
Abstract
Elevated parenting stress among parents of children with autism spectrum disorder is well-documented; however, there is limited information about variability in parenting stress and relationships with parent ratings of child functioning. The aim of this study was to explore profiles of parenting stress among 100 parents of young children with autism spectrum disorder enrolled in two clinical trials and potential relationships between parenting stress and parent ratings of child functioning at the baseline timepoint. Secondary aims examined differential patterns of association between parenting stress profiles and parent versus clinician ratings of child functioning. A k-means cluster analysis yielded three different profiles of parenting stress (normal, elevated, and clinically significant) using scores on the Parenting Stress Index–Short Form. One-way analyses of variance revealed differential patterns of parent ratings across the three parenting stress profiles on certain domains of child functioning (e.g. problem behaviors and social impairment) and family empowerment, but similar ratings of child receptive and expressive language abilities. Clinicians blinded to study conditions also rated child functioning, but clinician ratings did not differ by parenting stress profile. Findings emphasize the importance of identifying parenting stress profiles and understanding their relationship with parent ratings, with implications for interpreting parent-report measures and measuring child response in treatment trials.
Lay abstract
Elevated parenting stress among parents of children with autism spectrum disorder is well-documented; however, there is limited information about differences in parenting stress and potential relationships with parent ratings of child functioning. The aim of this study was to explore profiles of parenting stress among 100 parents of young children with autism spectrum disorder enrolled in two clinical trials and to explore relationships between parenting stress level and parent ratings of child functioning before treatment. Secondary aims examined differential patterns of association between parenting stress profiles and parent versus clinician ratings of child functioning. We show that stress may influence parent ratings of certain child behaviors (e.g. problem behaviors) and not others (e.g. language), yet clinician ratings of these same children do not differ. This new understanding of parenting stress has implications for parent-rated measures, tracking treatment outcome, and the design of clinical trials.
Autism spectrum disorder (ASD) has a prevalence rate as high as 1%–3% in the United States affecting 3–9 million families (Christensen et al., 2019). Individuals with ASD may require supports throughout the lifespan (Gerhardt & Lainer, 2011; Jensen & Spannagel, 2011); many of which are organized by parents (Brown et al., 2011; Mulligan et al., 2012). Simultaneously, these parents face unique parenting challenges and elevated, chronic, and ASD-specific stress (Estes et al., 2013; Hayes & Watson, 2013; Johnson et al., 2011; Weitlauf et al., 2014). High parental stress may negatively impact child development and treatment gains, particularly for parent-delivered interventions (Osborne et al., 2008).
It is important to note that experiences of stress are not universal across parents of children with ASD as some parents rate their parenting stress below the clinical cutoff on stress measures (e.g. Parenting Stress Index (PSI)), even though group means fall above this same cutoff (Minjarez et al., 2011, 2013; Stadnick et al., 2015). This differential stress response may suggest stress diversity among parents of children with the same diagnosis. Multiple factors may influence parenting stress including parent personal factors (Estes et al., 2013; McStay et al., 2014; Zaidman-Zait et al., 2017), child problem behaviors (Hayes & Watson, 2013; Walsh et al., 2013; Zaidman-Zait et al., 2014), available supports (e.g. family support groups, psychological services, and childcare options; Hall & Graff, 2011, 2012; Meadan et al., 2010), appropriate coping mechanisms (Lai & Oei, 2014), and severity of child social impairment (Ekas & Whitman, 2010; Huang et al., 2014). Similarly, positive indicators of parent well-being, such as family empowerment, may provide insight into the differential stress response. Only a few studies have explored parenting stress and family empowerment in ASD, but collectively suggest an inverse relationship between these constructs (i.e. higher stress associated with lower family empowerment, vice versa; Brookman-Frazee, 2004; Minjarez et al., 2013). Therefore, continued investigations into this potential relationship are warranted. An enhanced understanding of parenting stress is emerging in the literature; however, this is complicated by measurement challenges and/or models of parenting stress that report it as a singular construct above or below a clinical cutoff (Reed & Osborne, 2013). Many aspects of parenting stress in ASD remain unclear including stress diversity, potential influence on parent ratings of their children, and discrepancies between raters (parents vs clinicians) in conceptualizing a child’s abilities. These may be important factors to understand given parent participation in early interventions for children with ASD.
Parents of children with ASD engage in many aspects of early interventions including parent training and providing parent ratings of treatment outcome. Parent training can result in greater treatment efficacy among children (Nevill et al., 2018; Oono et al., 2013) and parent-rated measures are routinely used to assess treatment efficacy (Gengoux et al., 2015, 2019; Gulsrud et al., 2015; Hardan et al., 2015; Schreibman et al., 2015). These critical components are also dependent upon parents who face unique parenting challenges and elevated stress. Greater understanding of the relationship between parenting stress and ratings on standardized measures is critical for accurate interpretation of these tools both as predictors of treatment response and outcome measures in clinical trials.
Several studies reported significant discrepancies between parent, teacher, and clinician ratings of the same child with ASD in certain domains (e.g. problem behaviors and autism symptomology), yet other domains (e.g. language and adaptive skills) appear similar across raters (Rowberry et al., 2014; Rubenstein et al., 2017; Stadnick et al., 2017). Parents, teachers, and clinicians play distinct and integral roles in the child’s life and each observes the same child in different contexts, which highlights the importance of understanding potential differences in observations across raters. Differences may be crucial in enhancing screening efforts in ASD and elucidating treatment targets. In parent ratings, parenting stress has been identified as an important variable contributing to divergent ratings (Osborne et al., 2008; Reed & Osborne, 2013). Although caregiver report is the most common measure of change in pediatric psychiatry, a recent study found that parents reported treatment gains in their child following an 8-week observation period in which no active intervention was administered (Jones et al., 2017). These placebo-like effects on parent ratings represent significant challenges for randomized controlled trials (RCTs) that utilize parent ratings to measure treatment outcome (Jones et al., 2017). Viewing the child in a different context, teachers tend to provide ratings of child problem behaviors in a manner similar to clinicians blind to study conditions, but divergent from ratings provided by parents (Azad et al., 2016; Lane et al., 2013; Reed & Osborne, 2013; Stratis & Lecavalier, 2017). Similarly for ratings of child autism symptomology, several studies suggest discrepancies between teacher and parent ratings (Azad et al., 2016; Stratis & Lecavalier, 2017), while teacher ratings align more closely to clinician ratings (Azad et al., 2016). In terms of social functioning, studies on rater agreement between parents and teachers appear mixed (Foley Nicpon et al., 2010; Lopata et al., 2016; Murray et al., 2009) with some behaviors (e.g. initiations) dependent upon rater and social context (Murray et al., 2009).
In contrast, higher inter-rater agreement occurred between parents and teachers on ratings of child language abilities (Kwok et al., 2015; Nordahl-Hansen et al., 2013; Volden & Phillips, 2010) and child adaptive skills (Lane et al., 2013). Discrepancies may be accounted for by time scales involved in procuring ratings as well as the different contexts in which ratings are collected across raters. Rater differences are crucial to not only support the use of multi-method, multi-informant assessments in treatment trials but also to understand how parent perceptions of child behavior may affect early interventions. To date, no studies, to our knowledge, have explored discrepancies in the patterns of associations between parenting stress profiles and parent and clinician ratings of the same children with ASD, which is an important step to elucidating the role of parenting stress in measurement.
The goal of this study was to examine diversity of baseline parenting stress among 100 parents of children with ASD presenting for parent training across two completed RCTs of Pivotal Response Treatment (PRT; Gengoux et al., 2019; Hardan et al., 2015). The primary aim was to explore profiles of parenting stress and potential relationships with available baseline parent ratings of child functioning in domains such as child problem behavior, social ability, and language. While direct comparisons between parent and clinician ratings could not be made since clinicians completed different measures of problem behavior, social ability, and language, a secondary goal of the study was to examine differential patterns of association between parenting stress profiles and clinician ratings across available clinician-rated indices of child functioning. We hypothesized that elevated parenting stress would be associated with higher parent-rated problem behaviors and social impairment, yet parent ratings of child language abilities may not differ across parenting stress profiles. In addition, we hypothesized that differential patterns of association between parenting stress profiles and parent ratings would emerge, but clinician ratings would not differ across stress profiles.
Methods
Study design
This study analyzed baseline data from 100 parents of young children (2–6 years old) with ASD who were enrolled in two completed RCTs of PRT (Gengoux et al., 2019; Hardan et al., 2015). The present sample of 100 parents (80 female and 20 male; mean age=38.72 yeras) was comprised of 52 participants from the first RCT (Hardan et al., 2015) and 48 participants from the second RCT (Gengoux et al., 2019). Community stakeholders were not involved in this study.
Participants
Participants in both RCTs included children: (1) diagnosed with autism based on the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria, and confirmed by administration of the Autism Diagnostic Interview - Revised (ADI-R; Lord et al., 1994), Autism Diagnostic Observation Schedule (ADOS; Lord et al., 2000), and by expert clinical judgment, and (2) communication-delayed on the Preschool Language Scale -Fourth Edition (PLS-4; Zimmerman et al., 2002; 2- and 3-year olds were ≥1 standard deviation (SD) below the age level, 4-year olds were ≥2 SDs, and 5- to 6-year olds were ≥3 SDs). Parents were English-speaking and available to participate in parent training. In the first RCT, participating children were 2–6 years old and able to vocalize with intent when prompted by a clinician during the screening visit (Hardan et al., 2015). In the second RCT, children were 2–5 years old and there was no minimum communication ability required for enrollment (Gengoux et al., 2019). Exclusion criteria for both RCTs were children with: (1) individual speech therapy for more than 60 min a week, (2) comorbid severe psychiatric disorder, (3) genetic abnormality and (4) active medical problems. No changes in inclusion or exclusion criteria were applied during the two trials.
The total sample included 100 parents (20 fathers and 80 mothers) of children with ASD between 2 and 6 years old (mean age (M) = 2.98 and SD = 1.75) of diverse ethnicities, marital status, education, and socioeconomic backgrounds (see Table 1). The majority (94%) of all participating children were in school and placed in special day classes (76%) for an average of 19 h of school per week. The majority of all children were receiving weekly applied behavior analysis (ABA) (69%; M = 9.02 h per week) and speech therapy (94%; M = 56.4 min per week).
Characteristics of parents and children.
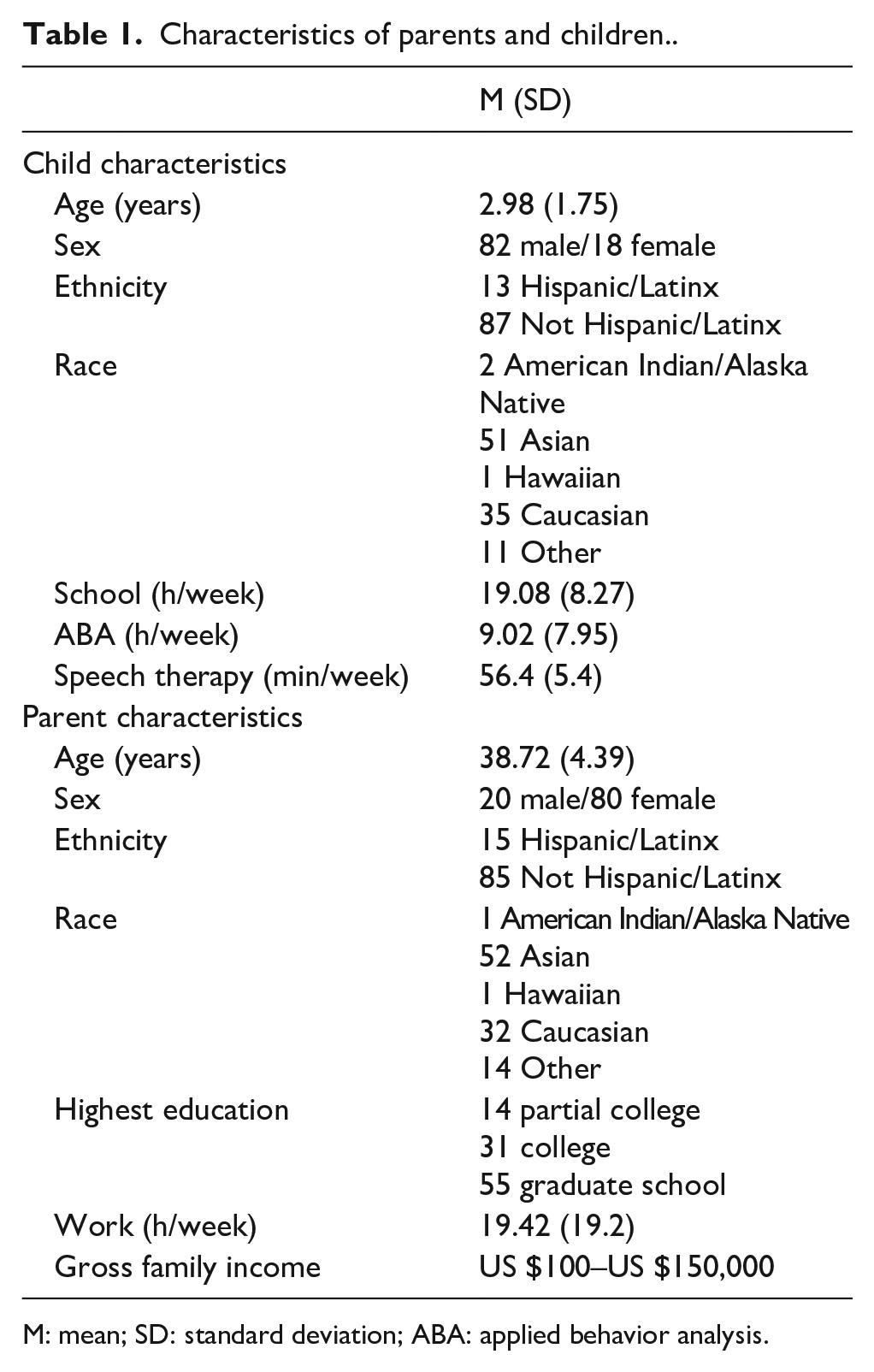
M: mean; SD: standard deviation; ABA: applied behavior analysis.
Procedures
Recruitment for the first RCT occurred over 24 months (July 2010–June 2012), and recruitment for the second RCT occurred over 32 months (December 2013–July 2016). Participants in both trials were recruited through distribution of fliers at clinics and autism awareness events, referrals by local professionals, and word of mouth. After the participant’s parent provided informed written consent in each trial, comprehensive evaluations were conducted including review of medical/psychiatric history and completion of psychological assessment batteries and parent-rated questionnaires. Both RCTs were approved by the Stanford University Institutional Review Board, and the data were managed using REDCap electronic data tools (Harris et al., 2009) hosted at the Stanford University Center for Clinical Informatics. Community members were not involved in the RCTs.
Measures
Primary measure
Parenting stress
To measure parenting stress, parents in both trials completed the Parenting Stress Index–Short Form, Third Edition (PSI-SF; Abidin, 1995) at the baseline study visit. The PSI-SF is a self-report questionnaire of 36 items that measures total parenting stress and raw scores are converted to standardized percentiles with percentiles ⩾85% indicating clinically significant parenting stress. Expanded cutoffs were recommended for the PSI-SF such that percentiles 15%–80% fall in the normal range, 81%–90% fall in the elevated range, and 91%–100% fall in the clinically significant range (Abidin, 1995). Total stress percentile scores of the PSI-SF were used to identify potential parenting stress profiles in this study. To explore diversity in parenting stress, the established cutoffs of the PSI-SF were not used, and instead, natural groupings of scores based on a k-means cluster analysis were explored.
Secondary measures
Child problem behaviors
Parent ratings of child problem behaviors were measured using the raw scores of the Aberrant Behavior Checklist (ABC; Aman et al., 1985) and the following scores from the Vineland Adaptive Behavior Scales–Second Edition (VABS-II; Sparrow et al., 1984): standard score on the maladaptive behavior domain and v-scale scores of the internalizing and externalizing subscales. Internal consistency values for the ABC ranged from acceptable to excellent (irritability = 0.92, lethargy/social withdrawal = 0.88, stereotypic behavior = 0.86, hyperactivity/noncompliance = 0.93, and inappropriate speech = 0.73) in a recent study of youth with ASD (Norris et al., 2019). Similarly, the Cronbach’s alpha values of the VABS were high in a sample of individuals with diverse developmental disabilities (communication = 0.98, daily living skills = 0.98, socialization = 0.97, and Vineland total = 0.99; de Bildt et al., 2005). The VABS accounts for child age in the calculation of norm-referenced standard scores.
Clinician ratings of child problem behaviors were measured using severity ratings of the maladaptive behavior subscale of the Clinical Global Impression Scale–Severity Subscale (CGI-S; Guy, 1976). The CGI was completed by an expert clinician to estimate the severity of the child’s behaviors at the time of assessment and children were assessed on a 7-point Likert-type scale with ratings ranging from “1—normal” to “4—moderately ill” to “7—extremely ill.” The CGI has been used in several clinical trials in ASD and found to be a reliable estimate of severity of symptoms (Bearss et al., 2015; King et al., 2009; McCracken et al., 2002).
Child social impairment
Parent ratings of child social impairment were measured using the T-scores of the Social Responsiveness Scale (SRS; Constantino, 2012; Constantino et al., 2003) and the following VABS-II scores: standard scores of the socialization domain and v-scale scores of the three subscales (interpersonal relationships, play and leisure skills, and coping skills). The SRS is a quantitative measure of autistic traits with high inter-rater reliability (0.75–0.91 for all subscales; Constantino et al., 2003). The SRS (Constantino et al., 2003) was completed by parents in the first RCT, while the SRS-2 (Constantino, 2012) was completed by parents in the second RCT. Clinician ratings of child social impairment were measured using scores from the ADOS, which was administered by research-reliable clinicians to all participants as a screening measure in both RCTs. Intraclass correlation coefficients for the ADOS are high (range = 0.82–0.93 for all domains; Lord et al., 2000).
Child language abilities
Parent ratings of child language abilities were measured with raw scores of the MacArthur-Bates Communicative Development Inventories (CDI; Fenson et al., 1993) Words and Gestures and Words and Sentences versions and the following VABS-II scores: standard scores of the communication domain and v-scale scores of the receptive and expressive subscales. The Cronbach’s alpha values of the MacArthur CDI ranged from 0.826 to 0.984 for children with language delays (Skarakis-Doyle et al., 2009). Clinician ratings of child language abilities were measured using the standard scores of the PLS-4 and the frequencies of child functional utterances during the Structured Laboratory Observation (SLO). The total number of functional utterances, and the spontaneous type of utterance, were analyzed in this study. For additional information on SLO procedures, please see Hardan et al. (2015). The PLS-4 accounts for child age in the calculation of norm-referenced standard scores.
Child developmental level
The Mullen Scales of Early Learning (MSEL; Mullen, 1995) was administered to all children as a screening measure in both RCTs. Developmental quotients (DQs) were calculated using the MSEL age equivalent divided by chronological age to yield an estimate of verbal DQ (based on Receptive and Expressive Language subscale scores), nonverbal DQ (based on Visual Reception and Fine Motor subscale scores), and a full-scale DQ (based on performance across the four subscales). High convergent validity was reported between the MSEL and similar indices of developmental functioning (range = 0.76–0.82) in a sample of youth with ASD (Bishop et al., 2011).
Parental empowerment
Parents completed the Family Empowerment Scale (FES; Koren et al., 1992) to provide ratings of parental empowerment at the family, service system, and community/political levels. The FES contains 34 items and raw scores per subscale range from 12 to 60 with higher scores reflecting higher empowerment. Internal consistency estimates of the FES subscales range from 0.78 to 0.89, and the split-half estimate of reliability was 0.93 (Singh et al., 1995).
Statistical analyses
Independent samples t-tests and Kruskal–Wallis H tests (e.g. gross family income and highest education level) were employed to assess differences on parent and child demographic variables across parenting stress profiles and to identify potential covariates. To examine the first hypothesis that distinct profiles of parenting stress exist among parents of children with ASD, a k-means cluster analysis was performed using the PSI-SF total percentile score. The k-means cluster analysis is a widely used type of analysis used to sort cases into groups (i.e. clusters) based on strong associations within members of the same cluster, and weak associations between members of different clusters (Milligan & Romesburg, 1985; Scott & Knott, 1974). In this study, a k-means cluster analysis was utilized to sort cases based on their relative distance from cluster means using an algorithm. Specifically in ASD, cluster analysis has been employed to identify sub-groups of individuals (Eaves et al., 1994; Schwartzman et al., 2016; Wiggins et al., 2012). Clusters of parenting stress were determined by the results of the k-means cluster analysis, rather than the recommended cutoffs of the PSI-SF, in order to explore parenting stress diversity in this sample. Following the k-means cluster analysis, parenting stress scores were then grouped by the recommended PSI-SF cutoff scores (15%–80% normal, 81%–90% elevated, and 91%–100% clinically significant) to assess similarities or differences between cluster scores and established cutoff scores (Abidin, 1995). Differences in group membership between cluster scores and established cutoff scores were assessed by totaling the number of parents with differing scores (e.g. cluster membership in normal range and recommended cutoff in elevated range).
In order to examine the second hypothesis that a relationship may exist between distinct stress profiles (i.e. clusters) and parent ratings, one-way analyses of variance (ANOVAs) were employed using the identified stress clusters as the independent variable and parent ratings of problem behaviors (ABC), social impairment (SRS), maladaptive behaviors (VABS), language (MacArthur CDI), and empowerment (FES) at baseline as dependent variables. To examine differential patterns of association between parenting stress profiles and clinician ratings, one-way ANOVAs were again employed using the identified stress clusters as the independent variable and clinician ratings of social impairment (ADOS), language (PLS-4 and SLO) and developmental ability (Mullen) as the dependent variables. Two-tailed tests were employed to test statistical significance, which was defined by p-values < 0.05. Post hoc t-tests were employed to examine differences in scores between the three clusters, and to correct for multiple comparisons, Bonferroni adjustments were applied. Finally, a Kruskal–Wallis H test was run to determine if there were differences in CGI-S maladaptive behavior scores between the three parenting stress profiles.
Results
Distinct profiles of parenting stress
A total of 100 parents completed the PSI-SF at baseline with an average percentile score of 75.51 (SD = 30.1; range = 5–100) for total stress, which is a group mean in the normal range. A three-cluster solution emerged as the best solution after reiterating the k-means cluster analyses using between three and seven group solutions (see Table 2). The three distinct clusters that emerged were significantly different from each other (p < 0.001): Cluster 1 reported the lowest stress percentiles with a group mean in the normal range (i.e. normal stress cluster), Cluster 2 reported higher stress percentiles with a group mean in the elevated range (i.e. elevated stress cluster), and Cluster 3 reported the highest stress percentiles with a group mean in the clinically significant range (i.e. clinically significant stress cluster). There were no significant differences on any parent or child demographic variables reported in Table 1 across the parenting stress profiles (p > 0.05). Comparison of group membership by cluster score and established cutoff score (Abidin, 1995) demonstrated that 96 parents exhibited similar membership across the scoring indices (i.e. parents in both the normal stress cluster and normal range on the recommended cutoff).
Characteristics of parenting stress profiles.
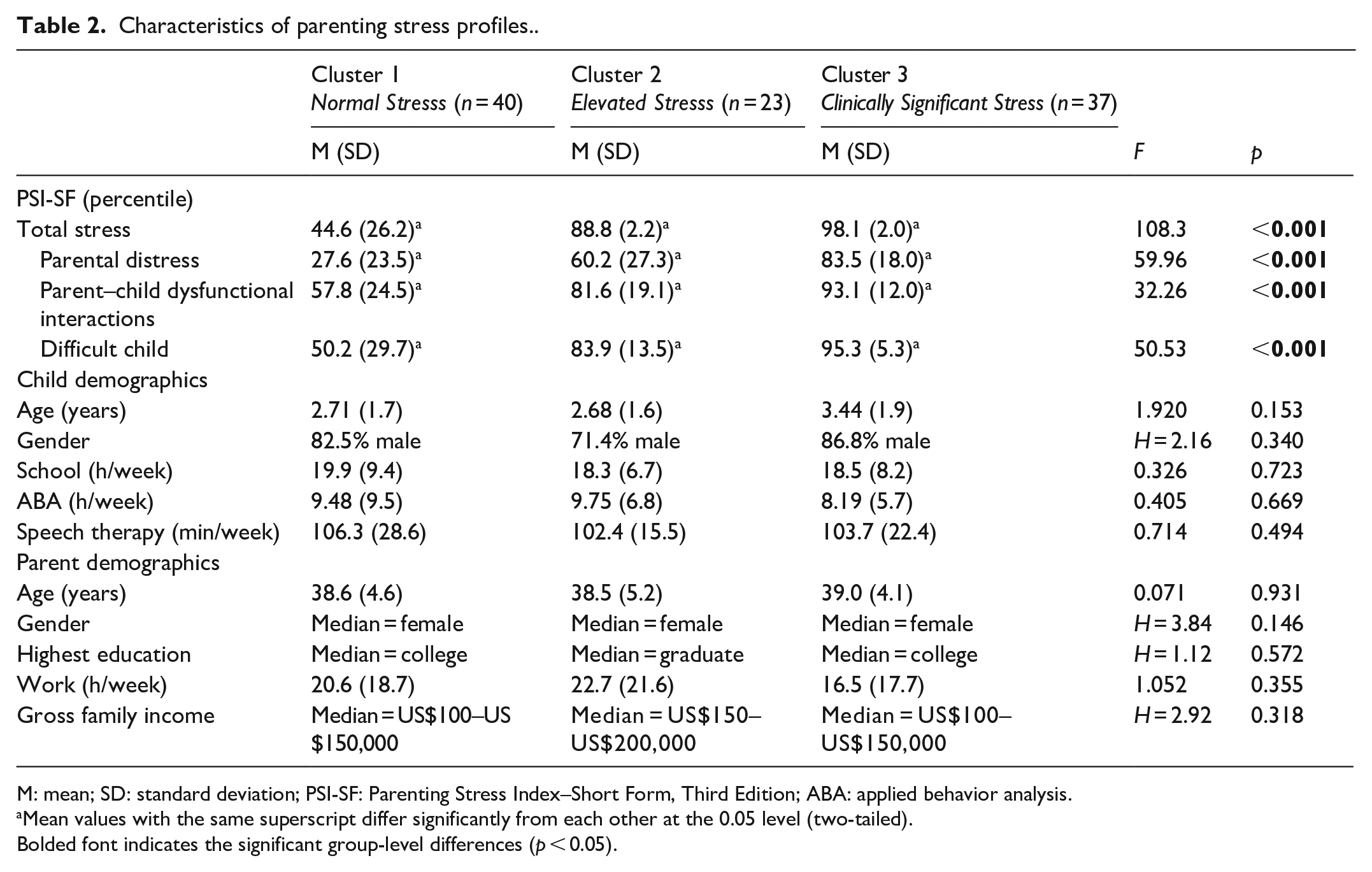
M: mean; SD: standard deviation; PSI-SF: Parenting Stress Index–Short Form, Third Edition; ABA: applied behavior analysis.
Mean values with the same superscript differ significantly from each other at the 0.05 level (two-tailed).
Bolded font indicates the significant group-level differences (p < 0.05).
Parent-report measures compared across parenting stress profiles
Table 3 presents parent ratings at baseline across the three stress profiles. Significant group differences emerged across the parenting stress profiles for parent ratings of total child problem behaviors on the ABC and the subscales of irritability, social withdrawal, hyperactivity, and stereotypic behaviors. However, no significant differences emerged for parent ratings of inappropriate speech on the ABC (p = 0.136). With regard to maladaptive behaviors on the VABS-II, there were also significant group differences with the highest ratings by Cluster 3, medium ratings by Cluster 2, and the lowest ratings by Cluster 1. In addition, significant differences in parent ratings of child social impairment on the SRS emerged across the parenting stress profiles with the lowest severity ratings in the mild range on the SRS among Cluster 1, the medium severity ratings in the moderate range among Cluster 2, and the highest severity ratings in the severe range among Cluster 3.
Parent ratings at baseline across parenting stress profiles.
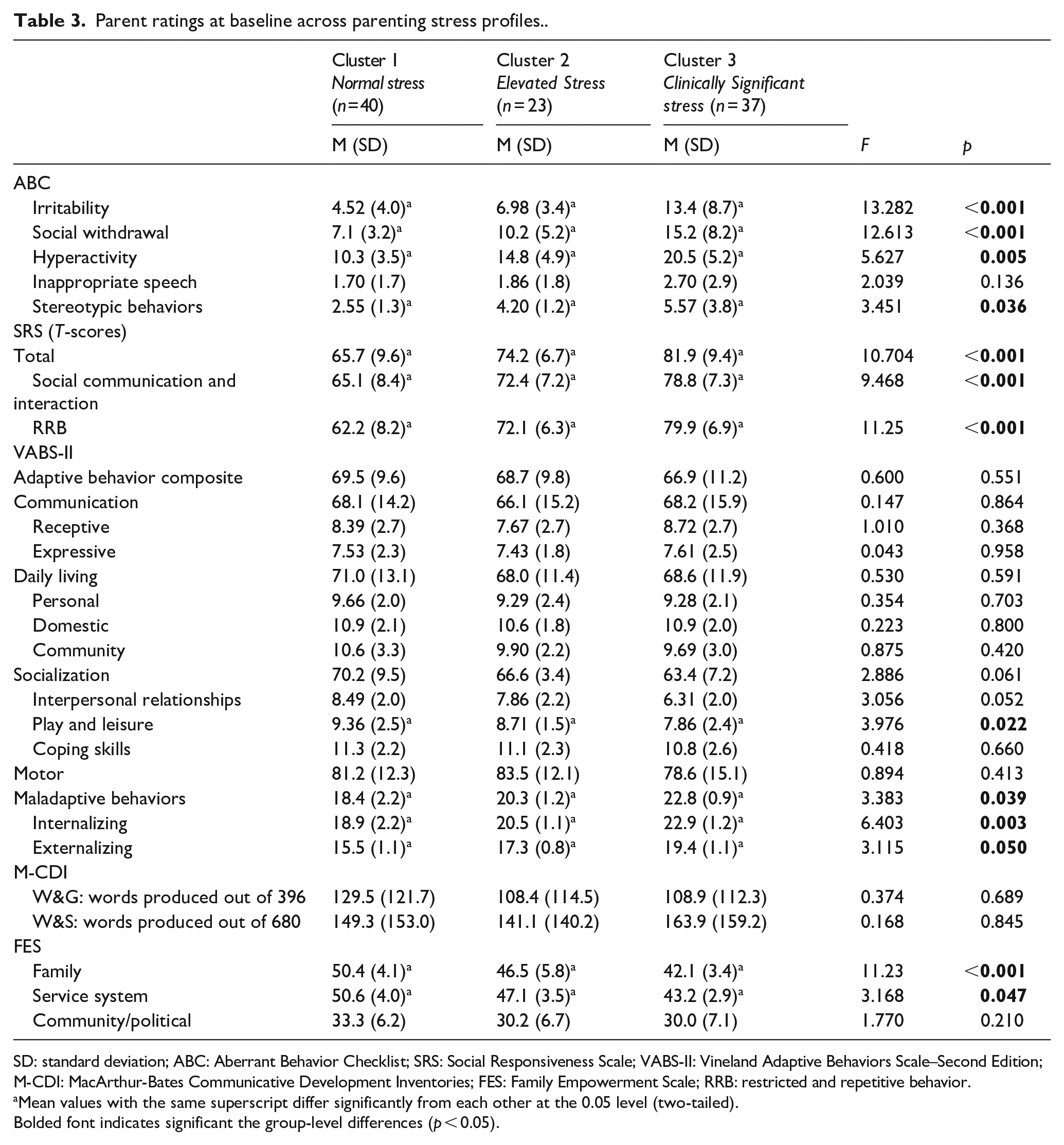
SD: standard deviation; ABC: Aberrant Behavior Checklist; SRS: Social Responsiveness Scale; VABS-II: Vineland Adaptive Behaviors Scale–Second Edition; M-CDI: MacArthur-Bates Communicative Development Inventories; FES: Family Empowerment Scale; RRB: restricted and repetitive behavior.
Mean values with the same superscript differ significantly from each other at the 0.05 level (two-tailed).
Bolded font indicates significant the group-level differences (p < 0.05).
In addition, there were no significant differences in parent ratings of child receptive and expressive language on the VABS-II across the three parenting stress profiles. Similarly, parent ratings on the MacArthur CDI forms were not significantly different. In terms of other adaptive skills on the VABS-II, there were no significant group differences on parent ratings of daily living and motor skills across the parenting stress profiles. However, parent ratings of child play and leisure skills were significantly different such that the highest ratings were provided by Cluster 1 (normal stress), the medium ratings by Cluster 2 (elevated stress), and the lowest ratings by Cluster 3 (clinically significant stress).
Divergent ratings emerged at the family and service system levels of empowerment on the FES with parents in Cluster 1 (normal stress) reporting the highest empowerment, parents in Cluster 2 (elevated stress) reporting the medium empowerment, and parents in Cluster 3 (clinically significant stress) reporting the lowest empowerment. There were no significant differences across clusters in empowerment at the community/political level (p = 0.210).
Clinician-rated measures compared across parenting stress profiles
In contrast to the pattern observed in parent ratings, clinician ratings of child maladaptive behaviors (CGI-S) and severity of social impairment (ADOS) including total, social affect, and restricted and repetitive behavior (RRB) scores were similar across the parenting stress profiles (see Table 4). In terms of language, clinicians provided similar ratings of child abilities in auditory comprehension (p = 0.384) and expressive communication on the PLS-4 (p = 0.670) and, like parents, clinician ratings did not vary in relation to parenting stress profile. Similarly, there were no differences in clinician ratings for total functional utterances (p = 0.805) and spontaneous utterances (p = 0.287) on the SLO. Furthermore, clinician ratings of child cognitive abilities on the MSEL—full-scale (p = 0.830), nonverbal (p = 0.852), and verbal DQ (p = 0.789)—did not differ across the parenting stress profiles.
Clinician ratings at baseline across parenting stress profiles.
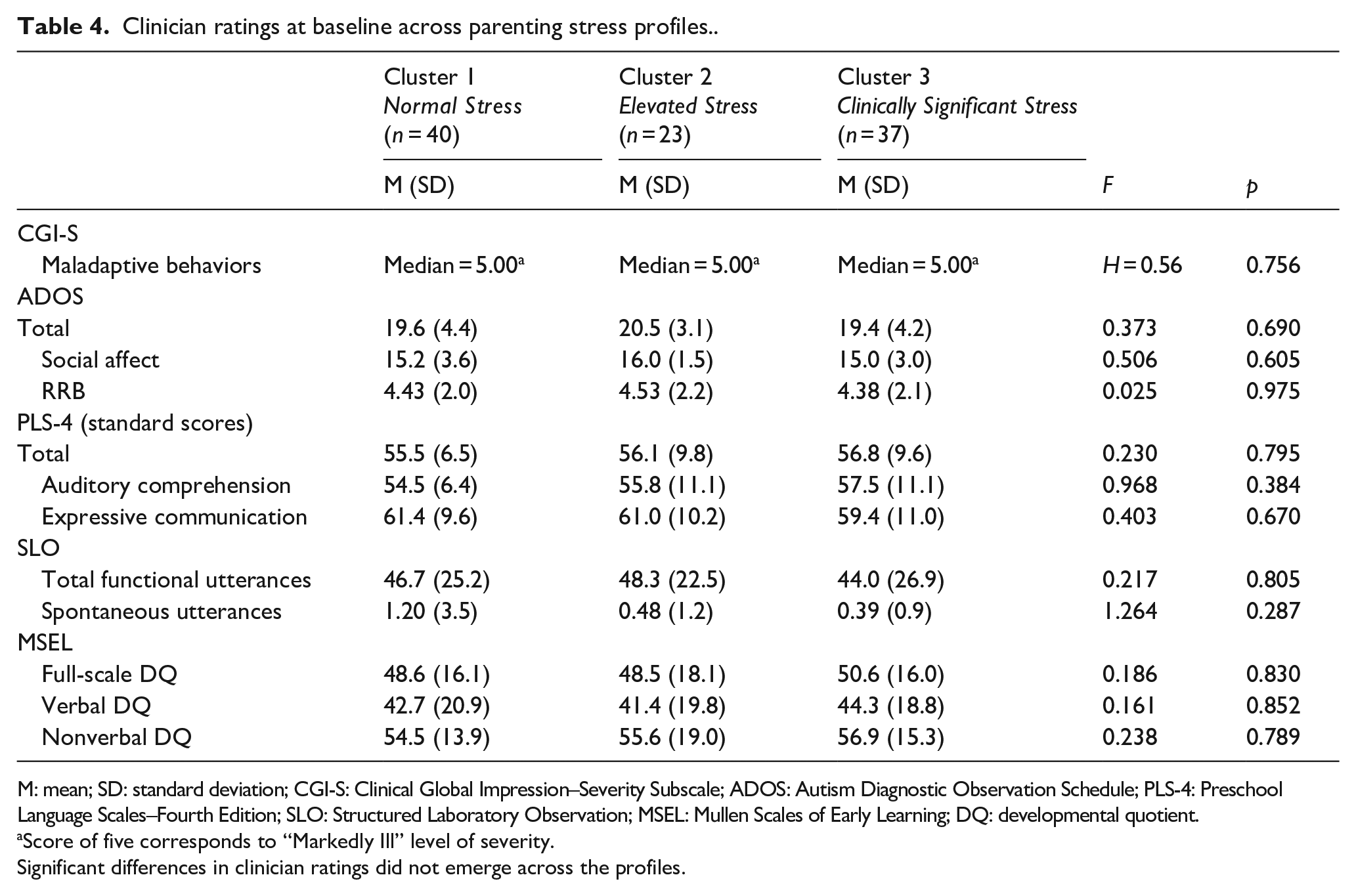
M: mean; SD: standard deviation; CGI-S: Clinical Global Impression–Severity Subscale; ADOS: Autism Diagnostic Observation Schedule; PLS-4: Preschool Language Scales–Fourth Edition; SLO: Structured Laboratory Observation; MSEL: Mullen Scales of Early Learning; DQ: developmental quotient.
Score of five corresponds to “Markedly Ill” level of severity.
Significant differences in clinician ratings did not emerge across the profiles.
Discussion
Although parents of children with ASD play vital roles in early interventions, they experience elevated stress that may inadvertently influence parent-rated measures. This study explored parenting stress among 100 parents of children with ASD and observed distinct parenting stress profiles, even among parents of children with the same diagnosis presenting for the same treatment. Significant relationships between parenting stress profiles and parent-rated measures were observed in certain domains (e.g. problem behaviors, social impairment, and parental empowerment), but not others (e.g. language and daily living skills). While parent ratings of problem behaviors and social impairment differed according to parent stress profile, available clinician-rated measures of these same functional areas (problem behaviors and social impairment) did not differ across the three clusters. Like parents, available clinician-rated measures of language ability did not differ by parent stress profile. Findings suggest that the level of parenting stress might affect parent ratings of child problem behaviors, social impairment, and parental empowerment, but not parent ratings of child language and daily living skills. These findings have important implications for researchers and clinicians working with parents of children with ASD and utilizing parent-rated measures to track treatment efficacy.
Findings from this study suggest that the experience of parenting stress may be diverse across parents of children with the same diagnosis and similar needs. Interestingly, the cluster analyses identified three unique profiles of parenting stress with group means similar to clinical cutoffs for the PSI-SF such that the mean of Cluster 1 fell in the normal range, Cluster 2 fell in the elevated range, and Cluster 3 fell in the clinically significant range. When comparing group membership by mean cluster scores and established PSI-SF cutoff scores (Abidin, 1995), 96 parents exhibited similar membership (i.e. parents in both the normal stress cluster and normal range on the established cutoff). These findings may further validate the cutoffs identified in the present investigation instead of a dichotomous structure of at or below 85%. This expanded approach may better capture the range of treatment needs and enhance characterization of parenting stress within and across populations (Barroso et al., 2016; Reed & Osborne, 2013). It would be important for future studies of parenting stress to consider an approach using the expanded cutoffs for parenting stress, particularly when trying to identify variables that may influence parenting stress.
With regard to parent ratings of child functioning, it appears that problem behaviors and social impairment differed depending on a parent’s stress profile, yet ratings of language and adaptive skills were less influenced by stress. Specifically, parent ratings of child problem behaviors (ABC and VABS-II) and social impairment (SRS and VABS-II) exhibited a unique, graded pattern depending upon stress profile—the highest stress and most negative parent ratings, the medium stress and medium parent ratings, and the lowest stress and most positive parent ratings. Ratings of child inappropriate speech (ABC) did not differ across parenting stress profiles. A positive relationship between parenting stress and child problem behaviors in ASD has been well-documented (Giovagnoli et al., 2015; Peters-Scheffer et al., 2012). However, the examination of ratings across stress profiles has not been explored and findings may provide a more nuanced understanding of this relationship given the graded pattern observed. The relationship between parenting stress and child social impairment appears mixed in the literature (Foley Nicpon et al., 2010; Lopata et al., 2016). Findings from this study may provide insight into this complex relationship. Future studies should rely on teacher-rated measures and/or performance-based, objective measures to help clarify this potential relationship.
In contrast to the graded pattern observed among parent ratings, there were similar ratings of child problem behaviors and social impairment by clinicians on available measures of these functional areas across the parent stress profiles. This discrepancy between patterns of associations in parent and clinician ratings and parenting stress profiles emphasizes the complex relationship between parenting stress, child problem behaviors, and social impairment. Discrepancies between raters have been similarly observed between parents and other professionals (e.g. teacher and clinician) in other studies of problem behaviors using the same measures across raters (Lane et al., 2013; Macintosh & Dissanayake, 2006) and social impairment (Azad et al., 2016; Blacher et al., 2014; Jepsen et al., 2012; Kaat et al., 2013).
Relationships between parenting stress, problem behaviors, and social impairment are complex and transactional in nature (Giovagnoli et al., 2015; Peters-Scheffer et al., 2012). While it is possible that certain types of problem behaviors or social skill deficits may cause more parenting stress and available clinician-rated measures may not be sensitive enough to detect these differences, it is also possible that parents experiencing heightened stress may be more likely to perceive a greater severity of problem behaviors and social impairment. Findings from this study may provide preliminary support for the hypothesis that greater parenting stress is associated with higher ratings of problem behaviors and social impairment given that children were rated similarly by clinicians on alternative indices of maladaptive behaviors (CGI-S), autism severity (ADOS), developmental level (MSEL), and language abilities (PLS-4 and SLO). Clinicians and researchers considering the use of parent-rated measures of problem behaviors and social impairment could therefore consider accounting for parenting stress in study design, measurement, and/or analyses.
Parent ratings of child language abilities across two parent-rated measures did not fluctuate across parenting stress profiles, which confirmed our second hypothesis and mirrored findings in the literature (Nordahl-Hansen et al., 2013; Volden & Phillips, 2010). While all participants in this study had significant language delays, this finding indicates that ratings of language ability may be minimally susceptible to the influence of parenting stress. An investigation of ratings from parents and clinicians among children with language disorders or other developmental disabilities may further clarify this finding. However, the same graded pattern of parent ratings emerged for social communication impairment on the SRS, which supported the relationship between parenting stress and social impairment (Brei et al., 2015; Estes et al., 2013). This may tentatively suggest that the social use of language, rather than the quantity of words understood or produced, is an important variable in understanding parenting stress in ASD.
Many domains of child adaptive skills (e.g. motor and daily living skills) were rated similarly by parents regardless of their parenting stress profile, which suggests that parent-rated measures of certain adaptive skills may also be minimally influenced by parenting stress (Estes et al., 2013; Hastings et al., 2005; Lane et al., 2013). However, this finding is limited by the lack of a comparable measure as rated by clinicians. In contrast, an inverse relationship emerged between parenting stress profiles and parent ratings of social adaptive skills such that parents with the highest parenting stress reported the lowest social adaptive behaviors. Although no studies have explicitly examined parenting stress profiles and ratings of adaptive skills, several studies observed a similar relationship between higher parental stress and lower ratings of social adaptive skills (Giovagnoli et al., 2015; Tomanik et al., 2004). A similar graded pattern of parent ratings emerged and may provide further support for the conceptualization of parenting stress as a multifaceted construct. This may be particularly important for researchers and clinicians implementing social skills programs for youth with ASD as parenting stress may influence parent perceptions of socialization abilities.
Finally, a graded pattern of ratings emerged for parental empowerment at the family and service system levels. Although an inverse relationship between parenting stress and empowerment has been identified in the literature (Minjarez et al., 2013; Weiss et al., 2012, 2015), a more detailed understanding of this relationship may be afforded by examination of parenting stress profiles. Surprisingly, multiple graded patterns of parent ratings emerged on various measures, even though clinicians rated the developmental level of children to be similar. This may suggest that child developmental level does not influence parenting stress, which is consistent with other studies (Davis & Carter, 2008; Giovagnoli et al., 2015). Given this, clinicians working with children with ASD of diverse developmental abilities may observe differential parenting stress among parents. Parents of children with ASD and varying developmental levels may benefit from psychoeducation about parenting stress and associated factors (e.g. social impairment, but not developmental ability), coping skills, and stress management techniques unique to the experience of parenting a child with ASD.
Clinicians alike would benefit from similar training to understand the diversity of stress experiences in parents of children with ASD, complexities of the parenting experience, and the ways in which stress may or may not influence parent perceptions of their child. A deeper exploration of parent and family factors (e.g. cultural influences and family traditions) and their association with parenting stress and empowerment is warranted. Similarly, an investigation into the role of clinician factors (e.g. previous training, ethnicity/race, and knowledge about parenting experiences in ASD) in their ratings of children with ASD is an important future direction.
There are several limitations of this study that warrant discussion. First, parents and clinicians completed different measures and direct comparisons between raters could not be made. As such, findings are preliminary and may only provide a global understanding of these graded relationships between parenting stress profiles and ratings. Future investigations should compare ratings between raters on identical measures and the extent to which parenting stress may or may not be associated with rating discrepancies. Second, the sample was moderately sized, and investigations with larger samples are warranted. Third, while we report information about the validity and reliability of each scale from prior published literature when available, we did not analyze item-level data for reliability within our sample. Fourth, expert clinicians completing the CGI-S incorporate some parent input into their ratings, and thus, this measure is not as objective as other direct clinician-administered measures (e.g. PLS-4). Finally, this study included measures at a single timepoint and do not afford insight into how parenting stress profiles may influence ratings of treatment outcome over time.
Collectively, findings suggest that perspectives of child functioning offered by parents can be interpreted in the context of an understanding of parenting stress. This may be particularly important for parent-rated measures of certain child characteristics (e.g. problem behaviors, social impairment, and social adaptive skills) which appear to be consistently associated with parenting stress level. It appears that a parent’s profile of parenting stress may provide a nuanced understanding of the relationship between parenting stress and parent-rated measures, with important implications for studying the efficacy of early interventions and monitoring treatment change in clinical work. Specific accommodations in study design, measurement, and analyses should be considered when working with parents of young children with ASD to account for parenting stress and its potential influence. These accommodations are relevant to research investigations in general and for clinical trials in particular.
Footnotes
Acknowledgements
The authors gratefully acknowledge the families for their participation. The authors are thankful for the contributions of Rachel Schuck, Maria Estefania Millan, Robin Libove, Christina M Ardel, Dr Jennifer M Phillips, Dr Kari Berquist, Dr Mendy Minjarez, and other members of the research team at the Stanford Autism and Developmental Disorders Research Program (ADDRP).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project utilized data from two published trials of Pivotal Response Treatment (PRT) conducted at Stanford University (Gengoux et al., 2019; Hardan et al., 2015). The first PRT trial (Hardan et al., 2015) was supported by an Autism Speaks Treatment Grant (#5773; PI: Hardan); the foundation was not involved in the trial. The second PRT trial (Gengoux et al., 2019) was supported by a grant from the National Institute on Deafness and Other Communication Disorders (DC01368902; PI: Hardan) and from the National Institute of Mental Health K01 Mentored Research Scientist Development Award (MH102428; PI: Abrams). Data management for both trials was supported by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health through grant UL1 TR001085.