
Abstract
Autism research and services have historically focused on individuals with a formal autism diagnosis. However, activists and self-advocates in the United States recognize that there are financial and clinical barriers impeding access to formal diagnostic evaluations for autism. Research also suggests that groups on the margins of autism, specifically those who are not White, young, or assigned male at birth, receive later diagnoses, if diagnosed at all. In particular, individuals who are autistic and LGTBQ+ are likely to not be afforded opportunities to be assessed and diagnosed. We conducted interviews with 65 queer and transgender autistic adults who either self-identified as autistic or had a formal autism diagnosis about their experiences with and perceptions of autism diagnosis. We found that participants derived a sense of meaning and affirmation from their autistic diagnosis and/or identity, faced significant barriers and deterrents to diagnosis, and experienced invalidation as both a barrier to and product of diagnosis. We argue that self-identified autistic individuals provide valuable context and data for many of the social processes and preferences reported by autistic people. We offer recommendations for research and services, specifically that many should not require formal autism diagnoses of participants.
Lay abstract
Most autism research and services focus on individuals with formal autism diagnoses. However, autism activists and self-advocates have raised awareness about the challenges that can prevent individuals from seeking or getting an autism diagnosis. We interviewed 65 queer and transgender adults who either self-identified as autistic without a formal diagnosis or who had a formal autism diagnosis. We found that participants made meaning of their autistic diagnosis and/or identity and found affirmation in this, faced significant barriers and deterrents to getting diagnosed, and experienced invalidation as both a barrier to and product of diagnosis. Due to the challenges that individuals face in getting a diagnosis, we recommend that researchers and advocates consider including self-identified autistic individuals in research and services.
Introduction
Autism is most often diagnosed in early life (van’t Hof et al., 2021) and, as such, most diagnostic infrastructure focuses on early detection in childhood. However, there are factors that may complicate the trajectory of seeking a diagnosis. In the United States, families and autistic individuals may wait months or years to be evaluated for a diagnosis due to inaccessibility of diagnostic services and the disjointed nature of the US healthcare system (Brewer, 2018). Families may also be reluctant to seek an autism diagnosis due to societal stereotypes and a poor understanding of what autism means (Azad et al., 2019; Rosenbrock et al., 2021). Children who do not display classic autistic traits, such as delays in verbal communication, may be overlooked (Bickel et al., 2015; Loubersac et al., 2023; McDonnell et al., 2019). This is even further complicated by the “lost generation” of autistic individuals resulting from changes in diagnostic criteria (Lai & Baron-Cohen, 2015; McDonald, 2020). Thus, autistic individuals may age out of early childhood without a diagnosis.
The process of receiving an autism diagnosis is made more complex by a lack of diagnostic infrastructure outside of early childhood services. Some clinicians are not comfortable diagnosing adults given the limited availability of assessment and diagnostic tools for this population, making healthcare access difficult for adults seeking a diagnosis or who are referred for assessment by other professionals (Baghdadli et al., 2017; de Broize et al., 2021). In addition, there is growing concern that the criteria for neurodivergent diagnoses, such as autism or attention-deficit/hyperactivity disorder (ADHD), do not adequately reflect autistic traits in adults, leaving many adults who do not meet diagnostic criteria designed for children without accurate diagnoses (Lewis, 2017; Mandy et al., 2018). Furthermore, many professionals who may recognize or suggest testing for autism operate in institutions that are focused on childhood, such as educational settings or pediatric medicine (Brewer, 2018). Thus, many individuals who do not receive a diagnosis in childhood may not recognize they are autistic, or pursue a diagnosis, until adulthood.
Sociodemographic patterns also predict who might receive a diagnosis (Fletcher-Watson, 2023). Historically, children of color in the United States have often gone undiagnosed or been misdiagnosed with other conditions, such as Oppositional Defiant Disorder or ADHD (Davis et al., 2022; Gourdine et al., 2011), and are more likely to be diagnosed with autism later in life, if diagnosed at all (Constantino et al., 2020). The androcentric roots of autism research, and specifically the emphasis on young White males (Lockwood Estrin et al., 2021; Moore, 2020; Roux et al., 2023), have led to clinical biases in perceptions of how autism presents (Jack, 2011; Krahn & Fenton, 2012). Individuals assigned female at birth (AFAB) are frequently underdiagnosed with autism because they present differently than clinicians expect, contributing to diagnostic delays for this population (Bargiela et al., 2016; Lockwood Estrin et al., 2021; Zener, 2019). These factors are magnified for AFAB of color (Botha & Gillespie-Lynch, 2022).
LGBTQ+ individuals may be at particular risk of facing barriers to a formal diagnosis (Lewis, 2017; Overton et al., 2023). There is a relative dearth of literature on the LGBTQ+ autistic population (Strang & Fischbach, 2023). Much of the previous research has focused on the co-occurrence of transgender and autistic identities, although often in pathologizing and stigmatizing terms (Gratton et al., 2023; Steinberg et al., 2022), including invalidation of individuals’ identities and use of controversial concepts such as male brain theory. There is also relatively little research on how LGBTQ+ identity is related to diagnostic timing of autism. Queer, gender nonconforming, and transgender children often struggle with finding affirming healthcare (Meadow, 2018), and individuals who identify as LGBTQ+ have historically had much more limited access to health services compared to heterosexual and cisgender individuals (Lund & Burgess, 2021; Matsuzaka et al., 2021; Meadow, 2018; Rattay, 2019). Individuals who are both autistic and queer and/or gender expansive face additional challenges to accessing healthcare services (Gratton, 2020; Hall et al., 2020) and likely experience unique and understudied barriers to autism diagnosis.
Self-identification as autistic remains controversial in most autism circles. Autistic self-advocates have raised concerns about the barriers faced by the undiagnosed autistic population (Autistic Self Advocacy Network, 2009). In light of the limitations in diagnostic practices and accessibility, some autistic self-advocates have critiqued the diagnostic criteria for autism, and some have supported the recognition of self-identification as legitimate. Although there are no current estimates of the proportion of autistic individuals who identify as autistic without a formal diagnosis, anecdotal evidence suggests that there may be a sizable number of individuals who fall into this category (Gratton, 2020; Overton et al., 2023; Sparrow, 2020). Thus, in this study, we used qualitative methods to focus on queer and transgender autistic adults who do not have a formal autism diagnosis but who self-identify as autistic, as well as those who were not diagnosed until later in life. We chose this population in part because it is worthy of study in its own right, but also because existing literature indicates that this population is likely to be overlooked for diagnoses and services.
This research is exploratory. We did not go into the research with a deductive research hypothesis. Our methods were qualitative and open-ended, and as such, themes and salient content came from interviewees themselves. We asked the following research questions: What are the experiences of queer and transgender autistic adults who did not receive a formal autism diagnosis in childhood? How does this population talk about diagnosis? What makes an individual decide whether to pursue an autism diagnosis in adulthood?
Methods
Participant recruitment
This study is part of a larger community-based study with 65 queer and transgender autistic adults, the details of which can be found here: https://doi.org/10.31235/osf.io/w3n7s. Nineteen local community organizations serving LGBTQ+ or disabled populations aided with recruitment. The recruitment flyer was advertised through these groups, on social media through the researchers’ academic department, and shared through snowball sampling. A screener allowed potential interviewees to share their preferences for how they wanted their interviews to be conducted. It also served as a mechanism to triangulate answers, which helped identify scam sign-ups (Pellicano et al., 2023). We allowed participants to choose their mode of interview. Sixty percent of participants chose Zoom video, 12% chose live text-based communication (via Zoom chat or Google docs), 12% chose email, 8% chose Zoom audio only, and 5% chose to be interviewed in person. In addition, we allowed participants to request specific interviewers, such as autistic interviewers or an interviewer of color. All interviewees identified as queer and/or transgender and autistic, understood English, and lived within 100 miles of Philadelphia.
Sample characteristics
Of the total sample of 65 queer and transgender autistic adults, 37 (57%) had a formal diagnosis and 28 (43%) self-identified as autistic without a formal diagnosis. Participants’ mean age was 29, with ages ranging from 18 to 71. Philadelphia is a diverse city, and we felt it was important to tap into networks of autistic people of color to adequately understand the experiences of queer and transgender autistic adults and to select a sample that was truly representative of the city’s population. Thus, we emphasized recruiting participants of color through mechanisms such as snowball sampling, the option of being interviewed by an interviewer of color, and community-based partnerships with organizations who served populations of color.
Although the self-identified and formally diagnosed groups presented with similar demographics, there was some variation between these groups. The formally diagnosed group was comprised of more cisgender participants, and the self-identified group was younger, on average. We note that all cisgender men (n = 5) received formal diagnoses. However, consistent with previous research, the demographics for the self-identified autistic subsample did not vary substantially from those reported by formally diagnosed individuals and the sample as a whole (Table 1).
Demographics of the entire sample, the subsample of formally diagnosed individuals, and the subsample of self-identified autistic individuals.
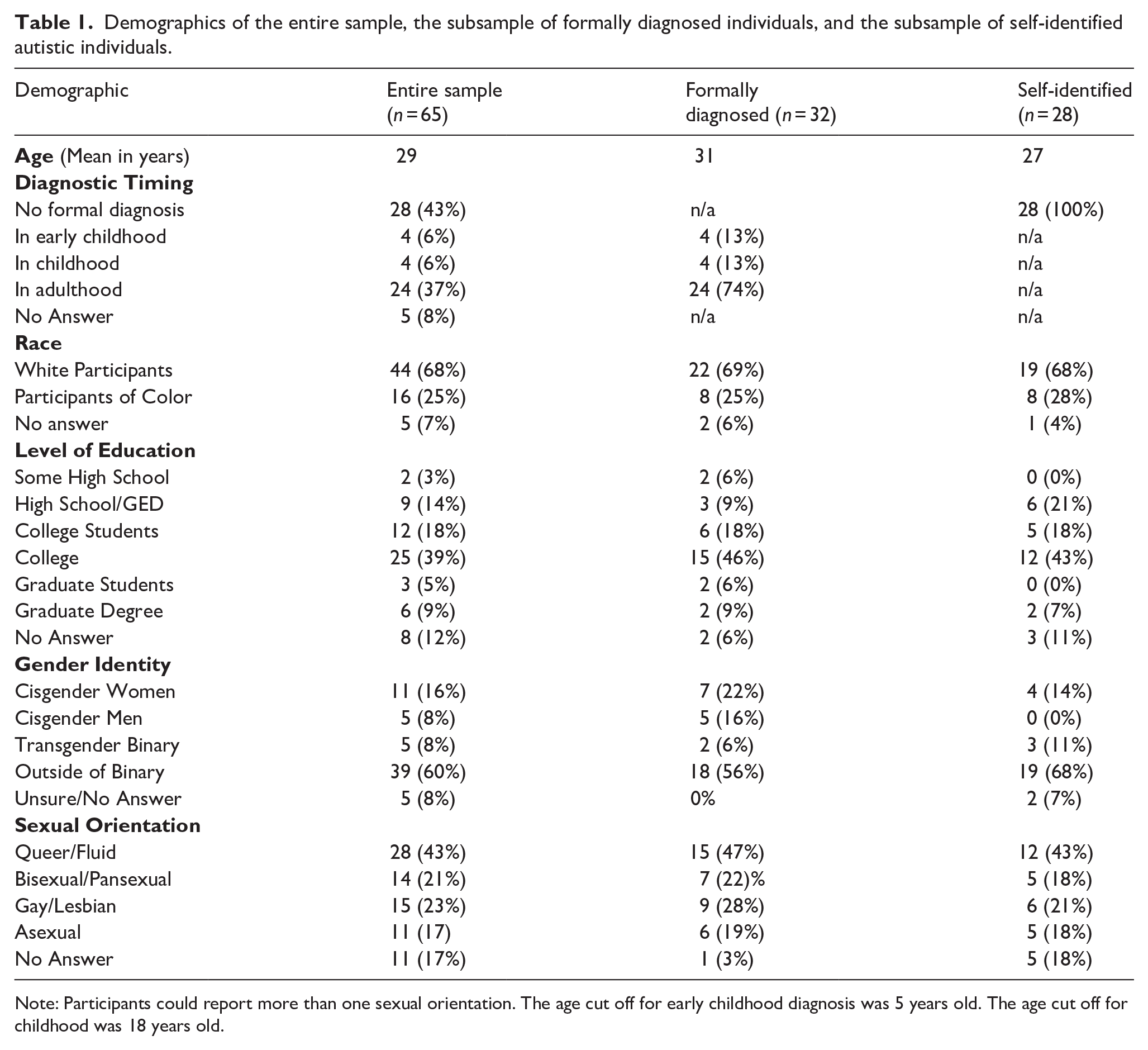
Note: Participants could report more than one sexual orientation. The age cut off for early childhood diagnosis was 5 years old. The age cut off for childhood was 18 years old.
Procedure
Participants underwent an extensive consent process that included sign-up, formal consent forms, and verbal check-ins before and during interviews. We reminded participants that they were in a study (Khan, 2013), allowed them to strike any information from the study, allowed them to skip answers or end the interview at any time, and gave them control of the flow of the interview. We conducted open-ended interviews given their utility in accessing hard to reach populations (Berger & Lorenz, 2015; Compton et al., 2018; Strang et al., 2019). Interview questions covered a wide range of topics and timeframes, including identity, childhood, aspects of adult life (e.g. employment, relationships), and experiences with healthcare and education. Many of the interviews in this study resembled life history interviews because participants had not had an opportunity to talk about these topics previously. This project was approved by the second author’s institutional review board.
Interviews typically lasted about 1.5 to 2 h. The interview guide can be found in Appendix 1. Participants were compensated with a US$50 gift card to Amazon, Target, or Walmart. All names used in this article are pseudonyms chosen by participants unless they declined to choose, in which case the interviewer selected a name.
Analysis
Interviews were transcribed by a third party and de-identified by the research team. The first author led an exploratory analysis on data related to self-identified autism and the diagnostic process, which developed from the team’s observations from an initial analysis on content related to mental health generally. During the first phase of analysis, we examined responses to two questions on the interview guide that directly asked about mental health and healthcare (“What is your view of your mental health?,” “What is seeking healthcare like for you?”) in order to better understand participants’ experiences with their mental health and seeking related care and services. We were not seeking to understand objective truth, but rather understand how interviewees felt and their motivations (Small & Cook, 2023).
During this stage of the analytic process, we noticed a recurring theme around experiences with and perceptions of autism diagnosis. We discovered that many participants in our sample self-identified as autistic or did so for a period of time before obtaining a formal diagnosis. Furthermore, although participants were not asked specifically about their motivations for pursuing a diagnosis, an open-ended question about whether interviewees had a diagnosis elicited answers about their motivations and perceptions. We also noticed when reviewing the full transcripts that participants often discussed their autistic identity with or without a formal diagnosis in response to other questions throughout the interviews, such as questions about relationships and their experiences with education and employment. This theme was so salient throughout the interviews that we felt it warranted its own investigation. As a result, we conducted an exploratory analysis of content related to autism diagnosis and self-identifying as autistic (Small & Cook, 2023) using thematic and line-by-line coding (Braun & Clarke, 2022) in NVivo (Deterding & Waters, 2018). Our team leaned into the strengths of interview data by focusing on motivations and narratives.
The research team engaged in active discussions and memoing during data collection and analysis, allowing us to refine our approach (Rubin & Rubin, 2012). Once we identified common themes, we sought out disconfirming evidence (Lareau, 2012; Tavory & Timmermans, 2013) and used the constant comparative method (Glaser, 1965). The team was familiar with the emerging literature on self-identified autism and with community sentiments around the topic. We did not have a formal hypothesis, and instead constructed themes based on what interviewees emphasized and patterns in the data. Thus, the analysis was both inductive and abductive (Timmermans & Tavory, 2012). This approach was used to center the experiences of the autistic individuals in our study, rather than relying on research and literature on autism conducted by predominantly non-autistic people (Ratto et al., 2023).
We engaged in reflexivity as defined as an iterative, collaborative process that influenced our decisions and focuses based on our positionality (Olmos-Vega et al., 2023). We prioritized the viewpoints, narratives, and lived experiences of our interviewees, and this was dictated by our experiences, including our analyses led by the authors who identify as queer and transgender autistic adults. Thus, rather than a focus on objectivity and validity in a positivist sense, we were more interested in catalytic validity, or the construction of social knowledge that reorients ideologically what we know and how we know it in our field of research (Lather, 1986).
Autistic and queer community involvement statement
We chose a qualitative community-based approach due to recognition that the study population can be hard to reach and is often disconnected from formal autism programs. Our research team and interviewers consist of scholars representing queer and autistic identities, including representation of self-identified autism. Our team includes a mix of community organizers, counselors, and academics. The first five authors interviewed participants, and the first two authors coded the interviews for this study. All the authors shaped each stage of research. Before submitting for publication, we engaged in member checking, which involved sending participants a draft of this article to ensure they agreed with how their experiences were portrayed. We will ensure that future directions of this research continue to include community feedback and involvement.
Findings
Our sample included participants who self-identified as autistic and did not have a formal diagnosis, as well as those who received a late diagnosis in adulthood. Three primary themes were identified related to diagnosis and reasons for self-identifying as autistic without a formal diagnosis. First, participants found meaning in their autistic diagnosis and/or identity, and this helped them make sense of their current and past experiences. Second, there were significant barriers and deterrents to obtaining a formal autism diagnosis. The third theme—invalidation—was illustrated in a range of ways, including invalidation of participants’ autistic identities and invalidation of their abilities as a response to their autistic identities. These themes are summarized in Table 2 and described in greater detail in the following sections.
Themes and subthemes of findings.
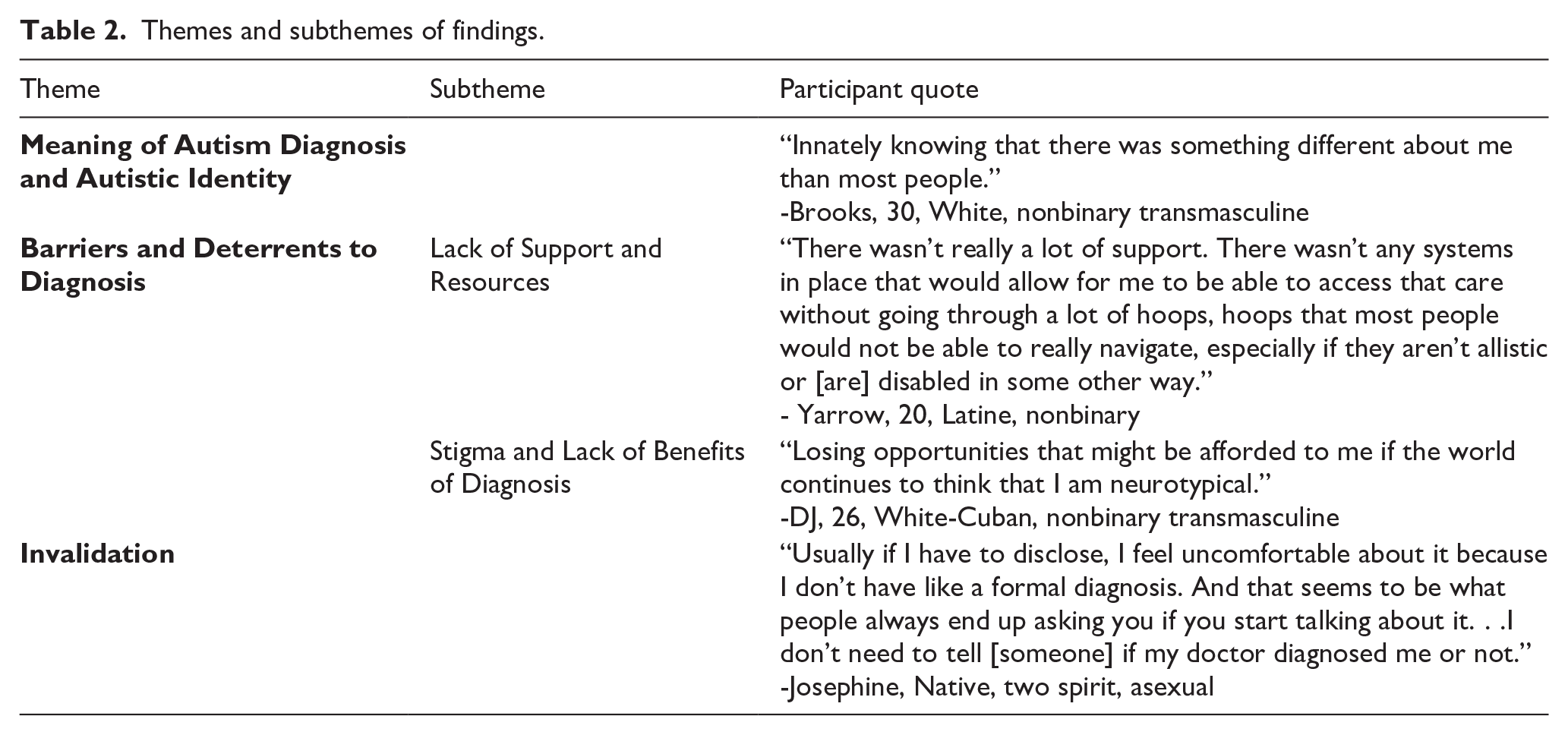
We found that some autistic adults who were not formally diagnosed desired a diagnosis. However, they had trouble obtaining a diagnosis or faced serious barriers to doing so. Others felt they did not need one because they were secure in their autistic identity, or actively avoided a diagnosis due to fears of invalidation or stigma.
Meaning of autism diagnosis and autistic identity
For many interviewees, their autistic identities provided a greater understanding of themselves, their experiences, and their relations with other people. This contributed to a process of meaning making that helped participants make sense of their experiences and find affirmation in their identities. Many interviewees who were not diagnosed as children began exploring a potential autistic identity in adulthood. They reported a range of reasons for identifying as autistic, including beliefs that they perceived the world differently from their peers and having common experiences of being “othered.” They described “innately knowing that there was something different about me than most people” (Brooks, 30, White, nonbinary transmasculine) or an awareness “that my brain works differently from other people’s” (Elizabeth, 26, White, cisgender woman). For some, this came about through reflecting on the impact of their early life experiences and the challenges they faced during childhood and adolescence that were consistent with an autism diagnosis. These perceptions set the foundation for many participants to consider the possibility of being autistic.
For some, looking into diagnostic criteria for autism provided them with a better understanding of themselves and clarified whether their characteristics were consistent with a diagnosis. Elizabeth shared how her exploration of her own autistic identity led to her investigating diagnostic criteria: “I started to suspect that I was autistic and so I looked up ‘symptoms of autism in adult women’ and felt rather, spoken to? I felt that I could identify a lot of the characteristics in myself.” Seeking a diagnosis or self-identifying as autistic helped many make sense of their experiences and ways of navigating the world. This, in turn, provided many participants with a sense of affirmation. For some, it was “the first time in my life I was truly able to love myself” (Paige, 23, White, cisgender) and signified a new chapter in their life. Others talked about how understanding and accepting their autistic identity benefited them psychologically, even helping to alleviate mental health issues. Some participants felt affirmed when their current therapists or doctors who may not have been qualified to diagnose autism acknowledged the possibility of them being autistic. Many of these participants did not feel the need to pursue a formal diagnosis.
Taking ownership of their autistic diagnosis or identity provided participants with a greater understanding of their experiences and affirmation of their perspectives. However, despite the importance and meaning that many participants attached to having an autism diagnosis, participants faced significant barriers to receiving a formal diagnosis and deterrents to embarking on this process.
Barriers and deterrents to diagnosis
For most participants, the diagnostic process was fraught with difficulties. Participants described obstacles to assessment and having their autistic traits acknowledged by others. For many, this study provided the first opportunity to share their experiences as autistic and gender diverse individuals. Lack of support and resources, stigma, and lack of perceived benefits of being diagnosed were some of the most frequently mentioned barriers and deterrents to seeking a diagnosis.
Lack of support and resources
Participants described barriers impeding them from seeking or receiving an autism diagnosis. Chief among these was a lack of support from their families and providers. Some participants reflected on how aspects of their family life or childhood interfered with them being evaluated for autism at an early age. In some cases, delays in diagnosis were a result of caregivers’ lack of resources. However, many participants who were not diagnosed reported that their families “[didn’t] really necessarily believe in affirming” (Tracy, 24, Black, agender masculine) their neurodivergent characteristics, or they were told that their child “might have autism, but it was written off” (Toad, 28, Latine and White, nonbinary transgender woman). Parents’ misunderstanding of autism and attempts to protect their children from the implications of a diagnosis interfered with receiving a timely evaluation in childhood. This meant that participants’ autistic traits often went unnoticed or were intentionally ignored throughout their childhood.
In many cases, participants were not diagnosed in childhood because they did not match the typical demographics of people who oftentimes receive autism diagnoses, namely, young White males. DJ (26, White-Cuban, nonbinary transmasculine), who was AFAB said, “My brother . . . was diagnosed as autistic really early in life. And that’s not something that was afforded to me because I was seen as a girl.” The accounts of many AFAB participants reflected their belief that being AFAB contributed to them not being diagnosed in childhood due to the fact that “the diagnostics are written for a very specific person” (Ky, nonbinary, intersex). Many participants worried that, “even though I qualified for [autism] . . . I don’t think I’m getting diagnosed” (Ky). In addition, many participants reported challenges with receiving an autism diagnosis in adulthood. For many, not receiving timely diagnoses in childhood often translated to continued challenges with seeking a diagnosis and appropriate supports as adults. Josephine (Native, two spirit, asexual) shared their experience of attempting to be assessed for ADHD and autism, only to find out that their psychologist, “wouldn’t diagnose me with [autism or ADHD] . . . because I didn’t have services as a child, I wasn’t in special education.” Thus, although participants perceived that it was generally more feasible to be diagnosed in childhood, many were still not afforded that opportunity during their early years.
Those who were interested in seeking a formal diagnosis faced a lengthy and exhausting process. To be assessed by a diagnostic specialist, individuals needed to obtain an initial referral from a primary care provider (PCP). Without a referral from a medical provider, insurance often would not cover the costs of diagnostic assessments. Financial barriers, including limited insurance coverage, impacted participants’ ability to engage in the diagnostic process, leaving many feeling like there were not “a lot of resources that would allow for someone to be able to access a diagnosis without having money” (Yarrow, 20, Latine, nonbinary).
In addition, lack of accessibility of diagnosticians was one of the most prominent barriers that participants encountered. Even with a referral from a PCP, long waitlists and a dearth of providers who were qualified to diagnose autism in adults proved to be significant barriers to diagnosis. Participants were “told it’d take years for [them] to see someone” (Joan, 27, White and Black biracial, nonbinary) or, in some cases, that they needed to stay in the same geographic area while being on a waitlist with an indefinite timeline just to get a first appointment. Thus, participants faced significant barriers to diagnosis and insufficient resources to allow them to overcome these barriers. This resulted in many participants wanting “to just give up and forget about it because there’s so little access to any resource to get a diagnosis” (Q, 19, White, nonbinary), despite their conviction in their autistic identity. The inaccessibility of diagnostic and assessment services that so many participants encountered was summarized by Yarrow:
There wasn’t really a lot of support. There wasn’t any systems in place that would allow for me to be able to access that care without going through a lot of hoops, hoops that most people would not be able to really navigate, especially if they aren’t allistic or [are] disabled in some other way.
Stigma and lack of benefits of diagnosis
Many participants shared how personal and societal stigma against autistic individuals interfered with their ability or desire to seek a diagnosis. Participants felt it was necessary to weigh “the pros and cons of actually getting a formal diagnosis and that it can be helpful or empowering and it can also sometimes in fact do the exact opposite” (Casey, 31, White, nonbinary transgender). The potential benefits of a diagnosis—such as accommodations at work or school—were often balanced against the possible risks of having their diagnosis misunderstood or weaponized. Brooks described his experience with this dilemma:
I definitely feel guarded about [disclosing autism diagnosis]. I would say the thing that I felt most tempted to get evaluated for was for workplace accommodations. But at the same time, I do feel very anxious to bring up being autistic in the workplace. Like even having very supportive coworkers and a supportive boss, it’s just something that I worry would be used against me in some way.
Consistent with what Brooks described, many participants expressed concerns about facing stigma and discrimination if they were to receive and disclose a formal diagnosis.
Participants had real reservations about going through the diagnostic process, especially if they believed there would be no tangible benefits to doing so. Many expressed concerns that they would be “losing opportunities that might be afforded to [them] if the world continues to think that [they are] neurotypical” (DJ). Some interviewees worried that having an autism diagnosis would hinder their ability to succeed in the future due to discrimination. A few believed that having an autism diagnosis on their record could curtail their ability to move to another country or interact positively with clinicians or coworkers. Lynn (30, White, cisgender woman) said she considered a diagnosis but, “I think that would be more harmful than helpful. Because when people find that sort of stuff out, they start to treat you differently and I’m not really interested.” Furthermore, real or potential experiences of having their diagnosis used against them deterred many participants from desiring a formal diagnosis. In some cases, participants’ autistic identity was used to deny them access to lifechanging health services. For example, DJ described how their experience of seeking a provider to write a letter of support for them to receive gender-affirming care was impacted by stigma against them as an autistic individual, even without having a formal diagnosis:
My mom decided to share with the gender therapist that I might be autistic, which was kind of the first time she acknowledged that. But she did it to make the therapist treat me with more scrutiny of can you really be making this decision for yourself? Questioning my autonomy because I’m autistic and I think if I face that, I’m sure somebody with an actual full diagnosis has struggled with getting either therapy or hormones or even a surgery date, I’m sure. It just opens up more avenues or reasons for a doctor to deny you those services based off of, well, you know, you have special needs, can you make a decision for yourself?
Thus, some individuals avoided an autism diagnosis because they feared it could lead to worse treatment and other negative consequences. For many, these concerns led them to conclude that the risks of a diagnosis outweighed the potential benefits.
Invalidation
Invalidation or the fear of invalidation from healthcare providers and others in their life proved to be both a barrier to and a product of receiving a diagnosis. Invalidation from healthcare providers created distrust of health professionals. Participants perceived that providers often lacked the knowledge and skills to work with autistic individuals, particularly those who were queer or transgender. Casey expressed that if they were to be assessed by a professional,
I would want to make sure that the person was competent when it comes to gender stuff and all the intersections of that. And I just don’t have faith that that’s what the majority of providers are doing right now.
Concerns about provider competence, along with feeling misunderstood by providers, proved to be additional deterrents to engaging in the diagnostic process.
Participants reported instances of providers questioning or dismissing their symptoms or desire for a diagnosis, including misdiagnosing them. Many participants reported being misdiagnosed by a professional at least once in their life, and quite a few experienced multiple instances of misdiagnosis. Interviewees described experiences of having their autistic traits mistaken for symptoms of other DSM diagnoses. Stephen (45, White, nonbinary demiguy) recounted the inconsistencies in the diagnoses he had received throughout his life: “So they, at the time, I think said I had bipolar disorder. Then I think they changed it to PTSD. I’ve had some bizarre diagnoses that I thought were really dissociative identity disorder. I had that for five minutes.” Many attributed these inconsistencies in diagnostic practices to providers not having an adequate understanding of how autism presented in adulthood. For many, the possibility of them being autistic was dismissed, and they were instead given an alternative diagnosis that they felt did not match their experience. Yarrow shared an example of the invalidation they experienced during their pursuit of an autism diagnosis:
I would have appointments for psychiatrists or people who were treating me and they would dismiss [an autism diagnosis] . . . And the thing about it was that the dismissal was usually not coming from a place of, oh, “this isn’t something that we’re able to help you with. You should see a specialist.” It was more so, “well, we feel that this might be depression instead, but we don’t have any validity surrounding those claims, but we’re still going to act like that’s the solution, even though you’re communicating that it’s not and it hasn’t been.”
Yarrow’s account demonstrates how perceived invalidation of participants’ experiences and expertise about their own lives often resulted in misdiagnosis or refusal to provide any diagnosis for participants seeking validation or clarity about their traits.
Participants without a formal diagnosis also experienced lack of acceptance or perceived validity of their autistic identity by others in their lives. Some described this as having “imposter syndrome” due to not having a formal diagnosis and, as a result, not being taken seriously. While they may have felt confident in their autistic identities, participants who experienced invalidation from people in their life often consequently felt uncomfortable sharing their identity with others or were “too terrified of other people invalidating [their] identity” (Paige). Josephine had similar concerns and described how they dealt with this issue:
Well, usually if I have to disclose, I feel uncomfortable about it because I don’t have like a formal diagnosis. And that seems to be what people always end up asking you if you start talking about it . . . I don’t need to tell [someone] if my doctor diagnosed me or not.
Participants who self-identified as autistic often felt silenced with regard to sharing their autistic identity. The real or potential experience of invalidation resulted in participants suppressing expression of their autistic identities, which prevented them from disclosing and further exploring their identities with others. This extended to denial of opportunities to participate in research and other chances of increasing general awareness and understanding of their experiences.
Discussion
In this study, we focused on the narratives and experiences of queer and transgender autistic adults who had not received a formal autism diagnosis or who were diagnosed in adulthood. Overall, most participants experienced professional, interpersonal, and logistical barriers to diagnosis that frequently dissuaded them from continuing with their search for a diagnosis or from seeking one at all. As a result, many participants turned to self-identification as an alternative to being formally diagnosed. Self-identified autistic adults in our study highlighted two major reasons that they were not diagnosed: lack of access to diagnostic services and concerns that a diagnosis would not improve their lives. This also presented a dilemma—lacking a formal diagnosis prevented some participants from receiving adequate therapeutic care and supports, but a diagnosis in adulthood also did not guarantee these services, especially if they were difficult to access.
The fact that a diagnosis would not necessarily grant participants access to appropriate services, and instead may have hindered their ability to achieve success in the ways they defined, reveals flaws and serious equity issues in how autistic adults are treated. Numerous barriers to obtaining an autism evaluation persist, including the availability of qualified evaluators, comprehensive health insurance, and substantial financial and time investments. These hurdles disproportionately impact autistic individuals from marginalized communities, including queer and transgender individuals, and LGBTQ+ individuals have increased challenges accessing autism diagnoses and services. As the participants in this study reflected, there are many subsets of autistic people who are at increased risk of not receiving formal diagnoses: those who may not have the resources to obtain a diagnosis, those who deviate from normative presentations of autism, or those who feel they are at risk of harm if they receive a diagnosis.
Self-identification does not equate to clinical diagnosis, but it does provide context for many of the social processes that autistic people without a formal diagnosis engage in. Therefore, to enhance autism research, we argue that many studies should not exclude individuals who do not have proof of a formal autism diagnosis without specific motivation to do so. Future research should include these individuals particularly to understand barriers to diagnosis, such as misdiagnosis or clinician bias. An increasing body of evidence suggests there is value in including self-identified autistic individuals in research, especially since they have similar results to those with formal diagnoses (Overton et al., 2023). In fact, the interviewees with self-identified autism in our study did not vary substantially from the other interviewees. Broadening the definition of who can be included in autism research will provide nuance to our overall understanding of autism.
In addition, it is the responsibility of the medical system and its connected infrastructure to meet the needs of autistic individuals and help them access appropriate services. Traditional clinical training and research related to autism may reinforce limiting stereotypes and views of autistic people (Botha & Cage, 2022). Clinicians should be prepared to support autistic people in forming a positive sense of neurodivergent identity (Chapman & Botha, 2023). This involves being understanding and respectful of autistic people’s choices related to seeking a formal diagnosis.
This study had several limitations. First, this study took place in one urban area with strong medical infrastructure and existing autism services. Issues with access to diagnostic services may be magnified in other areas, such as in rural settings. In addition, interview studies can never be truly replicable due to the nature of qualitative inquiry, including historicity and the nature of collecting a sample (Pugh, 2013; Rinaldo & Guhin, 2019). In addition, many of the interviewees who self-selected into our study were fairly new to identifying as autistic and may have been more excited to speak to us due to this discovery. Finally, we did not recruit as many nonspeaking individuals or individuals with high support needs for independent living as we anticipated. Future research on self-identified autism should focus on these understudied and hard to reach populations.
Conclusion
Autistic people who experience multiple compounding forms of marginalization associated with barriers to diagnosis are at risk of experiencing greater levels of stress and disadvantages, resulting in heightened disparities. Many autistic individuals may not be diagnosed in early childhood for a number of reasons and may face severe barriers in obtaining a formal diagnosis in adulthood. These, combined with stigma and lack of resources for autistic adults, sometimes drive those who identify as autistic to eschew a diagnosis. Thus, some autistic individuals cannot access a formal diagnosis despite their desire to obtain one. Without including individuals who have not received a formal diagnosis in research, those with the greatest service-related barriers are at increased risk for negative outcomes and may remain invisible in clinical care and research.
Footnotes
Appendix 1
Acknowledgements
We foremost thank the interviewees who contributed to this work for their care and time, and for sharing their viewpoints with us. We also thank the community organizations who believed in this work and partnered with us.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Eagles Autism Challenge provided material support and funding for this research. This project was supported by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) under cooperative agreement UT6MC45902 Autism Transitions Research Project. The information, content, and/or conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the US Government.