
Abstract
There is growing interest in the development of behavioral parent interventions targeting emotional and behavioral problems in children with autism spectrum disorders. Such interventions have potential to improve a number of child and parental well-being outcomes beyond disruptive child behavior. This systematic review and meta-analysis assesses evidence for the efficacy of behavioral parent interventions for disruptive and hyperactive child behavior in autism spectrum disorders, as well as parenting efficacy and stress. A total of 11 articles from nine randomized controlled trials were included. Sufficient data were available to calculate standardized mean difference and show favorable effects of behavioral parent interventions on parent-reported measures of child disruptive behavior (standardized mean difference = 0.67), hyperactivity (standardized mean difference = 0.31) and parent stress (standardized mean difference = 0.37); effects on parent efficacy are less clear (standardized mean difference = 0.39, p = 0.17). There were insufficient data to explore intervention effects on internalizing behavior in autism spectrum disorders, parenting behaviors, or observational and teacher-reported outcomes, providing important avenues for future research. This review adds to growing evidence of the efficacy of behavioral parent interventions for child behavior and parental well-being in autism spectrum disorders (Prospero: CRD42016033979).
Keywords
Autism spectrum disorders (ASD) are characterized by impaired social and communication skills, the presence of restrictive and repetitive interests and behaviors and sensory anomalies (American Psychiatric Association, 2013). Recent estimates from the Centers for Disease Control and Prevention (CDC) suggest that ASD may affect one in 59 children (Baio et al., 2018). Emotional and behavioral problems (EBPs) are also common in ASD and can manifest in the form of non-compliance, aggression, anxiety, and hyperactivity (Kanne & Mazurek, 2011; Simonoff et al., 2008; White, Oswald, Ollendick, & Scahill, 2009). In a population-derived sample of children with ASD, as many as 70% of children met diagnostic criteria for another psychiatric condition; social anxiety, attention deficit hyperactivity disorder (ADHD), and oppositional defiant disorder (ODD) were the most common diagnoses, with rates of approximately 28%–29% (Simonoff et al., 2008). The development and testing of targeted psychological intervention addressing comorbidities and associated impairment is warranted for the ASD population. This is especially true given the poor long-term outcomes associated with ASD and high levels of intellectual disability likely to add to the complex presentation and management of problematic behavior (Howlin et al., 2017; La Malfa et al., 2004).
In addition to impact on the individual with ASD, EBPs can also place increased demands on parents. Consequently, parents may struggle to know how best to respond to their child and report permissive management strategies (O’Nions, Happe, Evers, Boonen, & Noens, 2018). Low levels of parental limit-setting are related to later problem behavior in children with ASD and mediate the relationship between parenting stress and later child behavior problems (Osborne, McHugh, Saunders, & Reed, 2008). Parents also report low levels of parenting efficacy (belief in their ability to be a successful parent) (Rodrigue, Morgan, & Geffken, 1990) and higher levels of parenting stress compared with parents of typically developing (TD) children and children with other disabilities such as cerebral palsy (Hayes & Watson, 2013). EBPs in children with ASD are particularly associated with parenting stress (Lecavalier, Leone, & Wiltz, 2006; Salomone et al., 2018). The direction of association between parental well-being and child behavior problems is unclear; some report a bidirectional relationship (Lecavalier et al., 2006; Yorke et al., 2018), while Zaidman-Zait et al. (2014) found parent-driven effects of parent stress on later internalizing and externalizing behavior in children with ASD. While the relationship between child behavior and parental well-being is likely to be complex and bidirectional, it highlights the importance of ensuring that interventions for EBPs in ASD are also associated with improved parent outcomes and well-being to ensure the best long-term and family wide benefit (Tarver, Daley, & Sayal, 2015).
Behavioral parent interventions (BPIs) are well-established and effective interventions for the treatment of behavioral problems in neurotypical populations and other clinical groups (Barlow, Bergman, Kornor, Wei, & Bennett, 2016; Fabiano et al., 2009). Psychosocial intervention is recommended as a first-line treatment for problematic behavior in ASD (National Institute for Health and Care Excellence, 2013), but the potential heterogeneity and complex mechanisms underlying EBPs in ASD make it likely that traditional BPIs will require modification for this clinical group. It is acknowledged that some common features of BPIs, such as time out, may not be appropriate for children with ASD who may find social withdrawal rewarding (Dababnah & Parish, 2016). Similarly, the triggers for behavior problems may be quite different. For example, in children with ASD, anxiety may underlie externalizing behavior that is being used as strategy to avoid anxiety-provoking stimuli (Storch et al., 2012).
Consequently, there is growing interest in the development of BPIs for the treatment of disruptive behavior in ASD. A recent meta-analysis reviewed current evidence of BPIs for disruptive behavior in children with ASD (Postorino et al., 2017). The review reports a moderate benefit of BPIs on parent-reported child disruptive behavior, with an effect size (standardized mean difference (SMD)) of 0.59; the authors concluded parenting interventions for ASD are efficacious and recommended they should be more widely disseminated. However, in non-ASD populations, there is evidence for the efficacy of BPIs for outcomes beyond disruptive behavior including ADHD symptoms (Daley et al., 2014; Dretzke et al., 2009; Fabiano et al., 2009) and improved child internalizing behavior (Herman, Borden, Reinke, & Webster-Stratton, 2011; van den Hoofdakker et al., 2007). Furthermore, receipt of BPI has therapeutic effects for parents and improves parenting behavior and parenting efficacy and reduces parenting stress (Colalillo & Johnston, 2016; Daley et al., 2014; Leijten et al., 2018).
Given the additional benefits of BPIs on other child variables and parent outcomes in other neurodevelopmental conditions (e.g. Daley et al., 2014), this review set about to extend the findings of Postorino et al. (2017) and explore the additional benefits of BPIs developed for children with ASD. Because both anxiety and ADHD are common in children with ASD, and may underlie disruptive behavior, it is important to assess the effects of intervention on these domains of EBPs. Furthermore, parental functioning and well-being outcomes are important as they are also commonly impaired in families with a child with ASD (Estes et al., 2013) and could also be related to long-term child well-being outcomes (Yorke et al., 2018). While some other recent reviews have also explored the effects of BPIs on parental well-being in ASD, they have focused on interventions that aim to improve parental mental health or have included interventions aimed at improving social communication deficits in ASD (Da Paz & Wallander, 2017; Hemdi & Daley, 2017). This is the first review to focus on the additional benefits of BPIs on parental well-being (from randomized controlled trials (RCTs) only), where the main aim of the intervention is reduction of EBPs in ASD.
This article therefore aims to review potential additional benefits or secondary outcomes of BPIs in ASD on factors not specifically targeted by the intervention. Furthermore, the review will explore whether there is available evidence for the effects of intervention on measures of child behavior from other informants (e.g. observations, teacher report) rather than only parent report. While parent perception of child behavior has obvious clinical relevance, parental involvement and investment in BPIs means parent report following intervention may be prone to bias. In the ADHD literature, effect sizes of parenting interventions for core ADHD symptoms (but not oppositional behavior) become non-significant when considering outcomes from observers who are “probably blind” to treatment allocation, as opposed to parent report (Sonuga-Barke et al., 2013). Parent-reported outcome assessments may therefore need to be supplemented with assessments from other informants to improve confidence in trial findings. Where sufficient data are available, the review will report a meta-analysis of treatment effects on included outcomes.
Method
The protocol for this review is registered on the Prospero database (registration number CRD42016033979).
Search strategy
Records were identified through electronic searches of PubMed, PsychInfo, and Embase using the following search terms: ASD, Asperger disorder, autism or pervasive developmental disorder with parent training, parent trial or parent intervention and emotion, problem, behav*, anxi*, depress*, or social anxiety*. Searches were completed on 21 December 2017. No publication date or language filters were applied. Electronic searches were supplemented with the hand search of relevant review articles and reference lists of eligible articles.
Eligibility criteria
Studies were assessed according to the following inclusion criteria: (1) RCTs published in peer-reviewed journals; (2) at least one treatment arm assessing the effects of a BPI where the main aim of the intervention is the reduction of behavioral or emotional problems in children or young people with ASD. This includes trials assessing the effects of intervention compared with a no-treatment control (e.g. waitlist control (WLC)) or an active control group (e.g. parent support and counseling). Medication trials that contained a treatment arm assessing unimodal BPI were included (e.g. BPI + placebo), but only placebo arms were eligible for analysis in the review. Trials were included if usual treatment included medication; (3) children aged between 2 and 18 years; (4) diagnosis of ASD (reported existing clinical diagnosis or research confirmed diagnosis). The inclusion of trials reporting clinical diagnoses of ASD rather than research confirmed diagnoses was justified given that children with clinical diagnoses are those who will be offered intervention in clinical practice; (5) outcome measures included a validated measure of disruptive child behavior, ADHD symptoms/hyperactivity or emotional problems in children with ASD (see outcome measures below).
Studies were excluded using the following criteria: (1) while the secondary impact of BPIs on parental well-being are investigated in this review (see below), interventions directly addressing parental well-being (e.g. mindfulness-based interventions) are beyond the scope of this current review and were consequently excluded; (2) trials investigating multimodal psychosocial intervention including a BPI component (e.g. CBT + BPI) or the adjunctive benefit of BPI to pharmacological intervention (BPI + medication vs medication alone) were excluded. Given the large effect sizes associated with medication, this would allow us to better explore the effects of unimodal BPI; (3) case studies or studies with a small sample size (N < 10) were also excluded from the review.
Trial selection
Two reviewers (J.T. and S.W.) independently screened records and selected studies for study inclusion; discrepancies were resolved by consensus.
Risk of bias
Risk of bias for each study was assessed using the Cochrane risk of bias tool (Higgins & Green, 2011). Assessed domains included random sequence generation and allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), and selective reporting (reporting bias). Since blinding parents to intervention status is impossible in trials of BPI, studies were assessed as low risk of performance bias if they included a blinded measure of child behavior within its outcome measures. Risk of bias was assessed independently by two post-doctoral researchers (J.T. and M.P.) with discrepancies resolved by consensus including a third researcher (S.W.).
Outcome measures
For child outcomes, the focus of this review was three main child variables. Disruptive/non-compliant behavior, including symptoms of ODD or conduct disorder (CD) (e.g. tantrums, aggressive behavior, and refusal to follow rules). This included measures such as the irritability subscale of the Aberrant Behavior Checklist (ABC-I; Aman, Singh, Stewart, & Field, 1985) and the Eyberg Child Behavior Inventory (ECBI; Eyberg & Ross, 1978). Symptoms of ADHD (hyperactivity/impulsivity and inattention) assessed by measures including the hyperactivity scale of the ABC or the Swanson, Nolan, and Pelham (SNAP-HA) rating scale (Swanson et al., 2001) and the hyperactivity subscale of the Behavior Assessment System for Children (BASC; Reynolds, 2004). Child emotional problems included measures of depression (e.g. low mood, loss of interest in pleasurable activities/self-care), anxiety (phobias, concerns) from scales including the depression subscale of the BASC (Reynolds, 2004). It was anticipated that the majority of eligible studies would use parent-reported outcomes as their primary outcome and were subsequently the focus of the analysis. However, outcomes from other informants (e.g. observations/teacher report) were also included in the review. Observations of behavior included the Family Observation Schedule (FOS; Sanders, Waugh, Tully, & Hynes, 1996) and the Dyadic Parent–Child Interaction Coding System (DPICS; Bessmer, 1998).
Next, the review focused on parental behavior and well-being. This included parenting stress (measures concerned with parental strain and tension), for example, Parent Stress Index (PSI; Abidin, 1990). An analysis of parental efficacy including measures pertaining to parental confidence (e.g. the parental sense of competency scale (PSOC)/the being a parent scale; Johnston & Mash, 1989) or the Parenting Tasks Checklist (PTC; Sanders & Wooley, 2001) was also conducted. Finally, the review analyzed measures of parent techniques used in response to their child with ASD, for example, the Parenting Scale (PS; Arnold, O’Leary, Wolff, & Acker, 1993).
Data extraction and management
Mean change (difference between pre- and post-intervention mean) was calculated for all included outcomes. For clarity, some change scores (e.g. disruptive behavior) were reversed so that positive effect sizes were always associated with positive clinical outcome. Data were extracted by J.T. and independently checked by M.P. Outcomes were entered into a meta-analysis given they had been assessed via a psychometrically validated outcome in at least three included trials (see supplementary material for additional information about data extraction and management).
Analysis strategy
SMD were calculated using mean change and pre-intervention SD (Morris, 2008). Analyses were conducted using RevMan v.5.3. Given anticipated heterogeneity between trials and outcomes, a random effects model was used to assess SMD. The I2 statistic in RevMan was used to analyze heterogeneity among trials. However, the p value for assessment of heterogeneity was set at 0.1 since I2 is not good at assessing heterogeneity in analyses with few included trials (Higgins & Green, 2011). Analyses of publication bias require substantially more than 10 studies (Sterne et al., 2011); therefore, publication bias was not analyzed in this review.
Results
Searches returned 2121 articles, 2014 after removal of duplicates which were screened using title and abstract. A total of 79 articles were subject to a full-text assessment for eligibility, of which 11 articles (from nine RCTs) 1 met criteria for inclusion in the review (Figure 1). A further article was assessed following the search of reference lists of included articles but was not eligible for inclusion (see Table 1 for included study characteristics and Table 2 for intervention characteristics).
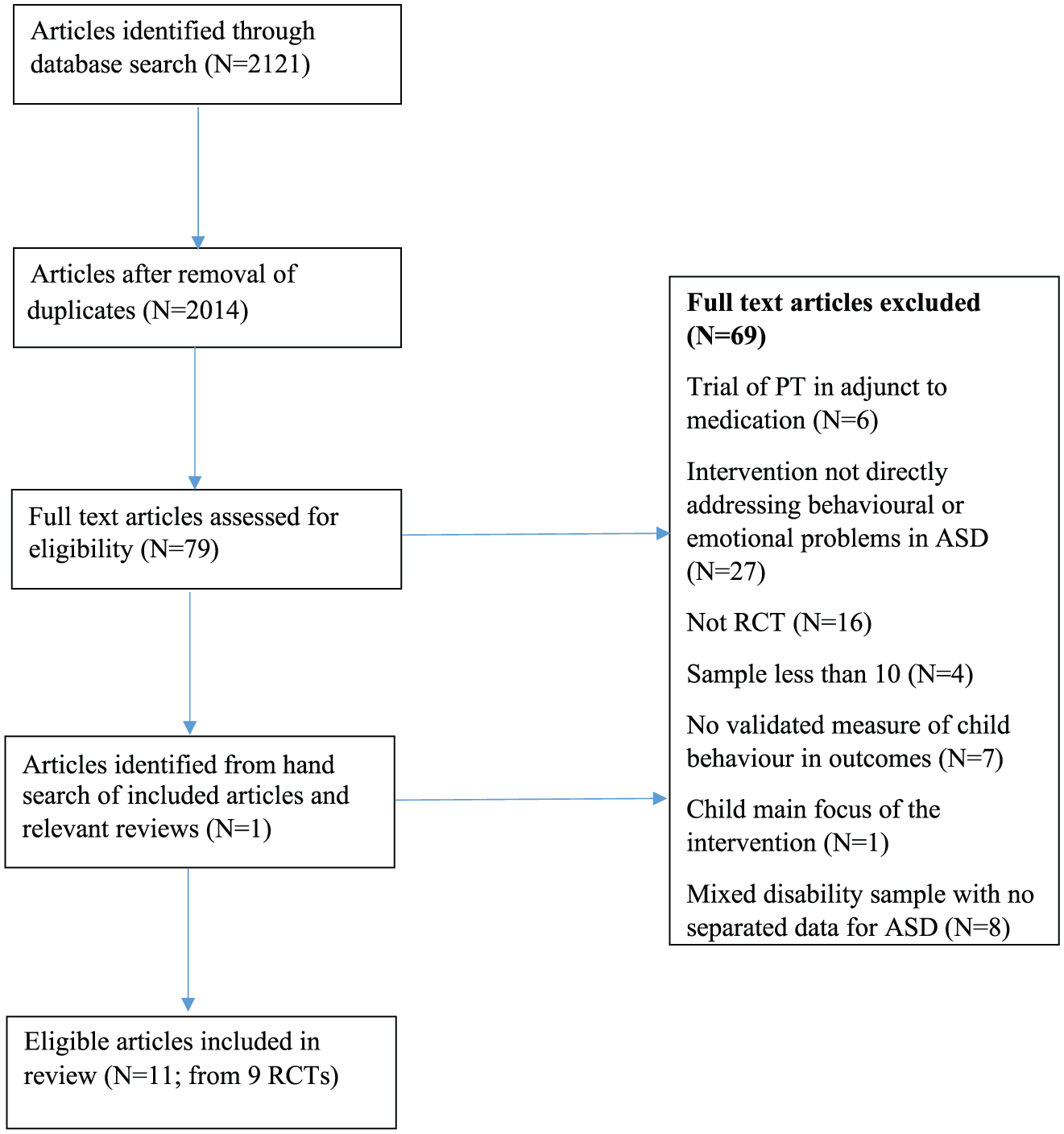
Flowchart of articles through the review.
Characteristics of included studies.
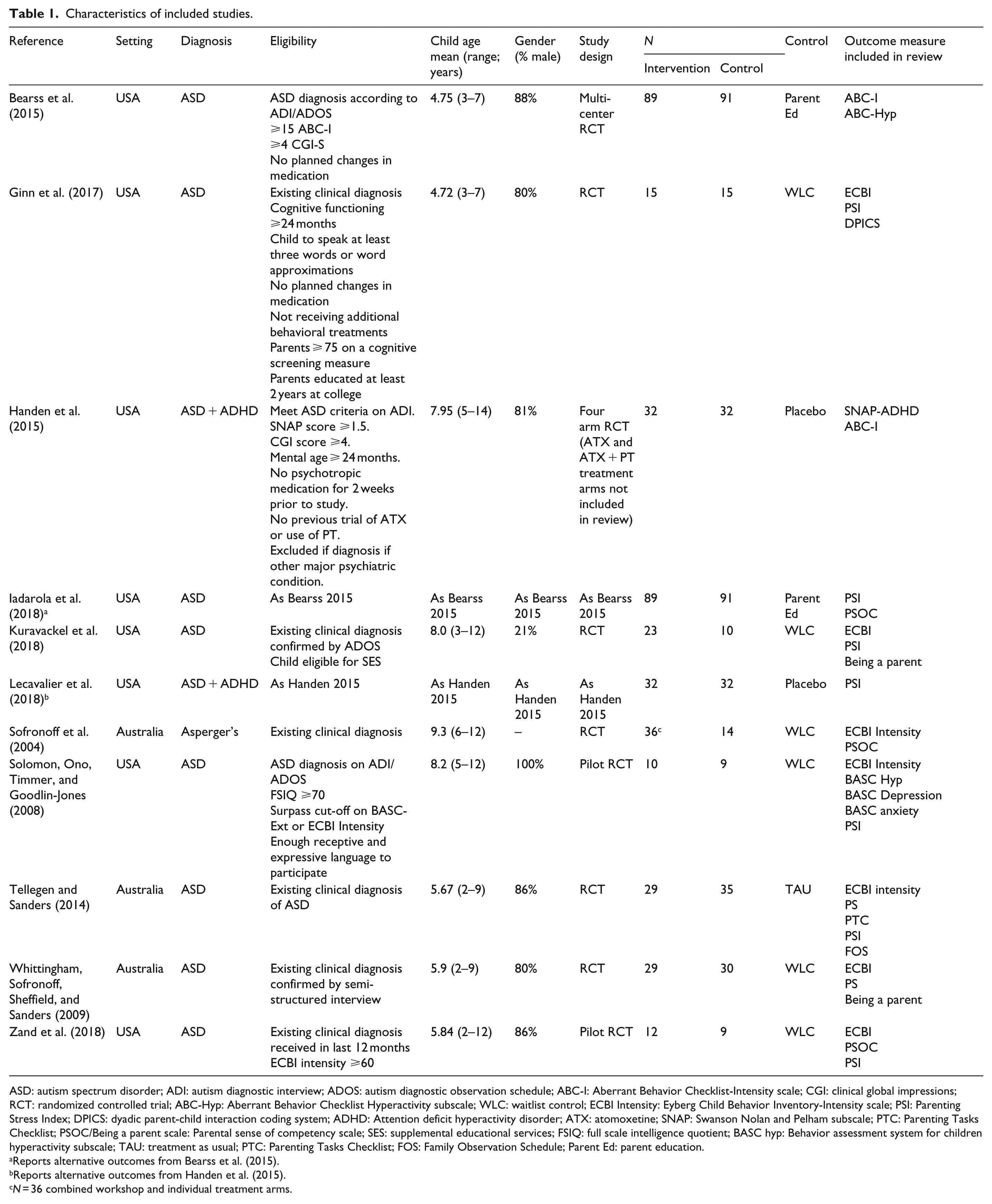
ASD: autism spectrum disorder; ADI: autism diagnostic interview; ADOS: autism diagnostic observation schedule; ABC-I: Aberrant Behavior Checklist-Intensity scale; CGI: clinical global impressions; RCT: randomized controlled trial; ABC-Hyp: Aberrant Behavior Checklist Hyperactivity subscale; WLC: waitlist control; ECBI Intensity: Eyberg Child Behavior Inventory-Intensity scale; PSI: Parenting Stress Index; DPICS: dyadic parent-child interaction coding system; ADHD: Attention deficit hyperactivity disorder; ATX: atomoxetine; SNAP: Swanson Nolan and Pelham subscale; PTC: Parenting Tasks Checklist; PSOC/Being a parent scale: Parental sense of competency scale; SES: supplemental educational services; FSIQ: full scale intelligence quotient; BASC hyp: Behavior assessment system for children hyperactivity subscale; TAU: treatment as usual; PTC: Parenting Tasks Checklist; FOS: Family Observation Schedule; Parent Ed: parent education.
Reports alternative outcomes from Bearss et al. (2015).
Reports alternative outcomes from Handen et al. (2015).
N = 36 combined workshop and individual treatment arms.
Intervention characteristics of included studies.
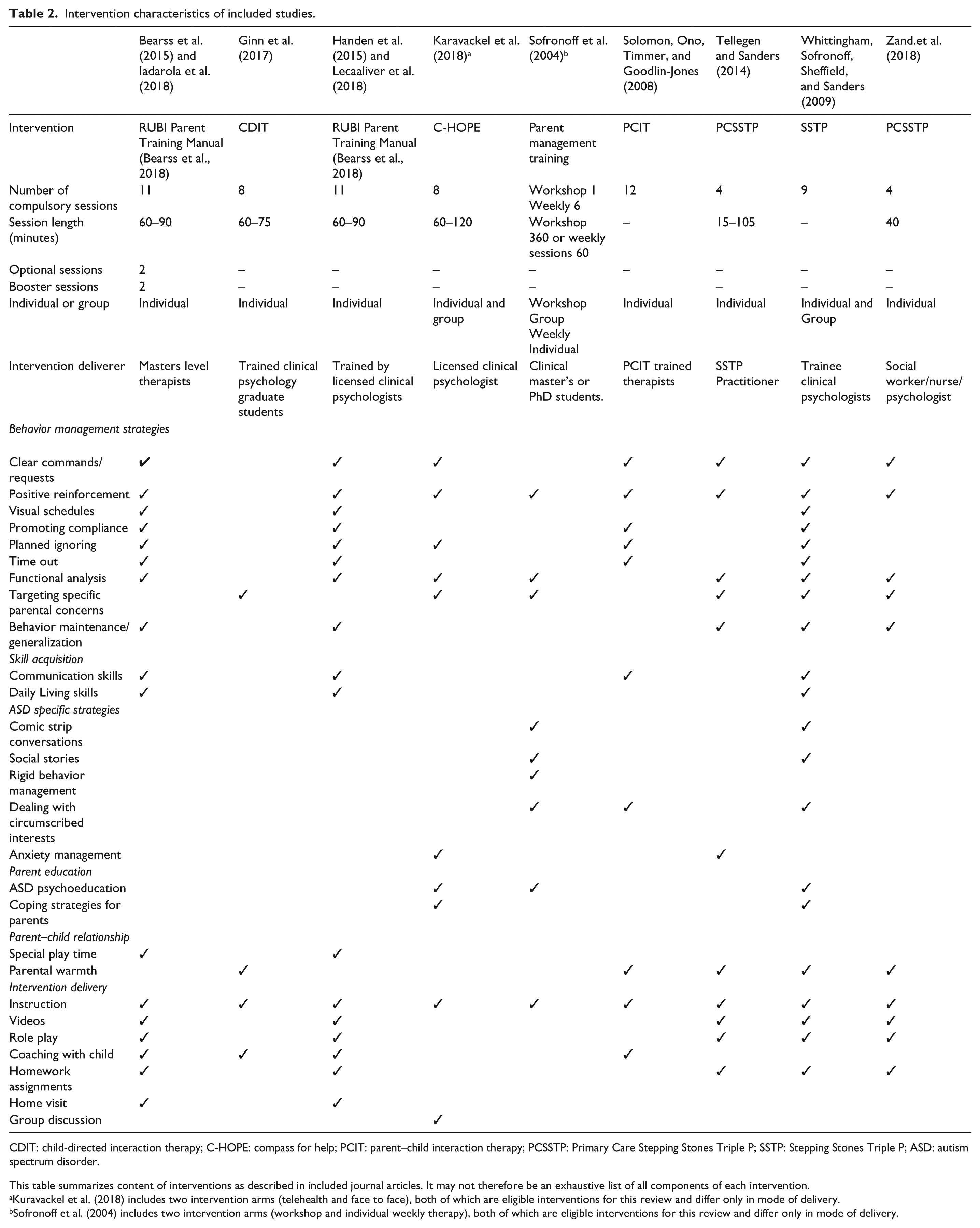
CDIT: child-directed interaction therapy; C-HOPE: compass for help; PCIT: parent–child interaction therapy; PCSSTP: Primary Care Stepping Stones Triple P; SSTP: Stepping Stones Triple P; ASD: autism spectrum disorder.
This table summarizes content of interventions as described in included journal articles. It may not therefore be an exhaustive list of all components of each intervention.
Kuravackel et al. (2018) includes two intervention arms (telehealth and face to face), both of which are eligible interventions for this review and differ only in mode of delivery.
Sofronoff et al. (2004) includes two intervention arms (workshop and individual weekly therapy), both of which are eligible interventions for this review and differ only in mode of delivery.
Parent-reported disruptive behavior
Nine articles included an analysis of parent reported child disruptive behavior and were entered into a meta-analysis involving 521 participants (Figure 2). There was a moderate effect of BPI on child disruptive behavior (SMD = 0.67, 95% confidence intervals (CI) = 0.49–0.85, Z = 7.31, p < 0.01). Heterogeneity among trials was non-significant (χ2(8) = 6.21, p = 0.62, I2 = 0%).
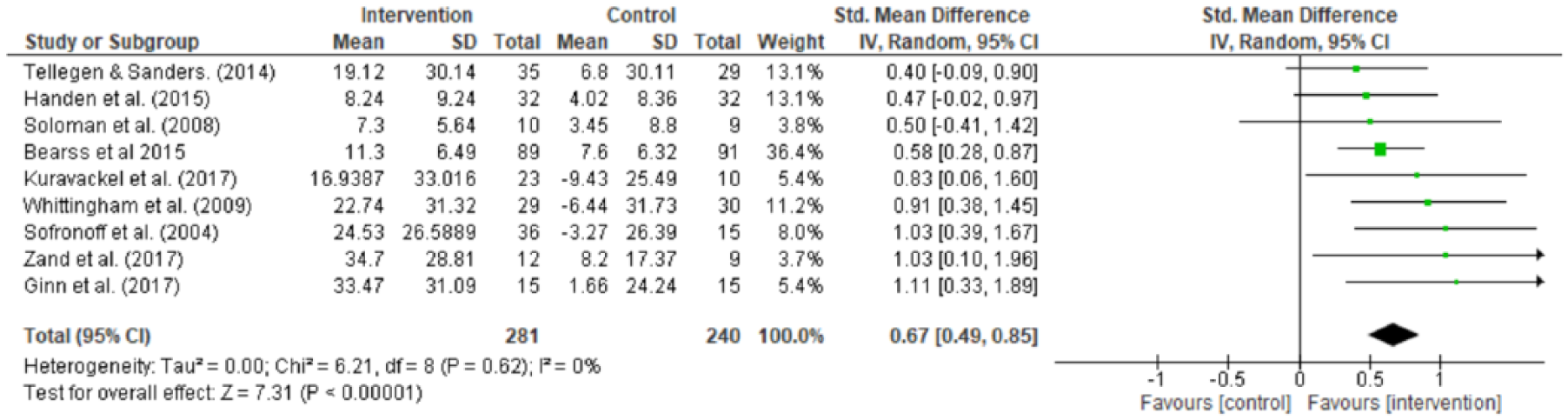
Parent intervention versus control for parent reports of child disruptive behavior.
Parent-reported hyperactivity
Parent-reported hyperactivity was used as an outcome in three trials. A meta-analysis involving 263 participants was conducted (Figure 3) revealing a small effect of intervention on hyperactivity (SMD = 0.31, 95% CI = 0.07–0.56, Z = 2.52, p = 0.01). Heterogeneity between trials was non-significant (χ2(2) = 1.23, p = 0.54, I2 = 0%).

Parent intervention versus control for parent reports of child hyperactivity.
Parenting stress
Seven trials (407 participants) were entered into an analysis of BPI effects on parent stress (Figure 4). There was a small effect of parent intervention on parenting stress (SMD = 0.37, 95% CI = 0.17–0.57, Z = 3.65, p < 0.01). Heterogeneity between trials was non-significant (χ2(6) = 3.33, p = 0.77, I2 = 0%).
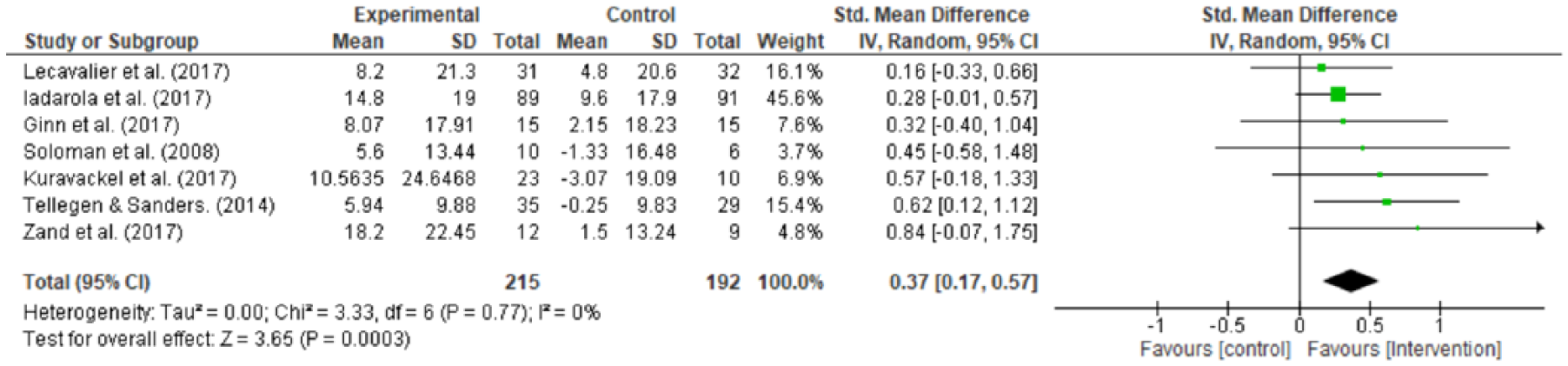
Parent intervention versus control for parent stress.
Parenting efficacy
Five trials (357 participants) assessed the effects of BPIs on parenting efficacy (Figure 5). There was no significant effect of interventions on parenting efficacy (SMD = 0.39, 95% CI = −0.17 to 0.95, Z = 1.38, p = 0.17) but heterogeneity among trials was significant (χ2(4) = 21.00, p < 0.01, I2 = 81%). Visual inspection of the forest plot indicated the Whittingham, Sofronoff, Sheffield, and Sanders (2009) trial was driving the heterogeneity. Upon removal of this study the effect of intervention on parenting confidence increased and became significant (SMD = 0.60, 95% CI = 0.36–0.84, Z = 5.00, p < 0.01); heterogeneity also reduced to non-significance (χ2(3) = 2.13, p = 0.55, I2 = 0%).
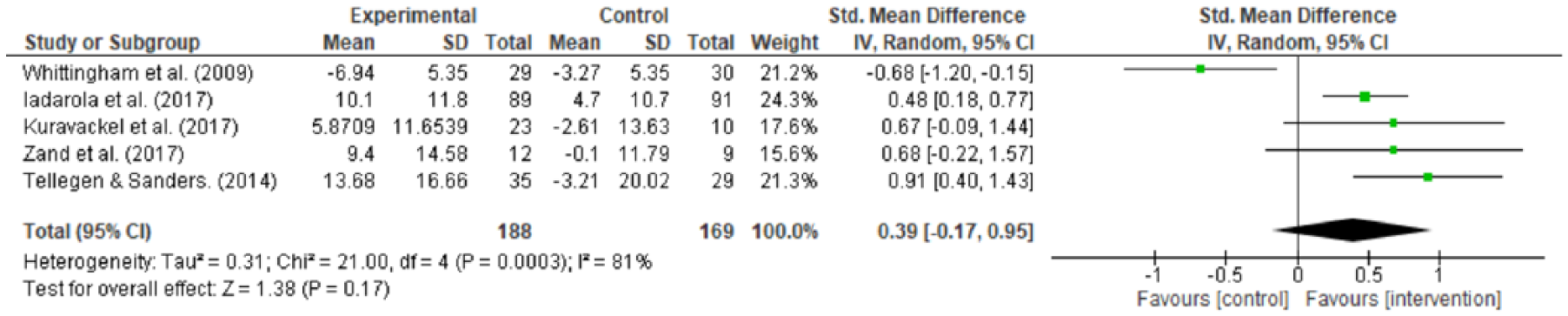
Parent intervention versus control for parenting efficacy.
Other relevant parent-reported outcome measures
Only one trial included measures of child internalizing symptoms in its outcome measures (Solomon, Ono, Timmer, & Goodlin-Jones, 2008), while two trials included outcomes measuring parent report of their own parenting behavior (Tellegen & Sanders, 2014; Whittingham et al., 2009). Given the dearth of literature in this area, the findings are not discussed further in this review.
Teacher-reported and observational outcomes
Teacher-reported and observational measures of behavior were also rarely reported in the outcomes of included trials. Measures of teacher-reported disruptive behavior and hyperactivity were included in one trial (Handen et al., 2015), while two trials included observations of child behavior (Solomon et al., 2008; Tellegen & Sanders, 2014). Two trials of parent–child interaction therapy (PCIT) included observations of parent behavior (Ginn et al., 2017; Solomon et al., 2008). Again, given the dearth of literature, the findings are not discussed further in this review.
Risk of bias
Risk of bias of included studies was assessed (Figure 6). All studies were judged low risk for selective reporting indicating all included outcome measures were analyzed and reported. Studies were assessed as low risk if they reported results for all outcomes listed in the methods section of the article. Published protocols could only be found for 3/9 included RCTs (see supplementary material). The main source of bias across studies was blinding of outcome assessment (5/11 studies high risk). Studies were deemed low risk if they included a blinded outcome of child behavior within outcome measures. In addition, Solomon et al. (2008) was judged high risk as observation data were not reported for the WLC group. However, it should be noted that for the majority of outcomes in this review, no blinded observation was included. Three of 11 studies were deemed high risk due to incomplete outcome data or lacking appropriate statistical adjustment for missing data or attrition. This can lead to inflated or inaccurate effect sizes as those with worse outcomes or experience little benefit of intervention may be most likely to drop out. Three of 11 studies were deemed unclear risk for random sequence generation. This was generally due to lack of information regarding method for random number generation. Kuravackel et al. (2018) reported the use of random number generator to assign families to groups. In the discussion of the article, the authors state that 10% of the sample could not be randomized due to parent scheduling constraints; this study was therefore deemed high risk for selection bias. The majority of studies (6/11) did not state whether research personnel were blind to treatment allocation.

Risk of bias summary: review authors’ judgments about each risk of bias item for each included study.
Discussion
This article reviewed evidence of the effects of BPIs for ASD for a range of child and parental well-being outcomes beyond their impact on disruptive behavior. There were sufficient data to conduct meta-analyses on the effect of BPIs for parent-reported disruptive child behavior, hyperactivity, parental stress, and parenting efficacy. For parent-reported disruptive child behavior, we report a comparable (SMD = 0.67) yet slightly larger effect size than Postorino et al. (2017) driven by the addition of the recently published Zand et al. (2018) and Kuravackel et al. (2018) studies. Visual inspection of the forest plots and study characteristics indicates that larger effect sizes for disruptive child behavior are evident in younger study populations. While there were insufficient data to test this formally, if confirmed by meta-regression, it would support the importance of early intervention for behavior in this population (Oono, Honey, & McConachie, 2013). However, in non-ASD populations, a recent meta-analysis found no reduced effect of BPI in older children across the age range 2–12 years (Gardner et al., 2017). We also report preliminary evidence for BPIs having a modest effect on parent-reported hyperactivity (SMD = 0.31), a similar effect size to parent reported ADHD symptoms following behavioral intervention in children with ADHD (SMD = 0.40) (Daley et al., 2014; Sonuga-Barke et al., 2013). While the meta-analysis only included three trials, this is an encouraging finding given the high levels of comorbidity of ADHD and ASD. Furthermore, only one of the trials included in the hyperactivity analysis screened for ADHD symptoms for study inclusion. However, it is worthy to note that ADHD severity can also moderate the effects of BPIs meaning management of ADHD symptoms may need to be considered prior to initiation of BPIs (Lecavalier et al., 2018). Nonetheless, this review adds to the increasing levels of evidence for the efficacy of BPIs for parental perceptions of child behavior in ASD.
To the best of the authors’ knowledge, only one study of BPI to date has assessed the effect of intervention on emotional problems and anxiety in children with ASD (Solomon et al., 2008), highlighting an important area for future research. Although BPIs are not traditionally developed for the treatment of anxiety and internalizing behavior, one could argue that BPIs in ASD might benefit from the addition of components targeting anxiety and internalizing conditions. There is evidence that levels of problem behavior are associated with internalizing disorders in ASD (Turygin, Matson, MacMillan, & Konst, 2013), suggesting that interventions targeting anxiety/low mood could also improve disruptive behavior. Cognitive behavioral therapy (CBT) programs are efficacious for anxiety in ASD (Sukhodolsky, Bloch, Panza, & Reichow, 2013); some include a substantial parent component and incorporate aspects such as psychoeducation about anxiety, graded exposure, and impact of parental anxiety. There is scope for future BPIs to borrow parental components of these interventions to form an early preventive therapy model for anxiety and behavior in ASD. However, it is possible that modification of parent behavior could also have detrimental effects on internalizing outcomes for children with ASD. Either way, given the dearth of available evidence to date, the exploration of the effects of BPIs on internalizing outcomes in children with ASD is an important area for future research.
There is also limited evidence to date on the effect of BPIs when considering outcomes from informants other than parent report (observations/teacher report). One trial (Tellegen & Sanders, 2014) reported no effect of intervention of observed child disruptive behavior despite improvements in parent-reported behavior. Solomon et al. (2008) reported improved observed child affect following PCIT, yet the lack of observation in the control group limits the reliability of this finding. Furthermore, the one trial that included teacher-reported outcomes found no significant effect of BPI on teacher-reported disruptive behavior or hyperactivity. In the ADHD literature, the effects of psychosocial intervention are reduced when considering outcomes reported by those “probably blind” to treatment allocation (Daley et al., 2014; Sonuga-Barke et al., 2013). There is insufficient evidence to date to explore whether this finding also generalizes to BPIs in the ASD population. However, the difficulty of conducting reliable and valid observations of child behavior in ASD for use in RCTs is noted, given the idiosyncrasies and heterogeneity of children with ASD and issues with floor effects (Handen et al., 2013; Johnson et al., 2009). Nonetheless, given the potential reporter bias associated with parent report of behavior following their involvement in intervention, the inclusion of blinded and teacher-reported outcomes in trials constitutes another important avenue for future research.
This is the first review to assess the effects of BPIs in ASD on parental stress and parenting efficacy. The findings reveal a small effect of interventions on parenting stress (SMD = 0.37). As anticipated, this effect size is generally smaller than interventions directly targeting parental well-being in ASD (e.g. mindfulness-based parent training) (Da Paz & Wallander, 2017). This is an encouraging benefit of BPIs which do not explicitly target parental well-being. Given evidence of child behavior influencing parent stress (Lecavalier et al., 2006), parent stress may decrease as a consequence of improved perception of disruptive child behavior. On the contrary, poor coping strategies and low levels of social support have been found to predict parenting stress in parents of children with ASD (Zaidman-Zait et al., 2018). BPIs may work to provide parents with new management strategies, improving their resource and capacity to cope, thereby decreasing feelings of parenting stress. However, parents presenting with high levels of stress will likely require additional support directly addressing their well-being (Barlow, Smailagic, Huband, Roloff, & Bennett, 2012). The complex relationship between child behavior and parent well-being is also highlighted by the lack of consistent relationships between effect sizes for parent and child outcomes in studies included in this meta-analysis. Visual inspection of the forest plots reveals consistent effect sizes for child behavior and parent outcomes in some trials (e.g. SMDs = 0.50, 0.47, and 0.45 for disruptive child behavior, child hyperactivity, and parent stress, respectively, in Solomon et al., 2008). However, other trials (e.g. Tellegen & Sanders, 2014) are associated with larger effect sizes for parent well-being compared with disruptive child behavior (SMDs = 0.40 and 0.91 for disruptive child behavior and parent stress, respectively). In the future, large trials should explore the factors mediating and moderating improved parental well-being following BPIs in ASD.
The effects of BPIs on parenting efficacy seem more variable. When considering all available data, this review found no effect of intervention on parenting efficacy. Significant heterogeneity in findings was driven by the Whittingham et al. (2009) study that was associated with reduced parenting efficacy following SSTP (Stepping Stones Triple P). This finding is curious especially given comparable levels of parenting efficacy at baseline between trials. Furthermore, two of the trials reporting increased parenting efficacy following intervention were testing a briefer version of SSTP (PCSSTP (Primary Care Stepping Stones Triple P)). However, PCSSTP focuses on aspects of child behavior parents are particularly concerned about and is delivered individually to parents rather than in group format. It could be this individualized aspect of intervention which better equips parents, resulting in improved parenting confidence. In support of this notion, two trials of PCSSTP (Tellegen & Sanders, 2014; Zand et al., 2018) also display the largest effect sizes for parenting stress in this review. Upon removal of Whittingham et al. (2009), heterogeneity reduced to non-significance and BPIs had a moderate effect on parenting efficacy (SMD = 0.60).
Finally, this review found limited evidence regarding the effect of intervention on parenting behavior. Two trials reported effects of BPI on parent reports of their own behavior and reported reductions in lax and over-reactive parenting and parental verbosity. In both the ASD and non-ASD literature, there is evidence that adverse parenting practices are associated with later problematic behavior (Keown, 2012; Osborne et al., 2008) highlighting the importance of including measures of parental behavior in future trials of BPI in ASD.
A further discussion point worthy of note is the influence of comparator groups on effect sizes. Two studies in this review (Bearss et al., 2015; Iadarola et al., 2018) used an active comparator arm (parent education). Use of an active comparator arm means one can be more certain of the impact of the behavioral management strategies of the intervention, rather than the confounding effects of therapist contact or psychoeducation components of interventions (Bearss et al., 2015). However, since active comparators are also associated with small improvements, smaller group differences are to be expected in trials using active comparators.
Limitations
Some limitations to this review are worthy of note. First, there were insufficient data to meta-analyze treatment effects for child internalizing behavior, parent behavior, and observational measures of parent and child behavior. Furthermore, only three trials were included in the meta-analysis of intervention effects on hyperactivity; therefore, the preliminary nature of this finding means it should be interpreted with caution. It is hoped this review will stimulate future research and thought into the effects of parent interventions for outcomes other than disruptive child behavior. Second, we focused on post-intervention data, it is unclear to what extent the treatment effects reported herein are maintained. Three trials (Bearss et al., 2015; Tellegen & Sanders, 2014; Whittingham et al., 2009) included a 6 month follow-up of intervention effects. All treatment effects were generally maintained with the exception of parenting efficacy in the Whittingham et al. (2009) study, where post-intervention reductions in efficacy were lost; at 6 month follow-up, efficacy increased to higher than baseline levels suggesting possible sleeper effects in this measure. Furthermore, there was some loss of intervention effects at 6 month follow-up on measures of parental over-reactivity in the Tellegen and Sanders (2014) study, although scores remained favorable compared with baseline.
Future research
Given the frequency with which anxiety and other internalizing behavior problems are seen in children with ASD (White et al., 2009), and the possibility of anxiety underlying disruptive behavior in this population (Storch et al., 2012), future trials should include measures of anxiety or internalizing symptoms within outcome measures. As previously mentioned, interventions could be modified to include components helping parents to identify and manage anxiety in ASD. Blinded measures of child behavior and assessments from informants other than parents (teacher report, observations) should also be included in future trials to remove potential reporter bias associated with parent report of child behavior following their investment in BPIs. Once larger trials have been conducted, mediator and moderator analyses will help to understand the mechanism underlying behavior change following BPIs in ASD, and to direct intervention to those most likely to benefit. Once more trials have been conducted, future research may also want to consider removal of low-quality studies from analyses to explore its impact on pooled effect sizes. Furthermore, meta-regression analyses may help to identify which components of behavioral intervention are most important for intervention success. Finally, RCTs to date are restricted to American or Australian populations; findings should be replicated in other countries, including those of lower and middle income.
Supplemental Material
AUT830042_Lay_Abstract – Supplemental material for Child and parent outcomes following parent interventions for child emotional and behavioral problems in autism spectrum disorders: A systematic review and meta-analysis
Supplemental material, AUT830042_Lay_Abstract for Child and parent outcomes following parent interventions for child emotional and behavioral problems in autism spectrum disorders: A systematic review and meta-analysis by Joanne Tarver, Melanie Palmer, Sophie Webb, Stephen Scott, Vicky Slonims, Emily Simonoff and Tony Charman in Autism
Supplemental Material
AUT830042_Supplemental_material – Supplemental material for Child and parent outcomes following parent interventions for child emotional and behavioral problems in autism spectrum disorders: A systematic review and meta-analysis
Supplemental material, AUT830042_Supplemental_material for Child and parent outcomes following parent interventions for child emotional and behavioral problems in autism spectrum disorders: A systematic review and meta-analysis by Joanne Tarver, Melanie Palmer, Sophie Webb, Stephen Scott, Vicky Slonims, Emily Simonoff and Tony Charman in Autism
Footnotes
Acknowledgements
The views expressed in this presentation are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review was funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research programme (RP-PG-1211-20016) awarded to Professor Emily Simonoff.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.