
Abstract
Autism is a lifelong condition characterized by repetitive and restrictive behaviors and differences in social communication. The reported prevalence of autism has risen exponentially in the past years. Early identification and subsequent early intervention are key to promoting better outcomes for autistic individuals. However, there is a dearth of research focusing on understanding variables that impact the age of diagnosis of autistic children in Paraguay. We collected data from 176 caregivers of autistic individuals aged 18 years or younger who lived in Paraguay and conducted a hierarchical regression analysis to understand whether demographic and clinical variables predicted the age of autism diagnosis in Paraguayan autistic children. Our results indicated that child’s age, child’s age at caregivers’ first concerns for their development, and child’s verbal skills were significant predictors of the age of autism diagnosis in Paraguay. Educating caregivers and professionals to increase awareness of autism characteristics and atypical behaviors in social communication beyond verbal skills may support the early identification of autism and subsequent access to early intervention.
Lay abstract
Autism is a lifelong condition characterized by repetitive behaviors and social communication differences. The reported cases of autism increased globally in the past years. Detecting autism early and providing appropriate supports promptly are crucial for better outcomes. Yet, little research focuses on what factors interplay in the diagnostic process of autistic children in Paraguay. We gathered data from 176 caregivers of autistic children under 18 years in Paraguay. Through a detailed analysis, we found that child’s age, child’s age at the caregiver’s first concerns about their development, and the child’s verbal skills are key in predicting the age of autism diagnosis in Paraguay. Educating caregivers and professionals about autism and social communication development can help identify autism early and provide timely support.
Autism is a lifelong condition characterized by repetitive and restrictive behaviors and differences in developing social communication skills (American Psychiatric Association [APA], 2013). The reported prevalence of autism has risen from early estimates of 10 in every 10,000 individuals (Matson & Kozlowski, 2011) to an estimate of 1 in every 36 children aged 8 years in the United States (Maenner et al., 2023). Similarly, Xu et al. (2019) reported that 2.79% of children aged 0 to 17 years had received an autism diagnosis in a large, nationwide health survey including more than 40,000 children. As autism affects people regardless of their race or ethnicity, the global prevalence of autism is also rising. Based on a review of epidemiological surveys in 37 countries, Zeidan et al. (2022) reported a global autism prevalence of 1%. Notably, researchers have reported that prevalence data from low- to middle-income countries are scarce and described difficulties in getting an exact prevalence due to the methodological variances in different places (Chiarotti & Venerosi, 2020; Elsabbagh et al., 2012; Fombonne et al., 2021).
As the prevalence of autism around the world continues to rise, emerging evidence suggests that early intervention during the first years of life has the potential to improve adaptive behavior, language, and cognitive outcomes for individuals with autism 1 (Clark et al., 2018; James & Smith, 2020). Notably, children with autism who received an earlier diagnosis and received early intervention had improved language and cognition outcomes when they reached school age compared to children with autism who received a later diagnosis (Clark et al., 2018). Thus, there have been efforts to identify autism as early as possible to provide the child the opportunity to receive early intervention (James & Smith, 2020). Researchers suggest that early signs of autism can be identified during the first and second years of age (Daniels & Mandell, 2014; James & Smith, 2020; Zwaigenbaum et al., 2015); however, there is wide variability in the age at which children receive their diagnosis, with some individuals receiving their diagnosis when they are school age, and others at adolescence, or adulthood (Avlund et al., 2021; Daniels & Mandell, 2014).
In the United States, several studies have investigated possible reasons for obtaining an autism diagnosis at a later age. Some of these factors included sociodemographic factors such as lower caregiver education, lower socioeconomic status, belonging to a minoritized group, and being a female (Avlund et al., 2021; Parikh et al., 2018). Other factors that were associated with a later autism diagnosis included clinical factors including higher language skills, average cognition, and fewer noticeable characteristics (Avlund et al., 2021). However, there is a dearth of research on factors that may impact the age of diagnosis in low- to middle-income countries, where 90% of individuals with autism live (de Vries, 2016; Samms-Vaughan, 2014). Specifically, very few studies investigated factors related to the identification and age of diagnosis of individuals with autism in Latin American countries (Montiel-Nava et al., 2024).
In a study in Colombia, Talero-Gutierrez et al. (2012) reported an analysis of data from 138 children, 83% of whom received an autism diagnosis. They reported that the average age of autism diagnosis in their sample was 45 months. Similarly, in a study conducted in Venezuela, Montiel-Nava, Chacin, and Gonzalez-Avila (2017) reported that 80% of caregivers in their sample reported some concerns for their child’s development by their child’s second birthday. The mean age of first concerns was 17 months, but the mean age of diagnosis for children with autism in this sample was 54 months. In Montiel-Nava et al.’s (2017) study, sociodemographic factors such as father’s age, mother’s age, and mother’s education level were significant predictors of the children’s age of autism diagnosis. In addition, clinical factors such as the existence of motor delays and cognition below average were also predictors of the age of diagnosis (Montiel-Nava et al., 2017). In an interview study, Ribeiro et al. (2017) interviewed 19 mothers of children with autism in Brazil to investigate the pathway from caregivers’ first developmental concerns to diagnosis. Mothers reported negative experiences related to the process of receiving their child’s autism diagnosis and their child’s age of diagnosis ranged from 39 to 197 months.
More recently, Montiel-Nava et al. (2024) collected data from 2520 caregivers of autistic children across six different Latin American countries including Argentina, Brazil, Chile, the Dominican Republic, Uruguay, and Venezuela. In their study, they collected data on the age of first developmental concerns and the age of autism diagnosis and investigated demographic and clinical predictors of the age of diagnosis. In this study, they reported that across the six countries, the mean age of diagnosis was 46.3 months (SD = 29.9), and the mean age of first concerns was 22.4 months (SD = 15.6). Among the sociodemographic factors, Montiel-Nava et al. (2024) found the age of the child with autism and type of health insurance (i.e. public, private, or both) to be significant predictors of age of autism diagnosis. Among clinical predictors, the type of diagnosis (e.g. autism, Asperger’s syndrome, pervasive developmental disorder, pervasive developmental disorder not otherwise specified), the severity of the symptoms, the language level, and medical comorbidities were reported to be significant predictors (Montiel-Nava et al., 2024).
The current study aimed to expand the small body of literature focused on understanding factors related to the identification and age of autism diagnosis in low- to middle-income countries in general, and in Latin American countries specifically, by analyzing data collected from caregivers of autistic children in Paraguay. Paraguay is a landlocked country, with approximately seven million inhabitants and classified as an upper middle-income country by the World Bank (2020), with an unknown autism prevalence. However, similar to caregivers of autistic children in other countries in the region (e.g. Argentina, Brazil, Chile, Uruguay), caregivers of autistic children in Paraguay have reported increased challenges associated with accessing diagnostic and support services for their autistic children, including services highly centralized in the capital and its surrounding area, and financial burdens associated with accessing diagnostic and support services (Paula et al., 2020; Terol et al., 2023). To our knowledge, this is the first study to investigate the age of first concerns, age of diagnosis, and related factors in Paraguay. Better understanding about autism diagnosis and its predictive factors in a specific context may aid in the creation of public policy to allocate appropriate funds to provide individuals with autism and their families with adequate health care and services (Salari et al., 2022). The following research questions guided our study:
Research Question 1. To what extent do sociodemographic factors predict a child’s age of autism diagnosis in Paraguay?
Research Question 2. To what extent do clinical factors predict a child’s age of autism diagnosis in Paraguay?
Based on previous literature, we hypothesized that demographic predictors such as caregivers’ level of education, child’s age, and geographical location will significantly predict the child’s age of autism diagnosis. In addition, we hypothesized that clinical predictors such as verbal skills, challenging behaviors, and number of early concerns will significantly predict the child’s age of autism diagnosis.
Method
Participants and recruitment
After obtaining approval from the Institutional Review Board of the University of Illinois Urbana-Champaign, we recruited participants using purposive sampling (Rumrill et al., 2020). Participants were eligible to participate if (a) they were caregivers of an individual with autism aged 18 years or younger, (b) the autistic individual had received an autism diagnosis in Paraguay, and (c) the caregiver and the autistic individual lived in Paraguay at the time of the study. Recruitment flyers in Spanish were shared on social media and via WhatsApp with professionals who worked with autistic individuals and their families. The recruitment flyer included a QR code and a link to an online screening questionnaire which included questions to confirm whether the participant met the inclusion criteria. If the participant met the inclusion criteria, they were redirected to an online consent form. After participants provided informed consent, they were redirected to an online questionnaire. Overall, 191 people started filling out the screening questionnaire. Fifteen did not meet the inclusion criteria or did not provide consent. Thus, data from 176 caregivers of autistic individuals aged 18 years or younger who live in Paraguay are included in this study. Data were collected from March to April 2023. No identifying data were collected from participants, and participants did not receive any compensation for their participation in the study. Overall, 88% of the respondents were mothers, 80% were married or living with a partner, 47% had a bachelor’s degree, and 58% lived in the capital or the central department. Caregivers reported 83% of the children to be male, 45% to have combined types of health insurance, and 83% to not have an additional medical diagnosis. The reported mean age of autism diagnosis was 46.38 months (SD = 30.80), range 12 to 192 months.
Instrument
Caregivers completed an adapted version of the Caregivers Needs Survey (Daniels et al., 2017), which was adapted to Spanish by the researchers from the Red Espectro Autista Latinoamerica network (Montiel-Nava et al., 2024; Paula et al., 2020). The instrument includes several sections including demographic characteristics of the caregiver, demographic characteristics of the autistic individual and the diagnosis process, information about access to services, and impact of the autism diagnosis on the child’s family (Daniels et al., 2017; Paula et al., 2020). Similar to what was reported by Montiel-Nava et al. (2024) and Paula et al. (2020), we further adapted this instrument to be used in Paraguay. Modifications were minor, for example, we revised the names used to refer to the different educational levels in Paraguay, we included the types of insurance and services available in Paraguay, and we added the different departments in Paraguay (i.e. geographical divisions similar to states in the United States). The survey took approximately 30 min to complete. Data reported in this article include data from the first two sections of the survey (a) characteristics of the caregivers and (b) child’s characteristics and autism diagnosis process.
Outcome variable
The outcome variable was the continuous variable of age of autism diagnosis in months. Caregivers indicated their child’s age in months when their child received a formal autism diagnosis.
Sociodemographic predictors
Five sociodemographic predictors were included in the multiple regression analysis.
Caregivers’ level of education
This was a categorical variable which included the highest level of education indicated by the caregiver who completed the questionnaire, or their spouse or partner when reported. We used a 4-category variable to measure participants’ level of education, ranging from “high school or less” to “graduate degree.” To account for the categorical nature of this variable, we created three dummy variables, with “high school or less” serving as the reference category. The dummy variables were labeled as “associate degree,” “bachelor’s degree,” and “graduate degree.”
Child’s gender
This was a binary variable. Originally, child’s gender included options such as “other” and “prefer not to say,” but none of the caregivers selected either option. To account for the categorical nature of this variable, we created a single dummy variable with a value of 1 for “male” and a value of 0 for “female.”
Age in months
This was a continuous variable. Caregivers entered their child’s date of birth in the questionnaire, and this was later transformed to their age in months based on the day the questionnaire was closed.
Geographic location
This was a binary variable. In the questionnaire, caregivers indicated their department of residency during the study. Paraguay has 17 departments which are geographical locations similar to states in the United States. However, caregivers in Paraguay have reported that services are highly centralized in the capital (i.e. Asunción) and its surrounding metropolitan area (Terol et al., 2023, under review). Thus, we created a single dummy variable with a value of 1 for “Asunción and Central,” and a value of 0 for “other geographic location.”
Type of health insurance
Type of health insurance was a categorical variable. We used a 4-category variable to measure types of insurance. To account for the categorical nature of this variable, we created three dummy variables, with “private insurance” serving as the reference category. The dummy variables were labeled as “social security insurance,” “public health,” and “combined insurance.” “Combined insurance” included those participants who selected two or more of the insurance categories (e.g. utilized both social security insurance and private insurance).
Clinical predictors
Five clinical predictors were included in the multiple regression analysis.
Age of first concerns
This was a continuous variable. Caregivers indicated their child’s age in months when they first had concerns about their children’s development.
Number of early concerns
This was a continuous variable that indicated the number of concerns that caregivers indicated they had about their child’s development from a list of 17 items spanning different developmental domains such as social communication, language, motor skills, cognition, behavior, and sensory profile.
Child’s verbal skills
This was a categorical variable. We used a 6-category variable to measure child’s verbal skills at the time they received their diagnosis ranging from “did not speak and did not use gestures to communicate” to “communicated using complex sentences.” To account for the categorical nature of this variable, we created five dummy variables, with “did not speak and did not use gestures to communicate” serving as the reference category. The dummy variables were labeled as “gestures only,” “single words,” “two-word phrases,” “simple sentences,” and “complex sentences.”
Additional medical diagnosis
This was a binary variable. In the questionnaire, caregivers indicated whether or not their child had medical diagnoses besides their autism diagnosis. Caregivers were able to select other medical diagnoses often associated with autism such as “epilepsy” or “Fragile X syndrome.” In addition, they were also given the opportunity to write other medical diagnoses. Each specific additional medical diagnosis was selected by a very small number of participants (e.g. 0.6% had aphasia). Therefore, instead of including this variable as a 13-categorical variable, we created a single dummy variable with a value of 1 for “additional medical diagnosis” and a value of 0 for “not additional medical diagnosis.” See Table 1 for additional information on the reported additional medical diagnosis of the sample.
Demographic characteristics.
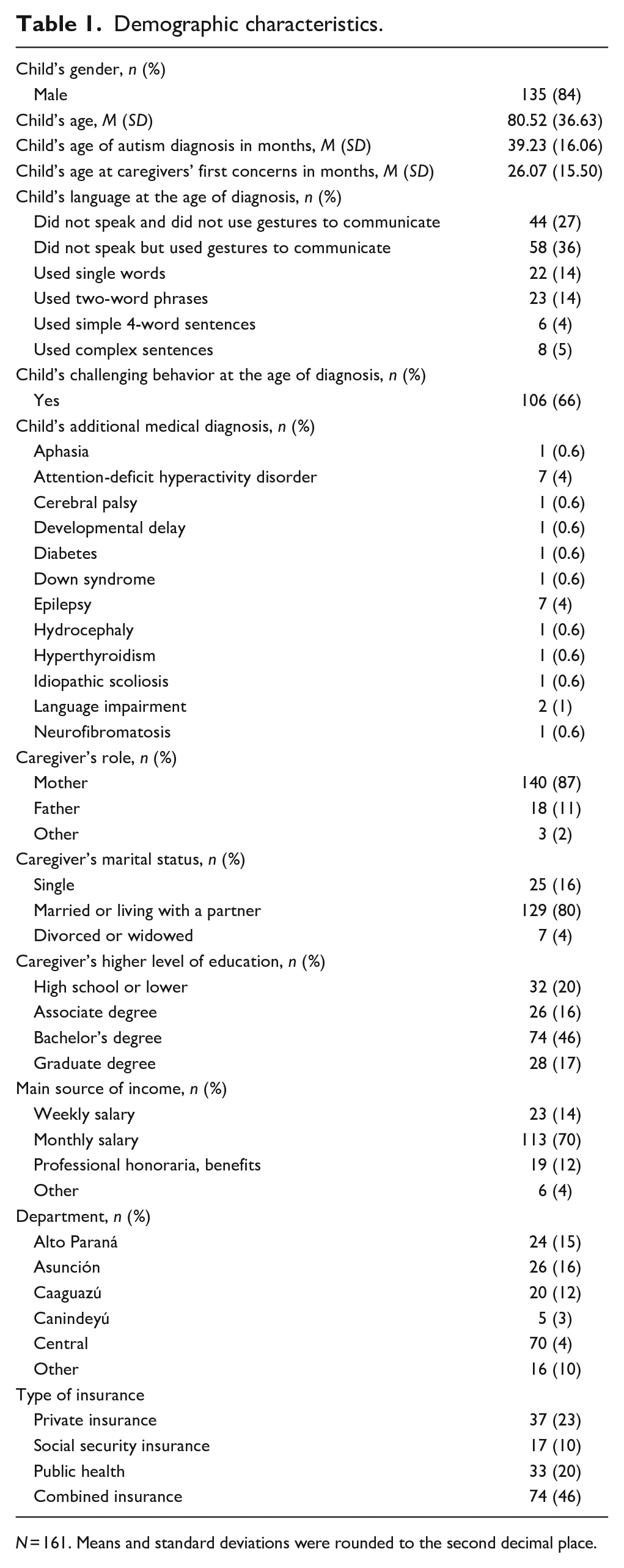
N = 161. Means and standard deviations were rounded to the second decimal place.
Challenging behavior
This was a binary variable. Caregivers were asked whether their child engaged in challenging behavior at the time when they received their autism diagnosis. Specifically, they responded to the question “Did your child have disruptive behaviors that affected his or her ability to participate in daily activities at the time he or she received their diagnosis?” To account for the categorical nature of this variable, we created a single dummy variable with a value of 1 for “yes” and a value of 0 for “no.”
Data analysis
Data were analyzed using descriptive statistics (e.g. frequencies, means, and standard deviations) to examine the demographic characteristics of caregivers and children and factors related to the age of child’s autism diagnosis. In addition, we used multiple linear regression to identify significant predictors of the individuals’ age of autism diagnosis. Specifically, we used hierarchical regression to identify the most significant variables that predict the outcome of interest, by grouping predictors in blocks and adding these blocks to the regression model (Cohen & Cohen, 1983).
Our first regression model included the five demographic predictors. In our second model, we introduced the five clinical predictors to identify which of these predictors significantly predicted the child’s age of autism diagnosis, after controlling for the demographic predictors.
Community involvement
Autistic individuals and their families were not involved in the design, data collection, and data analysis of this study. This study highlights the experiences of caregivers of autistic individuals and the process of obtaining an autism diagnosis in Paraguay.
Results
Demographic characteristics and age of diagnosis
We conducted diagnostic tests for the assumptions of multiple regression and found no violations of the assumption of non-multicollinearity, with all Variance Inflation Factor (VIF) scores below 1.8. However, the assumption of normality and homoscedasticity of the residuals was violated. Examination of the histogram of residuals revealed 15 potential outliers (out of the 176 participants), corresponding to individuals who had received their diagnosis when they were older than 100 months (range 102 to 196 months). Once we removed outliers (n = 161), we found no violations of the assumptions of normality and homoscedasticity of the residuals, and all VIFs were smaller than 1.4. Child’s age of autism diagnosis in months had a normal distribution. The dataset contains 11 missing data points (0.62%). We employed multiple imputation method for handling the missing data. Specifically, the predictive mean matching imputation approach was employed, with 10 imputed datasets, using the mice package (Van Buuren & Groothuis-Oudshoorn, 2011) in R 4.2.1 (2022-06-23). Of the participants included in the regression analysis, 87% were mothers, 80% were married or living with a partner, 46% had a bachelor’s degree, and 59% lived in the capital or the central department. Caregivers reported 84% of the children to be male. For the cases included in the regression analysis (n = 161), the mean of the child’s age of diagnosis in months was 39.23 (SD = 16.06). Table 1 shows the demographic characteristics of children and caregivers included in the regression analysis. Table 2 shows correlation coefficients between all predictor variables and the outcome variable.
Correlations between variables.
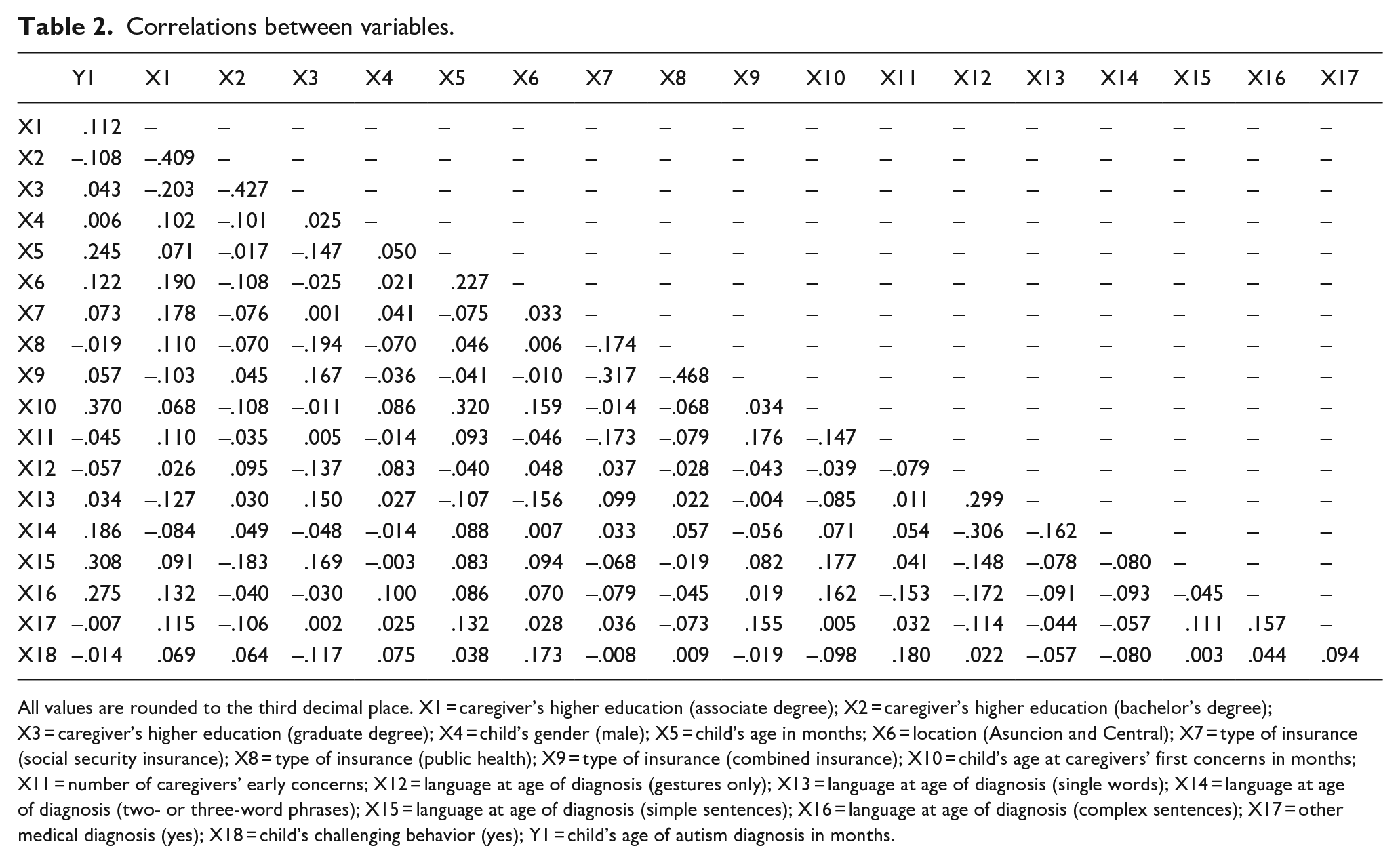
All values are rounded to the third decimal place. X1 = caregiver’s higher education (associate degree); X2 = caregiver’s higher education (bachelor’s degree); X3 = caregiver’s higher education (graduate degree); X4 = child’s gender (male); X5 = child’s age in months; X6 = location (Asuncion and Central); X7 = type of insurance (social security insurance); X8 = type of insurance (public health); X9 = type of insurance (combined insurance); X10 = child’s age at caregivers’ first concerns in months; X11 = number of caregivers’ early concerns; X12 = language at age of diagnosis (gestures only); X13 = language at age of diagnosis (single words); X14 = language at age of diagnosis (two- or three-word phrases); X15 = language at age of diagnosis (simple sentences); X16 = language at age of diagnosis (complex sentences); X17 = other medical diagnosis (yes); X18 = child’s challenging behavior (yes); Y1 = child’s age of autism diagnosis in months.
Hierarchical regression analysis
Table 1 includes the descriptive statistics of the five demographic predictors. The results of the hierarchical regression are presented in Table 3. According to the results for model 1, only the child’s age was a significant predictor (beta = 0.268, p = 0.002). Specifically, older children were more likely to receive a later autism diagnosis, after controlling for the other demographic predictors (R2 = 0.10, adjusted R2 = 0.05).
Results from hierarchical multiple regression analysis.
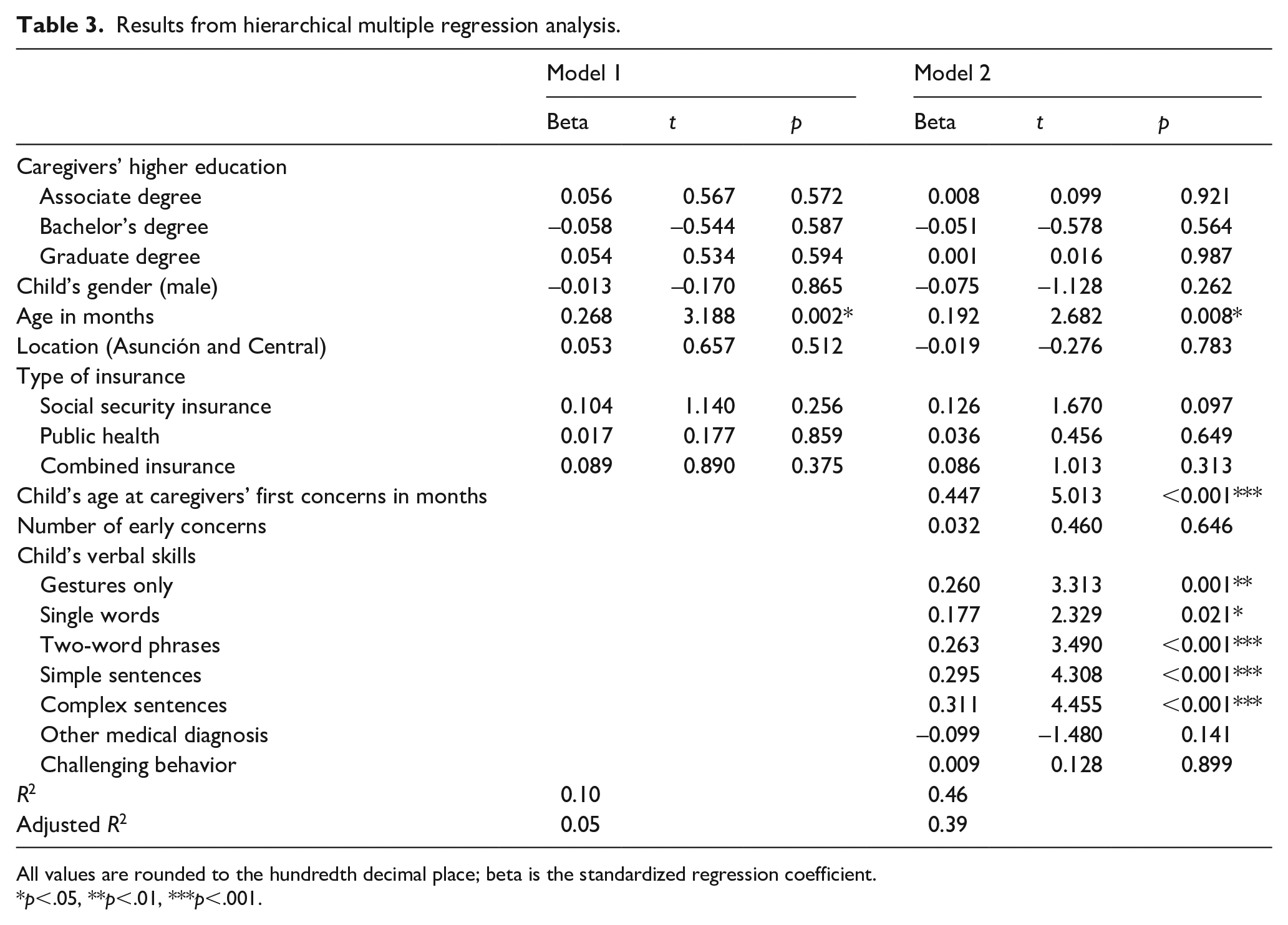
All values are rounded to the hundredth decimal place; beta is the standardized regression coefficient.
*p<.05, **p<.01, ***p<.001.
In the second model, we added the clinical predictors. The results of this hierarchical regression showed that child’s age was the only significant demographic predictor (beta = 0.192, p = 0.008), whereas child’s age at caregivers’ first concerns (beta = 0.447, p < 0.001) and child’s verbal skills (gestures only, beta = 0.260, p < 0.001; single words, beta = 0.177, p = 0.021; two-word phrases, beta = 0.263, p < 0.001; simple sentences, beta = 0.295, p < 0.001; complex sentences, beta = 0.33, p < 0.001) were significant clinical predictors of the child’s age of autism diagnosis. Specifically, the older the child’s age at caregivers’ first concerns, the older the predicted age of autism diagnosis, after controlling for the other predictors. In addition, all dummy variables for a child’s verbal skills remained significant, showing that compared to the baseline category (i.e. the children who did not speak and did not use gestures to communicate), the other categories yielded a significantly higher age of autism diagnosis (R2 = 0.46, adjusted R2 = 0.39).
Discussion
The purpose of this study was to investigate to what extent demographic characteristics and clinical characteristics of young autistic children in Paraguay predicted their age of diagnosis. This was the first study to investigate predictors of the age of autism diagnosis in Paraguay. In our sample, including all participants who completed the survey, we found that the mean age of diagnosis was 46.38 months (SD = 30.80). This is very similar to the findings reported by Montiel-Nava et al. (2024) for other countries in Latin America (46.3 months, SD = 29.9) and the United States (43 months for children without intellectual disabilities and 53 months for children with intellectual disabilities; Maenner et al., 2023). However, when removing outliers, the mean age of diagnosis of our sample was below than what was reported in other studies (M = 39.23, SD = 16.06).
In our regression analysis, we found that when including only the demographic predictors in the model, the only significant predictor was age in months. This aligned with the results reported by Montiel-Nava et al. (2024) for other countries in the region. This appears to imply that children who are older received a later diagnosis than children who are younger, suggesting that more recently, the average age of diagnosis has decreased. This finding is consistent with the global tendencies of decreasing age of autism diagnosis as awareness about autism and sensibility in screening and diagnostic tools has increased in recent years (Leng et al., 2023; Van’t Hof et al., 2021). However, given the difficulty in random sampling, we should note that it is possible that the present sample did not include younger children who have autism symptoms but have not received the diagnosis yet. Therefore, our finding regarding the decreased average age of diagnosis requires further investigation for validation.
When adding the clinical predictors, two clinical characteristics were significant predictors of child’s age of diagnosis. First, child’s age at caregivers’ first concerns was a significant predictor. This finding suggests that children often receive earlier diagnosis when caregivers identify early signs of autism in their children. Despite child’s age at caregivers’ first concerns being a significant predictor of child’s age of autism diagnosis, there is a gap of 13.16 months between the mean age of the child when caregivers first have concerns about child development (M = 26.07, SD = 15.50) and the child’s mean age of diagnosis (M = 39.23 SD = 16.06). The observed time gap between caregivers’ concerns and diagnosis was smaller than the gap reported in other studies. For example, Montiel-Nava et al. (2017) reported this gap to be 36 months in their sample of Venezuelan children, and Montiel-Nava et al. (2024) reported this gap to be 24 months in their sample across six countries in Latin America and the Caribbean. The time gap between caregivers’ concerns and diagnosis highlights potential barriers in the healthcare system that may hinder timely identification and assessment of autism. These barriers could include difficulties in accessing specialized developmental assessments, long waiting times for diagnostic evaluations, and challenges in obtaining accurate and comprehensive assessments of a child’s developmental and behavioral characteristics. Additional research is needed to understand more about the factors that impact this phenomenon and its variability.
Second, the child’s verbal skills were also significant predictors of the child’s age of diagnosis. These results indicate that children with better verbal skills tend to be diagnosed with autism at a later age, which could reflect the challenges in identifying autism in children with more advanced language skills. Researchers have reported that around 70% of individuals with autism acquire spoken language. However, those who develop verbal skills continue to exhibit atypical behavior in non-verbal communication (Bottema-Beutel, 2020). Thus, increased awareness of social communication characteristics of children with autism, beyond their verbal skills, among caregivers and professionals may increase the likelihood of early autism identification.
The variables we identified as significant predictors in our analysis are consistent with the reported results of Montiel-Nava et al.’s (2024) study for other countries in the region. However, some variables that were significant in their study, such as type of health insurance, and other medical diagnoses or comorbidities were non-significant in our analysis. The diagnostic criteria and practices used for autism diagnosis can vary across countries and regions. Different diagnostic guidelines, assessment tools, and clinical practices may lead to variations in the identification and diagnosis of autism. There may be unmeasured or unaccounted-for variables that differ between the studies and contribute to the differences in significant predictors. These variables could include cultural norms, regional variations, and other contextual factors that influence the diagnostic process. Further research is needed to understand why the included demographic predictors were not significant predictors of the age of autism diagnosis in Paraguayan children and more about the diagnostic process in the country in general.
Limitations and implications
Our findings should be interpreted considering some limitations. First, the caregivers who completed this survey were highly educated and had access to the Internet and other resources that allowed them to participate in the study. Thus, it is likely that our sample is biased, and our results may not reflect the age of diagnosis of the general Paraguayan population. In addition, demographic data from individuals with disabilities and their families are extremely scarce in Paraguay (Bascones Serrano et al., 2022). In the most up to date available report, based on the 2012 Paraguayan census, the Dirección General de Estadística Encuestas y Censos (2016) reported some sociodemographic characteristics of households of individuals with disabilities in Paraguay. In this report, the Dirección General de Estadística Encuestas y Censos (2016) reported that 4% or 49.117 households reported to have a member with intellectual disability, including Down syndrome, and/or autism. Data from households with individuals with disabilities were aggregated across disability categories for other analysis in this report. The limited availability of demographic data on children with autism and their families in Paraguay presents a challenge when attempting to draw conclusions about the representativeness of our data.
In addition, no identifying data were collected, and all data were reported by caregivers. Therefore, the research team did not verify any documentation related to the children’s demographic or clinical characteristics. Furthermore, this is a retrospective study, which means that it included only children who already have received an autism diagnosis and does not include information about children who are not yet diagnosed, or who did not access diagnostic services. These limitations warrant caution when interpreting the results.
The findings also have a few important implications. The identified predictors and the time gap between first concerns and diagnosis can inform further research efforts aimed at understanding the factors contributing to delayed autism diagnosis. In addition, these findings could influence policy initiatives focused on improving early screening and diagnosis of autism, as well as addressing systemic challenges that contribute to a delayed diagnosis.
Furthermore, these findings emphasize the critical role of caregivers’ awareness and concerns in the early diagnosis of autism. Routine parent-report screeners could be a helpful tool for clinicians to support the early identification of autism so that children can access early supports (Becerra-Culqui et al., 2018). Another way to promote early identification of autism may be education and awareness campaigns for parents and clinicians to help them identify characteristics of autism earlier (Becerra-Culqui et al., 2018). While recognizing caregivers’ early concerns is important, addressing the delay between concerns and diagnosis requires a multi-faceted approach involving education, healthcare system improvements, and community support to ensure that children with autism receive timely and appropriate interventions.
Conclusion
This study is the first to explore the complex interplay of factors influencing the age of autism diagnosis of children in Paraguay. By recognizing some factors that influence a timely diagnosis and the critical role of caregivers’ awareness, we can work toward ensuring that children with autism receive the best possible opportunities for growth and development. Collaborative efforts between healthcare providers, policymakers, researchers, and caregivers are essential to create a supportive environment that enables timely and effective diagnosis and subsequent access to adequate services for children on the autism spectrum.
Footnotes
Author contributions
Material preparation and data collection were performed by A.K.T., R.L.R.J., and H.M. All authors are contributing writers and reviewed all versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Institutional Review Board of the University of Illinois Urbana-Champaign. Informed consent was obtained from the participants, and no identifying information was collected.