
Abstract
Reaction to a child’s diagnosis can strongly affect the parent, but little is known about the aspects of the diagnostic process associated with such reactions. The pre-diagnostic levels of anxiety, depression, and parenting stress of 67 volunteer mothers of children subsequently diagnosed with autism spectrum disorder were assessed, along with the children’s functioning. The speed and number of professionals involved in the diagnosis were recorded, and mothers completed a post-diagnosis assessment of their perceptions of the process. Longer actual and perceived diagnosis speeds predicted resolved reactions to diagnosis. Mothers’ psychological states pre-diagnosis did not predict reactions to diagnosis. Providing a measured diagnostic process, and strong relationship with mothers, rather than aiming for speed alone, may well be more productive for the parent and child.
Keywords
The impact on the functioning of parents of a child receiving a diagnosis has been the subject of recent research attention for many disorders: cerebral palsy (Marvin & Pianta, 1996; Rentinck et al., 2010; Schuengel et al., 2009), general childhood psychiatric problems (Kearney, Britner, Farrell, & Robinson, 2011), childhood diabetes (Lowes, Lyne, & Gregory, 2004), and autism spectrum disorder (ASD) (Chamak, Bonniau, Oudaya, & Ehrenberg, 2011; Milshtein, Yirmiya, Oppenheim, Koren-Karie, & Levi, 2010; Osborne & Reed, 2008; Poslawsky, Naber, Van Daalen, & Van Engeland, 2014). Focusing on the effects of a child’s diagnosis on parents is important for a number of reasons, including its impact on parental stress (Chamak et al., 2011; Davis & Carter, 2008; Goin-Kochel, Mackintosh, & Myers, 2006; Osborne & Reed, 2008). This aspect of parental functioning relates to worse physical and mental health (Dumas, Wolf, Fisman, & Culligan, 1991; Reed & Osborne, 2012; Reed, Sejunaite, & Osborne, 2016). Parental health impacts their interactions with their children (Dempsey, Keen, Pennell, O’Reilly, & Neilands, 2009; Lecavalier, Leone, & Wiltz, 2006; Osborne & Reed, 2010) and the outcomes of interventions that the children receive (Osborne, McHugh, Saunders, & Reed, 2008a; Robbins, Dunlap, & Plienis, 1991). Thus, the diagnosis and subsequent parental reaction may be a key point in determining pediatric outcomes (Osborne, 2009).
An important aspect of parents’ experience of their child’s diagnostic process is their own “reaction to the diagnosis” (Marvin & Pianta, 1996; Milshtein et al., 2010; Øien & Eisemann, 2016; Poslawsky et al., 2014). This has been assessed by the Reaction to Diagnosis Interview (RDI), which classifies parents’ reactions as either “resolved” or “unresolved” (Marvin & Pianta, 1996). Resolved parental reactions reflect the ability to control emotions regarding the diagnosis and being able to deal with their child’s condition and their parenthood (Marvin & Pianta, 1996; Poslawsky et al., 2014). In contrast, “unresolved” reactions imply that the parent finds it difficult to change their hopes and beliefs about their child after the diagnosis, and they often report a prolonged “grieving” period (Marvin & Pianta, 1996; Poslawsky et al., 2014). Across a range of childhood problems, a “resolved” reaction is associated with better parental mental states (Marvin & Pianta, 1996; Reed, Picton, Grainger, & Osborne, 2016; Sheeran, Marvin, & Pianta, 1997), physical health (Herring et al., 2006), and relationships with their child (Fraiberg, Adelson, & Shapiro, 1983; Milshtein et al., 2010; Wachtel & Carter, 2008).
In several studies relating to parents of children with ASD, high percentages of unresolved reactions to diagnoses have been noted (Milshtein et al., 2010; Oppenheim, Koren-Karie, Dolev, & Yirmiya, 2009; Poslawsky et al., 2014). However, studies have not always noted such high rates of unresolved reactions (e.g. Poslawsky et al., 2014). This mixed pattern of results is mirrored in the findings of a number of qualitative studies of the reactions and experiences of parents of children with ASD to the diagnostic process (Andersson, Miniscalco, & Gillberg, 2014; Goin-Kochel et al., 2006; Osborne & Reed, 2008). The reasons behind the wide range of different reactions to diagnosis are unclear, but there are two plausible possibilities: parental functioning prior to the diagnosis (Milshtein et al., 2010) and the diagnostic process itself (Goin-Kochel et al., 2006). The former has been studied by Wayment and Brookshire (2018) and the latter by Reed, Picton, et al. (2016), but the two have not been related in a single study.
It might be that parents’ psychological state at the start of the diagnostic process predicts their reaction to the diagnosis of their child. Parents often notice potential child problems, long before a diagnosis of ASD is made (see Chawarska et al., 2007; Wayment & Brookshire, 2018). The stress and uncertainty that occur regarding their child, and what will happen, during this period, may take a psychological toll on the parents and generate many psychological problems like depression and anxiety (Chawarska et al., 2007; Osborne, 2009). Unfortunately, there have been no studies of the impact of psychological states at the start of the diagnostic process, such as depression or anxiety, on reaction to diagnosis. This might be important to know, as parents of children with ASD are at risk of higher levels of stress and associated mental problems than parents of children with many other disorders (Eisenhower, Baker, & Blacher, 2005; Floyd & Gallagher, 1997; Hayes & Watson, 2013; Wayment & Brookshire, 2018).
In addition, parents of children with ASD report high levels of dissatisfaction with the diagnosis process itself (Chamak et al., 2011; Crane, Chester, Goddard, Henry, & Hill, 2016; Goin-Kochel et al., 2006; Siklos & Kerns, 2007), often higher than the levels of dissatisfaction with diagnosis relating to more physically obvious childhood problems (Osborne & Reed, 2009). Parents of children with ASD have described the diagnostic process as poorly conducted and chaotic (Chamak et al., 2011; Goin-Kochel et al., 2006; Osborne & Reed, 2008). In particular, their concerns have involved the speed of the process (Moh & Magiati, 2012; Osborne & Reed, 2008), the numbers of professionals that they have had to see to obtain a diagnosis (Goin-Kochel et al., 2006), and the knowledge and interpersonal skills of the professionals involved (Goin-Kochel et al., 2006; Mansell & Morris, 2004; Osborne & Reed, 2008). These types of comments are found across systems in many countries, including those in France, Singapore, and the United Kingdom (Chamak et al., 2011; Moh & Magiati, 2012; Osborne & Reed, 2008). However, it has not been established whether any particular aspects of the diagnostic process, either actual or perceived, are associated with particular parental reactions to the diagnosis.
Although a range of factors connected to the diagnostic process, as outlined above, were considered in this study, the actual and perceived speed of the diagnostic process was of particular interest. This variable was highlighted because of some discrepancies in the literature regarding the desirability of a speedy diagnosis for a child with ASD (Andersson et al., 2014; Osborne & Reed, 2008). In almost all studies of parental views, a speedier diagnosis has been a key concern (Goin-Kochel et al., 2006; Moh & Magiati, 2012; Osborne & Reed, 2008); parents express a wish for a quick and clear diagnosis for their child (Moh & Magiati, 2012; Osborne & Reed, 2008), and this is related to reduced anxiety (Reed, Picton, et al., 2016). However, clinically, fast diagnosis is not always regarded as an optimal procedure (Andersson et al., 2014). Indeed, a speedy diagnosis has been seen to increase the levels of parenting stress (Lowes et al., 2004; Osborne et al., 2008) and ill health (Reed, Sejunaite, & Osborne, 2016). Thus, it was of interest to explore whether reactions to diagnosis were related to its actual and perceived speed.
To address the above gaps in knowledge, the current exploratory study followed mothers of children with ASD through the diagnostic process, assessing their levels of psychological functioning at the start of the process, documenting the diagnostic process, and then assessing mothers’ reactions to the diagnosis. It was hoped that this might highlight relationships between the actual diagnostic process, the mothers’ perceptions of the process, and the parent’s eventual reaction to diagnosis. Such findings might be able to answer the issue of whether these diagnostic process variables are related to the reaction to diagnosis over and above any initial parental functioning issues or child functioning variables. This information may allow professionals to target key aspects of the process to help parental adjustment.
Method
Participants
The mothers of 110 children consecutively referred for assessment and potential diagnosis of ASD, at a single assessment site, were asked to participate in research concerning their feelings about the diagnostic process. Mothers were selected, as it was felt that there may not be enough fathers available to make a meaningful comparison, and the inclusion of only a few fathers, who may react differently, might compromise the sample. Of the mothers approached, 95 (86%) agreed, 10 did not complete the diagnostic process, and 18 children did not receive an ASD diagnosis, leaving 67 mothers. A power analysis based on detecting a medium-sized effect (f′ = 0.25), with 80% power at the p < 0.05 level, suggested that 57 participants would be required in an analysis involving six predictor variables (to accommodate the variables from the Diagnostic Experience Scale, below).
The mean age of the participating mothers was 40.91 (±7.28, range = 21–54) years; 48 (71%) were married or in civil partnership, 3 (5%) were in another form of relationship, and 16 (24%) were single, divorced, or widowed. In terms of occupation, 8 (12%) were classed as laborers, 9 (13%) as skilled, 25 (37%) as managerial/professional, and 25 (37%) as unemployed or home-makers. The ethnic backgrounds of the mothers were as follows: 46 (69%) White, 3 (5%) mixed/multiple, 10 (15%) Asian, 6 (9%) Black/African/Caribbean, and 2 (2%) Other.
Of the children diagnosed with ASD, 52 (78%) were male and 15 were female (22%). The children’s mean age was 6.08 (±3.17, range = 2–14) years at the start of the diagnostic process. The ASD severity was assessed using the standardized severity score (Gotham, Pickles, & Lord, 2009) of the Autism Diagnostic Observation Schedule (ADOS; Lord, Rutter, DiLavore, & Risi, 1999); this mean was 6.53 (±1.41, range = 3–9). Table 1 shows the characteristics of the children (overall standard scores) for nonverbal intellectual functioning (Leiter International Performance Scale), verbal functioning (British Picture Vocabulary Scale (BPVS)), and adaptive behavior (Vineland Adaptive Behavior Scale (VABS).
Mean levels of autism severity (ADOS), nonverbal functioning (Leiter-R), verbal functioning (BPVS), and adaptive behavior (VABS) of the children, and their Pearson correlations.
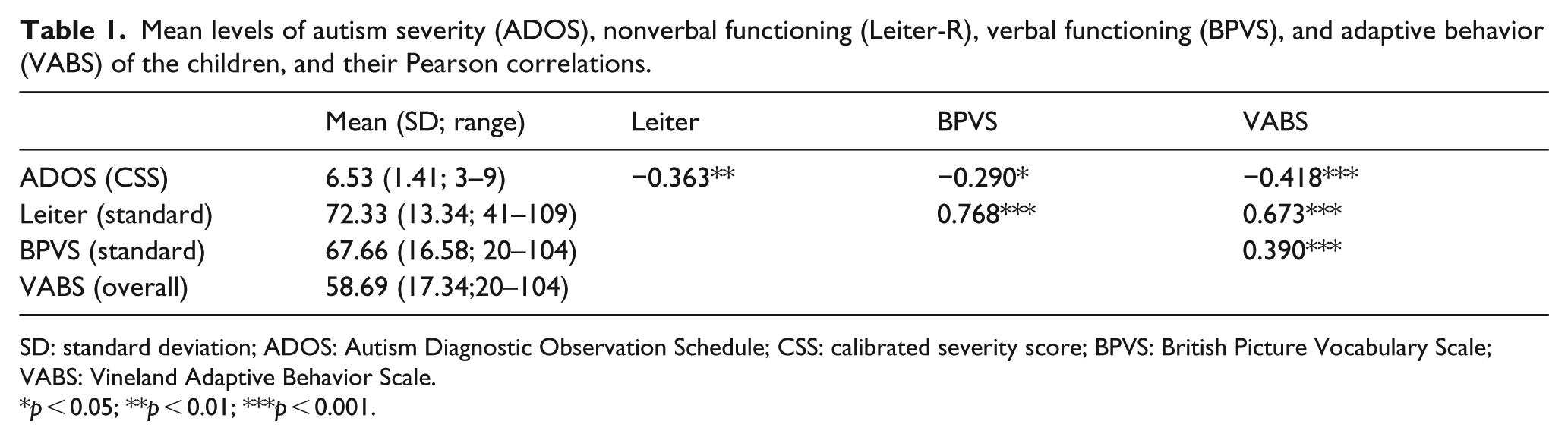
SD: standard deviation; ADOS: Autism Diagnostic Observation Schedule; CSS: calibrated severity score; BPVS: British Picture Vocabulary Scale; VABS: Vineland Adaptive Behavior Scale.
p < 0.05; **p < 0.01; ***p < 0.001.
Ethical approval was given by the Psychology Department Ethics Committee of the University.
Diagnostic process
Although variable across participants, the typical diagnostic process, in this context, was that the parent(s) would have approached their General Medical Practitioner with a concern about their child (not necessarily ASD). They would have received about a 10- to 20-min consultation with the general practitioner (GP) and then received a referral to a specialist ASD team if the GP thought it appropriate. A smaller number of children may have received this referral through Educational psychologists working within the school system, to whom the child had been referred. The diagnostic team comprised a number of healthcare professionals, based at a single assessment center. This team comprised a consultant pediatrician, along with educational psychologists and speech and language therapists, who, either working together or separately, would complete a series of assessments to make a diagnosis of the child. The form of this assessment process would differ, depending on the child’s characteristics and the responses to the diagnostic test. Each visit to the center could take up to 3 h, depending on the consultation process and/or tests being administered. The mean length of the diagnostic process, from first visit to the diagnostic team to receiving a formal diagnosis, was 12.06 (±5.76, range = 3–39) months. The number of visits was also recorded, and the mean was 2.81 (±0.82, range = 2–6) visits.
Formal diagnosis was always given by consultant pediatricians, who all used a combination of the general Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria, the ADOS (Lord et al., 1999), and clinical judgment, to make their diagnoses. Although there was some variation in practice, the consultant pediatrician typically saw the mothers at each appointment, but the assessments were sometimes conducted by other members of the diagnostic team. In addition, educational psychologists and speech and language therapists could be involved in this process. All of the diagnostic team members were independent of this study. Based on medical record review, mothers saw different combinations of clinicians, and some saw more than one clinician from the same profession. Of the sample, 11 (16%) mothers only saw one professional, 22 (33%) saw two professionals, 17 (25%) saw three, 11 (16%) saw four, and 6 (9%) saw five (mean = 2.69 ± 1.20, range = 1–5). The combinations of professionals were highly variable across participants. Further data regarding the characteristics of the diagnostic process are presented in the “Results” section (see Table 2).
Characteristics of the diagnosis process (mean age of parent and child at the start of process, length of process (months), number of visits, and number of professionals seen) and their Pearson correlations.
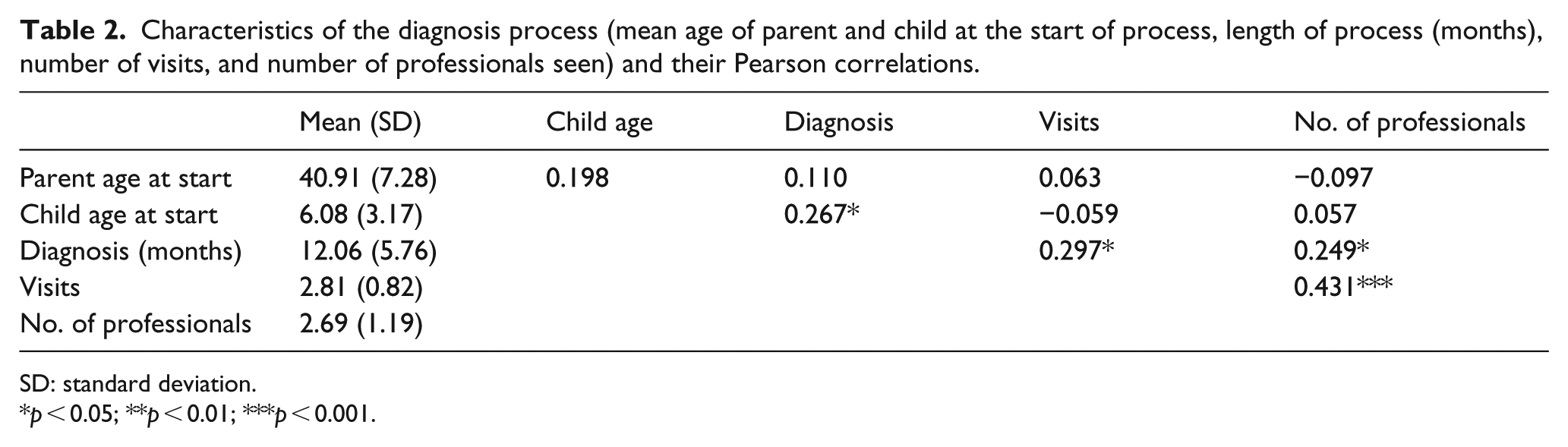
SD: standard deviation.
p < 0.05; **p < 0.01; ***p < 0.001.
Measures
RDI (Marvin & Pianta, 1996; Poslawsky et al., 2014) contains five semi-structured questions asked by a professional to a parent about their feelings and beliefs surrounding the diagnostic process, their child’s condition, and the participant’s reaction to the diagnosis (e.g. “When did you first realize that your child had a medical problem?”). The RDI is analyzed through content analysis, with participants being classified as either “resolved” or “unresolved” based on coding of their responses. There are three sub-types within the “resolved” classification (“feeling oriented,” “thinking oriented,” and “action oriented”), and six sub-types within the unresolved classification (“emotionally overwhelmed,” “angrily preoccupied,” “neutralizing,” “depressive/passive resignation,” “cognitive distortions,” and “disorganized/confused”). Previous studies have noted good inter-coder reliability of RDI classifications (Poslawsky et al., 2014). In this study, two coders (blind to the rest of the data relating to the participants) coded the responses according to the RDI manual. Inter-coder agreement was 100% on the main classifications, and 92% on the sub-classifications. Disagreements were settled by discussion.
ADOS (Lord et al., 1999) is a semi-structured standardized observation of the child by a professional that measures autism symptoms. A standardized calibrated severity score (CSS) regarding the symptoms of the children with ASD relative to other children with ASD can be calculated (Gotham et al., 2009), which has a range of 1–10, with 4 being the cut off for ASD.
Leiter International Performance Scale–Revised (Leiter-R; Roid & Miller, 1997) measures intellectual abilities of individuals with significant communication, cognitive, and learning disabilities. It is administered to the child by a professional. It provides a total nonverbal IQ score (mean = 100 ± 15). The internal reliability (α) previously has been noted to vary from 0.91 to 0.93 (Roid & Miller, 1977).
BPVS (Dunn & Dunn, 1997) measures receptive language ability for children aged 3–17 years. It is administered to the child by a professional. It has a previously established α of 0.93 (Dunn & Dunn, 1977).
Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983) is a self-assessment completed by the participant of their levels of anxiety and depression and contains seven items for anxiety and seven for depression. These scales give scores ranging from 0 to 21; 0–7 = “normal,” 8–11 = “mild,” 12–14 = “moderate,” and 15+ = “severe.” It has previously established test–retest reliabilities for a population of parents with ASD of 0.86 for anxiety and of 0.74 for depression (Hastings & Brown, 2002).
Questionnaire on Resources and Stress (QRS-F; Friedrich, Greenberg, & Crnic, 1993) is a self-assessment by parents of their perceptions of the impact of a developmentally delayed child on other family members. It comprises four sub-scales (Parent and Family Problems, Pessimism, Child Characteristics, and Physical Incapacity), which summate to produce a Total Stress Score. The α of the total stress scale for this sample is 0.89.
Diagnostic Experience Scale (DES; Reed, Picton, et al., 2016) is a self-assessment by parents of their perceptions of a number of aspects of the diagnostic process. Mothers rate their experience and views of the process on a 5-point scale (“very poor” to “very good”), which were scored on a 1 (very poor) to 5 (very good) scale. They are asked to rate five aspects of the process on this scale: “the speed of the diagnostic process,” “the interpersonal skills of the health professionals you have seen,” “the communication ability of the health professionals you have seen,” “the helpfulness of information provided to you in understanding ASD,” and “the coherence of the diagnostic system (e.g. was there a structure to the process that you were able to understand and prepared you in advance for each step of the process).” These questions were chosen on the basis of the aspects of the process that parents had mentioned in many qualitative studies of their experiences of getting a diagnosis of ASD for their child (Chamak et al., 2011; Goin-Kochel et al., 2006; Mansell & Morris, 2004; Moh & Magiati, 2012; Osborne & Reed, 2008). The internal reliability (α) of the scale for this sample was 0.81.
Procedure
On referral to the Child and Adolescent Mental Health clinic, mothers were approached by a member of the research team, who was a clinically trained psychologist, with 15 years of experience in working with individuals with ASD and their families, and who was independent of the clinical diagnostic team, and asked whether they would like to participate in the study. Once consent had been given, the above psychologist administered the HADS and QRS-F to the mothers at their initial appointment. The child was tested with the ADOS, Leiter, and BPVS during the diagnostic process, by assessors experienced with ASD, who were members of the diagnostic team and who were clinically trained in the administration of these tests. Apart from the ADOS, these tests were not part of the standard diagnostic evaluation. Permission was sought from the mothers to access the medical records of their children, and these were explored to ascertain the time taken for the diagnosis process (from first appointment to receiving a diagnosis), the child’s age at receiving a diagnosis, and how many professionals were involved in the process.
When the diagnosis had been received (within the same week), the mothers were contacted by telephone and asked by the above clinically trained member of the research team (experienced in dealing with families of individuals with ASD) whether they wished to participate in the RDI, and to complete the DES. Those wishing to participate were given the RDI over the telephone by the same psychologist. The responses from the RDI were coded by two research psychologists, who were independent from the study, blind to the study’s purpose, and who were trained to research-reliability levels with the RDI. The DES was sent to the mothers in the post with a stamped address return envelope for its return on completion.
Results
There were 41 (61%) mothers classified as “resolved” in their reaction to diagnosis: 18 (43%) “feeling-oriented,” 18 (43%) “thinking-oriented,” and 5 (14%) “action-oriented.” Of the 26 (39%) mothers with an “unresolved” reaction to diagnosis, 13 (50%) were classed “depressed/passive resignation,” 6 (23%) “neutralizing,” 4 (15%) “angrily preoccupied,” and 3 (12%) “cognitive distortions.”
The psychological state of the mothers prior to the diagnostic process was compared across resolved and unresolved classifications (sub-classifications were not analyzed due to the low numbers that this would entail). There was no difference in depression (HADS-D) between the resolved (mean = 9.49 ± 3.87) and unresolved (8.92 ± 4.30) groups, t < 1, d = 0.15. Although unresolved reaction include “depressed/passive resignation,” there are other sub-types of unresolved issues, and the former may be capturing differing aspects of depression than the HADS-D. There were no significant differences for anxiety (HADS-A): resolved group mean was 8.00 (±2.87) and the unresolved group mean was 6.84 (±3.06), t(65) = 1.57, p > 0.10, d = 0.38. These mean scores are in the mild range for depression and anxiety. There was no statistically significant difference in parenting stress (QRS-F); resolved group mean was 25.61 (±9.44) and unresolved group mean was 29.23 (±7.76), t(65) = 1.63, p > 0.10, d = 0.42.
A logistic regression was conducted to determine whether any of the pre-diagnosis child variables or mothers’ psychological variables—child’s autism severity (ADOS), nonverbal (Leiter) and verbal (BPVS) functioning, adaptive behavior (total VABS), mothers’ pre-diagnosis depression (HADS-D), anxiety (HADS-A), and parenting stress (QRS-F)—predicted reaction to diagnosis (0 = unresolved; 1 = resolved). Collinearity statistics were calculated for these variables, and there was tolerance to all variables of greater than 0.2, and variation inflation factors (VIFs) between 1.6 and 4.1, indicating no cause for concern. The model was not significantly related to reaction to diagnosis, −2LL = 81.07, χ2(7) = 8.42, p > 0.30, Nagelkerke R2 = 0.160, and none of the predictors were individually significantly related to diagnosis reaction: child autism severity (β = 0.125, p > 0.60); child nonverbal functioning (β = 0.017, p > 0.60); child verbal functioning (β = –0.034, p > 0.20); child adaptive functioning (β = 0.004, p > 0.80); mother depression (β = 0.022, p > 0.70); mother anxiety (β = 0.132, p > 0.20); and mother parenting stress (β = –0.066, p > 0.07).
The Pearson correlations between the diagnostic process characteristics are highlighted in Table 2 (which were all small in size, except for the number of visits and the duration, and the number of visits and number of professionals involved, as might be expected). A stepwise logistic regression was conducted to determine whether any of these diagnostic characteristics predicted reaction to diagnosis over and above the child’s and mother’s characteristics noted above (0 = unresolved; 1 = resolved). The child’s and mother’s psychological characteristics (as noted above) were entered in step 1 and the objective aspects of the diagnostic process (parent age at start, child age at start, duration, visits, and number of professionals) in step 2. Collinearity statistics were calculated for these latter variables, and there was tolerance to all variables of greater than 0.7, and VIFs between 1.0 and 1.4, indicating no cause for concern. Step 2 of the model was significant, −2LL = 67.92, χ2(5) = 13.16, p < 0.05, Nagelkerke R2 = 0.374. Of the individual predictors, only the duration of the process was significant (β = 0.132, p < 0.05, odds ratio = 1.129), with longer durations predicting a resolved reaction to diagnosis; none of the other aspects associated with the process—mother’s age (β = 0.014, p > 0.70), child age (β = –0.014, p > 0.10), number of visits (β = 0.960, p > 0.06), or number of professionals (β = –0.087, p > 0.70)—predicted the reaction to diagnosis.
The mothers’ responses to the DES are shown in Table 3, as well as their correlations with each other, and with the characteristics of the participants and diagnosis. There were only a few significant relationships between the characteristics of the participants and the mothers’ rating of the diagnostic experience. The only relationship to be noteworthy was that between the child’s age at the start of the diagnostic process and the perceived speed of diagnosis; as the age of the children increased, their mothers’ rating of the speed of the diagnostic process decreased (the rating of the process became poorer). There were also several negative relationships between pre-diagnosis parenting stress and the diagnostic experience. The actual speed of the diagnosis was negatively related to mothers’ rating of the diagnosis speed (meaning objectively faster diagnosis was associated with ratings of the speed as “good”).
Responses to the Diagnostic Experience Survey (DES) scored 1–5 (where 5 is good) and Pearson correlations between these and a range of other variables: autism severity (ADOS), nonverbal functioning (Leiter-R), verbal functioning (BPVS), adaptive behavior (VABS), mothers’ depression (HADS-D), mothers’ anxiety (HADS-A), and mothers’ parenting stress (QRS-F).
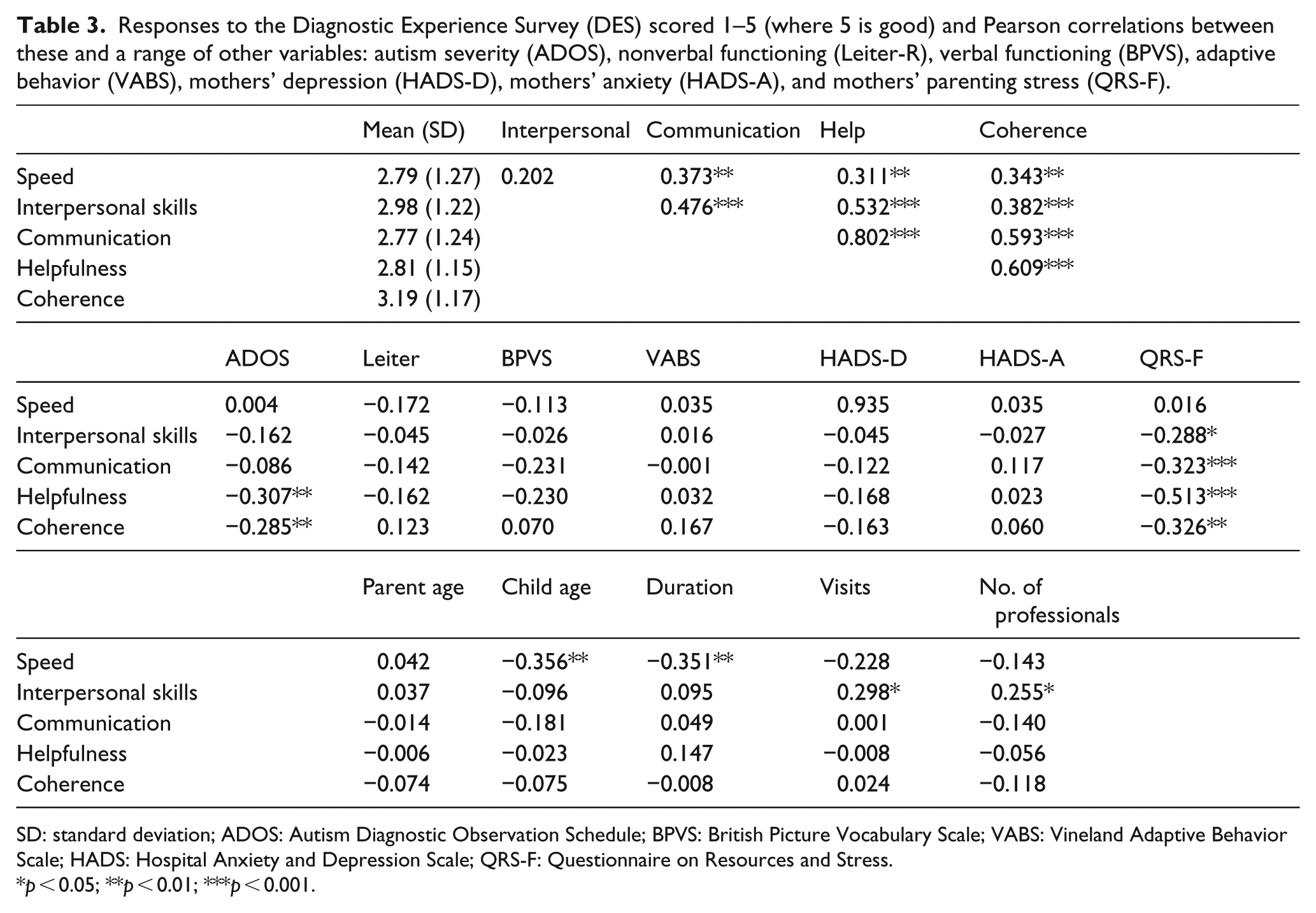
SD: standard deviation; ADOS: Autism Diagnostic Observation Schedule; BPVS: British Picture Vocabulary Scale; VABS: Vineland Adaptive Behavior Scale; HADS: Hospital Anxiety and Depression Scale; QRS-F: Questionnaire on Resources and Stress.
p < 0.05; **p < 0.01; ***p < 0.001.
A stepwise logistic regression was conducted to determine whether any of these diagnostic characteristics—speed, interpersonal skills, communication, helpfulness, and coherence—predicted reaction to diagnosis (0 = unresolved; 1 = resolved) over and above the child’s and mother’s psychological characteristics (as noted above). Child/mother characteristics were entered in step 1, and mothers’ perceptions were entered in step 2, which was significant, −2LL = 57.81, χ2(5) = 23.26, p < 0.001. Collinearity statistics were calculated for these latter variables, and there was tolerance to all variables of greater than 0.3, and VIFs between 1.1 and 3.2, indicating no cause for concern. Of the individual predictors, speed (β = −0.912, p < 0.01, odds ratio = 0.398), with durations rated as not a “poorer” predicting a resolved reaction to diagnosis and the interpersonal skills of the professionals (β = 0.933, p < 0.05, odds ratio = 2.543), with better rated interpersonal skills, predicting a resolved reaction to diagnosis; none of the other aspects predicted reaction to diagnosis: communication (β = 0.272, p > 0.60), helpfulness (β = –0.048, p > 0.90), or coherence (β = 0.627, p > 0.10).
Discussion
The key finding to emerge was that mothers who experienced a longer diagnostic process, and those who rated the speed of the process as “poorer,” tended to be “resolved” in their reaction to the diagnosis. Although somewhat counter-intuitive, the finding that a longer diagnosis period (actual or perceived) is associated with a greater tendency to resolution of diagnosis corroborates clinical impressions that more measured (and longer) approaches to diagnosis (Andersson et al., 2014) warrant further investigation as to their potential benefits. On first examination, this seems at odds with what parents claim they want in regard to the process—that is, a quicker diagnosis (Goin-Kochel et al., 2006; Moh & Magiati, 2012; Osborne & Reed, 2008). This apparent discrepancy will need to be explored; however, these two findings may not necessarily be in conflict with one another. A parent could have been both frustrated with a long process and also be better resolved because of the length of time taken, but may not integrate these two pieces of information. That is, the mothers were not rating the length of the diagnostic process in the light of their resolution of the diagnosis, and, when asked about the period, they may say that it took a long time, and the length of time was frustrating. These current findings are also consistent with cross-sectional studies of several disorders that have noted parents who experience a speedier diagnosis report higher levels of parenting stress (Lowes et al., 2004; Osborne, McHugh, Saunders, & Reed, 2008b), and worse physical health Reed, Sejunaite, & Osborne, 2016).
However, suggesting that the diagnosis period should be longer is not a straightforward implication of these results. A longer diagnosis period has been associated with increased parental anxiety and depression (Moh & Magiati, 2012; Reed et al., 2016). Increases in these aspects of parental functioning may, in themselves, lead to negative impacts on parental health (Osborne & Reed, 2010; Reed & Osborne, 2012; Reed, Sejunaite, & Osborne, 2016) and also to a worse prognosis for their children (Osborne et al., 2008a; Robbins et al., 1991). Moreover, participants might have differed in how they understood the question about the speed of the diagnostic process. When asked to rate “the speed of the diagnostic process,” mothers could have answered based on perceived duration, or on goodness or satisfaction. The wording on the question suggests the former, but what was actually rated might have differed. The distinctions among these possibilities may be important; for example, the process might have been perceived to take a long time, but the mother may have been happy that considerable care was taken to get it right. Thus, care is needed in interpreting these results.
As noted, the finding that longer diagnostic periods produce better resolution stands in apparent contrast to the demand that parents have for speedier ASD diagnosis (Goin-Kochel et al., 2006; Osborne & Reed, 2008). The explanation for this contrast is not immediately apparent, but it may relate to changes in the skills of professionals giving the diagnosis over the years since the above qualitative reports (Goin-Kochel et al., 2006; Moh & Magiati, 2012). Of course, it is difficult to make generalizations from such qualitative studies to the current quantitative study, and across potentially different diagnostic contexts (different countries, systems, etc.). However, in this study, the perceived interpersonal skills of the professionals were important in mothers reaching resolution of the diagnosis (Chamak et al., 2011; Mansell & Morris, 2004; Osborne et al., 2008). This is perhaps not surprising given the literature on the importance of the client–therapist relationship to successful outcomes (Duncan, Miller, Wampold, & Hubble, 2010; Zandberg, Skriner, & Chu, 2015). It may be that the interpersonal skills of the professional mediate or moderate the relationship between diagnostic speed and reaction-to-diagnosis: professionals with better skills produce more resolved reactions to diagnosis with a longer diagnostic period, but those with poorer skills have the opposite effect. Previously, interpersonal skills were noted to be poor (Goin-Kochel et al., 2006; Osborne & Reed, 2008), and changes in this aspect of the process might underlie the contrast between parents previously expressed views about speed and reaction (Goin-Kochel et al., 2006; Osborne & Reed, 2008) and the current findings—a suggestion needing exploration with a larger sample than in the current cohort. The analytic plan for the current sample was deliberately simple because the study was exploratory with few hypotheses.
Very few of the parental pre-diagnostic variables were related to the subsequent reactions to diagnosis in this study. This finding stands in contrast to previous results that have shown parental psychological states are associated with reactions to diagnosis (Milshtein et al., 2010; Wachtel & Carter, 2008). However, in these previous studies (Milshtein et al., 2010; Wachtel & Carter, 2008), the measures used were different to those employed in this study. In the previous studies, the measures assessed long-standing tendencies to display particular psychological reactions across multiple situations (i.e. trait measures). Due to the number of variables already assessed in this study, such trait measures were not included. It is unknown how such trait characteristics relate to the current psychological distress measures. Moreover, in the previous studies, the psychological variables assessed were measured simultaneously with the reaction to diagnosis, and not pre-diagnosis. Nevertheless, it is worth noting that parenting stress prior to diagnosis was negatively associated with a number of perceptions of the diagnosis process. This finding is consistent with the model of parent–child reactions (Osborne, 2009) in which pre-existing parenting perceptions of their own abilities is a factor in developing their subsequent reactions to professionals and their children.
Around two-thirds of the current sample reported a “resolved” reaction, which is somewhat higher than in several previous studies (Milshtein et al., 2010; Oppenheim et al., 2009), but in line with another study (Poslawsky et al., 2014), of this population. There are multiple factors that could have influenced these differences, and which cannot be resolved here, although it might be worth noting that studies with higher resolved reactions are more contemporary in time. That the mean ratings of the diagnostic process in this study were above the midpoint suggests that, at the very least, the processes experienced were broadly acceptable to the sample.
There were a number of limitations to this study that need to be acknowledged. First, the current sample was drawn from one site, and a larger multisite sample would extend the generalizability of these findings. Taking a fuller range of measures, and including a different set of tools in the psychometric battery, would also increase the generality of the findings. The current sample experienced a mean diagnosis period of about 12 (range = 3–39) months and a sample with different diagnosis periods may have recorded different results. It is notable that there was a large range in terms of the length of the process, which has previously been noted (Reed et al., 2016), but may not be seen in all contexts. Many of the children were diagnosed at a relatively old age, and this may have influenced the results. Most parents approached their GP with a concern for referral; it is unlikely that referral was purely on the basis of GP concern alone. Of course, sometimes parents are not worried, but their GP may be, and this situation may be different from that of a parent who was bringing the topic to their GP’s attention.
It was not possible to obtain a complete picture of what happened to the mothers during the diagnostic process, nor precisely what they were told by the clinicians, and this may have affected the outcomes. It is possible that some of the mothers, whose children were not diagnosed quickly, may have accessed medical advice outside the records that were available to the researchers. They might have engaged with people, articles, online material, and so on that affected their reaction to the diagnosis. For example, mothers who read certain online materials, or spoke to parents who were, themselves, more resolved regarding the diagnosis, might have been more likely to be resolved by the end of the diagnostic process. There are many factors other than the duration of the diagnostic process that will play a role in reaching a resolution, and these will need assessing in future work. Some important variables are the quality of the diagnostic process, the consistency in the language used across different members in the team, and the parents’ coping abilities, support, and resources.
In summary, relatively longer diagnostic periods and better interpersonal skills by the professional are associated with greater resolution for the mothers. In contrast, the pre-diagnostic attributes of the mothers have little predictive utility in terms of the reaction to the diagnosis. Strong interpersonal skills and a measured approach to the diagnostic process will help to produce a potentially beneficial resolution reaction toward the diagnosis in the parent of a child with ASD. However, both actual and perceived speedy diagnoses were associated with unresolved reactions to diagnosis.
Supplemental Material
AUT833676_Lay_Abstract – Supplemental material for Actual and perceived speedy diagnoses are associated with mothers’ unresolved reactions to a diagnosis of autism spectrum disorder for a child
Supplemental material, AUT833676_Lay_Abstract for Actual and perceived speedy diagnoses are associated with mothers’ unresolved reactions to a diagnosis of autism spectrum disorder for a child by Phil Reed, Ashleigh Giles, Shonagh White and Lisa A Osborne in Autism
Footnotes
Compliance with ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from all individual participants included in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.