
Abstract
Pediatric primary care practitioners (PCPs) are not typically trained to conduct autism assessments, contributing to delayed autism diagnosis in the United States. From February to September 2024, PCPs in Portland, Oregon, were trained to conduct standardized autism assessments with young children, based on similar U.S.-based training models. This training consisted of an asynchronous online autism course sponsored by the American Academy of Pediatrics; a 2-day, in-person workshop on diagnostic assessment; and eight posttraining community learning sessions. Twenty-four PCPs were trained to conduct autism assessments with children using the Modified Checklist for Autism in Toddlers, the Screening Tool for Autism in Toddlers and Young Children, and a parent interview based on the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5). A pilot trial of this program was conducted to examine its feasibility, acceptability, and initial outcomes related to self-reported PCP autism assessment knowledge and self-efficacy, as well as the number and characteristics of patients assessed. The program demonstrated high feasibility and acceptability. PCPs showed statistically significant improvement in their autism assessment knowledge and self-efficacy and used the assessment tools with 34 children ages 19–47 months during the study period. Similar training programs may help address PCP shortages and capacity contributing to diagnostic delays.
Lay Abstract
In Oregon and other places across the United States, parents often face long wait times to get their children evaluated for autism. Getting an autism diagnosis before age 3 can help children and their families to get the services and supports they need to thrive. Families might have shorter wait times if pediatric primary care practitioners (PCPs) were trained to do autism assessments. Programs nationwide have been developed and used to train PCPs to conduct autism assessments for these reasons. Twenty-four PCPs in the Portland, Oregon, metropolitan area were trained to conduct autism assessments with young children in 2024. The training asked PCPs to participate in an online autism course; a 2-day, in-person workshop on autism assessment; and eight community learning sessions. We studied this training to understand (a) how practical it was to implement this training, (b) whether PCPs’ self-reported knowledge and confidence about autism assessment changed, and (c) the number and characteristics of children who received autism assessments after the PCPs were trained. We collected data from the PCPs three times, including before training started, after the in-person workshop, and after the community learning sessions. We found that PCPs generally rated their participation and training experience positively. We also found that PCPs’ knowledge and confidence increased. They evaluated 34 children across diverse groups for autism. Similar training programs may help to address shortages of PCPs who are qualified to conduct autism assessments and increase access to early autism evaluation.
Keywords
In the United States, autism spectrum disorder (hereafter autism) diagnosis before the age of 3 years is associated with increased access to services and supports that can optimize health in the critical early childhood period and beyond (Gabbay-Dizdar et al., 2022; Zwaigenbaum et al., 2015). Yet, delayed autism diagnosis persists, with the median diagnostic age in U.S. children estimated at 3.9 years (47 months; Shaw, 2025). Delayed diagnosis has been attributed to myriad factors at the child, family, practitioner, community, and systems levels (Carbone et al., 2020; Daniels & Mandell, 2014; van ’t Hof et al., 2021). For example, children referred for an autism assessment in Oregon and other states often face wait times of more than one year due to a shortage of professionals trained to conduct these assessments (McBain et al., 2020). Pediatric primary care practitioners (PCPs), who see young children relatively frequently for well and sick visits, may be able to contribute to early autism identification. Yet, they often lack the requisite training to conduct autism assessments (Clarke & Fung, 2022).
An increasing number of U.S.-based PCP training initiatives have aimed to overcome these barriers over the past two decades (Bellesheim et al., 2020; Dreiling et al., 2022; Gerdts et al., 2025; Mazurek et al., 2017, 2019; McNally Keehn et al., 2020, 2023; Sohl et al., 2023; Swanson et al., 2014; Warren et al., 2011). Primary care autism diagnostic evaluation models can shorten the interval from referral to evaluation, retain high diagnostic accuracy compared to specialists, and maintain high levels of parental satisfaction (McNally Keehn et al., 2023; Nasir et al., 2024; Penner et al., 2023; Schieltz et al., 2023; Sohl et al., 2023). Building from this collective work to increase early autism identification through system-level primary care autism assessment models, we launched a PCP autism assessment training program in the Portland, Oregon, metropolitan area during 2024. This study aimed to (a) determine the PCP training program’s feasibility and acceptability, (b) examine changes in PCP perceived autism assessment-related knowledge and confidence, and (c) describe the characteristics and number of children who received autism assessment by participating PCPs.
Method
Positionality Statement
The research team members have complementary, interdisciplinary backgrounds in general pediatric medicine, psychology, and public health. They are comprised of differing racial and ethnic backgrounds (white or Latine), genders, and disability statuses. Several authors work extensively through clinical practice and/or participatory research with autistic children, youth, and adults, as well as caregivers and other family members of autistic individuals. The research team collectively used their training and expertise to help shape and guide this study.
Recruitment and Participants
PCPs in the Portland, Oregon, metropolitan area were recruited with flyers distributed through local healthcare systems and practitioner networks in February and March 2024. Nurse practitioners, physician assistants, and physicians with 2 or more years of clinical childhood experience as PCPs were included. PCPs had not conducted autism diagnostic evaluations before enrollment, though they may have implemented standard autism screening practices. Twenty-five PCPs were enrolled, with one withdrawing prior to the start of the in-person training, resulting in 24 participants completing baseline data collection. A majority were physicians (71%), between 35 and 44 years of age (33%), female (83%), white (79%), and lived in English-speaking households (85%). PCPs had an average of 13 years of practice and represented clinics in three counties (all PCP characteristics are shown in the supplemental material). PCPs were asked to estimate their panel size of children under the age of 5 years, for which 20 PCPs reported an average of 412 patients.
Measures
Feasibility
Study personnel tracked PCP completion of each training program component and data collection activity.
Participant Demographics, Training Acceptability, Knowledge, and Self-Efficacy
Data on PCP demographic characteristics, training experience (acceptability), and knowledge and self-efficacy related to autism assessment (initial outcomes) were collected as part of three surveys. These measures included the following:
Demographic characteristics (baseline survey): Participant race and ethnicity, gender, and sexual orientation were assessed with the Race Ethnicity Language Disability (REALD) and Sexual Orientation Gender Identity (SOGI) initiative measures (Oregon Health Authority, n.d.). Information on participant age, household language(s), county of practice, and PCP type was also gathered.
Training acceptability (first and second follow-up surveys): Three items rated on a 5-point Likert-type scale (1 = strongly disagree, 5 = strongly agree) were developed by the study team: “Participation in this training improved my knowledge and ability to care for children with developmental disabilities including autism”; “I feel I learned best practices for parents/caregivers with children with developmental disabilities including autism through participation in this training”; and “If a case vignette was presented it increased my knowledge about the topic”.
Autism knowledge (all surveys): Two items rated on a 4-point Likert-type scale (1 = not at all, 4 = very) from previous studies were included: (a) “How knowledgeable are you about ASD?”; and (b) “Generally, how knowledgeable are most pediatric PCPs about ASD?” (Zuckerman et al., 2013).
Autism assessment self-efficacy (all surveys): 36 items rated on a 6-point Likert-type scale (1 = no confidence, 6 = very confident) were adapted from the Primary Care Autism Self-Efficacy (PCASE) questionnaire to assess PCP confidence across the following six domains: (a) screening and identification, (b) assessment, (c) referral, (d) testing, (e) psychiatric management, and (f) additional areas (Mazurek et al., 2017). Relevant assessment and testing items were added (e.g., genetic and auditory testing), while items about the assessment and treatment of medical comorbidities were removed. The adapted PCASE demonstrated high internal consistency reliability at baseline in this study (α ⩾ .80 for the total scale and each subscale; supplemental material).
Practitioner Autism Assessment Activity and Patient Characteristics
Children ages 18–47 months were eligible to be evaluated. De-identified patient data were provided by PCPs on the (a) number of children they assessed using the tools they were trained on (see Procedure below); (b) assessment dates; and (c) age, biological sex, race and ethnicity, and language of the children assessed.
Procedure
Participants completed a sequential training program adapted from similar training programs (McNally Keehn et al., 2020, 2023; Sohl et al., 2023; Swanson et al., 2014) and with guidance from the larger project’s steering committee as well as developers of those prior programs. The training consisted of the following components: (a) an asynchronous online autism course (“Autism Identification and Collaborative Care”; Pedialink, 2024) that included autism characteristics, surveillance, and screening, including the Modified Checklist for Autism in Toddlers (M-CHAT; Robins et al., 2009); (b) two 1-day, in-person workshops that included additional information on autism services, training on the Screening Tool for Autism in Toddlers and Young Children (STAT; Stone et al., 2000) and parent interview methods based on the Diagnostic and Statistical Manual of Mental Disorders (5th ed., DSM-5; American Psychiatric Association, 2013) diagnostic criteria; (c) the requirement of obtaining an STAT training certification (Vanderbilt Kennedy Center & VU e-Innovations, 2026) by July 1, 2024; and (d) eight community of practice learning sessions using the Extension for Community Healthcare Outcomes (ECHO) model (Mazurek et al., 2017), which consisted of didactics on autism topics to deepen clinician knowledge, as well as case presentations and technical support for implementation. Case forms were provided to guide case presentations, although they were not required. PCPs were trained to assign one of the following three determinations in autism assessments: autism diagnosis, no autism diagnosis, or a deferred/undetermined diagnosis.
Participants completed three electronic, self-administered surveys at baseline (February–March 2024), post-in-person workshop (first follow-up; April 2024), and post-learning community (second follow-up; September 2024). De-identified patient data were reported by PCPs at two timepoints: following STAT certification (July 2024) and following the community learning sessions (September 2024). Data on diagnostic determinations were not collected. PCPs received a US $2,500 stipend for completing the program’s training and data collection activities. The Institutional Review Board at the senior author’s institution determined this was not human subjects’ research. Anonymized survey data and codebooks are available upon request from the corresponding author.
Analysis
Descriptive statistics (frequencies, relative frequencies, means, standard deviations) were computed to characterize the PCP sample and patients assessed. Based on skewness and kurtosis of the training acceptability, knowledge, and self-efficacy variables’ distributions, parametric tests including paired t-tests were used to examine change between baseline and the first or second follow-up. Effect sizes were computed using Cohen’s d. To examine differences in the characteristics of patients assessed by PCPs between July and September 2024, Fisher’s exact tests were performed for biological sex, race-ethnicity, and language. A Mann–Whitney U test was used to examine differences in patient age, although four participants were missing age data at Time 2, resulting in analytic samples of 14 at Time 1 and 16 at Time 2. Statistical significance was defined as p < .05. Due to small sample sizes for the patient data, race-ethnicity was examined as white versus all other racial-ethnic groups (Hispanic/Latino, Black, Native Hawaiian/Pacific Islander, American Indian/Alaska Native, Middle Eastern or North African, Asian, or Multiracial). PCP survey data were analyzed in SPSS 29.0. Patient data were analyzed in R V 4.5.1.
Results
Feasibility Results
PCP participation was high throughout the pilot trial. Twenty-four of the 25 PCPs (96%) who initially enrolled completed the PediaLink training and attended both days of the in-person workshop. Twenty-three PCPs (92%) achieved STAT certification. Over the eight ECHO sessions, 18 to 22 PCPs participated (M = 20). On average, PCPs completed 11 of the 12 total training program activities. Regarding PCP survey participation, 24 were assessed at baseline, 23 at first follow-up, and 21 at second follow-up. A total of 16 PCPs submitted data on patients assessed (seven PCPs at time 1 in July 2024, and 14 PCPs at time 2 in September 2024).
PCP Training Acceptability, Knowledge, and Self-Efficacy Results
Training acceptability ratings remained stable and favorable (agree to strongly agree) between the first and second follow-ups (Table 1). PCPs showed a statistically significant increase in beliefs about their own autism knowledge between baseline (M = 3.54, SD = 0.51) and both the first (M = 3.91, SD = 0.29, p = .001) and second (M = 3.86, SD = 0.36, p = .005) follow-ups. There was no statistically significant change in how knowledgeable PCPs believed other PCPs are about autism. From baseline to first follow-up, total PCASE scores and all but one of its subscales (psychiatric management) significantly improved (p < .05) with medium to large effect sizes. From baseline to the second follow-up, total and all PCASE subscale scores increased significantly (p < .001) with medium to large effect sizes (Figure 1; item-level results available in the supplemental material).
Primary Care Practitioner Training Program Acceptability and Autism Knowledge Results.
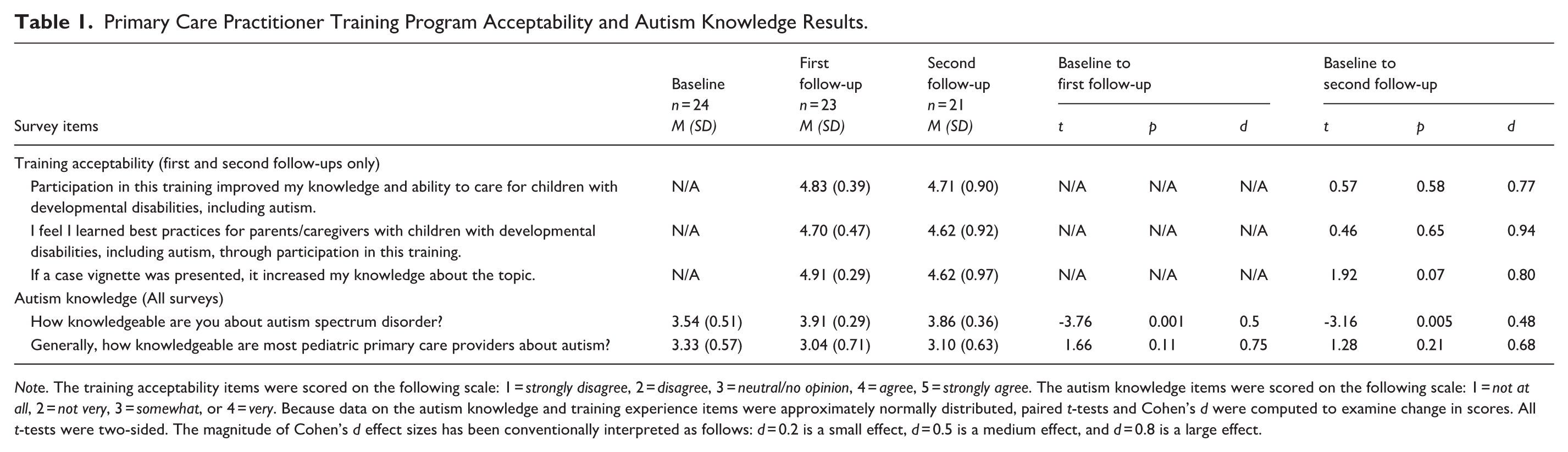
Note. The training acceptability items were scored on the following scale: 1 = strongly disagree, 2 = disagree, 3 = neutral/no opinion, 4 = agree, 5 = strongly agree. The autism knowledge items were scored on the following scale: 1 = not at all, 2 = not very, 3 = somewhat, or 4 = very. Because data on the autism knowledge and training experience items were approximately normally distributed, paired t-tests and Cohen’s d were computed to examine change in scores. All t-tests were two-sided. The magnitude of Cohen’s d effect sizes has been conventionally interpreted as follows: d = 0.2 is a small effect, d = 0.5 is a medium effect, and d = 0.8 is a large effect.
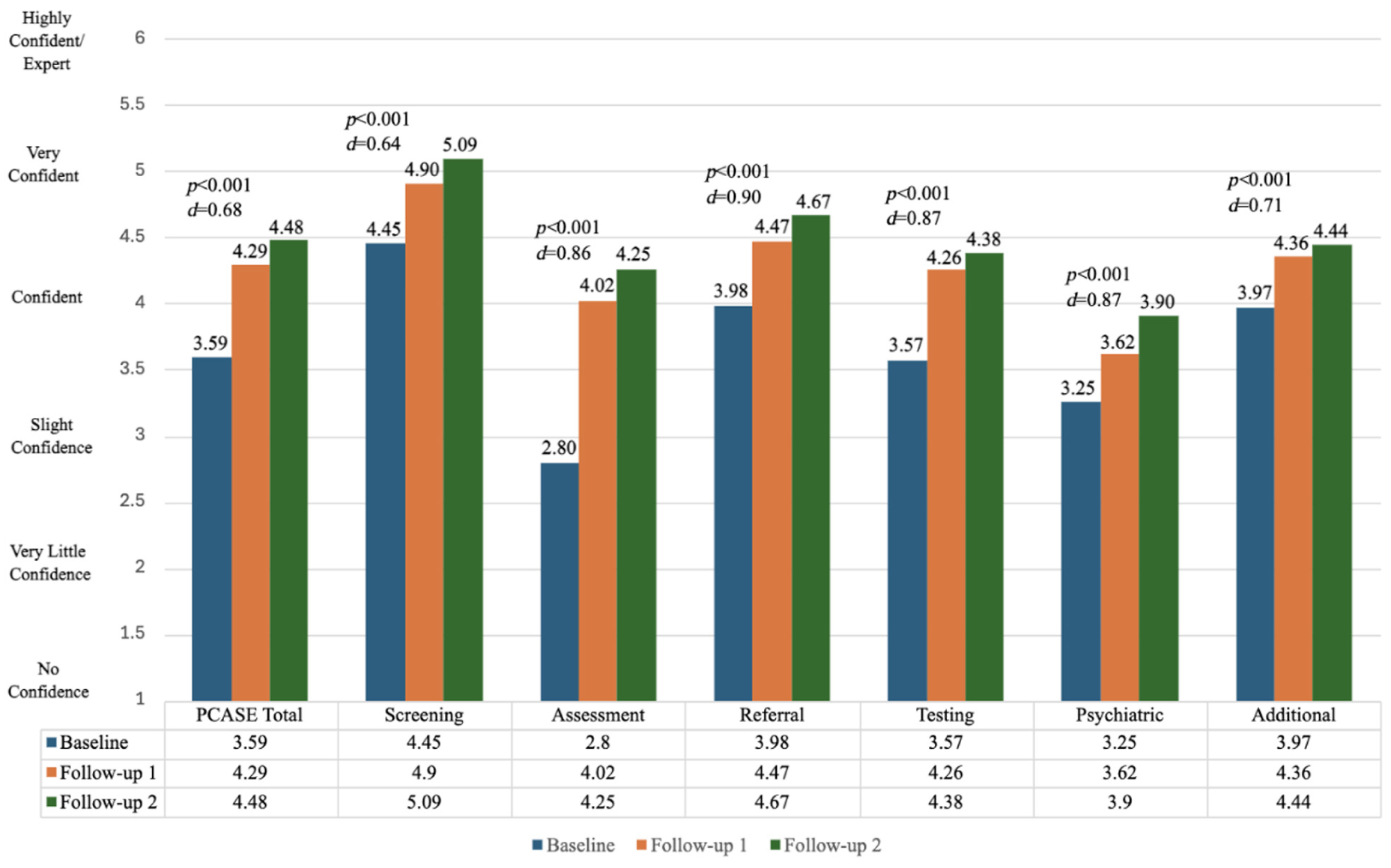
Adapted PCASE survey results at baseline, first and second follow-ups.
PCP Autism Assessment Activity and Patient Characteristics
Thirty-four patients were assessed (14 by July 2024 and 20 additional by September 2024) using the M-CHAT (n = 26), STAT (n = 26), and/or DSM-5 interview (n = 31). A total of 16 PCPs conducted these assessments, with seven who conducted their first assessment by July 2024 and nine who conducted their first assessment between July and September 2024. All patients who did not receive the M-CHAT or the STAT had already been identified as having a strong likelihood of autism or were referred to an autism evaluation at a previous visit in which screening was presumably completed. The patients assessed averaged 30.9 months of age (range: 19–47 months), were mostly white (n = 21, 61.7%) or Hispanic/Latino (n = 11, 32.3%), male (n = 23, 67.6%), and spoke English (n = 31, 91.2%). While no significant differences were found in comparisons of age (p = .10), sex (p = 1.00), or race-ethnicity (p = .34) from July 2024 (time 1) to September 2024 (time 2), the number of non-white patients assessed increased between those assessment dates (n = 6 to n = 14). No language comparison was made because there were no Spanish speakers in July. Descriptive patient characteristics are shown in the supplemental material.
Discussion
Autism assessment training programs for PCPs are burgeoning in the United States, given the need to address persistent autism diagnostic delays and improve timely service access. This training program was adapted from past PCP training program models, such as ECHO Autism STAT (Mazurek et al., 2019). Compelling features of this program include the training on the DSM-5 interview for autism and the collection of patient-level demographic data (Mazurek et al., 2019; Sohl et al., 2023). Conversely, limitations may include a lack of long-term follow-up with PCPs on their perceptions of practice changes, patient relationships, and community impact. The program demonstrated implementation effectiveness in terms of feasibility and acceptability for participating PCPs, as well as a modest penetration rate (i.e., 34 patients assessed during the relatively short pilot study period). Low-implementation costs, perceived appropriateness, and adoption of autism assessment by the participating PCPs within their respective practices further supported this program’s implementation (Proctor et al., 2011). PCPs demonstrated significant gains in autism assessment knowledge and confidence, and evaluated 34 children for autism in the three to five months following the in-person training. Assessments provided by the PCPs trained in this pilot were reimbursable, consistent with Oregon statutes and public and private insurance expectations (Individual Eligibility for Applied Behavioral Analysis Treatment, 2015; Oregon State Legislature, 2013), and served as the foundation for children accessing other services (e.g., Applied Behavior Analysis). Findings reinforce that PCP training programs can help increase access to autism assessments for young children (Clarke & Fung, 2022).
This pilot trial had key limitations. Self-reported measures of autism knowledge and assessment self-efficacy are subject to expectancy effects and social desirability bias, ultimately reflecting perceived rather than demonstrated competence in autism assessment. Because this study was focused on implementation and past research shows trained PCPs make accurate autism assessments compared to specialists for children with specific characteristics and autism presentations (e.g., McNally Keehn et al., 2023; Penner et al., 2023; Schieltz et al., 2023; Sohl et al., 2023), we did not examine PCP diagnostic accuracy or adherence to diagnostic standards. This limits conclusions that can be drawn about diagnostic accuracy or quality. Uncertainty regarding PCP autism screening practices before enrollment prevents comparisons of assessment tools used before and after the training program. In addition, the study consisted of a small and demographically homogeneous sample of self-selected participants, which likely introduced selection bias that favored highly motivated PCPs who had time to devote to the training program. This also limits generalizability to clinicians and may have influenced self-reported program feasibility outcomes. The small sample of PCPs and 5-month follow-up period limits robust analysis of the program’s sustainability, penetration, and scalability (Proctor et al., 2011). We also did not include a comparison group and did not collect data on diagnostic determinations from the assessments conducted. Finally, caregiver satisfaction with PCP assessment and long-term child outcomes (e.g., therapy use, quality of life) were not examined for the children assessed. Large-scale studies with follow-up spanning longer timeframes are, therefore, needed to determine how well PCPs sustain and increase integration of autism assessment into their practice, caregiver satisfaction with services, and the extent to which patients assessed by PCPs can more easily and quickly access needed services.
Since this study, ongoing work has included a voluntary 1-year follow-up survey that examined PCP assessment activities post-training and implementation barriers to inform future PCP training efforts. Because autism assessments take approximately 2.5-hrs and PCPs are often only able to bill them as a standard visit, this results in a financial loss for PCPs conducting these assessments. To help mitigate this loss, an alternative payment model has also been developed to reimburse participating PCPs for their time spent on autism assessments conducted with patients insured through an Oregon Coordinated Care Organization, though it was not part of this study.
Future research on PCP training programs would benefit from a more comprehensive examination of both implementation and treatment effectiveness, spanning diagnostic accuracy, fidelity, and long-term patient outcomes (e.g., autism therapy referrals and use). In addition, PCP training curricula adapted to focus on racial-ethnic and/or other established autism diagnostic disparities populations (e.g., females, languages other than English) may be future directions (Clarke & Fung, 2022). Geographic disparities in autism services availability (Drahota et al., 2020) also highlight how attempts to target PCP training programs in areas, where there is the lowest density of specialty care practitioners and autism services more generally may help to increase timely diagnosis. Combining PCP training with parent-mediated intervention in low autism service availability areas may further be helpful to better support families in starting down the pathway to autism diagnosis and services. Finally, future work may benefit from studies examining the effectiveness of individual training program components.
Conclusion
This PCP autism assessment training program pilot trial demonstrated feasibility, acceptability, and promising initial outcomes in autism assessment knowledge, confidence, and behavior. Similar programs may be helpful in areas where the autism assessment workforce is limited. Existing models such as this one may be adapted and combined with other autism services and supports to help optimize child, family, and community health.
Supplemental Material
sj-docx-1-aut-10.1177_13623613261457950 – Supplemental material for Short Report: Primary Care Autism Assessment Training Program Pilot Trial
Supplemental material, sj-docx-1-aut-10.1177_13623613261457950 for Short Report: Primary Care Autism Assessment Training Program Pilot Trial by Olivia J. Lindly, Corey Gorgas, Lucas Gooding, Lindsay Blankenship, Alison J. Martin, Raúl A. Vega-Juárez, Katharine E. Zuckerman and Kurt A. Freeman in Autism
Footnotes
Author contributions
Ethical Considerations
All procedures were approved by the relevant institutional review boards, and this study was determined to not be human subjects’ research. This report adheres to ICMJE and international authorship and ethics standards.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Health Share of Oregon, Portland, OR metropolitan area’s Medicaid coordinated care organization.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified data are available upon request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.