
Abstract
Social communication interventions to support autistic people are primarily developed and tested in Western countries with predominantly White, English-speaking participants. Although numerous frameworks have been developed to adapt these interventions for diverse ethnocultural groups, the quality of these adaptations is not well understood. This review used the Cultural Adaptation Checklist (CAC) to appraise the quality of cultural adaptations of social communication interventions for autistic children and adolescents. Searches across eight databases identified 16 studies involving 474 participants. Included studies reflected seven different culturally adapted interventions delivered across 12 countries in 11 languages. The methodological quality of the studies was assessed using QualSyst, and data were analyzed through narrative synthesis. All studies demonstrated at least adequate methodological quality, but only three reported using a specific framework to guide their cultural adaptations. The extent of adaptations varied, with fulfillment of CAC items across studies ranging from 44% to 91%. This review highlights the need for more comprehensively reported cultural adaptations to best support the global autistic community. The CAC offers a useful framework that researchers can use to facilitate this process. Future research should examine to what extent cultural adaptations are needed and which types of adaptations best support desired intervention outcomes.
Lay Abstract
Many programs have been designed in Western countries to support social communication skills such as understanding others, making friends, and building relationships in autistic people. Those who participate in these programs have mainly been English-speaking participants, so the suitability of these programs to other language, cultural, and ethnic backgrounds remains unknown. To make programs more culturally and linguistically relevant, researchers have adapted them in several ways. This study looked at how well programs for autistic children and adolescents have been adapted for various communities. Using the Cultural Adaptation Checklist (CAC), we examined 16 studies and found that the amount of adaptations varied widely. Only three studies mentioned using a framework that guided their adaptations. Our findings show that although all studies described some level of cultural adaptation, very few reported on ensuring stronger community involvement or making the programs more accessible for all. Using tools like the CAC can help researchers and clinicians make programs more inclusive and relevant for autistic individuals and their families worldwide.
Keywords
Social communication interventions support autistic individuals’ communication skills, social-emotional reciprocity, and ability to develop, maintain, and understand relationships (Watkins et al., 2017). Among studies that reported race and ethnicity data, intervention research has primarily relied on participants who are White and English-speaking (Horton & Munoz, 2021). A large systematic review conducted by Steinbrenner et al. (2022) revealed that out of 1,013 studies published between 1990 and 2017, only 25% reported participant race and ethnicity data. Among those studies that did report such data, White participants comprised 64.8% of the samples, followed by Hispanic/Latino (9.4%), Black (7.7%), and Asian (6.4%) participants, thus limiting the generalizability of findings to culturally and linguistically diverse groups. Lack of diversity in research populations, both within and outside Western countries, limits our understanding of autism interventions across different ethnocultural groups.
Social norms vary across and within cultures as they are intrinsically tied to the cultural values and practices of a community. Since there is no standard norm for appropriate social behaviors across cultures (American Speech-Language-Hearing Association [ASHA], n.d.), designing a universal approach for social communication interventions is not suitable for diverse communities. While delivering an intervention, it is considered part of both best and ethical practice to recognize and align with the client’s culture (Bernal et al., 2009). Culture is a multidimensional construct that can be defined as a “socially transmitted or socially constructed constellation consisting of such things as practices, competencies, ideas, schemas, symbols, values, norms, institutions, goals, constitutive rules, artifacts, and modifications of the physical environment” (Fiske, 2002, p. 85). The reciprocal relationship between culture and disability is understood by examining how societal norms, values, politics, and power dynamics shape the lived experience (such as disability) while simultaneously recognizing how disability restructures cultural understandings (Waldschmidt, 2017). Recent calls have emphasized shifting from “cultural competence” (which implies mastery of a specific culture, risks reinforcing stereotypes, and is challenged by intersectionality), toward “cultural humility,” which involves continuous self-reflection and an interpersonal and intrapersonal commitment to providing client-centered care (Lekas et al., 2020; Miller, 2009).
Cultural adaptation involves “the systematic modification of an evidence-based treatment or intervention protocol to consider language, culture, and context in such a way that it is compatible with the client’s cultural patterns, meanings, and values” (Bernal et al., 2009, p. 362). Cultural adaptation is necessary when there is an intervention-consumer mismatch. Evidence on whether culturally adapted interventions consistently outperform original versions is limited because it is not ethical to randomize minoritized participants to non-adapted conditions (Barrera et al., 2013). In such instances, researchers have often examined the differences in effect sizes between the original intervention and the adapted versions, which have resulted in mixed findings. For example, a recent meta-analysis by J. D. Lee, Kang et al. (2025) found that culturally adapted programs for autistic children generated comparable outcomes to those of the original interventions. In contrast, Zheng et al. (2021) reported larger effect sizes for the original intervention relative to their culturally adapted counterparts. However, studies have shown that culturally adapted programs achieve higher engagement and retention (Kumpfer et al., 2002). In addition, prior reviews have indicated that delivering programs using the child’s heritage language may yield slightly more favorable outcomes than when delivered in the mainstream language (see Cheatham et al., 2012; Lim et al., 2019). In addition to culturally adapting existing interventions, researchers have also created new culturally tailored programs specifically for target populations (e.g., Karanth et al., 2010; Rajesh & Venkatesh, 2019; Srinivasan et al., 2022).
Interventions should not be directly applied across cultures without considering the prevailing culture, socio-political environment, feasibility, and appropriateness. For example, if an evidence-based social communication intervention developed in Western countries is being delivered to children in Tamil Nadu (a state of South India), for whom Tamil is their local language, it is not sufficient to merely provide the intervention in Tamil. The goals, content, and implementation methods must be relevant to the Tamil-speaking children and families. For example, Indian culture typically follows a collectivistic, authoritarian, and adult-centered approach, in contrast to the individualistic approach common in Western cultures, which emphasizes individual autonomy (Chadda & Deb, 2013). In Indian culture, decisions for the child are predominantly made by the whole family, particularly the elders who are deeply respected for their beliefs and opinions due to their experience. According to Indian mothers, children learn language through direct, explicit, and adult-led methods rather than child-directed and indirect language facilitation approaches (Simmons & Johnston, 2007). In addition, it is a common local cultural belief in India that boys tend to speak later than girls (Leeuw et al., 2020). Therefore, the cultural and social fabric of the community needs to be considered (e.g., language used, stigma around disability, belief systems, and local practices) while providing services in different contexts (Hlayisi et al., 2024). In addition, researchers must also recognize the heterogeneity present within families in Tamil Nadu itself, including differences in socioeconomic levels, rural–urban contexts, regional and dialectal variations, and belief systems, which may require additional context-specific adaptations, to avoid creating stereotypes for a specific section of the population.
Multiple meta-analyses (e.g., Hall et al., 2016; J. D. Lee, Kang, et al., 2025; Li et al., 2023; Smith et al., 2011) have demonstrated positive outcomes for culturally adapted interventions. Fischer et al. (2024) identified 68 frameworks that have been used to guide cultural adaptations, which can be classified into two types (Baumann et al., 2015). The first type is content-oriented models that inform what aspects in the content and delivery of an intervention may require adaptations [e.g., Ecological Validity Model (Bernal et al., 1995); Cultural Sensitivity Model (Resnicow et al., 2000)]. They provide guidance on adapting domains such as language, content, goals, methods, and context to enhance cultural relevance for the target group. The second are process-oriented models, which focus on how the adaptation may be implemented [e.g., Heuristic Framework (Barrera & Castro, 2006); Selective and Directed Treatment Adaptation Framework (Lau, 2006)]. These models support decision-making, involving interest-holders and informally evaluating the adapted intervention.
The fidelity-adaptation dilemma has been debated by many researchers when evidence-based interventions are adapted and delivered to diverse ethnocultural groups (see Edmunds et al., 2022; J. D. Lee, Meadan, Kang, & Terol, 2023; Mejia et al., 2017; Miller, 2019; von Thiele Schwarz et al., 2019), and the evidence supporting either position remains inconclusive. Edmunds et al. (2022) describe that any intervention program consists of multiple components, with some being essential (core elements that are necessary for the intervention to work) and others being adaptable (i.e., peripheral elements that are recommended but not necessary). This distinction between these elements is important to ensure that modifications made improve the contextual fit without compromising the effectiveness of the intervention.
Preservation of the core components (i.e., fidelity-consistent) is usually recommended by implementation scientists since it improves internal validity. However, in specific situations, there might be a misalignment between the core element and the target population’s cultural values or practices, in which case, careful modifications of certain components (i.e., fidelity-inconsistent adaptations) may be warranted (J. D. Lee, Meadan, Kang, & Terol, 2023), which must be systematically documented and evaluated (Miller, 2019).
Although several comprehensive reviews have described elements that have been culturally adapted in social communication interventions (e.g., Albin et al., 2022; Cycyk et al., 2021; Davenport et al., 2018; DuBay, 2022), none have analyzed the quality of adaptations, possibly because there is no standardized tool available (Arora et al., 2021). It is important to examine the quality of cultural adaptations so that intervention developers can understand their impact on treatment outcomes and facilitate only necessary adaptations (Stirman et al., 2013). To address this issue, J. D. Lee, Meadan, Sands, et al. (2023) developed the Cultural Adaptation Checklist (CAC), grounded in the Ecological Validity Model. The CAC was developed both as a tool to guide researchers to culturally adapt interventions and also to systematically quantify the quality of cultural adaptations carried out in autism intervention research. In this review, we operationalize quality as the completeness and rigor of documented cultural adaptation activities captured by the CAC rubric, rather than the adequacy or effectiveness of the adaptations themselves.
To date, three studies have used the CAC to assess the extent of adaptations in interventions for autistic Black/African Americans and their families (Davis et al., 2025) and caregiver-mediated interventions for autistic children (Douglas et al., 2024; J. D. Lee, Meadan, et al., 2025). The former study was restricted to one ethnocultural group, and the latter two studies did not include interventions delivered by professionals. Therefore, the purpose of this review was to systematically appraise the quality of cultural adaptations incorporated into social communication interventions delivered by professionals for autistic children and adolescents up to the age of 18 years. We elected to use the CAC for this purpose, as it was specifically developed based on the autism literature. The CAC operationalizes quality by analyzing the extent to which specific adaptation indicators (32 in total) across seven dimensions during both the adaptation planning and intervention implementation phases are documented. This allows for quantifiable comparisons of adaptations across studies. Our research questions were:
Method
This systematic review follows the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines outlined by Page et al. (2021) (see Supplementary Material 1). The methodology was pre-registered on PROSPERO (ID: CRD42024531743) in April 2024, with deviations from the pre-registered protocol detailed in Supplementary Material 2. This review is inspired by the work of J. D. Lee, Meadan, et al. (2025).
Comprehensive searches were conducted in April 2024 across eight databases: ERIC, CINAHL, EMBASE, PsycINFO, MEDLINE, Scopus, Web of Science, and Nursing and Allied Health. An updated search was conducted before the final analysis in June 2024, along with handsearching of the reference lists of the included studies to add any new literature that fit the inclusion criteria. All searches were conducted and uploaded into Covidence (Covidence Systematic Review Software, 2024) for screening. Mesh terms were formulated based on four distinct domains pertaining to population, intervention, outcomes, and cultural adaptations. Full search strategies are provided in Supplementary Material 3.
An article was included if it (a) recruited individuals aged between 0 and 18 years who had a confirmed diagnosis of autism or suspected autism (with or without co-occurring conditions such as Attention-Deficit/Hyperactivity Disorder or language disorders/difficulties). We decided to include a broad age range (0–18 years) primarily because caregiver-mediated interventions were excluded (to avoid duplication of prior research), and our preliminary searches indicated the overall number of culturally adapted interventions was quite limited; (b) had a sample size where at least half of the participants were autistic or had suspected autism; (c) included a culturally adapted intervention or a tailored intervention that had at least one intervention outcome related to improving communication and/or social skills. We define culturally adapted interventions as those where the research team modified an existing intervention such that it aligns with the needs of a particular ethnocultural group, whereas culturally tailored interventions were those where the research team developed a novel intervention specifically for a particular group (J. D. Lee, Kang, et al., 2025); (d) explained the process involved in culturally adapting a social communication intervention even if no participants were recruited; (e) involved an intervention delivered primarily by professionals or trained non-specialists and/or was only assisted (not primarily delivered) by parents/caregivers; (f) employed an experimental (e.g., single-case design, multiple baseline design across subjects, randomized controlled trial, quasi-experimental group design), mixed methods, observational (e.g., cohort, cross-sectional), or descriptive design, and (g) was published in a peer-reviewed English journal between January 2000 and April 2024. Relevant literature reviews of culturally adapted interventions were examined to locate additional eligible studies. We excluded studies of interventions where caregivers acted as the primary facilitators to avoid duplicating recent appraisals of cultural adaptations for caregiver-mediated interventions by Douglas et al. (2024) and J. D. Lee, Meadan, et al. (2025).
Three reviewers were involved in the data extraction stage (Reviewer 1: first author, speech-language pathologist, and doctoral candidate, Reviewer 2: second author, graduate student in speech-language pathology, and Reviewer 3: third author, speech-language pathologist, and post-doctoral associate). Reviewers 2 and 3 were oriented by Reviewer 1 through an introductory meeting where the objective of the review and their specific roles and responsibilities were explained. Title and abstract screening were conducted by Reviewers 1 and 2 through Covidence software, followed by full-text reviews. Reviewers started with screening titles and abstracts for the first 20% of the total list to ensure an inter-rater reliability of ⩾90%. In instances of uncertainty about whether a specific title/abstract should be included, the reviewers employed an inclusive approach, and the final decision was taken during full-text reviews.
Reviewers 1 and 3 used QualSyst (Kmet et al., 2004) to provide a broad overview of methodological rigor of the included studies because it accommodates diverse study designs. Similar to other systematic reviews that used the QualSyst (e.g., Davenport et al., 2018; Lee et al., 2008; Liu et al., 2020; Tawankanjanachot et al., 2023), studies were classified based on their scores, with 80% or higher as strong, 70%–79% as good, 50%–69% as adequate, and below 50% as limited quality. We coded “No” when a specific criterion was applicable to the study design but not met, and “Not applicable” (N/A) when the criterion was not applicable to the study design. Items coded as N/A were excluded from the denominator while calculating the overall scores and were therefore not weighted the same as “No.” Consistent with QualSyst scoring guidelines, “Yes” was assigned a score of 2, “Partially Yes” a score of 1, and “No” a score of 0.
The CAC was used to assess the quality of cultural adaptations of the studies included. The CAC (see Supplementary Material 4) assesses cultural adaptation across two phases – adaptation (preparation and planning) and implementation (delivery) of the intervention. There are a total of 32 items categorized into seven dimensions: (a) Language (focuses on using culturally appropriate language and terminology), (b) Persons (emphasizes the involvement of all interest-holders), (c) Content (assesses the integration of the target populations’ cultural values), (d) Goals (determines the relevance of outcomes for all community interest-holders and participants), (e) Methods (assesses ways in which the intervention can be sustainable and accessible), (f) Context (focuses on how social constructs and environments are incorporated to enhance cultural sensitivity), and (g) Process (reflects on the iterative process of cultural adaptation and implementation). The CAC was paired with the rubric (J. D. Lee, Meadan, Sands, et al., 2023) to quantify the quality of cultural adaptation by coding whether researchers fulfilled each of the 32 adaptation activities as (a) Yes, (b) Partially yes, or (c) No (i.e., not reported or not applicable).
For example, the first item in the CAC pertains to the translation process, and increasing rigor and comprehensiveness in the adaptation process is reflected along a clear gradient: No evidence of translation (No); only forward translation by one person (Partially); and both backward and forward translation by a team of bilingual and bicultural people (Yes). Items that are “Not applicable” were excluded from scoring. A higher percentage of the overall score obtained on the CAC indicates that a greater number of quality indicators were addressed, and this reflects more rigor in the documented adaptations. However, the CAC does not have cut off scores to document what classifies as “adequate” or “inadequate” adaptations. Therefore, in this review, we interpret CAC scores as reflecting the extent to which quality indicators were documented in studies, rather than making claims about whether an adaptation was sufficient or not. In principle, a higher percentage reflects more comprehensively documented adherence to CAC indicators.
Reviewers 1 and 3 initially practiced coding using the CAC on three excluded papers to establish ⩾85% inter-rater reliability. After coding all included studies, the reviewers engaged in discussions to resolve any conflicts. Both reviewers used separate Excel workbooks to ensure masking while coding the CAC items. The final CAC scores reflect the percentage of items coded Yes or Partially yes, that is, any information in the article coded as full or partial adherence to the quality criteria of a given CAC item was considered as having satisfied that cultural adaptation activity (as per J. D. Lee, Meadan, et al., 2025). The mean percentage (and SD) of fulfilled CAC items was calculated for each study across the seven dimensions and two phases (adaptation and implementation), along with the overall percentage of fulfilled items across all dimensions. Narrative synthesis, supplemented with tables and figures, was adopted as the best method to provide a coherent summary of the extracted data to answer our research questions.
Results
Figure 1 shows the PRISMA flowchart of study selection. The searches across eight databases yielded 3,022 citations. Once duplicates were removed, 2,519 articles were screened, and 87 studies were assessed for full-text review. A total of 71 were excluded for various reasons (see Supplementary Material 5), and 16 articles met the inclusion criteria. Reviewers 1 and 2 screened 20% of the studies and achieved an inter-rater reliability of 97% before proceeding with the remaining studies. Cohen’s Kappa (κ) values were 0.54 (97.5% agreement) for title/abstract screening and 1.0 (100% agreement) for full-text review. The moderate Kappa value for screening was observed due to the high exclusion rate. Inter-rater reliability for extracting data to address the first two research questions was 91.3%.
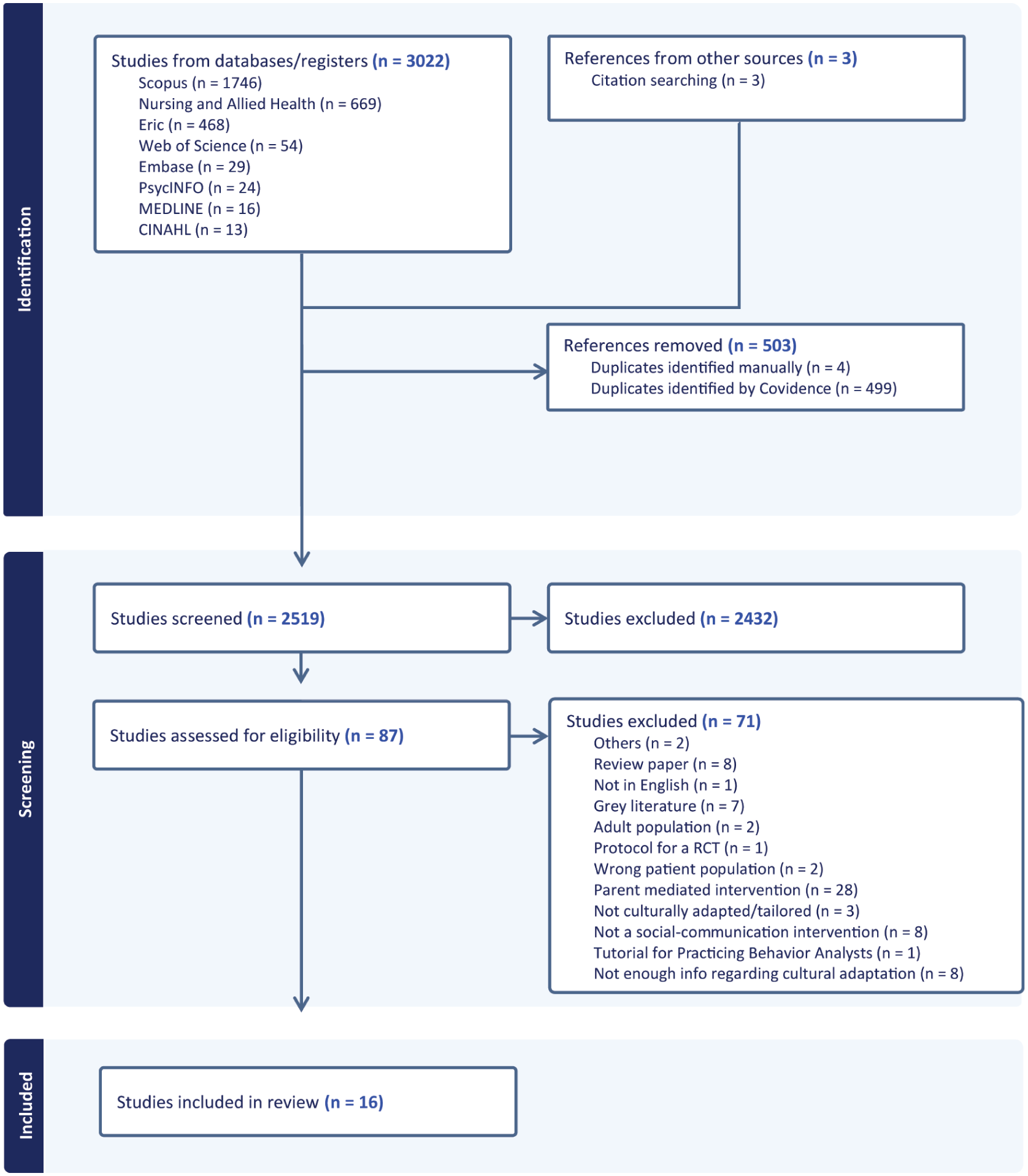
PRISMA diagram generated by Covidence.
Participant and Intervention Details (RQ1)
The 16 included studies consisted of a total of 474 participants ranging in age from 3.5 to 15.5 years, with 79.3% (n = 376) being male (see Supplementary Material 6). Among them, 457 were diagnosed with autism spectrum disorder (63 had co-occurring conditions), six had a diagnosis of social communication impairment, and 11 were non-autistic adolescents. Ethnicity was reported in five studies, and race in two. Study designs were all experimental, including single-case multiple baselines, pre- and post-intervention, quasi-experimental, and randomized controlled trials. All articles had QualSyst scores indicating at least adequate overall methodological quality. Ten studies were classified as strong, 3 as good, and 3 as adequate (see Table 1). Inter-rater reliability in assessing methodological quality was 90.2%.
Quality Assessment of the Included Studies Using QualSyst.
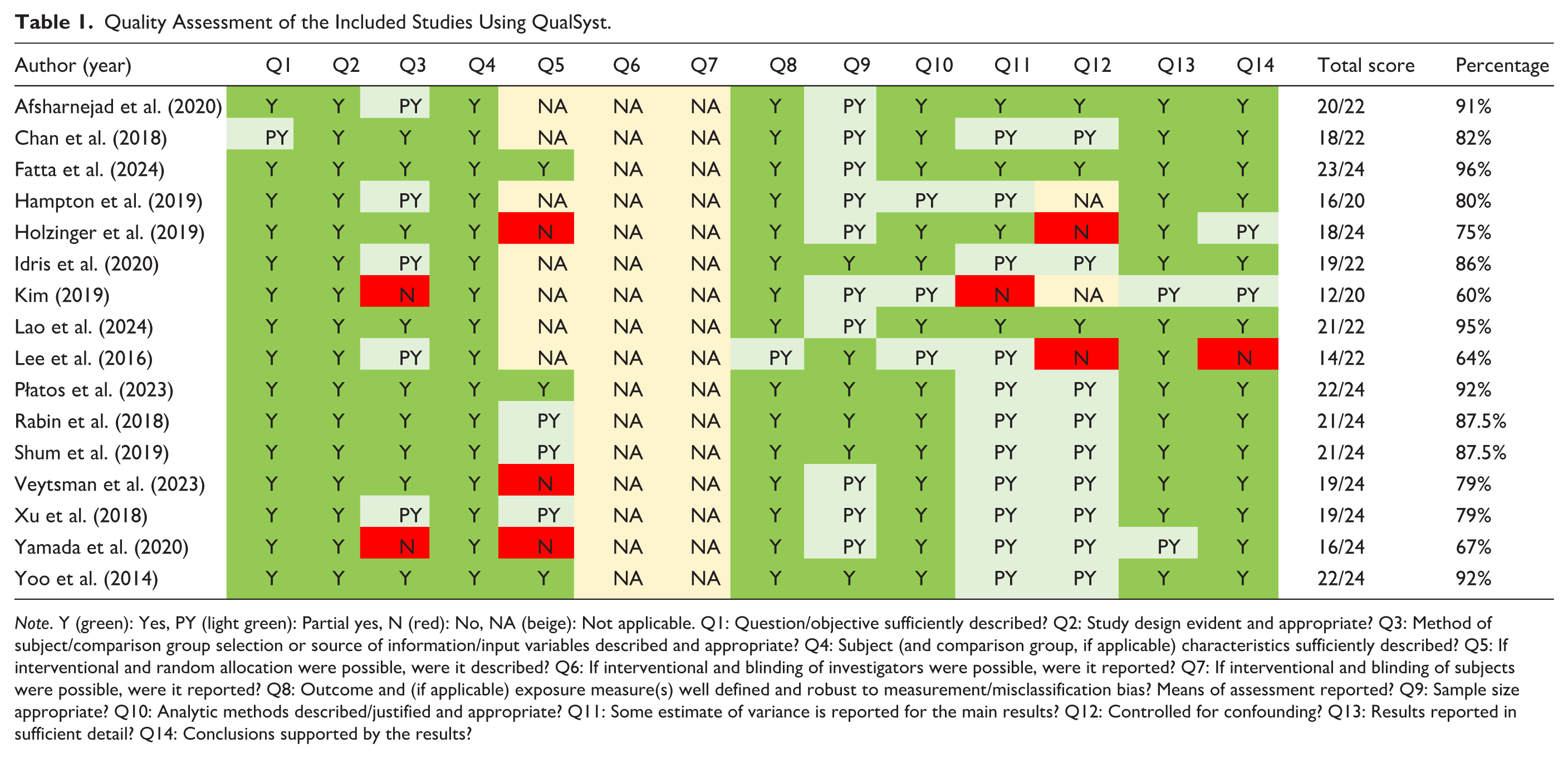
Note. Y (green): Yes, PY (light green): Partial yes, N (red): No, NA (beige): Not applicable. Q1: Question/objective sufficiently described? Q2: Study design evident and appropriate? Q3: Method of subject/comparison group selection or source of information/input variables described and appropriate? Q4: Subject (and comparison group, if applicable) characteristics sufficiently described? Q5: If interventional and random allocation were possible, were it described? Q6: If interventional and blinding of investigators were possible, were it reported? Q7: If interventional and blinding of subjects were possible, were it reported? Q8: Outcome and (if applicable) exposure measure(s) well defined and robust to measurement/misclassification bias? Means of assessment reported? Q9: Sample size appropriate? Q10: Analytic methods described/justified and appropriate? Q11: Some estimate of variance is reported for the main results? Q12: Controlled for confounding? Q13: Results reported in sufficient detail? Q14: Conclusions supported by the results?
The interventions delivered included the Early Start Denver Model (ESDM), peer-mediated Pivotal Response Training (PRT), Enhanced Milieu Teaching (EMT), Program for the Education and Enrichment of Relational Skills (PEERS), KONTAKT (German and Swedish for “contact,” no acronym), Cognitive Behavioral Therapy – Context-Based Social Competence Training for Autism Spectrum Disorder (CBT-CSCA), and Social Thinking (see Table 2). All interventions had evidence of their effectiveness in the country where they were developed: the United States (PEERS, EMT, PRT, ESDM, Social Thinking) and Germany (KONTAKT). The culturally adapted/tailored interventions were delivered across 12 countries in 11 languages in multiple settings including schools, community-based centers, the child’s home, mental health facilities, educational sites, clinical centers, and online. The duration of intervention ranged from 3 weeks (Kim, 2019) to 12 months (Holzinger et al., 2019), with intensity of sessions varying from 10 min (Kim, 2019) to 2 hr (Chan et al., 2018; Fatta et al., 2024). Frequency of sessions ranged from 5 times/week (Xu et al., 2018) to weekly (all the PEERS interventions). The interventions were delivered by therapists (speech-language pathologists, occupational therapists, psychotherapists, rehabilitationists), pediatricians, social workers, psychologists, counselors, psychiatrists, teachers, special educators, school inspectors, and trained peers.
Summary of the Culturally Adapted Social Communication Interventions.
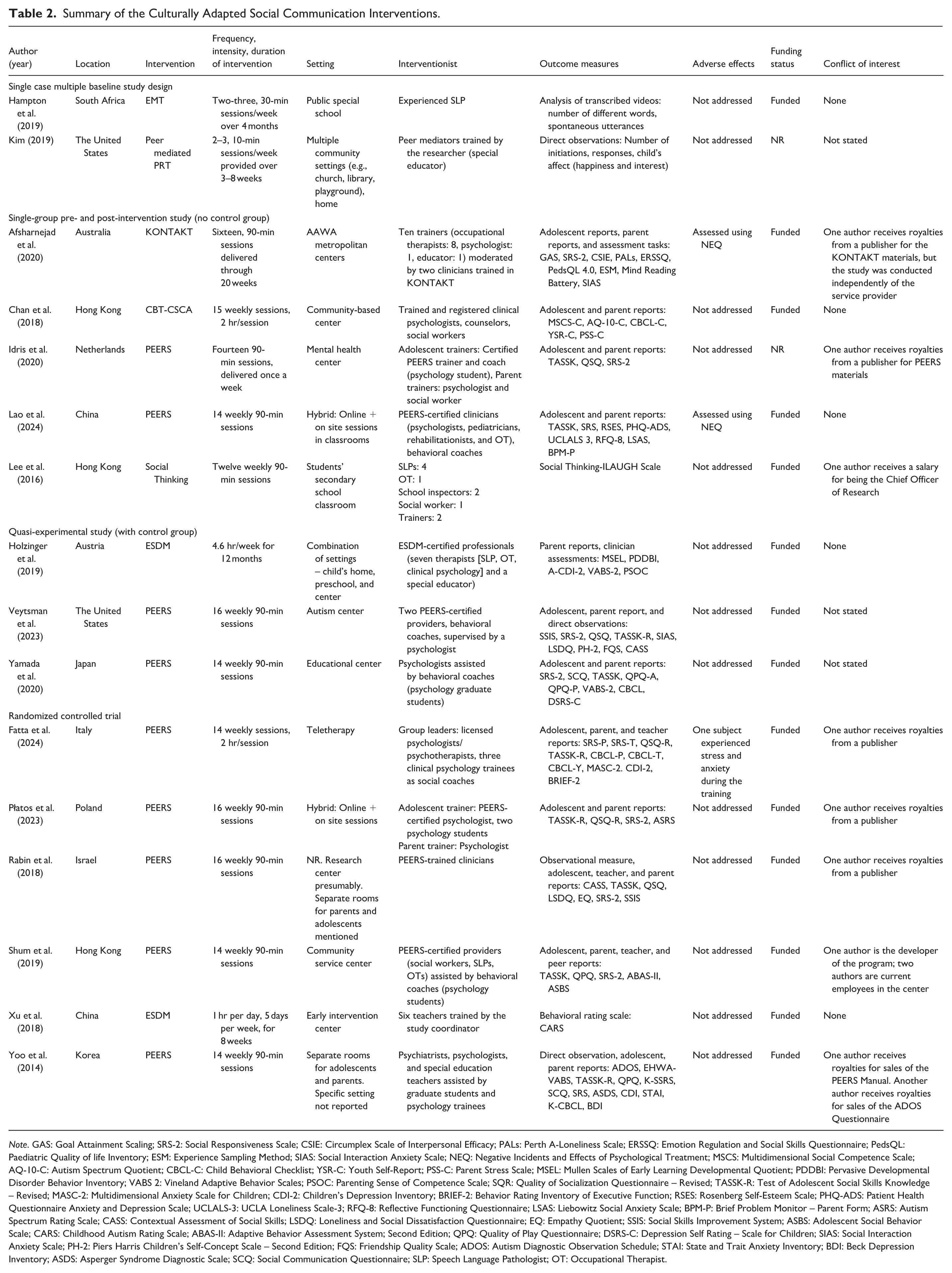
Note. GAS: Goal Attainment Scaling; SRS-2: Social Responsiveness Scale; CSIE: Circumplex Scale of Interpersonal Efficacy; PALs: Perth A-Loneliness Scale; ERSSQ: Emotion Regulation and Social Skills Questionnaire; PedsQL: Paediatric Quality of life Inventory; ESM: Experience Sampling Method; SIAS: Social Interaction Anxiety Scale; NEQ: Negative Incidents and Effects of Psychological Treatment; MSCS: Multidimensional Social Competence Scale; AQ-10-C: Autism Spectrum Quotient; CBCL-C: Child Behavioral Checklist; YSR-C: Youth Self-Report; PSS-C: Parent Stress Scale; MSEL: Mullen Scales of Early Learning Developmental Quotient; PDDBI: Pervasive Developmental Disorder Behavior Inventory; VABS 2: Vineland Adaptive Behavior Scales; PSOC: Parenting Sense of Competence Scale; SQR: Quality of Socialization Questionnaire – Revised; TASSK-R: Test of Adolescent Social Skills Knowledge – Revised; MASC-2: Multidimensional Anxiety Scale for Children; CDI-2: Children’s Depression Inventory; BRIEF-2: Behavior Rating Inventory of Executive Function; RSES: Rosenberg Self-Esteem Scale; PHQ-ADS: Patient Health Questionnaire Anxiety and Depression Scale; UCLALS-3: UCLA Loneliness Scale-3; RFQ-8: Reflective Functioning Questionnaire; LSAS: Liebowitz Social Anxiety Scale; BPM-P: Brief Problem Monitor – Parent Form; ASRS: Autism Spectrum Rating Scale; CASS: Contextual Assessment of Social Skills; LSDQ: Loneliness and Social Dissatisfaction Questionnaire; EQ: Empathy Quotient; SSIS: Social Skills Improvement System; ASBS: Adolescent Social Behavior Scale; CARS: Childhood Autism Rating Scale; ABAS-II: Adaptive Behavior Assessment System; Second Edition; QPQ: Quality of Play Questionnaire; DSRS-C: Depression Self Rating – Scale for Children; SIAS: Social Interaction Anxiety Scale; PH-2: Piers Harris Children’s Self-Concept Scale – Second Edition; FQS: Friendship Quality Scale; ADOS: Autism Diagnostic Observation Schedule; STAI: State and Trait Anxiety Inventory; BDI: Beck Depression Inventory; ASDS: Asperger Syndrome Diagnostic Scale; SCQ: Social Communication Questionnaire; SLP: Speech Language Pathologist; OT: Occupational Therapist.
Outcome measures included self-reports (e.g., Goal Attainment Scaling [GAS], Quality of Socialization Questionnaire [QSQ], Test of Adolescent Social Skills Knowledge [TASSK]); parent and teacher reports (e.g., Social Responsiveness Scale [SRS], Child Behavior Checklist [CBCL]); assessment tasks (e.g., Contextual Assessment of Social Skills [CASS]); scales (e.g., Childhood Autism Rating Scale [CARS]); analysis of transcribed videos; and direct clinician observations (e.g., number of initiations, responses, and child affect). Only three studies documented adverse outcomes experienced by the participants (Afsharnejad et al., 2020; Fatta et al., 2024; Lao et al., 2024). Afsharnejad et al. (2020) reported that 65% of the adolescents experienced at least one adverse effect such as anxiety and depression, feeling of hopelessness, and stigmatization. Most studies reported using culturally sound outcome measures, except for Rabin et al. (2018) and Veytsman et al. (2023). The culturally sound measures included a combination of culturally translated and/or validated measures (e.g., Chinese Version of the Multidimensional Social Competence Scale, Chan et al., 2018; SRS validated with the Italian population, Fatta et al., 2024; Polish adaptation of the Autism Spectrum Rating Scale, Płatos et al., 2023) as well as tools that were developed specifically for the study (e.g., Social Thinking – ILAUGH Scale [Initiation, Listening with eyes/brain, Abstract and inferential language, Understanding perspective, Gestalt processing, Humour and Human Relatedness], Lee et al., 2016).
Frameworks Employed (RQ2)
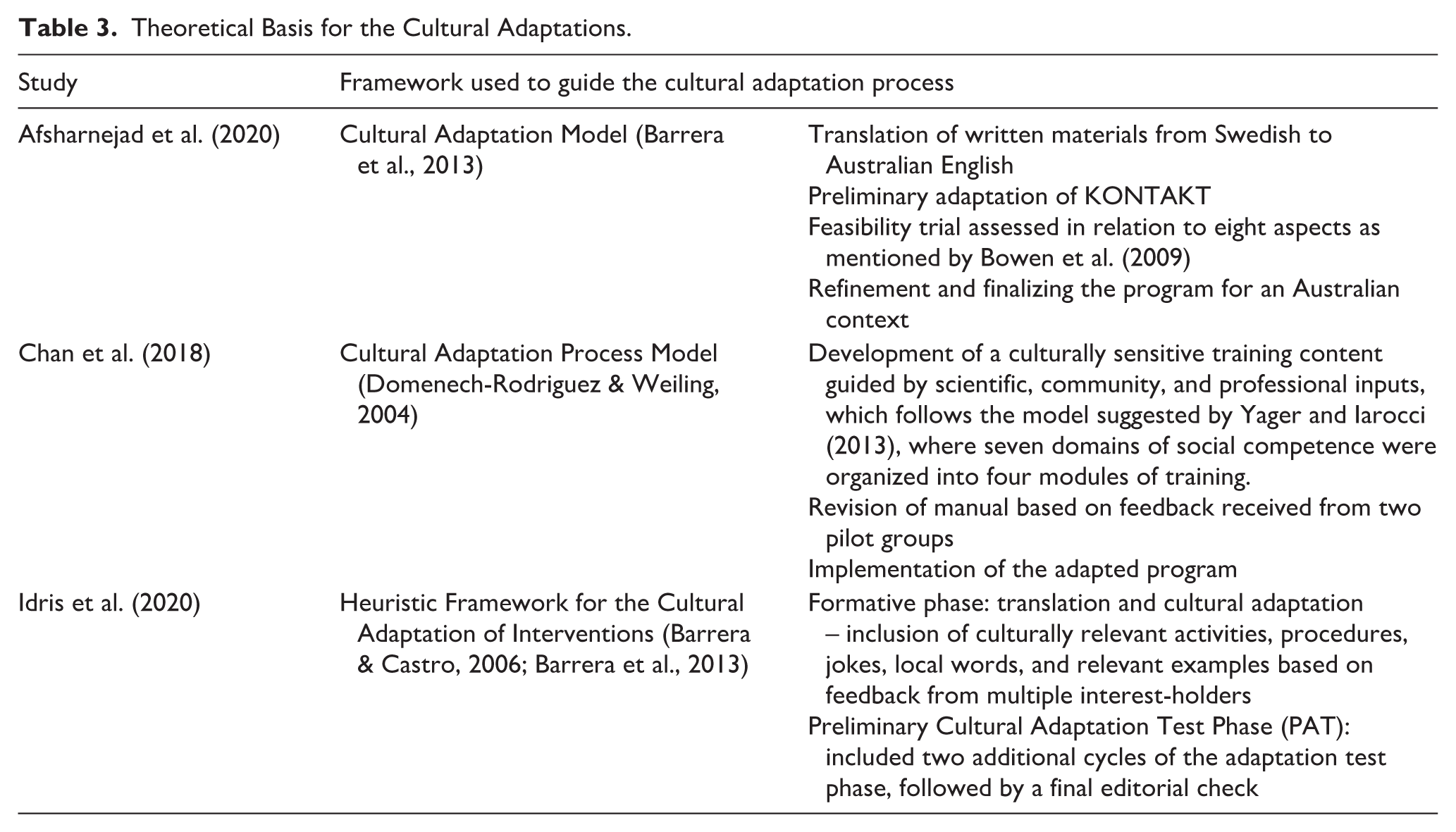
Three studies (Afsharnejad et al., 2020; Chan et al., 2018; Idris et al., 2020) used a framework or model to guide the cultural adaptation process (see Table 3). The other studies provided descriptive information about the methods employed in culturally adapting the intervention such as translation of materials, inclusion of culturally relevant activities, terms, and examples guided by community stakeholder involvement and professional inputs.
Theoretical Basis for the Cultural Adaptations.
Quality of Cultural Adaptations (RQ3)
Inter-rater reliability for the three practice articles coded by Reviewers 1 and 3 was 86.9%. To improve inter-rater reliability, Reviewer 1 consulted with the developer of the CAC to clarify specific items. Reviewers 1 and 3 achieved an inter-rater reliability of 91% for the included studies, with agreement ranging from 81.2% to 100%. The degree of cultural adaptations across the studies is presented in Table 4. The average percentage of reported items across all 16 studies was 66% (SD = 12.9), indicating that, on average, full or partial fulfillment of 21 out of 32 CAC items was documented by researchers. There was a wide percentage range of item fulfillment reported across the individual studies, from 44% to 91%. Except for two studies (Hampton et al., 2019; Veytsman et al., 2023), most studies reported use of 50% or more of the CAC items, with 14 studies documenting at least one item in each of the seven CAC dimensions.
Graphic Display of the Cultural Adaptation Checklist.
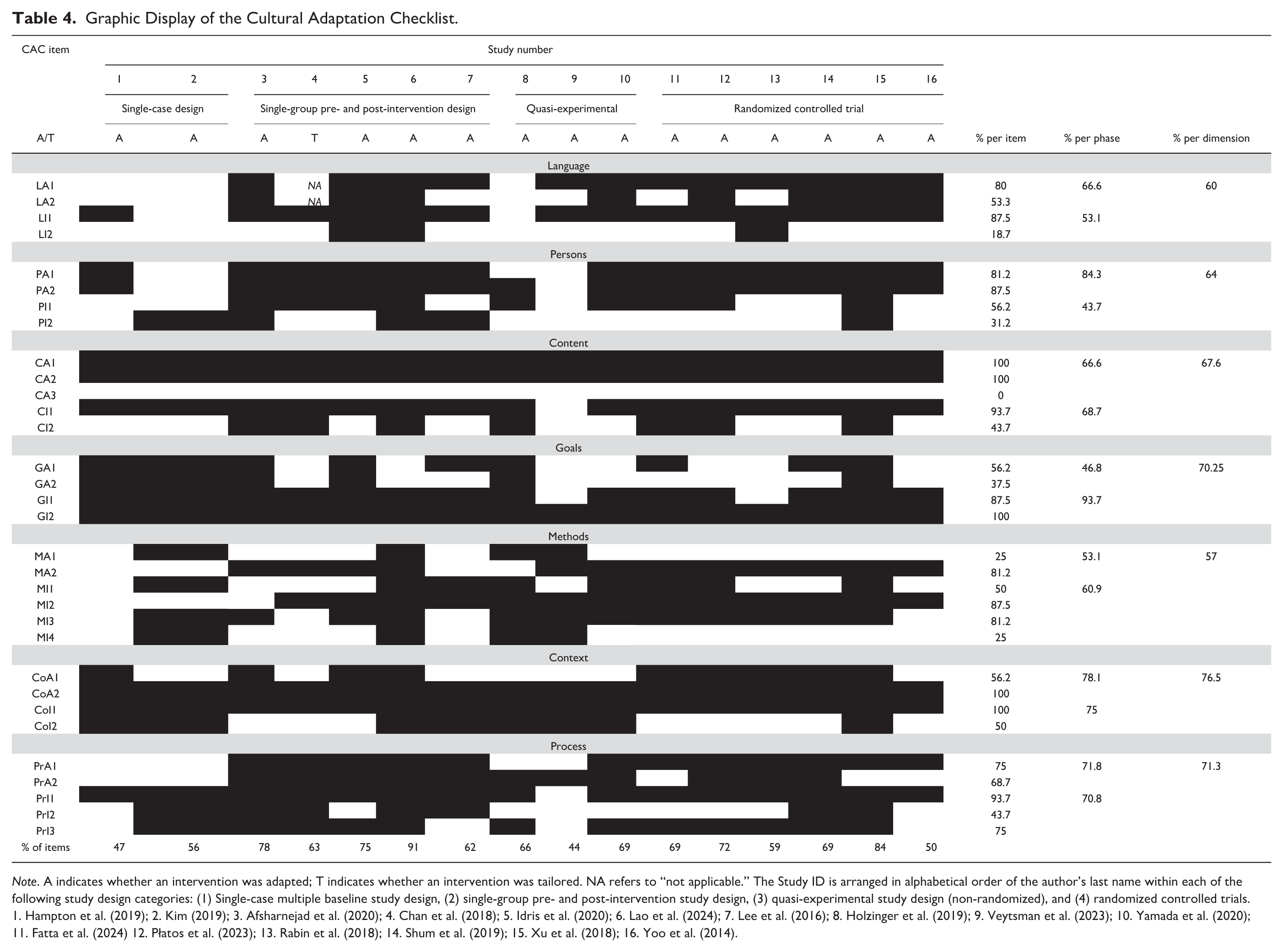
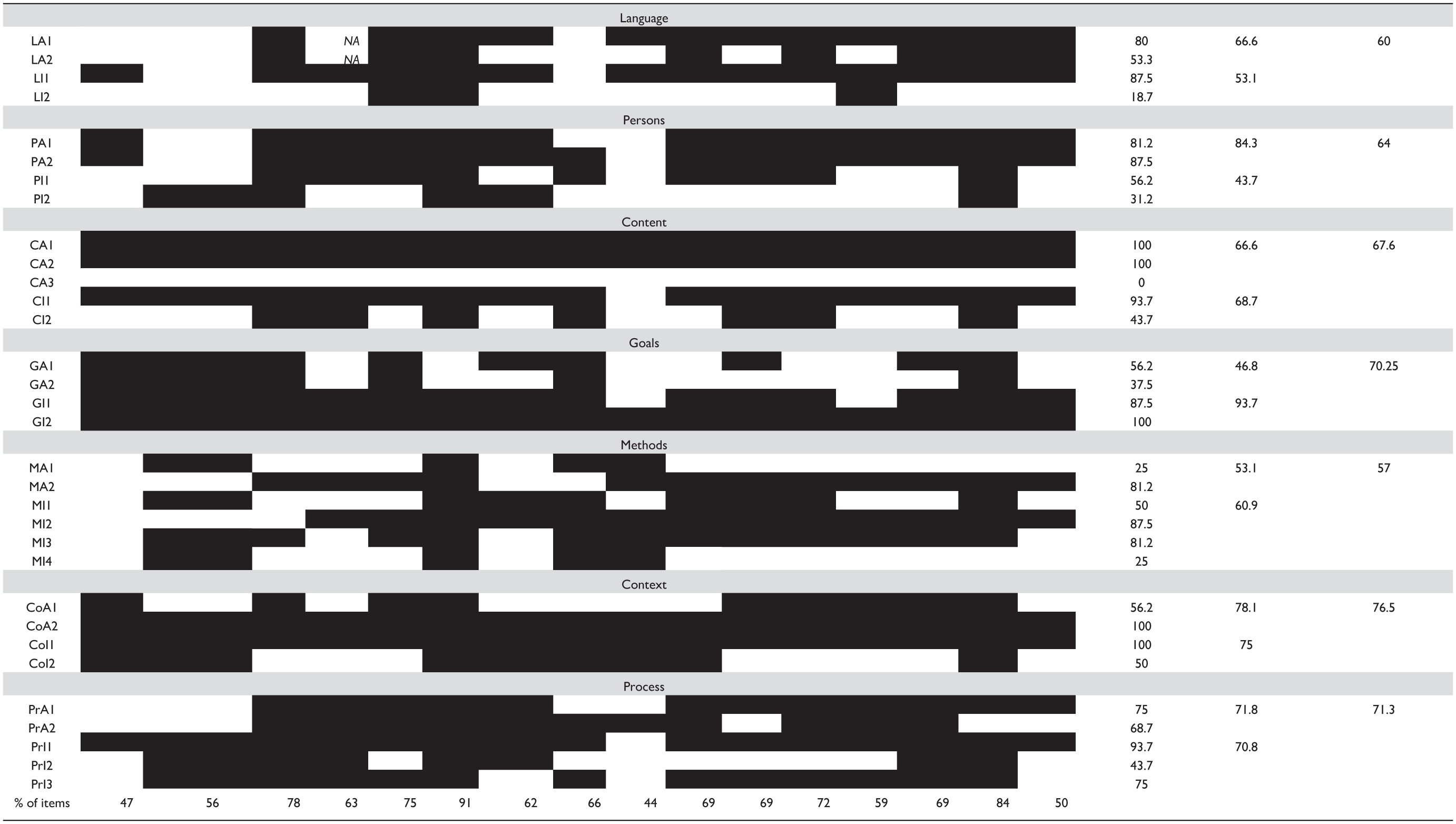
Note. A indicates whether an intervention was adapted; T indicates whether an intervention was tailored. NA refers to “not applicable.” The Study ID is arranged in alphabetical order of the author’s last name within each of the following study design categories: (1) Single-case multiple baseline study design, (2) single-group pre- and post-intervention study design, (3) quasi-experimental study design (non-randomized), and (4) randomized controlled trials. 1. Hampton et al. (2019); 2. Kim (2019); 3. Afsharnejad et al. (2020); 4. Chan et al. (2018); 5. Idris et al. (2020); 6. Lao et al. (2024); 7. Lee et al. (2016); 8. Holzinger et al. (2019); 9. Veytsman et al. (2023); 10. Yamada et al. (2020); 11. Fatta et al. (2024) 12. Płatos et al. (2023); 13. Rabin et al. (2018); 14. Shum et al. (2019); 15. Xu et al. (2018); 16. Yoo et al. (2014).
Five CAC items were satisfied by all 16 studies: Content Adaptation Planning Items #1 and #2, Goal Implementation #2, Context Adaptation #1, and Context Implementation #2. These items reflected the researchers’ efforts to ensure intervention content was culturally relevant (CA1) and related to the values, needs, and desired outcomes of the target population (CA2); assess the social validity of the goals and outcomes of the intervention (GI2); involve a research team that was knowledgeable of the target population’s culture (CoA2); and use an appropriate sociocultural environment for intervention delivery (CoI1), respectively. Fifteen of the 16 studies also satisfied Process Implementation Item #1 and Content Implementation #1, demonstrating the researchers’ efforts to learn about and individualize the intervention according to the participants’ needs (PrI1) and continually incorporate content of cultural significance to them throughout the intervention (CI1). We did not find evidence for any study having addressed Content Adaptation Item #3, which focuses on providing culturally accessible explanations for technical language (CA3). Three studies (Idris et al., 2020; Lao et al., 2024; Rabin et al., 2018) assessed the participant’s comprehension and acceptability of culturally adapted/translated terms during the intervention (Language Implementation Item #2, LI2).
The overall percentage of CAC items reported across the adaptation versus implementation phases was highly similar (66.7% and 66.5%, respectively), as was the range of scores for each (46.8–84.3% and 43.7–93.7%, respectively). There was some variation across the seven dimensions of the CAC, with the most commonly addressed dimension being Context (76.5% of studies) and the least reported Methods (57%). Researchers gave a similar level of attention to most dimensions across both adaptation and implementation phases with two notable exceptions. Most studies (93.7%) satisfied Goals items at the Implementation phase, which highlights use of culturally appropriate outcome measures and measuring the social validity of the goals and outcomes of the intervention during its delivery. However, less than half of the studies satisfied Goals items at the Adaptation phase, which emphasizes individualizing intervention goals with the target population. By contrast, 84.3% of the authors reported on completing Persons items in the Adaptation phase, whereas only 43.7% reported on Persons adaptations at Implementation, highlighting a potential gap in involving community interest-holders beyond the planning phase, that is, iteratively throughout program delivery to support ongoing consideration of recommendations and building trust. Figure 2 shows the percentage of studies reporting each CAC phase and dimension.
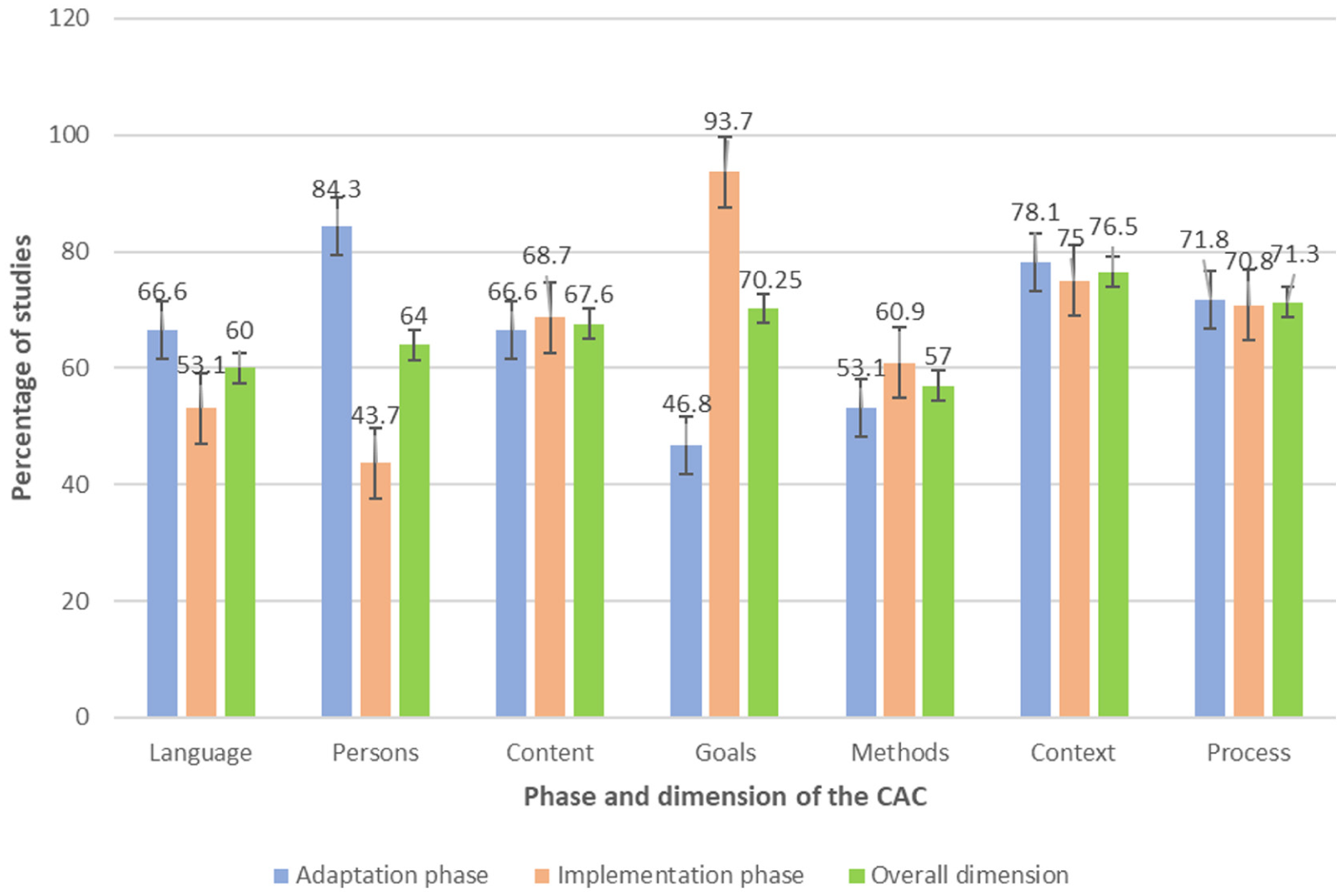
Percentage of studies reporting on each phase and overall dimension of the CAC.
Given that the PEERS intervention was culturally adapted across different geographical regions in nine of the included studies, we had the opportunity to conduct an exploratory analysis of how different cultural contexts might influence adaptations of the same intervention. The percentage of fulfilled CAC items varied widely from 44% in the United States (Veytsman et al., 2023) to 91% in China (Lao et al., 2024), indicating that despite the original intervention being the same (PEERS in this case), the degree of adaptations made was different for each cultural context (see Supplementary Material 7). The greatest extent of cultural adaptations was observed in East Asia (China, 91%) and Europe (the Netherlands, 75%). For example, when the PEERS intervention was delivered to Latinx adolescents in the United States (Veytsman et al., 2023), adaptations involved translating materials into Spanish and providing financial compensation. In China (Lao et al., 2024), adaptations were more extensive, involving translation of materials into Mandarin Chinese, a pilot study, culturally relevant role-play scenarios and scripts, extending parent-adolescent sessions, using culturally relevant assessment tools, and stakeholder involvement.
Discussion
This review identified seven social communication interventions for autistic children and adolescents that have been culturally adapted in 11 languages across 12 countries. One notable finding was incomplete documentation of the participants’ race and ethnicity, consistent with the findings of Steinbrenner et al. (2022), who found that only 25% of autism intervention studies reported these data. The first step toward improving transparency regarding participants’ demographics and cultural identities is to ensure that journals adopt guidelines requiring demographic reporting. The minimal use of cultural adaptation frameworks identified (n = 3) aligns with findings of Albin et al. (2022) and Cycyk et al. (2021) but contrasts with those of Arora et al. (2021). Arora et al. (2021) found that half (26/52) of mental health interventions utilized a cultural adaptation framework, possibly due to the public and mental health fields leading the way in developing cultural adaptation frameworks. In the current review, studies that used a framework reported a higher percentage of cultural adaptations (72%), compared to those that did not (64%). Utilizing frameworks may support more systematic planning and more transparent reporting of adaptation decisions; future work should test whether this translates into improved fit and outcomes. However, further research is needed to examine how the use of frameworks influences treatment outcomes (e.g., participant satisfaction and engagement, overall effectiveness).
Only three studies in this review reported adverse events, which aligns with findings of other recent studies. For example, Bottema-Beutel et al. (2021) identified that only 11 out of 150 studies in non-pharmacological autism interventions for young autistic children documented the adverse effects. In line with their recommendations, we encourage researchers to take active efforts in monitoring and reporting adverse effects to ensure families, clinicians, policymakers, and other interest-holders can weigh potential harms alongside potential benefits. This reporting could also be considered as an additional sub-item within the CAC to promote greater transparency in future adaptation research.
The results of our review reflect the cultural adaptations reported in professionally delivered social communication interventions. Had caregiver-mediated interventions been included, there may have been subtle variations in the way certain cultural adaptations were operationalized and reported (thus affecting the overall CAC scoring), given that such programs usually require the caregivers to integrate the learnt strategies into the child’s natural environment and daily routines. Nevertheless, our findings are broadly consistent with J. D. Lee, Meadan, et al. (2025), who observed similar trends in the quality of documented cultural adaptations within caregiver-mediated interventions.
One of the strengths of this review is that we moved beyond describing the included studies and coded each item, phase, and dimension of the CAC to ensure systematic assessment of the quality and extent of cultural adaptations. Through this approach, we identified high variability in cultural adaptation activities across the 16 studies, with authors having made on average 2/3 of the possible adaptations itemized in the CAC. Some authors made over 90% of the adaptations, while others made less than half. Why fewer adaptations were made in some studies is unclear. It is possible that researchers were unaware of some of the important considerations and possible adaptations to be made, or they deemed certain adaptations to be unnecessary for their target population. It is also possible that journal page limitations may have led authors to omit information about adaptation activities carried out.
The low percentage of items reported in the Methods dimensions (57%) aligns with the findings of J. D. Lee, Meadan, et al. (2025) for caregiver-mediated interventions. Together, these findings suggest that particular attention is needed on enhancing accessibility and sustainability of culturally adapted intervention in diverse ways, such as creating flyers/posters in multiple languages, providing transportation and financial assistance (e.g., in certain communities, gender roles influence access to transportation), providing the intervention based on the clients’ desired delivery mode and setting, having interpreters, and communicating with the clients in their preferred mode (e.g., in person, online, email, etc.). Our review also identified a need to ensure that trusting relationships are established and maintained with community interest-holders at every stage of cultural adaptation and implementation.
The key implication of our findings is the need to establish meaningful and sustained community engagement while adapting interventions for the autistic community. The CAC includes multiple items that emphasize reciprocal and ongoing community-academic collaborations throughout the phases of adaptation and implementation (including partnerships in translation and verification of materials, ensuring linguistic and cultural acceptability of terms, identifying contextually relevant goals, optimizing intervention delivery procedures, and ensuring an iterative revision process). Leveraging long-term, meaningful partnerships with communities and intended end-users will help address the research-to-practice gaps and build local capacity to support the development of culturally adapted interventions that align with target populations’ needs (J. D. Lee, Meadan, Kang, & Terol, 2023). Adopting a “nothing about us without us” approach is crucial in autism research (Hoekstra et al., 2018) to avoid perpetuating parachute research, a practice wherein researchers from high-resource settings collect data from low-resource settings without meaningfully collaborating or engaging with the local community interest-holders (Odeny & Bosurgi, 2022). This is of paramount significance in the context of social communication interventions, where social interaction, pragmatics, social understanding, and language processing are deeply embedded within one’s social identity and may vary with every culture.
We found a greater extent of cultural adaptations (66%) compared to J. D. Lee, Meadan, et al. (2025, 58%); however, we currently lack data to support nuanced interpretation of CAC item fulfillment levels, that is, to determine if an 8% higher average score suggests a “better” quality of cultural adaptation for interventions delivered by professionals compared to those mediated by caregivers. In other words, we are currently limited in our ability to assess what proportion constitutes poor versus adequate levels of adaptation or whether certain CAC items and dimensions might contribute greater weight toward the overall quality of cultural adaptation. Considering that some authors indeed achieved a high level of cultural adaptations (91%) and only one CAC item out of 32 was not fulfilled by any authors, it is clearly feasible to make these adaptations. As such, our results suggest a need for increased attention to the full range of cultural adaptations in future studies.
Nonetheless, it is equally important to determine the extent of cultural adaptations necessary for social communication interventions to achieve their desired outcomes, such as establishing CAC criterion cutoff scores or ranges through empirical studies, expert judgment, and consensus. Much like recent calls for identifying active ingredients of social communication interventions for autistic individuals (Frost et al., 2021; Gulsrud et al., 2016), an important next step may be to identify the active ingredients (i.e., core vs. supplementary elements) of cultural adaptation. Some researchers call for retaining the core components of the original intervention unless there is enough evidence to suggest otherwise (Card et al., 2011), suggesting that more adaptations are not necessarily better. However, in practice, researchers may consider modifying these active elements based on contextual considerations. For example, one study included in this review (Holzinger et al., 2019) culturally adapted the ESDM intervention to enhance contextual fit for the Austrian population by modifying a strategy that was an active ingredient of the original program. The usage of exaggerated affect (e.g., usage of animation, exaggerated facial expressions, and body language) is a key strategy taught to families in the ESDM program. However, Austrian clinicians and caregivers perceived this strategy as unnatural, and therefore, the researchers adapted this strategy to incorporate more culturally congruent and subtle forms of affect and body language.
In addition, Cycyk et al. (2021) recommend individualizing interventions to each individual, not only those individuals whose language, race, culture, and/or ethnicity align with the target population for whom the original intervention was designed, but also particularly for those whose culture differs, and thereby discouraging a “one size fits all” approach. More research in this domain will provide an enhanced understanding on the optimal level and type of adaptations required for an intervention to be effective and acceptable (Arora et al., 2021).
Future work might also consider that different levels of adaptation may be required based on acculturation and degree to which a target population’s culture differs from the population for whom the intervention was originally developed. Indeed, the variations in the quality of cultural adaptations of the nine PEERS interventions conducted in different geographical locations highlight the diverse requirements of the target population to ensure the contextual fit of the intervention. It may not be surprising that the least number of cultural adaptations (44%) were provided to Latinx participants in North America (Veytsman et al., 2023) because PEERS was developed in the United States. Other cultures made adaptations to social skill activities to fit within their local context. For example, in the activity of “having get togethers,” it is not culturally appropriate in some cultures to show guests their entire house as suggested in the original U.S. version of PEERS. Instead, these activities were modified to reflect local customs: in the Hebrew version (Rabin et al., 2018), guests are typically shown only the kitchen and bathroom, whereas in the Japanese version, it is customary to show only the living room and bathroom (Yamada et al., 2020). Another activity that differed across culture was “handling rumors and gossip.” In the U.S. version of PEERS, adolescents are taught to act “amazed” to show that nobody cares about the gossip/rumor, while the Dutch approach emphasized indifference, the Italian adaptation redirected with new gossip, and the Japanese version encouraged short verbal comebacks over non-verbal responses, all aligning with their respective cultural norms.
Limitations and Future Directions
The results of our review are subject to publication bias since only peer-reviewed journals published in English were included. Including gray literature or studies published in other languages might have yielded different scores. Expanding search strategies to include geographical locations, as done by Tawankanjanachot et al. (2023), who included a list of 47 countries in the search strategy, may allow for casting a wider net. As previously noted, adaptations may have been underreported due to journal word limits. This can be mitigated by making detailed reporting procedures mandatory and transparent (e.g., CAC item inventories in Supplementary Files). Future reviews might also communicate with authors to obtain unreported information, following approaches such as Douglas et al. (2024).
Although the CAC is comprehensive and actionable, clarity of items and scoring accuracy could be further developed. Furthermore, given that the CAC was recently developed, additional studies that utilize the CAC to evaluate the extent of cultural adaptations are warranted, alongside validation of the tool. Some areas of the rubric would benefit from clearer guidelines to ensure that items are not double-coded (e.g., the Partially yes items for PA1 and PA2 as well as PI2 and PrI2 are similar). This can become problematic, particularly when one adaptation satisfies multiple items, which risks an inflated score. For example, a single adaptation such as making the intervention hybrid due to the COVID-19 pandemic fulfills multiple items such as choosing a suitable environment (CoI1), ensuring accessibility (MI1), and understanding the political/social/economic situation of the target population (CoA1).
Conclusion
Our review highlighted a significant research gap in the availability of culturally adapted social communication interventions for the autistic community. The limited number of culturally adapted interventions identified (n = 16) appears to be disproportionate to the vast array of evidence-based social communication interventions available worldwide for autistic children and adolescents. This underscores the crucial need for culturally adapted approaches for autistic individuals from diverse ethnic backgrounds. In the interim, our review provides a quick summary for clinicians and families of the nature and extent of cultural adaptations made to date for interventions they may be planning to access or adapt. Our review also revealed a number of improvements needed to the cultural adaptation process. Although numerous frameworks have been developed to serve as a guide in the cultural adaptation process, their application has been limited in research on social communication interventions to date. Moreover, there is a need for further attention to the full range of cultural adaptions in future research; the CAC and its rubric will be of great value in this regard. Future work expanding the scope and quality of culturally adapted interventions will enhance accessibility, relevance, and effectiveness, ultimately promoting better outcomes and quality of life for autistic individuals worldwide. In conclusion, engaging with local communities (which may involve local clinicians, researchers, families, and other interest-holders) will shape the way interventions are co-designed, adapted, delivered, evaluated, and made sustainable within the communities they intend to serve.
Supplemental Material
sj-docx-1-aut-10.1177_13623613261455374 – Supplemental material for Extent and Rigor of Cultural Adaptations in Social Communication Interventions for Autistic Children and Adolescents: A Systematic Review
Supplemental material, sj-docx-1-aut-10.1177_13623613261455374 for Extent and Rigor of Cultural Adaptations in Social Communication Interventions for Autistic Children and Adolescents: A Systematic Review by Vipula Rajesh Kumar, Aditi Iyer, Theresa Pham, Marie Y. Savundranayagam, Sheila T. Moodie and Janis Oram in Autism
Footnotes
ORCID iDs
Ethical Considerations
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article and/or its supplementary materials. Additional data may be obtained from the corresponding author upon request.
Pre-registration
This study was pre-registered on PROSPERO (CRD42024531743).
Informed Consent Statements
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.