
Abstract
Clinician and caregiver reports of autism features are both integral to receiving an autism diagnosis and appropriate intervention, yet informant discrepancies are present in clinical practice and may differ by demographic characteristics of the child and family. The present study examined how clinician–caregiver discrepancies in ratings of a child’s autism-related behaviors relate to a child’s sex at birth, age at first diagnosis, and amount of intervention received. Participants were 280 children (76.8% male, 67.9% White), 6–11 years old (M = 8.5 ± 1.6), with a diagnosis of autism spectrum disorder. Variable-centered and person-centered approaches were used to examine relationships between standardized clinician–caregiver discrepancy and participant characteristics. Both analytic approaches indicated that clinicians rated autism-related behaviors lower than caregivers for females and higher than caregivers for males. In addition, lower clinician ratings of autism features, relative to caregiver ratings, were associated with older age at diagnosis and fewer hours of intervention. Findings underscore the importance of incorporating multiple informants, especially caregivers, in the diagnostic process and developing diagnostic procedures sensitive to the female autism phenotype to facilitate diagnosis, intervention, and subsequent development.
Lay abstract
In some cases, a clinician’s perceptions of a child’s autism-related behaviors are not the same as the child’s caregiver’s perceptions. Identifying how these discrepancies relate to the characteristics of the child is critical for ensuring that diagnosis procedures are unbiased and suitable for all children. This study examined whether discrepancies between clinician and caregiver reports of autism features related to the child’s sex at birth. We also explored how the discrepancies related to the age at which the child received their autism diagnosis and how much intervention they received. We found that clinicians rated autism features higher than caregivers for boys and rated autism features lower than caregivers for girls. In addition, lower clinician relative to parent ratings was related to being diagnosed at an older age and receiving less intervention. These findings suggest that there is more to learn about the presentation of autism-related behaviors in girls. When caregiver and clinician ratings of autism features do not align, it may be important to consider caregivers’ ratings to obtain a more accurate picture of the child’s autism features and the support they may need.
Introduction
A diagnosis of autism involves assessment of behavior across contexts and over time. This requires integration of information obtained from caregiver report and clinical observation. For this reason, standard diagnostic procedures often yield informant discrepancies between caregiver and clinician ratings of autism-related behaviors or features (Rubenstein et al., 2017; Ventola et al., 2006). Such discrepancies are often not due to measurement error alone and yield clinically meaningful information relevant to diagnosis, intervention, and subsequent clinical outcomes (De Los Reyes, 2011). Discrepancies may also provide valuable information about specific contexts in which children express certain behaviors (e.g., when behavior differs in the presence of different informants; De Los Reyes et al., 2009). Informant discrepancies may reflect informant characteristics as well. For example, mothers of children who did not meet diagnostic criteria for autism according to clinician report but did meet diagnostic criteria according to maternal report were higher in autistic traits than other mothers (Rubenstein et al., 2017). Longitudinal studies indicate that informant discrepancies demonstrate stability over time and predict clinical outcomes over and above individual informants’ reports (Brookman-Frazee et al., 2008; De Los Reyes, 2011; Ferdinand et al., 2006; Lerner et al., 2012).
A limited volume of research examining informant discrepancies in autism indicates that they correlate with child characteristics and trajectories. Prior work suggests that parent and child report of autism features differ significantly, and the magnitude of this discrepancy predicts response to intervention (Lerner et al., 2012). There is also evidence to suggest that discrepancies between parent and teacher ratings relate to the child’s age, intervention receipt, medication use, and clinician ratings (Lerner et al., 2017). In addition, discrepancies between parent and clinician ratings are moderated by demographic factors, like race and household income (Neuhaus et al., 2018). Given the importance of clinician and caregiver ratings in autism diagnostic procedures and the relevance of prompt diagnosis for future adjustment (Estes et al., 2015), further exploration of discrepancies between caregiver and clinician reports in autistic individuals is warranted.
Biological sex is one additional child characteristic that may be associated with informant discrepancy. Although not true of all studies (Rodgers et al., 2019), past literature includes several findings of differences in parent ratings of children’s autism characteristics depending on the child’s sex. In some studies, parents rate females as having more autism characteristics than boys, especially in the social domain (Evans et al., 2019; Ratto et al., 2018; Rodgers et al., 2019).
Research has also examined sex differences in clinician ratings of autism with mixed results. Ratto et al. (2018) found no sex differences in clinician ratings on the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2; Lord et al., 2012) Calibrated Severity Score (CSS). In other studies, however, sex differences were found in the restricted and repetitive behavior (RRB) domain, with boys having more RRB than girls, but not in the social domain (Hiller et al., 2014; Mandy et al., 2012). These sex differences in clinician ratings may be related to higher levels of social camouflaging in autistic females (Dean et al., 2017) and/or limitations of diagnostic instruments in appropriately capturing autistic features in both males and females (Adamou et al., 2018; Kalb et al., 2022; Kreiser & White, 2014; Langmann et al., 2017). Given that both parents and clinicians demonstrate differences in their ratings of autism characteristics for males compared with females, discrepancies between these two informants’ ratings may also uniquely relate to child sex.
Two analytic strategies for capturing informant discrepancies are the variable-centered and person-centered approaches (Laursen & Hoff, 2006). In the commonly used variable-centered approach, informant discrepancy is calculated as a composite statistic by combining rater reports through summing, averaging, or calculating a difference score (De Los Reyes & Kazdin, 2004). Then, clinical inferences are derived by correlating these discrepancy scores with child or informant characteristics. Prior work indicates that standardized difference scores (SDS) yield more reliable results than raw or residual difference scores (De Los Reyes & Kazdin, 2004). Although a benefit of the SDS approach is its ease of interpretability, there are nontrivial limitations (Laird & De Los Reyes, 2013). First, SDS are sensitive to differences in variance between the two scores used to derive the difference score. SDS also assume directionality, ultimately setting up one individual’s rating to be the “baseline” when, in reality, both ratings are likely influenced by bias (De Los Reyes et al., 2008; Laird & De Los Reyes, 2013). Thus, the present study used SDS to explore informant discrepancies in an accessible way but coupled these initial analyses with a person-centered approach to gain a more nuanced understanding of the relationship between informant discrepancy and child characteristics.
Person-centered approaches identify subgroups of a population based on the pattern of informant discrepancy that individuals display. The current study used latent profile analysis (LPA), a method that allows for the identification of different subgroups or profiles derived from reports from various informants (e.g., caregiver report and clinician report). This approach has previously been used to identify four subgroups of autistic children based on discrepancies between parent and teacher ratings of autism features (Lerner et al., 2017). A benefit of LPA is that it provides insight into differences in the shape of various informant discrepancy profiles, allowing for the identification of diverging patterns of informant discrepancy and subsequent identification of child characteristics associated with each profile.
The current study characterizes patterns of informant discrepancy in a large and well-characterized sample of autistic children to examine how clinician and caregiver discrepancies in ratings of a child’s autism features may relate to (1) the child’s sex at birth, (2) the timing of first autism diagnosis, and (3) the amount of intervention received. Application of both a variable-centered and person-centered approach allows for the consideration of method variance when exploring these aims. We acknowledge the difference between sex and gender as well as the importance of considering both constructs. The present study only had access to data on the child’s sex at birth and not their gender. Therefore, all references to boys/males and girls/females are specific to biological sex and findings may not generalize to gender identity. However, there is a vast literature on sex differences in autism that can be informed by the results of this study.
In line with previous findings of discrepancies between parent and clinician report of children’s autism-related behaviors (Rubenstein et al., 2017; Ventola et al., 2006), we hypothesized at least two informant discrepancy profiles: (1) clinicians endorsing more autistic features than caregivers and (2) clinicians endorsing fewer autistic features than caregivers. Based on unequal diagnosis rates for male versus female children (Christensen et al., 2016) and prior work examining sex differences in reports of children’s autism characteristics, we hypothesized that boys would be more likely than girls to have higher clinician ratings of autism features relative to caregiver ratings of autism features. With respect to diagnosis and intervention, we predicted that more autism features endorsed by the clinician relative to the caregiver would associate with earlier diagnosis and more hours of intervention, since clinicians determine diagnosis and service referral.
Method
Participants
Participants were 280 children with a pre-existing autism diagnosis, aged 6–11 (M = 8.5 ± 1.6 years), taking part in the Autism Biomarkers Consortium for Clinical Trials (ABC-CT), a longitudinal, multisite study designed to identify neurophysiological biomarkers for autism (McPartland et al., 2020). Participants were required to have an intelligence quotient (IQ) between 60 and 150 to ensure comprehension and compliance with the neurophysiological protocols of the larger study; complete inclusion and exclusion criteria are specified in the work by McPartland et al. (2020). Participants were recruited by contacting families who previously participated in research at each site, distributing flyers in surrounding communities, and advertising online. The study protocol and consent documents were approved by the Yale University Institutional Review Board (IRB), which served as the Central IRB for the ABC-CT (HIC#1509016477). Written informed consent was obtained prior to study participation.
Across the five sites, 76.8% of participants were male. Approximately 68% of participants identified as White, 16% identified as multiracial, 8% identified as Black or African American, 5% identified as Asian, 2% identified as “other,” and less than 1% identified as American Indian or Alaskan Native. More than half of families had an annual household income greater than US$100,000, while about 25% of families had a household income between US$50,000 and US$100,000 and approximately 22% of families had a household income less than US$50,000. More information on the demographic characteristics of the sample is provided in Table 1.
Participant characteristics.
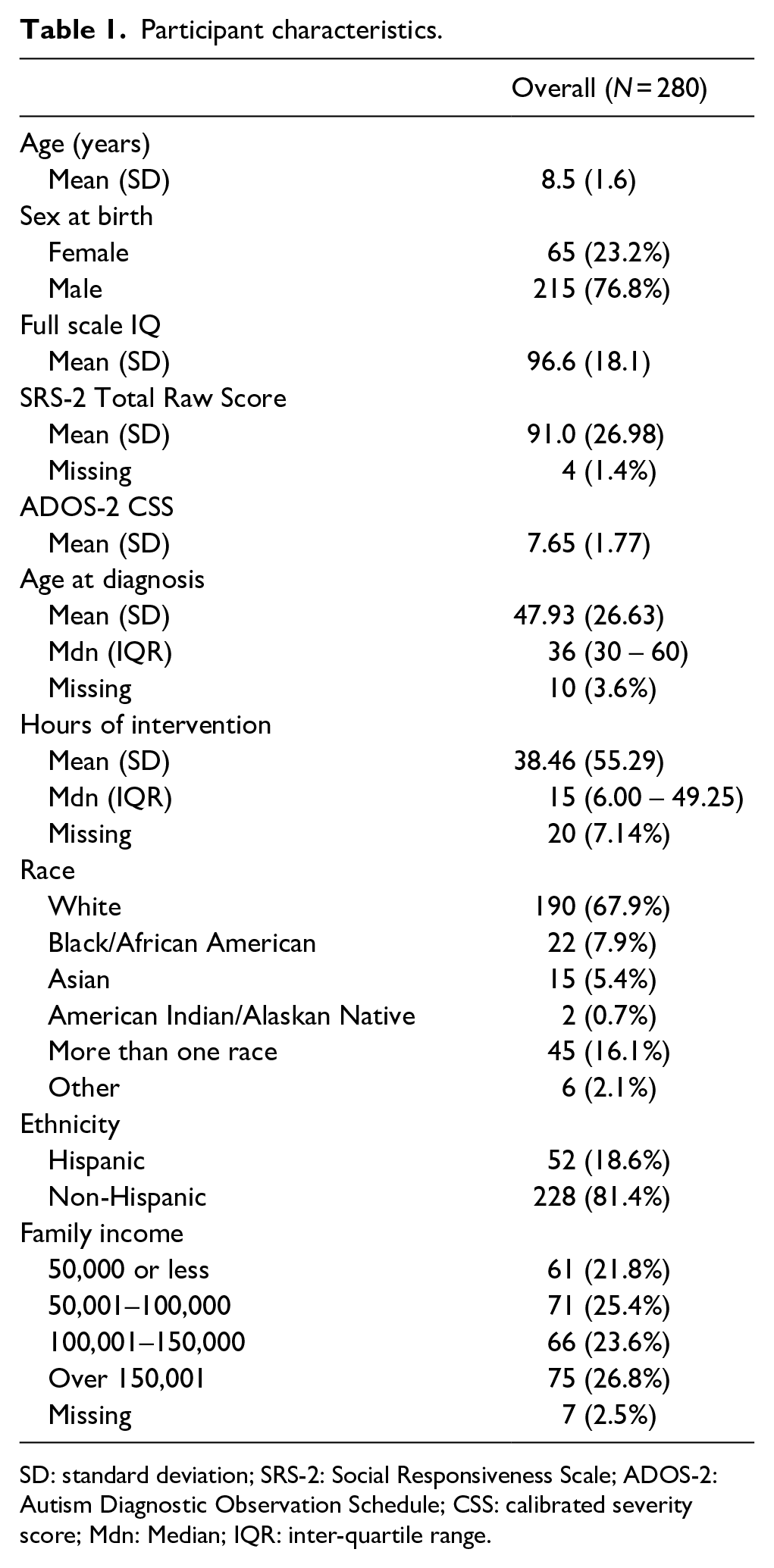
SD: standard deviation; SRS-2: Social Responsiveness Scale; ADOS-2: Autism Diagnostic Observation Schedule; CSS: calibrated severity score; Mdn: Median; IQR: inter-quartile range.
Measures
Autism features
The ADOS-2 (Lord et al., 2012) is a semi-structured, play-based autism diagnostic assessment in which a child’s behavior during an interaction with an examiner is observed and coded. Research-reliable clinicians assessed each participant with either Module 1, 2, or 3, depending on their expressive language abilities at the time of assessment. Children receive an Overall Total Score based upon all items on the assessment, a Social Affect (SA) Total Score for items related to communication and social interaction, and an RRB score for items related to stereotyped or repetitive speech and behaviors. In addition, a CSS, a standardized score on a scale of 1–10, is calculated for each child based upon their Overall Total Score and is intended to represent the extent of a child’s autism-related behaviors relative to their age and language abilities (Gotham et al., 2009). CSS SA and CSS RRB scores are also derived (Hus et al., 2014). The CSS has demonstrated good test–retest reliability in similar samples, particularly the CSS total and the CSS SA (Janvier et al., 2022). In this study, the CSS was used to harmonize scores across modules.
The Autism Diagnostic Interview-Revised (ADI-R; Rutter et al., 2003) is a 93-item caregiver interview designed to assess autism-related behaviors in individuals with a mental age of 2 years or older across three domains: (1) language/communication; (2) reciprocal social interactions; and (3) restricted, repetitive, and stereotyped behavior. The diagnostic algorithm is used to determine whether the assessed individual meets criteria for an autism diagnosis. In prior samples, the ADI-R has demonstrated high internal consistency among verbal children and high interrater reliability in childhood samples, with a study evidencing 95% agreement across all items scored by seven clinicians (Cicchetti et al., 2008; Lord et al., 1994).
The Social Responsiveness Scale, Second Edition (SRS-2; Constantino & Gruber, 2012) is a 65-item caregiver-report questionnaire that assesses features of autism. On the School-Age Form, caregivers of 4- to 18-year-old children rate each item on a scale of 1 (not true) to 4 (almost always true). Responses are summed to yield raw scores and T-scores for the total score, as well as for the social communication (SCI) and RRB domains. In addition to evidence of convergent validity with other common measures of autism features like the Social Communication Questionnaire (SCQ; Rutter & Bailey, 2003), the SRS has shown good internal consistency, test–retest reliability, and interrater reliability in prior research (Charman et al., 2007; Constantino & Gruber, 2012).
Other clinical assessments
The Differential Ability Scales, Second Edition (DAS-II; Elliot, 2007) is a cognitive assessment consisting of two separate batteries; the School-Age battery is appropriate for 7- to 17-year-old children, while the Early Years battery is appropriate for 2.5- to 6-year-old children or 7- to 8-year-old children of lower cognitive ability. Performance on the core subtests of the DAS-II determines a child’s General Conceptual Ability (GCA) score, an overall composite score reflecting cognitive abilities. Prior work evidences the DAS-II’s test–retest reliability, interrater reliability, and convergent validity (Elliot, 2007).
Procedure
Autism clinical diagnoses were confirmed via the ADOS-2, ADI-R, and clinical judgment based on Diagnostic and Statistical Manual of Mental Disorders (5th ed., DSM-5) criteria (American Psychiatric Association, 2013). Only participants who met diagnostic criteria on all three of these measures were included in the study. This was because the larger biomarker study from which this sample was drawn required participants to be deeply characterized and phenotypically similar across multiple sites. Cognitive ability was assessed using the DAS-II. As part of a larger questionnaire battery, caregivers reported on participants’ autism features using the SRS-2. Of the 276 SRS-2 respondents, approximately 91% were mothers, 7.5% were fathers, and 1.5% were of another relationship to the child. Parents also reported the child’s sex at birth (hereafter “sex”), the age at which their child received their initial autism diagnosis, and the number of hours of various interventions their child received in the 6 weeks prior to their research visit.
Analytic plan
To examine relationships between informant discrepancy and the child sex, diagnosis, and intervention variables in the variable-centered approach, continuous clinician–caregiver discrepancy variables were calculated by subtracting z-scores of the SRS-2 raw scores (caregiver report) from z-scores of the ADOS-2 CSS (clinician report). SDS were generated for total (z(ADOS-2 CSS)—z(SRS-2 total raw score)), social domain (z(ADOS-2 SA CSS)—z(SRS-2 SCI raw score)), and RRB domain (z(ADOS-2 RRB CSS)—z(SRS-2 SCI raw score)) autism features.
Variable distributions were first examined to accommodate assumptions of statistical tests. Nonparametric tests were used for variables that failed normality tests due to skewness. To accommodate skewness, the number of intervention hours and age at first diagnosis were natural log transformed.
Variable-centered approach
Mann–Whitney U and Kruskal–Wallis tests were used to explore how clinician–caregiver discrepancy scores differed by child sex. Relationships between clinician–caregiver discrepancies, the child’s age at first diagnosis, and intervention hours were examined using Spearman’s correlations.
Person-centered approach
A variable-centered approach is a more common and intuitive approach to studying informant discrepancies, but recent work has revealed limitations to using SDS (Laird & De Los Reyes, 2013). Thus, we also prioritized a person-centered approach. LPA was used to identify different person-centered profiles of informant discrepancy within the sample. After profiles were identified, logistic regression assessed how sex, amount of intervention, and diagnosis age predicted profile membership.
Community involvement
The design and administration of the ABC-CT included input from members of the autistic community who serve on the study’s External Advisory Board.
Results
Descriptive statistics
General demographic and clinical characteristics of the sample are presented in Table 1. Parent-report (SRS Total raw score) was not significantly associated with clinician-report (ADOS CSS; r = .08, p = .21). In addition, parent-reported social communication challenges (SRS-2 SCI) and RRBs (SRS-2 RRB) did not significantly correlate with clinician-report of social challenges (ADOS-2 SA CSS; r = .11, p = .08) or RRBs (ADOS-2 RRB CSS; r = .12, p = .06).
Variable-centered approach
Aim 1
The first aim of the present study was to examine differences in clinician–caregiver discrepancy score by the child’s sex. Overall discrepancy scores differed by child sex (U = 5553.00, p = .03). Relative to clinicians, caregivers reported lower levels of autism features for males (Mdn = .12) and higher levels for females (Mdn = −.20; Figure 1(a)). Discrepancies between the SRS-2 SCI domain and the ADOS-2 SA domain revealed a similar pattern, with caregivers reporting lower levels of social autism features for males (Mdn = .07) and higher levels for females (Mdn = −.42; U = 5408.50, p = .01; Figure 1(b)) relative to clinicians. Moreover, evaluating sex differences in ratings of autism features within each instrument (ADOS-2 or SRS-2) revealed that clinicians reported higher levels of overall autism features on the ADOS-2 in males (Mdn = 8.00) than in females (Mdn = 7.00; U = 4909.00, p < .001), but caregiver ratings of overall autism features on the SRS-2 did not differ for males and females (p = .85). Sex differences in clinician–caregiver discrepancy scores did not emerge for RRBs.
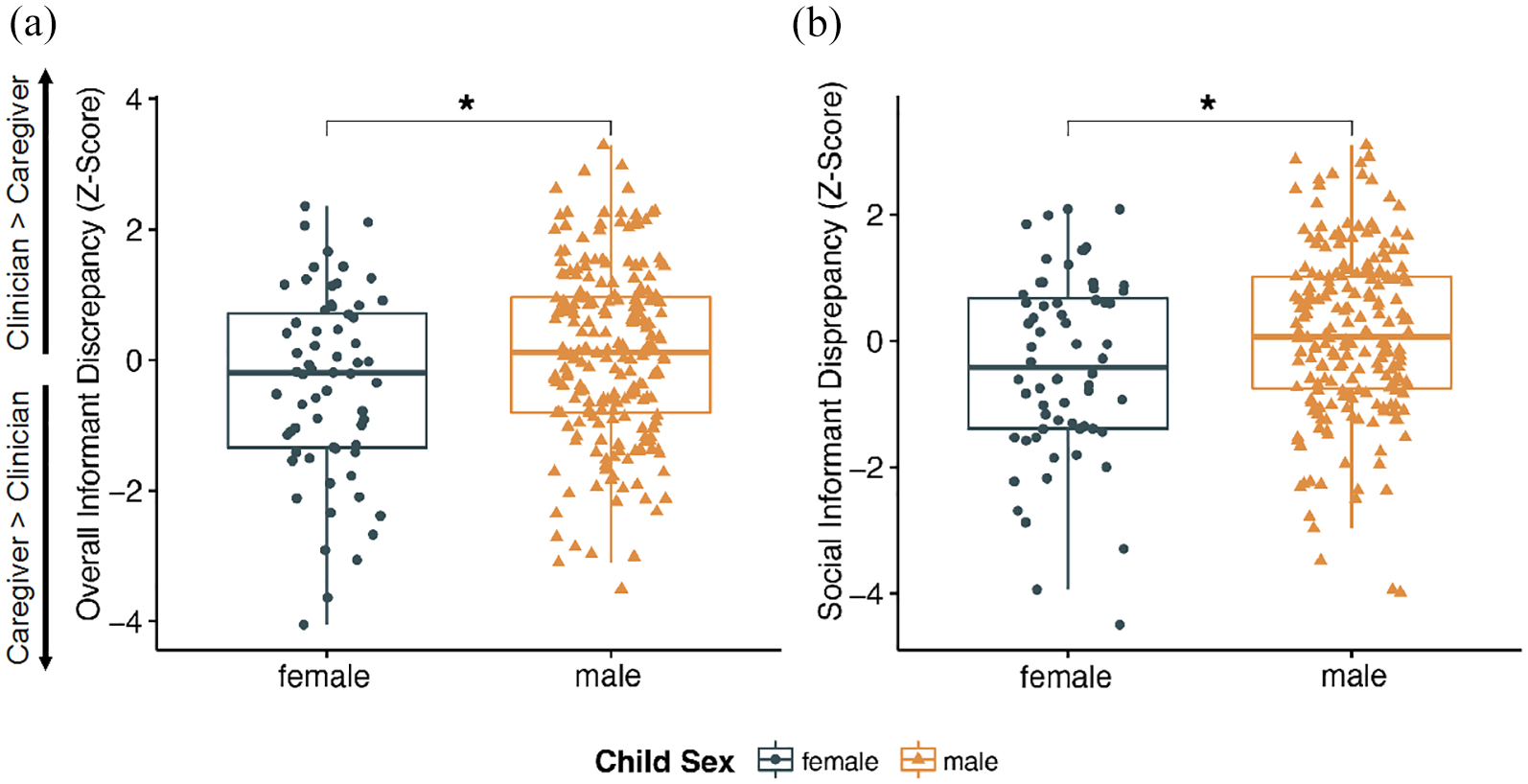
(a) Differences in clinician–caregiver overall discrepancy scores across female and male participants. (b) Differences in clinician–caregiver social discrepancy scores across female and male participants. *p < .05.
Aim 2
The second aim of the study was to investigate associations between clinician–caregiver discrepancies and the child’s diagnosis age. Higher clinician ratings of overall (r(264) = −.19, p = .001) and social autism-related behaviors (r(264) = −.19, p = .002), relative to caregiver ratings, was associated with earlier diagnostic age.
Aim 3
The third aim of the study was to explore the relationship between clinician–caregiver discrepancies and receipt of intervention. Similar to age at diagnosis, higher clinician relative to caregiver ratings was also associated with receiving more hours of intervention (overall autism features discrepancy [r(254) = .19, p = .003]; social autism features discrepancy [r(254) = .20, p = .001]) and more types of intervention (overall autism features discrepancy [r(274) = .12, p = .04]; social autism features discrepancy [r(274) = .14, p = .02]). Discrepancies in RRB ratings were not associated with intervention receipt (ps > .05)
Person-centered approach
The best fit model that emerged from LPA was a two-class model with varying variances and covariances. This model was selected due to the minimized Bayesian information criterion (BIC; see Table 2 for more information about model fit). Profile 1 includes participants for whom clinicians rated core autism-related behaviors, in both the RRB domain and social domain, higher than caregivers (Figure 2). This profile is referred to as the “clinician higher than caregiver” profile. Profile 2 includes participants for whom clinicians rated core autism-related behaviors lower than caregivers and is referred to as the “clinician lower than caregiver” profile.
Fit statistics for LPA.

Note. Models are specified in terms of how the variable variances and covariances are estimated. Model 1 refers to a model with equal variances and covariances fixed to 0. Model 6 refers to a model with varying variances and covariances. Model selection was decided based on evidence from multiple sources, including fit indices (Akaike information criterion, BIC), entropy, likelihood ratio tests, and parsimony. The bootstrapped likelihood ratio test for Model 6 with 2 classes was significant (p = .01).
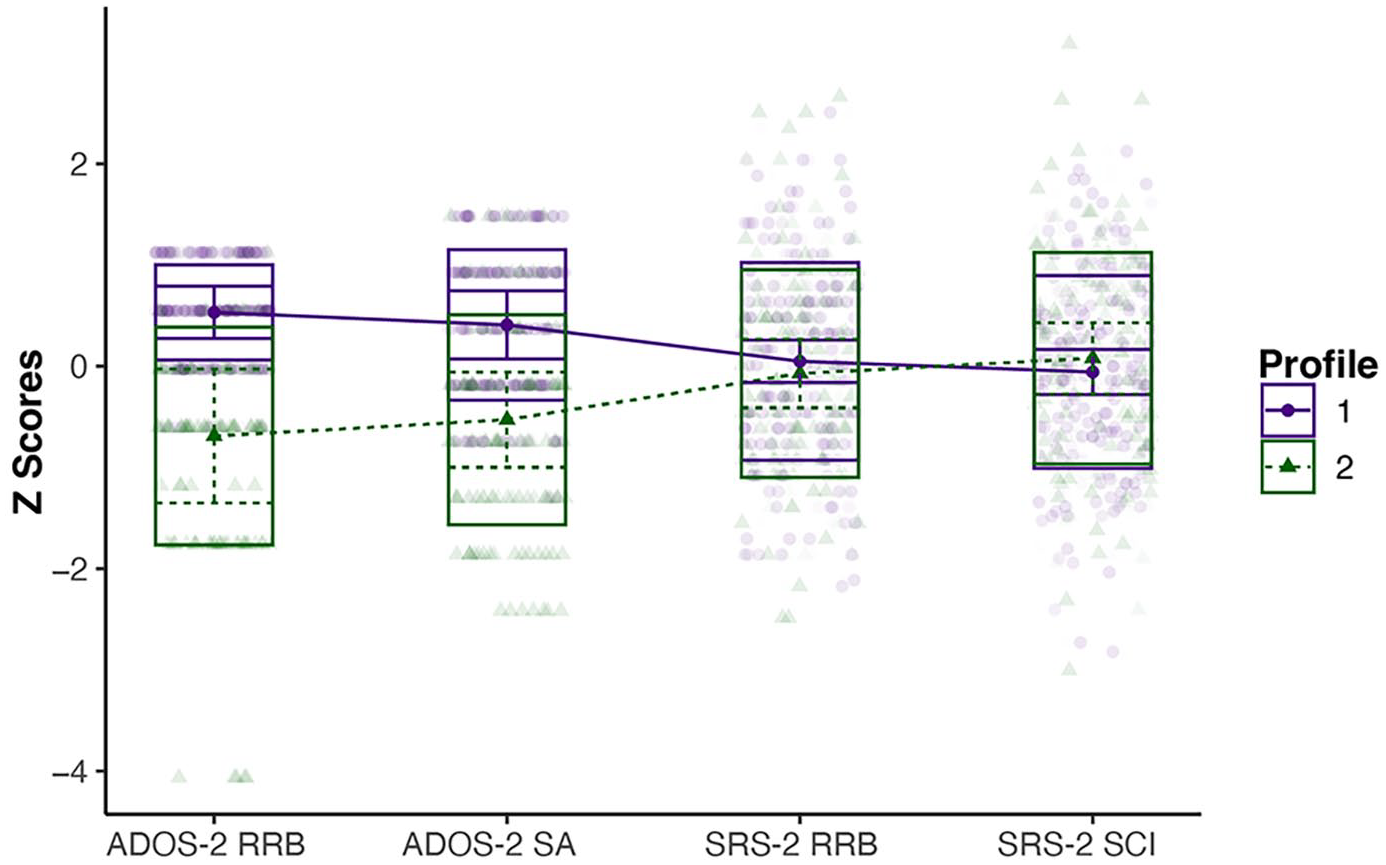
Two profiles emerged from the LPA. In the profile plot, each profile is differentiated by color and line type. Profile 1 (purple, solid line) consists of participants who were rated higher in autism features by clinicians (ADOS-2) compared with caregivers (SRS-2). Profile 2 (green, dotted line) consists of participants who were rated higher in autism features by caregivers (SRS-2) compared with clinicians (ADOS-2).
Aim 1
Using logistic regression, sex emerged as a significant predictor of profile membership. Being male predicted an odds ratio of .49 for being in the “clinician lower than caregiver” profile (ß = −.70, SE = .29, p = .02). An odds ratio less than 1 indicates that male participants had lower odds of being in the “clinician lower than caregiver” profile compared with female participants.
Aim 2
To examine whether a participant’s likelihood of belonging to one profile over the other differed based on age of diagnosis, we conducted a logistic regression with diagnosis age as the predictor. Acknowledging previous findings of greater agreement across informants for younger children (De Los Reyes & Kazdin, 2005), as well as the potential confound of current age on the relation between age at diagnosis and intervention receipt, we controlled for current age in all models for Aims 2 and 3. Age at first diagnosis was associated with profile membership, although it did not reach significance. Being older at first autism diagnosis was associated with an increased likelihood of belonging to Profile 2, the “clinician lower than caregiver” profile (OR = 1.65, ß = .50 SE = .27, p = .07). Diagnosis at a younger age was associated with an increased likelihood of belonging to the “clinician higher than caregiver” profile.
Aim 3
To explore whether intervention receipt was related to profile membership, we conducted two separate linear regressions with intervention hours and number of interventions received as predictors. Intervention hours emerged as a significant predictor of discrepancy profile membership (OR = .79, ß = −.24, SE = .10, p = .02). Receiving a greater number of intervention hours was predictive of significantly lower odds of being in the “clinician lower than caregiver” profile, or higher odds of being in the “clinician higher than caregiver” profile. The number of interventions a child received was not a significant predictor of profile membership.
Discussion
It is standard practice to integrate both caregiver report of a child’s development and autism features alongside clinician observation of a child’s behavior in the assessment and diagnosis of autism. However, discrepancies may arise between clinician and caregiver reports of children’s autism features (De Los Reyes & Kazdin, 2005; Neuhaus et al., 2018; Rubenstein et al., 2017; Ventola et al., 2006). The current study applied both variable-centered and person-centered approaches to understand patterns and predictors of caregiver–clinician informant discrepancies. Both approaches yielded comparable findings; clinicians endorsed more autism features in males than females, while caregivers of either males or females had comparable ratings. Higher clinician, relative to caregiver, ratings of autism features were also associated with earlier diagnosis and receipt of more intervention. Results highlight the relevance of considering perspectives of multiple informants to facilitate early identification of autism and access to intervention, especially for children with female sex.
The first aim of this study was to explore how children’s assigned sex related to clinician–caregiver discrepancies in the report of children’s autistic behaviors. As hypothesized, results from the variable-centered approach demonstrated that clinicians, relative to caregivers, reported lower levels of overall and social autism features in females (i.e., less difficulties with social communication and interaction) and higher levels of overall and social autism features in males. Results from the person-centered approach aligned with the variable-centered results, indicating that the probability of being in the “clinician lower than caregiver profile” was higher for females than males. Although Neuhaus et al. (2018) did not find differences in informant discrepancy based on child sex, the present sample may have been better powered to detect these differences given a larger proportion of female participants.
Post hoc analyses revealed that clinician ratings (ADOS-2 scores) differed significantly based upon child sex, with boys receiving higher scores than girls, while sex differences were not found for parent ratings (SRS-2 scores). Importantly, this does not mean that clinicians rated symptoms incorrectly, as neither reporter nor measure is inherently considered “correct” from an informant discrepancy perspective (De Los Reyes & Kazdin, 2008). Discrepancies on a particular measure may result from the specific behaviors the measure is designed to capture.
The standardized observation that takes place during the ADOS-2 represents a major strength of the instrument; however, the short interaction the clinician has with the child during the assessment, especially with girls who are camouflaging, may not be sufficient to observe all the behaviors parents see over more intimate and enduring interactions with their children (Kreiser & White, 2014). Females may feel more pressure to camouflage than males based on greater social expectations (Hull et al., 2020) or greater social consequences for behavior that does not meet these expectations (Kreiser & White, 2014). In addition, in certain contexts, like the unfamiliar setting the evaluation took place in during the present study, girls may camouflage more than they do in other contexts (e.g., home) which can give rise to discrepancies in ratings (Hull et al., 2020). Girls may also be able to camouflage more easily in simple social situations, like a structured assessment, than in more complex interactions, such as those that occur in natural, real-world interactions (Hull et al., 2020). Thus, caregivers may have a more comprehensive perspective of their child’s behavior because they are able to observe their child interact naturally with their peers rather than only in structured, lab-based social interactions.
Sex differences in ratings of autism features may also result from differences in how parents and peers perceive and interact with boys and girls based on their sex. Children are born into a gendered environment in which others’ perceptions of them may influence their behavior. Biologically male and biologically female children are exposed to differences in their environments beginning in infancy that may contribute to some of the sex differences in autism research (Cheslack-Postava & Jordan-Young, 2012) and to the differences in informant discrepancy by child sex in the present study. Caregivers may perceive girls as having more autism features in the social domain due to expectations of greater social motivation and social competence in females (Holtmann et al., 2007). Without a set of autism criteria in front of them, parents may be more likely to pick up on autistic characteristics in girls or rate girls higher in autistic features because they are not meeting their social expectations. In other words, a larger perceived gap between autistic girls’ social behavior and expected social behavior for girls compared with the gap between autistic boys’ behavior and expected social behavior for boys may contribute to sex differences in parent ratings (Holtmann et al., 2007; Kaat et al., 2021).
Moreover, based upon greater social expectations for females compared with males, caregivers may make more social bids toward daughters than sons, in turn giving autistic girls more practice with social interaction and equipping them to mask their social and communication difficulties (Cheslack-Postava & Jordan-Young, 2012; Kreiser & White, 2014). Girls’ peer relationships also tend to differ from boys in ways that promote masking or increased social skills. For example, smaller peer groups focused on conversation may help girls to better hone their communication skills out of either increased opportunity for social communication or fear of social rejection for those who do not engage (Kreiser & White, 2014). This additional practice with modeling social communication and/or masking may result in behavior among autistic girls that looks markedly different from autistic boys. Thus, to a clinician who is observing their behavior, social communication challenges may be more difficult to detect in girls.
Emerging work exploring the female autism phenotype suggests that some features of autism may present differently in autistic females than autistic males (Hull et al., 2020; Lai & Szatmari, 2020). Males tend to receive higher scores for RRBs (Kaat et al., 2021; Knutsen et al., 2019; Tsirgiotis et al., 2021) while females receive higher scores for anxiety (Tsirgiotis et al., 2021). RRBs sometimes manifest in less conspicuous ways in girls than in boys. While boys often have restricted behaviors and interests that revolve around objects, girls often have restricted behaviors and interests that focus on relationships, people, and animals (Gould & Ashton-Smith, 2011; Lai & Szatmari, 2020). Furthermore, autistic girls’ restricted interests may align in content with the interests of their neurotypical, same-sex peers, making them less obvious than those of their male counterparts (Kreiser & White, 2014). Thus, girls’ repetitive behaviors may be overlooked during shorter observations, while behaviors like lining up cars or pushing buttons may be easily flagged in males, especially since these items are readily available in the ADOS-2 materials. In addition, when coding RRBs, clinicians are instructed to only code behaviors that are inappropriate for their developmental stage. Therefore, if females display interests that align with those considered developmentally appropriate, they would not be captured in ADOS-2 scores.
Social difficulties may also manifest differently in boys and girls. For example, rather than withdrawing from others, girls may cling to familiar people and they tend to have more advanced verbal skills than boys, further masking their social difficulties (Kopp & Gillberg, 1992; Kreiser & White, 2014). Interestingly, the pattern of sex differences in autism characteristics may change with age. Kaat et al. (2021) found males only had higher RRB scores than girls on the ADOS and ADI during childhood; however, females had higher SRS scores in both the social and RRB domains during adolescence. As the field’s understanding of the female autism phenotype is nascent and evolving, differences in expression of autism-related behaviors by sex and gender warrant further research.
Although research on autism in females suggests RRBs are one area characterized by sex differences, the present study did not find differences in clinician–caregiver discrepancy scores for RRBs using the variable-centered approach despite discrepancies for social difficulties and overall autism features. This may be partly due to the nature of the RRB CSS. In developing the subdomain calibrated severity scores, the authors noted that since there are more SA items than RRB items on the ADOS-2, the overall CSS is more influenced by the SA items (Hus et al., 2014). Furthermore, since the range of the RRB CSS is more limited than the range of the overall CSS and social CSS (on a 5–10 scale rather than 1–10), correlations with this variable may be less robust (Hus et al., 2014). RRBs may also be more “observable” than social difficulties, allowing parents and clinicians to agree upon their presence or absence. Considering this, it is notable that the LPA-derived profiles were not specific to social symptoms and instead identified subgroups based on informant discrepancy of autism features across both domains. As RRBs are part of core autism symptomatology, continued work is needed to define RRBs and their manifestation in early development and to examine differences based on sex and gender.
The second aim of the present study was to examine how clinician–caregiver discrepancies in reports of children’s autism features related to diagnosis age. Consistent with study hypotheses, in the variable-centered approach, higher clinician, compared with caregiver, ratings of overall and social autism-related behaviors were associated with an earlier diagnosis age. The person-centered analysis yielded convergent findings such that older age at first autism diagnosis predicted increased odds of belonging to the “clinician lower than caregiver” profile, although this difference was not significant. Children often receive a diagnosis at a later age due to lower symptom severity (Daniels & Mandell, 2014). This may be reflected in the lower clinician ratings of autism features, relative to caregiver ratings, for this group in the present study. The relative newness of the diagnosis for parents may have also contributed to higher ratings from caregivers, relative to clinicians, for those with a later diagnosis in the present study. Conversely, children diagnosed at an earlier age may have greater symptom severity (Daniels & Mandell, 2014). Parents who have long been aware of their child’s diagnosis may rate their child’s autism features lower than clinicians in part because these children have been receiving services for a longer time and parents may observe changes in their child’s behavior over time. It is also important to recognize that boys and girls have been found to differ in their diagnosis age, with boys being diagnosed earlier (McDonnell et al., 2021). Thus, the sex differences in informant discrepancy in the present study may play a role in the differences in informant discrepancy by diagnosis age (Dillon et al., 2023), a moderation effect that warrants exploration in future studies.
Finally, the third aim was to investigate how informant discrepancy related to intervention receipt. In the variable-centered analyses, higher clinician ratings of autism behaviors (overall and social), relative to caregiver ratings, were associated with receipt of more intervention. This aligns with another recent report that clinician ratings of autism features are more predictive of receipt of services than parent ratings (Rosen et al., 2019). Number of intervention hours also significantly predicted profile membership with children receiving a greater number of intervention hours being more likely to belong to the “clinician higher than caregiver” profile. Considering the established body of literature implicating more intensive intervention in positive developmental trajectories and adaptive behavior (Orinstein et al., 2014), more efforts to ensure improved characterization of the female autism phenotype and development of interventions tailored to autistic girls is warranted.
In addition, the potential need for adaptations to current diagnostic instruments is supported by the finding that divergence of LPA profiles was primarily driven by clinician and not parent ratings (i.e., convergence of purple and green lines on the right-hand side of Figure 2 and divergence of purple and green lines on the left-hand side). Considering the post hoc analysis that revealed a difference by child sex in clinician ratings but not parent ratings, results of the person-centered approach underscore the need to (1) more deeply characterize the female phenotype and other presentations that may differ from a prototypical presentation, (2) develop or amend gold standard instruments to capture symptoms across all individuals, and (3) subsequently disseminate these tools in clinical training and practice. Doing so may facilitate access to care.
Limitations and directions for future research
A primary strength of this study was the use of both variable-centered and person-centered approaches to account for method variance and provide a more comprehensive account of predictors of informant discrepancy. However, this study is not without limitations. One limitation is the use of cross-sectional data. Future studies employing a longitudinal design could clarify temporal precedence in the relationships between informant discrepancy and diagnosis age and access to intervention. In addition, information on participants’ gender identity was not collected. Although information on gender identity was collected at a follow-up 4 years later, the sample had limited gender diversity. Acknowledging gender diversity in autistic individuals (Strang et al., 2014), additional studies with longitudinal follow-up may allow for the consideration of gender identity in informant discrepancy to further understand gender differences during the diagnostic process. The present study also examined informant discrepancy across two measures that do not have identical content. Thus, differences may be in part accounted for by differences in the autism characteristics that each measure captures, rather than solely due to differences in reporting across clinicians and caregivers. Future research that examines informant discrepancy in autism characteristics may benefit from incorporating measures that align more closely in content and structure.
The only demographic characteristic considered as a predictor of informant discrepancy in the present study was sex. While we originally hoped to examine differences in clinician–caregiver discrepancy scores based on family income and child race and ethnicity, there was not enough variability in family income or racial/ethnic diversity in our sample for these analyses. Previous research has demonstrated larger clinician–caregiver discrepancies in ratings of autism-related behaviors for lower socioeconomic status (SES) compared with higher SES children and for Black compared with White children (Neuhaus et al., 2018). Considering the directionality of the discrepancy for race is complicated given the mixed literature on racial and ethnic differences in prevalence rates. Based on some research reflecting racial disparities in autism diagnosis (Shenouda et al., 2021, 2023) and the reliance of diagnosis on clinician judgment, children from minoritized racial and ethnic backgrounds may have lower ratings of autism features by clinicians than parents. On the contrary, prior findings suggest that parents of children from certain racial minority backgrounds (e.g., Black/African American) report fewer concerns about autism-related behaviors than parents of White children (Donohue et al., 2019), which may delay clinician diagnosis (Twyman et al., 2009). Thus, it is possible that children from minoritized racial and ethnic backgrounds could have lower ratings of autism features by caregivers than clinicians. A recent study even found higher prevalence of autism among non-Hispanic Black, non-Hispanic Asian or Pacific Islander, and Hispanic children compared with non-Hispanic White children (Maenner et al., 2023). Therefore, clinicians may rate certain autism-related behaviors higher than caregivers in non-White, non-Hispanic children and Hispanic children relative to White, non-Hispanic children.
Still, some work indicates similarities in age and rates of diagnosis across racial and ethnic groups (Maenner et al., 2020; Pham et al., 2022). Given these findings, one may expect no differences in informant discrepancy as it relates to race and ethnicity. To further complicate matters, ethnic and racial differences in diagnosis rates may be influenced by specific clinical presentations, such as co-occurring autism and intellectual disability (ID; Maenner et al., 2020, 2023) and the additive impact of SES (Durkin et al., 2017). Thus, it remains unclear whether and how race and ethnicity would associate with informant discrepancy. Future work using a person-centered approach to explore how race and SES may predict informant discrepancies in more diverse samples is needed. Furthermore, given that Hispanic/Latinx individuals may not conceptualize their race and ethnicity as separate identities (Allen et al., 2011), future work may wish to examine differences in informant discrepancy across intersectional ethnoracial identities, rather than examining race or ethnicity in isolation. Considering that the sample of this study is also relatively small for an LPA (Spurk et al., 2020), future research would benefit from replication in a larger sample with a more balanced proportion of autistic girls and boys which would be better powered to detect differences.
Finally, the present study was limited in its ability to reflect the full autism spectrum. First, participants were required to meet cutoffs for autism on the ADOS-2, ADI-R, and clinical judgment based on DSM-5 criteria. Recent work revealed a larger proportion of females than males excluded from research studies that rely on ADOS/ADOS-2 cutoffs to determine eligibility (D’Mello et al., 2022). Therefore, our findings regarding sex differences may be influenced by the study’s strict inclusion criteria and possible over-exclusion of autistic females. Participants were also required to have an IQ above 60, resulting in a relatively high average IQ in the present sample. Service utilization and diagnosis age differ among autistic children with ID compared with those without ID (Maenner et al., 2023; Zablotsky et al., 2015). Given evidence of earlier diagnosis age for children with ID, there may be less discrepancy between parents and clinicians in ratings of autism behaviors for this subgroup as parents have long been in communication with clinicians about their child’s behaviors. Moreover, some behaviors that are more common among children with ID, like self-injurious behaviors and verbal communication challenges, may be more readily apparent to both clinicians and parents which may, in turn, facilitate higher agreement in ratings. In addition, racial and ethnic differences in informant discrepancy may be influenced by the presence of ID given that rates of ID are higher among Black autistic children compared with White autistic children (Maenner et al., 2023). Thus, future work sampling a broader range of cognitive abilities will be important for determining generalizability.
Conclusion
The present study found that discrepancies in clinician versus caregiver report of autism-related behaviors differed by the child’s sex and were associated with differences in diagnosis age and the amount of intervention the child received. Convergence of a variable-centered and person-centered approach to quantify informant discrepancy provides confidence in the associations between clinician–caregiver discrepancies in ratings of autism-related behaviors and child sex, age at diagnosis, and intervention receipt. Autism diagnostic practices may be strengthened by considering the manifestation of autism features across social contexts and as observed by multiple informants (e.g., parents, teachers, clinicians), especially considering that autism is inherently a condition characterized by social differences.
Footnotes
Acknowledgements
The authors thank the families who participated in this research and Dr. Charles Nelson for his contributions to the ABC-CT.
Data accessibility
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: G.D. is on the Scientific Advisory Boards of Akili, Inc., Nonverbal Learning Disability Project, and Tris Pharma, Inc., provided consultation to Apple, Inc., Gerson Lehrman Group, and Guidepoint Global, LLC, received speaker fees from WebMD and book royalties from Guilford Press, Oxford University Press, Springer Nature Press. G.D. reports grant funding from NICHD, NIMH, and the Simons Foundation; G.D. has developed technology, data, and/or products that have been licensed to Apple, Inc. and Cryocell, Inc. and G.D. and Duke University have benefited financially. R.A.B. is currently employed by Apple. F.S. consults for Roche Pharmaceutical Company and Janssen Research and Development. J.C.M. consults with Customer Value Partners, Bridgebio, Determined Health, and BlackThorn Therapeutics, has received research funding from Janssen Research and Development, serves on the Scientific Advisory Boards of Pastorus and Modern Clinics, and receives royalties from Guilford Press, Lambert, Oxford, and Springer.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support was provided by NIMH U19 MH108206 (McPartland), the Autism Biomarkers Consortium for Clinical Trials.