
Abstract
Accurate identification of autism is critical for timely intervention, yet validated screening tools remain limited in Latin America. This study evaluated the psychometric properties of the Spanish-translated Social Communication Questionnaire (SCQ) in a clinic-based sample of children in Quito, Ecuador. Caregivers of 94 children aged 4-18 years completed the SCQ Lifetime form as part of a diagnostic evaluation that included cognitive testing, developmental history, and the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2). Internal consistency of the SCQ was good (Cronbach’s α = .843). However, the SCQ showed poor diagnostic accuracy, with an area under the receiver operating characteristic curve (AUC) of .60. At the conventional SCQ cut score of 15, sensitivity and specificity were .56 and .60, respectively; using a lower cut score of 11 increased sensitivity (.72) but decreased specificity (.43). These findings indicate limited utility of the SCQ as a screening instrument for autism in this clinical context. Results align with other studies showing variability in SCQ performance across diverse populations and settings, highlighting the need for locally validated screening tools.
Lay Abstract
Early and accurate identification of autism helps children and families access helpful supports, yet most screening tools have been developed and tested mainly in English-speaking countries, and we know less about how well they work in Latin America. In this study, we examined how well a Spanish translation of the widely used Social Communication Questionnaire (SCQ) identified autism in a clinic in Quito, Ecuador. Caregivers completed the questionnaire as part of a full clinical evaluation by trained professionals. We found that the SCQ was not very accurate at distinguishing which children did or did not have autism in this setting, meaning it may not be reliable on its own for screening. These results suggest that screening tools should be carefully tested with local communities before widespread use and highlight the need for tools that better reflect the languages, cultures, and experiences of families.
Introduction
Autism is a neurodevelopmental condition that is prevalent worldwide, with global estimates suggesting that 1% of children meet criteria for this diagnosis (Zeidan et al., 2022). However, prevalence estimates vary widely between countries (Zeidan et al., 2022), reflecting differences in health care systems to diagnose autism. Several valuable screening tools have been established to help facilitate greater screening and diagnosis of autism (e.g. Modified Checklist for Autism in Toddlers, Robins et al., 2014; Social Communication Questionnaire (SCQ), Rutter et al., 2003). However, some evidence-based autism-screening tools commonly used in Western, high-income, English-speaking countries have been found to be less useful when translated and adapted in linguistically diverse low- and middle-income countries (LMICs) (Bauer et al., 2022). A review of autism-screening tools highlighted that while there are dozens of autism-screening tools available across all languages, only five are available in Spanish for early autism screening, and thus far, the study of their psychometric properties has been limited (Alonso-Esteban et al., 2020). The limited availability of feasible and valid autism-screening tools for use among linguistically diverse children in LMICs very likely contributes to delayed identification and under-identification of autism. This is concerning because autism identification and intervention earlier on in childhood is linked to better child outcomes (Estes et al., 2015; Kasari et al., 2010; Shi et al., 2021). Taken together, these findings suggest an urgent need to validate Spanish language autism-screening tools for children in LMICs.
The SCQ (Rutter et al., 2003) is a brief, caregiver-report screening instrument derived from the Autism Diagnostic Interview-Revised (ADI-R) and is widely used internationally. It assesses social communication deficits and restricted or repetitive behaviors, two core domains of autism. In terms of its validity, a meta-analysis of 17 studies, 15 of which were conducted in either North America or Western Europe, found that the sensitivities and specificities of the SCQ ranged widely by study (Chesnut et al., 2017). For the included studies, sensitivities ranged from .470 to .960, and specificities ranged from .520 to .999. The authors highlighted that individual study methodological decisions such as sample characteristics, which version of the SCQ was used, and child ages impacted the measure’s screening accuracy. Other factors that may impact the accuracy and validity of the SCQ as a screening tool include various cultural and linguistic contexts where the meaning of SCQ items may vary, as well as decisions related to cutoff scores. For example, one recent study conducted with 205 adolescents and their parents in urban areas of Nigeria found the SCQ’s validity was optimized when the cutoff score was lowered from the standard cutoff score of 15–10 (Nwokolo et al., 2024). At a cutoff score of 10, the SCQ’s sensitivity was .81, and the specificity was .88 (Nwokolo et al., 2024). Another study conducted with 819 Chinese children and their parents using a simplified Chinese version of the SCQ found that, in order to maximize sensitivity and specificity, SCQ cutoff scores should vary by child age and child diagnosis (Liu et al., 2022), specifically recommending a lower cut score for those under the age of 4 years. Taken together, these results underscore the need for local validation of the SCQ and highlight the role of methodological decisions on the SCQ’s screening accuracy. Only one unpublished dissertation study has examined its psychometric properties in a Spanish-speaking Latin American country (López Chávez & Catalina, 2016) and found that using the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2; Lord et al., 2012) as a proxy for formal diagnosis, the SCQ showed excellent diagnostic accuracy, with sensitivity and specificity of .92 and .93, respectively. This study did not employ other measures of comprehensive autism evaluation, such as developmental history and cognitive assessment.
Objectives
The primary objective of this study was to evaluate the psychometric properties of the Spanish-translated version of the SCQ in a clinic-based sample in [LATIN AMERICAN CITY]. Specifically, we aimed to assess internal consistency, overall discriminatory ability, and the sensitivity and specificity at two commonly recommended cut scores. By providing evidence on the SCQ’s performance in a Latin American context, we sought to inform its utility as a screening instrument and contribute to the broader effort of improving accurate identification of autism in this region.
Method
Participants
Study participants were children referred to a specialty clinic in [LATIN AMERICAN CITY] for developmental or behavioral concerns. Children were eligible if they were between 4 and 18 years old. A total of 94 children (age M = 8.11, SD = 3.16) met inclusion criteria and were included in analyses. Of these children, 90.4% were verbal, as defined by SCQ Item 1 (“Is the child now able to talk using short phrases or sentences?”). SCQs were completed by the child’s mother (78.7%), father (9.6%), both parents together (8.5%), or another family member (3.2%). Gender for the majority of participating children was reported as male (72.3%).
Measures
The SCQ Lifetime version was completed by caregivers. The Lifetime version captures behaviors across the child’s developmental history, with 19 items asking about current behaviors and 21 items asking about behaviors when the child was between 4 and 5 years old. All items are dichotomous (i.e. present/not present) and scored as a “1” if indicative of a behavior associated with autism and a “0” if not. The first item on verbality does not count for scoring, so total scores range from 0 to 39, with higher scores indicating more autism-related behaviors. A standard cut score of 15 is typically recommended in clinical practice, although some studies suggest lower thresholds, that is, 11, may be more appropriate in certain populations to improve sensitivity (Corsello et al., 2007). This study used the standard Spanish translation of the SCQ (Rutter et al., 2019), without adaptation. Details on the process of translating and/or adapting the measure are not provided by the publishers. All children were assessed using the Spanish ADOS-2, and many also completed the Spanish version of the Wechsler Intelligence Scale for Children (WISC; Wechsler et al., 2017), as part of the evaluation. The WISC was included in this study to characterize overall child cognitive functioning and determine if SCQ screening performance was associated with child cognitive ability.
Procedure
Caregivers completed the SCQ as part of the diagnostic evaluation process. Clinicians helped clarify the meaning of items if caregivers had questions or were unsure. Final clinical diagnoses were established using a comprehensive assessment that also included cognitive testing, detailed developmental history, and the ADOS-2, administered by trained clinicians. SCQ scores were then compared to final clinical diagnoses to assess screening performance.
Data Analysis
Receiver operating characteristic (ROC) analyses were conducted to evaluate the overall discriminatory ability of the SCQ, with the area under the curve (AUC) providing a measure of accuracy. Sensitivity, specificity, positive predive value (PPV), and negative predictive value (NPV) were calculated for the commonly recommended cut score of 15 and the alternative lower cut score of 11. Internal consistency of the SCQ was evaluated using Cronbach’s alpha. Group differences in cognitive ability were examined using one-way ANOVA comparing WISC-V Full Scale IQ scores across true positive, true negative, false positive, and false negative screening outcome groups. Data are available upon request.
Results
Of the 94 children in this sample, 64 (68.1%) received a diagnosis of autism, while 30 (33.0%) did not. For those who did not receive an autism diagnosis, the most common alternative diagnoses were attention-deficit/hyperactivity disorder (ADHD), oppositional defiant/conduct disorders, anxiety disorders, language or communication disorders, and learning disorders. The mean SCQ score across all participants was 14.88 (SD = 6.98), with scores ranging from 1 to 29. There was no significant difference in SCQ scores between non-verbal or minimally verbal children (M = 15.33, SD = 6.25) and verbal children (M = 14.84, SD = 7.08), t(92) = 0.20, p = .840). Internal consistency was good, with Cronbach’s alpha = .84, 95% CI [.79, .88], indicating that items on the SCQ were reliably measuring a cohesive construct. ROC analyses indicated an AUC of .60, suggesting poor discrimination between children who did and did not receive autism diagnoses (see Figure 1). At the standard cut score of 15, the SCQ demonstrated a sensitivity of .56 and a specificity of .60, indicating that the SCQ correctly identified 56% of children ultimately diagnosed with autism while accurately excluding 60% of children without autism. The PPV, or the likelihood that a positive screen correctly indicated autism, was .75, and the NPV, or the likelihood that a negative screen correctly indicated no autism, was .39. Using the lower cut score of 11 increased sensitivity to .72 but decreased specificity to .43; at this threshold, the PPV was .73, and the NPV was .42.
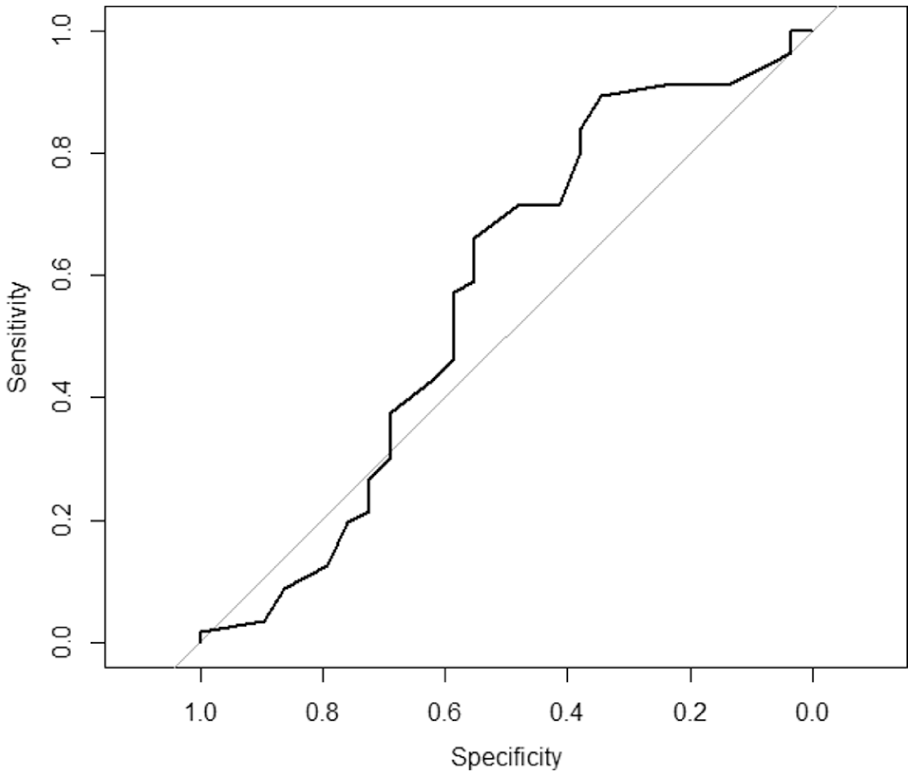
ROC curve of SCQ scores for classification of autism diagnosis.
Children’s cognitive scores on WISC-V were below average overall (M = 75.13, SD = 17.85). However, mean IQ did not differ significantly across screening outcome groups, F(3, 63) = 1.37, p = .259, and was not significantly correlated with SCQ score r = −.18, p = .138, indicating that SCQ screening performance was not associated with children’s cognitive ability.
Discussion
Findings from this study indicate that the Spanish-translated SCQ demonstrates poor accuracy as a screening instrument in this clinic-based sample in [LATIN AMERICAN CITY]. This study adhered to methodological conventions identified as critical in prior SCQ reviews, including the use of the Lifetime form, exclusion of children under 4 years of age, and reliance on a clinic-based sample (Corsello et al., 2007). These considerations strengthen validity and comparability with prior research in international contexts. Neither the overall AUC score, nor the commonly accepted cut scores indicated that the measure accurately discriminated between children with and without autism. The sensitivity and specificity found in this study are within, if albeit on the lower end of, the range of scores found in a metanalysis of the measure from international samples.
This study was also unique in focusing exclusively on a clinic-based sample without neurotypical controls. This likely reduced SCQ performance and may indicate its utility in identifying clear cases of autism in the general population, rather than diagnostically complex clinic referrals.
These results also corroborate anecdotal experiences of providers in this clinic who requested we conduct this study due to feeling as though clients were often having difficulty understanding the meaning of SCQ items even after explanation. We do not believe that these results should be taken to mean that the SCQ is necessarily unhelpful for conducting autism evaluations in Latin America. Rather, we believe they underscore the need for further work to examine the understandability and utility of the measure with larger samples and the potential value of creating or more deeply adapting assessment tools within local context rather than relying solely on translations from abroad (López et al., 2023; Mata-Iturralde et al., 2024). Consistent with prior studies outside the United States, these findings highlight that cultural and contextual factors can influence SCQ performance and that local validation is essential to ensure accurate screening.
Limitations
Several limitations should be noted. Most notably, the relatively small sample size may have influenced the precision of sensitivity and specificity estimates and did not allow for examination of age-specific cut scores. In addition, the children in this sample demonstrated IQ scores on the lower side of average, which may have further influenced SCQ performance and highlights the need to consider cognitive factors when interpreting screening results. Demographic characteristics such as caregiver age and caregiver educational attainment were not collected. Thus, we could not assess if these factors were associated with SCQ responses. We also did not assess how well participants felt they understood the items of the translated SCQ, and thus, we cannot conclusively say that misinterpretation factored into the results.
Conclusion
Results are consistent with the variability reported in other SCQ studies in diverse contexts and underscore the importance of developing and validating autism-screening tools in local settings. Future research should investigate additional barriers related to language and comprehension that may influence screening accuracy and consider the role of cognitive ability in screening outcomes.
Footnotes
Acknowledgements
We would like to thank the Neurodesarrollo Quito clinic staff for their valuable work and support in preparing and maintaining the dataset used in this study.
Ethical Considerations
Ethical approval was not required for this study, as the dataset was prepared by the clinic director and was completely deidentified prior to analysis.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research did not receive any grant funding. The first author’s time was supported by award 1K23MH136346-01A1.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.