
Abstract
This mixed methods analysis examined provider perspectives on barriers and facilitators to parent training use with Medicaid-enrolled clients. Provider survey data were analyzed using hierarchical linear regression models and thematic analysis was used to analyze follow-up interviews with providers. Qualitative themes were developed inductively from interview transcripts without preconceived hypotheses. Barriers and facilitators were identified at the family-, provider-, and organization-level. Family-level barriers were the only barriers to uniquely predict parent training extensiveness (β = −0.27, p = 0.007), which is a composite measure of parent training frequency and quality. No facilitators uniquely predicted extensiveness, but provider skills and professional training experiences marginally predicted extensiveness (ps < 0.06). Five themes regarding barriers to parent training emerged as follows: logistical barriers, limited family engagement/interest, limited agency support/norms, limited professional training, and family stressors/family structures. Four themes about facilitators emerged as follows: logistical facilitators, agency support/norms, high family engagement/interest, and professional training. Recommendations are provided to increase the use of parent training in low-resourced community settings.
Lay abstract
Using quantitative data from an online survey and qualitative data from follow-up interviews with applied behavior analysis providers, researchers examined barriers and facilitators to providing parent training to Medicaid-enrolled youth with autism spectrum disorder. Barriers and facilitators were identified at the family-, provider-, and organization-levels. Family-level barriers were significantly related to less frequent parent training use and poorer quality of use. Two recommendations are provided to increase the use of parent training in low-resourced community settings: (1) provide professional training opportunities to providers about best practices in parent training and (2) increase agency support for parent training, particularly in reducing logistical barriers.
Introduction
Parent 1 training is an evidence-based intervention approach for youth with autism spectrum disorder (ASD; Bearss, Burrell, et al., 2015; Steinbrenner et al., 2020). Parent training is effective for improving social communication, autism symptom severity, challenging behavior, and adaptive skills (Bearss, Johnson, et al., 2015; Nevill et al., 2018; Scahill et al., 2016), and is considered a best practice in the treatment of ASD (National Autism Center, 2015; Wong et al., 2015). Parent training provides benefits for the child and family, including increased hours of intervention throughout the day, skill generalization and maintenance (Koegel et al., 1982), improvements in parent self-efficacy (Karst & Van Hecke, 2012), and reduced parental stress (Iadarola et al., 2018; Ingersoll et al., 2016).
Despite research and best practice guidelines supporting the use of parent training for children with ASD, it is underutilized in community settings (Hume et al., 2005; Straiton et al., 2020; Thomas et al., 2007). This underutilization may be more pronounced for families from traditionally underserved backgrounds (e.g. racial or ethnic minority, language minority, or low socioeconomic status (SES) backgrounds; Straiton et al., 2020), who tend to receive fewer hours of behavioral health services overall (Harrington & Kang, 2008). Indeed, in a recent study, families of children with ASD from lower SES backgrounds were more likely to report parent training as an unmet service need, suggesting service access disparities families of lower-resourced backgrounds (Pickard & Ingersoll, 2016).
Only one study has specifically examined the extent to which parent training is utilized by families of youth with ASD from traditionally underserved backgrounds. Straiton and colleagues (2020) found that 45% of Medicaid-enrolled youth with ASD served in the community mental health (CMH) system in Michigan did not receive a parent training session over the course of a 6-month time period, and those who did received an average of less than one session every other month. Moreover, only 2.7% of youth in the sample received parent training sessions at a frequency consistent with evidence-based parent training models. Given the low rate of parent training for youths with ASD within this system, it is important to consider factors that may influence its use.
Providers’ use of evidence-based practices in parent training is influenced by a number of family-level factors (e.g. perceived appropriateness of the intervention for the client’s presenting problem and the perception that caregivers are unmotivated to participate in treatment), provider-level factors (e.g. knowledge of the intervention and theoretical orientation), and organization-level factors (e.g. availability of supervision regarding the intervention and agency recognition of providers who use the intervention; Sanders et al., 2009; Shapiro et al., 2012). Focusing on provider perspectives is important, as one recent study suggests that only provider-level variables (and not family- or organization-level variables) predicted the use of evidence-based practices in CMH agencies (Beidas et al., 2017). Thus, understanding provider perspectives on the use of parent training for youth with ASD in community settings can provide critical information for community agencies to increase their providers’ use of these practices and improve clients’ quality of care.
Most studies that have examined barriers and/or facilitators to parent training use for youth with ASD refer to a specific program (e.g. Chlebowski et al., 2020; Pickard et al., 2016). For example, Pickard and colleagues (2016) identified barriers within the Medicaid system related to the delivery of Project ImPACT, a parent training program focused on social communication development. Less work has focused on providers’ perceptions of barriers to parent training with youth with ASD more generally. What has been done suggests that providers’ perceptions of barriers at the family-, provider-, and organizational-level all influence their use of parent training. For example, Ingersoll and colleagues (2020) surveyed applied behavior analysis (ABA) providers regarding their prior professional training experiences and their use of parent training practices for with youth with ASD. Providers’ ratings of family-, provider-, and organization-level barriers partially mediated the relationship between the number of professional training experiences and parent training use, suggesting the importance of providers’ perceptions of these barriers in their use of parent training. However, as this study focused on ABA services across settings it is not clear to what extent these same barriers are endorsed by providers who work in low-resourced settings specifically. In addition, no studies to our knowledge have examined facilitators to parent training for youth with ASD; only barriers have been identified thus far. Facilitators are important to identify so that policymakers can prioritize means of support to enable the successful implementation of parent training programs for youth with ASD in community settings.
Parent training in the Michigan Medicaid Autism Benefit
In 2012, the State of Michigan authorized a Medicaid Autism Benefit for Behavioral Health Treatment to fund intensive ABA for Medicaid-enrolled youth with ASD under the age of 21 years served by the state’s CMH system. Medicaid-enrolled youth with ASD can also receive additional services (e.g. psychotherapy and case management) through CMH in addition to these ABA services covered by the Medicaid Autism Benefit. Medicaid eligibility in Michigan requires a household income cutoff that is at or below 133% of the federal poverty level; thus, families served by the Michigan Medicaid Autism Benefit are from lower-income backgrounds.
Working within the system of CMH agencies in Michigan is an ideal environment for studying the use of parent training for children with ASD from underserved backgrounds. While other service systems can be accessed by youth with ASD of lower-income backgrounds in Michigan, such as the early intervention system (0–3 years old) or special education system (3–21 years old), CMH agencies in Michigan have been the primary mechanism for ABA service delivery for youth served by Medicaid.
Present study
This study utilized a subset of data from a community-partnered research project examining parent training practices for youth with ASD by ABA providers in the CMH system in Michigan. One investigation from the project has already been published (Straiton et al., 2020). As described earlier, that study documented low frequency of parent training use for youth with ASD in the Medicaid Autism Benefit. In addition, providers infrequently defined parent training in ways that were consistent with best practices, frequently mentioning psychoeducation and treatment management as opposed to evidence-based strategies such as instruction of a new technique, modeling the technique, and providing time for parent practice with provider feedback (Straiton et al., 2020). Given that providers are infrequently providing parent training and are likely unaware of evidence-based components of parent training that are associated with improved child outcomes (such as modeling and parent practice with feedback; Ruppert et al., 2016; Wyatt Kaminski et al., 2008), efforts to increase the implementation of these interventions in community settings should commence. However, prior to selecting any implementation strategies to increase parent training use in community settings, it is important to unpack provider perspectives on barriers and facilitators to parent training use within CMH systems and ensure that implementation efforts directly address factors that are prioritized by end users. The aim of this study is to leverage quantitative data (barrier and facilitator scales) and qualitative data (interviews) from this same sample to elucidate the provider perspective on parent training within their system.
Methods
Methodological approach
The present mixed methods analysis utilized a convergent design with an equal emphasis on quantitative and qualitative data (QUAN + QUAL; as described in Palinkas et al., 2011). Information was gathered through an online survey and semi-structured follow-up interviews. Quantitative methods provided information about the relationship between parent training extensiveness (a composite measure of frequency and quality) and perceived barriers and facilitators, while qualitative methods provided deeper insight into providers’ experiences. In this study, we integrate mixed methods findings in a narrative discussion in the “Results” section, where we provide all results and describe how they are similar and dissimilar (Creswell & Clark, 2017, p. 226).
Participants
Participants were recruited by three administrators who oversaw ABA services within CMH agencies in three regions of Michigan. These administrators either sent a recruitment email to their providers or provided the research team with provider email addresses (n = 294). Participants had to be eligible to bill for ABA services within the Medicaid Autism Benefit, which required certification as a Board Certified Behavior Analyst (BCBA), certification as a Board Certified Assistant Behavior Analyst (BCaBA), or a Qualified Behavioral Health Professional (QBHP) who had a master’s-level degree and extensive coursework in ABA. Participants also needed to have at least one client on their CMH caseload who was: (1) diagnosed with ASD; (2) under the age of 21 years; and (3) enrolled in the Medicaid Autism Benefit. All participants received a US $5 gift card for participation in the survey. Follow-up interviews were offered to all participants. Those who opted to complete an interview received an additional US $20 gift card. Providers worked with at least one client enrolled in the Medicaid Autism Benefit. Medicaid billing claims for 1028 youth in the Medicaid Autism Benefit from one region of Michigan indicated that youth had a mean age of 7.56 years old (range = 1–20), were predominantly male (79.5%), White (70.7%), Black (12%), or multiracial (12.5%) and were 10.7% Hispanic/Latino (Straiton et al., in press). Rurality, family structure, and language spoken at home are not possible to determine at the client level, as claims data did not include that information. All youth enrolled in the Medicaid Autism Benefit have a household income that is at or below 133% of the federal poverty level.
The present mixed methods analysis utilized the same sample of 97 providers from the Straiton et al. (2020) study. One hundred and fifty-five ABA providers responded to the survey, which included survey branching logic to screen out providers who were ineligible to bill for the Medicaid Autism Benefit. One hundred and two providers provided complete data. Upon inspecting the data, the research team determined that five providers were not eligible to bill for the Medicaid Autism Benefit even though they had taken the survey; therefore, they were removed from the sample. The final sample thus had 97 ABA providers. Participants were primarily BCBAs (59.8%) or QBHPs (26.8%) and were predominantly White (87%), non-Hispanic (97%), and women (81%). It was not possible to calculate the exact response rate since it is possible that other providers were forwarded the link from the recruitment emails; however, the upper bound of the response rate was 33% (97 out of 294 emails sent). Most providers worked with school-aged children (51.5%) as opposed to children 3–5 years old (33%) or older than 10 years old (15.5%), and none worked with children under 3 years old. Most providers held a caseload of 7–12 clients with ASD (51.5%). To participate, providers had to have at least one client in the Medicaid Autism Benefit. Most providers had 7–12 clients in the Medicaid Autism Benefit (44.3%) or 1–6 clients in the Medicaid Autism Benefit (34%) and spent an average of 11–20 h per week working specifically with clients in the Medicaid Autism Benefit (33%), although there was a range from 1–10 h per week (24.7%) to 40+ h per week (5.2%). A subset of 13 providers (13% of the sample) opted to complete a follow-up interview. Providers who completed the interview were comparable to those who completed the survey. Table 1 presents the ABA provider demographic information.
Provider demographic information.
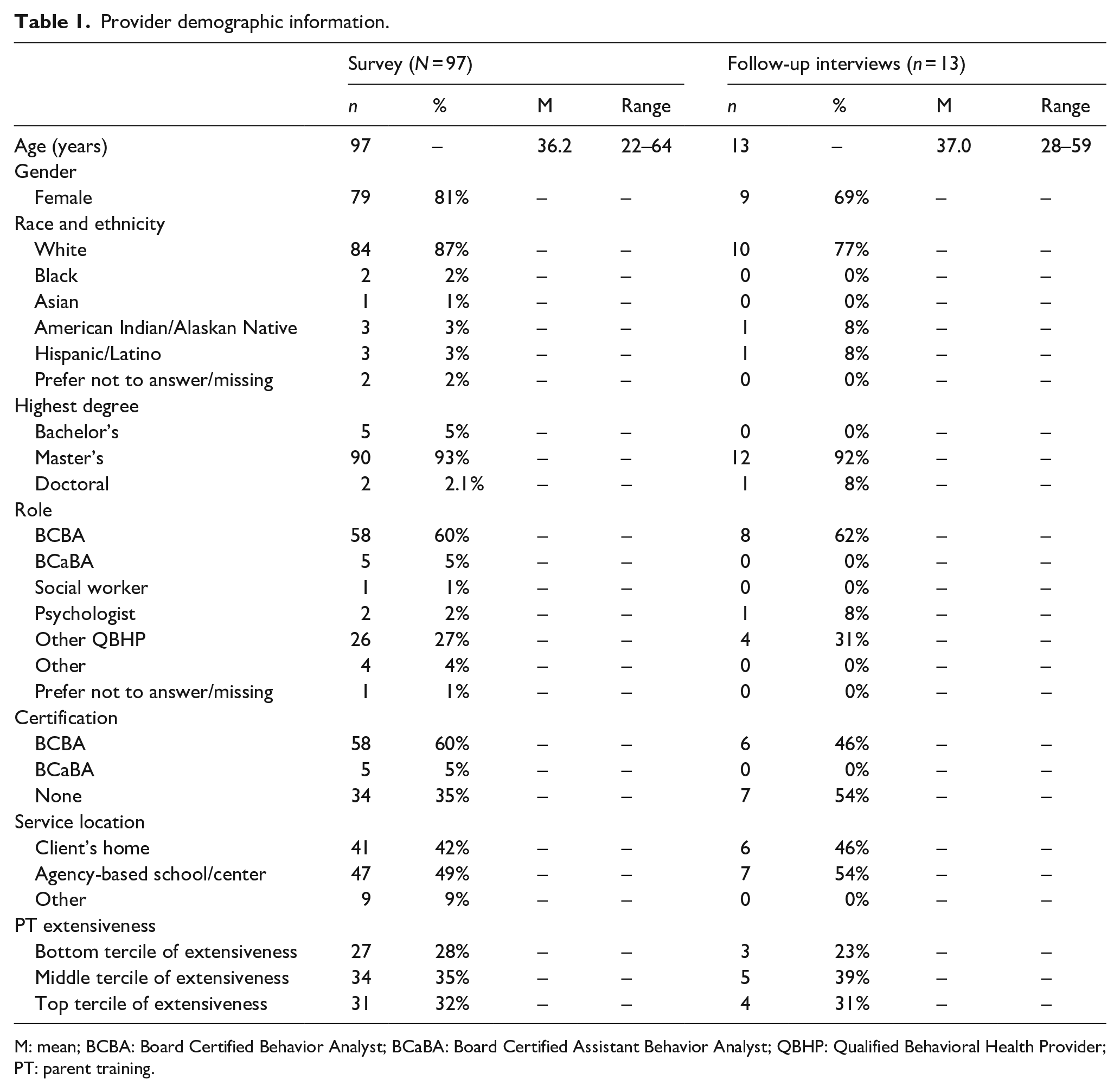
M: mean; BCBA: Board Certified Behavior Analyst; BCaBA: Board Certified Assistant Behavior Analyst; QBHP: Qualified Behavioral Health Provider; PT: parent training.
Measures
Provider survey
A pilot survey was emailed to 34 agency leaders who supervise ASD services within one region in the state. Twenty-one agency leaders (62%) provided feedback on survey language and formatting, which was incorporated into the final survey.
ABA provider demographic information
Providers reported their gender, age, race and ethnicity, educational attainment, disciplinary background, professional role, professional certifications, employment setting (CMH agency, contracted agency, or private practice), caseload, hours of overall service provision within the Medicaid Autism Benefit, years of experience working with clients with ASD and using parent training, and number of professional training experiences they had related to parent training (see Ingersoll et al., 2020).
Parent training extensiveness
In order to create a measure of parent training use that accounts for both the frequency of use as well as the quality of parent training practices delivered, a composite measure of “parent training extensiveness” was created. Providers used a five-point Likert-type scale to rate the frequency and quality of their parent training practices. Frequency was measured by the number of parent training sessions delivered to a typical client (no encounters per month (1); 1–2 encounters per month (2); 3–4 encounters per month (3); 5–8 encounters per month (4); and more than 8 encounters per month (5)). Quality was measured by ratings of how often they used seven evidence-based parent training strategies (see Barton & Fettig, 2013) with a typical client (not at all (1) and very much (5)). Ratings for each strategy were averaged to produce a measure of the overall quality of parent training. Parent training extensiveness was calculated by z-scoring the values for both the frequency and quality measures and summing the z-scores.
Barriers to parent training use
Providers rated 11 common barriers to their use of parent training on a five-point Likert-type scale (strongly disagree (1) and strongly agree (5)). Items were adapted from a barrier scale developed for the Triple P parenting program (Shapiro et al., 2012), with subscales determined using exploratory factor analysis (Ingersoll et al., 2020). Internal consistency for the family- (α = 0.68), provider- (α = 0.82), and organization-level (α = 0.82) subscales in this sample were adequate to strong.
Facilitators to parent training use
Providers rated 10 common facilitators to their use of parent training on a five-point Likert-type scale (strongly disagree (1) and strongly agree (5)). The scale included items adapted from the facilitator scale used by the Triple P program (Shapiro et al., 2012), the Implementation Climate Scale (Ehrhart et al., 2014), and variables from the Theory of Planned Behavior (Ajzen, 1985). The facilitator scale was co-developed by the research team and an administrator from one of the regional CMH authorities from which data were collected. Items were selected and adapted from the three scales listed above based on feedback from the community partner. The scale included family-, provider-, and organizational-level facilitators from each of the three measures. Item content is presented in Table 4. The family-level facilitator subscale (α = 0.79) and organization-level facilitator subscale (α = 0.82) had good internal consistency. The provider-level facilitator subscale had poor internal consistency (α = 0.55); thus, the individual items were entered in analyses as opposed to the subscale.
Provider interviews
Interviews were conducted in a semi-structured format that covered four topic areas: (1) content and structure of parent training sessions; (2) barriers and facilitators; (3) billing practices for parent training sessions; and (4) training experiences related to using parent training. The interview guide was created based on discussions with community partners who supervise ABA services within the Medicaid Autism Benefit and a cursory literature review of provider perspectives on barriers and facilitators to the use of evidence-based practices in community settings (Aarons, 2005; Sanders et al., 2009; Shapiro et al., 2012; Stahmer et al., 2019).
Data analysis
Quantitative analysis
Descriptive statistics were used to examine providers’ endorsement of barriers and facilitators of parent training use. Bivariate relationships between parent training extensiveness, provider demographic information, and each of the barriers and facilitators were examined using Pearson’s correlations, Spearman’s rho, and one-way analysis of variance (ANOVA) as appropriate.
A hierarchical regression examined whether family-, provider-, and organizational-level barriers predicted parent training extensiveness. A second hierarchical multiple regression examined whether family-, provider-, or organizational-level facilitators predicted parent training extensiveness.
Qualitative analysis
Interviews were transcribed and uploaded to Dedoose 7.5.9. Four coders utilized thematic analysis (Braun & Clarke, 2012) to analyze the qualitative interviews. All themes were developed inductively from transcripts. Data analysis focused on barriers and facilitators and followed the six phases of thematic analysis outlined by Clarke et al. (2015): (1) familiarization with data, (2) coding, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and (6) writing the report. Each transcript was reviewed by two independent coders and any disagreements on coding were resolved by consensus for each excerpt. Final codes for each excerpt were agreed upon by both coders. We utilized an approach that centered consensus-based decisions as the means of establishing agreement among coders (Harry et al., 2005; Mayan, 2016; Morse, 1997). This approach prioritizes consensus as an agreement goal as opposed to quantitative measures such as intercoder agreement, positioning consensus as a methodologically rigorous agreement goal since the process of qualitative analysis is an inherently interpretive enterprise in and of itself (Mayan, 2016, p. 107; Saldaña, 2015). Saturation was met after follow-up interviews with all interested providers were completed (n = 13); all coders agreed that no additional themes were discussed by the final interview that had not already been presented in the preceding interviews.
Community involvement
This mixed methods analysis was conducted as part of a larger mixed methods research project that involved community stakeholders from within the CMH system in Michigan. The research team included three members at the Department of Psychology at a university and one regional autism coordinator who serves as a Waiver Coordinator at Mid-State Health Network and oversees ABA services within the Michigan Medicaid Autism Benefit (second author). The larger project examines provider and caregiver perspectives on the use of parent training in the Michigan Medicaid Autism Benefit. The current analysis focuses on provider perspectives. Authors for this article include two of the university researchers (first and third authors) and our community partner who serves as the Waiver Coordinator at Mid-State Health Network (second author). The research team worked with state administrators at the Michigan Department of Health and Human Services to circulate recruitment information to all regional administrators who coordinate ABA services within the Michigan Medicaid Autism Benefit. Recruitment efforts were supported by the community partner from the research team (second author) as well as two of her peers who also serve as regional coordinators of ABA services within the Medicaid Autism Benefit. These efforts included passing along recruitment information via email. Our community partner also reserved time in one of her monthly meetings with agency leaders for the research team to discuss recruitment. In addition to help with recruitment efforts, community stakeholders were also involved in pilot testing the survey. Twenty-one agency leaders within one region of Michigan provided feedback on survey language and formatting. In sum, many state, regional, and local administrators within Michigan were involved in the development of the project. However, no autistic individuals were involved.
Results
Barriers to the use of parent training
Quantitative analysis
The most highly endorsed barriers on the Barriers to Parent Training Use measure included difficulty engaging families (M = 3.06 and SD = 1.02), a lack of agency-based training (M = 2.88 and SD = 1.49), and the view that families are not interested in participating (M = 2.81 and SD = 1.08; see Table 2). All individual family-, provider-, and organization-level barriers were related to parent training extensiveness.
Correlations between barriers and parent training extensiveness (N = 92).
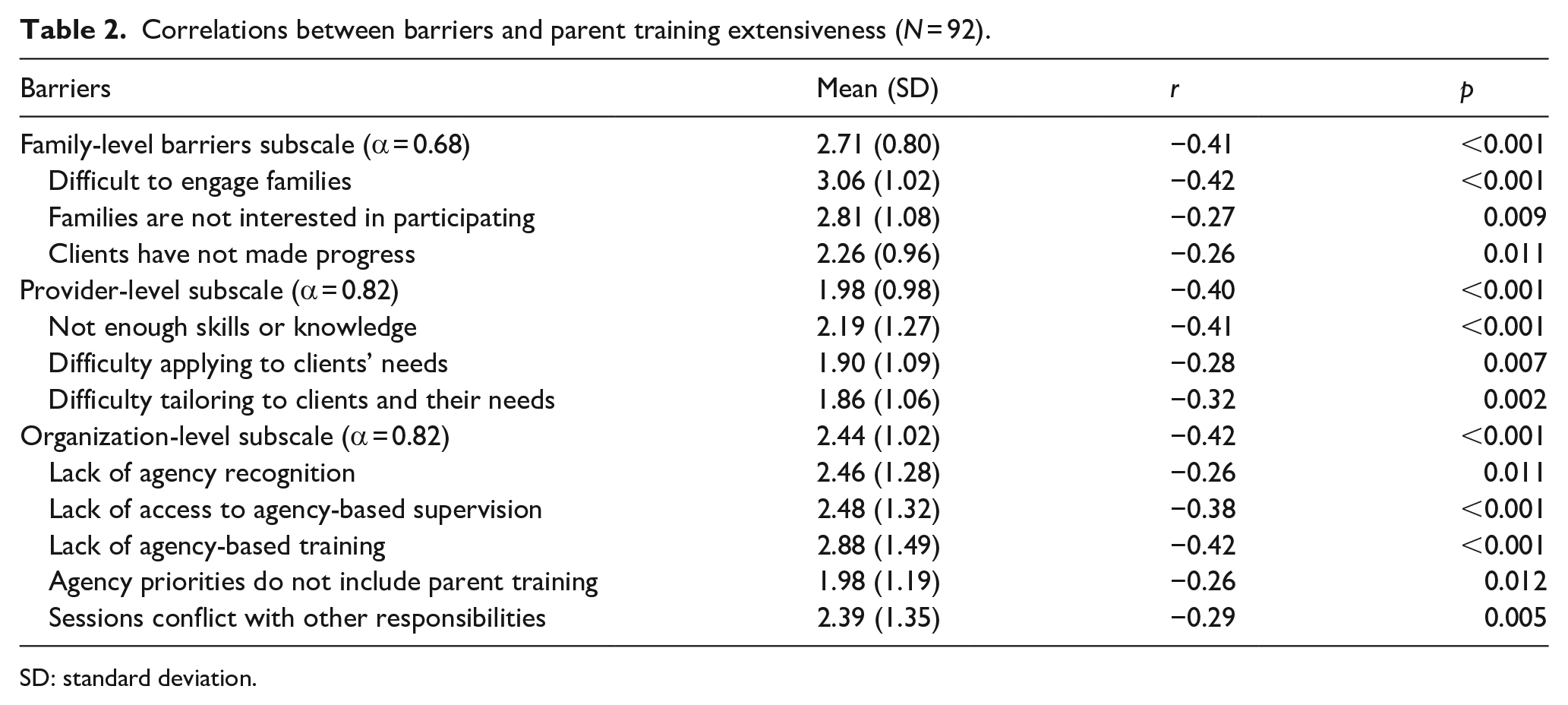
SD: standard deviation.
A hierarchical regression with years of experience working with children with ASD, professional training experiences, and the barrier subscales was significant (F(5, 86) = 8.14, p < 0.001), and accounted for 32% of the variance in parent training extensiveness, a composite measure of parent training frequency and quality (see Table 3). Family-level barriers explained unique variance in the final model (β = −0.27, t = −2.75, p = 0.007), suggesting that providers’ perceptions of family-level barriers play an important role in their use of parent training. The provider-level subscale was marginally significant (β = −0.19, t = −1.84, p = 0.07).
Hierarchical regression model of demographic variables, training experiences, and barriers predicting parent training extensiveness.
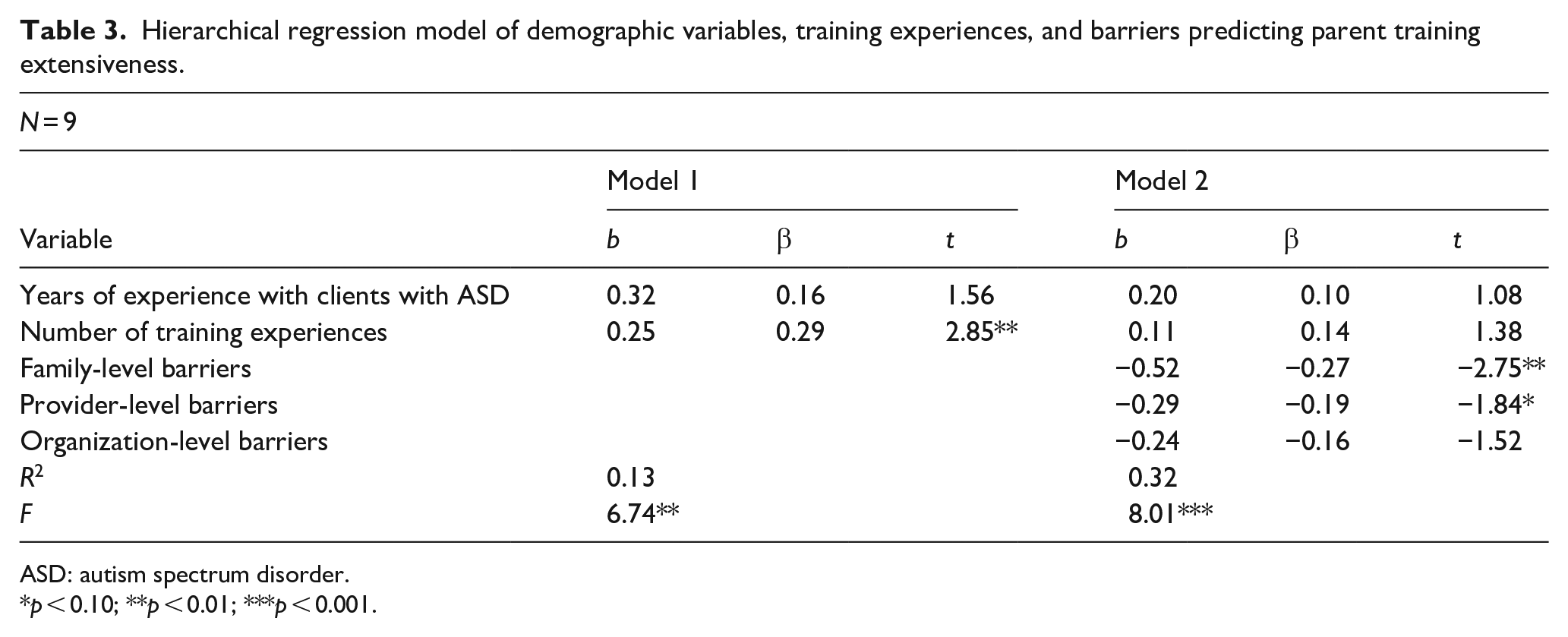
ASD: autism spectrum disorder.
p < 0.10; **p < 0.01; ***p < 0.001.
Qualitative interviews
Five themes regarding barriers to parent training emerged as follows: logistical barriers, a perception of limited family engagement and interest in parent training, limited agency support or agency norms regarding parent training, having limited training in providing parent training, and family stressors and family structures that interfere with parent participation.
Logistical barriers
All providers described logistical barriers to using parent training with their clients. These barriers included logistical barriers for parents and providers. Parent logistical barriers included scheduling difficulties (e.g. hard to reach parent and incompatible parent work schedules), transportation issues, and location concerns (e.g. rural areas that are difficult to access and concerns about the safety of the client’s home). Provider logistical barriers included difficulty using parent training in clinic settings, juggling other work responsibilities (e.g. time to supervise behavior technicians), lack of printed materials, large caseloads, having many administrative responsibilities, and time restrictions on session length.
Limited family engagement and/or interest in parent training
Perceptions of limited family engagement and interest were noted by 92% of providers. Providers described that parents had limited buy-in regarding parent training. Some described that interest was worst when first beginning parent training. For instance, one provider explained, When you start off . . . there often is no buy-in from the parent. They are doing this because it is being requested of them and not something that they are necessarily wanting or thrilled to have you come in and go through it with them.
This perceived limited engagement was viewed as frustrating: And I kind of get frustrated occasionally because I do have a couple of parents who are like “just take my child,” but not realizing that fixing the child doesn’t just happen with me, it happens across all dimensions of the child’s life.
One provider gave a potential explanation for why families might appear disinterested, noting that parents may be less interested because sessions may focus too much on progress monitoring: A lot of clinicians do just meet with the family and kind of check in, and say you know “How are things going?” and kind of more just a discussion of current progress instead of . . . putting things into practice. I think clinicians sometimes get worried that the parents will get overwhelmed with a lot of this information.
This sense of limited engagement and interest from families was sometimes linked to social class, suggesting clinician bias may play a role in the utilization of parent training. Most providers (95%) held a master’s degree or higher and likely were of a higher SES than their clients (whose household incomes were at or below 133% of the federal poverty line). In addition, most providers were White (87%) and non-Hispanic/Latino (97%), and only 6% were of non-White backgrounds, whereas many clients in this setting are of racial and ethnic minority backgrounds (12% Black, 12.5% multiracial; Straiton et al., in press). These differences in lived experiences may have biased providers’ perceptions of parent interest or engagement in services. In some cases, providers suggested that “Medicaid parents” viewed ABA services as a babysitting service as opposed to therapy and that these parents were uninterested in putting forward effort: Some of our Medicaid parents will view us more as a babysitter rather than something they have to actually do, so they kind of want us to fix their kid without having to actually do things, and that can be tricky.
Limited agency support and/or agency norms regarding parent training
Most providers (85%) described limited agency support regarding parent training or that it was not a norm at their agency. Some providers described feeling that parent training sessions were merely a requirement from their agencies that was monitored for compliance rather than for quality: I think they just see it as . . . talk to the family and . . . make sure you have that billing code for that once a month, twice a month requirement, whatever it is, per client. So that when it comes time for an audit, we aren’t penalized.
Providers described feeling overburdened by administrative duties, evidenced by statement such as “Sometimes [I feel] that the administrative responsibilities take away from time that could be allocated otherwise” and “I mean we can only do so much.”
In addition, some providers indicated that parent training was not a norm at their agency, or that providers offered it for financial gain rather than for clients’ benefits: I believe that my coworkers . . . are doing it for that billable hour increase . . . and umm possible bonus opportunities . . . And other people, I feel like they don’t do it just because I feel like families are very difficult to get ahold of . . . families don’t take your recommendations . . . so it just becomes frustrating and essentially feels like a waste of your time when you have, you know, supervision hours to make up or an assessment to write up.
Limited pre-service and in-service training
The majority of providers (85%) described having limited professional training experiences in providing parent training. Providers commented about their training being focused on direct child intervention and rarely including information about training parents: Clearly we are taught how to implement ABA therapy with children with autism . . . but not necessarily then how to take it and teach parents in a way that makes sense to them.
Many providers felt that they had underdeveloped skills in how to effectively provide parent training and thus felt unprepared to provide this type of service.
Family stressors and family structures
Most providers (69%) mentioned family stressors and family structures as a barrier. Providers mentioned stressors such as financial strain, parent mental health concerns, and family structures such as single parent households. Often, these concerns were described in combination with each other: I see a lot of families that I work with, especially single parent families . . . where the parent has significant substance use or comorbid kind of you know psychological substance use, mental health issues, those type of things.
Many providers mentioned this theme of family stressors with the theme of limited family engagement or interest. For instance, one provider noted, I’ve seen with foster parents that are just like, “I’m licensed to take this child and I don’t want anything to do with it. I want you to take as much of it [as possible],” and they have no buy in, no intention to try and develop, they don’t have the skills.
Perceptions such as these likely decrease the probability that a provider will offer parent training to the family. In this way, observed or perceived family stressors and family structures may serve as a precursor to providers’ perceptions of family engagement or interest in parent training. Classism may also play a role in the way that these stressors are linked to perceived disinterest in these services. From our thematic analysis, it appears that classism may affect decisions made by providers who assume the gatekeeping role when offering parent training sessions.
Facilitators to the use of parent training
Quantitative analysis
All facilitators were significantly related to parent training extensiveness except for believing that parent training can be tailored to clients’ needs (p = 0.138; see Table 4). A hierarchical regression with years of experience in working with children with ASD, number of professional training experiences, the individual provider-level facilitator items, and the family- and organizational-level facilitator subscales was significant (F(7, 84) = 5.20, p < 0.001) and accounted for 30% of the variance in parent training extensiveness, a composite measure of parent training frequency and quality (see Table 5). No facilitators uniquely predicted parent training extensiveness, but the number of related training experiences (β = 0.19, p = 0.06) and having the necessary skills to do parent training (β = 0.24, p = 0.06) were marginally statistically significant.
Correlations between facilitators and parent training extensiveness (N = 92).
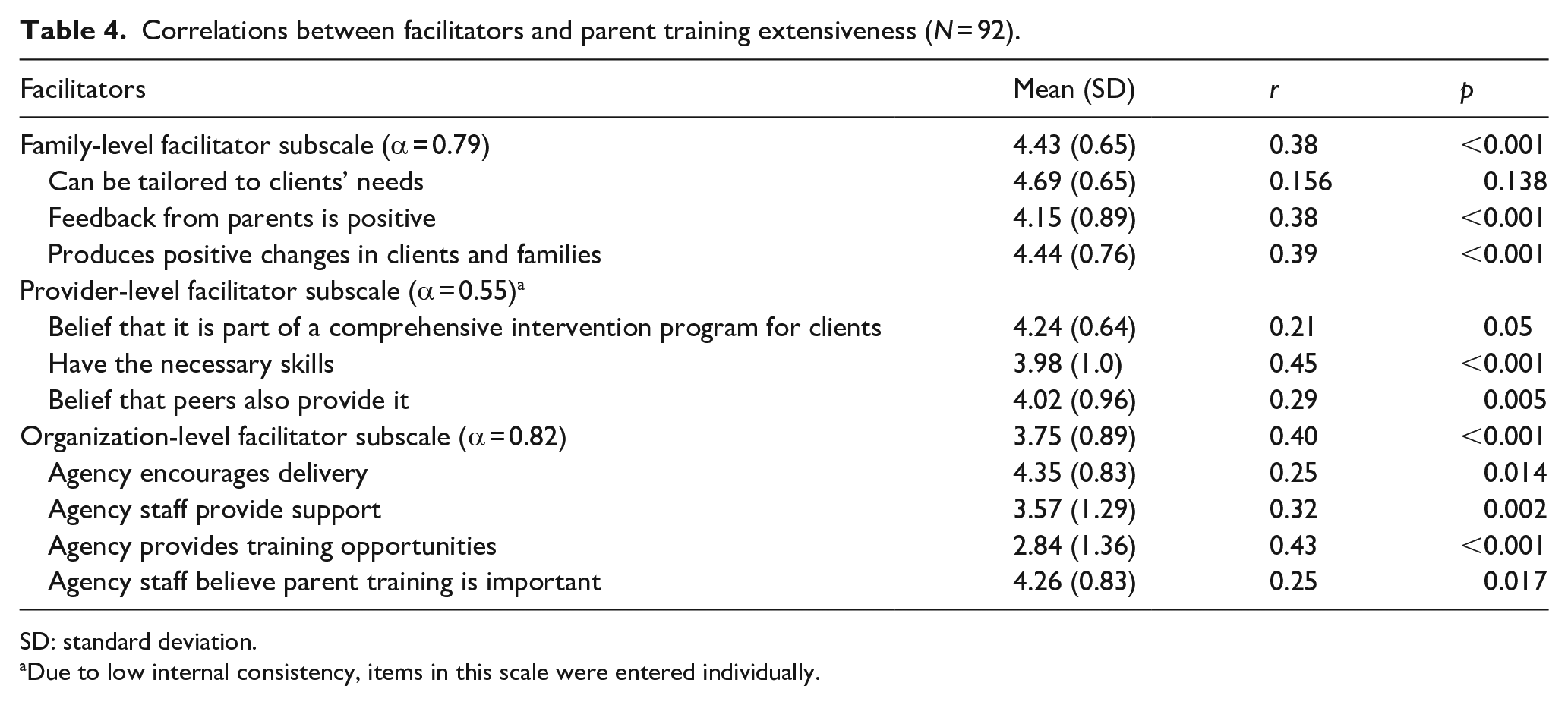
SD: standard deviation.
Due to low internal consistency, items in this scale were entered individually.
Hierarchical regression model of demographic variables, training experiences, and facilitators predicting parent training extensiveness.
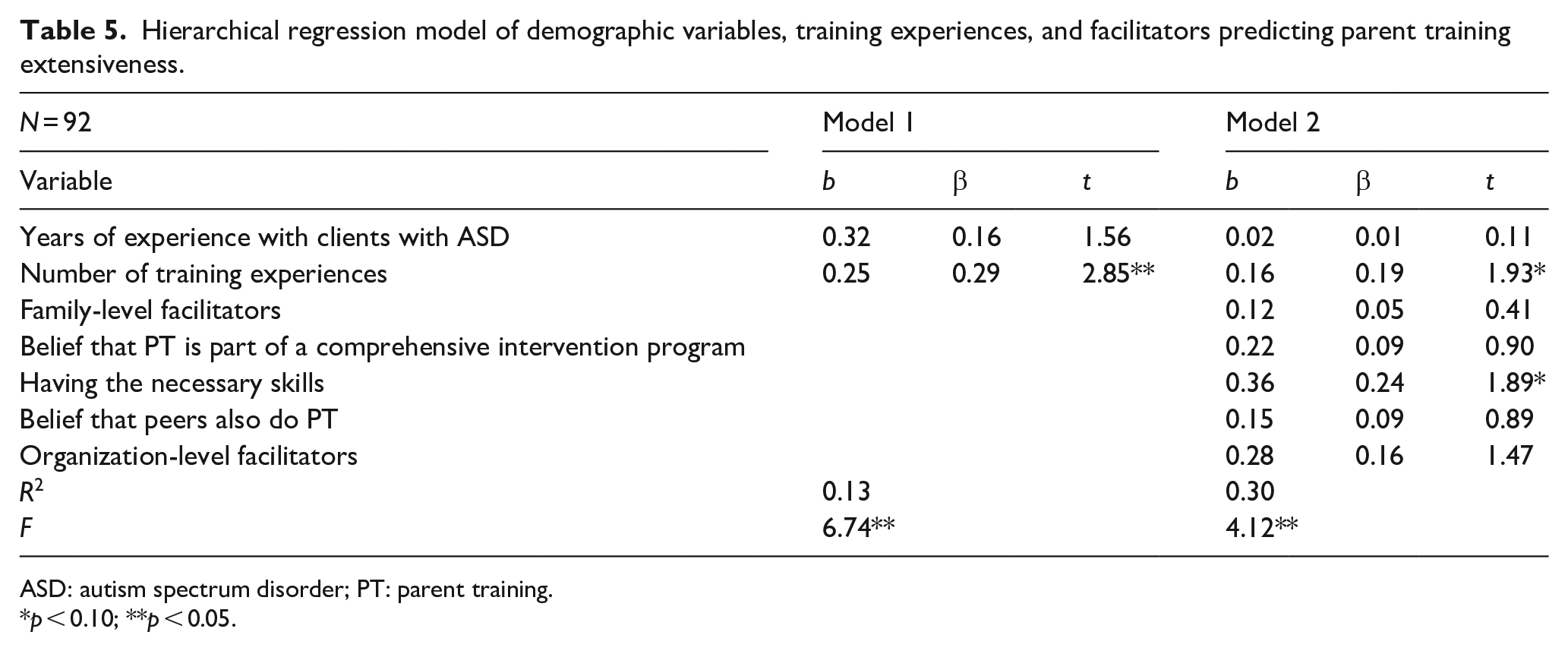
ASD: autism spectrum disorder; PT: parent training.
p < 0.10; **p < 0.05.
Qualitative interviews
Four themes about facilitators emerged as follows: logistical facilitators, agency support for using parent training and/or using parent training is an agency norm, high family engagement and interest in parent training, and having professional training in how to provide parent training. If providers made a comment about wishing or hoping for a form of support that they did not currently have, this was also coded as a facilitator, as the research team concluded that desired supports were mentioned because providers viewed them as helpful.
Logistical facilitators
All providers mentioned logistical facilitators that made it easier to provide parent training to their clients. Most logistical facilitators mirrored the logistical barriers, including methods to make scheduling easier (e.g. scheduling parent training at the beginning or end of a child-directed session or at drop-off), greater ease in providing parent training for in-home services rather than clinic-based services, having premade materials (e.g. handouts), and having manageable caseloads.
Providers also mentioned unique logistical facilitators. One facilitator was group formats. This facilitator was noted to be helpful in addressing providers’ time constraints, providing social support for parents, and reducing the time that clients spent on a waitlist prior to receiving ABA services. One provider described their excitement at the possibility of being able to support clients on the waitlist: As you know with the Medicaid Benefit, we’re not allowed to have a waitlist, yet we seem to have families in the dozens who . . . we don’t have the clinicians for . . . but they’re still waiting for support and we’re in the process of starting family training groups and individual training for these parents . . . and it’s really exciting to see that these families will get some sort of support.
Another provider noted that it would be nice to have “a group training . . . for families that have a lot of similar questions and concerns about things, and to be able to create a support group for the families.” Thus, group parent training was viewed not only as a logistical facilitator in terms of reducing costs for agencies but also as a service that included social support for parents.
Another logistical facilitator was access to manualized parent training programs. Providers described positive experiences with using manuals, with one stating that “it’s so nice to have a guided curriculum . . . for parents with children with challenging behaviors . . . and to have some sort of way to have it individualized but curriculum written.” Those who did not have access to manualized programs mentioned the desire for their agency to provide them: I know there are manuals and things out there for parent trainings. I would feel that if our company provided more access to those trainings or to the products or books . . . that would give us a good guide to help our families . . . right now it’s kind of like if we find something, we have to purchase it on our own and implement it.
In addition, telehealth was mentioned as a logistical facilitator that was helpful as a service delivery method that could mitigate logistical barriers: The counties that I work in do not allow us to do tele-anything. We can’t give tele-information or tele-parent training and I wanted to, especially in those rural areas in the wintertime—it can be difficult to get to. It’s dirt roads, really hilly and . . . the middle of the state [is] not plowed and not taken care of as nice. So, with those families, tele-parent training would be . . . a huge benefit for them as well as myself.
Agency support and/or agency norms regarding parent training
All providers mentioned agency support and agency norms for parent training as a facilitator. Some providers explicitly noted norms surrounding parent training. One provider explained: “Our supervisors track our activity and keep track of how many family trainings and supervisions and assessments and all those other things we do on a quarterly basis.” Agency support often overlapped with logistical facilitators, including the provision of manuals or manageable caseloads. In some cases, providers listed financial incentives as a means of agency support, such as increasing the likelihood that a bonus is given to a provider who consistently provides parent training.
High family engagement and interest in parent training
High family engagement and interest was described by 54% of interviewed providers as a facilitator to use of parent training. Yet when this theme was mentioned, it was usually stated in the context of frustration that many families do not have this interest or motivation: I need you to be willing and for you to trust me . . . If I have a family who has a lot of barriers they just can’t move past . . . they say “You need to fix it. You need to take the full responsibility of changing my child.” That’s not going to work. I need a parent to be like, “I am responsible for my child to change at the end of the day.”
Professional training in how to provide parent training
Professional training experiences that explicitly taught providers how to deliver parent training were viewed as a facilitator. 23% of participants mentioned that professional training opportunities were helpful in increasing confidence and skills to provide parent training. This training included coursework and/or in vivo practice with a supervisor. One provider described taking a course that covered relevant content: One of the courses focused more on huge issues in the home and on autism and . . . I learned a lot about what family training is . . . It focused more so on the other issues, sibling issues in the home, the sexuality issues, feeding programming, social skills, community engagement, and I thought that part was probably the most valuable in terms of adopting family training because it offers great resources to reference but also makes you aware of the issues of the families that are underlying your family training, that, you know, parents might not want to be speaking about.
In addition to coursework, providers highlighted hands-on training with supervision as helpful: At my university, a couple of professors had created a center for autism, so we got practical experience from doing that for at least a semester. For most of us, it was a couple of years, so we got to participate in a . . . family training model, so I felt well prepared.
Thus, providers who received professional training felt better prepared to provide parent training sessions. However, professional training experiences about parent training were uncommon.
Discussion
Results from this study suggest that providers serve as gatekeepers to parent training access, with providers deciding whether or not to offer parent training based on barriers and facilitators at the family-, provider-, and organization-level. Providers in this sample were predominantly White (87%) and non-Hispanic/Latino (97%); only 6% were of non-White backgrounds. Yet many clients in this setting are of racial and ethnic minority backgrounds (12% Black, 12.5% multiracial; Straiton et al., in press). Moreover, most providers (95%) held a master’s degree or higher and thus likely were of higher SES than their Medicaid-enrolled clients. These differences in lived experience may have biased their perceptions of clients, such as perceptions of family disinterest. Indeed, these perceptions were frequently cited as a rationale for not offering or providing parent training. Results from this study suggest that classism and provider competency in parent engagement and parent training play a large role in providers’ gatekeeping decisions. This also appears to intersect with family buy-in. For instance, providers with limited competency may still decide to provide parent training if a family indicates strong motivation and interest in the intervention. Training and additional support (e.g. consultation) would increase provider competency in engaging parents and delivering evidence-based parent training, thereby equipping providers to feel comfortable offering this type of intervention regardless of initial caregiver buy-in.
Because providers serve in a gatekeeping role, they may label disinterest in current practices as disinterest in parent training more broadly. Yet providers are largely unaware of evidence-based components of parent training and instead view treatment management and progress monitoring as key features of parent training (Straiton et al., 2020); this perceived disinterest may be specific to current practices that are not evidence-based. In fact, parents of Medicaid-enrolled clients with ASD indicate that they are not interested in parent training sessions focused on treatment management and progress monitoring, but are motivated to participate in sessions that incorporate caregiver practice with feedback (Casagrande et al., in preparation). In addition, parents of lower-resourced backgrounds view limited parent engagement in services as a result of providers not approaching them in a collaborative manner (Pickard et al., 2016; Stahmer et al., 2019). Providers are likely unaware of this discrepancy.
There appears to be confusion regarding what parent training sessions should entail; ABA providers often do not mention evidence-based components such as caregiver practice with feedback when defining parent training (Straiton et al., 2020). Thus, agencies and licensing boards should create guidelines for parent training sessions that are in line with best practices, emphasizing instruction in intervention techniques, modeling of intervention techniques, and caregiver practice with feedback. These guidelines should specify that sessions should not solely be used for treatment management or progress monitoring, which is how many ABA providers within low-resourced settings view parent training (Straiton et al., 2020). Consistent language and messaging around what evidence-based parent training looks like is critical, given that parent training has been defined in a variety of distinct ways (Bearss, Johnson, et al., 2015; Straiton et al., 2020). In addition, most of what we know about behavioral science is based on studies of upper-middle class White families from Western, educated, industrialized, rich, democratic societies (Hendriks et al., 2019). Thus, practice recommendations should incorporate the perspectives of clients of lower-resourced backgrounds and the providers who work with them, as well as the efficacy of evidence-based interventions in under-resourced contexts.
Recommendations to increase parent training use for youth with ASD
The following two recommendations are presented as a means to increase parent training use in community settings for youth with ASD:
Provide high-quality pre-service and in-service professional training experiences regarding best practices in parent training and parent engagement.
Increase agency support for the provision of parent training, including support to improve logistics of sessions and implementation climate.
Provide professional training experiences
Providers noted that pre-service and in-service professional training experiences were an important facilitator of parent training use. Results converged across data sets, supporting this recommendation, including the following evidence: (1) greater number of professional training experiences and having the necessary skills were the only two predictors in the facilitators’ hierarchical linear regression model that were marginally associated with increased extensiveness and (2) having limited professional training experiences was a theme discussed as a barrier by 85% of providers in follow-up interviews.
Both pre-service and in-service training should be targeted. Only 37.1% of providers on the survey endorsed receiving structured pre-service training opportunities (e.g. taking a course about parent training) and only 13.4% endorsed having training in a specific intervention approach (e.g. Project ImPACT and Early Start Denver Model). Training providers in graduate school would provide them with the necessary skills to feel confident in providing parent training. This pre-service training should explicitly target how to train parents in intervention techniques, which would likely reduce perceived barriers (Ingersoll et al., 2020). In addition, this training should provide explicit instruction in best practices for parent engagement, given that perceived family disinterest was a prominent barrier cited by providers in this sample. In-service training efforts must also be established, as much of the current workforce did not receive explicit pre-service training. In general, training should include supervision, as ongoing support strategies like supervision allow for improvement in increasing providers’ use of evidence-based practices (Beidas et al., 2012; Herschell et al., 2010). Professional training efforts should also include explicit instruction in best practices for engaging caregivers in treatment. This could also help to promote positive interactions between families and providers, which increase parent participation in child therapy sessions and improve attendance (Haine-Schlagel et al., 2018).
Increase agency support
To increase the use of parent training in community settings, agency support should be targeted. Based on facilitators outlined in this study, agencies should focus on mitigating logistical barriers via the provision of manualized programs, group formats, and reduced administrative responsibilities. Other supportive methods should also be incorporated into agency support, such as consultation or financial incentives (Powell et al., 2012).
Some providers described the ability to provide parent training sessions via telehealth as a facilitator to reduce logistical barriers. It is worth noting that, while the Michigan Medicaid Autism Benefit has the infrastructure to use telehealth for parent training sessions, billing claims’ data demonstrated that only 10 children (1%) received parent training via telehealth, and all of those youth were from the same CMH agency (Straiton et al., 2020). Telehealth models of parent training for children with ASD have demonstrated improved child and family outcomes (Ingersoll et al., 2016; Vismara et al., 2013). Telehealth models may be especially helpful for families that live in remote rural areas and those who experience transportation difficulties. Thus, agencies and state administrators should consider ways to make telehealth sessions more accessible.
Limitations and future directions
We acknowledge several limitations to this study. First, there are limited psychometric data on both scales used in this study and the facilitator scale had poor internal consistency for the provider-level subscale. Future research should investigate the psychometric properties of both scales and establish a better measure to capture provider-level facilitators to parent training extensiveness. In addition, our interviews’ sample size was relatively small (n = 13). We reached saturation after completing 13 interviews, and triangulation of the quantitative and qualitative data confirms the qualitative findings, suggesting that our findings are valid. However, future research should include more qualitative data to replicate these findings in other low-resourced service contexts. Nevertheless, this mixed methods analysis demonstrated convergent findings, allowing for a more in-depth understanding of facilitators to parent training use than using only one method.
Furthermore, using provider perspectives alone to characterize service contexts will not provide a complete depiction of the service landscape. Perspectives of parents and agency leaders should also be analyzed. Future research should explore these perspectives, particularly with families from lower-resourced backgrounds. It is also important to recognize that our findings are situated within a particular context in the Michigan Medicaid Autism Benefit and thus may not extend to other ASD service contexts, as service systems vary greatly across the United States and our global context.
To our knowledge, this is the first investigation of provider perspectives of parent training use within CMH agencies for youth with ASD. Clients of lower-resourced backgrounds already face a number of additional stressors that make receipt of youth mental and behavioral health services difficult (e.g. financial burden and limited transportation; Stahmer et al., 2019). Parent training is not only a best practice for treating youth with ASD (Steinbrenner et al., 2020; Wong et al., 2015) but also has been demonstrated to improve skill generalization and maintenance (Koegel et al., 1982), improve parent self-efficacy (Karst & Van Hecke, 2012), and reduce parental stress (Iadarola et al., 2018; Ingersoll et al., 2016). While these findings are based on predominantly White, upper-middle class families, it is likely that these benefits would extend to families of lower-resourced backgrounds as well. Future research should investigate this within lower-resourced contexts.
Our recommendations serve as a roadmap for policymakers and leaders at the state and regional levels to make necessary changes to promote the use of parent training for youth with ASD served in community settings. Future research efforts should establish community-academic partnerships to implement and study the effects of these changes on the service landscape. Future studies should also further analyze provider biases and develop explicit strategies to address them.
Footnotes
Acknowledgements
The authors thank the providers who participated in this study for their time.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by the Blue Cross Blue Shield of Michigan Foundation Student Award Program (003701.SAP).