
Abstract
The current study examined the role of informal supports in predicting resilience among families of children with autism spectrum disorder. Participants included 153 caregivers of children with autism spectrum disorder, who were between the ages of 2 and 18 years (M = 10.45; SD = 4.32). Caregivers completed a measure of satisfaction with informal supports as well as the Family Resilience Assessment Scale-autism spectrum disorder. After controlling for demographic factors and child behavioural problems, regression analyses revealed that satisfaction with informal supports significantly predicted family resilience. The findings highlight the importance of specifically strengthening informal support networks when providing services and interventions to families of children with autism spectrum disorder to foster the family’s resilience.
Lay abstract
The study of resilience among individuals with disabilities and their families represents a paradigmatic shift from a deficits orientation towards a more holistic and contextualized approach focused on strength and adaptation. The current study investigated whether informal supports could help improve families’ capacity for resilience. We recruited 153 caregivers of children aged between 2 and 18 years who all had a diagnosis of autism. Participants were asked to complete surveys assessing resilience in their families as well as their satisfaction with informal supports (e.g. friends and family). Families more likely to report higher satisfaction with their informal support networks demonstrate greater resilience. The results suggest that informal social supports are a valuable resource for families in strengthening their capacity for resilience. The findings may help inform the development of interventions and services that work collaboratively and innovatively with families and their social networks to provide assistance and support in meaningful and effective ways.
The study of resilience among individuals with disabilities and their families represents a paradigmatic shift from a deficits orientation towards an approach that is more holistic and contextualized, focusing on strength and healthy adaptation. Family resilience is defined as the ‘characteristics, dimensions, and properties which help families to be resistant to disruption in the face of change and adaptive in the face of crisis situations’ (McCubbin & McCubbin, 1988, p. 247). The emerging research in this field has broadened its scope by examining how a child’s environment, comprising their families, peers and communities, can impact developmental outcomes, but can also be modified and structured to meet a child’s individualized needs (Zuna et al., 2010). Furthermore, theoretical foundations advanced by Bronfenbrenner’s (1979) ecological model and Family Systems Theory (Turnbull et al., 1984) have guided empirical studies on resilience and have provided a framework for the development of interventions for children with disabilities and their families (Gardiner & Iarocci, 2012). Bronfenbrenner’s ecological model conceptualizes development as embedded within a tiered context whereby various systems (individual, microsystem, mesosystem, exosystem, macrosystem) exert their influence, and ultimately have a critical impact on overall functioning. Family systems theory considers the specific characteristics of the family, such as sibling relationships, as well as kinship networks beyond the nuclear family, that contribute to risk and resilience (Walsh, 2003, 2006). Incorporating both frameworks in our understanding of family resilience emphasizes the importance of the family unit as an interconnected and dynamic system, offering a more nuanced approach and allowing researchers to explore potentially new avenues for developing interventions and services that better meet families’ needs and enhance already existing strengths.
While there are a growing number of studies examining resilience in the broad disability field, less research has been dedicated to investigating this concept within the autism spectrum disorder (ASD) population. The few exceptions have primarily focused on characteristics related to the caregivers of children with ASD. For example, optimism and caregiver coping style have both been linked to greater resilience among caregivers. In a study by Kayfitz et al. (2010) that comprised 23 mother–father dyads of children with ASD between the ages of 5 and 11 years, researchers investigated the role of optimism on parental well-being and distress. Parents reporting greater optimism and positive experiences with their child were more likely to indicate less stress and better overall well-being. The findings were consistent with those of Ekas et al. (2010), who had a larger sample of 119 mothers of children between the ages of 2 and 18 years. The results revealed a positive relationship between optimism and maternal well-being, positive affect, life satisfaction and psychological well-being. There has also been a focus on the relation between caregiver coping style and resilience. In a sample of 153 mothers of toddlers with ASD, researchers found that higher levels of problem-focused coping, which aims to solve problems or modify sources of distress, was more effective in improving maternal well-being, compared with utilizing emotion-focused coping which aims to reduce the feelings of distress (Smith et al., 2008).
Although these studies have provided insight into factors that may enhance resilience in the ASD population, there is a gap in our knowledge related to outcomes of resilience at the family level. This is not to be confused with the research on the absence of stress and mental health challenges, which has historically been used as a proxy for resilience. This is an important distinction, as resilience encompasses not just the absence of problems, but also evidence of strength whereby families are functioning optimally and thriving despite the presence of adversity in their lives.
A number of exceptions have looked at the role of both formal and informal supports. Formal supports are delivered through organizations or agencies and include educational supports, mental health professionals, respite and behavioural intervention (Boyd, 2002; Bromley et al., 2004; McIntyre & Brown, 2018). In contrast, informal supports comprise a network that may include family, friends and other parents of children with disability in the community (McIntyre & Brown, 2018). The positive impact of both types of support are well-documented for parents of children with ASD (e.g. Barker et al., 2011; Ekas et al., 2010; Gouin et al., 2016; Robinson et al., 2016).
Eskow et al. (2019) assessed the impact of enrolment in state autism waiver programmes on family quality of life. Participants included 230 families of children above the age of 9 years (M = 15.91; SD = 2.85) enrolled in the waiver programme and a matched comparison group comprised 230 families on a waitlist. The results indicated that formal support services (e.g. intensive individual support services and respite) provided through the waiver programme had a positive impact on family quality of life. Examining social supports in 26 mother–father pairs of children aged 3–16 years, Altiere and von Kluge (2008) observed a positive relation between quality of social support and family functioning. Convergent findings were obtained in a larger sample of 78 primary caregivers of children with ASD (M = 57.06 months; SD = 36.31), where Stuart and McGrew (2009) found a protective effect of social support on family well-being in the context of high stress after receiving an ASD diagnosis.
Satisfaction with informal supports may play a crucial role in impacting family resilience in the context of raising a child with ASD. Previous research has demonstrated that satisfaction with informal support networks is a significant predictor of improved physical health (Gallagher & Whiteley, 2012; Lovell et al., 2012) and mental health functioning (Benson & Karlof, 2009; Bromley et al., 2004; Khanna et al., 2011), and has been shown to reduce stress (Renty & Roeyers, 2007; Ruiz et al., 2014). However, despite these findings, numerous studies have reported that families of children with ASD tend to report poorer quality of life and lower levels of social support and friendships (Weiss, 2002). Hodgetts et al. (2015) evaluated service and support needs in 143 parents of children with ASD ranging in age between 2 and 18 years. Analysis of the Family Needs Survey (FNS-R; Bailey & Simeonsson, 1990) revealed that a significant proportion (89%) of caregivers identified family and social support as a priority. This identified need was prioritized more frequently compared with more formal supports, including financial aid and childcare. These findings highlight the importance of further examination into informal supports and its relation to resilience given its potential in buffering negative impacts and promoting adaptive functioning.
To date, there have been no studies that have investigated the role of informal supports on resilience among families of children with ASD using validated resilience measures. The current study used a modified version of the Family Resilience Assessment Scale (FRAS; Sixbey, 2005), the FRAS-ASD (Gardiner et al., 2019). The FRAS has been used in a range of contexts, with families of children with ADHD (Holman, 2014), ASD and other neurodevelopmental disabilities (Leone et al., 2016). It has also been validated cross-culturally in samples from Croatia (Ferić et al., 2016), China (Li et al., 2016), and Poland (Nadrowska et al., 2017). The FRAS-ASD was recently validated as an assessment of resilience among a sample of caregivers of children with ASD (Gardiner et al., 2019). The FRAS-ASD aligns with Walsh’s (1998) three-domain model of resilience, which includes family communication processes, organizational patterns and belief systems. This assessment tool considers outcomes related to the entire family unit to identify areas of strength and/or areas in need of improvement.
While previous studies have examined the role of informal supports on family functioning, these studies have not controlled for important demographic factors and child behavioural problems in the same study. In the current study, regression models accounted for child age, child gender and family income as covariates, as previous research has shown significant relations between these variables and family functioning in the ASD population (Gardiner & Iarocci, 2015; Hsiao, 2018; Hu et al., 2012). Child externalizing behaviours are also important to consider, as they have consistently been shown to significantly impact both caregiver stress (Firth & Dryer, 2013; Khanna et al., 2011; McStay et al., 2014) and family functioning (Pozo et al., 2014).
To address this gap, we examined whether satisfaction with informal supports predicts overall family resilience as well as the various domains of family resilience, controlling for child behaviour problems and demographic factors such as child age, gender and family income. We predicted that satisfaction with informal supports would significantly predict overall family resilience, as well as the various domains of family resilience after controlling for important child and family demographics.
Methods
Participants
Data used for the current analysis originated from a larger mixed methods study. Inclusion criteria specified that study participants must be caregivers of children with an official ASD diagnosis and be fluent in English in order to complete relevant study questionnaires. All participants were caregivers of children with ASD living in British Columbia, Canada. Recruitment flyers and posters were advertised and posted on various social media pages and waiting rooms of community ASD organizations. Participants were also recruited from our laboratory database comprising families of children with ASD who had expressed interest in participating in future research. The final study sample comprised 153 caregivers (mothers, fathers) of children with ASD. All caregivers participated voluntarily in the current study and provided informed consent.
The majority of participants were mothers (80%) and the age range of respondents was between 27 and 64 years (M = 43.85; SD = 6.59). The most frequent family income reported ranged between CA$80,000 and CA$109,999, which is slightly above the national average income of CA$70,366 (Statistics Canada, 2016). Complete demographics information is provided in Table 1.
Family demographic characteristics.
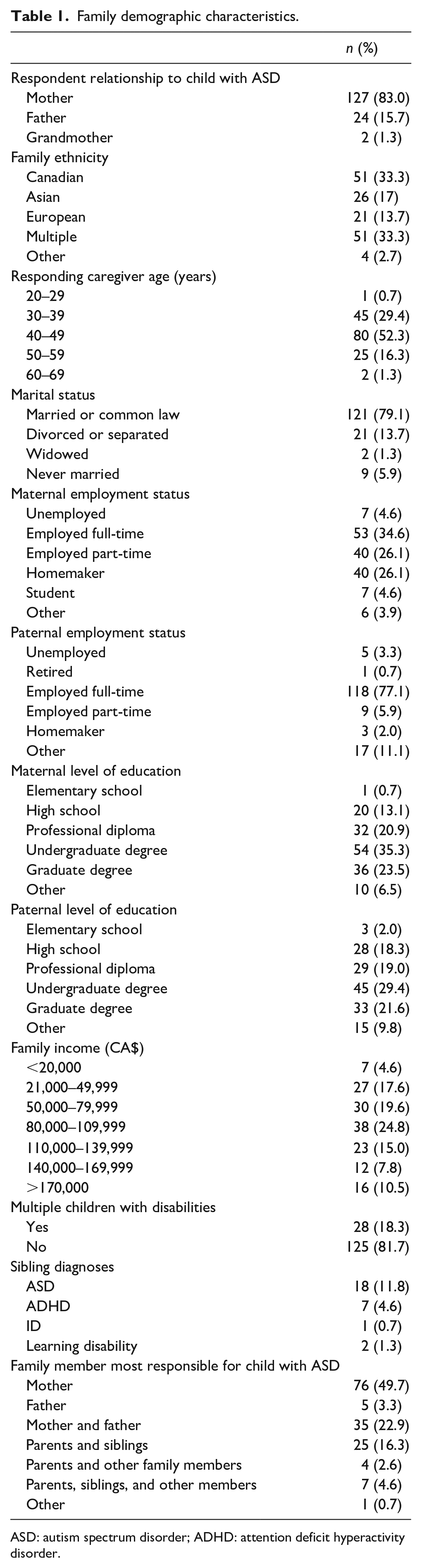
ASD: autism spectrum disorder; ADHD: attention deficit hyperactivity disorder.
The age range of the study child was between 2 and 18 years (M = 10.45; SD = 4.32). Child intellectual functioning, as rated by their caregivers, was negatively skewed with the majority of children being described as ‘Average’. Social ability, based on caregiver reports, was positively skewed with the majority of children described as ‘Low’. This intellectual and social profile is consistent with the diagnostic features of ASD without comorbid intellectual disability (ID) (Gardiner & Iarocci, 2015). Also consistent with previous research, 97.1% of caregivers reported that their child had another comorbid condition aside from ASD (Gillberg & Billstedt, 2000; Posserud et al., 2018). The most commonly reported conditions were anxiety (66.7%), behavioural problems (57.5%), speech/language problems (49.7%) and sensory integration impairment (37.3%). See Table 2 for demographic characteristics.
Demographic characteristics of focal child with ASD.
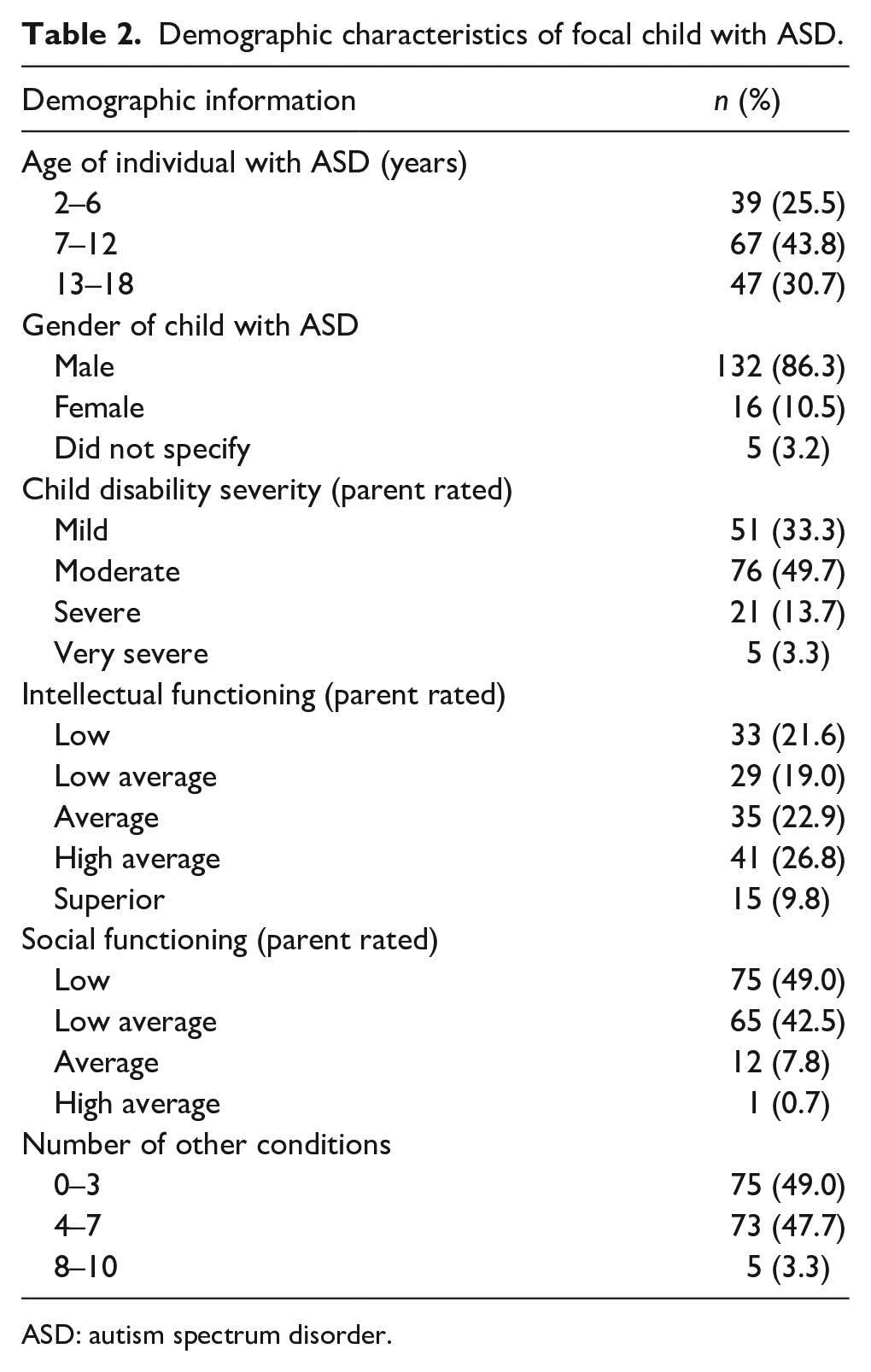
ASD: autism spectrum disorder.
Diagnostic confirmation
The main study child received an official, standardized, clinical diagnosis of ASD from a qualified psychologist, paediatrician or psychiatrist based on provincial government-funded autism assessment standards. The child’s diagnosis was based on the Diagnostic and Statistical Manual of Mental Disorders and confirmed with the Autism Diagnostic Intervention – Revised (ADI-R) and the Autism Diagnostic Observation Schedule (ADOS). The ADI-R and ADOS are both considered as gold standard diagnostic tools. Given that provincial funding programmes are directly dependent on an official ASD diagnosis, British Columbia has instituted standardized diagnostic practices. The children of participants in the current study were diagnosed according to these standardized diagnostic procedures.
Measures
Behaviour problems
The problem behaviour scale (includes 66 items) of the Nisonger Child Behaviour Rating Form – Parent Version (NCBRF; Aman et al., 1996) was used to measure this variable. Caregivers rated child behaviours on a 4-point Likert-type scale with responses ranging from did not occur or was not a problem (0) to occurred a lot or was a severe problem (3). As this measure was only used to control for child behaviour problems in general, as opposed to examining specific types of problem behaviours, a total score was used rather than the individual subscale scores. Total behaviour problems were calculated by summing all 66 items, across eight subscales, of the NCBRF. Possible scores range from 0 to 198, where higher scores indicate greater problem behaviours. This scale was shown to demonstrate good internal consistency (α = 0.93).
Satisfaction with informal supports
The emotional well-being domain, consisting of four items from the Beach Centre Family Quality of Life Scale (FQOL; Hoffman et al., 2006), was used to assess satisfaction with informal supports. Items from this domain included statements such as ‘My family members have friends or others who provide support’. Statements are rated on a 5-point scale where 1 = very dissatisfied, 3 = neither satisfied nor dissatisfied, and 5 = very satisfied. Scores for this scale are calculated by taking the average across domain-relevant items with potential scores ranging from 1 to 5, where higher scores suggest greater satisfaction with informal supports. This scale was found to have good internal consistency (α = 0.90).
Family resilience
The Family Resilience Assessment Scale-ASD (FRAS-ASD; Gardiner et al., 2019) is a validated and adapted version of the FRAS (Sixbey, 2005) and was used to measure resilience as it specifically relates to the ASD population. The FRAS-ASD comprises three subscales: Family Communication and Problem Solving (e.g. ‘our family is flexible to deal with the unexpected’), Utilizing Social and Economic Resources (e.g. ‘we feel secure living in this community’), and Family Spirituality (e.g. ‘we participate in church activities’). Cronbach’s α for the Family Communication and Problem Solving, Utilizing Social and Economic Resources, and Family Spirituality subscales were found to be 0.91, 0.71 and 0.57, respectively. Respondents are asked to rate the extent that each item describes their family based on a 4-point Likert-type scale ranging from strongly disagree (1) to strongly agree (4). Scores for this scale are calculated by taking the average across domain-relevant items. Potential scores on this scale range from 1 to 4, where higher scores indicate greater resilience. The FRAS-ASD total score was found to have an internal consistency of 0.93.
Demographic questions such as family income and disability severity were also included in this measure. Family income comprised seven categories ranging from less than CA$20,000 to more than CA$170,000. Caregivers also rated their child’s disability severity, from mild to very severe, as consistent with previous quality of life and resilience research (Gardiner & Iarocci, 2015; Hu et al., 2012; Wang et al., 2004).
Procedure
Caregivers completed an online survey, which included demographic questions, the NCBRF, measure of satisfaction with informal supports and FRAS-ASD. Hierarchical multiple regressions were conducted with the FRAS-ASD total and subscale scores entered as the dependent variables. Consistent with past research, age, gender and family income were entered in the first block; total problem behaviours were entered in the second block; and satisfaction with informal supports entered in the final block.
Results
Data analysis was conducted using SPSS, Version 24. All data points were converted to z-scores and inspected for significant outliers. All assumptions required to conduct multiple regressions were confirmed with no significant deviations from normality detected. Lack of multicollinearity among the predictor variables was also confirmed (VIF < 10; tolerance > 0.20) (Stevens, 2009). Descriptive statistics for each measure are provided in Table 3 and correlations between the subscales of the FRAS-ASD are provided in Table 4.
Scale descriptive statistics.
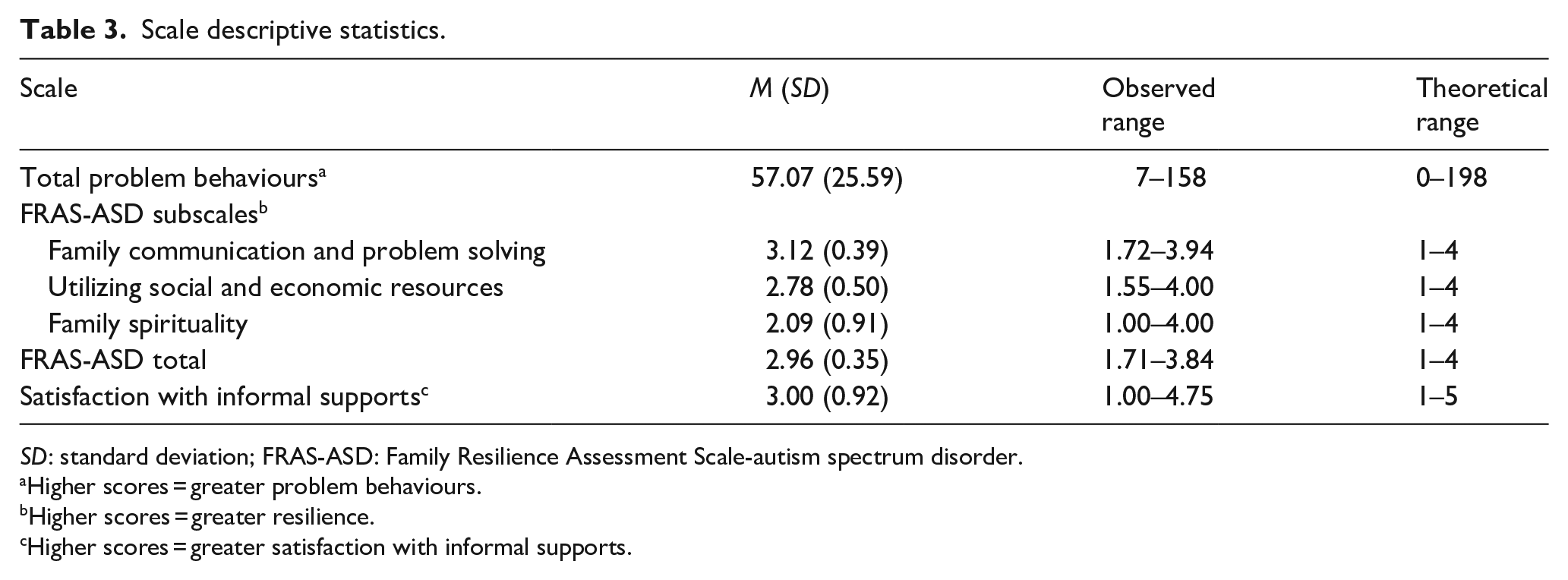
SD: standard deviation; FRAS-ASD: Family Resilience Assessment Scale-autism spectrum disorder.
Higher scores = greater problem behaviours.
Higher scores = greater resilience.
Higher scores = greater satisfaction with informal supports.
FRAS-ASD subscale correlations.
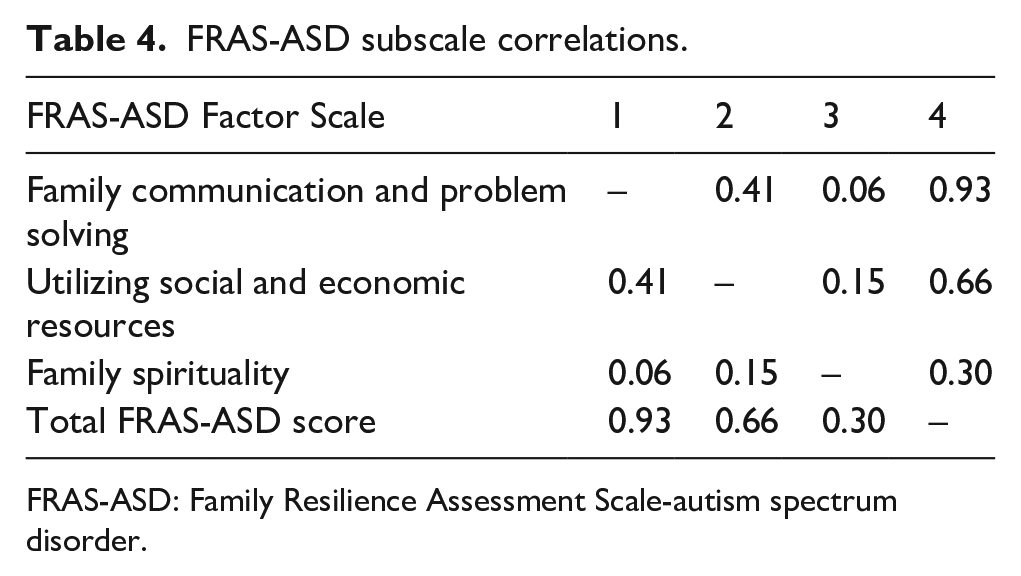
FRAS-ASD: Family Resilience Assessment Scale-autism spectrum disorder.
Hierarchical regression analyses were conducted to determine whether the main predictor variable of interest (e.g. satisfaction with informal supports) could explain a significant amount of variance in family resilience (total and subscales) after controlling for demographic variables such as child age and gender, family income and child behaviour problems.
FRAS-ASD subscale analyses
Family communication and problem solving
The first model, which accounted for child gender and age, and family income, accounted for 2.9% of the variance in Family Communication and Problem Solving (F(3, 143) = 1.41, p = 0.243). The second model, which additionally accounted for total problem behaviours, was significant (R2 = 0.061, F(4, 142) = 2.287, p = 0.063), and accounted for an additional 3.2% of the variance in family resilience above and beyond Model 1 (ΔF(1, 142) = 4.815, p = 0.030). The third model was also statistically significant (R2 = 0.17, F(5, 141) = 5.76, p < 0.001, and the inclusion of satisfaction with informal supports accounted for an additional 10.9% of the variance in the model above and beyond the other predictors (ΔF(1, 141) = 18.54, p = 0.000). The associated regression coefficient for the informal supports variable was significant (p = 0.000). See Table 5 for a summary of the model at each step.
Hierarchical multiple regression analysis predicting family resilience subscales from demographic variables, behaviour problems, and satisfaction with informal supports.
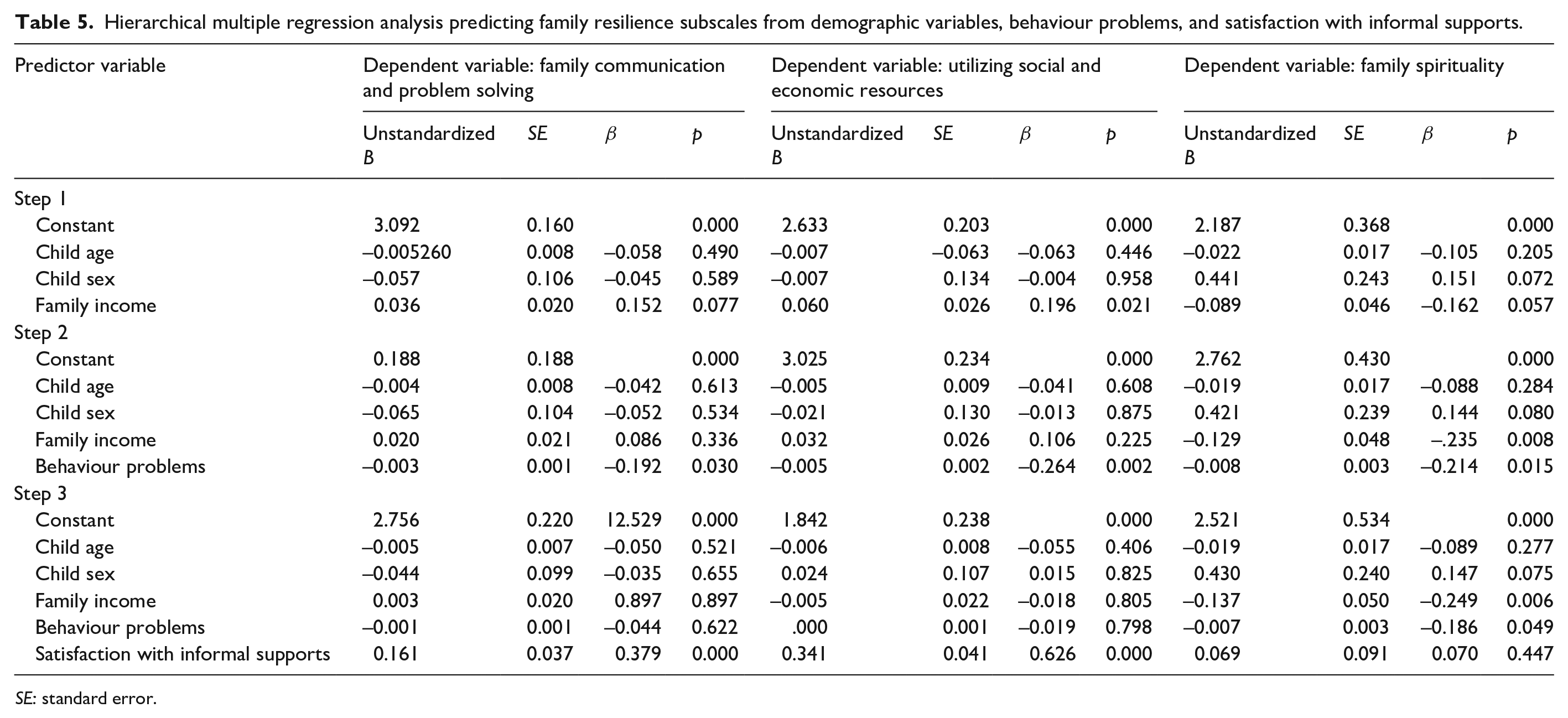
SE: standard error.
Utilizing social and economic resources
The first model, which accounted for demographic factors accounted for 4.6% of the variance in Utilizing Social and Economic Resources (F(3, 143) = 2.30, p = 0.079). The second model, which additionally controlled for total problem behaviours, was significant (R2 = 0.106, F(4, 142) = 4.218, p = 0.003), and accounted for an additional 6% of the variance in family resilience above and beyond Model 1 (ΔF(1, 142) = 9.546, p = 0.002). The third model was also statistically significant (R2 = 0.40, F(5, 141) = 19.15, p = 0.000), and the inclusion of satisfaction with informal supports accounted for an additional 29.8% of the variance in the model above and beyond the other predictors (ΔF(1, 141) = 70.59, p = 0.000). The associated regression coefficient for the informal supports variable was significant (p = 0.000) (see Table 5).
Family spirituality
Controlling for child gender and age, and family income in the first model accounted for 4.6% of the variance in Family Spirituality (F(3, 143) = 2.29, p = 0.081). The second model, which included child problem behaviours, was significant (R2 = 0.085, F(4, 142) = 3.31, p = 0.013), and accounted for an additional 3.9% of the variance in family resilience above and beyond Model 1 (ΔF(1, 142) = 6.12, p = 0.015). The third model was also statistically significant (R2 = 0.089, F(5, 141) = 2.76, p = 0.021), though the inclusion of satisfaction with informal supports did not account for significant additional variance in Family Spirituality above and beyond the other predictors (ΔR2 = 0.00, ΔF(1, 141) = 0.582, p = 0.447). See Table 5 for a summary of the model at each step.
FRAS-ASD scale analysis
The first model, which accounted for child gender and age, and family income, accounted for 3.3% of the variance in family resilience (F(3, 143) = 1.63, p = 0.185). The second model, which additionally accounted for total problem behaviours, was significant (R2 = 0.10, F(4, 142) = 3.91, p < 0.01), and accounted for an additional 6.6% of the variance in family resilience above and beyond Model 1 (ΔF(1, 142) = 10.42, p < 0.01). The third model was also statistically significant (R2 = 0.30, F(5, 141) = 11.80, p < 0.001), and the inclusion of satisfaction with informal supports accounted for an additional 19.6% of the variance in the model above and beyond the other predictors (ΔF(1, 141) = 39.14, p < 0.001). The associated regression coefficient for the informal satisfaction with informal supports variable was significant (p < 0.001). See Table 6 for a summary of the model at each step.
Hierarchical multiple regression analysis predicting family resilience from demographic variables, behaviour problems and satisfaction with informal supports.
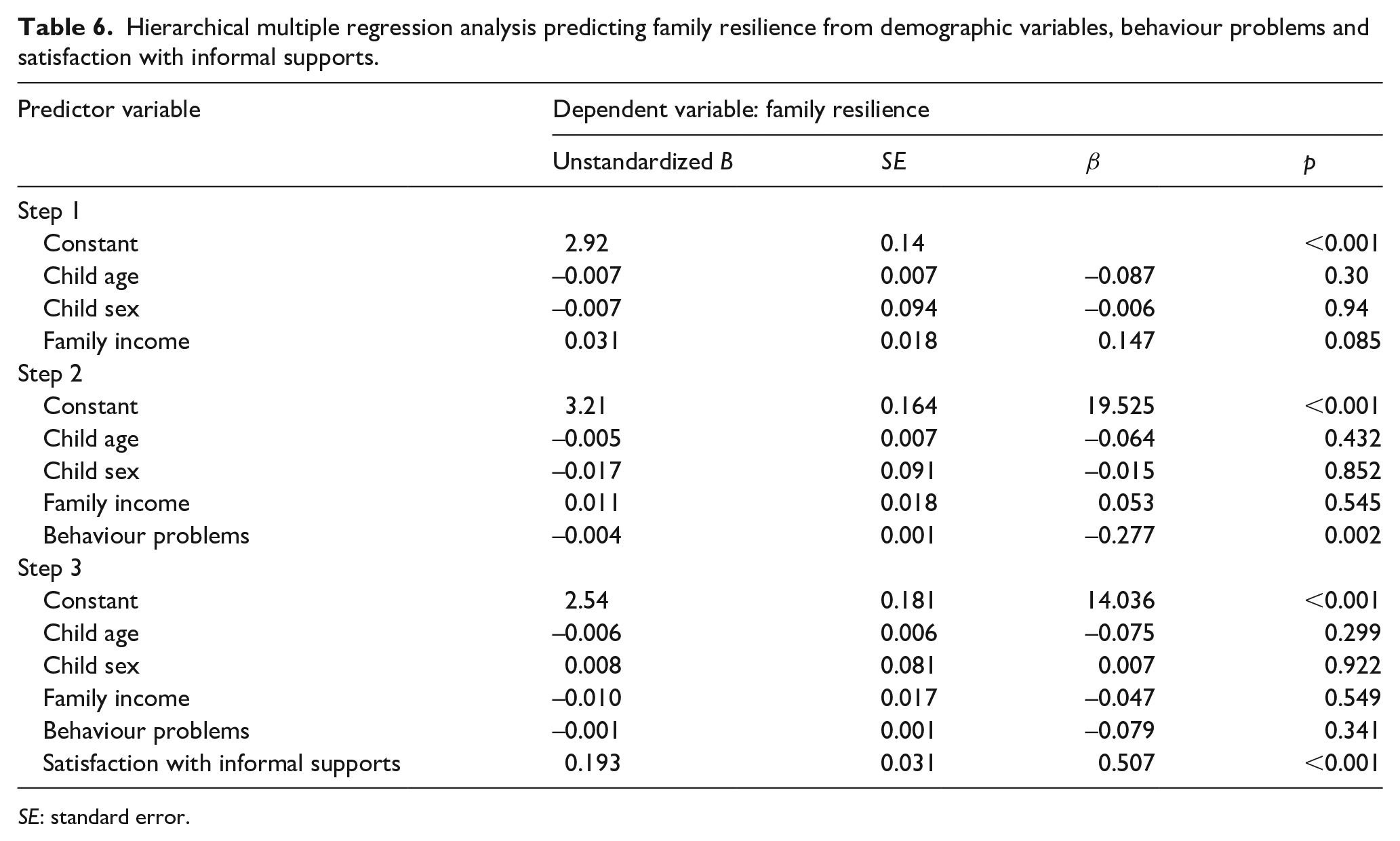
SE: standard error.
Discussion
The purpose of the current investigation was to determine whether satisfaction with informal supports could predict resilience in families of children with ASD. The focus on resilience (rather than the absence of negative outcomes) is important because it emphasizes the family’s potential to adapt and thrive. Having a child with ASD in the family confers risk but can also provide growth fostering opportunities for the family (Altiere & von kluge, 2009; Myers et al., 2009; Sim et al., 2019), especially with adequate and appropriate supports. Our hypothesis that satisfaction with informal supports would significantly predict overall family resilience as well as the various domains of family resilience, after controlling for important demographic factors and child behavioural problems, was partially supported. Satisfaction with informal supports significantly predicted the first two subscales of the FRAS-ASD, specifically Family Communication and Problem Solving and Utilizing Social and Economic Resources, but not Family Spirituality. Overall family resilience, as measured by the total FRAS-ASD score, was also significantly predicted by satisfaction with informal supports.
The present findings are consistent with the growing body of research demonstrating the importance of informal supports for caregiver resilience (Al-Kandari et al., 2017; Ruiz Robledillo et al., 2014), and extend these findings to the construct of ‘family-level’ resilience. We were able to control for important demographic factors and child behavioural problems, providing greater precision and confidence in confirming the relations between satisfaction with informal supports and our outcome of interest.
Social supports are known to exert positive effects on caregivers of children with a range of disabilities (Boyd, 2002; Smith et al., 2012), including those with ASD (Barker et al., 2011; Robinson et al., 2016) but less is known about whether informal supports predict resilience for families of children with ASD. The results of this study confirm that indeed, better informal support networks are associated with greater family resilience for families raising a child with ASD.
Given the research demonstrating heightened levels of stress among families of children with ASD compared with families of children with other developmental disabilities and typically developing children (Davis & Carter, 2008; Hodapp et al., 2003; Kasari & Sigman, 1997), these results are especially relevant. The findings suggest that strengthening informal supports comprised that family and friends may help improve outcomes for families and enhance their overall capacity for resilience. This may be due to the empathy, comfort and companionship that informal supports provide to families, as well as the facilitation of information-sharing, thus allowing families to better adapt to challenging circumstances. In addition, the availability of social supports protects families from experiencing isolation, which is frequently reported in this population and can increase the risk for depression (Gray & Holden, 1992), anxiety (Chan et al., 2018), and distress (Wong et al., 2017). Indeed, this concern was voiced by one parent who participated in the interview portion of the larger study from which these data were drawn: ‘When you have no one that you can talk to about these things . . . that isolates you more . . . your world shrinks dramatically which really does impact the family’ (Gardiner, 2014, p. 90).
Current findings suggest that interventions may be improved by targeting families’ informal support networks. This can be achieved by mobilizing already existing social support networks and informing caregivers of the value that these relationships serve for the entire family. This may be achieved through psychoeducation to families on the dangers of isolation and how maintaining friendships and expanding one’s social network can improve one’s health and well-being. Indeed, there is preliminary research demonstrating that social media, online support, and chat groups may provide access to high quality social support systems and is a convenient and cost-effective option for families especially those who are remote and/or experience mobility challenges (Dam et al., 2017).
To mobilize extended family or other support networks, families may need help with learning how to communicate about ASD to their families, co-workers and friends so as to preserve relationships and potentially important sources of practical support. Clinicians working with families who are struggling with specific issues could help them connect with and share their experiences with other families of children with ASD with similar issues when appropriate. Providing families with access to respite services is another, albeit indirect, way to support families by allowing them more opportunity and time to step outside of their caregiving role to nurture friendships and relationships with significant others.
Limitations
Although the current findings advance our understanding of informal supports and the link to resilience in families of children with ASD, there are a few limitations to acknowledge. The first relates to the reliance on a single informant, in many cases from mothers, who were asked to respond with the whole family in mind, when completing the various measures and scales used in the present study. Future studies including the perspectives of other family members, such as fathers, siblings and individuals with ASD (Burrell et al., 2017) will help to provide greater insight into the relations between the variables examined. However, there is research suggesting moderate to high agreement rates between maternal and paternal reports in this population (Stratis & Lecavalier, 2015; Wang et al., 2006). Another limitation is the cross-sectional design of the current study, whereby causality cannot be determined. It is plausible that rather than informal supports predicting resilience, resilience may help to enhance families’ help-seeking behaviours and strengthen bonds within their informal support networks. Alternatively, another explanation for the current findings may be that informal supports are another dimension of family resilience. In future studies the relation between satisfaction with informal supports and family resilience could be examined longitudinally to confirm the direction and strength of these relations over time. This would also illuminate how different type of supports may be needed at different points in the family’s life cycle. A final issue relates to the conceptual overlap between measures of resilience and informal social supports, as it is possible that families access informal supports through their community and spiritual activities, which the FRAS-ASD addresses. Cross-validation of the current measures should be conducted in future studies to address this concern.
Conclusion
Despite the breadth of research examining social supports in the broad developmental disability literature, this was the first study to examine the link between satisfaction with informal supports and family resilience in the ASD population, controlling for important demographic variables such as age, gender, family income and child behavioural problems. The results suggest that informal social supports are a valuable resource for families in strengthening their capacity for resilience. Research is needed to investigate other characteristics related to informal supports such as the quality, quantity and type available to families. This area of research may help inform the development of interventions and services that recognize and foster the resilience of families nurturing a child with ASD by helping them connect to and strengthen their social networks, in order to provide assistance and support in meaningful and effective ways.
Footnotes
Acknowledgements
The authors would like to thank all of the families for their support and participation in this research.
Author contribution
V.F., E.G., and G.I. conceived the study and participated in its design. V.F. coordinated the manuscript. E.G. conducted all the data collection. V.F. and E.G. performed the statistical analysis. All authors participated in interpretation of the data and helped to draft the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in the current study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funding from the Social Sciences and Humanities Research Council of Canada (SSHRC) and the Canadian Institute of Health Research (CIHR) awarded to Emily Gardiner and a grant from SSHRC and a Michael Smith Foundation for Health Research (MSFHR) Scholar Award to Grace Iarocci.
Informed consent
Informed consent was obtained from all participants included in the study.