
Abstract
Parent-mediated interventions are cost-effective ways to increase access to appropriate treatment services to children with autism spectrum disorder. We aimed to engage parents working as partners within rural autism identification teams to facilitate prompt initiation of autism-specific treatment services and expand the amount of treatment available to young children with autism spectrum disorder. To do this, we sought to employ a two-phase training approach: (Phase 1) train parents to fidelity in an evidence-based parent-mediated intervention (reciprocal imitation training), and (Phase 2) evaluate the extent to which parents could effectively coach other parents of newly diagnosed children to implement reciprocal imitation training with their child. We experienced several unexpected barriers to completing all aspects of the Phase 1 training workflow. This led us to pivot toward a process evaluation. We used qualitative interviewing with our partner parents to systematically identify barriers and enhance the likelihood for successful future efforts at such an approach. The lessons we learned and recommendations for others attempting this type of research are presented.
Keywords
Introduction
Despite well-established research support for the efficacy of autism spectrum disorder (ASD)-specific early intervention, children with ASD encounter significant difficulties accessing clinical care. This is magnified for families who live in rural and/or underserved areas. In large frontier states like Oregon, toddlers in rural areas with a recent diagnosis of ASD may only receive weekly or biweekly home visits for an hour, or at most a 2 h weekly toddler group through state-supported Early Intervention/Early Childhood Special Education programs.
There is a growing body of evidence showing the benefits of parent-mediated interventions, including studies that have demonstrated the fidelity of parents in implementing specific treatments (e.g. Oono et al., 2013). Parent-mediated interventions are cost-effective ways to increase access to appropriate treatment services to children with ASD. One early intervention that has been adapted to a parent-mediated approach is reciprocal imitation training (RIT). RIT is a naturalistic developmental behavioral intervention (NDBI, Schreibman et al., 2015) designed to teach young children with ASD to imitate spontaneously during on-going interactions with a play partner. A recent review cited RIT as one of only seven early intervention packages with “strong” evidence for efficacy with children <3 with or at risk for ASD (Zwaigenbaum et al., 2015). RIT can be implemented in a variety of play settings (e.g. inside, outside) as well as during daily routines (e.g. bath time). Because RIT focuses on pivotal skills that emerge early in development and does not require language competency, it can be used with children at very young chronological, language, and developmental levels. Research on RIT shows that it is effective for teaching object and gesture imitation skills (Ingersoll, 2010). In addition, RIT increases other social-communication skills such as social engagement, language, pretend play, and gesture use (Ingersoll, 2012). This approach can be very effective when implemented by parents with their own children (Ingersoll and Gergans, 2007).
The Autism Program at Oregon Health & Science University’s (OHSU) Doernbecher Children’s Hospital (DCH) provides a large portion of ASD diagnoses in Oregon, including children living in rural areas. In addition, DCH clinical staff have collaborated with the Oregon Center for Children and Youth with Special Health Needs at OHSU to provide training and on-going support to several community-based multidisciplinary autism identification teams (AITs). These teams are typically composed of a local pediatrician, a mental health provider, educational staff, and a Parent Partner (PP; parent of a child with ASD), who functions as a parent advocate. They conduct ASD diagnostic evaluations with children up to 5 years of age, many of whom reside in rural areas.
Our intention for the project was to leverage the PPs from local AITs as interventionists in order to facilitate prompt initiation of ASD-specific treatment services and expand the amount of treatment available to young children with ASD. A two-phase training approach, modeling the approach used to train professional direct service providers in RIT and related NDBIs (see Wainer et al., 2017), was planned: (Phase 1) train the PPs to fidelity in RIT and (Phase 2) evaluate the extent to which PPs could effectively coach parents of newly diagnosed children (NDP) to implement RIT with their child. However, during Phase 1 (see Table 1), we experienced several unexpected barriers to completing all aspects of the training workflow and eventually training procedures were terminated. As such, we shifted to a process evaluation approach and used qualitative interviewing to more systematically identify barriers and enhance the likelihood for successful future efforts at such an approach. The purpose of this short report is to describe findings from the process evaluation.
Phase 1 project workflow for Parent Partners.
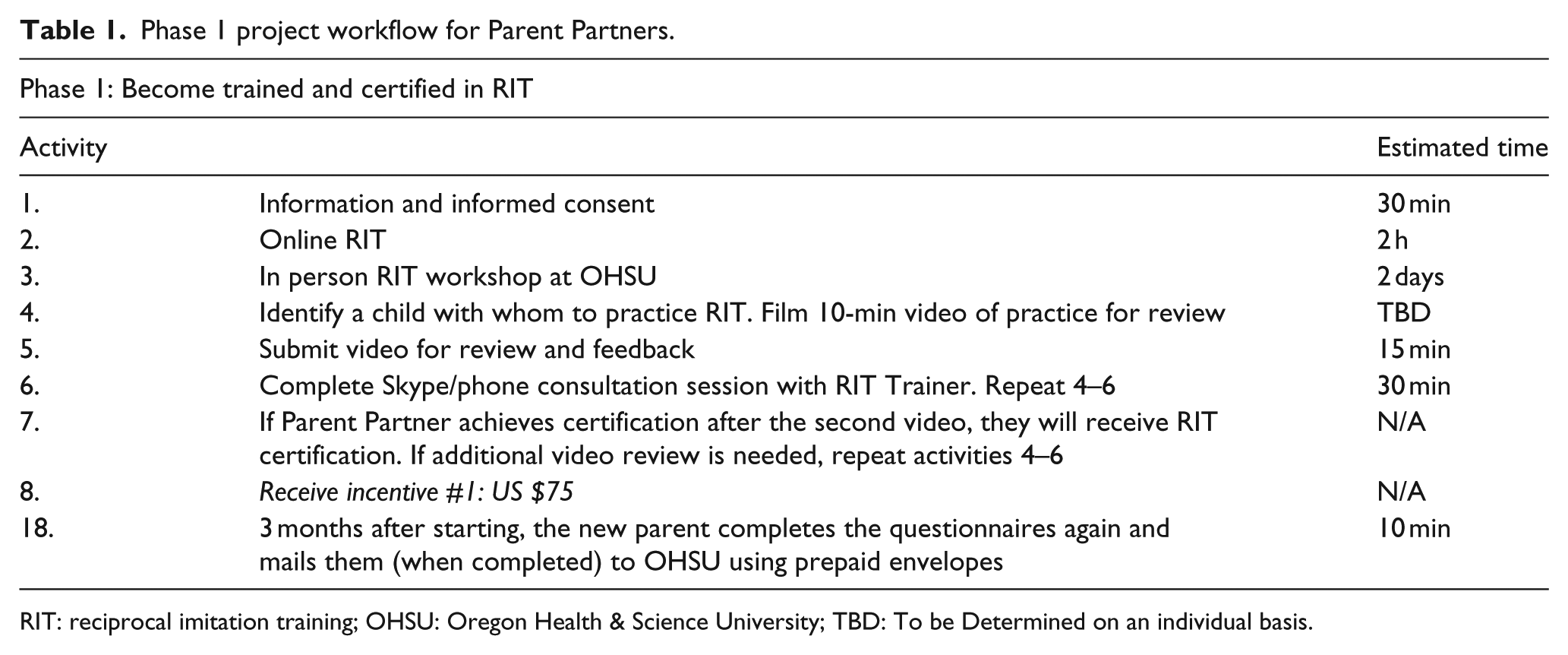
RIT: reciprocal imitation training; OHSU: Oregon Health & Science University; TBD: To be Determined on an individual basis.
Method
This study was carried out under an Institutional Review Board approved protocol. PPs underwent an informed consent procedure prior to beginning the study.
Initial training experience
While all eight parents PPs on the local AITs were contacted about participation, four eventually agreed to participate. Initially, only two PPs consented to participate, reviewed the Online RIT materials, and traveled to OHSU to attend the 2 day face-to-face workshop. The other six PPs could not attend this workshop due to the long distance to training center and the need to take time away from work and family. As such, we added a second 1-day remote RIT workshop, which resulted in two additional PP participants.
After completing the workshop, all four PPs searched for a family with a young child with ASD with whom to practice RIT, in order to establish fidelity and become certified. One PP discontinued participation due to personal life events that happened shortly after the initial workshop. The other PPs encountered a myriad of logistical challenges that stalled the study at this stage.
Given the many difficulties recruiting and supporting the PPs in completion of the project activities, we pivoted our study design to conduct qualitative interviews with the four of the PPs to identify barriers to participation and perspectives on what worked and what did not to help determine the feasibility of similarly structured projects in the future.
Data collection and analysis
An interview guide was developed to examine participants’ experience with the training model. Questions for the interview were generated based on the study goals and discussions with the participants throughout the training procedures (see Appendix 1). Questions were intentionally open-ended, and participants were asked to use their own words when providing their responses. All answers were recorded and transcribed for analysis.
Data analysis was guided by thematic content analysis (Burnard, 1991). First, transcripts were read through and notes made throughout the reading, on general ideas emerging from the interview. Then, notes were reviewed and names of categories to describe the different ideas were generated. The research team then reviewed the notes and categories and collapsed similar ideas into overarching themes. Original transcripts were re-read to ensure that no additional themes were missed during initial review and coding.
Results
Overarching themes across participants are summarized in Table 2.
Themes from interview.
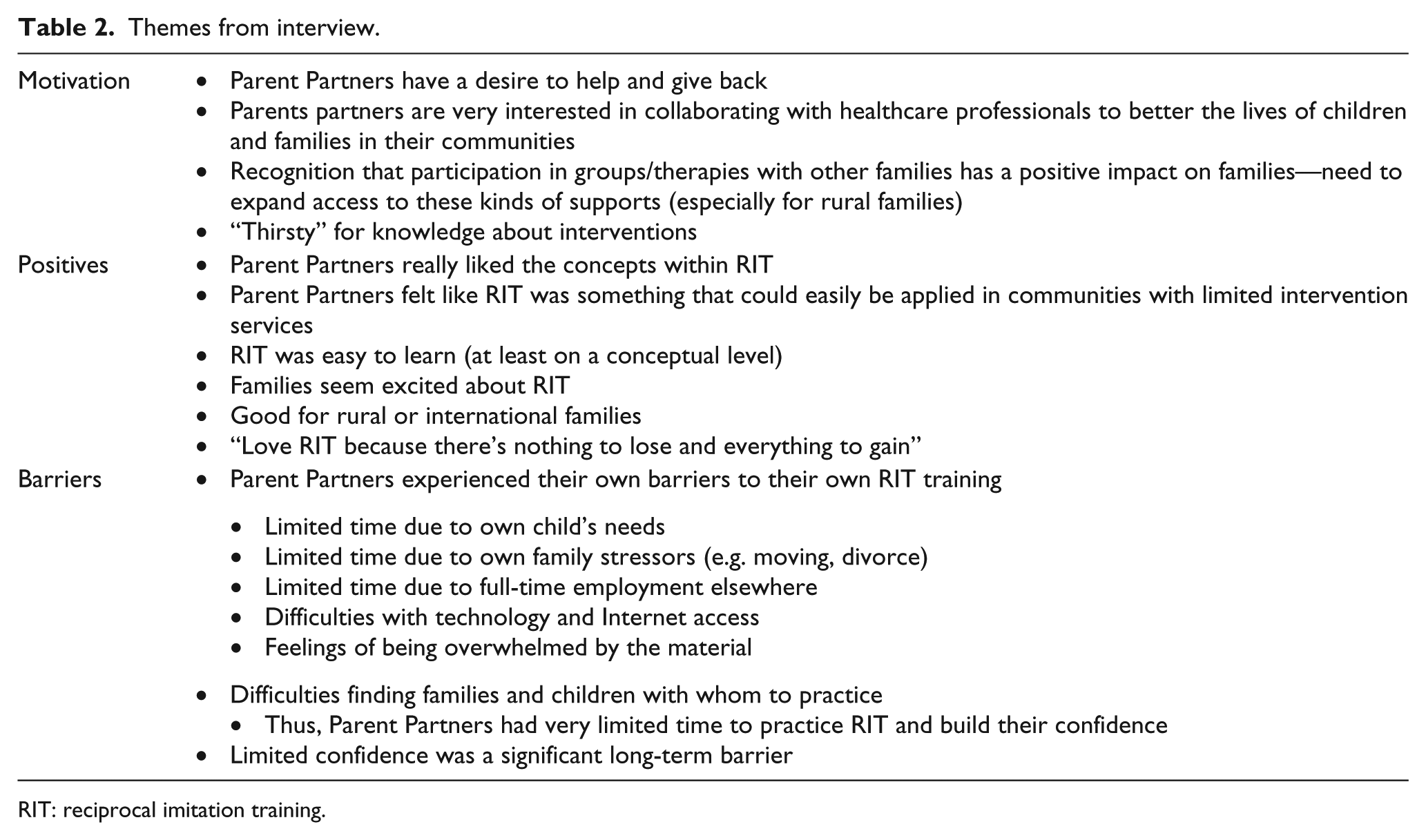
RIT: reciprocal imitation training.
Motivation for participation
In general, PPs were motivated to support other families in learning effective early intervention practices. They indicated a desire to collaborate with healthcare professionals to give back to their communities and to help other families. They felt that being able to connect with other families is critical for NDPs, and that such opportunities are very limited, particularly for families in rural and underserved areas. The PPs recognized their unique potential in being able to serve as this critical family connection for NDPs. Finally, PPs indicated a “thirst” for knowledge about interventions that could be helpful for other parents as well as for themselves.
One of the things I’ve noticed is the differences in the families once they start the group they play, interact, socialize as family that type of support helps them. So I wanted to look into more ways to do that on a broader scale how to work one on one or with kids in general on the spectrum.
Buy-in with the intervention
The PPs spoke about RIT in an encouraging way. They were positive about the goals of RIT and the techniques and concepts that are taught as part of the program. Indeed, it was noted that the concepts in RIT seemed easy to learn (at least on a conceptual level). PPs felt as though RIT was ideal for rural, international, or underserved families as it could be easily implemented with limited resources and time. When PPs spoke to other parents about RIT, the other parents expressed enthusiasm about the approach.
Love RIT because there’s nothing to lose and everything to gain.
RIT [is] a particularly interesting technique, especially in a rural community.
RIT is a resource that doesn’t cost anything, is easy to facilitate, and easy to provide in rural areas where we need things like that.
Barriers
Despite strong motivation to participate and enthusiasm about RIT, the PPs reported on several barriers which made it challenging to complete the training procedures. From a logistical standpoint, PPs reported that difficulties finding children with whom they could practice was a consistent and significant barrier. Because of this, PPs felt as though they never reached a sufficient level of confidence in using RIT and commented that a lack of confidence in the intervention would serve as a profound long-term individual barrier to using RIT in their roles as PPs. Another frequently cited individual barrier was related to time; PPs reported limited time to commit to training due to their own child’s significant needs, unexpected family stressors (e.g. divorce, moving), and full-time employment outside of the PP role. There were no notable differences observed in terms of barriers among the PPs. However, the PP who completed the RIT workshop in-vivo cited that the in-person practice was the most helpful part of the workshop; moreover, that same PP reported slightly higher confidence about the intervention than the PP who completed the workshop remotely. Although PPs were excited about RIT, they recognized a need for practice and supervision in order to feel comfortable with the intervention. Importantly, supervision was offered as part of the training model. Although parents did not explicitly mention difficulties seeking supervision, only one parent successfully scheduled and completed supervision, suggesting some structural communication challenges may have served as another potential barrier.
Learning the techniques was easy, actually doing them was totally different!
There was not a lot of confidence not because of lack of training, but just self-confidence. That was the hardest thing in initiating things not feeling too confident in my own ability to actually perform RIT.
I work full time and have a large family.
Discussion
Results from this work lend support to the notion that intent and engagement are necessary, but not sufficient, conditions for adoption of evidence-based interventions in real world settings (Damschroder et al., 2009). This project has inspired careful consideration of two critical questions:
What is the most appropriate role for PPs in early intervention for ASD?
Initial enthusiasm suggested that PPs were excited about the role of parent coach; however, this role may not be best for utilizing the invaluable experience, expertise and perspectives of PPs. It may behoove the field to considered alternative ways to include PPs in parent coaching interventions, such as a parent navigator supporting direct service providers responsible for parent coaching, as a “practice partner” for a parent while she or he learns the specific intervention strategies, or as a parent to parent mentor trained to provide emotional support, practical parenting information and information about accessing services and supports (e.g. Singer et al., 1999). Although an answer to this inquiry is not immediately clear, it remains an important empirical question that can, and should, be investigated in future mixed-method research studies. In the meantime, experiences from the current project suggest that at a very minimum, exploration of ways to enhance the training and capacity of PP as parent coaches is warranted and led to our second question:
2. How can we improve training and system to increases the likelihood of PPs success in the role of parent coach?
Candidly, we modified a procedure typically used to train professionals in NDBIs, but this approach was not feasible or effective for PPs. We did not fully appreciate that these PPs are not typical professionals, do not have protected professional time, and have highly stressful lives outside of their PP role. Indeed, the training model we used was met with structural (e.g. communication challenges), logistic/resource (e.g. difficulties finding practice families), and individual (e.g. limited PP confidence, high levels of PP personal life stress) barriers. PPs may need more background knowledge, intensive training, on-going supervision, financial compensation, organizational/administrative support, time, and peer support than was provided in the current model in order to deliver parent coaching in early interventions for ASD. Specifically, our data suggest that increased stipends for participation, more frequent supervision during training, greater peer support (e.g. training multiple PPs in a given area as parent coaches), and identifying and assigning practice families in advance would each be beneficial in supporting a more successful RIT and parent coaching training endeavor.
Recently, we have become aware of a program in which PPs can be trained and certified as community health workers and peer support specialists. Completion of training and certification would empower our PPs and allow them to bill health plans for their services in providing RIT. This may prove to be a necessary step that will enable at least some of the PPs to complete RIT training and actively participate in teaching this parent-mediated intervention to other families.
Supplemental Material
AUT815643_Lay_Abstract – Supplemental material for Parents training parents: Lessons learned from a study of reciprocal imitation training in young children with autism spectrum disorder
Supplemental material, AUT815643_Lay_Abstract for Parents training parents: Lessons learned from a study of reciprocal imitation training in young children with autism spectrum disorder by Trevor A Hall, Sarah Mastel, Robert Nickel and Allison Wainer in Autism
Footnotes
Appendix 1
In this first part of our interview, my questions are going to be about the factors involved in your decision to participate.
In this next portion of the interview, my questions are going to center on the online RIT training, and how easy and/or hard it was to access the RIT website and learn from it.
In this next part of our interview, my questions are going to center on the RIT Workshop.
Additional questions are as follows:
Acknowledgements
The authors thank the OHSU Autism Clinical Program and the Oregon Center for Children and Youth with Special Health Needs for their support of this research. The authors also acknowledge the families who participated.
Declaration of conflicting interests
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Funding
Research reported in this publication was supported by the Friends of Doernbecher Foundation. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Friends of Doernbecher Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.