
Abstract
Despite consensus on the importance of early detection and intervention for autistic children, health disparities exist, limiting access to timely services. One specific service type in the United States is Individuals with Disabilities Education Act, Part C Early Intervention programs, which are federally funded interventions for children birth-to-three with developmental delays. This study aimed to assess access to Part C, Early Intervention services for children who were evaluated for autism spectrum disorder and to examine factors that predicted parent-reported access to these services. This study extracted sociodemographic and service access data from the medical records of 709 children aged 12–40 months who were evaluated for autism spectrum disorder. Results showed that only 50% of the sample had reportedly accessed Part C, Early Intervention services. Those who identified as Black had decreased odds of having accessed Part C, Early Intervention, relative to those who identified as White, while those with a lower age of first parent concern had increased odds of having accessed Part C, Early Intervention. When inputting the independently significant variables into the model, both variables, identifying as Black and a lower age of first concern, remained significantly associated with accessing Part C, Early Intervention. Future work should investigate how these disparities come to be.
Lay abstract
Health disparities are defined as preventable differences in the opportunities to achieve optimal health outcomes experienced by marginalized and underrepresented communities. For families with autistic children, health disparities limit accessing early intervention services—which have been found to improve quality of life and other outcomes. One specific early intervention service in the United States is Individuals with Disabilities Education Act, Part C Early Intervention programs, which are federally funded interventions for children birth-to-three with developmental delays. This study adds to this topic by examining which factors impact accessing Part C, Early Intervention services for children who were evaluated for autism. Results showed that only half of the sample received these services despite there being concerns about development for all children. In addition, results showed that those who identified as Black had decreased odds of having accessed Part C, Early Intervention compared to those who identified as White. These results suggest that there are disparities when it comes to accessing important early intervention services that may be negatively impacting the Black autistic community.
Introduction
Over the last decade, the prevalence of autism has risen substantially, with the Centers for Disease Control and Prevention (CDC) currently estimating a prevalence of 1 in 36 children (Maenner et al., 2023). During this same time, research has shown that early detection and intervention are crucial to support developmental outcomes, educational and vocational opportunities, and quality of life (Dimian et al., 2021; Elder et al., 2017; Zwaigenbaum et al., 2015). A crucial avenue for accessing these services in the United States is the Individuals with Disabilities Education Act (IDEA) Part C, Early Intervention (EI) systems (IDEA, 2004), which are federally funded to provide therapeutic services to children birth to 3 years of age with developmental delays. This means that they are provided at no cost to families and the agencies are required to provide an assessment and subsequent services once a referral is made. Part C EI services are available to children before they have received a medical diagnosis of autism, constituting a crucial window for the receipt of services to begin as early as possible.
Overview of treatment disparities
Although early access to intervention for autism is important, research continues to reveal marked treatment disparities (Angell et al., 2018). That is, families from marginalized groups experience more barriers to accessing EI, begin intervention at a later time point, receive fewer and lower quality intervention services, and report less satisfaction with the services that are received (Dallman et al., 2021; Zablotsky et al., 2017). These disparities persist, even when controlling for insurance by only looking at the services accessed by children enrolled in Medicaid—or the medical assistance program in the United States that helps cover medical bills for individuals with limited income or resources with state or federal funds (Bilaver et al., 2021). In response, there has been growing interest in evaluating factors that contribute to treatment disparities for certain marginalized groups, as this understanding may lay the foundation for more equitable service delivery models that explicitly address these factors. It is important to note that the factors that contribute to treatment disparities are complex, intersectional, and rooted in systems that facilitate structural racism (Straiton & Sridhar, 2022). For example, persistent unjust practices like redlining—or discriminatory housing practices—and segregation have led to long-term decreased financial investment in community resources for low-income neighborhoods that tend to be composed of families of color (Aylward et al., 2021). Divestment in these communities and in families of color has been accompanied by a history of research excluding and/or causing harm to these communities, leading to healthcare mistrust and the development of evidence-based practices for educated, resourced, and White families (Broder-Fingert et al., 2020) that are delivered. It is important to note that a comprehensive review of factors contributing to autism treatment disparities has been documented elsewhere and is outside the scope of this article (Angell et al., 2018; Bishop-Fitzpatrick & Kind, 2017; Straiton & Sridhar, 2022). Here, we briefly review some factors known to contribute to autism treatment disparities, including early access to an autism diagnosis, age of first parental concern, English language proficiency, and socioeconomic status (SES).
The timing of an autism diagnosis is one factor that drives treatment disparities, as many specialty autism services in the United States (e.g. applied behavior analysis) require having a medical diagnosis of autism to access insurance coverage. The CDC has recently identified a higher prevalence of autism in Black and Latinx 8-year-old children compared to White children (Maenner et al., 2023). However, disparities still emerge when closely evaluating autism service access across all stages of the diagnostic and treatment process. For example, for Latinx children, prevalence estimates vary based on English proficiency, with limited English proficiency being associated with drastically lower prevalence rates (Jo et al., 2015). Black children are significantly less likely than White children to receive an autism diagnosis before 36 months (Maenner et al., 2020) and are more likely to have a co-occurring intellectual disability, suggesting that Black children with milder presentations of autism may be missed (Maenner et al., 2023). Similarly, children from Latinx communities with no prior enrollment in services, and public insurance are also less likely to be referred to a diagnostic evaluation by their primary care provider after a positive autism screen on the Modified Checklist for Autism in Toddlers—Revised (Kuhn et al., 2021).
Driving factors for treatment disparities
In addition to a delayed autism diagnosis, a number of factors may contribute to autism service disparities, including differences in how and when parents express concern about their child’s development (Daniels & Mandell, 2014; Matheis et al., 2017). The age at which caregivers first express concern about their child’s development is a well-studied factor that is influenced by cultural variation in how child development is viewed and expressed to providers. Specifically, Black parents have been shown to be less likely to report autism-related concerns than White parents, though these groups do not differ in their likelihood of expressing non-autism developmental concerns. Similarly, research has shown that while Latinx mothers will report general developmental delays, they are less likely than White mothers to report autism-specific concerns (Angell et al., 2018). Other research demonstrated that White caregivers are more likely to believe their child had autism during the evaluation process when compared to Black or Latinx caregivers (Azad et al., 2022).
Although there may be some variability in how and when caregivers express concern about their child’s development, it is important to note that most parents have already expressed concern to a provider about their child’s development before their child is 3 years old (Zablotsky et al., 2017). However, parental concern may not be a sufficient precursor to accessing diagnostic and treatment services for families from marginalized groups. Recent research has found that nearly 36% of Black families report experiencing a significant wait to receive an ASD evaluation, with 27% of families reporting needing to see 3–5 professionals prior to a diagnostic evaluation and 14% reporting visiting more than 6 professionals prior to a diagnosis (Constantino et al., 2020). Latinx parents report similar experiences, enduring multiple visits to providers prior to accessing evaluation services (Iland et al., 2012; Zuckerman et al., 2014).
In addition to parental concern, factors such as English language proficiency, SES, and insurance type may intersect with a family’s race and ethnicity to influence access to EI services. Research has demonstrated that Latinx families with low English proficiency in the United States face increased barriers to accessing autism treatment and report having more unmet therapy needs (Zuckerman et al., 2017). For example, children of non-English-speaking households report receiving fewer hours of individual intervention services than those from English-speaking households (Nguyen et al., 2016). The dearth of Spanish-speaking licensed psychologists in the United States further exacerbates barriers to care as Latinx families report this lack of Spanish-speaking providers as a major reason for their difficulty navigating and accessing services (Angell et al., 2018). Workforce issues are also notable within Black communities (Broder-Fingert et al., 2020), and may contribute to families accessing fewer and lower quality services or being less satisfied with their provider relationships (Aylward et al., 2021).
Finally, research examining the role of socioeconomic factors on autism treatment access has been somewhat mixed. After obtaining a diagnosis, higher gross family income has been identified as increasing service utilization for families with autism (McIntyre & Zemantic, 2017). Higher maternal education has also been linked to greater knowledge about autism services and, thus, service access (Pickard & Ingersoll, 2016), and may affect how caregivers recognize development differences and navigate healthcare systems (Aylward et al., 2021). On the other hand, more recent research has identified public health insurance, often associated with lower SES, as being related to increased access to autism services, likely as a result of expanded Medicaid waivers for autistic children and their families (Zhang & Baranek, 2016). Although Medicaid waivers have reduced the unmet service needs reported by Black families, it is important to note that the unmet service needs of Latinx families have persisted (LaClair et al., 2019) and limited research has compared the quality of autism services associated with Medicaid waivers versus those accessed through private insurance.
The vast majority of research to date has examined disparities as they relate to accessing autism specialty services after a medical diagnosis has been obtained. It has yet to examine the extent to which treatment disparities may exist prior to obtaining an autism diagnosis. This is an important gap, given recent research to suggest that many children, including those from marginalized backgrounds, receive services prior to obtaining a medical diagnosis of autism (Constantino et al., 2020). As such, it is important to consider the receipt of treatments within systems that serve young children with developmental delays prior to an autism diagnosis, such as the Part C, EI system. EI services are particularly important to study because these services are federally mandated for children birth through 36 months of age with developmental delays (IDEA, 2004), and as many as 10% of children who receive EI services eventually obtain an autism diagnosis, making it a first-line intervention for this population (Eisenhower et al., 2021). Given that the average age of diagnosis is 49 months (Maenner et al., 2023), EI services may help to support developmental outcomes before a child is seen for a diagnostic evaluation. In addition, EI has emerged as a potential setting for the successful deployment of early and iterative screening for autism that may particularly help in providing timely diagnostic services for marginalized communities (Wallis et al., 2020). Finally, autistic children of marginalized background face barriers in accessing services well into the school years (Suhrheinrich et al., 2021) and having accessed EI may help in streamlining service access during those subsequent years.
Present study
Despite a growing interest in the EI system as a point of treatment access, little is known about the extent to which disparities exist in accessing EI services specifically for young children with an increased likelihood of having autism. Instead, research has shown that, broadly speaking, Black toddlers are less likely to be enrolled in EI services than White toddlers (Feinberg et al., 2011; Rosenberg et al., 2008), with non-White children less likely to be referred to EI prior to developmental screening (Wallis et al., 2020). The goal of this study was to address the gaps outlined above by examining disparities in parent-reported EI service utilization among children with an increased likelihood of having autism. Specific aims include examining (1) the proportion of children who accessed EI service prior to an ASD-specific diagnosis, and (2) whether reported EI service access is predicted by various implicated sociodemographic factors, including a child’s race, ethnicity, their caregivers’ age of first concern, insurance type, sex, and home language. Given the importance of EI services in providing foundational support to young children with or without an increased likelihood of having autism, it is important to understand factors that may predict access to these services.
Methods
Procedures
This study included a retrospective review of the medical records of children aged 12–40 months (M = 29.02 months) evaluated at an autism-specific diagnostic clinic between March 2019 and October 2020 (N = 706). The diagnostic clinic is located within a children’s hospital and serves primarily children from the larger metro area. Data were gathered from the intake questionnaire collected at the time when families make the request for an autism diagnosis. At this time, caregivers indicate sociodemographic data as specified below and whether they had ever accessed EI services for their child. All diagnostic evaluations are completed by licensed psychologists who had the discretion of selecting assessments they deemed most appropriate. Therefore, not all children had the same diagnostic assessments completed. However, additional data, including all diagnostic outcomes of the evaluation, were also obtained from the electronic medical record. The Children’s Healthcare of Atlanta institutional review board approved all procedures used in this study.
Participants
Participants included in this study were N = 706 children who completed an intake questionnaire and an evaluation (at least one autism-specific measure completed, and some cognitive measures completed) at an autism specialty clinic. Children were included if they were under the age of 40 months at the time of their diagnostic evaluation. This age range was selected because the average length of time from intake to diagnostic evaluation is approximately 4 months. Setting an upper age limit at 40 months helped to ensure that all participants were 36 months or younger at the time of intake, in which they were reporting on EI service access.
Measures
Sociodemographic data included child race, ethnicity, sex, home language, insurance, and age of first parental concern. These variables were extracted from the intake questionnaire families complete prior to their diagnostic assessment. In the United States, where these data were collected, the census follows the standards set by the U.S. Office of Management and Budget in 1997 (Standards for the Classification of Federal Data on Race and Ethnicity, 1997) which suggests that data on Hispanic origin and race be collected in two separate questions. Thus, this study utilized the same format. Families who identified their child as being American Indian, Asian, and Mixed Race represented a small proportion of the current sample (0.01%, 0.04%, and 0.11%, respectively) in comparison with families identifying their child as Black or White. As such, these racial categories were collapsed in an “other” category to increase analytic power. Ethnicity was coded as Hispanic and not Hispanic. Child sex was coded as male and female. Caregivers reported the age in months that they were first concerned about their child’s development. This constituted the “age of first concern” variable. Home language was recoded to English and non-English. English comprised any family who listed English as their primary language. Non-English comprised any family who listed any other language as their primary language. Families who included more than one language as the primary language, and English was one of them, were coded as English. Insurance type was recoded as Medicaid and non-Medicaid. All insurance companies that were part of Medicaid or Medicare were coded as Medicaid. All others were coded as being non-Medicaid insurance, including Care Managment Orgainzations (CMOs; Aetna, Blue Cross Blue Shield, Amerigroup). Finally, parents reported whether their child had ever accessed EI services by the time of the evaluation.
Statistical methods
All statistical analyses were completed in SAS v.9.4 (Cary, NC), and statistical significance was evaluated two-sided at the 0.05 threshold. Bivariable logistic regression was used to determine whether variables of interest were individually predictive of having reported accessed Part C, EI services. Once variables were examined independently, all variables that were statistically significant were placed into one multivariable logistic regression model interpreted. Multicollinearity for predictors was assessed throughout by examining Spearman correlations and variance inflation factors and it was not found to be of concern. Final regression results are reported as odds ratios for early EI accessed, with respective 95% Wald confidence intervals (CIs) and p values.
Community involvement statement
This study included a retrospective chart review of medical records of children who were evaluated for autism. Stakeholders were not involved in other aspects of the research project.
Results
Sample characteristics
The sample was 74.5% male, and 86.5% of the sample received a diagnosis of autism during the evaluation. In terms of race and ethnicity, the sample was 36.5% Black and 17.4% Hispanic/Latinx; 16% of all children in the sample were enrolled in Medicaid, and 50% of all children in the sample reported being enrolled in Part C, EI services at the time of their diagnostic evaluation. There were no omnibus statistical differences in sex, ethnicity, or insurance type between the sub-sample of toddlers whose parents reported enrollment in EI and those whose parents reported not being enrolled. Similarly, there were no statistically significant differences in cognitive ability scores between toddlers who were enrolled in EI and those who were not. See Table 1 for sample characteristics.
Summaries, bivariable, and multivariable binary logistic regression models for EI, considering children sociodemographic and clinical characteristics.
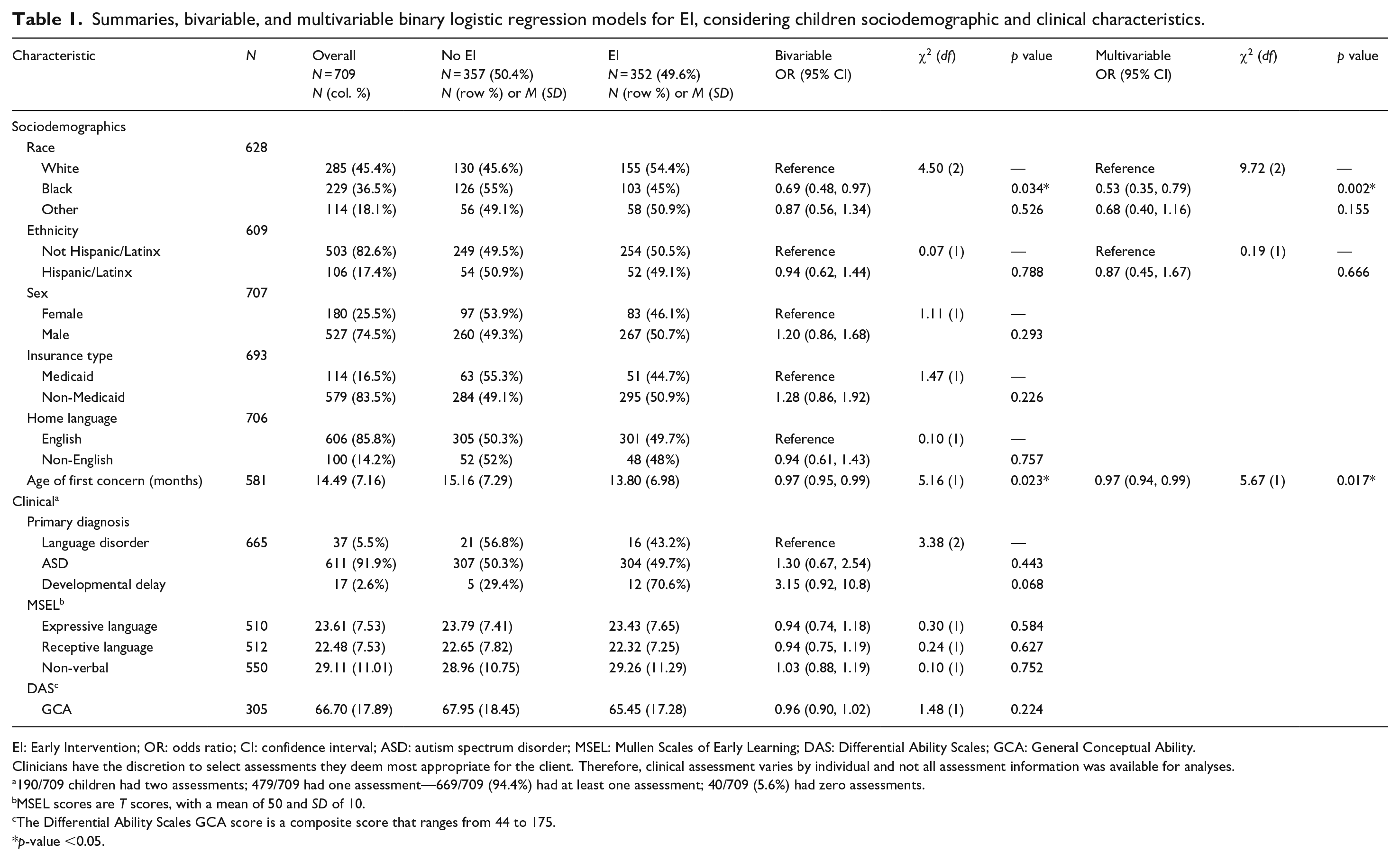
EI: Early Intervention; OR: odds ratio; CI: confidence interval; ASD: autism spectrum disorder; MSEL: Mullen Scales of Early Learning; DAS: Differential Ability Scales; GCA: General Conceptual Ability.
Clinicians have the discretion to select assessments they deem most appropriate for the client. Therefore, clinical assessment varies by individual and not all assessment information was available for analyses.
190/709 children had two assessments; 479/709 had one assessment—669/709 (94.4%) had at least one assessment; 40/709 (5.6%) had zero assessments.
MSEL scores are T scores, with a mean of 50 and SD of 10.
The Differential Ability Scales GCA score is a composite score that ranges from 44 to 175.
p-value <0.05.
Analyses
Bivariable logistic regression was used to analyze the relationship between race, ethnicity, sex, age of first concern, home language, and health insurance type on the odds of having accessed EI services. Results revealed that only race and age of first concern were independently related to having accessed EI services (p < 0.05). The odds of having accessed EI services were 31% lower for Black families and their children than White families (95% CI = (0.48, 0.97)). For all children, the odds of having accessed EI services decreased by 3% for every 1-month increase in age of first concern (95% CI = (0.95, 0.99)). See Table 1 for results.
Multivariable logistic regression was then used to collectively analyze the relationship between race and age of first concern on the probability of having accessed EI services. It was found that holding age of first concern constant, the odds of having accessed EI services were 39% lower for Black families and their children (95% CI = (0.42, 0.90)), compared to White families and their children. Concurrently, the relationship between age of first concern and having accessed EI services did not change, after controlling for race.
A second set of follow-up analyses included only children who were diagnosed with autism to determine if findings held true for this narrower sample. In this narrower sample, only 50% of children reported having accessed EI prior to their diagnostic evaluations. Bivariable logistic regression was used to analyze the same relationships between sociodemographic variables and the odds of having accessed EI services. Results revealed that only race was independently related to having accessed EI services (p < 0.01). The odds of having accessed EI services were 40% lower for Black autistic children and their families than for White families (95% CI = (0.41, 0.87)). See Table 2 for results.
Summaries, bivariable, and multivariable binary logistic regression models for EI for children diagnosed with autism, considering children sociodemographic and clinical characteristics.
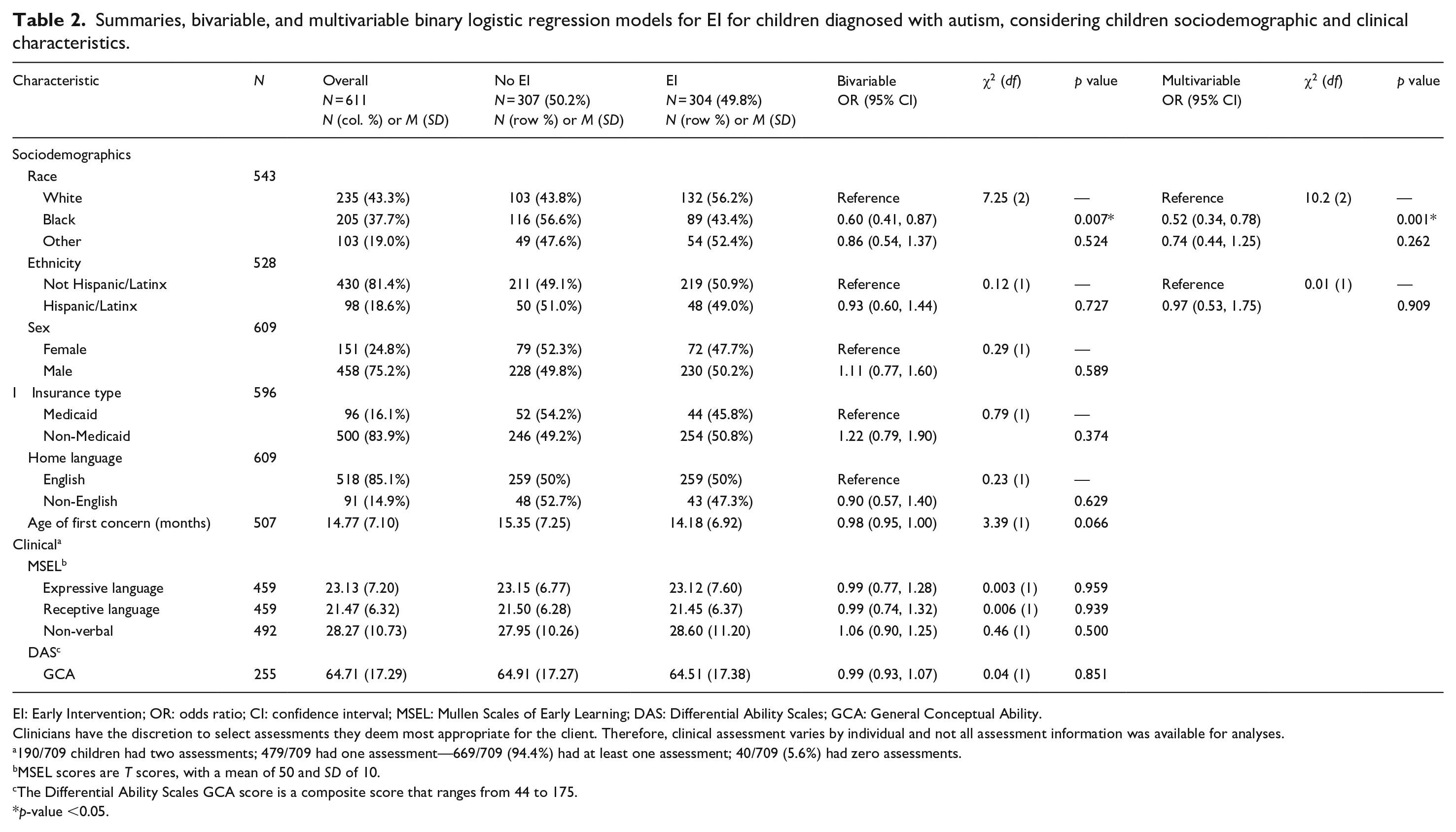
EI: Early Intervention; OR: odds ratio; CI: confidence interval; MSEL: Mullen Scales of Early Learning; DAS: Differential Ability Scales; GCA: General Conceptual Ability.
Clinicians have the discretion to select assessments they deem most appropriate for the client. Therefore, clinical assessment varies by individual and not all assessment information was available for analyses.
190/709 children had two assessments; 479/709 had one assessment—669/709 (94.4%) had at least one assessment; 40/709 (5.6%) had zero assessments.
MSEL scores are T scores, with a mean of 50 and SD of 10.
The Differential Ability Scales GCA score is a composite score that ranges from 44 to 175.
p-value <0.05.
Discussion
This study aimed to examine the proportion of children with an increased likelihood of having autism who were enrolled in Part C, EI services prior to an autism evaluation. The second aim was to identify sociodemographic characteristics that impacted reported access to EI services. The study sample included a diverse population of young children largely representative of the broader metro area, thus providing a rich ground from which to study the questions asked. Results revealed that only half of the children were receiving EI services prior to their autism evaluation. Of the sociodemographic factors examined, identifying as Black was the only factor that significantly decreased the odds of being enrolled in EI. This finding persisted, even when controlling for parental age of first concern. Of note, the odds of being enrolled in EI were also lower for Black children who were later diagnosed with autism. For this subset of children, parental age of first concern was not significantly associated with accessing EI.
This study provides important information on treatment disparities for children with an increased likelihood of having autism prior to receiving a diagnostic evaluation for autism. This is an important question to understand, given the growing recognition of the EI system being an entry point to therapeutic supports for many children who go on to receive a medical diagnosis of autism (Eisenhower et al., 2021). Although families of children with developmental delays are able to access Part C EI services irrespective of a medical diagnosis of autism, only half of the participating children were reportedly receiving EI services prior to their diagnostic evaluation, despite all children having developmental concerns that supported a referral for an autism evaluation. In fact, available data on clinical characteristics, including intellectual and developmental skills, revealed no significant differences between children who were and who were not reportedly receiving EI services. This finding persisted even when only considering children who were later diagnosed with autism—only 50% of autistic children had accessed EI services prior to their diagnostic evaluation. These children would have shown clinically significant levels of impairment in social communication and restrictive and repetitive behavior and therefore have all been eligible for EI services.
Although research has not yet examined the developmental trajectories of children who do and do not receive EI services, it is possible that delayed or no enrollment in EI services has negative consequences for child development and family well-being (Adams et al., 2013). Access to Part C, EI may also support enrollment into Part B special education services through the school system. Research suggests that 88% of children enrolled in Part C, EI go on to receive Part B services (i.e. special educations services), whereas only 46.5% of children with developmental delays receive Part B services if they were not previously enrolled in Part C EI services (Shenouda et al., 2022). Therefore, missing the opportunity to enroll in EI services can have long-term effects in the enrollment of and access to special education services after children turn 3 years old.
When investigating the unique role of sociodemographic factors on parent-reported access to EI services, race and age of first parental concern were each related to reported EI service access. More specifically, Black families reported a lower likelihood of having received EI services. This finding is largely consistent with literature demonstrating that Black children experience a number of disparities in accessing autism services, and EI services specifically (Constantino et al., 2020; Shenouda et al., 2022). However, we now know that these disparities are present within broader systems of care that support children prior to an autism diagnosis. Furthermore, the results of this study corroborate the importance of first parental concern (Angell et al., 2018). For this sample, children whose parents became concerned about their development at a younger age were slightly more likely to access EI services. Given that EI services are only available for children birth to 3 years old, it follows that those whose parents notice developmental differences earlier have more time to access those services.
It is interesting to note that when age of first concern was held constant, the likelihood of accessing EI services slightly decreased for Black children and the CI narrowed. Although it is important to note that this difference was not statistically different. This suggests that amid a handful of sociodemographic variables like health insurance type, home language, race, ethnicity, sex, and age of first concern, identifying as Black was the most significant contributor to decreased access to EI services. This finding echoes prior research that documents disparities that Black families face at every stage of seeking services for their children. These disparities are structural in nature and impacted by implicit and explicit biases (Straiton & Sridhar, 2022). Structural racism must be combatted in a number of ways, beginning with the awareness that it exists to the parties that perpetuate it, including healthcare providers who serve as the gatekeepers to EI and other services. Once the biases and structures that perpetuate racism are acknowledged, efforts aimed at increasing accessibility and equity by decreasing bias can follow.
This study did not assess the reasons driving families to not access Part C services. To that end, future research is needed to understand the referral pathways to EI services and family experiences along this pathway. More specifically, understanding how healthcare providers respond to parental concern may elucidate factors that impact how and when caregivers report developmental concern and how and when providers gatekeep referrals to EI services. In addition, even though referrals or information about EI services may be provided to families, additional research is needed to understand the many factors that caregivers weigh when deciding whether to enroll their child in EI services and the structural barriers, Part C eligibility criteria, and other factors that may interfere with enrollment. Utilizing publicly available records to examine the demographic characteristics of children flagged as having developmental delays within the primary care system as compared to census track data may also help to clarify the extent to which disparities exist within the developmental screening process versus those that may appear following screening, identification, and referral.
It is important to highlight the limitations of this study. First, although the study sample was racially and ethnically representative of the metro area, it also represented caregivers who accessed an autism-specific evaluation center prior to their child turning 3 years old. Given that most children are diagnosed with autism after age 3 years (Maenner et al., 2023), our study sample may not be representative of all children and particularly those who obtain an autism diagnostic evaluation at a later age. In addition, race and ethnicity intersect with many other marginalizing factors. While we were able to include many of these in our analyses, due to the nature of the data, we were unable to fully account for all intersecting identities. Furthermore, there are important factors that we were unable to assess. Although we examined the role of insurance status in EI service access, we were unable to examine the role of SES. Having additional variables such as gross household income, maternal education, or zip code would have provided richer information regarding the role of SES on EI service access. This study was based on parents’ report of EI service access instead of confirmed record of EI access. Thus, it may be vulnerable to errors in caregivers misremembering. However, children were included in this study who were 40 months of age or younger at the time of their evaluation, meaning that caregiver report was occurring during a period of time in which the receipt of EI services was either current or recent. Furthermore, not all parents answered every question in the intake form, meaning that there was some missing data. Analyses of missing data revealed that parents who did report the age they first became concerned about their child’s development were more likely to be non-Hispanic, English speaking, and have male children (Supplemental Table A). Finally, this study was based in the United States. Thus, both prior work and the conclusions of this study should be understood in the context of the U.S. medical and social system. Future work should examine how the political and social climates of other countries may or may not influence service access.
Despite the aforementioned limitations, this study provides valuable information about the sociodemographic factors that impact parent-reported access to EI services prior to obtaining an autism diagnosis. It adds to the literature in this area by suggesting that treatment disparities emerge prior to the receipt of an autism diagnosis and especially for Black families. These findings may corroborate recent work drawing attention to the impact of structural racism on access to care (Straiton & Sridhar, 2022). Future research studies examining referral processes, using public claims data, and understanding the structures and systems that contribute to these disparities are needed. Growing understanding in this area may support emphases on service equity by proactively supporting systemic factors that impede early access to EI services.
Supplemental Material
sj-docx-1-aut-10.1177_13623613241229150 – Supplemental material for Access to Part C, Early Intervention for children younger than 4 years evaluated for autism spectrum disorder
Supplemental material, sj-docx-1-aut-10.1177_13623613241229150 for Access to Part C, Early Intervention for children younger than 4 years evaluated for autism spectrum disorder by Adriana I. Mendez, Emma McQueen, Scott Gillespie, Ami Klin, Cheryl Klaiman and Katherine Pickard in Autism
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.