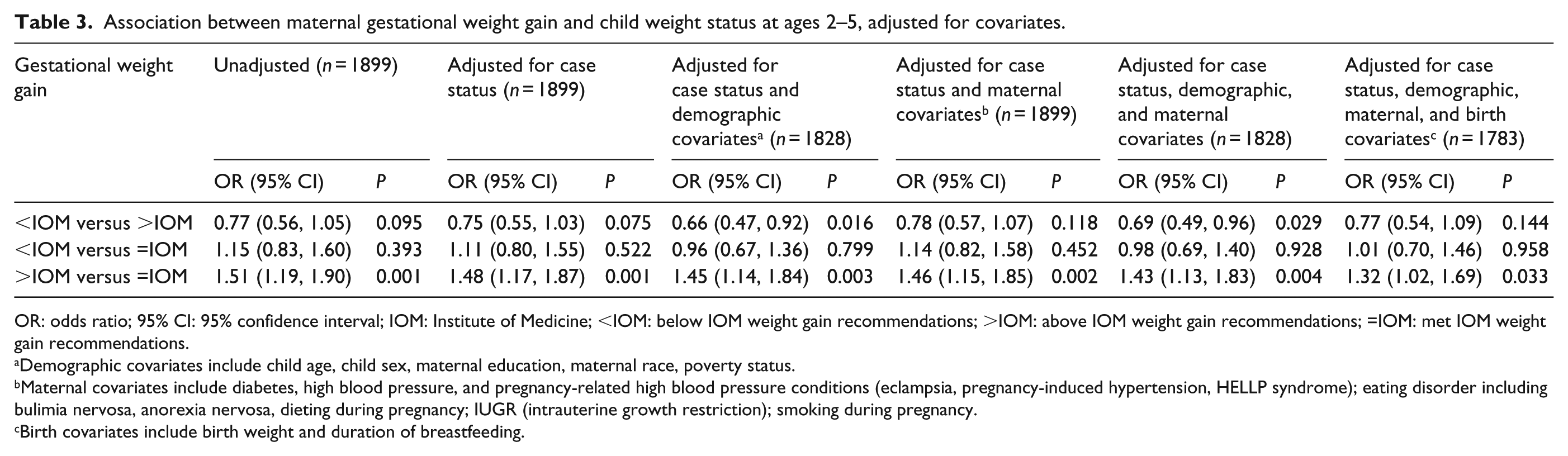
OR: odds ratio; 95% CI: 95% confidence interval; IOM: Institute of Medicine; <IOM: below IOM weight gain recommendations; >IOM: above IOM weight gain recommendations; =IOM: met IOM weight gain recommendations.
Demographic covariates include child age, child sex, maternal education, maternal race, poverty status.
Maternal covariates include diabetes, high blood pressure, and pregnancy-related high blood pressure conditions (eclampsia, pregnancy-induced hypertension, HELLP syndrome); eating disorder including bulimia nervosa, anorexia nervosa, dieting during pregnancy; IUGR (intrauterine growth restriction); smoking during pregnancy.
Birth covariates include birth weight and duration of breastfeeding.
Rapid weight gain during infancy and child weight status
Among children with ASD, those with rapid weight gain (i.e. change in weight-for-age z-scores from birth to 6 months >0.67 SD) showed a significantly higher frequency of overweight/obesity at ages 2–5 years compared to those without (37.6% vs 19.1%; P < 0.001). When adjusting the model for covariates, the association between rapid weight gain and childhood overweight/obesity among those with ASD remained significant (Table 4). Children with ASD and rapid weight gain during infancy had 3.47 times greater odds of being overweight/obese during early childhood than children with ASD who did not show rapid weight gain after controlling for all covariates (95% CI: 1.85–6.51; P < 0.001). The variable responsible for this increase in the odds ratio was the addition of birth covariates (infant birth weight) to the model, indicating that low birth weight infants were at greater risk for rapid weight gain.
Association between rapid weight gain during infancy and child weight status at ages 2–5 by group, adjusted for covariates.
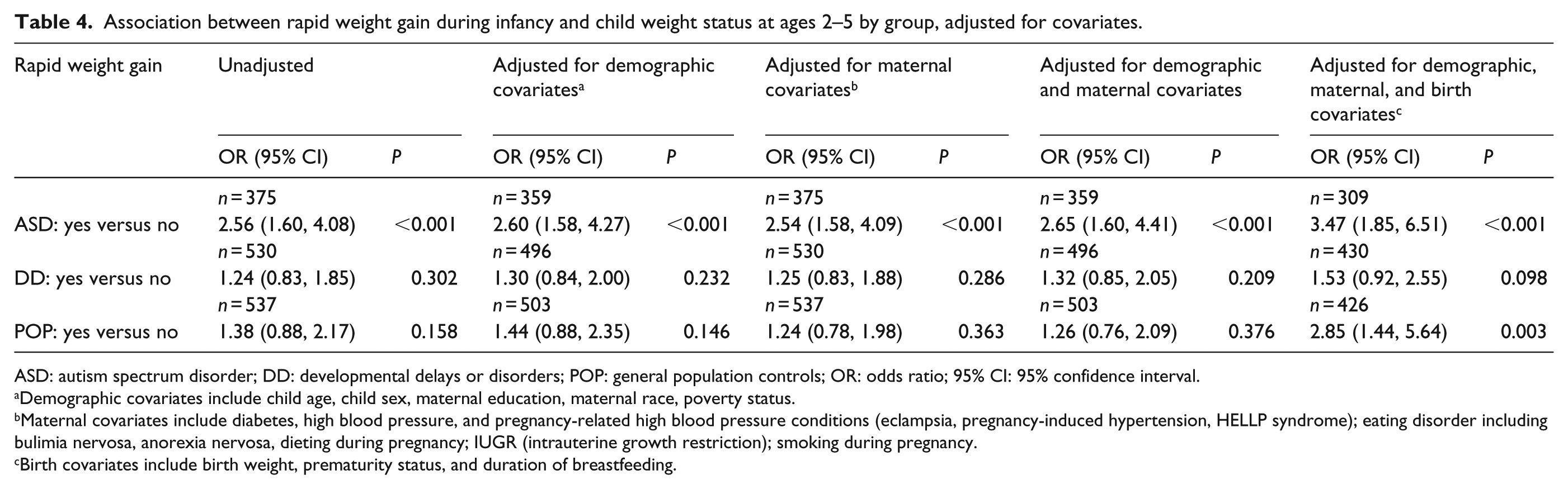
ASD: autism spectrum disorder; DD: developmental delays or disorders; POP: general population controls; OR: odds ratio; 95% CI: 95% confidence interval.
Demographic covariates include child age, child sex, maternal education, maternal race, poverty status.
Maternal covariates include diabetes, high blood pressure, and pregnancy-related high blood pressure conditions (eclampsia, pregnancy-induced hypertension, HELLP syndrome); eating disorder including bulimia nervosa, anorexia nervosa, dieting during pregnancy; IUGR (intrauterine growth restriction); smoking during pregnancy.
Birth covariates include birth weight, prematurity status, and duration of breastfeeding.
Discussion
The findings of this analysis are among the first to show that early life influences, including maternal pre-pregnancy overweight/obesity and excess GWG, are associated with increased odds for overweight/obesity during early childhood for children with ASD, children with non-ASD developmental disorders, and children from the general population alike. Children with ASD showed the highest frequency of rapid weight gain during the first 6 months of life, which may in part contribute to the higher obesity risk observed in this group during early childhood.
Our findings showed that mothers who were overweight/obese pre-pregnancy were more than twice as likely to have an overweight/obese child at ages 2–5 as compared to mothers who were underweight/normal weight. This association was consistent across groups as determined by examining a potential interaction between pre-pregnancy BMI and child case status and remained significant when controlling for covariates. This result corroborates findings from previous studies showing that maternal obesity during pregnancy was associated with an increased risk of obesity (Koupil and Toivanen, 2008; Mesman et al., 2009; Whitaker, 2004), coronary heart disease and stroke (Eriksson et al., 2014), insulin resistance (Catalano et al., 2009; Mingrone et al., 2008), and asthma (Reichman and Nepomnyaschy, 2008) in offspring. Putative mechanisms underlying this association include maternal obesity-mediated proinflammatory factors, in utero fetal programming, and genetic and shared environmental influences affecting offspring growth (Gaillard, 2015; Segovia et al., 2014). These findings emphasize the potential public health impact of maternal pre-pregnancy overweight/obesity on weight outcomes in children with or without developmental disabilities including children with ASD.
Pre-pregnancy maternal obesity has also been identified as a risk factor for GWG outside of the IOM recommendations (Deputy et al., 2015). Based on data from the 2010/2011 Pregnancy Risk Assessment Monitoring System, women with overweight and class 1 obesity (BMI 30.0–34.9 kg/m2) were almost three times as likely to exceed the weight gain recommendations compared with normal-weight women. A prospective cohort study of women who had a singleton live birth indicated that exceeding the IOM weight gain recommendations was associated with a 46% increase in odds of having an overweight/obese child at ages 2–5 years (Sridhar et al., 2014). Our data corroborated findings from earlier studies and showed that mothers who exceeded the weight gain recommendations during pregnancy were 1.48 times more likely to have an overweight/obese child compared to mothers who met the recommendations—a finding that was consistent across groups. The association between excess GWG and child overweight/obesity remained significant when controlling for infant birth weight and breastfeeding. A systematic review of 28 studies (Woo Baidal et al., 2016) showed that higher birth weight was consistently associated with higher weight status during childhood. Gaining less than the recommended amount of weight during pregnancy may be predictive of postnatal maternal behaviors such as breastfeeding; an association which needs to be examined in future studies.
Children with ASD showed the highest frequency of rapid weight gain and those with rapid weight gain were almost four times as likely to be overweight/obese during childhood when controlling for covariates. This finding corroborates results from a meta-analysis of 47,661 participants from 10 cohort studies showing that each one-unit increase in weight SD scores during the first year of life conferred a twofold higher obesity risk among typically developing children (Druet et al., 2012). Putative mechanisms underlying this association include metabolic programming, feeding practices, expression of a genetic predisposition to obesity, endocrine effects, and alterations of inflammatory/oxidative stress (Stettler et al., 2003; Stunkard et al., 1999; Young et al., 2012). The relationship between rapid weight gain during infancy and childhood overweight/obesity strengthened when birth weight was added to the model. The greater risk for rapid weight gain seen in newborns with low birth weights may in part be explained by catch-up growth elicited by low birth weight (Fabricius–Bjerre et al., 2011). Catch-up growth in low birth weight infants has been associated with an increased risk for later obesity, disturbances in glucose metabolism, insulin resistance, and cardiovascular disease (Jain and Singhal, 2012). These findings indicate that children with ASD, in particular, may be at greater risk for rapid weight gain during infancy, which places them at increased risk for overweight/obesity and related comorbidities later in life.
Other findings from this analysis that are noteworthy are the between-group differences in maternal medical conditions. Mothers in the ASD and DD groups, when compared to mothers in the POP group, showed higher rates of pre-pregnancy overweight/obesity, GWG, gestational diabetes, hypertension, smoking, and preterm deliveries and shorter durations of breastfeeding. Each of these medical conditions may carry independent risks for obesity development in the offspring. Therefore, future studies should delineate the relative contribution of each of those medical conditions on offspring obesity risk.
The large, geographically diverse sample and the thorough case classification based on in-person examinations are considered strengths of this study. The inclusion of two distinct groups of children with developmental disabilities (ASD and DD) is unique and enabled us to show that some early life risk factors (e.g. rapid weight gain) differ among children with different developmental disabilities. Limitations include a possible (1) recall bias of self-reported maternal data (e.g. height, pre-pregnancy weight), (2) underestimated IUGR prevalence, and (3) selection bias (DiGuiseppi et al., 2016) and limited representativeness of the sample (Schendel et al., 2012). A prior analysis of characteristics of responders and non-responders during recruitment revealed that several demographic characteristics, such as maternal age, education, and race/ethnicity, were associated with nonresponse but perinatal biologic factors, such as preterm delivery, were not (unpublished data). We controlled for several of these demographic factors in this analysis.
Conclusion
These findings provide evidence that maternal pre-pregnancy overweight/obesity and excess GWG are significant risk factors for overweight/obesity in children with ASD and non-ASD developmental disorders, similar to typically developing children. Our data further showed that children with ASD had the highest frequency of rapid weight gain during the first 6 months which may place them at increased risk for childhood obesity. Helping mothers achieve a healthy pre-pregnancy weight and adequate GWG and fostering healthy growth during infancy represent important targets for all children, but healthy growth patterns during infancy, in particular, may carry special importance for children with DD and with ASD or at increased risk for an ASD diagnosis, as in high-risk populations such as former premature infants, younger siblings of children with ASD, children with genetic disorders that predispose to ASD, and others (Boyle et al., 2011; Lai et al., 2014).
Supplemental Material
AUT791545_Lay_Abstract – Supplemental material for Early life influences on child weight outcomes in the Study to Explore Early Development
Supplemental material, AUT791545_Lay_Abstract for Early life influences on child weight outcomes in the Study to Explore Early Development by Tanja VE Kral, Jesse Chittams, Chyrise B Bradley, Julie L Daniels, Carolyn G DiGuiseppi, Susan L Johnson, Juhi Pandey, Jennifer A Pinto-Martin, Neloufar Rahai, AnnJosette Ramirez, Laura A Schieve, Aleda Thompson, Gayle Windham, Whitney York, Lisa Young and Susan E Levy in Autism
Footnotes
Acknowledgements
Dr Kral conceptualized and designed the study, interpreted study findings, and drafted the initial manuscript; Mr Chittams, Ms Thompson, and Ms York performed the data analysis, provided interpretation of the data, and reviewed and revised the manuscript; Dr Levy, Dr Pinto-Martin, Dr Daniels, Dr DiGuiseppi, Dr Johnson, Dr Pandey, Dr Schieve, Dr Windham and Mrs Bradley, Ms Rahai, Ms Ramirez, and Mrs Young interpreted the study findings and reviewed and revised the manuscript, and all authors approved the final manuscript as submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by Centers for Disease Control and Prevention (CDC) Cooperative Agreement Numbers U10DD000180 (Colorado Department of Public Health); U10DD000181 (Kaiser Foundation Research Institute (CA)); U10DD000182 (University of Pennsylvania); U10DD000183 (Johns Hopkins University); U10DD000184 (University of North Carolina at Chapel Hill); and U10DD000498 (Michigan State University).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.