
Abstract
Autism spectrum disorder in China differs considerably from autism spectrum disorder in the West in terms of prevalence estimates, education opportunities, and life outcomes of autistic people. The lack of autism spectrum disorder awareness could be a key factor underlying the disparities. To date, there has been no evaluation of autism spectrum disorder knowledge among the general public of China. Using the Autism Stigma and Knowledge Questionnaire developed for use in diverse cultural contexts, this study uncovered profoundly different public views about autism spectrum disorder in China compared with the United States. Determined by cognitive diagnosis modeling, 86%–91% of the surveyed U.S. citizens (N = 1127) achieved adequate autism spectrum disorder knowledge in diagnosis/symptoms, etiology, and treatment, whereas for the Chinese citizens (N = 1254) the percentages were only 57%–65%. Moreover, 14% of the participants from the United States were classified to endorse autism spectrum disorder stigma; in comparison, 38% of the Chinese participants endorsed autism spectrum disorder stigma. The Chinese citizens displayed knowledge deficits primarily in the areas of autism spectrum disorder core symptoms, comorbid intellectual impairment, and prognosis. Sociodemographic factors associated with the Chinese citizen’s misconceptions included gender, ethnicity, social economic factors, among others. These results have important implications for increasing public awareness and promoting community participation for autistic individuals in China.
ASD in China differs considerably from ASD in the West in terms of prevalence estimates, education opportunities and life outcomes of autistic people. The lack of ASD awareness could be a key factor underlying these disparities. We asked 1127 U.S. citizens and 1254 Chinese citizens about their autism knowledge using the Autism Stigma and Knowledge Questionnaire (ASK-Q).The results indicated profoundly different public views about ASD in China compared to the U.S. Specifically, only 57%-65% of the Chinese citizens demonstrated adequate ASD knowledge compared to 86%-91% in the U.S. citizens. Fourteen percent of the U.S. citizens were shown to hold stigma beliefs towards ASD; in comparison, 38% of the Chinese citizens indicated ASD stigma. The Chinese citizens displayed misconceptions about ASD related to symptoms, causes, and possible long-term outcomes. In China but not in the U.S., male citizens and citizens with lower social economic status were more likely to have misconceptions about ASD than others were. The findings of this research can help increase public awareness about ASD and create a more inclusive environment for autistic people in China.
Identifying and providing services for autism spectrum disorder (ASD) have been identified as meaningful global challenges (Khan et al., 2012). The estimated worldwide prevalence of ASD is 1 in 160 children (World Health Organization, https://www.who.int). In the United States, it is estimated that 1 in 59 children are affected by ASD as of 2014 (Baio et al., 2018). However, the number in China has been historically lower, ranging from 1 in 255 (Wang et al., 2018) to 1 in 1205 (Jin et al., 2018). Only recently, a Chinese population study using standardized case identification protocol reported a prevalence estimation comparable to the West (about 1 in 100; Sun et al., 2019). Given research has suggested that prevalence should not differ dramatically across geographical regions (Elsabbagh et al., 2012), it is compelling to explore what underlying factors might contribute to the significant under-diagnosis in a country hosting nearly 20% of world population.
For children with an ASD diagnosis, China also differs considerably from the United States, in terms of providing education opportunities. In China, only 7.23% of autistic children were enrolled in regular classrooms according to a survey of nine Chinese provinces (Xiong & Sun, 2014). According to the Ministry of Education of China, the enrollment rate of compulsory education for children with mental disabilities was only 26.96% as of 2016. In comparison, 91% of autistic children in the United States were enrolled in general education as of 2016, as reported by the National Center for Education Statistics. A national survey conducted in 2007–2008 revealed that about one-third of autistic students in the United States were or had attended college (Shattuck et al., 2012). This proportion is likely to have increased with more of a focus on inclusion and transitional services in the United States.
There are multiple reasons for the disparities between China and the West. It has been suggested that lack of ASD awareness might be a key factor contributing to the under-identification of autistic children in China (Jin et al., 2018; Liu et al., 2016; Pang et al., 2018; Sun, Allison, Matthews, et al., 2013; Sun et al., 2019). Studies in the United States have suggested that lower prevalence estimates and increased diagnosis age in ethnic minority groups were associated with difficulty in obtaining ASD knowledge and accessing services (Magaña et al., 2013; Mandell et al., 2009). A population-based study in northeast China indicated that only 57.8% of caregivers were able to recognize at least three ASD symptoms (Wang et al., 2012). A survey study in southern China (N = 471) reported that 83% of preschool teachers answered over half of the ASD knowledge questions incorrectly (Liu et al., 2016). For example, the majority of the teachers regarded ASD as a psychological condition and believed that with proper intervention, ASD can be outgrown. More than 70% of the teachers could not account an ASD advocacy organization, and more than 60% were unfamiliar with evidence-based practices for ASD (Liu et al., 2016). Autistic children with intellectual disability tend to be less likely to receive an ASD diagnosis in China, which is also considered one of the main reasons for the lower prevalence estimates compared with the West (Sun et al., 2019). Another factor is the significant shortage of qualified mental health facilities and professionals as well as intervention service providers in China (Pang et al., 2018; Sun, Allison, Auyeung et al., 2013). As of 2014, there were only about 300 hospitals that diagnose ASD in China in comparison to the thousands of hospitals and other facilities that provide ASD diagnostic evaluation in the United States (Pang et al., 2018); there are also only 25 board-certified behavior analysts (BCBAs) in Mainland China (Behavior Analyst Certification Board, 2019) in comparison to 16,000 in the United States (Deochand & Fuqua, 2016). Moreover, education has suffered from a long-standing shortage of teachers with ASD knowledge (Huang et al., 2013; Liu et al., 2016). Although inclusive education for autistic students and other mental disabilities is being vigorously promoted, inadequate institutional support persists, including insufficient policies and resource allocation (Huang et al., 2013; McCabe, 2013; Wu Cai Lu Autism Research Institute, 2017).
Misconceptions and stigmatization of ASD can be major barriers to diagnosis, treatment, and education (Mandell et al., 2005). Denial or unwillingness to accept the condition of a child may impede the access to early intervention and diminish prognostic opportunities. Recent surveys show that in China, only 9% of parents who notice child’s atypical early behaviors choose to seek professional help immediately (Sun et al., 2015), whereas about 80% of parents choose to “wait and see” if their child outgrows presenting symptoms (Huang et al., 2013). Lack of scientific understanding about ASD may lead to discrimination and prejudice toward autistic individuals, as well as affiliated stigma experienced by family members. Previous research found three common misconceptions of ASD frequently reported in five major Chinese newspapers (Tang & Bie, 2016). First, ASD was often referred to as a childhood disorder; second, autistic people were often depicted as either patients or savants; third, negative images of autistic people were over-represented with minimal mention of positive depictions. All of these frequently observed misconceptions contribute to the proliferation of ASD stereotypes, such as autistic people being a burden to society. The experience of rejection by society can have detrimental consequences. In 2018, a mother and autistic son in Guangzhou, China died by suicide after the son having an incident with classmate and the mother being verbally attacked by other parents (http://www.bjnews.com.cn/opinion/2019/01/02/535793.html). Increasing public knowledge of ASD is a pressing need to improve the lives of autistic individuals in this country (Khan et al., 2012).
To date, there has been no data available on ASD knowledge among the general public of China, nor examination of personal factors directly associated with misconception and stigma. The Autism Stigma and Knowledge Questionnaire (ASK-Q) is an instrument developed to evaluate ASD knowledge in cross-cultural contexts (Harrison, Bradshaw, et al., 2017). Whereas the original measure development study reported on average across subscales 62% of participants fell in the adequate ASD knowledge range (Harrison, Bradshaw et al., 2017), a recent study reported that over 90% of the participants in a U.S. sample demonstrated adequate ASD knowledge (Stronach et al., 2019). The four subscales of ASK-Q: diagnosis/symptoms, etiology, treatment, and stigma endorsement can provide in-depth information about the knowledge construct of the tested population for increasing education opportunities.
This study aimed to compare public knowledge of ASD among citizens from China and the United States. The United States has been a global leader in the advancement in ASD research and practice. Despite having the largest population and economic growth, China is lagging behind the international community in ASD service provision. Given the disparities between China and the United States in ASD identification and treatment, it is prudent to see whether distinct knowledge gaps between the two countries may be a contributing factor. A comparison with the United States will not only potentially inform the low prevalence estimates, critical shortage of education and service provision, and inadequate advocacy efforts in China, but might also provide novel evidence for cultural differences in ASD knowledge constructs that could generalize to other parts of the developing world. Although the ASK-Q was developed with cross-cultural sensitivity in mind, most of the published validation research relied on samples from the United States (Harrison, Bradshaw et al., 2017; Harrison et al., 2019; Stronach et al., 2019). With the exception of a very small dataset from Mongolia (Harrison et al., 2019), research has yet to verify whether similar psychometric performance of ASK-Q would hold in a distinct cultural and linguistic setting. This study has the following specific aims: (1) translate and adapt the ASK-Q into Chinese and examine the cross-cultural validity within a large Chinese sample, (2) gather information about and compare public perception of ASD in China and the United States, and (3) identify the specific knowledge deficits and sociodemographic factors associated with misconceptions and stigma among the Chinese public.
Methods
Participants
The Chinese sample was obtained using social media platforms (e.g. WeChat and Weibo.com). An online survey was created using Wenjuanxing (https://www.wjx.cn) and posted on the social media. Readers may share the survey link on their own pages and chat groups. Utility of these social media platforms for survey studies has demonstrated high feasibility in China (Mei & Brown, 2018). Participants were restricted to Chinese citizens above the age of 18 years. To include participants from diverse regions and minority groups, residents from historically underrepresented and remote areas (e.g. Tibet) were contacted through social media and asked to share the survey link to the locals. To increase the participation of males, the survey link posts were targeted at male users on a major social media site, Weibo.com, during the data collection. No other recruitment strategies were used. Given that we focused on residents in China, responses from oversea participants were excluded based on their IP addresses. A total of 1254 responses were included for analysis.
The U.S. sample was obtained online via Amazon’s Mechanical Turk (MTurk) following procedures described in Harrison, Bradshaw, et al. (2017) and in-person as described in Stronach et al. (2019) for community participants. Participants were restricted to English-speaking U.S. citizens above the age of 18 years. A total of 1127 participants (817 in-person and 310 online) completed the survey. A subset of the U.S. data (n = 325 participants) is taken from Stronach et al. (2019). Demographic characteristics of the samples are shown in Table 1. Since the concept of race is not officially defined and recognized in the Chinese society (The State Council of China), racial subgrouping was not available for the Chinese sample.
Basic demographic characteristics of the participants.
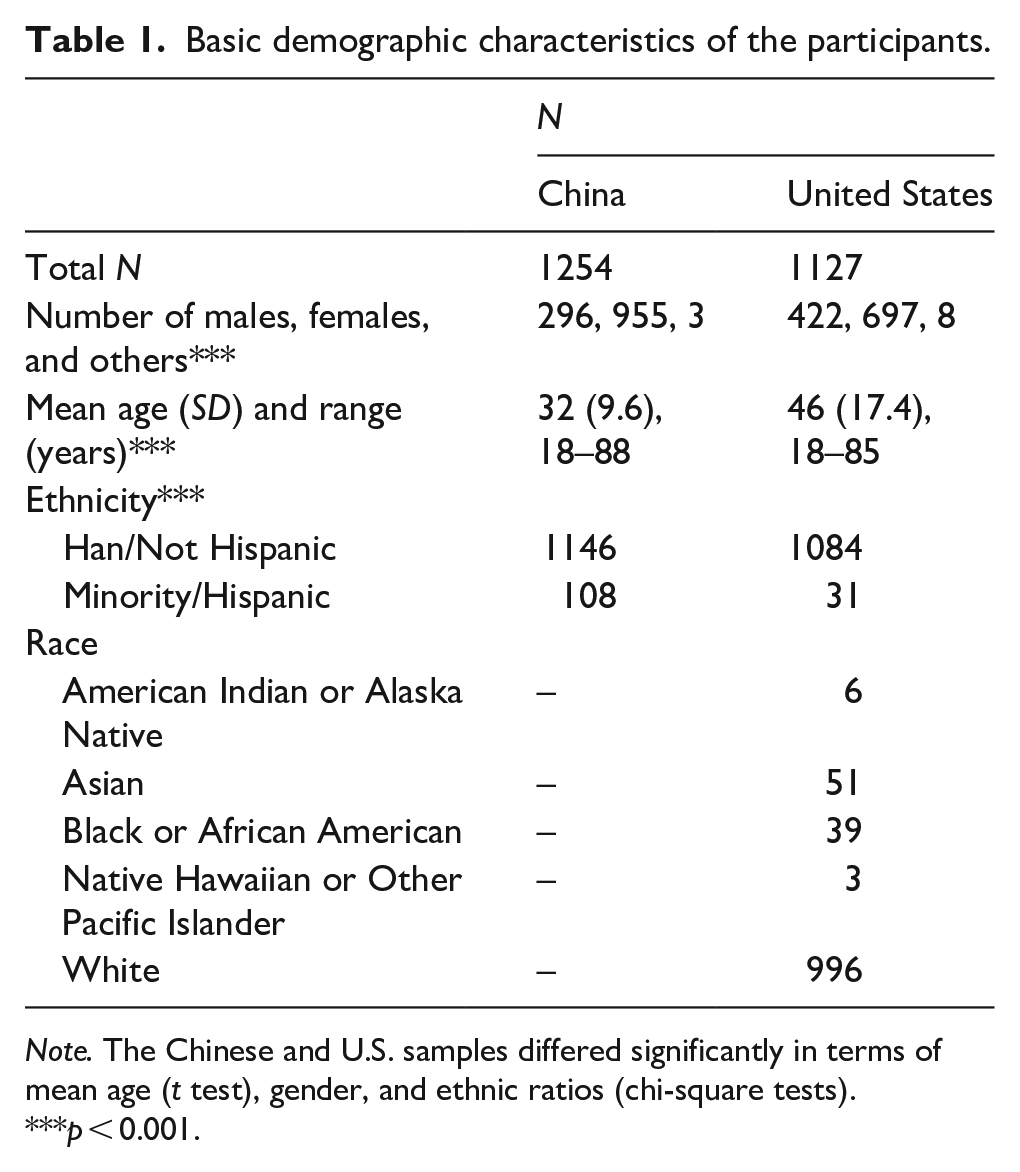
Note. The Chinese and U.S. samples differed significantly in terms of mean age (t test), gender, and ethnic ratios (chi-square tests).
p < 0.001.
Overview of ASK-Q
The ASK-Q is a 49-item questionnaire designed to evaluate ASD knowledge in the categories of diagnosis/symptoms (D/S, 18 items), etiology (ET, 16), and treatment (TR, 14), as well as endorsement of stigma (ST, 7). The items were derived from a comprehensive review of existing ASD knowledge instruments (Harrison, Slane, et al., 2017). Item selection was guided by ratings from a group of multi-cultural researchers to minimize cultural biases (for details, see Harrison, Bradshaw, et al., 2017). Items were reviewed and adapted to ensure the response to each item was either “Agree” or “Disagree.” The original study determined cutoff scores on each subscale using the Diagnostic Classification Model (DCM; Table 3). For example, correct responses on 11 or more items indicates adequate knowledge on D/S, otherwise scores below this threshold indicate inadequate knowledge.
Translation and adaptation of ASK-Q
The Chinese translation of the ASK-Q followed a rigorous translation-back-translation procedure (Guillemin et al., 1993). The 49 items were first translated into Chinese by the first author who is a native Chinese speaker, then back-translated by a Chinese–English bilingual researcher blind to the ASK-Q. The back-translated material was reviewed by a Chinese–English bilingual speech-language pathologist blind to the ASK-Q. The first author then made edits of the Chinese translation accordingly. To examine the cross-cultural validity of the ASK-Q, three bilingual ASD researchers reviewed the Chinese translation following guidelines in Guillemin et al. (1993) for semantic equivalence, idiomatic equivalence, experiential equivalence, and conceptual equivalence. Following recommendations on cultural committee review (i.e. Bracken & Barona, 1991; Guillemin et al., 1993), the three multi-disciplinary reviewers were from distinct parts of China with varying oversea experiences and diverse professional backgrounds. Item acceptance required agreement by all three reviewers that it was easily comprehensible in the Chinese context. Attributable to cross-cultural scrutiny involved in the original development of ASK-Q (Harrison, Bradshaw et al., 2017), little adaptation was suggested by the cultural reviewers except for item number 27—“Autism is the result of a curse or evil eye put upon/inflicted on the family.” The term “evil eye” was substituted by the word “nemesis” (bao4 ying4) to better reflect Chinese stigmatization of mental disorders (Ng, 1997).
Survey procedure
The online survey began with a consent form approved by the local institutional review boards, followed by demographic questions and then the translated ASK-Q. For online surveys, participants were additionally asked their yearly income, occupation category, and self-rank of social economic status (SES). Since the two countries differ in absolute income and occupation prestige ranking, we adjusted the income and occupation items for better alignment across countries. The establishment of income levels was based on data from the National Bureau of Statistics of China (2017) and U.S. Census Bureau (2018). The establishment of occupation prestige levels was based on one study of occupation prestige in Mainland China (Li, 2005) and the well-known Hollingshead (1975) study in the United States. Subjective or self-rank SES was also measured using a method known as the MacArthur ladder scale (Adler et al., 2000). Participants were shown with a ladder image on which the highest rung represents the most well-off people in his or her community and asked to place himself or herself at a relative position on the ladder. Questions such as “Where does your knowledge about autism come from?” and “Do you know someone with autism?” were also included in the survey. The U.S. data were collected during September 2017 to January 2019, and the Chinese data were collected during September 2018 to January 2019.
Data analysis
Parallel analyses were carried out for the Chinese and U.S. samples. The ASK-Q responses were scored as correct or incorrect for each item. To determine the overall knowledge levels of the Chinese and the U.S. citizens, we utilized the Cognitive Diagnosis Model (CDM; Rupp et al., 2010). The same statistical approach was used in the original study to examine measure validity (Harrison, Bradshaw, et al., 2017). CDM models participants’ responses based on the assumption that the tested ability is multi-dimensional. In this case, ASK-Q has four dimensions/subscales, namely D/S, ET, TR, and ST. A Q-matrix is pre-defined to store matrix of skill(s) required to succeed at each item. The CDM thereby produces classifications of participants into dichotomous latent skill classes and allows the prediction of how many individuals in the tested population have adequate knowledge in each dimension. The reliability was measured by the Kuder–Richardson 20 (KR-20) coefficient and the CDM classification consistency.
The CDM does not generate cutoff scores for skill mastery/classification. Here, we followed the approach described in Harrison et al. (2017) and identified the cutoffs such that it produces participant classifications with the highest agreement with the CDM classifications. To provide further verification for these cutoffs, we additionally performed K-means clustering analysis (Hartigan & Wong, 1979). The K-means clustering separated participants into high knowledge and low knowledge clusters such that each participant belonged to the cluster with the nearest mean score. How the clustering “boundaries” and the previously identified cutoffs aligned with each other served as evidence for or against the validity of these cutoffs.
Second, chi-square tests were carried out to examine effects of sociodemographic characteristics on participants’ ASD knowledge adequacy. These characteristics included gender, ethnicity, rural or urban residency, objective SES attributes (education attainment, income, occupation prestige), subjective SES, and parenthood, experience with ASD, and source of ASD knowledge. Finally, correct rate on each item was reported to determine the potential ASD knowledge shortcomings. The CDM analysis was implemented using the R package CDM (George et al., 2016). All data analyses were carried out in R (https://www.r-project.org/).
Results
Comparing mean scores with published ASK-Q data
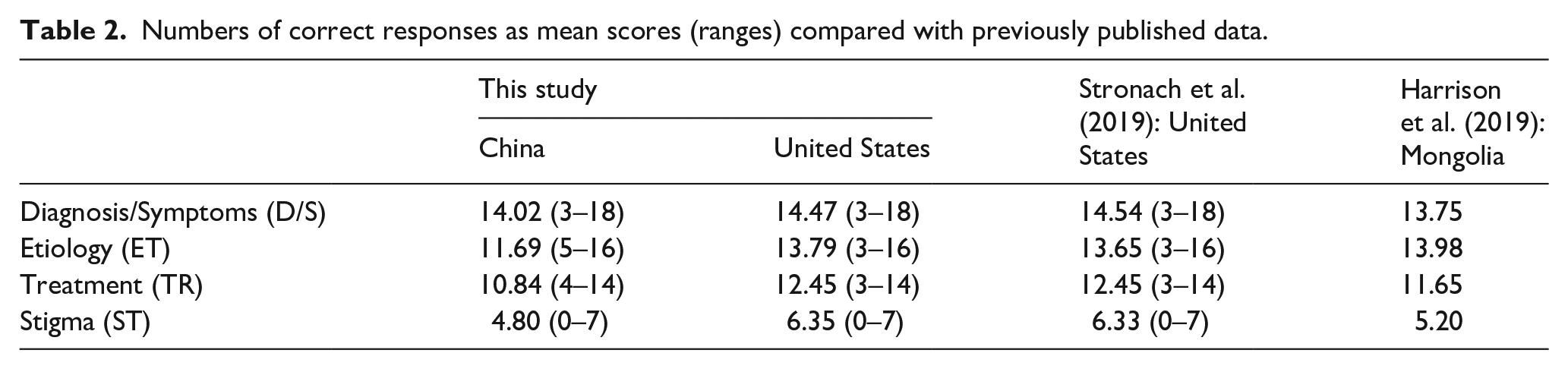
Mean scores on the four ASK-Q subscales are presented in Table 2, along with previous data from a U.S. community sample (N = 478; Stronach et al., 2019) and a Mongolian parent sample (N = 40; Harrison et al., 2019). Judging by the numbers, the current Chinese sample, but not the United States, sample scored consistently lower compared with the published U.S. data on all four subscales.
Numbers of correct responses as mean scores (ranges) compared with previously published data.
The KR-20 coefficient for internal consistency is 0.72 for the Chinese sample and 0.82 for the U.S. sample. The CDM classification consistency measures were 0.91 on D/S, 0.84 on ET, 0.92 on TR, and 0.87 on ST for the Chinese sample. The numbers were 0.95, 0.97, 0.96, and 0.93 for the U.S. sample. These values reveal acceptable to excellent cross-cultural reliability of the ASK-Q.
CDM classifications of participants
Participant classifications produced by the CDM are illustrated in Figure 1. In the Chinese sample, 65% of the participants were classified as having adequate knowledge on the D/S subscale; 61% on the ET subscale; 57% on the TR subscale; and 62% were classified as not endorsing ASD stigma. In the U.S. sample, the percentages were 86% (D/S), 91% (ET), 86% (TR), and 86% (Stigma). The values are interpreted in terms of skill mastery probabilities. For example, 65% of the tested Chinese population and 86% of the tested U.S. population were predicted to have adequate knowledge on ASD diagnosis/symptoms.
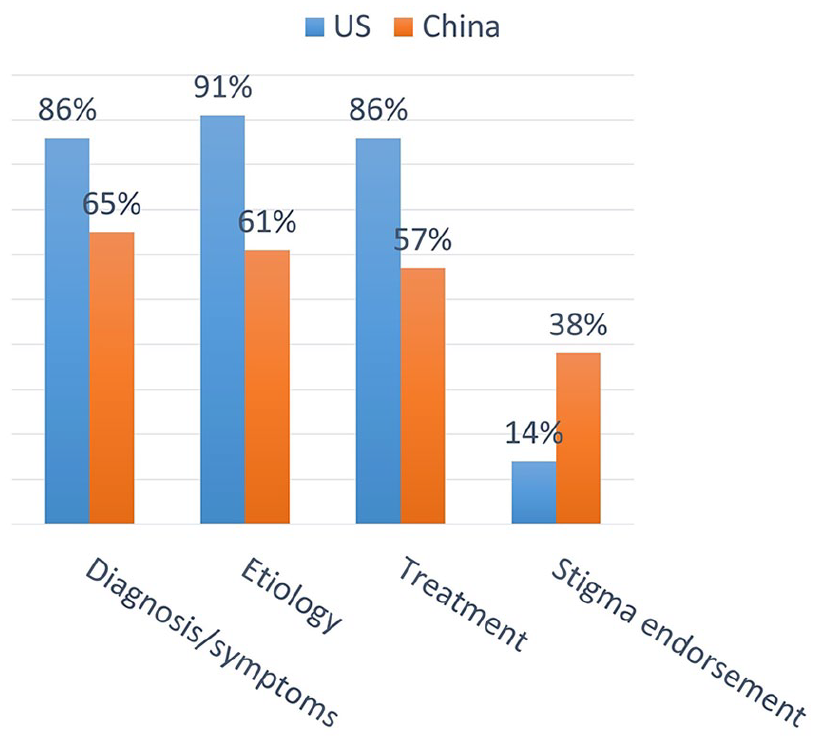
Skill mastery probabilities produced by cognitive diagnosis modeling.
Cutoffs for knowledge adequacy and stigma endorsement
The cutoffs identified in this study along with the cutoffs provided in the original study are presented in Table 3. For the Chinese sample, the cutoffs identified using the CDM approach were 13 for D/S, 10 for ET, 10 for TR, and 4 for ST. The agreements with the CDM classifications were 89.3%, 86.8%, 85%, and 97.9%, respectively. The cutoffs produced by the K-means clustering were 13, 11, 10, and 4.
Cutoff scores in the four subscales identified by CDM approach and K-means clustering approach, in comparison with the original study.
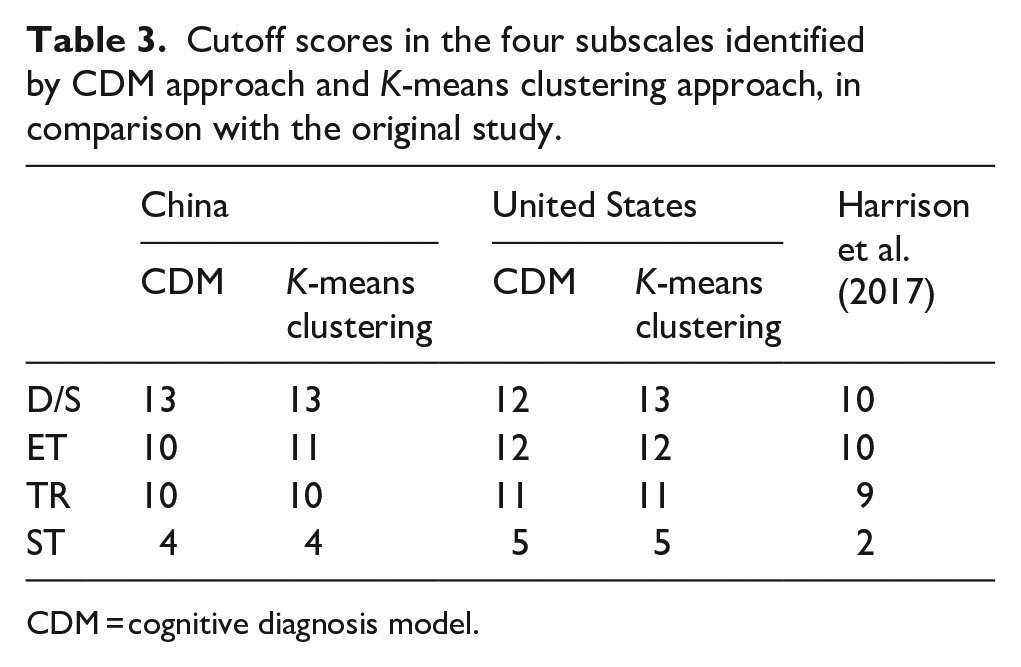
CDM = cognitive diagnosis model.
For the U.S. sample, the cutoffs identified using the CDM approach were 12, 12, 11, and 5. The agreement with the CDM classification were 97.6%, 94.4%, 96%, and 96.8%. The cutoffs provided by K-means clustering were 13, 12, 11, and 5.
The alignment between the two computational approaches observed for both samples further indicates the validity of ASK-Q in discrimination of individuals with adequate knowledge and those without. Nonetheless, these cutoffs appeared to be slightly higher than the original cutoffs of 10 for D/S, 10 for ET, 9 for TR, and 2 for ST in Harrison et al. (2019).
Item response difference between China and the United States
The results in this section are presented to identify knowledge deficits, especially those that the Chinese citizens display. For this purpose, items with difficulty index (Crocker & Algina, 1986) below 0.7 were identified (Table 4). Difficulty index is calculated the same way as percent correct. A smaller difficulty index value indicates that the item is more difficult for and/or unfamiliar to the participants. There are 13 items that met this criterion (range: 0.26–0.7) in the Chinese sample and 5 items in the U.S. sample (0.39–0.61). Table 5 presents items that produced the largest difference between the Chinese and U.S. sample in terms of percent correct. The Chinese sample did consistently poorer on these five items than the U.S. sample did.
Items with difficulty index below 0.7 in the Chinese sample and the U.S. sample.
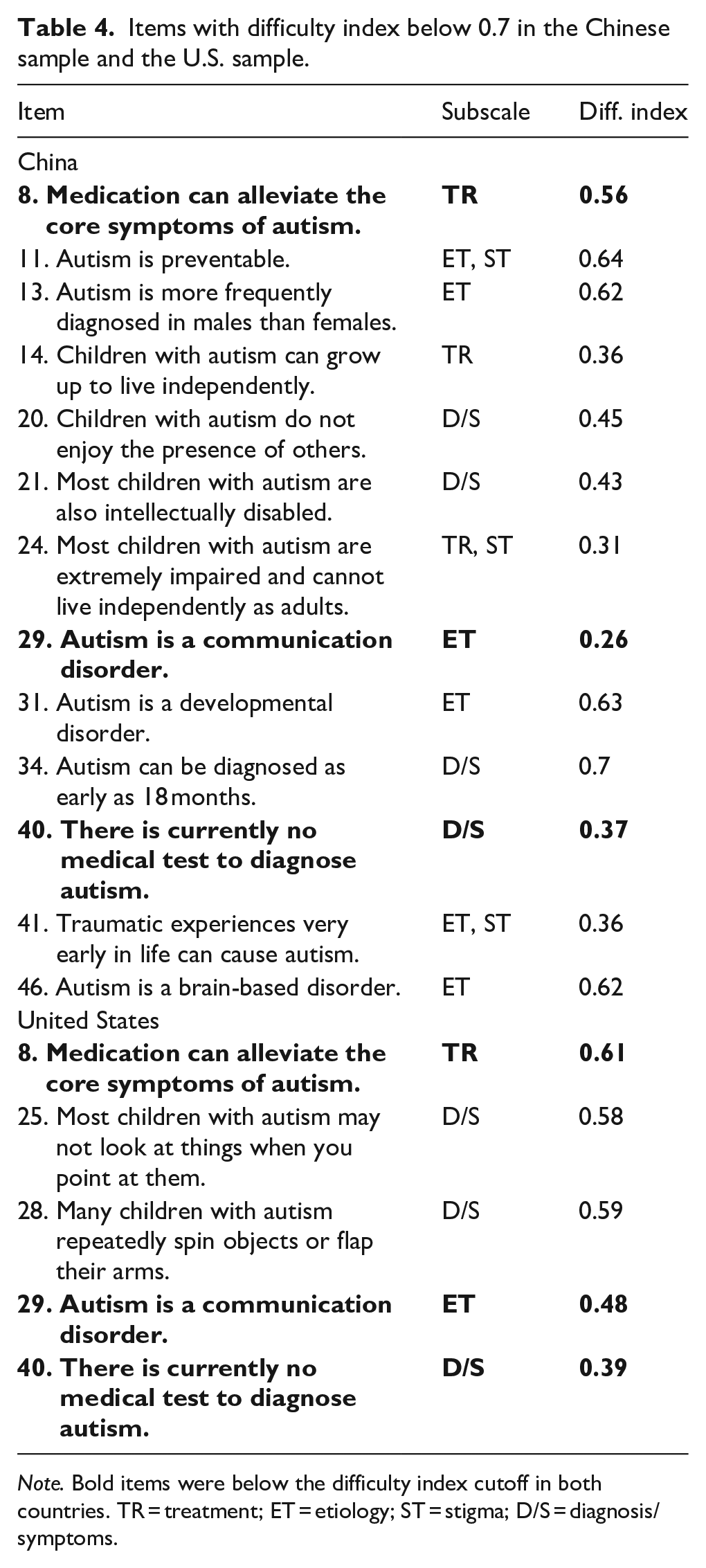
Note. Bold items were below the difficulty index cutoff in both countries. TR = treatment; ET = etiology; ST = stigma; D/S = diagnosis/symptoms.
Five items that most strongly differentiated between China and the United States in terms of correct rate.
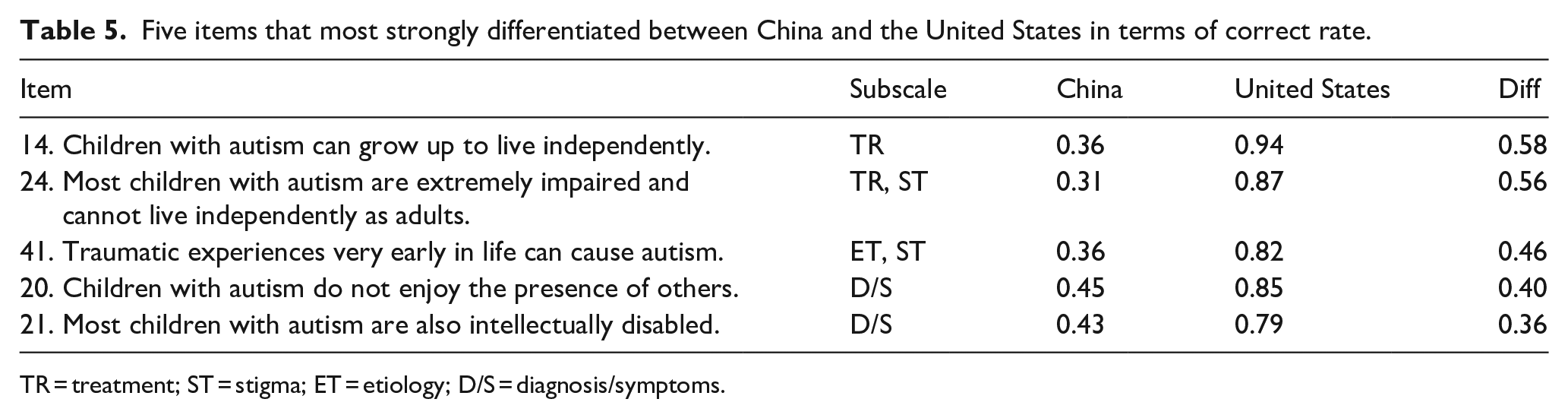
TR = treatment; ST = stigma; ET = etiology; D/S = diagnosis/symptoms.
Factors associated with low knowledge and stigma of ASD
The results of chi-square tests are shown in Tables 6 and 7. In the Chinese sample, more males displayed knowledge inadequacy or misconceptions in D/S (χ2 (1, N = 1251) = 40.77, p < 0.001), ET (χ2 (1, N = 1251) = 9.04, p < 0.01), and TR (χ2 (1, N = 1251) = 26.25, p < 0.001) than females did. In the U.S. sample, gender also played a role but to a lesser extent (D/S, χ2 (1, N = 1119) = 27.72, p < 0.001; ET, χ2 (1, N = 1119) = 7.59, p < 0.01; TR, χ2 (1, N = 1119) = 6.3, p < 0.05). Meanwhile, males in China were more likely to endorse ASD stigma than females (χ2 (1, N = 1251) = 36.93, p < 0.001), whereas in the United States, gender was not associated with stigma endorsement (χ2 (1, N = 1119) = 0.21, p = 0.643). In the Chinese sample, reported ethnic minority was associated with misconceptions and stigma endorsement (D/S, χ2 (1, N = 1254) = 9.94, p < 0.01; ET, χ2 (1, N = 1254) = 6.86, p < 0.01; TR, χ2 (1, N = 1254) = 7.96, p < 0.01; ST, χ2 (1, N = 1254) = 15.44, p < 0.001). In the U.S. sample, there was a similar trend that Hispanic ethnicity was associated with misconceptions although the effect was only significant for TR (χ2 (2, N = 1115) = 9.89, p < 0.01) and not the other subscales. It is worth noting that Hispanic population was underrepresented in this sample, as only 2.7% were reported as Hispanic which was far less than the official figure of 18.1% (U.S. Census Bureau, 2018). The rural residents in China were more likely to have misconceptions about ASD and endorse stigma (D/S, χ2 (1, N = 1254) = 10.2, p < 0.01; ET, χ2 (1, N = 1254) = 12.19, p < 0.001; TR, χ2 (1, N = 1254) = 12.49, p < 0.001; ST, χ2 (1, N = 1254) = 15.56, p < 0.001). This was not the case in the U.S. sample. In fact, the urban residents in the Unites States were more likely to have misconceptions about D/S (χ2 (2, N = 310) = 9.27, p < 0.01) but not the other knowledge domains.
Demographic characteristics and the influence on ASD knowledge adequacy indicated by chi-square test results.
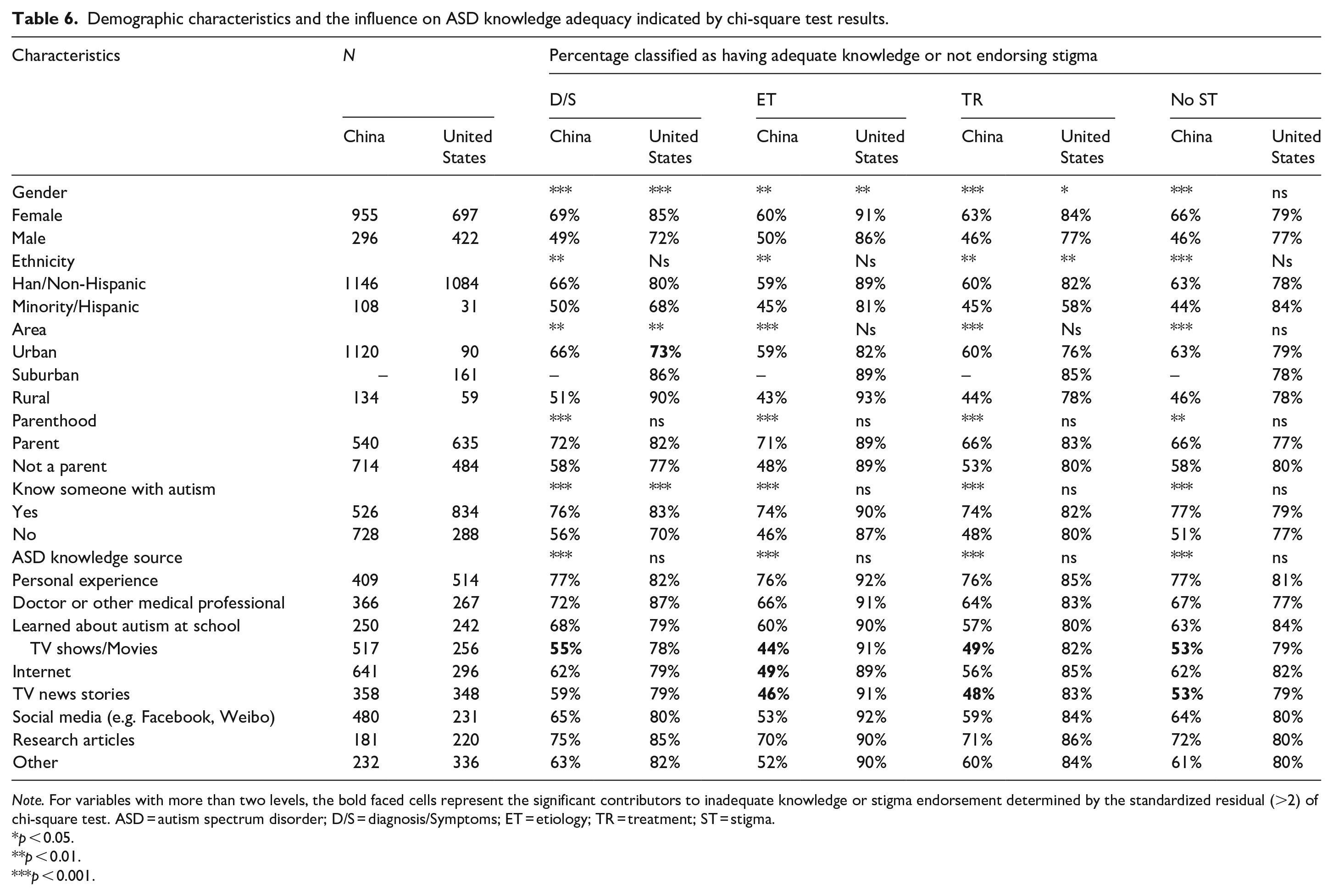
Note. For variables with more than two levels, the bold faced cells represent the significant contributors to inadequate knowledge or stigma endorsement determined by the standardized residual (>2) of chi-square test. ASD = autism spectrum disorder; D/S = diagnosis/Symptoms; ET = etiology; TR = treatment; ST = stigma.
p < 0.05.
p < 0.01.
p < 0.001.
Influence of participants’ SES characteristics on ASD knowledge adequacy indicated by chi-square test results.
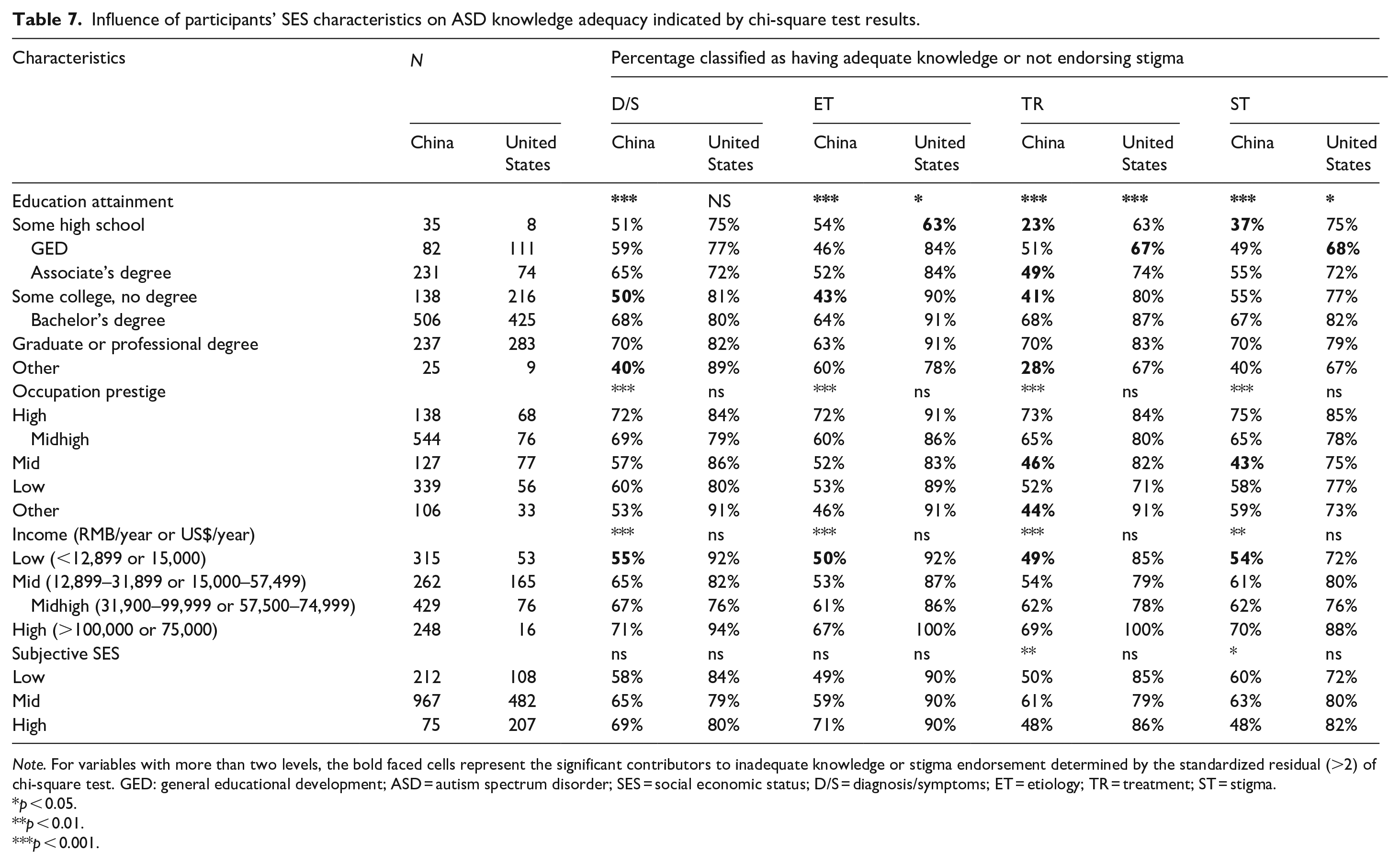
Note. For variables with more than two levels, the bold faced cells represent the significant contributors to inadequate knowledge or stigma endorsement determined by the standardized residual (>2) of chi-square test. GED: general educational development; ASD = autism spectrum disorder; SES = social economic status; D/S = diagnosis/symptoms; ET = etiology; TR = treatment; ST = stigma.
p < 0.05.
p < 0.01.
p < 0.001.
In the Chinese sample but not in the U.S. sample, parenthood was associated with higher ASD knowledge (D/S, χ2 (1, N = 1254) = 26.2, p < 0.001; ET, χ2 (1, N = 1254) = 62.96, p < 0.001; TR, χ2 (1, N = 1254) = 23.64, p < 0.001; ST, χ2 (1, N = 1254) = 7.3, p < 0.01). Similarly, Chinese participants who reported knowing autistic people personally were more likely to have adequate knowledge and not endorse stigma than the Chinese who reported not knowing autistic people (D/S, χ2 (1, N = 1254) = 53.12, p < 0.001; ET, χ2 (1, N = 1254) = 92.04, p < 0.001; TR, χ2 (1, N = 1254) = 86.83, p < 0.001; ST, χ2 (1, N = 1254) = 85.67, p < 0.001). This was not the case for the U.S. sample where knowing autistic people did not elevate one’s knowledge except for on the D/S subscale (χ2 (1, N = 1122) = 23.57, p < 0.001).
Interestingly, in China but not in the United States, the source from which participants reported to obtain ASD knowledge significantly impacted their knowledge adequacy and stigma endorsement (D/S, χ2 (8, N = 3434) = 71.4, p < 0.001; ET, χ2 (8, N = 3434) = 156.8, p < 0.001; TR, χ2 (8, N = 3434) = 104.38, p < 0.001; ST, χ2 (8, N = 3434) = 79.69, p < 0.001). From the standard residual values of the chi-square tests, we were able to identify specific source(s) that substantially contributed to misconceptions and stigma. In particular, TV shows/movies, Internet, and TV news stories were main contributors to misconceptions and stigma endorsement (Figure 2), as compared with personal or professional experience, social media, research articles and other sources.
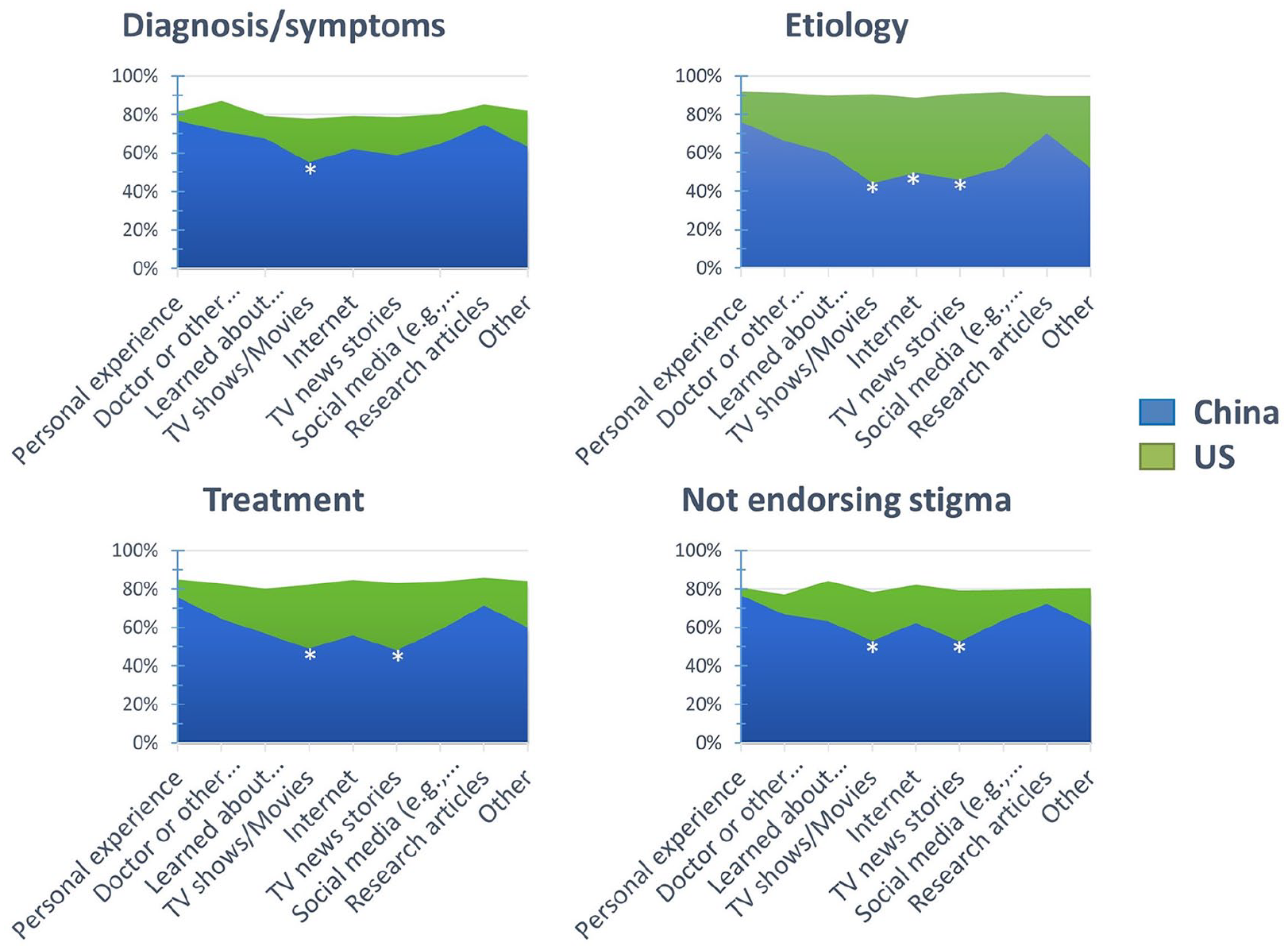
Percentage of people with adequate ASD knowledge as functions of knowledge source and country.
Table 7 displays the effects of SES on ASD knowledge adequacy. Both the objective and subjective SES significantly impacted the Chinese participants’ knowledge, whereas only education attainment impacted the U.S. participants’ knowledge (ET, χ2 (6, N = 1126) = 14.74, p < 0.05; TR (χ2 (6, N = 1126) = 29.89, p < 0.001; ST, χ2 (6, N = 1126) = 13.36, p < 0.05). Generally, the Chinese participants who had high school degrees or went to college without earning degrees were the more likely to have misconceptions than participants with more education (D/S, χ2 (6, N = 1254) = 29.74, p < 0.001; ET, χ2 (6, N = 1254) = 29.47, p < 0.001; TR, χ2 (6, N = 1254) = 87.72, p < 0.001; ST, χ2 (6, N = 1254) = 39.34, p < 0.001; Figure 3). Low yearly income (<12,899 RMB) consistently contributed to the Chinese participants’ misconceptions and stigma (D/S, χ2 (3, N = 1254) = 19.52, p < 0.001; ET, χ2 (3, N = 1254) = 19.85, p < 0.001; TR, χ2 (3, N = 1254) = 27.53, p < 0.001; ST, χ2 (3, N = 1254) = 15.03, p < 0.01). In the U.S. sample, income did not relate to how well a person understood ASD. For the subjective SES measured by the MacAuthor Ladder, the trend suggests that the Chinese participants who ranked themselves high on SES were more likely to endorse ASD stigma (χ2 (2, N = 1254) = 6.9, p < 0.05), which is deviant from patterns seen with objective SES. Self-ranked middle SES was related to the highest knowledge in TR (χ2 (2, N = 1254) = 12.9, p < 0.01).
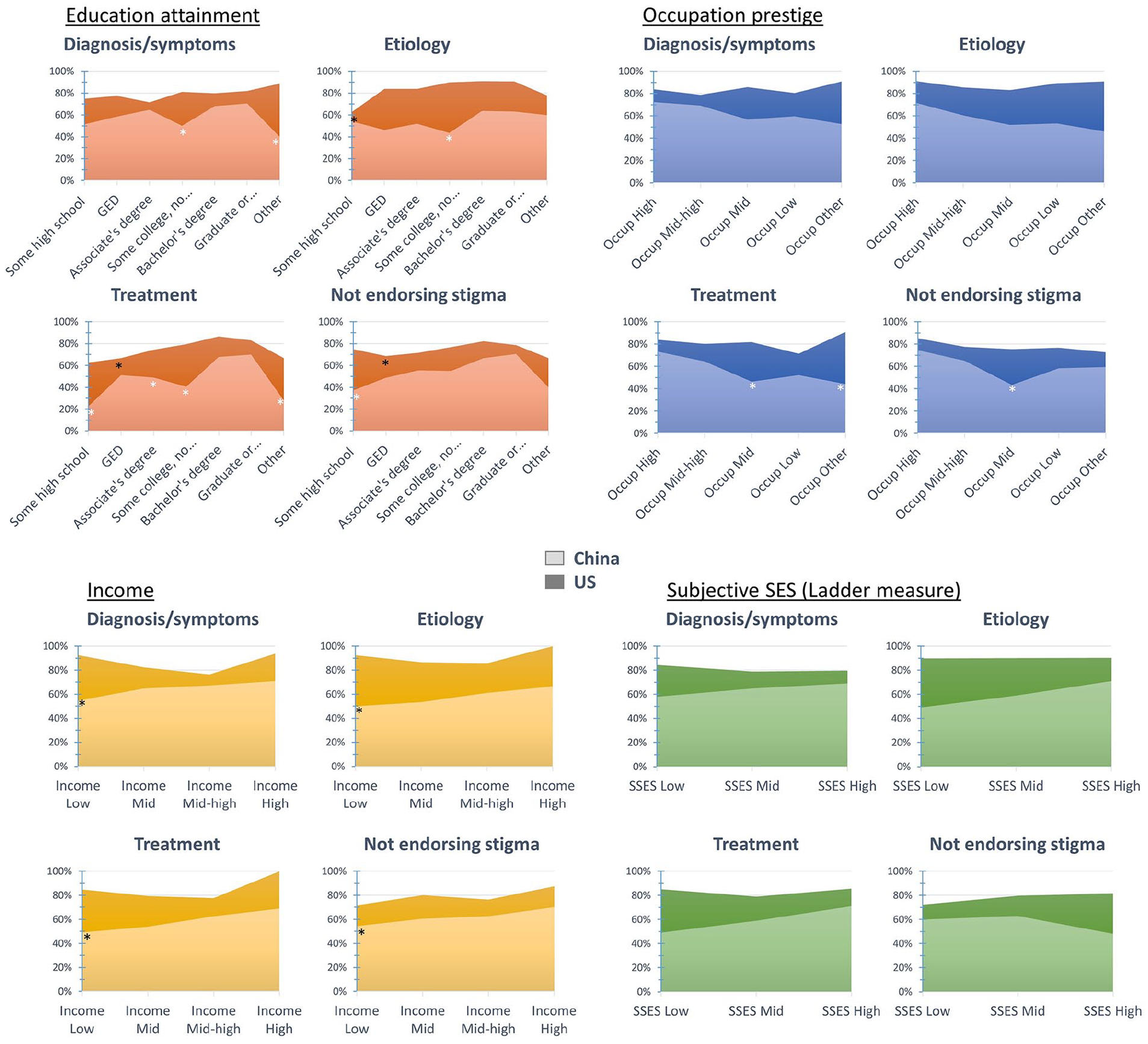
Percentage of people with adequate ASD knowledge as functions of SES factors and country.
Discussion
This study adapted the ASK-Q into Chinese and demonstrated satisfactory psychometric properties in cross-cultural context through the surveying of nation-wide samples in China and the United States. The survey results revealed that the general public in China and in the United States viewed ASD differently, as evidenced by the Chinese sample’s overall lower knowledge and higher stigma endorsement. In accordance with the documented profound disparities in ASD diagnosis, education and service provision existing between China and the West, the current observations highlight specific ASD knowledge deficits that may contribute to these observed disparities. In addition, this study identified specific sociodemographic factors in both countries that relate to ASD knowledge and stigma. Understanding specific cultural differences in knowledge and associated personal factors that relate to knowledge and stigma can aid future efforts to increase public education opportunities in China.
ASD knowledge and stigma in China versus United States
The CDM classification results provide a glimpse of how the two countries differ in the understanding of ASD. The fundamental misunderstandings of ASD among the Chinese citizens were highlighted by the gaps between the two countries. Approximately 90% of the general U.S. citizens had adequate knowledge about ASD in the domains of diagnosis/symptoms, etiology and treatment, which is consistent with previous report of accurate understanding of ASD by U.S. citizens (Mitchell & Locke, 2015). However, for Chinese citizens, this number was only about 60%. In other words, nearly 40% of Chinese citizens were likely to have misconceptions about ASD in various domains. Moreover, 14% of the surveyed U.S. citizens were classified to endorse ASD stigma and for the Chinese citizens this number was nearly 40%. The discrepancies are not surprising given the past data on Chinese educators and caregivers’ ASD knowledge and attitudes (Huang et al., 2013; Liu et al., 2016; Sun et al., 2015; Wang et al., 2012). Our result is a clear evidence that additional funding must be invested not only to mandate professional training but also to educate the public in China.
It is worth noting that the cutoffs for adequate knowledge identified in this study were higher than the cutoffs provided in the original study (Harrison, Bradshaw et al., 2017). The elevated cutoffs were observed for both the Chinese and U.S. samples, indicating that guessing bias is not culturally specific. Unlike the original ASK-Q in which a response choice of “Don’t know” in addition to the dichotomous “Agree/Disagree” was provided, the current ASK-Q uses dichotomous scale. The dichotomous scale likely increased the probability of guessing the correct answer, and thus contributed to the elevated cutoffs. Nonetheless, the successful identification of cutoffs using different analytical approaches, CDM and K-mean clustering, and the alignment of results produced by the two approaches suggest that elevated cutoff does not affect ASK-Q’s effectiveness in the assessment of ASD knowledge cross-culturally.
Specific ASD knowledge deficits among Chinese and U.S. citizens
As indicated in Table 4, the majority of our surveyed Chinese citizens considered ASD to be a communication disorder (item 29, 74%), in contrast to the fact that ASD by definition is a group of complex disorders characterized by symptoms in social communication as well as in restricted and repetitive patterns of behavior (American Psychiatric Association, 2013). That said, this item may warrant consideration in subsequent versions of the ASK-Q due to the fact that “social communication” deficits could easily be mistaken for “communication” impairment. More people in China (55%) than in the United States (15%) seemed to confuse ASD with psychosocial disorders such as social anxiety. A first step for increasing public knowledge could be to help the public understand the differences between ASD and other clinical disorders. Many Chinese participants also believed that ASD was preventable (item 11, 36%) and possibly caused by early traumatic experiences (item 41, 64%). These misconceptions have important implications due to the potential stigmatizing impact low knowledge in these areas could reflect and thus, should be specifically targeted in future interventions to improve knowledge in China. Misconceptions that place potential blame on parents such as these may diminish the likelihood that parents seek important, early help.
The majority of the Chinese participants thought that autistic children were extremely impaired (item 24, 69%), were intellectually disabled (item 21, 57%), and could not live independently as adults (items 14 and 24, 64%), despite the fact that 70% of autistic children do not have intellectual disability (Baio et al., 2018). These three items were also the ones that produced the greatest differences between the Chinese sample and the U.S. sample. Indeed, recent studies following standardized case identification procedures and instruments have estimated similar prevalence in China comparable to the West (Sun et al., 2015, 2019). Notably, in both studies, most of the newly identified ASD cases in mainstream schools had never received ASD diagnoses. The skewed perception of ASD in the Chinese citizens probably reflects the reality of intellectually capable children with ASD being historically overlooked. In other words, the autism spectrum has been artificially “narrowed” by Chinese people to only include individuals with more severe symptoms and intellectual impairment. Another factor, among others, contributing to the skewed knowledge of ASD in China could be that the quality of rehabilitation services is insufficient to lead to systematic positive outcomes. According to the “Report on the Development of China’s Autism Education Rehabilitation Industry” published in 2019 (2019 Report henceforth), there is a serious disconnection between theory and practice in the field of ASD intervention in China (Wu Cai Lu Autism Research Institute, 2019). For example, evidence-based practices that require relatively longer time to show effects are not favored by most intervention providers, whereas non-evidence-based practice, such as sensory intervention, is rated as one of the most effective methods by intervention providers (also see McCabe, 2013). Evidence-based practice such as pivotal response training and social-story-based interventions are less used.
Both Chinese and U.S. citizens responded poorly to item 8. Many of them believed medication can alleviate ASD core symptoms (44%, 39%), despite the fact that so far there is no Food and Drug Administration (FDA)-approved medication to treat ASD core symptoms. The only drugs approved by the FDA for ASD are antipsychotics for alleviating autism-related irritability and aggression, rather than the core symptoms (LeClerc & Easley, 2015). In China, previous surveys of parents of autistic children indicate that some parents hold strong beliefs of promising pharmaceutical treatment in near future and thus feel no current targeted behavioral intervention is needed (Hu et al., 2015). Our findings suggest broad public misunderstanding of pharmaceutical treatment for ASD in China as well as in the United States.
Sociodemographic factors associated with misconceptions and stigma of ASD
By examining sociodemographic factors associated with ASD knowledge, we can help to identify subgroups particularly lacking ASD knowledge and holding stigmatizing beliefs to target in future intervention. All the surveyed sociodemographic factors were significantly related to Chinese participants’ knowledge adequacy and stigma endorsement. These factors included gender, ethnicity, urban versus rural residency, parenthood, familiarity with autistic people, ASD knowledge source, and all SES factors. On the contrary, the U.S. participants across sociodemographic subgroups appeared to have roughly equivalent knowledge about ASD. Such discrepancies suggest a strong cultural and societal influence on people’s understanding and attitudes toward ASD, such that information about ASD is more pervasively spread throughout the U.S. population but is still limited to specific sociodemographic groups in China.
The male Chinese citizens were more likely to stigmatize autism than the female Chinese citizens, whereas gender effect was absent in the U.S. sample. Moreover, the U.S. sample had a larger portion of male participants than the Chinese sample did. Such cross-cultural difference might reflect more persistent traditional gender roles in China compared with the United States. In a society that endorses traditional gender roles, males are often expected to have achievement and success, whereas females are usually expected to care for others (Abele, 2003; Hofstede, 1986). It is possible that Chinese males have lower level of empathy for disadvantaged individuals who are more likely to be underachieving and, as a result, display greater stigmatization toward people with disabilities.
Not knowing autistic people personally and not being a parent contributed to lower knowledge and greater stigma endorsement only in China, but not as much in the United States. This cross-cultural difference provides strong evidence to the essential role advocacy and public education play in elevating ASD awareness (Silverman & Brosco, 2007; Trainor, 2010; Wright & Taylor, 2014). That is, in the United States, experience as a parent and direct experience with autistic people do not relate to ASD knowledge. Again, this could reflect that in China, because legitimate information about ASD might not be reaching the broader masses, people become more aware of ASD when they have personal connections with autistic individuals.
Another factor shaping the Chinese citizens’ ASD knowledge was where the knowledge comes from. Our results identified three major sources related to the Chinese citizens’ misconceptions and stigma, including TV shows/movies, Internet, and TV news stories. In sharp contrast, the U.S. citizens appeared to benefit equally from the different knowledge sources. Compared with the U.S. citizens, the Chinese citizens were much more reliant on TV shows/movies (41% vs 23%), Internet (51% vs 26%), and social media (38% vs 20%). This data mirrors the rocketing Internet usage in China. According to “The 43rd Statistical Report on Internet Development in China,” as of 2018, the country has 829 million Internet users among which 98.6% are mobile Internet users, and the daily hours spent online per person is 3.92 (China Internet Network Information Center, 2019). Although media coverage of ASD has increased substantially over the past decades, our results seem to indicate that the content still needs substantial improvement. The 2019 Report surveyed four major newspapers and presented several useful findings. Among all news topics related to ASD, reports of “public awareness” appears the most frequently, accounting for 57% of the total news, far above topics of “intervention institutes,” “policies, laws and regulations,” and “employment service and pension.” Such reports are mostly short, “soft text” about public welfare activities sponsored by commercial entities, typically published around the Autism Awareness Day and Children’s Day. Although some of these groups and individuals may genuinely care about raising ASD awareness, many of such activities are motivated by commercial purposes such as building public images of charity. In the meantime, the opportunity to acquire ASD knowledge from medical professionals and educators specialized in ASD is very limited (Pang et al., 2018; Sun, Allison, Auyeung et al., 2013).
SES was found to be a significant factor associated with the Chinese citizen’s ASD knowledge and stigma endorsement. Generally, higher SES was associated with higher ASD knowledge and less stigma. Similarly, the rural Chinese residents tended to have lower knowledge and higher stigma than the urban residents did. However, the effect of SES was minimal within the U.S. sample. Chinese rural population was under-represented in the current study given that 42% of China’s population live in rural areas (World Bank, 2017). Nonetheless, the current results are alarming, as the knowledge adequacy in the Chinese sample was likely overestimated by the disproportionally large urban subgroup. Given that the current survey was distributed online and rural Internet users only constitute 26.7% of all Internet users in China (China Internet Network Information Center, 2019), future investigations should use recruitment strategies that are more accessible to rural communities. In addition, we observed that the Chinese citizens who subjectively ranked themselves the highest on SES ladder had the highest stigma, a trend different from the objective SES measures. However, caution should be taken here as only 75 Chinese participants (5.9%) ranked themselves high SES compared with the majority (77%) who ranked themselves mid-SES. It is possible that the 75 participants were not fully representative of high SES citizens, as more people who should be in this subgroup have placed themselves in the mid-subgroup.
Extensive ethnic disparities were found in the Chinese sample. In China, minority is defined as non-Han Chinese (e.g. Tibetan) which comprised 8.49% of its population (http://www.stats.gov.cn). The Minority Chinese had lower knowledge across the board compared with the Han Chinese. This finding is the first evidence to show ethnic differences in ASD-related issues within China. As we further look at the data, this disparity was unlikely driven by the urban–suburban gap because the ratio of rural residents did not differ between the Minority and Han subgroups, but rather a reflection of the SES gap. Specifically, 20% of the Han participants had a graduate or professional degree whereas this percentage in the Minority subgroup was only 9.3%. This finding can be put into the context of widening disparities between Han and Minority Chinese in education, earnings, and occupation over the past three decades (Wu & He, 2016). In the U.S. sample, difference between the Hispanic and non-Hispanic was only found for the Treatment (TR) subscale. Ethnic disparities between Hispanic and non-Hispanic groups in the United States have been frequently documented, including ASD prevalence, age of diagnosis, access to services (Baio et al., 2018; Magaña et al., 2013; Mandell et al., 2009), and symptom presentation (Harrison, Long, et al., 2017; Stronach & Wetherby, 2017). The current result is in line with the finding that compared with non-Hispanic mothers, Hispanic mothers have fewer sources of knowledge after their child diagnosed with ASD, which accumulates to unmet treatment needs (Magaña et al., 2013).
Limitations
This study is not without its limitations. First, the U.S. sample sizes with available occupation and income data were relatively small. Although we did not observe effects of these factors on the U.S. participants’ ASD knowledge, further confirmatory evidence is needed. Second, Chinese rural population and Hispanic-American population were under-represented in the study. Although urbanization in China is rapidly taking place and the ethnic gap is closing in the United States, much more work is needed to serve the historically underrepresented groups. As previously mentioned, diversified recruitment efforts may remediate this issue in future research. In addition, the cross-sectional nature of this study limits our ability to make causal interpretations about how low knowledge and the presence of stigma actually impact early assessment and treatment seeking.
Conclusion
The carefully adapted Chinese ASK-Q performed well psychometrically with a large national sample. The proximity between the Chinese and the U.S. cutoffs for knowledge adequacy provides further verification for ASK-Q as a powerful instrument to evaluate ASD knowledge in cross-cultural context. The general public in China and in the United States demonstrated profoundly different views about ASD. Overall, the Chinese citizens showed substantial misconceptions about ASD in various domains and higher level of stigma endorsement. The study is the first to identify factors associated with ASD misconception and stigma in Chinese citizens, which has important implications for addressing the knowledge gaps and implementing public education campaigns in China.
Footnotes
Acknowledgements
The authors thank Dan Huang, Deyu Wang, and Timothy Huang for their contribution in ASK-Q translation.
Authors’ Note
Sheri Stronach is also affiliated with University of Wisconsin River Falls, USA.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by South China Normal University Young Investigator Research and Development Fund.